Fluid and Electrolytes. Objectives Identify functions of each electrolyte Identify electrolyte...
111
Fluid and Electrolytes
-
Upload
joan-hopkins -
Category
Documents
-
view
220 -
download
1
Transcript of Fluid and Electrolytes. Objectives Identify functions of each electrolyte Identify electrolyte...
Fluid and Electrolytes
Objectives• Identify functions of each electrolyte• Identify electrolyte levels• Identify signs and symptoms of each
electrolyte; either hypo or hyper.• Identify different buffer systems in body• Identify basic blood gas values and identify
abnormalities• Identify what happens to cells with isotonic,
hypotonic, and hypertonic fluids• Identify differences between whole blood,
packed red blood cells, FFP, and platelets.
Fluid (Hydration)
• Functions of water– Provides an extracellular transportation
route to deliver nutrients to the cells and carry waste products from the cells
– Provides a medium in which chemical reactions, or metabolism, can occur within the cell
– Acts as a lubricant for tissues– Aids in the maintenance of acid-base balance– Assists in heat regulation via evaporation
Fluids (water)
• Functions cont.
– Another important influence on the amt. of water in the body is the amt. of fat on an individual
– Fat contains relatively little water• The more obese an individual, the smaller the % of
body water
– Both obese and older adults are at risk for complications of illness from dehydration or fluid shifts d/t ↓ fluid reserve
Fluids (Water)
• Percentage of body weight that is water depends on several factors.– Age• Premature infant: 90%• Newborn: 70-80%• Twelve years to adult: 50-60%• Older adults: 45-55%
See Figure 22-1 p. 661 FON
Fluid Compartments
• Intracellular Fluid (ICF)– Fluid contained within the cells– 2/3 to 3/4 of all body fluids are in this category
• Extracellular Fluid (ECF)– Fluid contained outside the cells• Interstitial Fluid: fluid located in the spaces between
the cells – Eg. Lymph, CSF, GI secretions
Fluid Compartments
• Extracellular fluid cont.
– Intravascular fluid: fluid that is within the blood vessels (plasma)• Plasma = water + molecules, electrolyes, proteins
– (Minus blood cells and platelets)
Intake and Output
• The normal daily loss of fluids must be met by the normal daily intake
• Daily water intake and output is approx. 2500 ml.
• Fluid leaves the body through the kidneys, lungs, skin, and GI tract
• Water loss is replenished by ingestion of liquids and foods and by metabolism of food
Intake and Output
• Homeostasis– “Relative constancy in the internal environment”– Naturally maintained by adaptive responses
healthy survivalBALANCE– Intake includes: all fluids entering the body– Output includes: all fluids leaving the body
Intake and Output
– Output includes:• Urine• Diarrhea• Vomitus• Ng suction• Drainage bags/wound drainage• Insensible loss: perspiration, expiration
Intake and Output
• Role of the Kidneys in fluid balance– Proper functioning of the kidneys healthy
regulation of fluid balance– Nephrons (kidney cells) filter blood urine output– Kidneys must excrete a minimum of 30ml/hr of
urine in order to eliminate waste products from the body
Intake and Output
– If the body loses 1-2% of its fluid:• Kidneys conserve fluid by reabsorbing more
water from the renal filtrate concentrated urine
– If there is excess body fluid, the kidneys excrete more urine and it is more dilute• This rids the body of excess fluid and conserves
electrolytes
Intake and Output• Nursing Implications:– I and O Record– Daily weight
• Same time • Same amt. of clothing and/or bed linens• Same equipment• Empty all drainage bags
– Checking urine Specific Gravity• Nml range: 1.010 1.030• < 1.010 = dilute urine• > 1.030 = concentrated urine
Intake and Output
• Note: 1 L of fluid = 2.2 lbs (1 kg.)• A weight change of 2.2 lbs will reflect a loss
or gain of 1 L body fluid
Movement of Fluid and Electrolytes
• To carry out cellular functions, substances must cross the semipermeable membrane surrounding each body cell to enter the cell.
• The fat and protein molecules that make up the membrane are arranged so that some substances can enter the cells and others cannot.
Solutions
• Isotonic, hypotonic, hypertonic• “Iso” – “the match”– Has the same solution concentration as another
solution– Ex. : normal saline solution – the concentration of
sodium in the solution nearly equals the concentration of sodium in the blood.
Isotonic fluids
• Can be helpful in hypotensive or hypovolemic patients.
• Can be harmful. There is a risk of fluid overloading, especially in patients with CHF and hypertension.
Solutions
• “hypotonic” solution:– Has a lower solute concentration than another
solution– Ex. “0.5 % NS” is considered hypotonic because the
concentration of sodium in the solution is lower than the concentration of sodium in the pts. blood
– Water is pulled from the vascular compartment into the interstitial fluid compartment. Then, as the interstitial fluid is diluted, this assists in the transpor- tation of water into the adjacent cells.
Hypotonic fluids
• Can be helpful when cells are dehydrated such as a dialysis patient on diuretic therapy. May also be used for hyperglycemic conditions like diabetic ketoacidosis, in which high serum glucose levels draw fluid out of the cells and into the vascular and interstitial compartments.
Solution
• “Hypertonic”:– Has a higher solute concentration than another
solution- for our uses- blood– Ex. A solution of D5W 0.9%NS is considered
hypertonic because the concentration of solution in the solution is greater than the concentration of solutes in the patient’s blood.
Hypertonic Solution
• Pulls fluid and electrolytes from the intracellular and interstitial compartments into the intravascular compartment.
• Can help stabilize blood pressure, increase urine output, and reduce edema.
• Used in head trauma to decrease swelling of the brain.
• Care must be taken with their use. Dangerous in the setting of cell dehydration.
Movement
• A number of processes allow this mass movement of substances into and out of cells
• Transport Processes =– Passive Transport – Active Transport
Movement
• Active Transport Process– Chemical substance called “ATP” (adenosine
triphosphate) is produced in cells• Releases energy cell able to work
– For active transport to occur, need:• Breakdown of ATP + use of related (cell) energy
– Substances actively transported through the cellular membrane includes:• Na⁺, K⁺, Ca⁺⁺, Fe⁺, H⁺ and amino acids• Glucose
Movement
• Passive Transport– Movement of small molecules by diffusion across
a cell membrane– No cellular energy required to move substances
from a ↑ concentration to a ↓concentration• Active Transport– Cellular energy is required to move substances
from ↓ concentration ↑ concentration
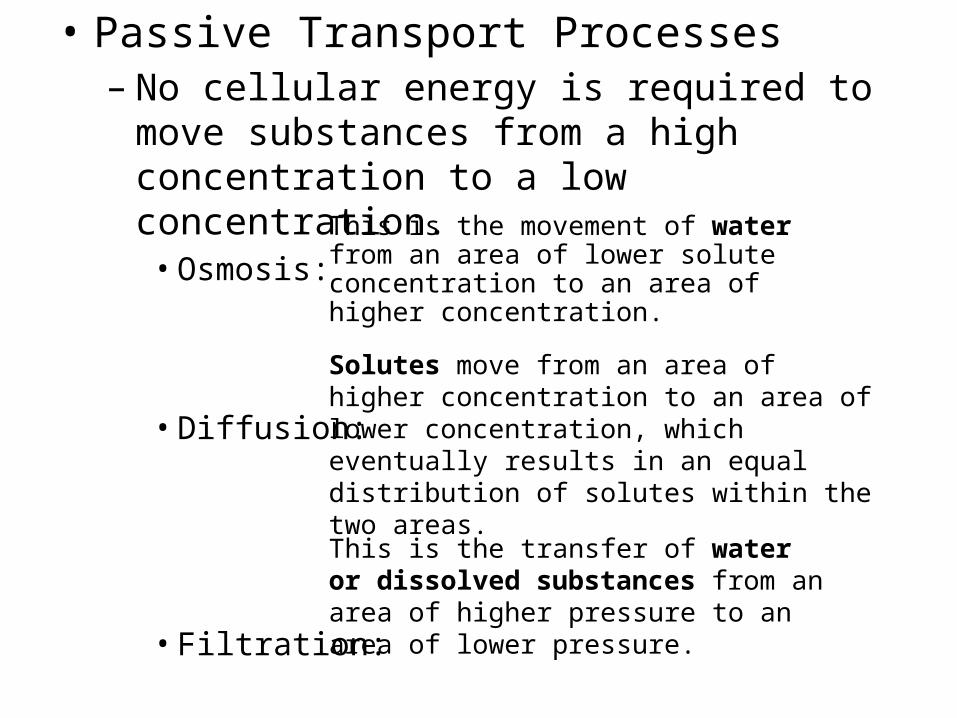
• Passive Transport Processes– No cellular energy is required to move substances
from a high concentration to a low concentration.• Osmosis:
• Diffusion:
• Filtration:
Solutes move from an area of higher concentration to an area of lower concentration, which eventually results in an equal distribution of solutes within the two areas.
