FLEXI HEALTH PLAN - alsagrins.ae · Proposal Form and Declaration of Health Questionnaire ......
7
1 | Page Individual and Family Health Insurance ﺑﺭﻧﺎﻣﺞ ﺍﻟﺗﺄﻣﻳﻥ ﺍﻟﻁﺑﻲ ﺍﻟﻔﺭﺩﻱ ﻭﺍﻟﻌﺎﺋﻠﻲProposal Form and Declaration of Health Questionnaire ﻧﻣﻭﺫﺝ ﺍﻻﻟﺗﺣﺎﻕ ﻟﻠﺗﺄﻣﻳﻥ ﺍﻟﻁﺑﻲFLEXI HEALTH PLAN ﺑﺮﻧﺎﻣﺞ ﻓﻠﻴﻜﺴﻲ ﺍﻟﻄﺒﻲINDIVIDUAL AND FAMILY HEALTH INSURANCE PLAN ﺑﺭﻧﺎﻣﺞ ﺍﻟﺗﺄﻣﻳﻥ ﺍﻟﻁﺑﻲ ﺍﻟﻔﺭﺩﻱ ﻭﺍﻟﻌﺎﺋﻠﻲAPPLICATION FORM ﻁﻠﺐ ﺍﻻﻟﺘﺤﺎﻕ
Transcript of FLEXI HEALTH PLAN - alsagrins.ae · Proposal Form and Declaration of Health Questionnaire ......

1 | P a g e
Individual and Family Health Insurance برنامج التأمين الطبي الفردي والعائلي
Proposal Form and Declaration of Health Questionnaire الطبي نموذج االلتحاق للتأمين
FLEXI HEALTH PLAN
برنامج فليكسي الطبي
INDIVIDUAL AND FAMILY HEALTH INSURANCE PLAN
الفردي والعائليبرنامج التأمين الطبي
APPLICATION FORM طلب االلتحاق
2 | P a g e
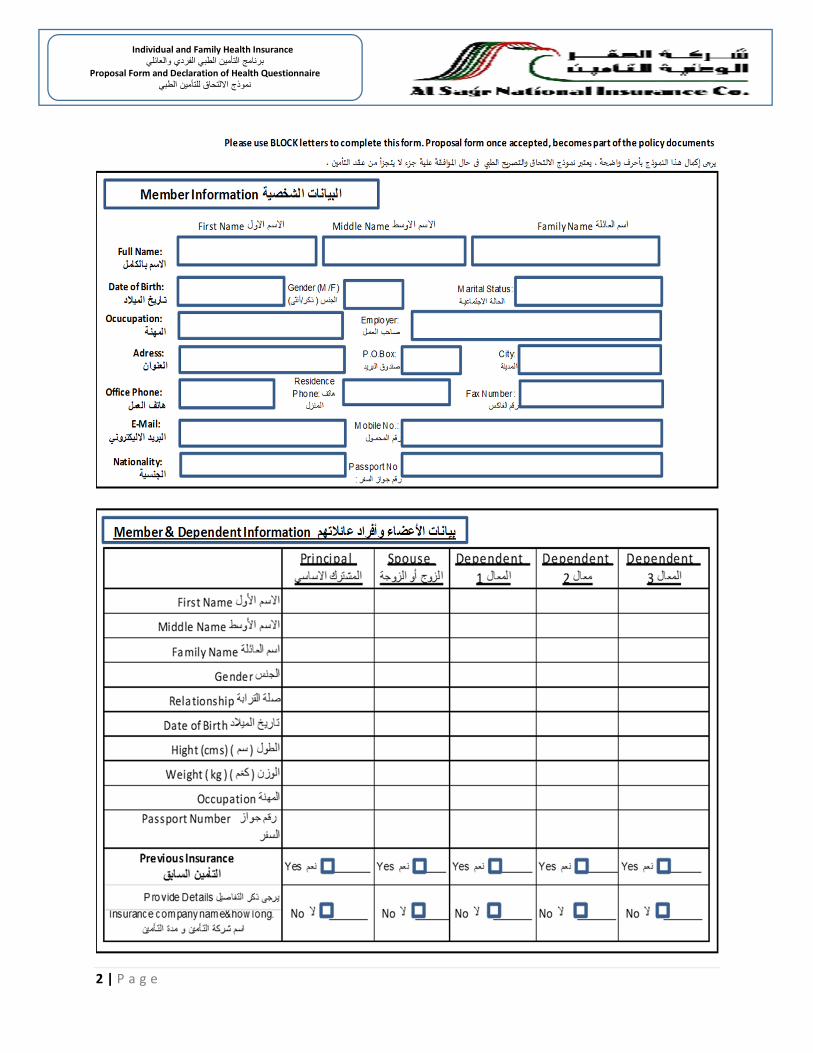
Individual and Family Health Insurance برنامج التأمين الطبي الفردي والعائلي
Proposal Form and Declaration of Health Questionnaire الطبي نموذج االلتحاق للتأمين

3 | P a g e
Individual and Family Health Insurance برنامج التأمين الطبي الفردي والعائلي
Proposal Form and Declaration of Health Questionnaire الطبي نموذج االلتحاق للتأمين
No
الرقمQuestions السؤال
Principal
املش��ك االسا�Spouse
الزوج أو الزوجةDe pe nde nt
المعال 1 De pe nde nt
2 المعال De pe nde nt
المعال 3
No
الرقمQuestions السؤال
Principal
املنتفع
Spouse
الزوج أو الزوجةDe pe nde nt
المعال 1 De pe nde nt
2 المعال De pe nde nt
المعال 3
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
