First-line management of follicular lymphoma: Will induction and maintenance treatment prolong...
27
First-line management of follicular lymphoma: Will induction and maintenance treatment prolong survival? Robert Marcus Department of Haematology, Addenbrooke’s Hospital, Cambridge, UK
-
Upload
keyon-masker -
Category
Documents
-
view
217 -
download
0
Transcript of First-line management of follicular lymphoma: Will induction and maintenance treatment prolong...
First-line management of follicular lymphoma: Will induction and maintenance treatment prolong survival?
Robert Marcus Department of Haematology,
Addenbrooke’s Hospital, Cambridge, UK
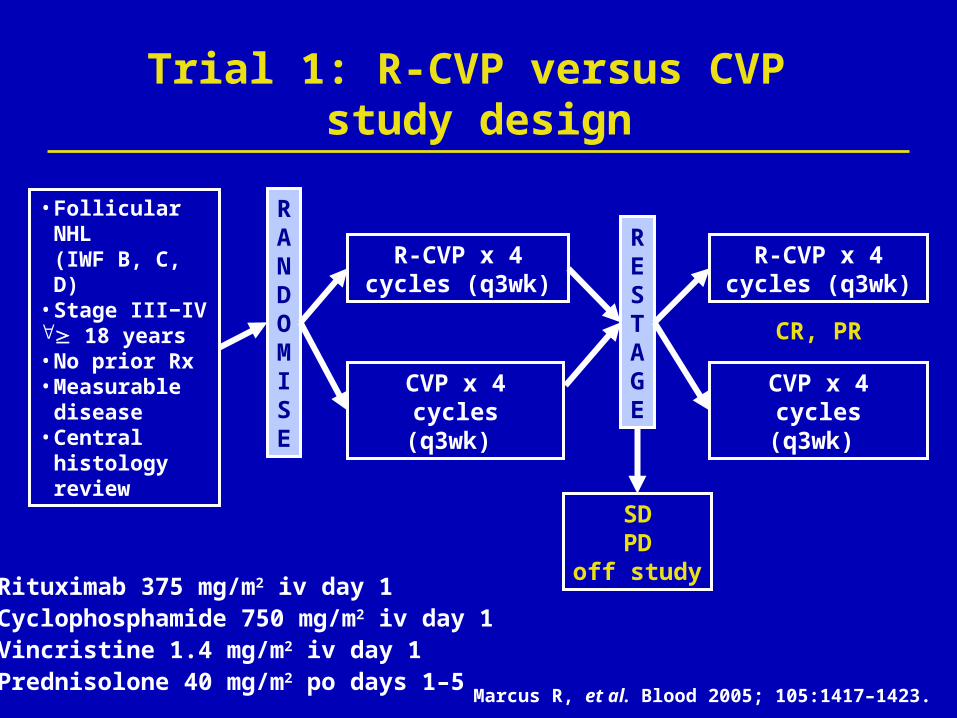
Trial 1: R-CVP versus CVP study design
• Follicular NHL (IWF B, C, D)
• Stage III−IV 18 years• No prior Rx• Measurable
disease• Central
histology review
RANDOMISE
CVP x 4 cycles(q3wk)
R-CVP x 4 cycles (q3wk)
CVP x 4 cycles(q3wk)
R-CVP x 4 cycles (q3wk)
SD PD
off study
CR, PR
Rituximab 375 mg/m2 iv day 1Cyclophosphamide 750 mg/m2 iv day 1Vincristine 1.4 mg/m2 iv day 1Prednisolone 40 mg/m2 po days 1–5
RESTAGE
Marcus R, et al. Blood 2005; 105:1417–1423.

Participating sites
Australia K Bradstock, J Catalano, R Herrmann, J McKendrick, J Norman, D Rosenfeld, K Taylor
Belgium M Bron, R De Bock, F Offner
Brazil C Chiattone
Canada A Belch, I Bence-Bruckler, M Crump, D Forrest, K Imrie, KS Robinson, C Shustik
France S Castaigne, P Solal-Céligny
Israel M Shaklai
Poland A Dmoszynska, K Kuliczkowski, J Walewski
Portugal F Placido, J Raposo, J Veiga
Spain JN Batista, M Constenla, E Flores, J Gomez Codina, J Guma, A Rueda
Switzerland T Cerny, R Zenhausern
UKD Cunningham, DJ Dunlop, E Fitzsimons, BW Hancock, C Hatton, P Johnson, R Marcus, G Morgan, A Pagliuca, R Pettengell, M Potter, C Poynton, S Proctor

Patient characteristics
CharacteristicR-CVP
(n = 162)CVP
(n = 159)
Median age, years 52 53
Histology
Grade 3 FL, % 9 8
Bulky disease, % 39 46
FLIPI 3−5 (poor prognosis), % 40 47
FLIPI 2 (intermediate prognosis), % 41 37
FLIPI 0−1 (good prognosis), % 19 15
Central review of pathology performed on 90% of patientsFL diagnosis confirmed in 95% of patients
Marcus R, et al. Blood 2005; 105:1417–1423.
