
Five-Year Metabolic, Functional ...care.diabetesjournals.org/content/diacare/38/9/1714.full.pdf ·...
9
Five-Year Metabolic, Functional, and Safety Results of Patients With Type 1 Diabetes Transplanted With Allogenic Islets Within the Swiss-French GRAGIL Network Diabetes Care 2015;38:1714–1722 | DOI: 10.2337/dc15-0094 OBJECTIVE To describe the 5-year outcomes of islet transplantation within the Swiss-French GRAGIL Network. RESEARCH DESIGN AND METHODS Retrospective analysis of all subjects enrolled in the GRAGIL-1c and GRAGIL-2 islet transplantation trials. Parameters related to metabolic control, graft function, and safety outcomes were studied. RESULTS Forty-four patients received islet transplantation (islet transplantation alone [ITA] 24 patients [54.5%], islet after kidney [IAK] transplantation 20 patients [45.5%]) between September 2003 and April 2010. Recipients received a total islet mass of 9,715.75 6 3,444.40 IEQ/kg. Thirty-four patients completed a 5-year follow-up, and 10 patients completed a 4-year follow-up. At 1, 4, and 5 years after islet transplantation, respectively, 83%, 67%, and 58% of the ITA recipients and 80%, 70%, and 60% of the IAK transplant recipients reached HbA 1c under 7% (53 mmol/mol) and were free of severe hypoglycemia, while none of the ITA recipients and only 10% of the IAK transplant recipients met this composite criterion at the preinfusion stage. Thirty-three of 44 patients (75%) experienced insulin independence during the entire follow-up period, with a median duration of insulin independence of 19.25 months (interquartile range 2–58). Twenty-nine of 44 recipients (66%) exhibited at least one adverse event; 18 of 55 adverse events (33%) were possibly related to immunosuppression; and complications related to the islet infusion (n = 84) occurred in 10 recipients (11.9%). CONCLUSIONS In a large cohort with a 5-year follow-up and in a multicenter network setting, islet transplantation was safe and efficient in restoring good and lasting glycemic control and preventing severe hypoglycemia in patients with type 1 diabetes. Over the last decade, islet transplantation has emerged as a promising treatment for type 1 diabetes. Currently, islet transplantation can be offered to patients with type 1 diabetes who are experiencing major glucose variability and lack of predictability and unawareness of hypoglycemic episodes despite intensive insulin therapy and 1 Department of Endocrinology, P ˆ ole DigiDune, Grenoble University Hospital, Joseph Fourier Uni- versity, Grenoble, France 2 Centre Hospitalier Universitaire Jean Minjoz, Ser- vice d’ Endocrinologie-M´ etabolisme et Diab´ etologie- Nutrition, Besançon, France 3 Centre Hospitalier de Montpellier, Pˆ ole Rein Hy- pertension M´ etabolisme, Service d’Endocrinolo- gie, Montpellier, France 4 Department of Nephrology, Pˆ ole DigiDune, Gre- noble University Hospital, Joseph Fourier Univer- sity, Grenoble, France 5 Hospices Civils de Lyon, Service d’Urologie et de Chirurgie de la Transplantation, Pˆ ole Chirurgie, Lyon, France 6 Hospices Civils de Lyon, Service d’Endocrinologie Diab` ete Nutrition, Lyon, France 7 Hospices Civils de Lyon, Service de N´ ephrologie M´ edecine de la Transplantation et Immunologie Clinique, Lyon, France 8 Centre Hospitalier Universitaire de Nancy, Ser- vice de N ´ ephrologie, Nancy, France 9 Service d’Endocrinologie, Diab´ etologie et Mal- adies M´ etaboliques, Centre Hospitalier Sud- Francilien, Corbeil-Essonnes, France 10 H ˆ opitaux Universitaires de Strasbourg, Ser- vice d’ Endocrinologie Diab` ete et Maladies M´ etaboliques, P ˆ ole NUDE, Strasbourg, France 11 Hospices Civils de Lyon, P ˆ ole Information M´ edicale Evaluation Recherche, and Universit´ e de Lyon, EA Sant´ e-Individu-Soci´ et´ e 4129, Lyon, France 12 CHU de Clermont-Ferrand, Service Endocrino- logie-Diab` ete-Maladies M ´ etaboliques, Clermont Ferrand Universit´ e, Clermont-Ferrand, France 13 Departement of Surgery, Islet Isolation, and Transplantation Center, Geneva University Hos- pitals, Geneva, Switzerland Corresponding author: Sandrine Lablanche, [email protected]. Received 15 January 2015 and accepted 25 May 2015. Clinical trial reg. nos. NCT00639600 and NCT00321256, clinicaltrials.gov. This article contains Supplementary Data online at http://care.diabetesjournals.org/lookup/ suppl/doi:10.2337/dc15-0094/-/DC1. *Members of the GRAGIL Network can be found in the Supplementary Data online. © 2015 by the American Diabetes Association. Readers may use this article as long as the work is properly cited, the use is educational and not for profit, and the work is not altered. Sandrine Lablanche, 1 Sophie Borot, 2 Anne Wojtusciszyn, 3 Francois Bayle, 4 Rachel T´ etaz, 4 Lionel Badet, 5 Charles Thivolet, 6 Emmanuel Morelon, 7 Luc Frimat, 8 Alfred Penfornis, 9 Laurence Kessler, 10 Coralie Brault, 11 Cyrille Colin, 11 Igor Tauveron, 12 Domenico Bosco, 13 Thierry Berney, 13 and Pierre-Yves Benhamou, 1 on behalf of the GRAGIL Network* 1714 Diabetes Care Volume 38, September 2015 EMERGING TECHNOLOGIES AND THERAPEUTICS
Transcript of Five-Year Metabolic, Functional ...care.diabetesjournals.org/content/diacare/38/9/1714.full.pdf ·...

Five-Year Metabolic, Functional,and Safety Results of PatientsWithType 1 Diabetes TransplantedWith Allogenic Islets Within theSwiss-French GRAGIL NetworkDiabetes Care 2015;38:1714–1722 | DOI: 10.2337/dc15-0094
OBJECTIVE
To describe the 5-year outcomes of islet transplantation within the Swiss-FrenchGRAGIL Network.
RESEARCH DESIGN AND METHODS
Retrospective analysis of all subjects enrolled in the GRAGIL-1c and GRAGIL-2 islettransplantation trials. Parameters related to metabolic control, graft function,and safety outcomes were studied.