This is the movement of water from an area of lower solute concentration to an area of higher concentration.
This is the transfer of water or dissolved substances from an area of higher pressure to an area of lower pressure.
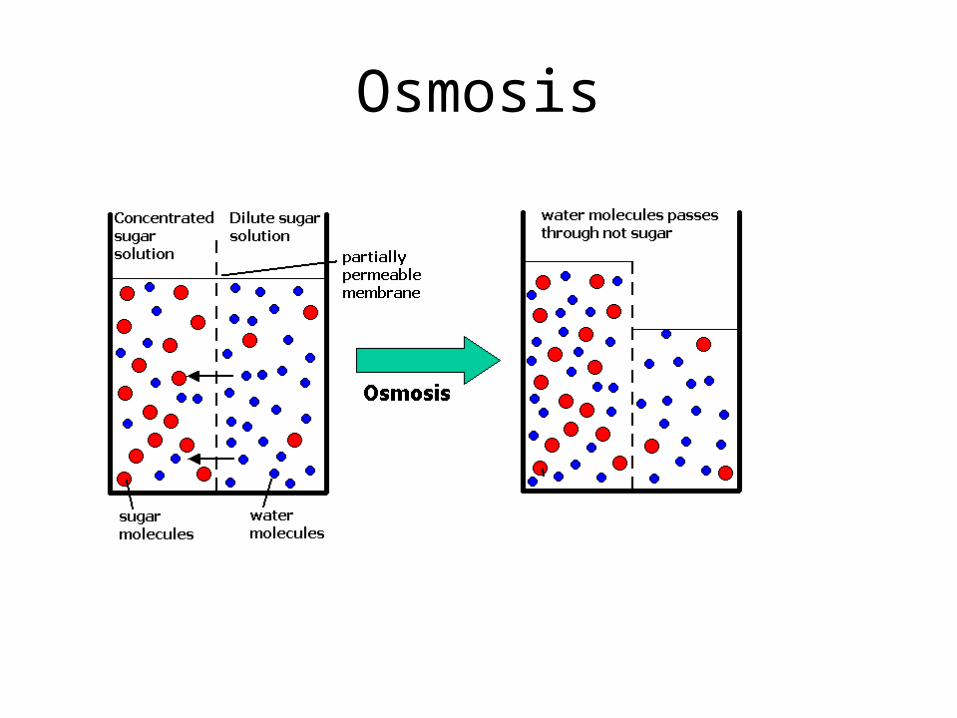
Osmosis
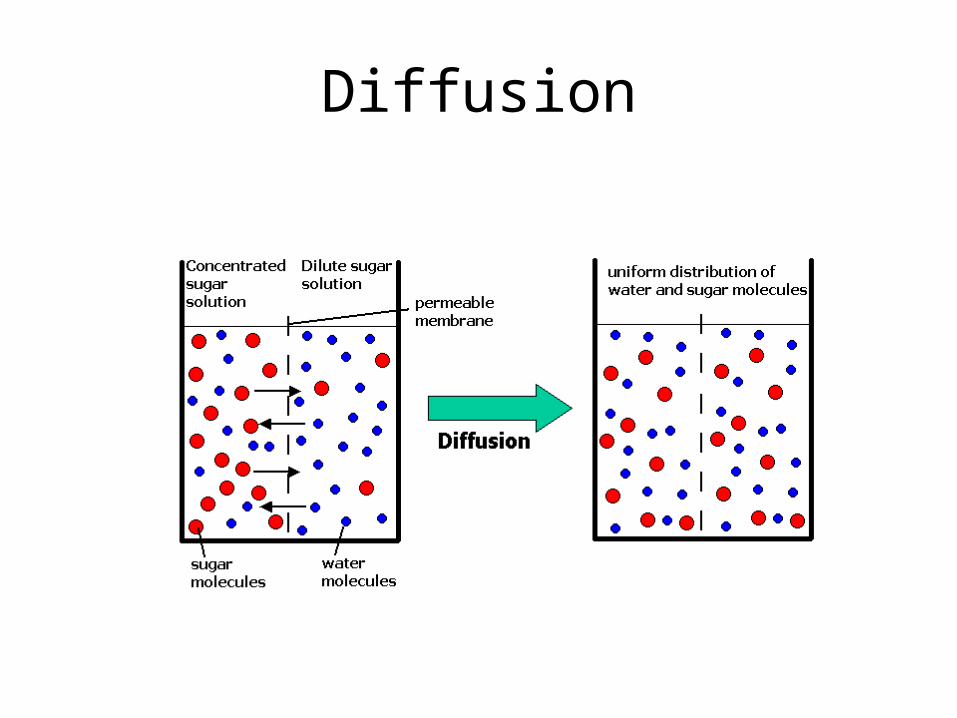
Diffusion
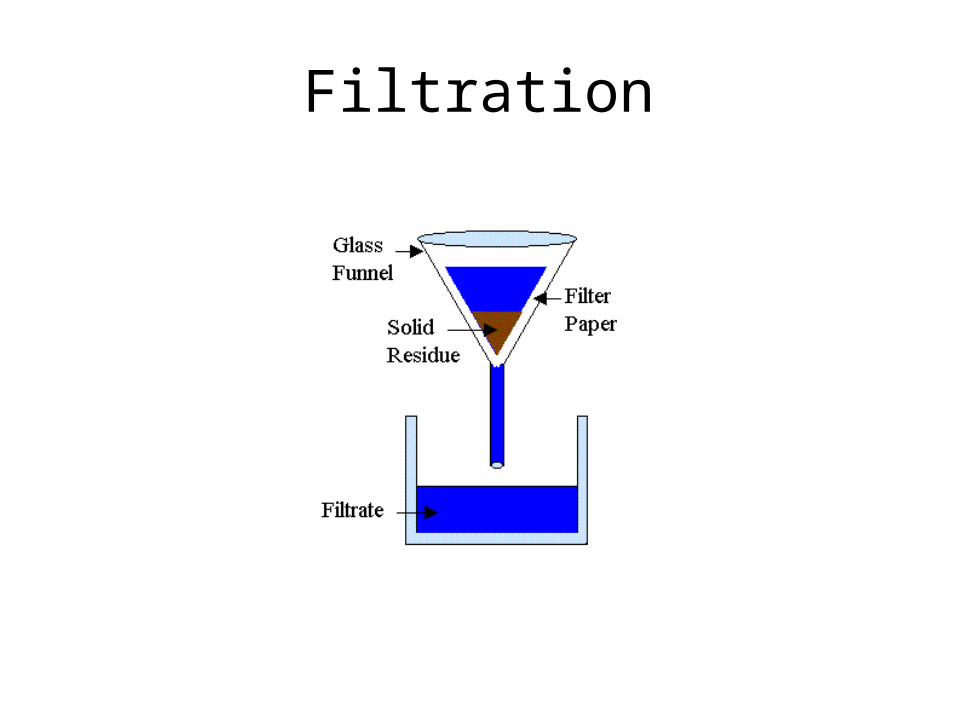
Filtration
Movement
• Filtration: – Ex.: at the capillary level of the circulation– Force behind filtration: hydrostatic pressure = the
force of fluid pressing outward on a vessel wall– The pumping action of the heart is responsible for
the amount of force that causes water and electrolytes to move from the capillaries to the interstitial fluid.
