
Reactors for Fluid Fluid Reactions Fluid Reactions Fluid-Fluid ...

96/03/27 Book Reading
Fluid and Electrolyte Management of the Surgical Patient
Intern 9031119

Outline
• Body fluids / Disturbance / Therapy
• Electrolytes abnormalities :Sodium, Potassium, Mgnesium, Calcium, Phosphorus
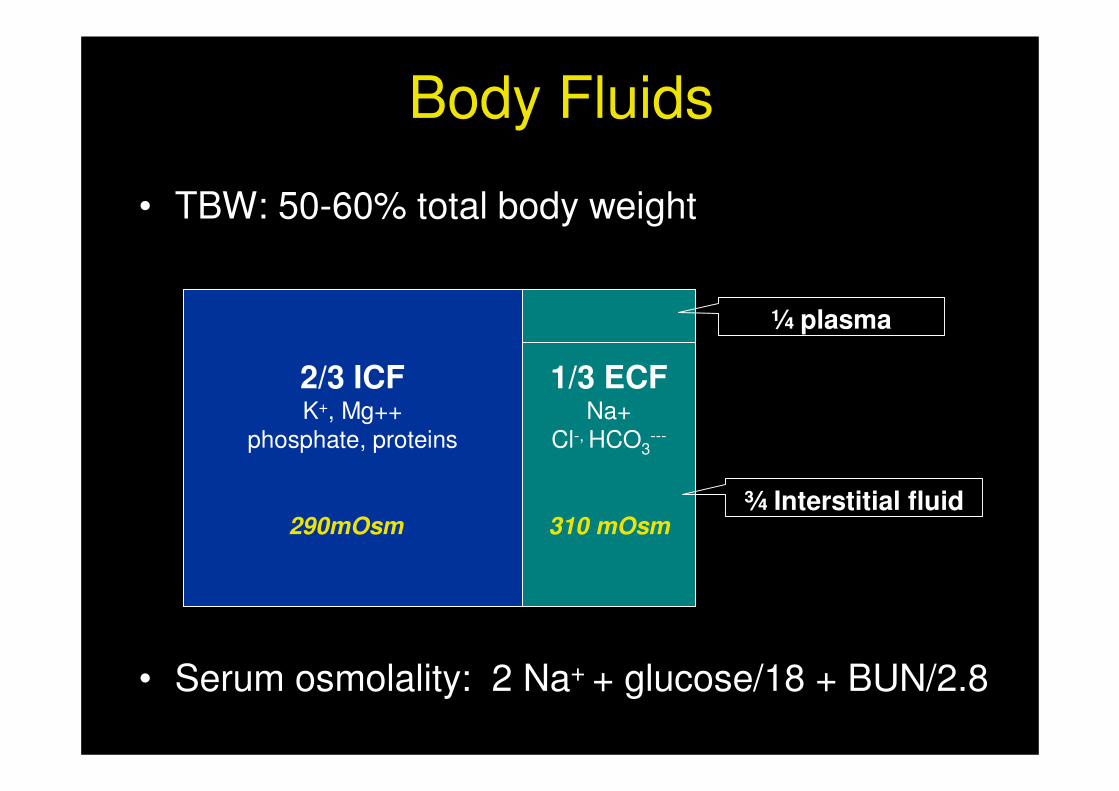
Body Fluids
• TBW: 50-60% total body weight
• Serum osmolality: 2 Na+ + glucose/18 + BUN/2.8
2/3 ICFK+, Mg++
phosphate, proteins
290mOsm
1/3 ECFNa+
Cl-, HCO3---
310 mOsm
¼ plasma
¾ Interstitial fluid

Daily water loss

Disturbance in Fluid Balance
• Extracellular volume deficit� The most common fluid disorder in surgical P’t� Loss of GI fluid ……
• Extracellular volume excess � iatrogenic, renal dysfunction, CHF, cirrhosis…..
Fluid and Electrolyte therapy:
Parenteral solutions
• Isotonic: L/R, N/S� Replace GI loss, ECF deficits
• 0.45 % NaCl + 5 % Dextrose� Maintenance fluid therapy ( post-op ),
Replace ongoing GI loss� 200 kcal / L

