
Fluid Management and Electrolyte Balance in Neurosurgical ...
48
Fluid Management and Electrolyte Balance in Neurosurgical Patients Jennifer Willison CNRN, MS, NP Neurosurgical Nurse Consultant May 14, 2016
Transcript of Fluid Management and Electrolyte Balance in Neurosurgical ...
Fluid Management and Electrolyte Balance in Neurosurgical Patients
Jennifer Willison CNRN, MS, NPNeurosurgical Nurse Consultant
May 14, 2016

Objectives
• Review neurologic problems that require special consideration for fluid and electrolyte management.
• Define increased intracranial pressure (IICP).
• List causes of IICP.• Synthesize nursing actions to manage fluid
& electrolyte balance in patients with IICP.

Objectives
• Compare and contrast: syndrome of inappropriate antidiuretic hormone (SIADH) with diabetes incipidus (DI) and cerebral salt wasting (CSW).
• Synthesize nursing actions to manage sodium in a patient with neurologic disease.
• Discuss the use of triple H therapy.

Areas of focus
• Increased intracranial pressure• Pituitary dysfunction: Antidiuretic hormone
(ADH)– Syndrome of inappropriate antidiuretic
hormone (SIADH)– Diabetes Insipidus (DI) – Cerebral Salt Wasting (CSW)
• Sodium balance

Increased Intracranial Pressure
The Monroe-Kellie Doctrine
• The pressure volume relationship amongst and between brain tissue, blood and cerebral spinal fluid (CSF).
• The cranial vault is a fixed volume and it’s constituents (brain tissue, blood, CSF) create a state of equilibrium, so that any increase in one of these must be compensated for by a decrease in another.
Greenberg, Mark, Handbook of Neurosurgery, 7th edition, 2010

What Causes Increased Intracranial Pressure? • Mass effect:
– Tumor– Infarction with edema– Contusions– SDH/EDH– Abscess
• Generalized brain swelling:– Ischemic/anoxic states including stroke– Acute liver failure– Hypertensive encephalopathy– Pseudo tumor cerebri– Hypercarbia
• Obstruction to CSF flow and or absorption:– Hydrocephalus– Chiari malformations– Meningeal disease (infectious, hemorrhagic, cancerous)
• Increase in venous pressure:– Venous sinus thrombosis– Heart failure– Any venous obstruction of blood flow from brain

Understanding Pressures and Data
• Cerebral perfusion pressure (CPP): is the pressure of the blood normally flowing to brain – NL is around 60 mm Hg. – 40 is incompatible with life
• Mean arterial pressure (MAP) calculated by SBP+2(DBP)/3
• Intracranial Pressure (ICP) – NL 5-15 in an adult.
CPP=MAP-ICP
Patient Case 1 IICP
• Patient has suffered a large ischemic stroke• BP=180/90• ICP monitor was placed, ICP=20• Patient is unresponsive on exam• Intubated and sedated• CNE is normal
Patient Case 1 IICP
• What is the cerebral perfusion pressure? • What does this mean for the patient?
• What if BP falls to 80/50?
Patient Case 1 Nursing Management
• What nursing actions are necessary for this patient survive?– BP goal – Monitor MAP– Decrease ICP
– ABC’s

Fluid Administration
• The type of fluid is important as impacts• Cerebral edema• Glucose• Sodium
• CPP
• 0.9% NS is best maintenance fluid• Do not use D5W!

Crystalloids vs. Colloids
• Crystalloids• Isotonic to blood• Mineral salts & water
soluble molecules• Volume replacement• No chance of allergy• 0.09% NS and LR• Minimal cost
• Colloids• Hypotonic • Larger molecules like
albumin and blood itself
• Albumin & FFP• Expensive
Wikipedia Nov. 15, 2015

Sign and Symptoms IICP
• Headache• Vomiting without nausea• Cranial nerve palsies• Altered level of consciousness• Papilledema• Pupil dilation and CNE VI palsy with or without
decreased light reflex• Cushing’s triad (late signs)
– Increased SBP with widening pulse pressure– Bradycardia (more common in pediatrics)– Abnormal respiratory pattern

Neurologic Exam
• You need a baseline exam: – History– Physical Examination– Consciousness; usually tested using the GCS– Cranial Nerves– Motor function– Sensory function– Reflexes: Including gag reflex
– Focus is on ABC’s then LOC, CN function and motor exam.