Electrolytes
• As water moves through the compartments of the body, it contains substances that are sometimes called “minerals” or “salts”
• These are technically known as “electrolytes”
• Electrolytes develop tiny electrical charges when they dissolve in water and break up into particles known as ions.
Electrolytes
• Ions develop either a positive or negative electrical charge.
• Cations have a positive charge.• Anions have negative charge.
– A balance exists between the electrolytes; for each positively charged cation, there must be a negatively charged anion.
– Chemical designations: Na+, K+, Cl-, Ca++
Electrolytes
• Measured by their electrical activity– To measure: blood sample drawn– Expressed as “milliequivalents” – mEq• A mEq refers to the combining power of an ion
Sodium (Na⁺)
– Most abundant electrolyte in the body– Normal level: 134 to 142 mEq/L– Major source is the diet; frequently must be limited– Functions of sodium: • regulates water balance, • controls extracellular fluid volume – water follows
sodium in the body• increases cell membrane permeability, • stimulates conduction of nerve impulses,• helps maintain neuromuscular irritability, • controls contractility of muscles
Hyponatremia
• Less than normal concentration of sodium in the blood
• Caused by a sodium loss or a water excess (e.g. excessive hydration)
• With the lower sodium, the body’s compensation results in decreased water excretion
• Dilution of the extracellular fluid, causes a fluid shift into the cells, which in turn causes swelling. The brain is the most susceptible.
Signs and Symptoms of Hyponatremia
• Headache, fatigue, Postural Hypotension• Muscle weakness, twitching or tremors• Apathy, lethargy• Nausea & Vomiting• Abodominal cramping• Death by shock or coma
She had successfully completed a marathon 2 years prior to running in Boston.
By all accounts she looked great all throughout the 19 miles of the 2002 Boston Marathon.
Yet, she became unsteady and collapsed between miles 19 and 20. She was placed in an ambulance and had a seizure on her way to the hospital.
She never regained consciousness. Since Cynthia's passing there have been several reports intended to warn athletes about the dangers of hyponatremia so that runners can be better informed.
Remember , Fluid excess or Sodium loss or Both

Hypernatremia
• Greater than normal concentration of sodium in the blood
• Can occur when there is a sodium excess or a water loss (dehydration)
• Body attempts to correct the imbalance by conserving water through renal reabsorption
• Causes fluid to shift from the cells (high concentration) to the interstitial spaces (low concentration), resulting in cellular dehydration
Signs and Symptoms of Hypernatremia
• Dry, tenacious mucous membrane• Reduced and concentrated urine output• A decrease in the turgor of the skin which
might appear as a sunken dark look to the skin around the eyes
• Restlessness, agitation, confusion, flushed skin• Tachycardia, capllary refill time (>2 seconds),
even cyanosis, mottling, and reticulation
Signs and Symptoms of Hypernatremia
Weight loss
Principal manifestations involve the CNS - confusion, altered mental status, obtundation, stupor, coma, increased neuromuscular irritability (twitching, seizures)
Intracerebral and subarachnoid hemorrhage may result if shrinkage of brain volume leads to tearing of the bridging veins.
Death by cardiac arrythmias
Potassium (K⁺)
• Normal level is 3.5 to 5 mEq/L• Well-balanced diet usually provides adequate
potassium.• The kidneys control the excretion of potassium.– Na⁺ and K⁺ seem to pair off against each other and
the kidneys prefer to conserve Na⁺ and excrete K⁺– Any condition that causes a decrease in urine output K⁺ retention
Potassium (K⁺)
• Function of potassium– Main function is regulation of water and
electrolyte content within the cell.– Required for nerve conduction, muscle function– Involved in cellular enzyme activities– Role in acid-base balance: control hydrogen ion
concentration
Hypokalemia
• Decrease in body’s potassium to a level below 3.5 mEq/L
• The major cause of loss is renal excretion (diuretics).
• The kidneys do not conserve potassium and excrete it even when the body needs it.
• Potassium can be depleted due to excessive GI losses from gastric suctioning or vomiting and the use of diuretics.
• Affects skeletal and cardiac function.
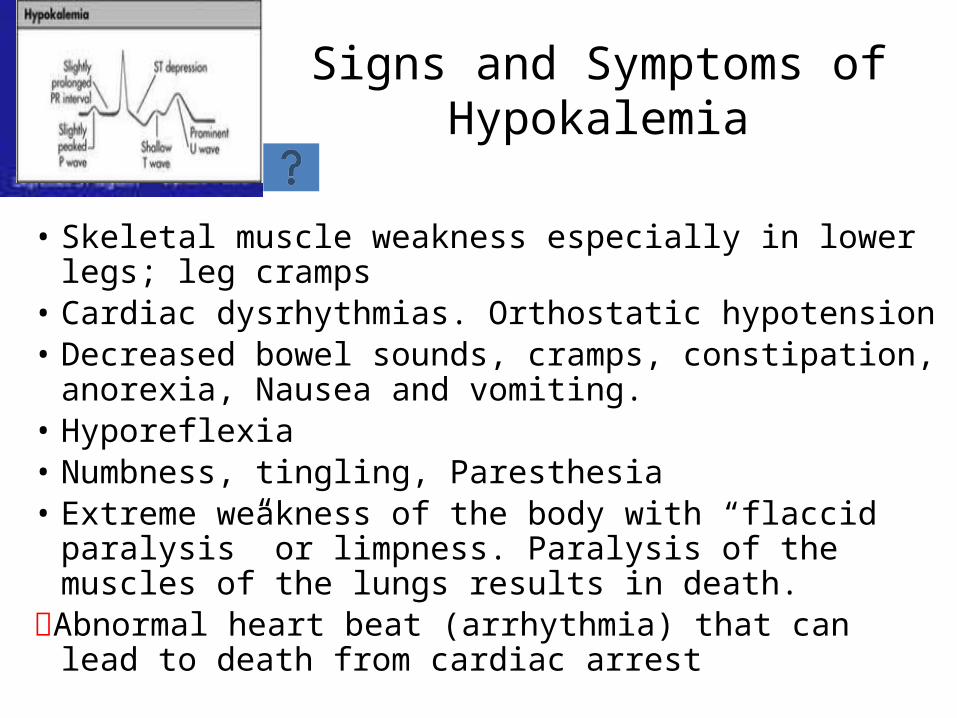
Signs and Symptoms of Hypokalemia
• Skeletal muscle weakness especially in lower legs; leg cramps• Cardiac dysrhythmias. Orthostatic hypotension• Decreased bowel sounds, cramps, constipation, anorexia,
Nausea and vomiting.• Hyporeflexia• Numbness, tingling, Paresthesia• Extreme weakness of the body with “flaccid paralysis” or
limpness. Paralysis of the muscles of the lungs results in death.
Abnormal heart beat (arrhythmia) that can lead to death from cardiac arrest
Hyperkalemia
• Increase in the body’s serum potassium level above 5 mEq/L
• The major cause of excess potassium is renal disease or ingestion, orally or IV
• Severe tissue damage causes potassium to be released from the cell.
• Excessive increase in foods high in potassium can cause serum levels to increase.