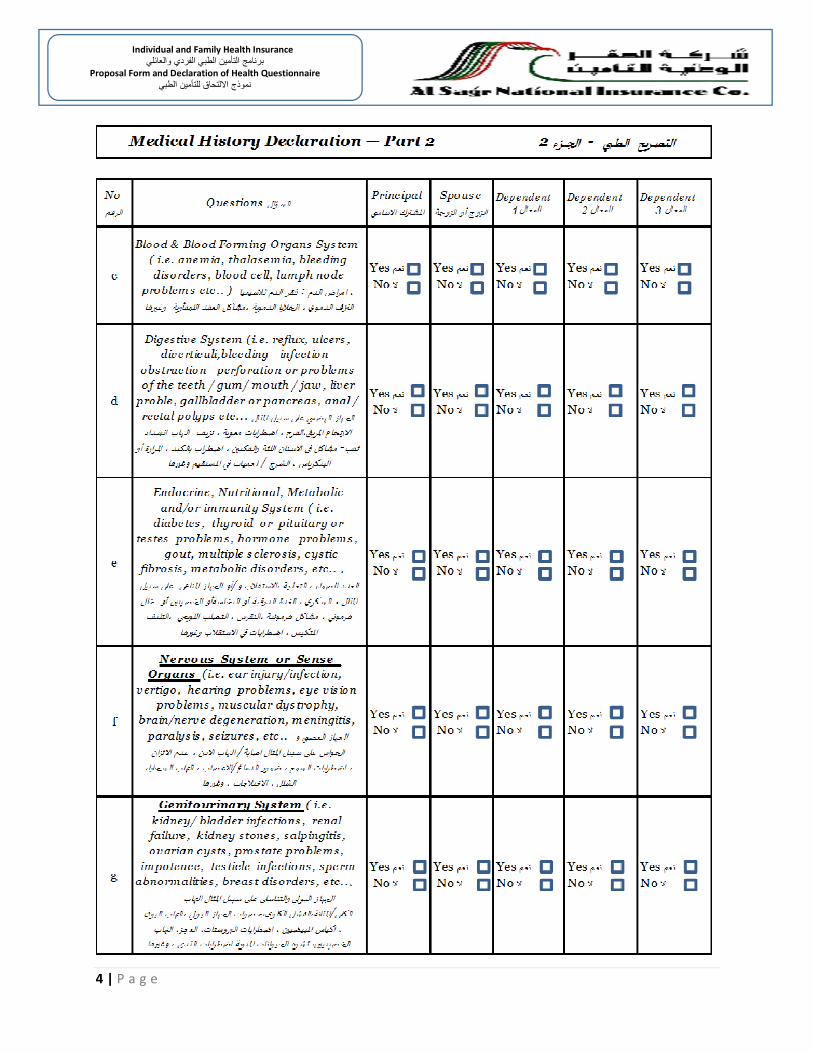
Medical History Declaration — Part 2 2 ا��زء - التصر�ح الط��
a
Musculoskeletal & / or Connective
tissue System (i.e. fracture, jo int or
cartilage problems, back bone
infections , osteoporosis , arthritis ,
rheumatism, etc و ا+*%از العض'& وال%ي#ل العظ /
أو ا+*%از ال:سي89 ع'& س6يل املثال الكسور، اضطرابات املفاصل
@شاشة العظام ، ال=>اب املفاصل والغضارBف ، ال=>اب عظم الظ%ر ،
وغ�D@ا والعظام، االل=>اب الرثوى ،
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Please answer the fo llowing questions which apply to all named applicants. Have you ever been diagnosed or received any treatment ( including
Hospital or surgery ) or felt any disorder or pain or had symptoms including ( please tick the relevant box ). If any o f the below questions is left
unanswered, it will be assumed that the answer is “ No” . False declaration shall result in no coverage and cancellation o f the insurance po licy
under consideration in this application as from the effective date, with no premium refund.
�دمين بااللتحاق بالت�أمين الصحي . هل سبق لك أن تم تشخيص أو تلقى أي عالج، (بم�ا في ذلك الدخول الى المستش�فى أو الجراحة) أو ش�عرت� يرجى اإلجابة على األسئلة التالية التي تنطبق على جمي�ع المتق�ذكورة أدناه (يرجى وضع عالم�ة في الخانة المناس�بة). إذا تم ترك أي م�ن األسئلة أدناه بدون اجابة، سوف يفترض أن الجواب هو " ال". يؤدي� بأي اضطراب أو ألم أو لديك أية أعراض للحاالت الم
التصريح الخاطئ إلى عدم التغطي�ة وإلغ�اء وثيقة الت�أمين اعتبارا م�ن تاريخ بداية عقد الت�أمين الطبي، م�ن دون رد اية أقساط
5
Are you Pregnant now ? If Yes , when