Neurologic Exam
• Use Glasgow Coma Scale• Best eye opening (none=1 spontaneous=4)• Best verbal response (none=1 oriented=5)• Best Motor response (none=1 obeys=6)
• GCS is standard of care and best indicator of level of consciousness
Normal=15 <8=intubate

Brain Herniation
• a. Midline shift• b. Uncal herniation• c. Tonsillar herniation• d. Decompression thru
opening in bone• e. Coning: herniation
thru foramen magnum.
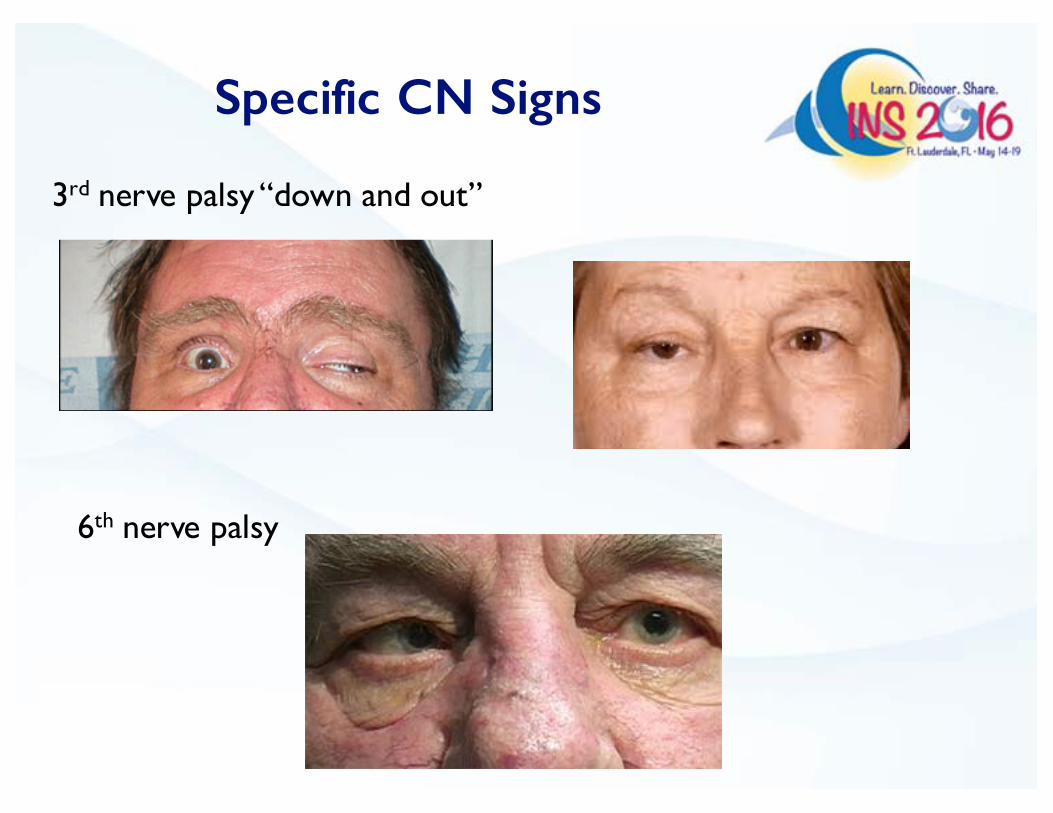
Specific CN Signs
3rd nerve palsy “down and out”
6th nerve palsy