Signs and Symptoms of Hyperkalemia
• EKG changes • Irregular heartbeat;
hypotension• Difficulty breathing
• Nausea & Vomiting• Diarrhea, colic• Skeletal muscle
weakness • Tingling, numbness, or
other unusual sensations
• Flaccid paralysis
Hyperkalemia
• The primary cause of morbidity and death is potassium's effect on cardiac function.
• The mortality rate can be as high as 67% if severe hyperkalemia is not treated rapidly.
Chloride (Cl⁻)
• Normal level is 96 to 105 mEq/L.• It is the chief anion in interstitial and intravascular
fluid.• It has the ability to diffuse quickly between the
intracellular and extracellular compartments and combines easily with sodium to form sodium chloride (Na⁺Cl⁻) or with potassium to form potassium chloride (K⁺Cl⁻)
• The main route of excretion is the kidneys
Chloride (Cl⁻
Hypochloremia• Usually occurs when Na⁺ is
lost• (Na⁺ and Cl⁻) are frequently
paired)• From:
– Vomiting – Prolonged Ng suctioning– Fistula drainage
Hyperchloremia• Poss. when bicarbonate
level falls ↑ in Cl⁻ ions
• Chloride imbalances rarely occur independently of other electrolytes no s/sx to identify a Cl⁻ imbalance
Calcium (Ca⁺⁺)
• Normal level is 4.5 mEq/L.• Dietary Intake is source especially milk and cheese• Calcium is deposited in the bones, and• Mobilized as needed to help keep the blood level
constant during any period of insufficient intake.• Vitamin D, calcitonin, and parathyroid hormone
are necessary for absorption and utilization of calcium.
Calcium (Ca⁺⁺)
• 3 considerations are important in blood calcium level:– 1. deposition and resorption of bone– 2. absorption of calcium from GI tract– 3. excretion of calcium in urine and feces
Function of Calcium
– Required for bone and teeth formation– Required for neuromuscular impulse
transmission– Helps regulate normal muscle
contraction/relaxation– Involved in blood clotting– Excitation of cardiac and skeletal muscles– Synthesis and regulation of the endocrine
and exocrine glands
Hypocalcemia
• Develops when the serum level is below 4.5 mEq/L
• A deficiency may be caused by– Infusion of excess amounts of citrated blood
(citrate binds Ca), – Excessive loss through diarrhea, – Inadequate dietary intake, – Surgical removal of parathyroid function, – Pancreatic disease, or small bowel disease.
Hypocalcemia
• Signs and symptoms are neuromuscular irritation and increased excitability and tetany; tingling around mouth, nose, ears, fingers and toes; Hyperactive tendon reflexes
• Spontaneous muscle cramps in hands or feet.
• Prolonged contraction of the respiratory and laryngeal muscles causes stridorous breathing and can cause cyanosis
Hypocalcemia can lead to
• Extrapyramidal symptoms (similar to Parkinson’s)
• Hypotension• Cardiac dysrhythmias
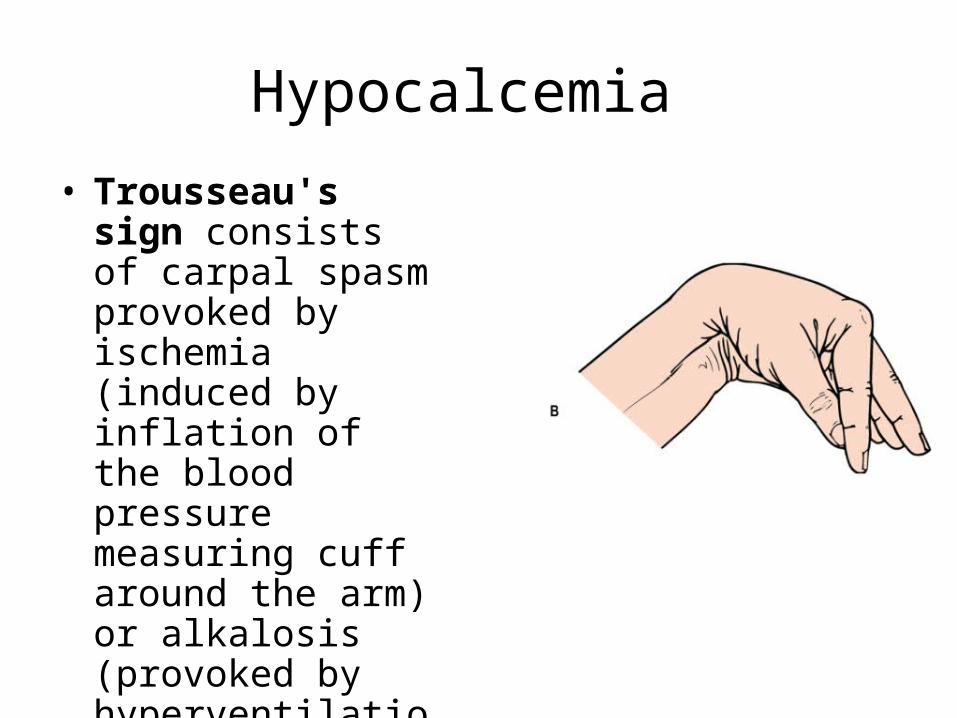
Hypocalcemia
• Trousseau's sign consists of carpal spasm provoked by ischemia (induced by inflation of the blood pressure measuring cuff around the arm) or alkalosis (provoked by hyperventilation for a few minutes)
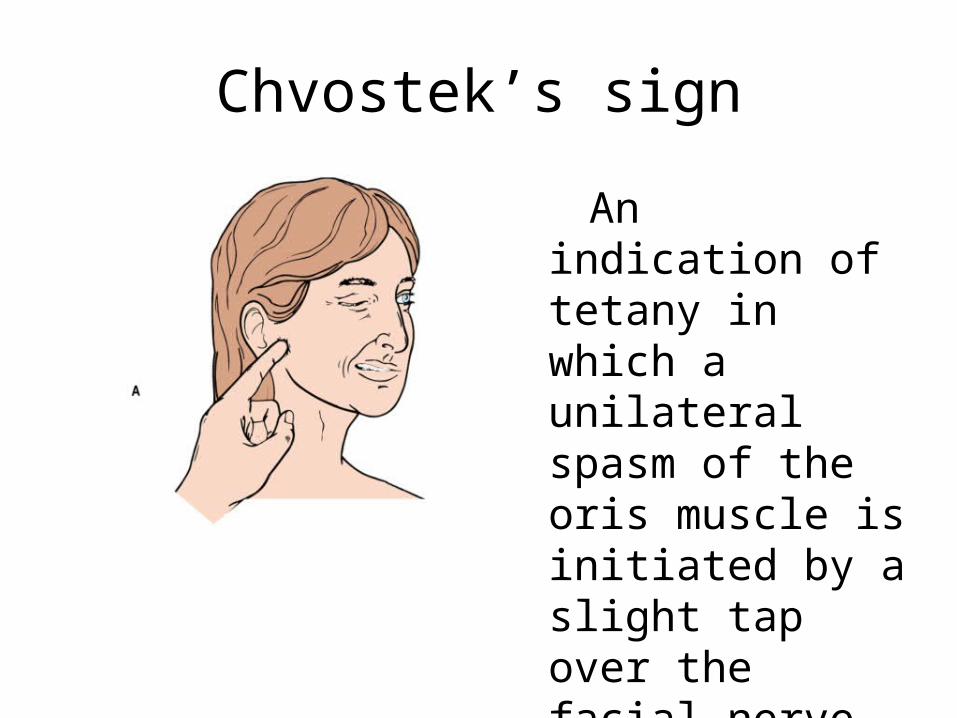
Chvostek’s sign
An indication of tetany in which a unilateral spasm of the oris muscle is initiated by a slight tap over the facial nerve anterior to the external auditory canal.
Hypercalcemia
• It occurs when calcium levels exceed 5.8 mEq/L.• It may occur when calcium stored in the bones
enters the circulation; occurs with immobilization.• An increased intake of calcium or vitamin D also
may be a cause.• Neuromuscular activity is depressed and renal
calculi may develop.