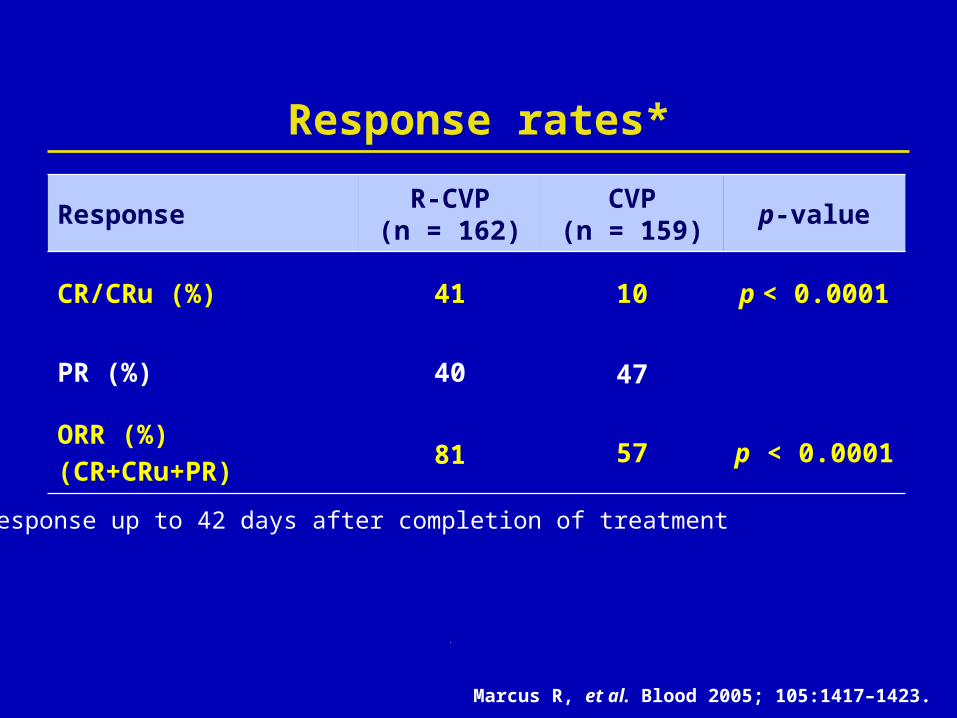
Response rates*
* Response up to 42 days after completion of treatment
ResponseR-CVP
(n = 162)CVP
(n = 159)p-value
CR/CRu (%) 41 10 p < 0.0001
PR (%) 40 47
ORR (%)(CR+CRu+PR)
81 57 p < 0.0001
Marcus R, et al. Blood 2005; 105:1417–1423.
Conclusions
Rituximab plus CVP improved:─ Overall and complete response rates─ TTP, TTNLT, DFS─ Overall survival
Addition of rituximab did not substantially increase regimen toxicity
8 cycles of R-CVP should be considered as standard treatment for previously untreated FL

Trial 2: R-CHOP versus CHOP study design
RANDOMISATION
6–8 cycles x CHOP
6–8 cycles x CHOP plus
rituximab
RANDOMISATION
PBSCT
Standard IFN-maintenance
Intensive IFN-maintenance
Standard IFN-maintenance
Hiddemann W, et al. Blood 2005; 106:3725–3732.
Patients > 60 years (> 65 years)
Patients < 60 years (< 65 years)
CR, PR
CR, PR
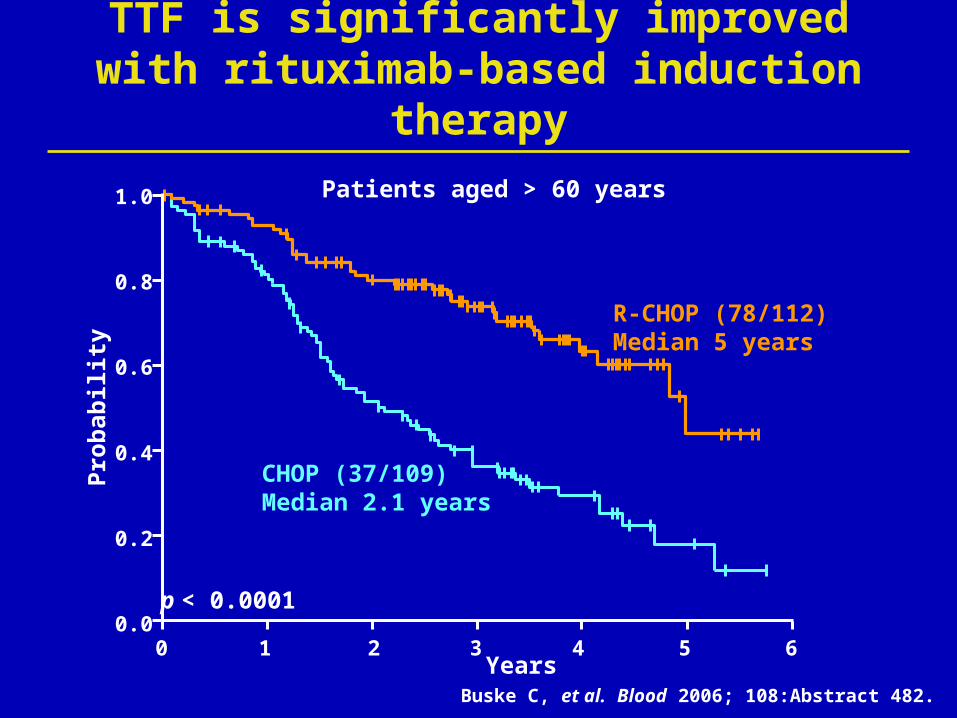
TTF is significantly improved with rituximab-based induction therapy
Buske C, et al. Blood 2006; 108:Abstract 482.