RESULTS
Forty-four patients received islet transplantation (islet transplantation alone [ITA]24 patients [54.5%], islet after kidney [IAK] transplantation 20 patients [45.5%])between September 2003 and April 2010. Recipients received a total islet mass of9,715.75 6 3,444.40 IEQ/kg. Thirty-four patients completed a 5-year follow-up,and 10 patients completed a 4-year follow-up. At 1, 4, and 5 years after islettransplantation, respectively, 83%, 67%, and 58% of the ITA recipients and 80%,70%, and 60% of the IAK transplant recipients reached HbA1c under 7% (53mmol/mol)and were free of severe hypoglycemia, while none of the ITA recipients and only10% of the IAK transplant recipients met this composite criterion at the preinfusionstage. Thirty-three of 44 patients (75%) experienced insulin independence duringthe entire follow-up period, with a median duration of insulin independence of19.25 months (interquartile range 2–58). Twenty-nine of 44 recipients (66%)exhibited at least one adverse event; 18 of 55 adverse events (33%) were possiblyrelated to immunosuppression; and complications related to the islet infusion (n = 84)occurred in 10 recipients (11.9%).
CONCLUSIONS
In a large cohort with a 5-year follow-up and in amulticenter network setting, islettransplantation was safe and efficient in restoring good and lasting glycemiccontrol and preventing severe hypoglycemia in patients with type 1 diabetes.
Over the last decade, islet transplantation has emerged as a promising treatment fortype 1 diabetes. Currently, islet transplantation can be offered to patients with type1 diabetes who are experiencing major glucose variability and lack of predictabilityand unawareness of hypoglycemic episodes despite intensive insulin therapy and
1Department of Endocrinology, Pole DigiDune,Grenoble University Hospital, Joseph Fourier Uni-versity, Grenoble, France2Centre Hospitalier Universitaire Jean Minjoz, Ser-vice d’Endocrinologie-MetabolismeetDiabetologie-Nutrition, Besançon, France3Centre Hospitalier de Montpellier, Pole Rein Hy-pertension Metabolisme, Service d’Endocrinolo-gie, Montpellier, France4Department of Nephrology, Pole DigiDune, Gre-noble University Hospital, Joseph Fourier Univer-sity, Grenoble, France5Hospices Civils de Lyon, Service d’Urologie et deChirurgie de la Transplantation, Pole Chirurgie,Lyon, France6Hospices Civils de Lyon, Service d’EndocrinologieDiabete Nutrition, Lyon, France7Hospices Civils de Lyon, Service de NephrologieMedecine de la Transplantation et ImmunologieClinique, Lyon, France8Centre Hospitalier Universitaire de Nancy, Ser-vice de Nephrologie, Nancy, France9Service d’Endocrinologie, Diabetologie et Mal-adies Metaboliques, Centre Hospitalier Sud-Francilien, Corbeil-Essonnes, France10Hopitaux Universitaires de Strasbourg, Ser-vice d’Endocrinologie Diabete et MaladiesMetaboliques, Pole NUDE, Strasbourg, France11Hospices Civils de Lyon, Pole InformationMedicale Evaluation Recherche, and Universite deLyon, EA Sante-Individu-Societe 4129, Lyon, France12CHU de Clermont-Ferrand, Service Endocrino-logie-Diabete-Maladies Metaboliques, ClermontFerrand Universite, Clermont-Ferrand, France13Departement of Surgery, Islet Isolation, andTransplantation Center, Geneva University Hos-pitals, Geneva, Switzerland
Corresponding author: Sandrine Lablanche,[email protected].
Received 15 January 2015 and accepted 25 May2015.
Clinical trial reg. nos. NCT00639600 andNCT00321256, clinicaltrials.gov.
This article contains Supplementary Data onlineat http://care.diabetesjournals.org/lookup/suppl/doi:10.2337/dc15-0094/-/DC1.
*Members of the GRAGIL Network can be foundin the Supplementary Data online.
© 2015 by the American Diabetes Association.Readers may use this article as long as the workis properly cited, the use is educational and notfor profit, and the work is not altered.
Sandrine Lablanche,1 Sophie Borot,2
Anne Wojtusciszyn,3 Francois Bayle,4
Rachel Tetaz,4 Lionel Badet,5
Charles Thivolet,6 Emmanuel Morelon,7
Luc Frimat,8 Alfred Penfornis,9
Laurence Kessler,10 Coralie Brault,11
Cyrille Colin,11 Igor Tauveron,12
Domenico Bosco,13 Thierry Berney,13 and
Pierre-Yves Benhamou,1 on behalf of the
GRAGIL Network*
1714 Diabetes Care Volume 38, September 2015
EMER
GINGTECHNOLO
GIESANDTH
ERAPEU
TICS

who use innovative technologies such ascontinuousglucosemonitoring andcontin-uous subcutaneous pump. Islet transplan-tation is associated with improvement inkidney graft function and survival in pa-tients with type 1 diabetes who have al-ready undergone kidney transplantation(1). Consequently, islet transplantationhas been offered to patients with type1 diabetes with a functional kidney allo-graftwho are not candidates for pancreastransplantation.The results of islet transplantation
have improved significantly in recentyears. Before 1999, the achievement ofinsulin independence was obtained in,10% of transplant recipients. Evolu-tion of the immunosuppression regi-men, an increase in transplanted isletmass (2), and improvement in islet prep-aration quality (3) have allowed to ob-tain insulin independence in .60% ofpatients at 1 year in experienced centers(4,5). Insulin independence was not wellmaintained in the initial period, withonly 27% of patients remaining insulinfree after 5 years (4). More recently,mainly thanks to more potent immuno-suppressive protocols, insulin indepen-dence rates have improved, reaching upto 50% at 5 years (6). Despite the overalllow rate of long-term insulin indepen-dence, islet transplantation is beneficialin allowing improvements in quality oflife (7), metabolic control (4), preven-tion of hypoglycemic events (8), andprotection of recipients against the pro-gression of microangiopathy (9,10). De-spite these long-term benefits, islettransplantation exhibits variable suc-cess depending on the experience ofthe center and the protocols used.Moreover, beneficial metabolic effectsmay be counterbalanced by adverseevents, especially due to immunosup-pressive treatment.The GRAGIL consortium is a French-
Swiss Network (11) comprising severaltransplant centers (Geneva, Switzer-land, and Besançon, Grenoble, Lyon,Montpellier, Nancy, Strasbourg, andClermont-Ferrand, France), each ofwhich permits pancreas procurement,recipient recruitment, performance oftransplant procedures, and clinical follow-up, whereas islet isolation is performedin two facilities sharing the sameprocedure(Geneva and, more recently, Grenoble).In the 2003–2010 period, the follow-
ing two trials were conducted within
the network, in two different settings:islet after kidney (IAK) transplantation(GRAGIL-1C trial, clinical trial reg. no.NCT00639600, clinicaltrials.gov) andislet transplantation alone (ITA) (GRAGIL-2trial, clinical trial reg. no. NCT00321256,clinicaltrials.gov) (12,13). The purposeof the current study was to describethe 5-year outcome and safety profileof islet transplantation in the GRAGIL-1candGRAGIL-2patientswith type1diabetes.