Signs and Symptoms
• Thirst, polyuria• Malaise-fatigue, hypotonicity in smooth and
striated muscles• Anorexia, nausea and/or vomiting • Headache• Bone pain • Cardiac dysrythmias • Death by cardiac arrest
Phosphorus (PO₄⁻)• Chiefly present as hydrogen phosphate (HPO₄⁻)
an intracellular anion• Normal level is 4 mEq/L.• Phosphorus and calcium have an inverse
relationship in the body; an increase in one causes a decrease in the other.
• The majority is found in bones and teeth combined with calcium.
• An adequate intake of vitamin D is necessary for the absorption of both calcium and phosphorus.
Phosphorus
• Hypophosphatemia– Can occur from a dietary insufficiency, impaired
kidney function, or maldistribution of phosphate– Muscle weakness (esp. respiratory muscles)
possible• Hyperphosphatemia– Most commonly occurs as a result of renal
insufficiency; also can occur with increased intake of phosphate or vitamin D
– Signs and symptoms: tetany, numbness and tingling around the mouth, and muscle spasms
Magnesium (Mg⁺⁺)
• Normal level is 1.5 to 2.4 mEq/L.• Although only small amounts are in the blood, it
is important in maintaining normal body function.• The majority is found in bone, muscle, and soft
tissue.• It is commonly distributed in foods: whole grains,
fruits, vegetables, meat, fish, legumes, and dairy products.
• The major route of excretion is the kidneys.
Hypomagnesemia
• Develops when blood levels fall below 1.5 mEq/L• A decreased level often parallels decreased
potassium.• Signs and Symptoms: Similar to hypocalcemia– Mental changes, Paresthesias– Agitation, confusion– Anorexia, N&V – Tetany, Tremors, Hyperactive reflexes, seizure– Arrhythmias, hypotension, tachycardia
Hypermagnesemia
• Develops when blood levels exceed 2.5 mEq/L• It rarely occurs when kidney function is
normal.• 3 Major causes:– impaired renal function– excess magnesium administration (MOM)– diabetic ketoacidosis when there is severe water
loss.
Hypermagnesemia
• An excess of magnesium severely restricts nerve and muscle activity.
• Signs and Symptoms– Hypotension, Vasodilatation– N&V, Thirst– Loss of deep tendon reflexes– Respiratory Depression
• Death by Cardiac arrest
Risk for Fluid and Electrolyte Disorders
• Patients with:– Diarrhea Trauma Patients – Vomiting IV Therapy – Gastric Suction Diuretic Therapy – Edematous Tissue Hormonal Disorders – Surgical Patients Diabetes – Burn Patients Renal Disease
Bicarbonate (HCO₃⁻)
• An anion of the extracellular fluid.• Normal level is 22 to 24 mEq/L.• Major function is the regulation of the acid-
base balance.• It acts as a buffer to neutralize acids in the
body • The kidneys selectively regulate the amount of
bicarbonate retained or excreted.
Carbonic Acid
• Produced by lungs, which results from combining carbon dioxide and water.
• By speeding up or slowing down respirations, the lungs can increase or decrease the C02 in the blood
Blood Buffers
• Considered chemical sponges• Neutralize excess acids or bases• Work within a fraction of a second to
prevent excess change in the hydrogen ion concentration
Acid-Base Balance
• Acid-base balance concerns the homeostasis of the hydrogen ion concentration in the body fluids.
• Normal blood pH is 7.35-7.45.– A pH of 7.0 is “neutral”
• Arterial blood gases determine whether blood serum is acid, neutral, or alkaline
Acid-Base Balance• Carbonic Acid and Sodium bicarbonate form the
most important buffer system• Carbonic Acid is controlled by the respiratory
system H2CO2 CO2 + H2O
• Sodium bicarbonate is controlled by the kidneys– Strong acids are neutralized by sodium bicarbonate
into sodium salts and water– HCl + NaOH H2O + NaCL
Normal Blood Gas Values
• (PaO2): 75-100 mm Hg • (PaCO2): 35-45 mm Hg • (O2CT): 15-23% • (SaO2): 94-100% • (HCO3): 22-26 mEq/liter • pH: 7.35-7.45
Acid-Base Balance
• Acidosis and alkalosis are categorized as metabolic or respiratory, depending on their primary cause.
• Metabolic acidosis and metabolic alkalosis are caused by an imbalance in the production of acids or bases and their excretion by the kidneys.
• Respiratory acidosis and respiratory alkalosis are caused primarily by lung or breathing disorders.
Acid-Base Balance
• 4 primary types of acid-base imbalance:– Respiratory acidosis– Respiratory alkalosis– Metabolic acidosis– Metabolic alkalosis
• 3 systems to keep the pH in the narrow range of normal:– Blood buffers– Respiratory system– kidneys
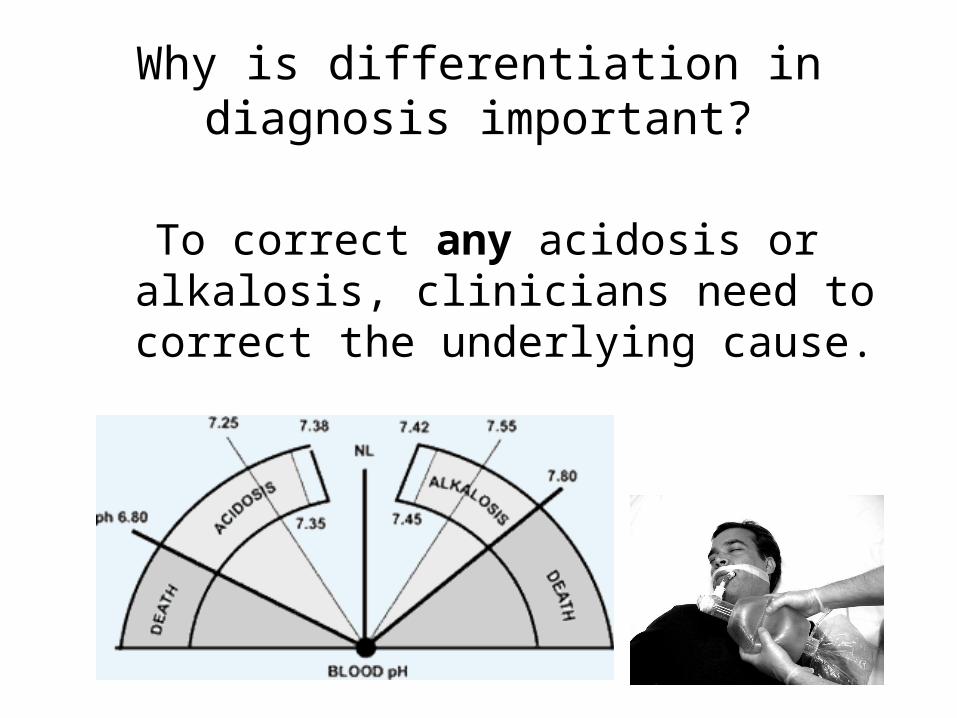
Why is differentiation in diagnosis important?
To correct any acidosis or alkalosis, clinicians need to correct the underlying cause.
Metabolic Acidosis
• Symptoms are aspecific, and diagnosis can be difficult unless the patient presents with clear indications for blood gas sampling
• Physical examination occasionally reveals signs of disease, but is otherwise normal.
Metabolic Acidosis• Symptoms: lethargy, headache, ↓LOC, Kussmaul’s
respiration (deep, rapid), dysrhythmmias, anorexia, n/v/d
• Extreme acidosis leads to neurological and cardiac complications:– Neurological: lethargy, stupor, coma, seizures – Cardiac: ventricular tachycardia, decreased
response to epinephrine; both lead to hypotension.– Treatment is the administration of sodium
bicarbonate.