CHOP (37/109)Median 2.1 years
R-CHOP (78/112) Median 5 years
p < 0.0001
Patients aged > 60 years
Years0 1 2 3 4 5 6
Pro
bab
ilit
y
0.0
0.2
0.4
0.6
0.8
1.0
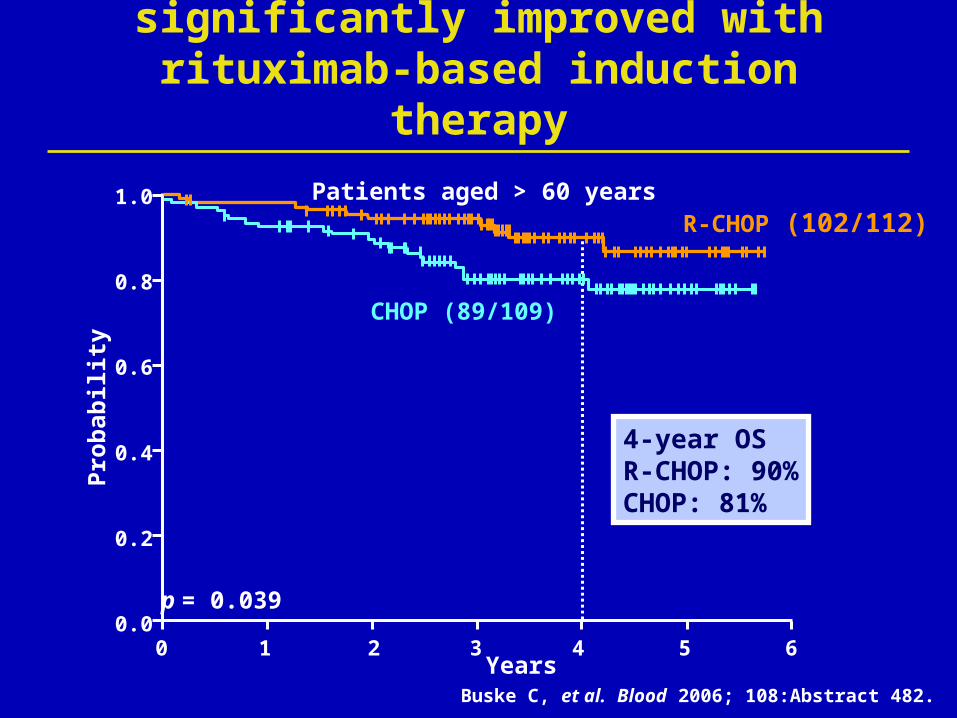
Overall survival is significantly improved with rituximab-based induction therapy
CHOP (89/109)
R-CHOP (102/112)
4-year OS R-CHOP: 90%CHOP: 81%
Years0 1 2 3 4 5 6
Pro
bab
ilit
y
0.0
0.2
0.4
0.6
0.8
1.0
p = 0.039
Buske C, et al. Blood 2006; 108:Abstract 482.
Patients aged > 60 years

Survival is significantly improved with R-CHOP in all FLIPI subgroups
FLIPI 0–1: Low risk p = 0.0091FLIPI 2: Intermediate prognosis p < 0.0001 FLIPI 3–5: Poor prognosis p = 0.0001
Median NR
Time (years)
Su
rviv
al p
rob
abil
ity
01 2 3 40 5
0.2
0.4
0.6
0.8
1.0
6
R-CHOP
Median NR
CHOP
Time (years)
Su
rviv
al p
rob
abil
ity
01 2 3 40 5
0.2
0.4
0.6
0.8
1.0
6
Median 4.1 years
Median 3.0 yearsMedian 4.0 years
Median 2.0 years
Buske C, et al. Blood 2006; 108:Abstract 482 and unpublished data.