RESEARCH DESIGN AND METHODS
PatientsData from the GRAGIL-1c and GRAGIL-2trials were retrospectively analyzed. Allstudy subjects were receiving the origi-nal immunosuppressive regimen of theEdmonton protocol. The GRAGIL-2 trialwas designed for C-peptide–negativepatients with type 1 diabetes, with agebetween 18 and 65 years, and a mini-mum disease duration of 5 years. Islettransplantation was considered if pa-tients experienced frequent episodesof severe hypoglycemia despite well-conducted, intensive insulin therapy.The main exclusion criteria were kidneydiseases (glomerular filtration rate ,50mL/min/1.73 m2, proteinuria.500 mg/24 h), liver and coagulation abnormali-ties, unstable ischemic diabetic retino-pathy, and poor cardiovascular prognosis.Patients who were overweight (bodyweight .70 kg in women and $75 kgin men, or BMI $26 kg/m2) and/orneeded excessive doses of exogenous in-sulin (0.7 UI/kg/day or 50 UI/day) wereexcluded from the study. Details aboutthis trial have been published previously(12). The GRAGIL-1c trial targeted pa-tients with type 1 diabetes with a func-tional kidney graft (13). Inclusion criteriafor islet transplantation were creatinineclearance .50 mL/min, proteinuria,0.5 g/day, daily insulin requirement, 0.7 units/kg/day, BMI ,26 kg/m2,and a body weight of ,75 kg (male) or,70 kg (female). Metabolic lability andhypoglycemia unawareness were not aprerequisite for study inclusion. Themain exclusion criteria were liver and co-agulation abnormalities, unstable diabeticretinopathy, andpoor cardiovascular prog-nosis. All inclusionswere reviewed and ap-proved by the GRAGIL Network steeringcommittee.
Details on the management of thenetwork have been published previ-ously (11,14). The protocols were
approved by the institutional reviewboard (Person Protection Committeeof Grenoble University Hospital), andeach patient gave written informed con-sent. Patients underwent transplanta-tion between September 2003 andApril 2010 within the GRAGIL Networkat the University Hospitals of Grenoble,Besançon, Lyon, Montpellier, Nancy,and Strasbourg. Islet preparations withthe number of islets .5,000 IEQ/kg/injection and islet purity.50% were re-leased. As per the protocol, patientswere scheduled to receive up to threeislet infusions with a target islet mass of10,000 IEQ/kg body wt. Regardless ofthe achievement of insulin indepen-dence, second and third infusions wereperformed ideally within a time frame of3 months when previous islet infusionsdid not permit achievement of the10,000 IEQ/kg body wt threshold.
Islet Isolation and TransplantationPancreata were obtained from brain-dead multiorgan donors through theSwiss Transplant Agency and the FrenchBiomedicine Agency (Agence de la Bio-medecine). Standard donor criteria forpancreas acceptance were used as pre-viously described (14). Islets were iso-lated using the automated methoddescribed by Ricordi et al. (15), with lo-cal modifications as previously reported(16). Islet preparations were condi-tioned in gas-permeable transfer bags(Biorep Technologies, Miami, FL) inCMRL 1066 Medium supplementedwith human albumin (4%) and heparin(35 units/kg recipient body wt), andwere shipped by ambulance to thetransplant centers. Transit time neverexceeded 4 h. Islets were transplantedintraportally through a percutaneoustranshepatic procedure with emboliza-tion of the punction tract using theoriginal Edmonton steroid-free immu-nosuppressive regimen combining siro-limus and tacrolimus with daclizumab orbasiliximab induction (17). Immunosup-pression comprised high-dose sirolimus(Rapamune; Wyeth, New York, NY), withtarget trough levels of 12–15 mg/L forthe first 3 months and 10–12 mg/Lthereafter, and low-dose tacrolimus(Prograf; Astellas, Tokyo, Japan), withtarget trough levels of 4–6 mg/L. Induc-tion was performed with intravenousdaclizumab (Zenapax; Roche, Basel,Switzerland) at a dosage of 1 mg/kg
care.diabetesjournals.org Lablanche and Associates 1715

infused immediately before islet infusionand repeatedbiweekly for up tofivedoses.For the second islet transplantation, afull daclizumab protocol was startedagain, regardless of the time that hadelapsed since the first injection. Aftercommercial withdrawal of daclizumabin 2009, basiliximab (Simulect; Novartis,Basel, Switzerland) was used for induc-tion at a dosage of 20mg on days 0 and 4of each islet infusion.
Follow-upThe protocol required a monthly super-vision of patients by the diabetologistinvestigator for the first year after thefirst infusion. After year 1, patients wererequired to see the diabetologist inves-tigator every 6 months. For each visit,fasting plasma glucose level, basalC-peptide level, exogenous insulinrequirement, glycated hemoglobin(HbA1c) level, creatinine level, protein-uria, insulin antibody (insulin binding ca-pacity of serum threshold .3.5%)(radioimmunological assay kit; CisBioInternational), the number of mild-to-moderate hypoglycemic events (hypogly-cemia symptoms or glycemia,4 mmol/L)experienced during the preceding week,the number of severe hypoglycemicevents that occurred since the last fol-low-up visit (hypoglycemia without pos-sibility of self-treatment), and theoccurrence of adverse events were as-sessed and recorded. Severe hypoglyce-mic events were declared prospectivelyas adverse events. Adverse events wereclassified according to their severity aslife threatening, serious, moderate, ormild. A life-threatening event was de-fined as an event in which the patientwas at risk for death at the time of theevent. It does not refer to an event thathypothetically might have caused deathif it was more severe. A serious adverseevent is defined as any medical occur-rence that results in death, that is lifethreatening, that requires inpatient hos-pitalization or prolongation of an existinghospitalization, and that results in persis-tent or significant disability/incapacity orinduces a congenital anomaly/birth defect.A moderate adverse event is an event re-quiring corrective/complementary treat-ment. A mild adverse event does notrequire any corrective/complementarytreatment (18).Islet graft function was assessed by
calculating the b-score developed by
the University of Alberta (Edmonton,AB, Canada). This previously validatedscoring system is a composite scorethat allocates 2 points each for normalfasting glucose, HbA1c, and stimulatedC-peptide and the absence of insulinor oral hypoglycemic agent use. Nopoint is awarded if the fasting glucosewas in diabetic range, HbA1c was.6.9%(51.9 mmol/mol), C-peptide secretionwas absent on stimulation, or daily in-sulin use was in excess of 0.24 units/kg.One point is given for intermediate val-ues. The score ranges between 0 (nograft function) and 8 (excellent graftfunction) (19). The b-score is a simpleclinical scoring system that correlateswith physiological measures of b-cellfunctions such as postprandial glycemia(19) and arginine-induced insulin secre-tion (20). This score represents an over-all assessment of b-cell transplantfunctions. It gives a b-cell transplantevaluation as a continuum that maybe more informative than the too strin-gent insulin independence criteria.The b-score is now well correlatedwith islet graft outcomes (21,22). In-sulin independence was predefinedas the ability to maintain HbA1c ,6.5%(48 mmol/mol), a 2-h postprandial glu-cose ,10 mmol/L, and a mean ampli-tude of glycemic excursion index of,3.33 mmol/L, without exogenous in-sulin and with a basal plasma C-peptide$0.5 ng/mL. Complete graft failurewas defined by an undetectable C-peptidelevel (,0.3 ng/mL).