Monitoring
• Direct– Ventriculostomy– Readings greater than 20mm Hg lasting more
than 5 minutes = intracranial hypertension.
• Indirect– Serial neuro checks– Early s/s can be subtle– Late s/s pupillary changes, Cushing's triad

Cushing’s Triad
• Increased systolic BP (widening pulse pressure)
• Decreased pulse• Change in respiratory pattern
– Loss of airway protection
Monitor the ABC’s! Look for pupillary changes…

Management of Acute IICP
§ Must consider STAT CT if sudden change§ HOB up to decrease ICP, check airway, head is midline,
no neck compression§ Make sure patient is sedated and paralyzed§ Hyperventilation (CO2) to PaCO2 30-35 mm hg.§ Direct drainage of CSF via EVD *drain off 3-5 ml CSF§ BP management § Osmotic Therapy§ Dexamethasone & Mannitol§ Na+: use of 3% saline, or 10-30ml of 23.4% saline
§ Surgical decompression

1st Decrease Intracranial Pressure
• Decrease ICP by decreasing the volume of one of the components:
• CSF drainage• Decrease cerebral blood volume
– paCO2 30-35– BP control
• Barbiturate coma• Decrease brain mass• Euvolemia (use 0.9% NS never use D5W!)• Osmolality <320—hypertonic saline, avoid hypotonic
solutions• Sodium goal 145-150• Mannitol-improves blood flow, enhances O2 delivery

2nd Improve Cerebral Perfusion Pressure
• Maintain MAP• Assess for volume loss--bleeding• Administer IV fluids… normal saline • Inotropes, vasopressors• Calcium channel blockers to prevent
vasospasm

3rd Maintain Adequate O2 & Glucose Supply
• PaO2 WNL• Hct >30• Glycemic control - may need insulin gtt.• Maintain cardiac output (CO) with fluids
and or inotropes

4th Prevent Increases in Peripheral Vascular Resistance
(PVR)• Prevent vasospasm• IV fluids, Ca++ Channel blockers• Prevent thrombosis• Anticoagulation if OK!• Prevent hypocapnia (causes cerebrovascular
constriction) • Avoid over sedation• Ventilation to maintain PaO2 and PCO2 in
prescribed parameters

5th Decrease Metabolic Demands
• Prevent seizures• Anticonvulsants
• Pain control*• Induced coma• Comfort
• Normothermia• Cooling blankets
• Use of hypothermiaInduced hypothermia is an acknowledged useful therapy for treating conditions that lead to cell and tissue damage caused by ischemia, including traumatic brain injury, stroke, and cardiac arrest. An accumulating body of clinical evidence, together with several decades of research, has documented that the efficacy of hypothermia is dependent on achieving a reduced temperature in the target tissue before or soon following the ischemia-precipitating event. The temperature must be lowered to within a rather small range of values to effect therapeutic benefit without introducing collateral problems. Rewarming must be much slower than cooling. Many different methods and devices have been used for cooling, with mixed results. The annual review of bio med engineering,2009;11:135-62. doi: 10.1146/annurev-bioeng-061008-124908
Nursing management