Fluid and Electrolyte therapy:
Alternative Resuscitative Fluids
• Hypertonic saline solution ( 3.5, 5 %) � Severe sodium deficit
• Colloids� effective volume expanders ?!
Hydroxyethylstarch
4000 / 70007000
GelatinsHetastarchDextransAlbumin

Pre-operative Fluid Therapy
Pre-Operative Volume Deficits• Obvious GI loss + poor oral intake• Third space losses • Prompt fluid replacement• Isotonic crystalloid
Maintenance Fluids0-10 Kg 100 ml/kg per day11-20 kg 50 ml/kg per day>20 kg 20 ml/kg per day

• Loss of compensatory mechanism due to anesthesia � hypotension
• Continued third space fluid losses
Intraoperative Fluid Therapy
• Bases on current estimated volume status + ongoing fluid loss
• isotonic fluids � 0.45 % saline + dextrose• potassium : renal function, urine output
Post-Operative Fluid Therapy

Body Fluids
• TBW: 50-60% total body weight
• Serum osmolality: 2 Na+ + glucose/18 + BUN/2.8
2/3 ICFK+, Mg++
phosphate, proteins
290mOsm
1/3 ECFNa+
Cl-, HCO3---
310 mOsm
¼ plasma
¾ Interstitial fluid
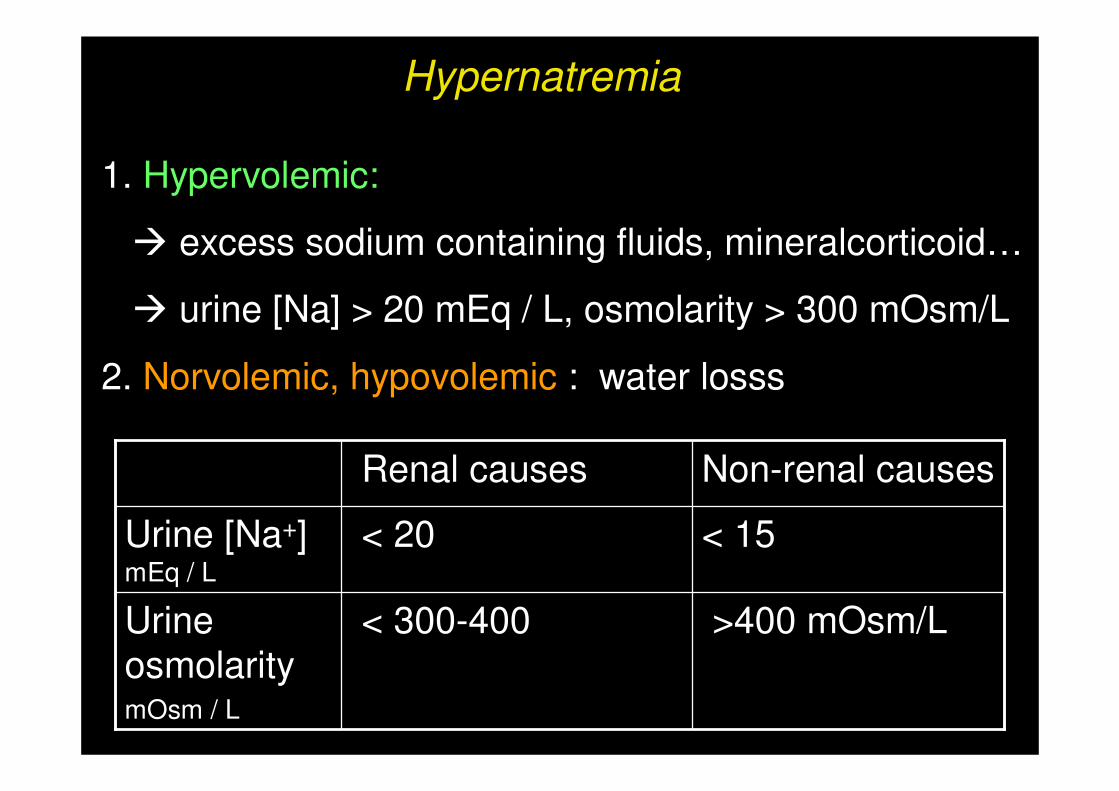
Hypernatremia
1. Hypervolemic:
� excess sodium containing fluids, mineralcorticoid…
� urine [Na] > 20 mEq / L, osmolarity > 300 mOsm/L
2. Norvolemic, hypovolemic : water losss
Urine osmolaritymOsm / L
Urine [Na+] mEq / L
>400 mOsm/L < 300-400
< 15 < 20
Non-renal causesRenal causes