Statistical AnalysisIslet characteristics are expressed as themean 6 SEM. Continuous variableswere expressed as themedian and inter-quartile range (Q1; Q3) and were com-pared using repeated-measures ANOVA.The threshold of significance was set at5%. All data were processed and ana-lyzed using XLStat-Pro Software (Addinsoft,Paris, France).
RESULTS
Recipient CharacteristicsThis analysis was based on 44 recipientsof allogenic islet transplants performedbetween September 2003 and April2010. ITA was performed in 24 patients(54.5%), and IAK grafts were performedin 20 patients (45.5%). Recipient charac-teristics at baseline are summarized inTable 1.
Islet Infusion CharacteristicsEighty-four infusions were performedin 44 patients: 8 patients (18%) re-ceived one infusion, 32 patients (73%)received two infusions, and 4 patientsreceived three infusions (9%). The mediancold ischemia time was 7.2 h (3.5–11.5).The total mean IEQ infused was606,617 6 214,695 IEQ per recipient(9,715.75 6 3,444.40 IEQ/kg), with a me-dian stimulation index of 1.9 (1.2; 2.3)and a viability of 92% (81; 95). Themediantime frame between the first and secondinfusions was 6.35 months (1.9; 12.6).
Metabolic ResultsA significant and lasting improvement inHbA1c was observed: HbA1c was 6.20%(44 mmol/mol) (4.60; 9.60 [27; 81]),6.60% (49 mmol/mol) (5.50; 9.40 [37;79]), and 6.70% (50 mmol/mol) (5.40;9.60 [36; 81]), respectively, at 12, 48,and 60 months after islet transplanta-tion vs. 8% (64 mmol/mol) (7.6; 9 [60;75]) at baseline (P , 0.05) in the wholecohort (Fig. 1A). No significant differ-ence was observed in the improvementin HbA1c between ITA and IAK transplantpatients (Fig. 1B and C). At 12, 48, and 60months after islet transplantation, re-spectively, 84%, 70%, and 59% of therecipients reached HbA1c of #7%(53 mmol/mol) or exhibited a drop inHbA1c of $2% (14 mmol/mol) vs. only9% before islet infusion (P , 0.005)(Supplementary Fig. 1E). Fasting bloodglucose improved significantly andlastingly after islet transplantation:8.19 mmol/L (1.56; 22.4) at baseline vs.6.44 mmol/L (4.11; 11.3), 6.57 mmol/L(3.4; 11.8), and 7.28 mmol/L (4.1; 15.1)at 12, 48, and 60 months after islet in-fusion in the global population (P ,0.05). Severe hypoglycemia was mainlyprevalent in ITA candidates before trans-plantation with 4.31 events/patient/year in ITA candidates and 0.29 events/patient/year in IAK transplant candi-dates. The number of severe hypoglyce-mic events/patient/year had fallen to0.27 in IAT recipients and 0.02 in IAKtransplant recipients 1 year after islettransplantation. This benefit was lastingand persisted throughout the 5-yearfollow-up period with no hypoglycemicevent occurring in ITA recipients and0.01 severe hypoglycemia/patient/yearoccurring in IAK transplant recipients(P , 0.005 vs. preinfusion) (Fig. 1D).As an overall evaluation of metabolic
1716 Islet Transplantation Within GRAGIL Network Diabetes Care Volume 38, September 2015
results of islet transplantation, 83%,67%, and 58% of the ITA recipients and80%, 70%, and 60% at 1, 4, and 5 yearsreached HbA1c of ,7% (53 mmol/mol)and were free of severe hypoglycemia,while none of the ITA recipients and only10% of IAK transplant recipients met thiscriterion before infusion (Supplemen-tary Fig. 1F).
Graft FunctionThe median basal C-peptide level was1.43 ng/mL (0; 3.95), 1.49 ng/mL (0;3.14), and 1.54 ng/mL (0; 3.73) 12, 48,and 60 months after islet transplanta-tion vs. 0.1 ng/mL (0; 0.24) at baseline(P , 0.005). In the global population,39 of 44 patients (89%) had a basalC-peptide level of .0.3 ng/mL (i.e.,functional islet graft) 12 months afterislet infusion. The decline of islet func-tion over 5 years of follow-up waslimited, as 33 of 44 patients (75%) and25 of 34 patients (74%) kept a functionalislet graft at 48 and 60 months post-transplant (Fig. 2A). The median insulindose was significantly reduced, asfollows: 0.15 UI/kg (0; 0.47), 0.17 UI/kg(0; 0.7), and 0.18 UI/kg (0; 0.57) at 12, 48,
and 60months after islet transplantationvs. 0.5 UI/kg (0.42; 0.58) at baseline (P,0.05) (Fig. 2B). Among recipients, 91%,70%, and 75% exhibited a b-score of$3at 12, 48, and 60 months post-transplant,with 25%, 14%, and 4% of recipientshaving an optimal b-score of$7 (Fig. 2C).No significant differences in b-scorewere observed between the IAK trans-plant and ITA populations (Supplemen-tary Fig. 2E and F).