Respiratory Acidosis
• Respiratory acidosis is a condition that occurs when the lungs cannot remove all of the carbon dioxide produced by the body – i.e. any condition that impairs normal ventilation
• Symptoms may include shortness of breath, shallow respirations, easy fatigue, chronic cough, or wheezing, tachycardia, cardiac dysrhytmias
Respiratory Acidosis
• When respiratory acidosis becomes severe, confusion, irritability, or lethargy may occur
• Treatment is aimed at improving ventilation; correcting the primary condition responsible for the imbalance– IPPB – promote exhalation of CO₂– Adequate hydration– Antibiotic if infection present– bronchodilators
Metabolic Alkalosis
• Metabolic alkalosis may be suspected based on symptoms, but often may not be noticeable.
• Slowed breathing may be the initial symptom. The patient may have episodes of apnea that may go on 15 seconds or longer.
Metabolic Alkalosis
• Slow, shallow respirations• Nausea, vomiting, and diarrhea may also
occur. • Severe cases can lead to convulsions and
coma• Treatment is aimed at the cause
Analyzing ABG Results
• In acidosis, the pH is down (< 7.35)• In alkalosis, the pH is up (> 7.45)
• The respiratory function indicator is the PC02 value
• The metabolic function indicator is the HCO3 level
Respiratory Acidosis
• The pH is down• The pco2 level is up
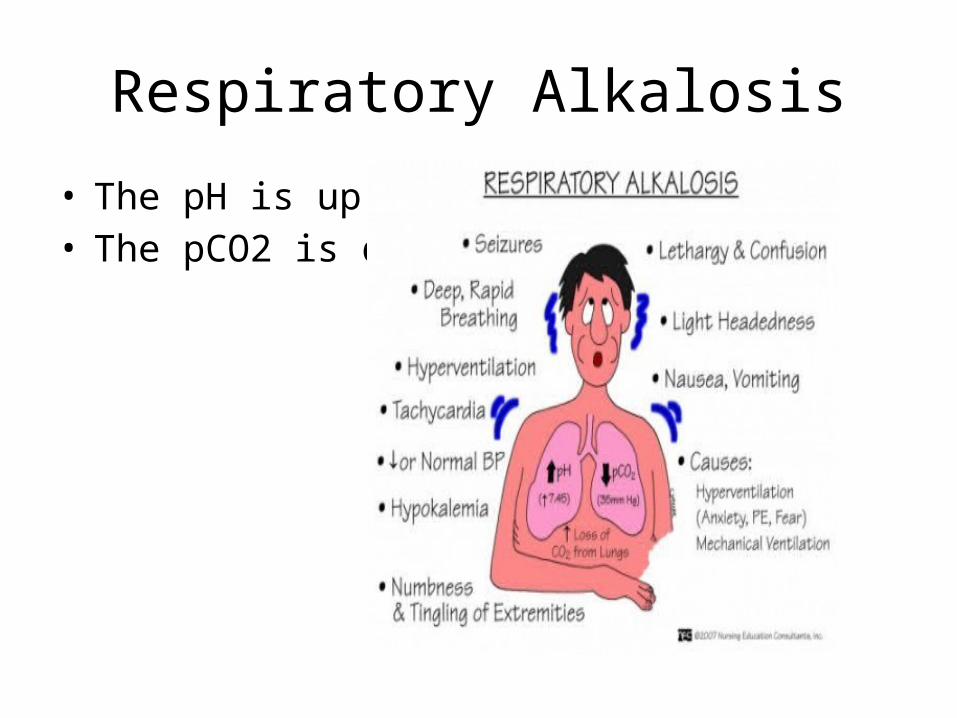
Respiratory Alkalosis
• The pH is up• The pCO2 is down
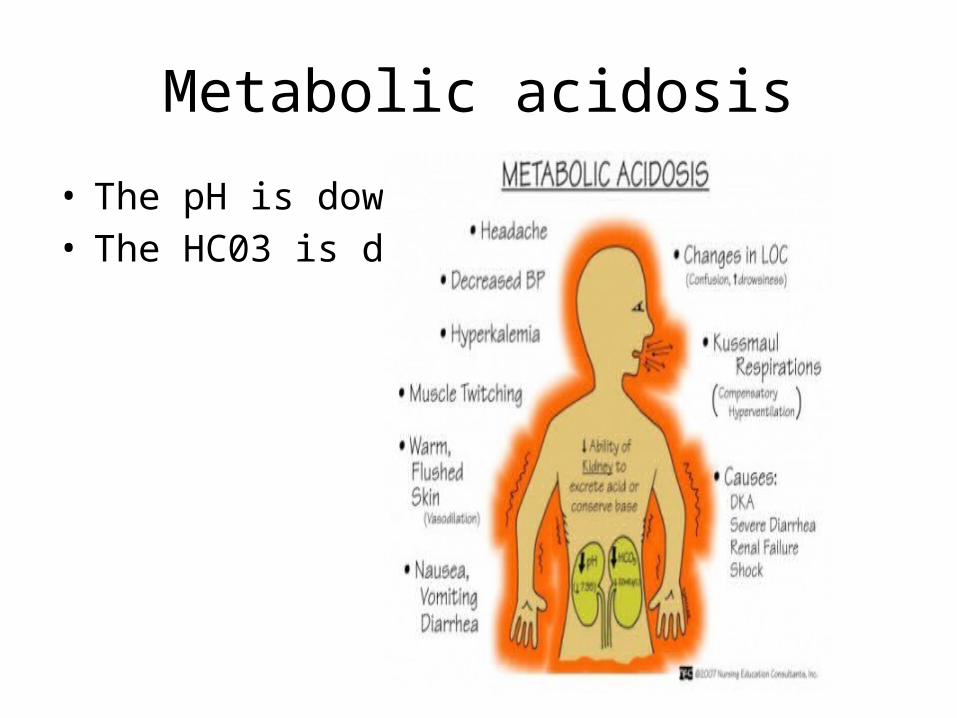
Metabolic acidosis
• The pH is down• The HC03 is down
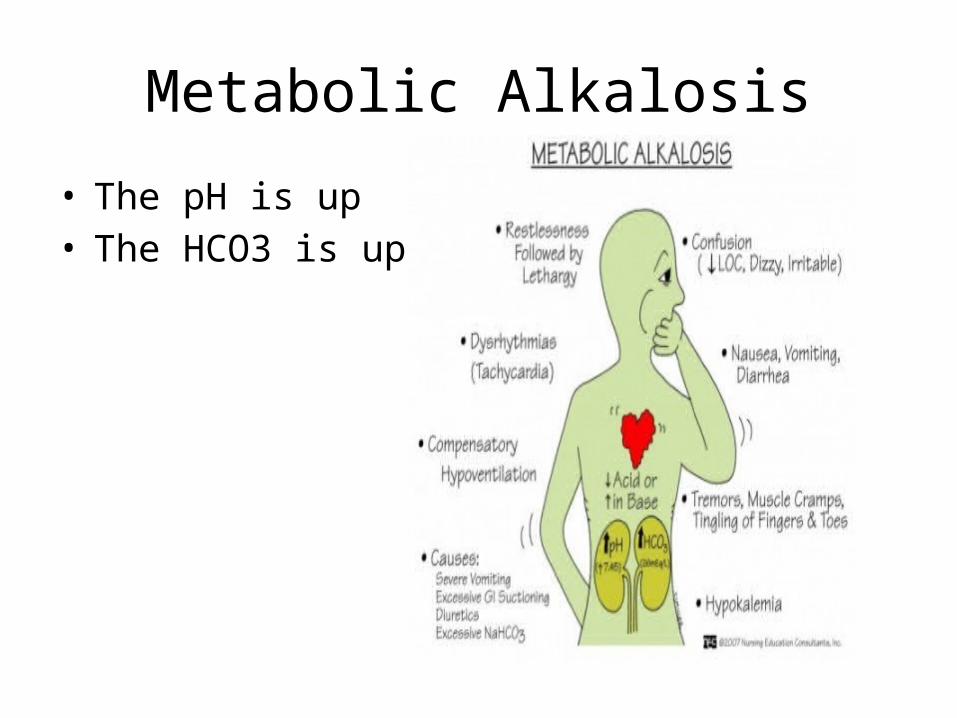
Metabolic Alkalosis
• The pH is up• The HCO3 is up
Blood Products
• Connective tissue without structure• Essential in the sustenance of life• When blood levels are low (anemia)– Perfusion of organs is compromised – Tissue Hypoxia– S/SX• Shortness of breath • Dizziness • Headache • Coldness in the hands and feet • Pale skin • Chest pain
Whole Blood
• Composed of red blood cells, plasma, white blood cells and platelets
• Not the preferred treatment• Seldom used today– Blood is separated into it’s component parts• RBC known as Packed Cells• Plasma which is usually frozen known as FFP• Platelets known as Platelets
Packed Red Blood Cells
• Used to improve the oxygen-carrying capacity for patients with symptomatic anemia unresponsive to medical treatment
• Operative blood loss of 1200 ml or more• Always crossmatched in the ABO and Rh system• Involves double checking with another health
care professional before administration
Packed Red Blood Cells
FFP• Plasma is separated within 8 hours of collection• Can be stored up to a year at -18⁰F or 7 years at -76⁰F• Used primarily to replace lost coagulation factors e.g.