do you expect to deliver? حاليا ؟ حامل @ل أنت , فما @و موعد الوالدة املتوقع ؟ اذا Sانت االجابة �عم
b
Neoplasms, Cancer, Tumors (Specify
type, location, treatment, w hether
malignant or benign ). &Uالسرطان واألورام ير تحديد النوع ، امل#ان و العالجات، فيما اذا Sان من النوع ا+[ب]ث
أو ا+cميد
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Medical History Declaration — Part 1 1 ا��زء - التصر�ح الط��
Yes عم�
No ال
Yes عم�
No ال
4
Do you involve yourself in any
dangerous sporting activities OR ride
motorcycle? وب الدراجاتSاضات خطرة أو رBل تمارس ر@
النارBة ؟
2
Have you ever been declined for health
and/or life insurance? ل سبق أن تم رفض طلبك@ لالنlساب للتامDن الص8j و / أو ا+cياة ؟
3
Have your ever been accepted for
health and/or life insurance on
substandard terms? ل سبق أن تم قبول طلبك@ لالنlساب للتامDن الص8j و / أو ا+cياة nشروط غ�D معيارBة ؟
1
Are you in good health and free from
any deformity or defect? ة جيدةcoل انت ب@ qشو@ات خلقية؟ والqعا�ي من اي خلل أو
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
4 | P a g e
Individual and Family Health Insurance برنامج التأمين الطبي الفردي والعائلي
Proposal Form and Declaration of Health Questionnaire الطبي نموذج االلتحاق للتأمين

5 | P a g e
Individual and Family Health Insurance برنامج التأمين الطبي الفردي والعائلي
Proposal Form and Declaration of Health Questionnaire الطبي نموذج االلتحاق للتأمين
No
الرقمQuestions السؤال
Principal
املنتفع
Spouse
الزوج أو الزوجةDe pe nde nt
المعال 1 De pe nde nt
2 المعال De pe nde nt
المعال 3
Yes عم�
No ال
Yes عم�
No ال
j
Skin Sabcutaneous T issue (i.e.