Regarding IAK transplant recipients,45%, 40%, 40%, 35%, and 31.5% metthe criteria of insulin independence at12, 24, 36, 48, and 60months, respectively.Regarding IAT recipients, 37.5%, 45.8%,37.5%, 25%, and 14% met the criteriaof insulin independence at 12, 24, 36,48, and 60 months, respectively (P = NS).In the whole cohort, during the entirefollow-up period, 33 of 44 patients(75%) experienced an insulin inde-pendence period with a medianduration of insulin independence of19.2 months (2; 58). Regarding the to-tal islet mass infused, no significant dif-ference was observed in terms ofinsulin independence rate (Fig. 2D). InITA recipients, the mean duration of
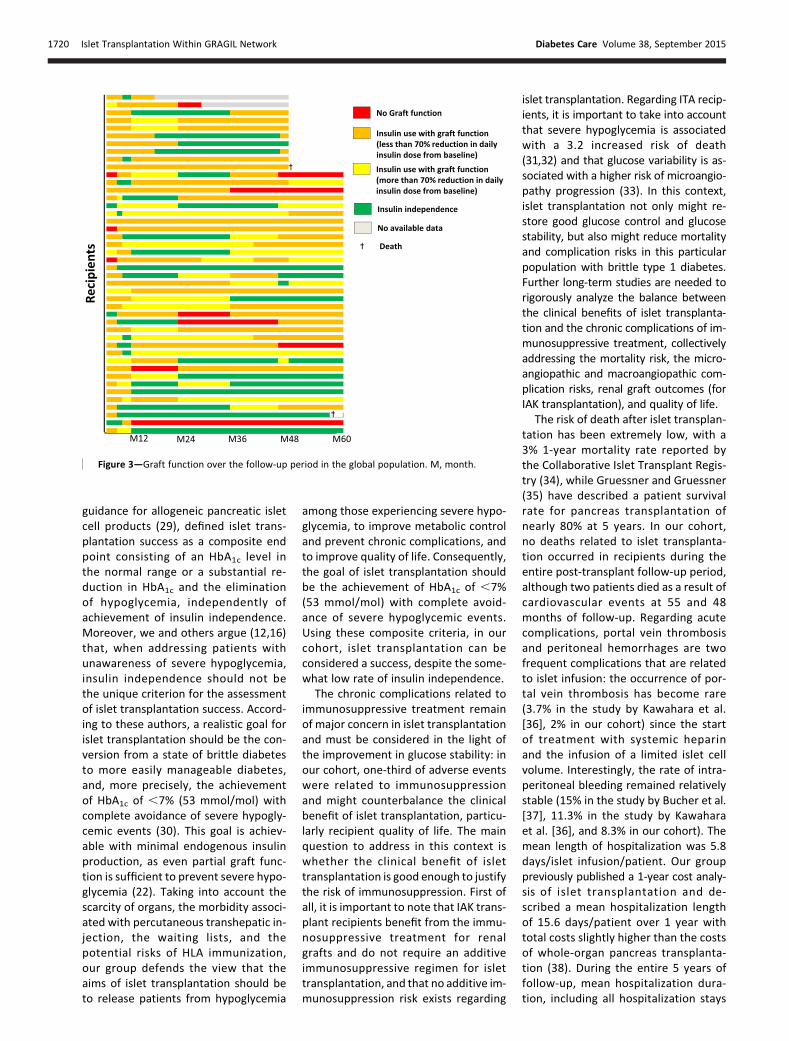
insulin independence was 20.18 614.06 months in recipients infusedwith $10,000 IEQ/kg vs. 12 6 17.34months in recipients infused with#10,000 IEQ/kg (P = 0.4 [differencewas not significant]). In IAK transplantrecipients, the duration of insulin inde-pendence was 27.5 6 26.08 months inrecipients infused with $10,000 IEQ/kgvs. 22.6 6 19.59 months in recipientsinfused with #10,000 IEQ/kg (P = 0.3[difference not significant]). A total of26% of recipients (9 of 34 recipients)remained insulin independent at 60months (Fig. 3).
Adverse Events and SurvivalNo deaths related to islet transplanta-tion occurred in recipients during theentire post-transplant follow-up period(two patients died as the result of a car-diovascular event at 55 and 48 monthspost-transplant). With all types of sever-ity taken together, 29 of 44 recipients(66%) experienced at least one adverseevent during the 5-year follow-up pe-riod. Fifty-five adverse events occurredin these 29 patients, as follows: mild ad-verse events 14%, moderately adverse
Table 1—Recipient clinical and biological characteristics at baseline
Recipient clinical and biological characteristics at baseline Global population ITA recipients IAK transplant recipients
Recipients 44 24 (54.5) 20 (45.5)
Age (years) 46 (42–55) 47 (40–56) 46 (43–55)
Male sex 27 (61.4) 11 (45.8) 16 (80)
Weight (kg) 63 (57–68) 61 (55–69) 65 (61–67)
BMI (kg/m2) 23 (20–24) 22 (20–23) 23 (22–24)
Diabetes duration (years) 33 (26–37) 31 (25–36) 35 (31–41)
Multiple daily injections 26 (59.1) 13 (54.1) 13 (65)
Daily insulin requirements (UI/kg) 0.5 (0.42–0.6) 0.47 (0.4–0.59) 0.55 (0.47–0.6)
HbA1c (%) 8.1 (7.5–9.1) 8.1 (7.4–9.10) 7.9 (7.6–8.9)
HbA1c (mmol/mol) 65 (58.5–76) 65 (57.4–9.1) 62.8 (59.6–73.8)
Creatinine (mmol/L) 100 (75–111) 77 (69–93) 108.5 (103–136.2)
IA-2 autoantibody (+) 1 (2.3) 1 (4.2) 0
GAD autoantibody (+) 4 (9.1) 0 4 (20)
Insulin autoantibody 12 (27.3) 7 (29.2) 5 (25)
HypoglycemiaNo occurrence 2 (4.5) 2 (8.3) 0Awareness 11 (25) 0 11 (55)Partial unawareness 13 (29.5) 8 (33.3) 5 (25)Unawareness 13 (29.5) 12 (50) 1 (5)Unknown 5 (11.4) 2 (8.33) 3 (15)
Severe hypoglycemiaAt least one episode of severe hypoglycemia in the
12 months prior to islet grafting 26 (59.1) 20 (83.3) 6 (30)Number of episodes of severe hypoglycemia in the
12 months prior to islet infusion 5.5 (2–10) 6 (2–10) 2 (2–4.5)
Data are provided as n (%) or median (Q1; Q3).
care.diabetesjournals.org Lablanche and Associates 1717

events 9%, serious adverse events 67%,and life-threatening adverse events 9%.A total of 55% of the adverse eventsoccurred during the first year post-transplant. Eighteen of 55 adverseevents (33%) were related to or possiblyrelated to immunosuppression (Supple-mentary Table 2). Regarding the islet in-fusion procedure, 10 of 84 islet infusions(11.9%) were complicated by an adverseevent (cytolysis 1, abdominal pain 1,segmental portal vein thrombosis re-solved after anticoagulation 1, and hem-orrhages 7; 4 patients required bloodtransfusion, 2 patients required laparot-omy, and 1 patient was treated by inter-ventional radiology) (SupplementaryTable 3). The length of hospitalizationwas not significantly increased in pa-tients with bleeding (6.3 vs. 5.8 days/islet infusion/patient in the whole co-hort). Regarding renal function, crea-tinine levels remained stable over thefollow-up period in the global population
and ITA recipients: after 5 years offollow-up, the median creatinine levelswere 102.5 mmol/L (74.7; 139.25) and80 mmol/L (72; 104) in the global pop-ulation and among ITA recipients, re-spectively, vs. 100 mmol/L (75; 111)and 77 mmol/L (69; 93) at baseline, re-spectively. After 5 years of follow-up,the median clearance creatinine ratewas 83 mL/min (60; 93) in ITA recipientsvs. 79.5 mL/min (69; 95) at baseline, re-spectively (P = NS). In IAK transplant re-cipients, we described the followingnonsignificant increase in creatininelevels: after 5 years of follow-up, theme-dian creatinine level was 140 mmol/L(112.5; 154.5) vs. 108.5 mmol/L (103;136.2) at baseline. In IAK transplant re-cipients, creatinine clearance remainedstable over the follow-up period: atstudy inclusion, the median creatinineclearance rate was 59.5 mL/min (51.5; 69)vs. 51 mL/min (47; 66) after 5 years offollow-up (P = NS).
