FlashPath - Lung - Carcinoid Tumor
25
FLASHPATH Hazem Ali
Transcript of FlashPath - Lung - Carcinoid Tumor

FLASHPATHH a z e m A l i

CARCINOID TUMOR
H a z e m A l i

CLINICAL
Carcinoid tumors are part of the spectrum of neuroendocrine lung tumors that includes:• Large cell neuroendocrine carcinoma• Small cell carcinoma• Typical carcinoid• Atypical carcinoid

CLINICAL• Well-differentiated neuroendocrine carcinoma
– Locally invasive, rarely metastasizes• < 5% of all primary lung cancers
– Lung being the second most common site after the gastrointestinal tract• More common in adults
– can occur in children• Central vs Peripheral carcinoid:
– Central: obstructive symptoms due to mass effect• Cough, wheezing, dyspnea, chest pain, hemoptysis, and recurrent pneumonia
– Peripheral: usually asymptomatic

CLINICAL
• Typical vs Atypical carcinoids:– Typical carcinoid:
• Rarely metastasize• 90% 5-year survival rate after complete resection (better prognosis)
– Atypical carcinoid:• Greater propensity for metastasis• 60% 5-year survival rate (less better prognosis)
• Note that pancreas and intestine do not have an “atypical” category as seen in the lung. Nevertheless, some pathologists do flag intestinal and pancreatic lesions as “atypical” based on the lung criteria (see later)

CLINICAL• Lung Carcinoid tumors are rarely associated with smoking
– But small cell and large cell neuroendocrine carcinomas are highly associated with smoking
• Lung Carcinoid tumors rarely occur in MEN I– MEN I association highest for mediastinum carcinoid, followed by pancreas, and low for
lung and ileum.
• Lung Carcinoid tumor rarely present with Carcinoid syndrome or Cushing syndrome– About 10 % of pulmonary carcinoids have secretory functions

GROSS
• Well-demarcated• Nodular, Fungating• Tan / yellow mass, glistening cut surface• Usually measure less than 2 cm in diameter
– But should be > 0.5 cm in diameter• The overlying mucosa usually intact
– May be ulcerated in some cases

GROSSCentral vs peripheral carcinoid:• Central (70%):
– Arise in the main or major bronchi and have endobronchial component– Solitary– Dumbbell-shaped: when penetrate the bronchial wall to fan out in the peri-
bronchial tissue– Shows post-obstructive changes distally
• Peripheral (30%):– Usually sub-pleural– Multiple– No association with a bronchus, No post-obstructive changes distally– Discovered incidentally as “ Coin lesions “ by radiology

MICROSCOPIC• Patterns:
– Organoid (nests)– Trabeculae / Cords– Rosette-like– Pseudo-glandular– Pseudo-papillary
• Bland neuroendocrine cells:– Polygonal cells with eosinophilic (finely granular) cytoplasm– Round to oval monotonous nuclei– Finely granular (salt and pepper) chromatin– Inconspicuous (absent) nucleoli

MICROSCOPIC
• Can have spindle cell morphology– Especially peripheral carcinoid tumors
• Stroma:– Typically fibro-vascular (prominent vascularity)– Less commonly:
• Bone, cartilage• Dense fibrosis• Amyloid

MICROSCOPIC
Typical vs Atypical carcinoid:• Typical carcinoids:
– < 2 mitoses/10 hpf– No necrosis
• Atypical carcinoids:– 2–10 mitoses/10 hpf– And/or necrosis
• HPF (high power field) = field diameter with a 40X objective (0.2 mm2)

SPECIAL STUDIES• Neuroendocrine markers
– Chromogranin, Synaptophysin, Neuron Specific Enolase, and CD56– Atypical carcinoid may show reduced staining than Typical cases
• Pan-keratin– Cam 5.2 is better than AE1/AE3 (to be safe, use both)– CK 7 and 20 are generally negative
• TTF-1 – 30% of pulmonary carcinoid– Weak in comparison to small cell lung carcinoma (strong)
• Ki67 (Mib1)– Typical: < 2%– Atypical: 2 – 20%
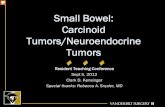
A) Lung carcinoid tumor, H&E stainB) Synaptophysin stains the cytoplasmC) pan-keratin shows dot-like and diffuse staining of the cytoplasm

SPECIAL STUDIES• Chromogranin:
– Acidic glycoprotein in neurosecretory granules– (Cytoplasm, granular)
• Synaptophysin:– Transmembrane glycoprotein found in presynaptic vesicles– (Cytoplasm, granular)
• CD56:– NCAM “Neural Cell Adhesion Molecule”– (Membranous)