Rituximab 375mg/m2 iv d 1Mitoxantrone 8 mg/m² iv d 3 and 4Chlorambucil 3 x 3mg/m² po d 3–7Prednisolone 25 mg/m² po d 3–7
Advanced FL, IC and MCL
18–75 yearsNo prior
rituximabCentral histology
reviewWritten informed
consent
RANDOMISED
R-MCP6 cycles(q4wk)
MCP6 cycles(q4wk)
RESTAGING
SDPD
off study
CR, PR
IFN-maintenance for FL
Trial 3: R-MCP versus MCP study design
R-MCP2 cycles(q4wk)
MCP2 cycles(q4wk)
Herold M, et al. J Clin Oncol 2007; April 9 (Epub).

Rituximab-based induction therapy significantly improves survival in patients with FL
p = 0.0096
R-MCP: Median NR
MCP: Median NR
0
0.25
0.50
0.75
1.00
0 10 20 30 40 50 60
Su
rviv
al d
istr
ibu
tio
n f
un
ctio
n
Time (months)
ITT population: Median follow-up 47 months
4-year OS R-MCP: 87%MCP: 74%
Herold M, et al. J Clin Oncol 2007; April 9 (Epub).
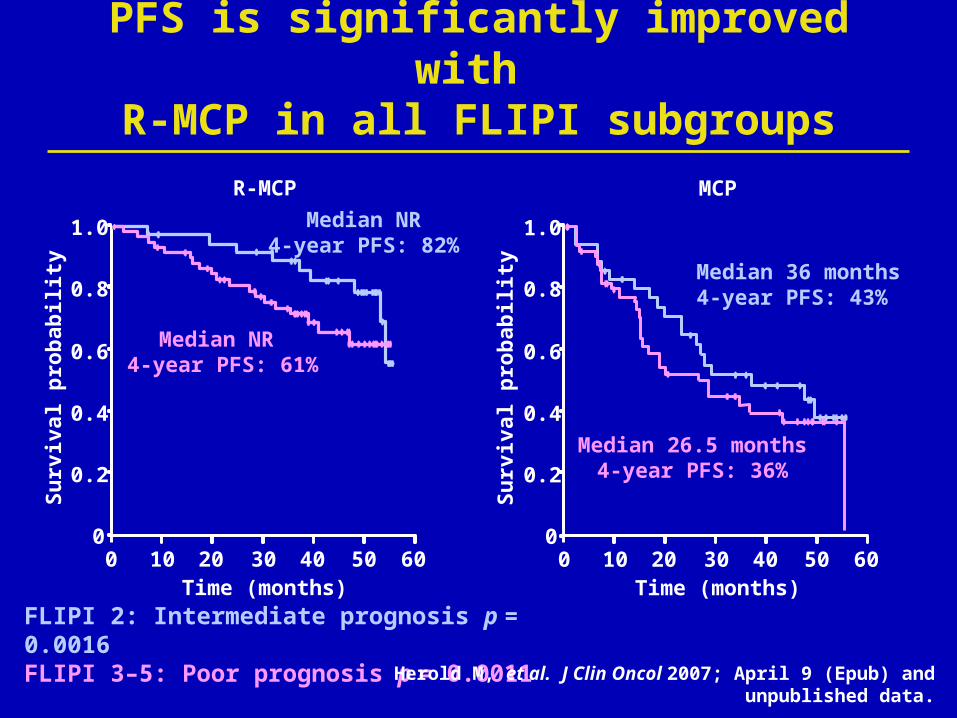
PFS is significantly improved with R-MCP in all FLIPI subgroups
FLIPI 2: Intermediate prognosis p = 0.0016 FLIPI 3–5: Poor prognosis p = 0.0011
Time (months)
Su
rviv
al p
rob
abili
ty
010 20 30 400 50
0.2
0.4
0.6
0.8
1.0
60
Median NR4-year PFS: 82%
Median NR 4-year PFS: 61%
Time (months)
Su
rviv
al p
rob
abili
ty
010 20 30 400 50
0.2
0.4
0.6
0.8
1.0
60
Median 36 months4-year PFS: 43%
Median 26.5 months4-year PFS: 36%
R-MCP MCP
Herold M, et al. J Clin Oncol 2007; April 9 (Epub) and unpublished data.