CONCLUSIONS
This retrospective cohort study showedthat long-term islet graft survival andsignificant glycemic improvement havebeen achieved after islet transplantationin most recipients with type 1 diabeteswho underwent transplantation withinthe GRAGIL Network. Few data are avail-able on 5-year outcomes of islet trans-plantation using a typical Edmontonprotocol (4,6,23). In our cohort, 1 yearand 5 years after undergoing isletgrafting, a good metabolic control(HbA1c #7% [53 mmol/mol] or a de-crease in HbA1c of $2% [14 mmol/mol])was achieved in 84% and 59% of recipi-ents, respectively, compared with only9% before islet transplantation. A totalof 89% and 74% of patients kept a func-tional islet graft 12 and 60 months afterislet infusion. Insulin independence forat least 1 month was achieved in 33 of44 patients (75%) and persisted for a
Figure 1—Evolution of HbA1c after islet transplantation in the global population (A), in IAK transplant recipients (B), and in ITA recipients (C).D: Percentage of patients experiencing severe hypoglycemia at preinfusion and after islet transplantation in the global population and in IAKtransplant and ITA recipients. M, month; Pre inf, preinfusion.
1718 Islet Transplantation Within GRAGIL Network Diabetes Care Volume 38, September 2015

median duration of 19.2 months. This re-sult was obtained with a significant andlasting reduction in insulin requirementsand in the rate of severe hypoglycemia.Our study is an actual analysis and notactuarial, as in the study by Ryan et al.(23), in which only four patients com-pleted the 5-year follow-up. In our co-hort, we reported a higher long-terminsulin independence rate and higher in-sulin independence duration comparedwith the study by Ryan et al. (23) (10%of 5-year insulin independence in Ryanet al. [23] vs. 29% in our cohort; 15months of insulin independence dura-tion in Ryan et al. [23] vs. 19 months inour cohort). The 5-year islet graft survivalrate reported in our cohort is concordantwith what is described by Ryan et al. (23)(;80%).In our cohort, per protocol, transplan-
tation of$10,000 IEQ/kg in up to threeinfusions was planned. However, eightpatients (18%)declined theadministration
of a second infusion, which is responsiblefor the lower total islet mass infused perrecipient that was observed in our cohortcompared with recent studies (21). Ifhigher numbers of injections have beenassociated with better overall long-termfunctional results (13), the high numberof infused IEQper kilogramof bodyweightseems to be better correlated with long-term graft survival and better metaboliccontrol. Indeed, since the landmark Ed-monton Trial, 10,000 IEQ/kg was classi-cally recommended to reach short-terminsulin independence (24,25), but this isless clear-cut in more extensive cohortsin which .20% of patients required15,000 IEQ/kg to achieve insulin indepen-dence (23). Interestingly, in our cohort,the total dose of transplanted islets didnot seem to significantly affect the rateof insulin independence. Since islet func-tionality is heterogeneous and dependson several factors, importantly, donorfactors, it explains why a transplanted
islet mass is not strictly correlated tograft function (26). In fact, some studies(27,28) have demonstrated that humanislet function in vivo correlated poorlywith transplanted islet numbers. Inmore recent studies, a better rate of in-sulin independence (57% at 3 years) wasachieved with a rate.10,000 IEQ/kg. Inour cohort, probably due to the lowertotal mean islet mass infused per recipi-ent, primary graft function and graft sur-vival (i.e., insulin independence withHbA1c ,7% [53 mmol/mol]) are lowerthan described in the study by Vantyghemet al. (21). Nevertheless, despite this lowerlevel of primary graft function, our cohortexhibited results that were similar, interms ofmetabolic control (HbA1c, insulinrequirement and reduction in severe hy-poglycemia), at 5 years post-transplant tothose of recent studies.
The criteria defining islet graft successremain largely a matter of debate. TheU.S. Food and Drug Administration, in its
Figure 2—Percentage of patients with a C-peptide level of.0.3 ng/mL at preinfusion and after islet transplantation in the global population, in IAKtransplant recipients, and in ITA recipients (A); the evolution of insulin dose (UI/kg/day) after islet transplantation in the global population, in IAKtransplant recipients, and in ITA recipients (B); and the b-score over the follow-up period in the global population (C). D: Percentage of patientsexperiencing insulin independence during follow-up in relation to infused islet mass. M, month; Pre inf, preinfusion.
care.diabetesjournals.org Lablanche and Associates 1719
guidance for allogeneic pancreatic isletcell products (29), defined islet trans-plantation success as a composite endpoint consisting of an HbA1c level inthe normal range or a substantial re-duction in HbA1c and the eliminationof hypoglycemia, independently ofachievement of insulin independence.Moreover, we and others argue (12,16)that, when addressing patients withunawareness of severe hypoglycemia,insulin independence should not bethe unique criterion for the assessmentof islet transplantation success. Accord-ing to these authors, a realistic goal forislet transplantation should be the con-version from a state of brittle diabetesto more easily manageable diabetes,and, more precisely, the achievementof HbA1c of ,7% (53 mmol/mol) withcomplete avoidance of severe hypogly-cemic events (30). This goal is achiev-able with minimal endogenous insulinproduction, as even partial graft func-tion is sufficient to prevent severe hypo-glycemia (22). Taking into account thescarcity of organs, the morbidity associ-ated with percutaneous transhepatic in-jection, the waiting lists, and thepotential risks of HLA immunization,our group defends the view that theaims of islet transplantation should beto release patients from hypoglycemia
among those experiencing severe hypo-glycemia, to improve metabolic controland prevent chronic complications, andto improve quality of life. Consequently,the goal of islet transplantation shouldbe the achievement of HbA1c of ,7%(53 mmol/mol) with complete avoid-ance of severe hypoglycemic events.Using these composite criteria, in ourcohort, islet transplantation can beconsidered a success, despite the some-what low rate of insulin independence.
The chronic complications related toimmunosuppressive treatment remainof major concern in islet transplantationand must be considered in the light ofthe improvement in glucose stability: inour cohort, one-third of adverse eventswere related to immunosuppressionand might counterbalance the clinicalbenefit of islet transplantation, particu-larly recipient quality of life. The mainquestion to address in this context iswhether the clinical benefit of islettransplantation is good enough to justifythe risk of immunosuppression. First ofall, it is important to note that IAK trans-plant recipients benefit from the immu-nosuppressive treatment for renalgrafts and do not require an additiveimmunosuppressive regimen for islettransplantation, and that no additive im-munosuppression risk exists regarding
islet transplantation. Regarding ITA recip-ients, it is important to take into accountthat severe hypoglycemia is associatedwith a 3.2 increased risk of death(31,32) and that glucose variability is as-sociated with a higher risk of microangio-pathy progression (33). In this context,islet transplantation not only might re-store good glucose control and glucosestability, but also might reduce mortalityand complication risks in this particularpopulation with brittle type 1 diabetes.Further long-term studies are needed torigorously analyze the balance betweenthe clinical benefits of islet transplanta-tion and the chronic complications of im-munosuppressive treatment, collectivelyaddressing the mortality risk, the micro-angiopathic and macroangiopathic com-plication risks, renal graft outcomes (forIAK transplantation), and quality of life.