dermatitis , acne, seborrhea, purities ,
etc. حب (. اال�u*ة وا+*لد ع'& س6يل املثال . ال=>اب ا+*لد ،
وغ�D@ا الشباب،االكزBما، ا+cكة،
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
i
Cardiovascular System ( i.e.
s troke, cerebral ischemia, rheumatic
fever arthroscleros is ,ischemic heart
disease, hypertens ion, heart valve
disease, irregular heart beat,
pulmonary embolism, phlebitis , etc
ا+*%از الوعائية والقلب ع'8 س6يل املثال. ا+*لطات الدماغية والوعاwي
حlشاء القلب ، ارتفاع ضغط الدم ، امراض ، روماتD|م القلب ، ا
وغ�D@ا صمام القلب ، اضطراب نبضات القلب جلطات الرئة،الدوا{& .
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
l Mental Disorders اضطرابات العقلية
Medical History Declaration — Part 2 2 ح الط�� - ا��زء�التصر
h Respiratory System (i.e.s inusitis ,
allergies , tonsillitis/laryngitis ,
bronchitis , emphysema, etc..
ا+*%از التنف~ ع'& س6يل املثال ال=>اب ا+*يوب ، ا+cساسية ، ال=>اب
وغ�D@ا اللوزتيDن/ الرغامي ، ال=>اب القصبات ، االختناق ،
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
k
Pregnancy,complication of
pregnancy,child birth and the
puerperium .مل،املواليد،النفاسc+مل ومضاعفات اc+ا
ماnعد الوالدة
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
nCongenital anomalies , hereditary
diseases الlشو@ات واالمراض ا+[لقية والوراثية
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
mInfectious and paras itic diseases االل=>ابات
والديدان والطفيليات
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
p Injury and poisoning سمماتlوال ا+*روح Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
oCertain conditions originating in the
perinatal ت:شأ قبل والدتك االت ال�c+عض اn
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
q
Previous medical / surgical
hospitalization, procedures and
operations ( if any ) حية اجراءات طبية سابقة / جرا
املسlشفى ، اجراءات و عمليات ( ان وجد ) .داخل
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
r
Have you ever been tested positive
for HIV (AIDS) and for other infectious
diseases (e.g. Hepatitis B, C ) or Have
any medical condi- tion or symptoms
indicative of HIV infection or AIDS? ل@
ص االيدز صات وSانت النlيجة ايجابية مثل - فح قمت nعمل اية فحو
ب،ج ) أو لديك صات المراض معدية ( مثل ال=>اب الكبد و أية فحو
ص املناعة املكlسبة حالة أو عرض qش�D لوجود ايدز أو نق
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال
Yes عم�
No ال

6 | P a g e
Individual and Family Health Insurance برنامج التأمين الطبي الفردي والعائلي
Proposal Form and Declaration of Health Questionnaire الطبي نموذج االلتحاق للتأمين
7 | P a g e
Individual and Family Health Insurance برنامج التأمين الطبي الفردي والعائلي
Proposal Form and Declaration of Health Questionnaire الطبي نموذج االلتحاق للتأمين
Chronic Diseases:
A disease with one or more of the following characteristics: lasts 3 months or more, leaves residual disability, is caused by non-reversible pathological alteration, requires special training of the patient for rehabilitation, or may require la long period of supervision, observation, or case.
In case the answer is YES to any of the conditions/diseases above, please specify full details on additional questionnaire attached to this application form.
Declaration: I/We hereby declare with respect to both, myself and my dependents that to the best of my knowledge and belief, the state ment on application are full, true and correct and have declared all material facts related to this application.
I/We understand that non-disclosure or misrepresentation of any material fact may invalidate the quoted terms. I/We agree that all the documents issued in connection with the policy shall be read together.