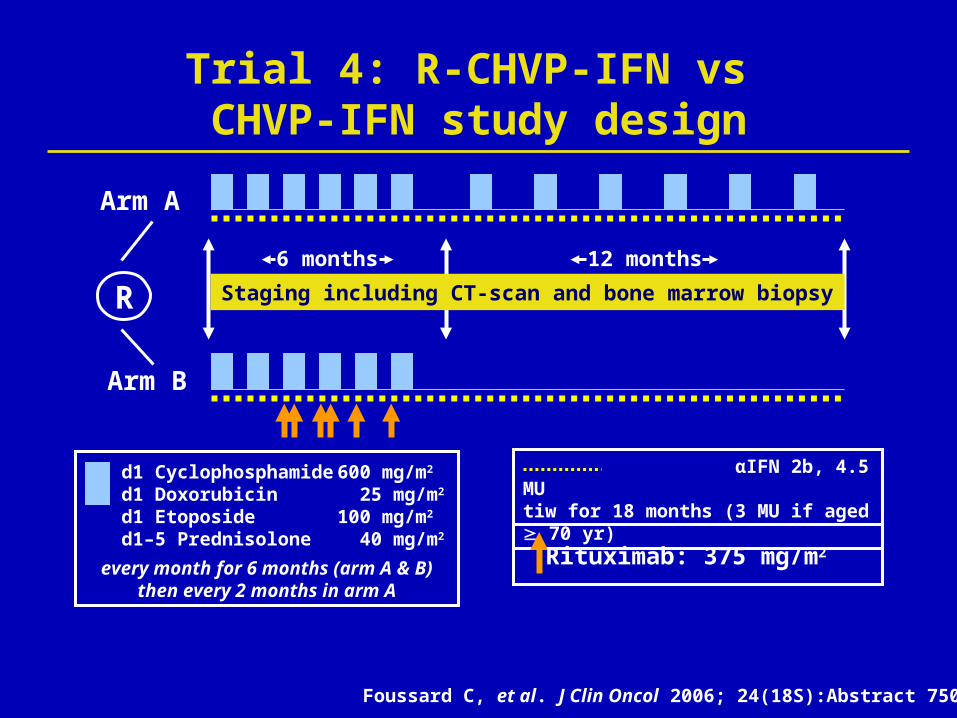
Trial 4: R-CHVP-IFN vs CHVP-IFN study design
αIFN 2b, 4.5 MU tiw for 18 months (3 MU if aged 70 yr)
d1 Cyclophosphamide 600 mg/m2
d1 Doxorubicin 25 mg/m2 d1 Etoposide 100 mg/m2 d1–5 Prednisolone 40 mg/m2
every month for 6 months (arm A & B) then every 2 months in arm A
Rituximab: 375 mg/m2
R
Arm A
Arm B
Staging including CT-scan and bone marrow biopsy
12 months6 months
Foussard C, et al. J Clin Oncol 2006; 24(18S):Abstract 7508.
Eve
nt-
free
su
rviv
al
0
25
50
75
100
0 10 20 30 40 50 60
p < 0.0001
70Months
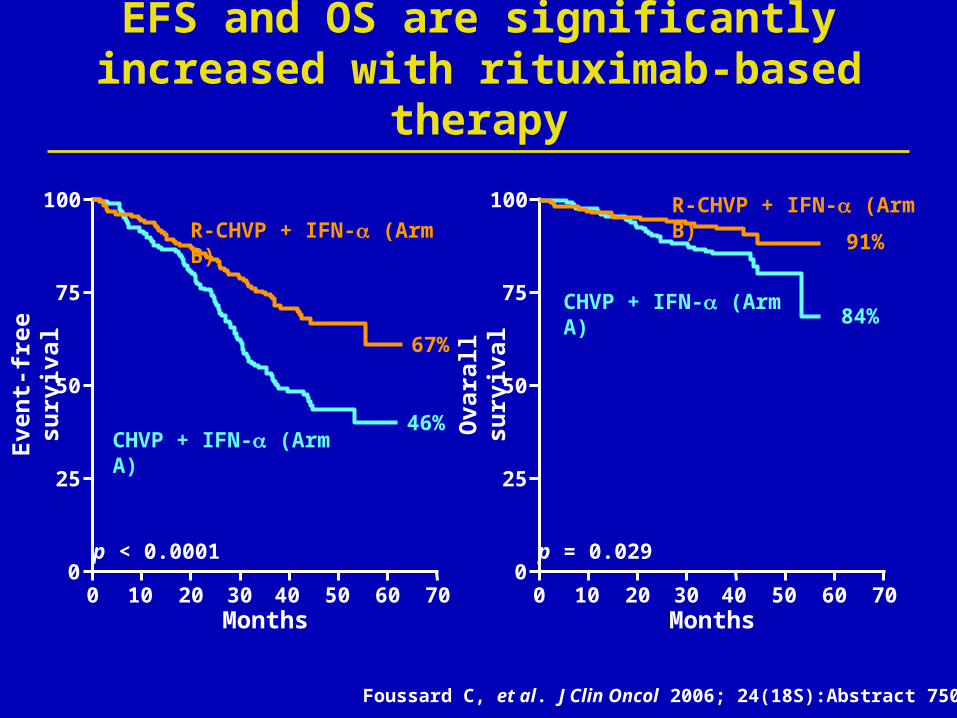
EFS and OS are significantly increased with rituximab-based therapy
67%
46%
R-CHVP + IFN- (Arm B)
91%
84%CHVP + IFN- (Arm A)
Ova
rall
su
rviv
al
0
25
50
75
100
0 10 20 30 40 50 60
p = 0.029
70Months
CHVP + IFN- (Arm A)
R-CHVP + IFN- (Arm B)
Foussard C, et al. J Clin Oncol 2006; 24(18S):Abstract 7508.