Position of HOB
• Raising HOB can improve venous drainage and decrease ICP by gravity, but may also decrease cerebral perfusion so specific HOB orders need to be written for each patient.
• Keep neck in neutral position.
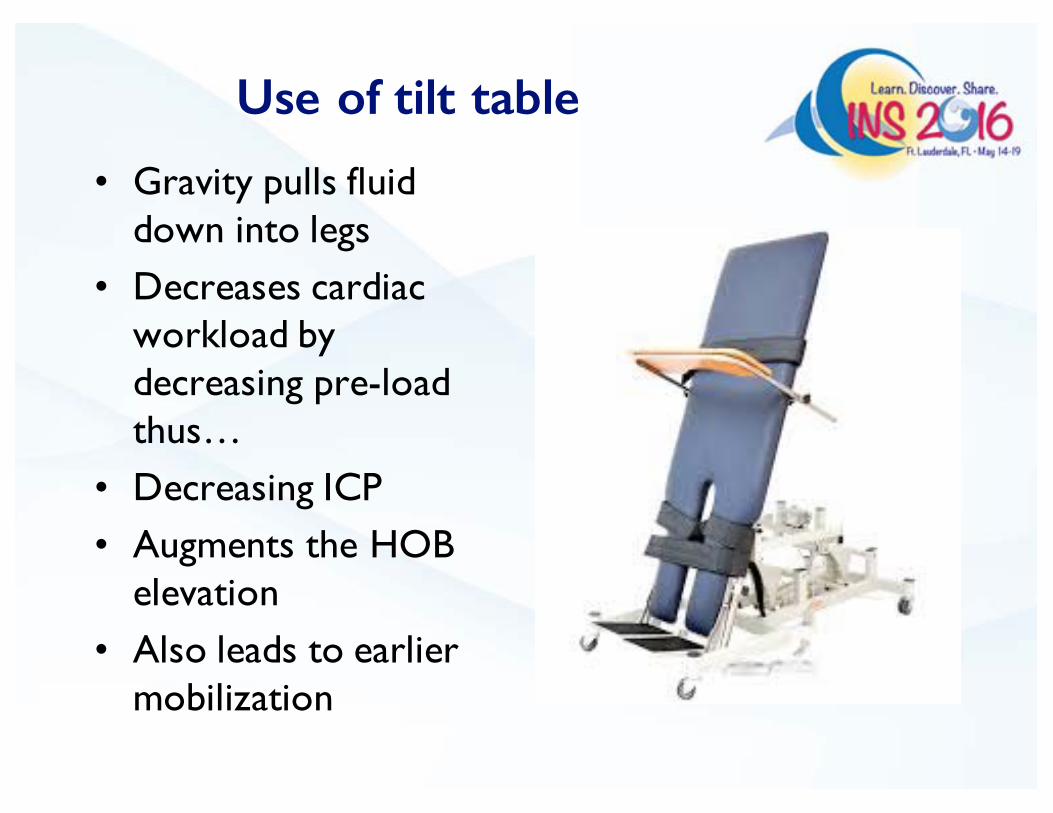
Use of tilt table
• Gravity pulls fluid down into legs
• Decreases cardiac workload by decreasing pre-load thus…
• Decreasing ICP• Augments the HOB
elevation• Also leads to earlier
mobilization

Use of Hyperventilation
• High CO2 levels cause blood vessels in brain to dilate
• Hyperventilation blows off CO2• Vasoconstriction occurs decreasing ICP
however CPP goes down as well• Used short term (20 min) as brain will
adjust to new CO2 levels in 48-72 hrs.
• MUST ALSO MAINTAIN AIRWAY AND ADEQUATE OXYGENATION!

Direct CSF Drainage
• Extra ventricular drain (EVD)
• Bolt• Lumbar drain (why
not?)• Can monitor (patient
who is not awake/alert) and directly drain CSF as well.

Medications
• Dexamethasone reduces cellular edema. *steroid side effects exist.
• Mannitol creates a hypertonic environment in blood to draw fluid out of neurons. *rebound IICP can occur with prolonged use.
– Wean off

Use of Sodium Na+
• Salt tabs• 3% saline IV
Both raise serum Na+ levels creating an osmotic gradient (Na+ and H2O stick together) which draws fluid out of brain tissue decreasing tissue edema.
3% Saline infusion
• Can only be given via central line • Sodium and osmolality must be monitored
every 6 hours• Cannot change sodium too fast • Risk Central Pontine Myelinolysis
– Rare condition that occurs when Na+ is corrected to quickly
– Myelin sheaths are destroyed in brain stem/pons.

Patient Case 2
• 33 yo male in MVC• Primary head injury: multiple areas of
contusion, small SDH and DAI• Responsive after 10 hours, remained
intubated but following commands• Na+ goal 145 • BP goal 120 systolic • Goal were being met and he was stable for
first 7 days after injury.