prolonged PT, PTT or Prothrombin• Need to double check with second health care
professional before administration• Indications– Liver disease– Disseminated Intravascular Clotting (DIC)– Induced coagulation anomalies from medical treatments

Fresh Frozen Plasma
Platelets• Used to control or prevent
bleeding from platelet deficiencies– Infections– Chemotherapy– Idiopathic
thrombocytopenia– Cancer in the bone
marrow • Packaged in 60 cc syringe• Need to double check with
second health care professional before administration
Nursing Assessment
• Assess risk for fluid and electrolyte, and acid-base balances– Gather assessment data• Nsg. Hx., I&O, lab studies, physical exam,
Nursing Process• Nursing Diagnoses– Actual or risk for deficient fluid volume – Imbalanced nutrition, less than body requirements– Fluid volume excess– Impaired or risk for impaired skin integrity– Impaired tissue integrity– Impaired oral mucous membrane– Ineffective tissue perfusion– Decreased cardiac output– Impaired gas exchange– Ineffective breathing pattern
MISCELLANEOUS Slides
Electrolytes• Sodium (Cation)
– Maintains osmotic balance– Maintains body fluid volume– Main positive ion in extracellular fluids– Required for nerve conduction– Assists with acid-base balance in the body
• Potassium (Cation)– Required for nerve conduction, muscle function– Major positive ion in intracellular fluid– Primary buffer within the cell– Involved in cellular enzyme activities– Regulates the chemical reaction in production of protein– Regulates neuromuscular activity– Contributes to clotting mechanism
ElectrolytesMagnesium (Cation)
Required for the use of ADP as a source of energyNecessary for the action of numerous enzyme systemsContraction of muscular tissueRegulates neuromuscular activity and the clotting
mechanismCalcium (Cation)
Required for bone formationRequired for neuromuscular impulse transmissionInvolved in blood clottingExcitation of cardiac and skeletal musclesSynthesis and regulation of the endocrine and exocrine
glands
Electrolytes
• Phosphate (Anion)– Essential in carbohydrate and lipid metabolism– Required in bone formation– Assists with acid-base balance – Found in plasma membranes, DNA, RNA and ATP– Assists with storage and transfer of energy
• Chloride (Anion)– Used in formation of HCL in stomach– Assists in fluid balance– Assists with acid-base balance– Most abundant negative ion in extracellular fluid
Sodium and Osmolarity
– Osmolarity is a function of the number of solute particles present per 1 liter of water, expressed as moles(molecules)/liter.
– Normal osmolarity of blood/serum is about 300-310 mOsm/L
– Body fluid osmolarity is regulated • by renal control of water retention or excretion and• by control of water ingestion by the thirst mechanism.
– Since Na+ is the major osmotic solute of the ECF, • conditions of excess water are characterized by
hyponatremia • conditions of water deficit are associated with
hypernatremia
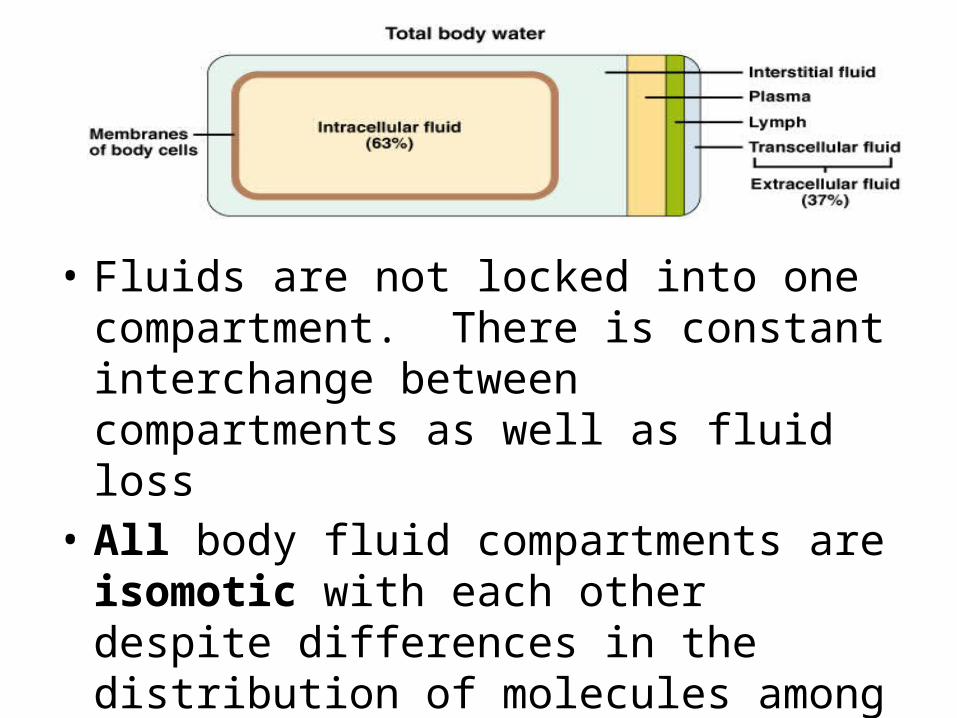
• Fluids are not locked into one compartment. There is constant interchange between compartments as well as fluid loss
• All body fluid compartments are isomotic with each other despite differences in the distribution of molecules among the compartments.