First-line rituximab-based induction therapy improves overall survival
1. Foussard C, et al. J Clin Oncol 2006; 24:Abstract 7508.2. Herold M, et al. J Clin Oncol 2007; April 9 (Epub).3. Hiddemann W, et al. Blood 2005; 106:3725–3732.
4. Marcus R, et al. Blood 2006; 108:Abstract 481.
Induction regimen Outcome (median) Overall survival
CHVP R + IFN-1 EFS NR vs 3 yrs p < 0.0001
3.5 yr 91% vs 84%p = 0.029
MCP R2 PFS NR vs 29 mo p < 0.0001
4 yr 87% vs 74%p = 0.0096
CHOP R3 TTF NR vs 31 mop = 0.0006
2 yr 95% vs 90%p = 0.016
CVP R4 TTP 34 mo vs 15 mop < 0.0001
4 yr 83% vs 77%p = 0.0290
Rituximab-based induction therapy: Conclusions
R-Chemo yields superior results to chemotherapy in four prospective randomised trials
The FLIPI predicts outcome in all studies─ Prognosis was worse with a high FLIPI score─ Majority of patients with poor prognosis will relapse
within 4–5 years─ There does not seem to be a TTP/PFS ‘plateau’
of any subgroup in any trial yet
24
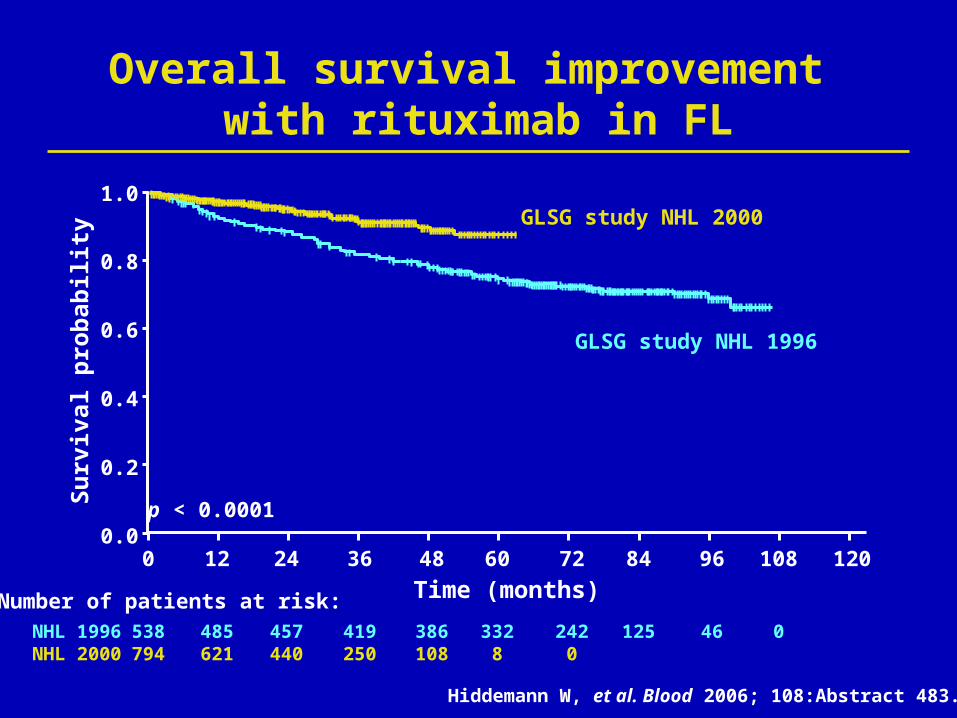
Hiddemann W, et al. Blood 2006; 108:Abstract 483.