Correction of Electrolytes Abnormalities:Hypernatremia
• S/S : rare, unless > 160 mEq / L, CNS effect
• in serum Na: < 1 meq/L/h, < 12 mEq/L/ 24h
• 5% dextrose � avoid overly rapid correction

Hyponatremia
• Sodium depletion or dilution� Dilution: post-op patient : ADH � Depletion: decrease intake, increase loss
• Excess solute: hyperglycemia, mannitol…
• Pseudohyponatremia:
plasma lipid, protein
Serum Osmolality:2 Na + glucose/18 + BUN/2.8

Hyponatremia
Post-OP P’t� ADH
Corrected [Na] Plasma glucose 100 mg/dL� plasma Na 1.6 meQ/L

• S/S does not occur until serum Na < 120 mEq/L• Neurologic symptoms present � 3% N/S, no more than 1 mEq/L/h
(no more than 8 mEq/L in the first 24 hours )
� serum Na >130 mEq/L or improved symptoms• Asymptomatic : � < 0.5 mEq/L� maximal increase: 12 mEq / L / day
Correction of Electrolytes Abnormalities: Hyponatremia

Potassium Abnormalities
N/V, intestinal colic, diarrhea, weakness, fatigue, respiratory failure,
Excesses intakerelease from cellexcretion by kidney
Hyperkalemia
Ileus, constipation, weakness, fatigue, tendon reflex , paralysis, cardicarrest,,
Inadequate intakeexcretion
Magnesiun depletion
Hypokalemia

EKG pattern in Potassium abnormalities
Merck and The Merck Manuals
• U wave• T-wave
flattening• ST changes • Arrythmia
• peak T• flatten P • PR prolong • wide QRS• VF

• Oral repletion: Mild, asymptomatic
• IV repletion :< 10-20 mEq/ L /h ……. no monitor< 40 mEq/ L /h ……… EKG monitor
Correction of Electrolytes Abnormalities: Hypokalemia

Correction of Electrolytes Abnormalities: Hyperkalemia
• Discontinue all exogenous sources • Cation-exchange resin : kayexalate• Glucose + insulin • Bicarbonate• EKG changes:
calcium choride or calcium gluconate (5-10 ml , 10%)
• Dialysis

Calcium Abnormalities
• Total serum calcium is affected by albumin � 0.8 mg / dL in calceium for 1g/dL in albumin
• Ionized fraction � neuromuscular stability
• PH � affect the ionized level ex acidosis � protein binding � ionized calcium
Calcium abnomalities
• Hypercalcemia:
hyperparathyroidism malignancy
• Hypocalcemia:pancreatitis, massive soft tissue infection, malignancy with osteoclastic activity ….

Correction of Electrolytes Abnormalities:
Calcium abnomalities
• Symptonatic hypercalcemia: ( > 12 mg/dL )
Repleting the associated volume deficit Brisk diuresis with normal saline
• Symptomatic Hypocalcemia:
IV 10 % calcium gluconate (� 7-9 mg/dL )correct the associated deficits in Mg+, K++, PH

• Hypermagnesium:withhold exogeneous soursescorrect volume deficitcalcium chloride (5-10 ml) dialysis
• Hypomagnesium� hypocalcemia � persistent hypokalemiaoral or IV , for severe deficit
Correction of Electrolytes Abnormalities
Magnesium abnormalities

Correction of Electrolytes AbnormalitiesPhosphate Abnormalites
• Hyperphosphatemia:phosphate binder, calcium acetate, dialysis
• Hypophosphatemia: oral or IV supplementation

Thanks*^_^*

Comments


