The risk of death after islet transplan-tation has been extremely low, with a3% 1-year mortality rate reported bythe Collaborative Islet Transplant Regis-try (34), while Gruessner and Gruessner(35) have described a patient survivalrate for pancreas transplantation ofnearly 80% at 5 years. In our cohort,no deaths related to islet transplanta-tion occurred in recipients during theentire post-transplant follow-up period,although two patients died as a result ofcardiovascular events at 55 and 48months of follow-up. Regarding acutecomplications, portal vein thrombosisand peritoneal hemorrhages are twofrequent complications that are relatedto islet infusion: the occurrence of por-tal vein thrombosis has become rare(3.7% in the study by Kawahara et al.[36], 2% in our cohort) since the startof treatment with systemic heparinand the infusion of a limited islet cellvolume. Interestingly, the rate of intra-peritoneal bleeding remained relativelystable (15% in the study by Bucher et al.[37], 11.3% in the study by Kawaharaet al. [36], and 8.3% in our cohort). Themean length of hospitalization was 5.8days/islet infusion/patient. Our grouppreviously published a 1-year cost analy-sis of islet transplantation and de-scribed a mean hospitalization lengthof 15.6 days/patient over 1 year withtotal costs slightly higher than the costsof whole-organ pancreas transplanta-tion (38). During the entire 5 years offollow-up, mean hospitalization dura-tion, including all hospitalization stays
Figure 3—Graft function over the follow-up period in the global population. M, month.
1720 Islet Transplantation Within GRAGIL Network Diabetes Care Volume 38, September 2015

for each islet infusion, and eventuallyfor the occurrence of adverse events,fell to 7.05 days/patient/year. Even ifan accurate cost analysis has not beenperformed in this study, islet transplan-tation costs might be lower than thoseof whole pancreas transplantation inview of its significant rates of morbidityand surgical reinterventions. Furtherlong-term cost analysis studies are nec-essary to accurately address this ques-tion and will be performed in a Frenchnational trial to be launched in thecoming months.In conclusion, islet transplantation
within the multicenter GRAGIL Networkprovided important and lasting clinicalbenefits to patients with type 1 diabe-tes, permitting improvement of glucosevariability and preventing the occur-rence of severe hypoglycemia. Thebenefits of islet transplantation aresomewhat tarnished by decreasinglong-term insulin independence andimmunosuppression-related adverseevents. Safer immunosuppression andfurther strategies to promote long-term islet graft survival or other sourcesof islets remain an absolute prerequisitefor improving islet transplantation out-comes and increasing the availability ofthe procedure.
Acknowledgments. The authors thank thetechnical staff of the Cell Isolation and Trans-plantation Centers of Geneva (Solange Masson,David Matthey-Doret, Nadine Pernin, CarolineRouget, and Corinne Sinigaglia, Department ofSurgery, Islet Isolation, and TransplantationCenter, Geneva University Hospitals, Geneva,Switzerland) and Grenoble (Harald Egelhofer,Virginie Persoons, Florence de Fraipont, AnaickMoisan, and Marie-Jeanne Richard, CellularTherapy Unit [EFS Rhone-Alpes, Grenoble Uni-versity Hospital, Grenoble, France]); the trans-plant coordinators (Grenoble UniversityHospital, Geneva University Hospital); the ra-diology teams (Grenoble University Hospital);the clinical research associates (Grenoble Uni-versity Hospital); all of the Swiss and Frenchsurgical procurement teams (Grenoble Uni-versity Hospital, Geneva University Hospital);and Laure Nasse (Grenoble University Hospi-tal) for data management.Funding. The GRAGIL-1c and GRAGIL-2 trialswere supported by grants from ALFEDIAM, Asso-ciation Française des Diabetiques, Aide auxJeunes Diabetiques, Agir pour lesMaladies chron-iques, and the PHRC (Hospital Program for ClinicalResearch) from the FrenchMinistry of Health andby grant 3200B0-102134 from the Swiss NationalFoundation for Scientific Research.Duality of Interest. No potential conflicts ofinterest relevant to this article were reported.
Author Contributions. S.L., T.B., and P.-Y.B.participated in the research design, the perfor-mance of the research, the data analysis, andthe writing of the article. S.B., A.P., L.K., C.B.,and D.B. participated in the performance of theresearch and in the writing of the article. A.W.,F.B., R.T., L.B., C.T., E.M., L.F., and C.C. partic-ipated in the performance of the research. I.T.participated in the writing of the article. S.L. isthe guarantor of this work and, as such, had fullaccess to all the data in the study and takesresponsibility for the integrity of the data andthe accuracy of the data analysis.