Su
rviv
al p
rob
abil
ity
Time (months)
0.0
0.2
0.4
0.6
0.8
1.0
0 12 36 48 60 72
p < 0.0001
Number of patients at risk:NHL 1996NHL 2000
538 485 457 419 386 332794 621 440 250 108 8
2420
125 46 0
84 96 108 120
GLSG study NHL 2000
GLSG study NHL 1996
Overall survival improvement with rituximab in FL
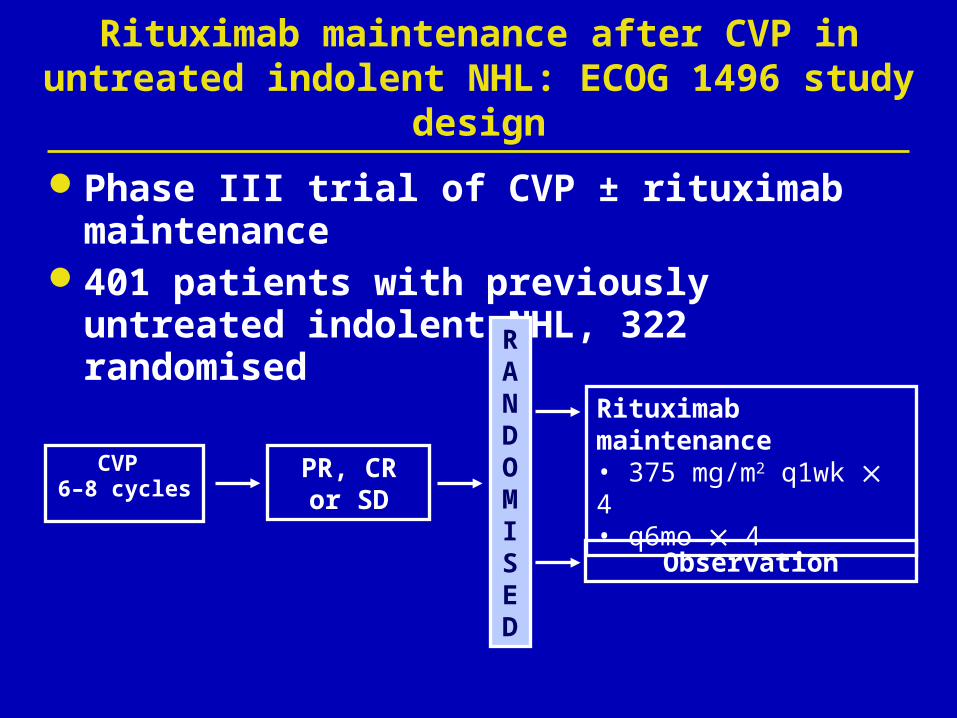
Rituximab maintenance after CVP in untreated indolent NHL: ECOG 1496 study design
Phase III trial of CVP ± rituximab maintenance401 patients with previously untreated
indolent NHL, 322 randomised
Observation
Rituximab maintenance • 375 mg/m2 q1wk 4• q6mo 4
RANDOMISED
PR, CR or SD
CVP 6–8 cycles
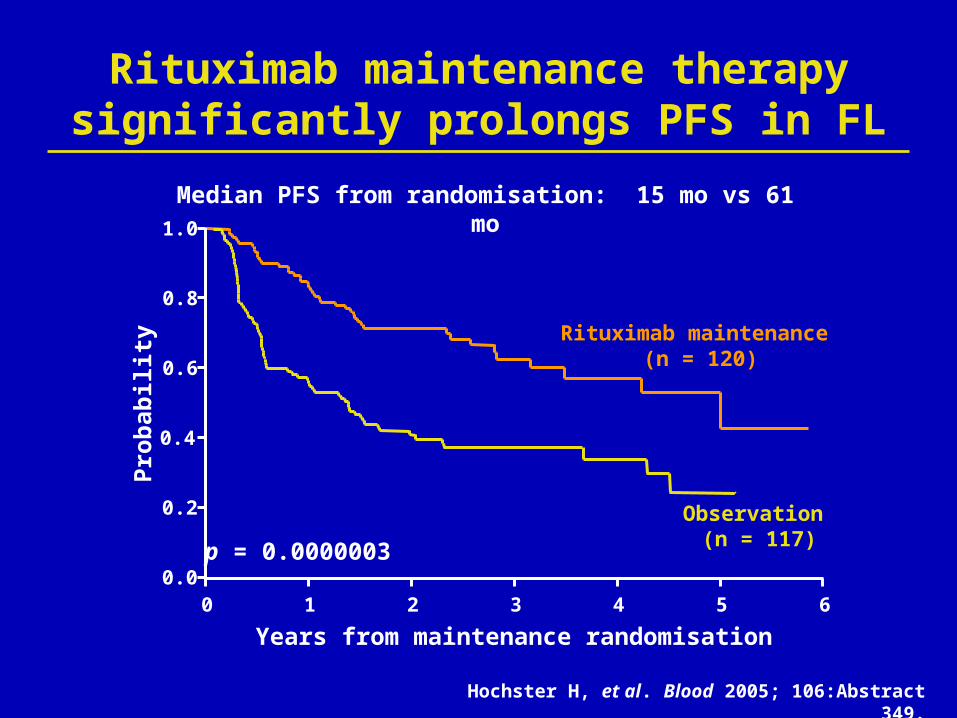
p = 0.0000003
Median PFS from randomisation: 15 mo vs 61 mo
Years from maintenance randomisation
Rituximab maintenance (n = 120)
Observation (n = 117)
Rituximab maintenance therapy significantly prolongs PFS in FL
0 1 2 3 4 5 60.0
0.2
0.4
0.6
0.8
1.0
Pro
bab
ilit
y
Hochster H, et al. Blood 2005; 106:Abstract 349.