Patient Case 2 Data
• Brain remained “tight” on CT, no new hemorrhage or infarcts seen
• BP 150/88• Na+ dropped to 132 on weekend on PID 7• Neuro status declined progressing to
herniation syndrome• Urgent decompressive hemicranioectomy
required

Nursing management
• What could have been done to prevent his deterioration?
• How could BP management make a difference?
• What about sodium balance?• This patient did not have an ICP monitor
in, do you think that would have made a difference?

Brain Code: Use of the Salt Bullet 23.4%
• Small volumes of hypertonic saline have been used in a Brain Code to quickly reverse herniation and buy time.
• Used in acute life saving situations only. Must be given by a provider!

Neurologic Effects of Na+
• Hyponatremia– Serum Na+ <130mEq/L.– Anorexia– HA– Irritability
• Severe <125mEq/L– Confusion– Cerebral edema– Seizures– Neurologic
injury/coma/death
• Hypernatremia– Serum sodium >150mEq/L– Less common (1%)
• Central or nephrogenic
– May be asymptomatic or associated with severe disease state
• Irritability• Hyperreflexia• MS changes
– Highly associated with DI

Sodium Imbalance
• Syndrome of inappropriate antidiuretic hormone (SIADH)– Release of ADH in absence of osmotic stimulus– Hypervolemia: true fluid volume overload– Hyponatremia: dilutional effect– Urine osm >100m/osm/L– Can increase ICP– Fluid restriction to treat, oral salt, slow
correction of Na+• Severe cases need NaCl IV replacement

Sodium Imbalance
• Cerebral Salt Wasting – Active excretion of sodium in response to
cerebral disease/injury– True dehydration – Can drop BP – Requires sodium replacement 3% IVF or salt
tabs– Hydrate with 0.9% normal saline at 125 ml/hr
fluid replacement. – Fluticasone