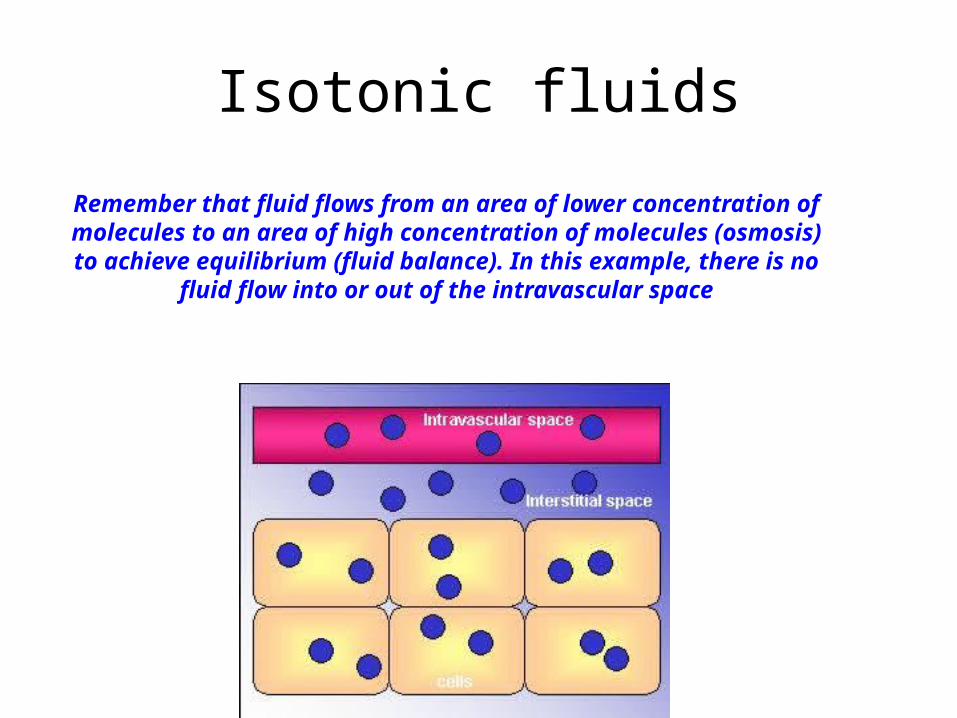
Isotonic fluids
Remember that fluid flows from an area of lower concentration of molecules to an area of high concentration of molecules (osmosis) to achieve
equilibrium (fluid balance). In this example, there is no fluid flow into or out of the intravascular space
Osmolarity of Fluid
• Normal osmolarity of blood/serum is about 300-310 mOsm/L.
• The tonicity of an IV fluid dictates whether the solution should be delivered via the peripheral or central venous route. Hypotonic and hypertonic solutions may be infused in small volumes and into large vessels, where dilution and distribution are rapid.
Osmolarity of Fluid
• When solutions with extremes of tonicity are infused, fluids shift into or out of cells, including endothelial cells of the tunica intima near the catheter tip and blood cells. The resulting changes in the cell size of the vein wall causes the inflammatory and clotting processes to occur, leading to phlebitis and thrombophlebitis.
Hypotonic fluids
• Can be dangerous to use because of the sudden fluid shift from the intravascular space to the cells. This can cause cardiovascular collapse and increased intracranial pressure (ICP) in some patients.
• Normal osmolarity of blood/serum is about 300-310 mOsm/L.
• The generally accepted upper limit for a peripheral IV is 900 mOsm/L. When the osmolarity exceeds 900 mOsm/L, the ability of the peripheral veins to dilute parenteral infusions sufficiently is compromised, and chemical irritation of the vein intima occurs. Admixtures greater than 600 to 900 mOsm/L are associated with a dramatic increase in phlebitis and should be administered via a central line.
• Most people have been taught 0.45% sodium chloride, at 154 mOsm/L, is the lowest osmolarity that should be used via any IV route. Very hypotonic IV solutions such as 1/4 NS cause red blood cells to swell and burst. If a sufficient number of RBC's are so affected, the patient may develop anemia. This condition is usually referred to as hemolytic anemia.
Intake and Output• Intake includes all fluids entering the body– Tube feedings– IV fluids– Blood components– Total parenteral nutrition
• Liquid output includes all fluids leaving the body– Urine– Diarrhea– Vomitus– NG suction– Chest tube drainage– Surgical Wounds drainage
• The importance of accurate record keeping cannot be overstressed when determining a patient’s fluid needs
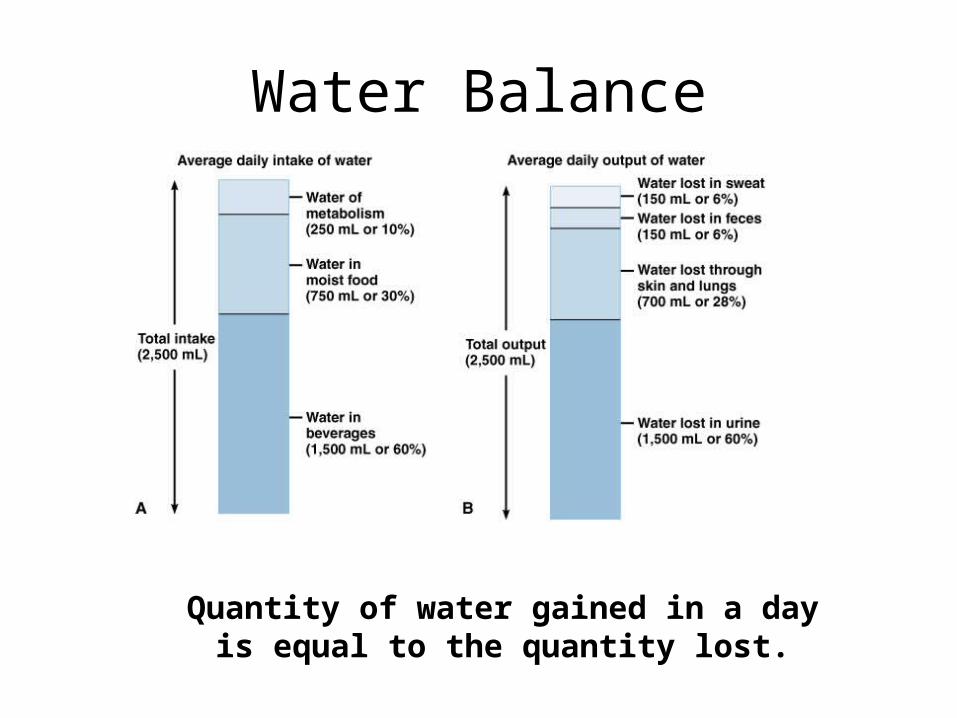
Water Balance
Quantity of water gained in a day is equal to the quantity lost.
Obligatory Water Loss• Kidneys must excrete a minimum of 30 ML/hr of urine
to eliminate waste products from the body• Individuals who are, for whatever reason, deprived of
water have only one defense. They must rely on the kidney’s concentrating mechanism for maximal retention of body water.
• As the process continues, the Na+ concentration increases and intracellular dehydration will follow with its impairment of cellular function, particularly of neural cells.
• In post surgical and/or stressed individuals, this obligatory loss is much higher. WHY?
Adequate Hydration
A simple and accurate method of determining water balance is to weigh the patient under exact conditions.– Weight change of 1 kg will reflect a loss or gain of 1 L
of body fluid.
Two Main Types of Volume Replacement
1. Crystalloid – Isotonic, therefore, effective volume expanders for a short period of time.
However, both the water and the electrolytes in the solution can freely cross the semi-permeable membranes of the vessel walls, but not the cell membranes, into the interstitial space and will achieve equilibrium in two to three hours. They are ideal for patients who need fluid replacement.
– When using an isotonic crystalloid for fluid replacement to support blood pressure from blood loss, remember that 3 mL of isotonic crystalloid solution are needed to replace 1 mL of patient blood. This is because approximately two thirds of the infused crystalloid solution will leave the vascular spaces into the interstitial space in about one hour.
– Generally, a good rule of thumb is that initial crystalloid replacement should not exceed three liters before whole blood is instituted. Continued use of crystalloids increases the risk that the more fluid will occupy the interstitial space. This will result in edema (third spacing) as well as pulmonary edema.
Examples: Lactated Ringer's (LR), NS (normal saline).
2. Colloid – These contain molecules (usually proteins) that are too
large to pass out of the capillary membranes and therefore remain in the vascular compartment. The large protein molecules give colloid solutions a very high osmolarity.
– As a result, they draw fluid from the interstitial and intracellular compartments into the vascular compartment. They work well in reducing edema (as in pulmonary or cerebral edema) while expanding the vascular compartment.
– Colloids can produce dramatic fluid shifts and place the patient in considerable danger if they are not administered in a controlled settings.
Examples: albumin and steroids