SPECIAL STUDIES• Overall, SYN and CD56 are more sensitive than CHR but CHR is more specific.
• CD57 can be used as “2nd line” neuroendocrine marker
• NSE is no longer used in neuroendocrine tumors diagnosis (very low specificity)
• Some NE tumors will label for either CHR or SYN but not both– so to be safe, use both
• SYN and CHR are usually strongly expressed in low-grade NE neoplasms (e.g. carcinoid), whereas expression may be weak/focal in high-grade NE neoplasms (e.g. small cell carcinoma)
– Fortunately, CD56 is positive in high-grade NE tumors

SPECIAL STUDIES
Electron microscopy: Dense-core secretory granules– Membrane-limited dense-core granules– Vary in size (50–400 nm), shape, and density
• depending on the protein contained in the granule– Usually have a halo between the core and the membrane
• Carcinoid tumor contains serotonin-secreting pleomorphic granules

CYTOLOGYTypical Carcinoid:• Cellular smear• Monotonous round to oval cells• Small N/C ratio• Finely granular “salt and pepper” chromatin• Cohesive clusters, loosely cohesive sheets, and single cells are seen
– Can show many patterns:• Mixture of epithelial cells/spindle cells (biphasic)• Plasmacytoid cells• Acinar pattern• Trabecular pattern
• Note that most of the carcinoid cases have negative cytology, because the bronchial mucosal covering is often intact.

CYTOLOGY
Atypical carcinoid:• Similar to that of typical carcinoid at low magnification• Higher magnification:
– Slight to moderate nuclear pleomorphism– More prominent nucleoli– Occasional mitotic activity– Single-cell necrosis

CYTOLOGY
Spindle Cell Carcinoid:• Commonly seen in peripheral carcinoid• Can be typical or atypical.• The smear:
– Cellular– Monotonous population of fusiform cells appearing as single cells or loose aggregates– The nuclear chromatin is finely granular “salt and pepper”– Having moderate cytoplasm with elongated processes appearing like a whip– May fold on themselves forming comma shapes and arches

DIFFERENTIAL DIAGNOSIS• Other neuroendocrine tumors:
– Carcinoid tumorlets– Small cell carcinoma– Large cell neuroendocrine carcinoma– Intestinal or pancreatic carcinoid tumors
• Adenocarcinoma / other carcinomas:– Pulmonary adenocarcinoma– Mucoepidermoid carcinoma– Acinic cell carcinoma– Metastatic
• Spindle cell tumors

DIFFERENTIAL DIAGNOSIS
Small cell lung carcinoma (SCLC):• Absent organoid pattern• Small cells with scant cytoplasm (higher N/C ratio than carcinoid)• Nuclear molding• Nuclear pleomorphism• Fine granular chromatin• Absent nucleoli• High mitotic rates > 10 mitosis/10 hpf (median, 70/10 hpf)• Frequent, extensive necrosis• Ki67 (Mib1) > 20%

DIFFERENTIAL DIAGNOSIS
Large cell neuroendocrine carcinoma (LCNEC):• Organoid pattern is less extensive than carcinoid• Larger cell size with large cytoplasm (lower N/C ratio than carcinoid)• Nuclear pleomorphism• Vesicular, coarse, or fine chromatin• Visible nucleoli• Greater than 10 mitosis/10 hpf (median, 70/10 hpf)• Relatively more necrosis than atypical carcinoid• Ki67 (Mib1) > 20%

DIFFERENTIAL DIAGNOSIS
Carcinoid tumorlets:• Resemble typical carcinoid• By definition it is less than 5 mm (0.5 cm) in diameter
Intestinal or pancreatic carcinoid:• Not express TTF-1 (positive in pulmonary carcinoids)• Intestinal carcinoids express CDX2 (usually negative in pulmonary
carcinoids)

DIFFERENTIAL DIAGNOSIS
Adenocarcinoma:• More Atypia• Gland formation and mucin secretion are common• No neuroendocrine markers

WWW.• PathPedia
– http://www.pathpedia.com/education/eatlas/histopathology/lung_and_bronchi/carcinoid_typical.aspx• Center For Genomic Pathology
– http://ctrgenpath.net/2011/07/slide-of-the-week-carcinoid-in-the-lung-july-25th-2011/• WikiMedia
– https://commons.wikimedia.org/w/index.php?search=carcinoid&title=Special:Search&go=Go&uselang=en&searchToken=42t2jqm6ok37vpnunahkve974
• FlickerView– http://www.flickriver.com/photos/pulmonary_pathology/tags/carcinoid/
• Some EM slides– http://pathology.osu.edu/residents/StudyGuides/EM/Carcinoid/carcinoid1.htm
• Pathorama– http://alf3.urz.unibas.ch/pathopic/e/intro.htm

THANK YOUH a z e m A l i