If my application gets accepted, I/We agree to be bound by the terms and conditions of the policy. I/We hereby authorize any doctor, Hospital, Clinic or Medical Provider, any Insurance Company or any other Company, institution or any other person who has any record or information about me and/or any of my family members to provider Al Sagr National Insurance Company, with the complete information, including copies of their records with reference to any sickness or accident, any treatment, examination, advice or hospitalization or any other medical information required by Al Sagr National Insurance Company.
The Coverage of Health Services provided by Al Sagr National Insurance Company is described in the policy wording. By signing this for, I/We acknowledge that I/We read, understood and agree to the terms and conditions as stated in the policy wording.
I/We agree that after acceptance of the quoted premiums in the quotation, I/We shall be liable to pay all the premiums to Al
Sagr National Insurance Company as per the specified and selected plan of our choice. Al Sagr National Insurance Company reserves the right to reject any authorization/claims reques t for conditions (pre- existing, chronic) not declared by the applicant at the inception of the policy.
االمراض المزمنة :
باثولوجي ال يمكن تصحيحه، يتطلب تدريب خاص للمريض ٍالعادة التأهيل ، يتصف بواحدة أو اكثر من الصفات التالية: مرض يدوم ثالث أشهر أو أكثر ، ويترك عجز ، وينجم عن تغيير أو قد يتطلب فترة طويلة من االشراف و المراقبة .
بي .في حال االجابة بنعم على أي من الحاالت / االًمراض المذكوره أعاله ، يرجى تحديد التفاصيل الكاملة في المكان المخصص من التصريح الط
االقرار :
حة و حقيقية و بانني افصحت عن جميع الحقائق قر (نُقر) أنا (نحن) الموقع أدناه باالصالة عن نفسي و بالنيابة عن جميع المعالين لدي بأن جميع االفصاحات في هذا الطلب كاملة و صحيأ الخاصة بهذا الطلب على حد علمي و معرفتي .
متعلقة بهذا الطلب قد يؤدي الى اٍبطال شروط عرض التأمين . وأوافق (نوافق) بأن جميع الوثائق الصادرة والمتعلقة بعقد التأمين يجب أنتحريف للحقائق ال أواٍنني على علم بأن اًي اخفاء تقرأ معاً .
مؤسسة أوي شركة أا أوجهة طبية، أو شركة تأمين حكام عقد التأمين و أفوض (نفوض)اًي طبيب، مستشفى ،عيادة،أوأفي حال الموافقة على طلبي ، أوافق (نوافق) على االلتزام بشروط و أوحادث أولشركة الصقر الوطنية للتأمين بما في ذلك تقديم نسخة عن سجل اًي مرض كامل عن اًي من اًفراد عائلتي تقديمها بشكل أوسجل طبي عني و/ أوشخص لديه اًي معلومات أو
للمستشفى أو أي معلومات طبية اخرى تطلبها شركة الصقر الوطنية للتأمين .اٍدخال أواٍ ستشارة طبية أوفحص أومعالجة
(نعترف) بأنني (بأننا) قرأت و فهمت و أن التغطيات الخاصة بالخدمات الطبية المقدمة من شركة الصقر للتأمين مشروحة ضمن عقد التأمين الطبي . بالتوقيع على هذا الطلب ،أعترفام عقد التأمين الصحي .أوافق على جميع شروط و أحك
منافع التي تم اختيارها من بأن بعد قبول أقساط عرض التأمين ، فٍانني (اٍننا) مسؤول عن تسديد جميع أقساط التاًمين لشركة الصقر الوطنية للتأمين بحسب الخطة وال و أوافق (نوافق) قبلي(قبلنا) .
موافقة / مطالبة لحاالت (سابقة للتأمين/ مزمنة) لم يتم التصريح عنها بواسطة مقدم الطلب عند بداية التأمين . طلب أيوتحتفظ شركة الصقر الوطنية للتأمين بحقها برفض
Name of Applicant & signature :
اٍسم معبئ الطلب والتوقيعDate & place of signing: مكان وتاريخ التوقيع
Witness Name & signature:
: اٍسم الشاهد والتوقيع