References1. Fiorina P, Folli F, Zerbini G, et al. Islet trans-plantation is associated with improvement ofrenal function among uremic patients withtype I diabetes mellitus and kidney transplants.J Am Soc Nephrol 2003;14:2150–21582. Shapiro AM, Lakey JR, Ryan EA, et al. Islettransplantation in seven patients with type 1diabetes mellitus using a glucocorticoid-free im-munosuppressive regimen. N Engl J Med 2000;343:230–2383. Linetsky E, Bottino R, Lehmann R, AlejandroR, Inverardi L, Ricordi C. Improved human isletisolation using a new enzyme blend, liberase.Diabetes 1997;46:1120–11234. Barton FB, Rickels MR, Alejandro R, et al. Im-provement in outcomes of clinical islet trans-plantation: 1999-2010. Diabetes Care 2012;35:1436–14455. Bellin MD, Kandaswamy R, Parkey J, et al.Prolonged insulin independence after isletallotransplants in recipients with type 1 diabe-tes. Am J Transplant 2008;8:2463–24706. Bellin MD, Barton FB, Heitman A, et al.Potent induction immunotherapy promoteslong-term insulin independence after islettransplantation in type 1 diabetes. Am J Trans-plant 2012;12:1576–15837. Benhamou PY,Milliat-Guittard L,WojtusciszynA, et al.; GRAGIL group. Quality of life after islettransplantation: data from the GRAGIL 1 and 2trials. Diabet Med 2009;26:617–6218. Leitão CB, Tharavanij T, Cure P, et al. Restora-tion of hypoglycemia awareness after islet trans-plantation. Diabetes Care 2008;31:2113–21159. Warnock GL, Thompson DM, Meloche RM,et al. Amulti-year analysis of islet transplantationcompared with intensive medical therapy onprogression of complications in type 1 diabetes.Transplantation 2008;86:1762–176610. Thompson DM, Meloche M, Ao Z, et al. Re-duced progression of diabetic microvascularcomplications with islet cell transplantationcompared with intensive medical therapy.Transplantation 2011;91:373–37811. Benhamou PY, Oberholzer J, Toso C, et al.;GRAGIL consortium. Human islet transplanta-tion network for the treatment of type I diabe-tes: first data from the Swiss-French GRAGILconsortium (1999-2000). Groupe de RechercheRhin Rhĵne Alpes Geneve pour la transplanta-tion d’Ilots de Langerhans. Diabetologia 2001;44:859–86412. Badet L, Benhamou PY, Wojtusciszyn A,et al.; GRAGIL Group. Expectations and strate-gies regarding islet transplantation: metabolicdata from the GRAGIL 2 trial. Transplantation2007;84:89–96
13. Borot S, Niclauss N, Wojtusciszyn A, et al.;GRAGIL Network. Impact of the number of in-fusions on 2-year results of islet-after-kidneytransplantation in the GRAGIL network. Trans-plantation 2011;92:1031–103814. KempfMC, Andres A,Morel P, et al.; GRAGILgroup. Logistics and transplant coordinationactivityin the GRAGIL Swiss-French multicenter networkof islet transplantation. Transplantation 2005;79:1200–120515. Ricordi C, Lacy PE, Finke EH, Olack BJ,Scharp DW. Automated method for isolationof human pancreatic islets. Diabetes 1988;37:413–42016. Brons G. One more step along the road.Transplantation 2007;84:15–1617. TosoC,Baertschiger R,Morel P, et al.; GRAGILGroup. Sequential kidney/islet transplantation:efficacy and safety assessment of a steroid-freeimmunosuppression protocol. Am J Transplant2006;6:1049–105818. International Conference on Harmonisa-tion of Technical Requirements for Registrationof Pharmaceuticals for Human Use (ICH). Guide-line for IndustrydClinical Safety Data Manage-ment: Definitions and Standards for ExpeditedReporting. Brussels, Belgium, ICH, 200719. Ryan EA, Paty BW, Senior PA, Lakey JR,Bigam D, Shapiro AM. Beta-score: an assess-ment of b-cell function after islet transplanta-tion. Diabetes Care 2005;28:343–34720. Caumo A, Maffi P, Nano R, et al. Transplantestimated function: a simple index to evaluateb-cell secretion after islet transplantation. Di-abetes Care 2008;31:301–30521. Vantyghem MC, Kerr-Conte J, Arnalsteen L,et al. Primary graft function, metabolic control,and graft survival after islet transplantation. Di-abetes Care 2009;32:1473–147822. Vantyghem MC, Raverdy V, Balavoine AS,et al. Continuous glucose monitoring afterislet transplantation in type 1 diabetes: anexcellent graft function (b-score greater than7) is required to abrogate hyperglycemia,whereas a minimal function is necessary to sup-press severe hypoglycemia (b-score greaterthan 3). J Clin Endocrinol Metab 2012;97:E2078–E208323. Ryan EA, Paty BW, Senior PA, et al. Five-yearfollow-up after clinical islet transplantation. Di-abetes 2005;54:2060–206924. Ryan EA, Lakey JR, Paty BW, et al. Successfulislet transplantation: continued insulin reserveprovides long-term glycemic control. Diabetes2002;51:2148–215725. Shapiro AM, Ricordi C, Hering BJ, et al. In-ternational trial of the Edmonton protocol forislet transplantation. N Engl J Med 2006;355:1318–133026. Niclauss N, Bosco D, Morel P, et al. Influ-ence of donor age on islet isolation and trans-plantation outcome. Transplantation 2011;91:360–36627. Caiazzo R, Gmyr V, Kremer B, et al. Quanti-tative in vivo islet potency assay in normoglyce-mic nude mice correlates with primary graftfunction after clinical transplantation. Trans-plantation 2008;86:360–36328. Ichii H, Pileggi A, Molano RD, et al. Rescuepurification maximizes the use of human isletpreparations for transplantation. Am J Trans-plant 2005;5:21–30
care.diabetesjournals.org Lablanche and Associates 1721

29. Food and Drug Administration. Guidelinefor industrydclinical safety data manage-ment: definitions and standards for expeditedreporting [article online], 1995. Availablefrom http://www.fda.gov/downloads/drugs/guidancecomplianceregulatoryinformation/guidances/ucm073087.pdf. Accessed March199530. Lehmann R, Spinas GA,MoritzW,WeberM.Has time come for new goals in human islettransplantation? Am J Transplant 2008;8:1096–110031. Tanenberg RJ, Newton CA, Drake AJ. Con-firmation of hypoglycemia in the “dead-in-bed”syndrome, as captured by a retrospective
continuous glucose monitoring system. EndocrPract 2010;16:244–24832. McCoy RG, Van Houten HK, Ziegenfuss JY,Shah ND, Wermers RA, Smith SA. Increasedmortality of patients with diabetes reportingsevere hypoglycemia. Diabetes Care 2012;35:1897–190133. Retinopathy and nephropathy in patientswith type 1 diabetes four years after a trial ofintensive therapy. Am J Ophthalmol 2000;129:704–70534. Collaborative Islet Transplant Registry(CITR). Seventh annual report [article online],2011. Available from http://www.citregistry.org/. Accessed 30 December 2011
35. Gruessner RW, Gruessner AC. The currentstate of pancreas transplantation. Nat Rev En-docrinol 2013;9:555–56236. Kawahara T, Kin T, Kashkoush S, et al. Portalvein thrombosis is a potentially preventablecomplication in clinical islet transplantation.Am J Transplant 2011;11:2700–270737. Bucher P, Mathe Z, Bosco D, et al. Morbidityassociated with intraportal islet transplanta-tion. Transplant Proc 2004;36:1119–112038. Guignard AP, Oberholzer J, Benhamou PY,et al.; GRAGIL Group. Cost analysis of humanislet transplantation for the treatment of type1 diabetes in the Swiss-French ConsortiumGRAGIL. Diabetes Care 2004;27:895–900
1722 Islet Transplantation Within GRAGIL Network Diabetes Care Volume 38, September 2015





![212 - ŒIL ROUGE ET/OU DOULOUREUX- Ce qu’il …20_2010[1].pdf · - 115 - œil rouge et/ou douloureux sans traitement ; elle doit faire rechercher une hy-pertension artérielle.](https://static.fdocuments.net/doc/165x107/5b9568a409d3f2214e8cbe9c/212-oeil-rouge-etou-douloureux-ce-quil-2020101pdf-115-oeil-rouge.jpg)