Sodium Imbalance
• Diabetes Insipidus – Low levels of ADH – Increased urine output (low SG <1.003)
leading to true dehydration– Hypernatremia Na+ >150– High serum osmolality – Seen with brain injury, sella region or pituitary
dysfunction – Treat underlying cause! – Fluid replacement and DDAVP
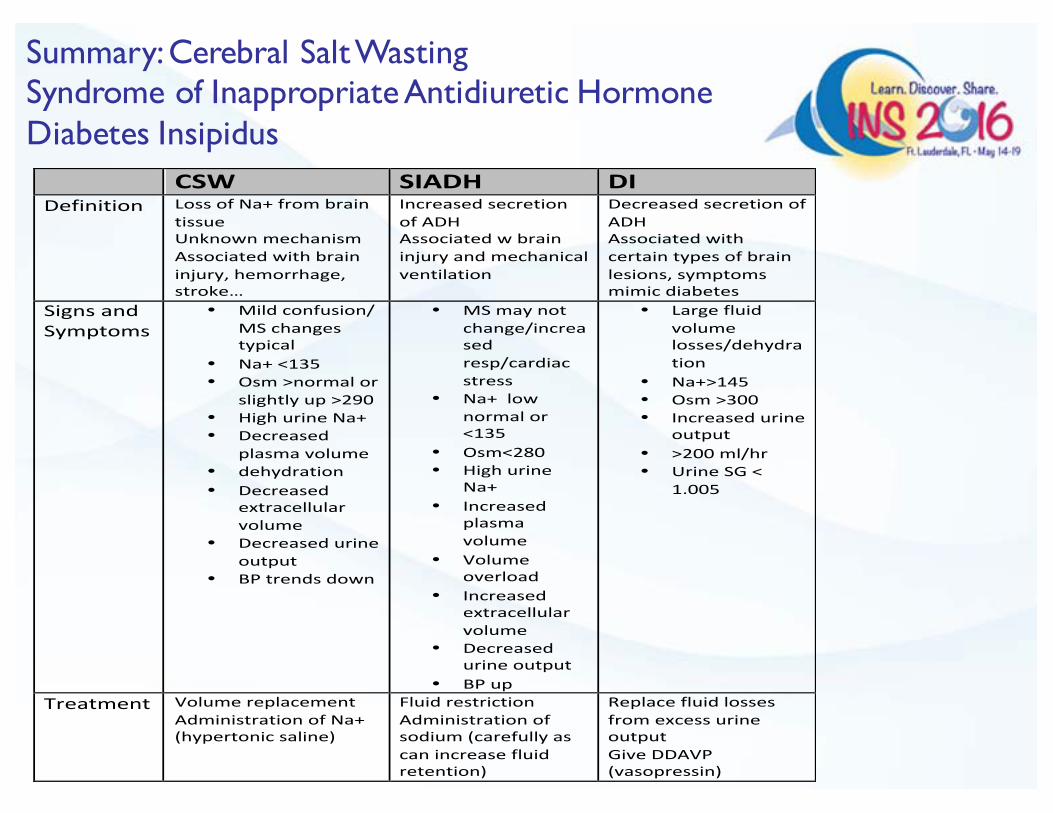
! CSW$ SIADH$ DI$Definition! Loss!of!Na+!from!brain!
tissue!Unknown!mechanism!!Associated!with!brain!injury,!hemorrhage,!stroke…!
Increased!secretion!of!ADH!Associated!w!brain!injury!and!mechanical!ventilation!
Decreased!secretion!of!ADH!!Associated!with!certain!types!of!brain!lesions,!symptoms!mimic!diabetes!
Signs!and!Symptoms!
• Mild!confusion/!MS!changes!typical!
• Na+!<135!• Osm!>normal!or!
slightly!up!>290!• High!urine!Na+!• Decreased!
plasma!volume!• dehydration!• Decreased!
extracellular!volume!
• Decreased!urine!output!
• BP!trends!down!
• MS!may!not!change/increased!resp/cardiac!stress!
• Na+!!low!normal!or!<135!
• Osm<280!• High!urine!
Na+!• Increased!
plasma!volume!
• Volume!overload!!
• Increased!extracellular!volume!
• Decreased!urine!output!
• BP!up!
• Large!fluid!volume!losses/dehydration!!
• Na+>145!• Osm!>300!• Increased!urine!
output!!• >200!ml/hr!• Urine!SG!<!
1.005!
Treatment! Volume!replacement!Administration!of!Na+!(hypertonic!saline)!!
Fluid!restriction!Administration!of!sodium!(carefully!as!can!increase!fluid!retention)!!
Replace!fluid!losses!from!excess!urine!output!Give!DDAVP!(vasopressin)!
!
Summary: Cerebral Salt WastingSyndrome of Inappropriate Antidiuretic Hormone Diabetes Insipidus
Know your Normals
• Na+ 135-145mEq/L• Serum osmolality 275-295 mosm/kg• Uric acid 0.18-0.480 mmol/L• BUN 8-21mg/dL• Creatinine 0.8-1.3mg/dL
Greenberg, Mark, Handbook of Neurosurgery 7th edition, 2010

Clinical Pearl
• Serum uric acid is normal in CSW and low in SIADH so can help distinguish between the two
• So if sodium starts to fall, check the serum uric acid level

Triple H Therapy
• Hypervolemia, hypertension, hemodilution
• Induced hypertension to preserve CPP in patients with severe IICP or with cerebral vasospasm seen in aneurysmal SAH.
• Must be used with caution so as not to increase cerebral edema.
• FVO can cause cardiac stress– Takotsubo syndrome

Summary
• Neurologic patients require careful administration of fluids with close monitoring of fluid balance.
• BP control is critical.• Sodium imbalance can occur in this population
and Na+ values should be monitored and measures should be taken to prevent SIADH, CSW and/or DI.
• Early recognition and treatment improves outcomes.
• The RN should be aware that any patient with a neurologic diagnosis/injury is at higher risk.

QUESTIONS?
Thank you, go enjoy the sunshine!


