Rituximab monotherapy induction and maintenance in first-line treatment of FL
Patients(n)
Median FU
(months)
Induction regimen
Maintenance schedule
Median PFS/EFS(months)
Minnie PearlPhase II1
38† 55 R-Mono* q6mo x 4* PFS: 52
SAKK 35/982
64 36 R-Mono* q2mo x 4EFS: 19 vs 36
p = 0.009
1. Hainsworth JD, et al. Blood 2003; 102:Abstract 1496.2. Ghielmini M, et al. Blood 2004; 103:4416–4423.
* 375 mg/m2 rituximab once weekly x 4† Follicular lymphoma patients onlyFU = follow-up

Rituximab maintenance q2mo x 4
PD, SD off study
Long maintenance
Rituximab375 mg/m²weekly x 4
Short maintenance
RPR, CR
Rituximab maintenance q2mo until relapse (maximum 5 years)
SAKK 35/03 study: Efficacy of extended rituximab maintenance therapy in FL
SDPD
off study
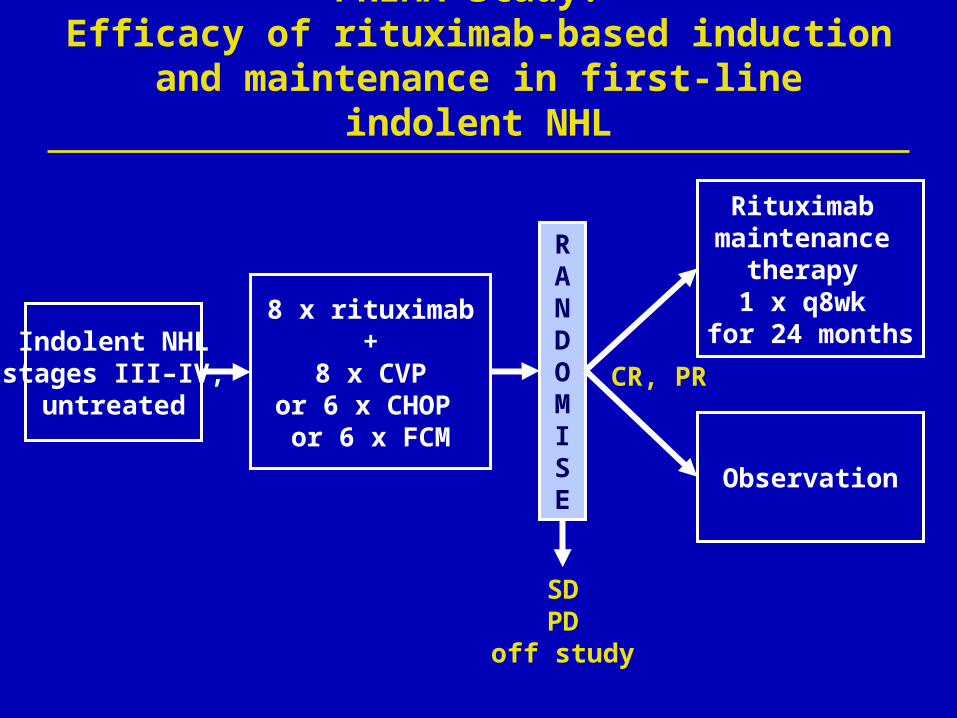
Indolent NHLstages III–IV,
untreated
Rituximab maintenance
therapy 1 x q8wk
for 24 months
Observation
8 x rituximab+
8 x CVPor 6 x CHOP or 6 x FCM
CR, PR
PRIMA study: Efficacy of rituximab-based induction and
maintenance in first-line indolent NHL
RANDOMISE

RiCHOP trial: Efficacy of ASCT followed by rituximab
maintenance in indolent NHL
Rituximab maintenance
1 x q8wk for 24 months
CR, PRR-CHOP x 6 + R x 2
HDTASCT
RANDOMISE
SDPD
off study
N > 600 patients with indolent FL (< 65 years old). Study start 2007

A note of caution! Incidence of hepatitis B reactivation with rituximab
Out of 456 patients, 32 were Hep B positive ─ 14 received rituximab monotherapy ─ 18 received rituximab plus chemotherapy
Group Patients (n) HBsAg HBsAb HBcAbLiver event
(%)
A 12 – + + 3 (25)
B 6 – – + 2 (33)
C 8 – Not available + 2 (25)
D 6 + Variable Variable 4 (66)
A total of 5 patients developed liver failure (15%)
Hanbali A, et al. Blood 2006; 108:Abstract 2766.

But…prophylactic lamivudine can reduce the incidence of hepatitis during chemotherapy
Non-randomised comparison of lymphoma patients treated with prophylactic lamivudine during chemotherapy with historical controls─ 100 mg was administered daily for up to 64 weeks
% Control(n = 116)
% Lamivudine
(n = 40) p-value
Hepatitis incidence during chemo 52 18 0.000
Disruption in chemo administration 37 10 0.001
Li Y, et al. Cancer 2006; 106:1320–1325.
Lamivudine prophylaxis reduced the incidence of hepatitis
Outstanding questions in first-line therapy for FL
Do more intensive therapies yield superior results than R-CVP?─ If so do ALL patients require such therapy, or only
poor prognosis patients? ─ Which component provides superior results?
Anthracycline, interferon or both?Does maintenance have a role in first-line FL?─ PRIMA trial to provide evidence
Do PBSCT or other approaches have a role in first-line therapy?