FIRST-AID TRAINING PROGRAMME: AN OVERVIEW
56
FIRST-AID TRAINING PROGRAMME: AN OVERVIEW REFERENCE
Transcript of FIRST-AID TRAINING PROGRAMME: AN OVERVIEW

FIRST-AID TRAINING PROGRAMME: AN OVERVIEW
REF
EREN
CE


FIRST-AID TRAINING PROGRAMME: AN OVERVIEW

2 FIRST-AID TRAINING PROGRAMME: AN OVERVIEW
CONTENTS
Preface .................................................................................................. 3
Abbreviations ........................................................................................ 6
1. General introduction ........................................................................ 7
2. The ICRC First-Aid Programme: What we do .................................... 92.1 Provisionoffirstaid .......................................................................................... 92.2 Respondingtocontext-specificneeds ....................................................... 102.3 Empowermentoftheemergencycareresponder .................................. 112.4 Chainofcasualtycare ....................................................................................... 14
3. The ICRC First-Aid Programme: What we offer ................................ 203.1 Deliveryoftrainingcourses............................................................................ 213.2 Technicalsupport ............................................................................................... 283.3 Sharingandreviewingexperiences ............................................................. 313.4 Provisionofmaterials,equipmentandfinance ...................................... 32
4. The ICRC First-Aid Programme: With whom we work ...................... 344.1 Firstaidforweaponbearers ........................................................................... 344.2 Firstaidforcommunities ................................................................................ 364.3 Firstaidforambulancepersonnel ............................................................... 374.4FirstaidforNationalSocietyvolunteersandstaff ................................ 384.5 Firstaidforhealthprofessionals.................................................................. 40
5. The ICRC First-Aid Programme: How we implement our programmes ............................................................................... 445.1 Results-basedmanagement ........................................................................... 445.2 Needsassessments............................................................................................. 455.3 Results,reviewandevaluation ...................................................................... 52
6. Final note ......................................................................................... 54

FIRST-AID TRAINING PROGRAMME: AN OVERVIEW 3
PREFACE
FirstaidonthebattlefieldwasoneofthefirstservicesprovidedbytheInter-nationalCommitteeoftheRedCross(ICRC).Furthermore,theInternationalRedCrossandRedCrescentMovement(Movement)has,sinceitsinception,beenmainlyassociatedwiththedeliveryoffirstaid.Provisionofanimmediateresponsetotheconsequencesofwars,disastersandepidemics,byfirst-aidersandlocalcommunities,wasaconceptpioneeredbytheMovement.Morethan150yearslater,firstaidisnowacoreactivityofmanyNationalRedCrossandRedCrescentSocieties(NationalSocieties).TheICRC,inaccordancewithitsmandate,remainsthechiefadvocateandthemaininternationalactorwithregardtotheprovisionoftraumafirstaidinarmedconflictandothersitua-tionsofviolence;theInternationalFederationofRedCrossandRedCrescentSocieties(IFRC),andtheNationalSocieties,usuallytakeabroaderapproachtofirstaid.AllMovementactorsareinvolvedinorsupportthedevelopmentoffirst-aidguidelinesonalocal,national,regional,andevenaninternational,basis.No guidelinefits all contexts; and to apply international guidelinesindiscriminately–withoutregardtodifferencesincustomandculture–istoignorerealityandtheneedsthatexist.Itiswidelyacknowledged–andnowthesubjectofagreatdealofdiscussion–thatfirst-aidguidelinesandactivi-tiesmustbemorecontext-specific.Thereisgeneralagreementthattwoissuesdeserveparticularlycloseattention.
Thefirstconcernstheneedforclearguidelines for first-aid programmes and for first-aid frameworks that enable the delivery of trauma first aid and basic emergency care in conflict-affected settings.Standardizedfirst-aidguidelinesandhandbooks–internationalandevennational–oftendonottakeintoaccountoraddresscontextsaffectedbyconflictorotherviolence.Asaresult,implementingtheseguidelinesinsuchcontextsmaysimplynotbepossible.Inthepastthreeyears,theICRC’sHealthUnitandtheICRC’sfirstaidandpre-hospitalemergencycareprogrammehavedevelopedfirst-aidguide-linesandframeworksthatareadaptedspecificallyforuseinsettingsaffectedbyconflictorotherviolence,andforusebythosewhotypicallyworkinsuchsettings.
4 FIRST-AID TRAINING PROGRAMME: AN OVERVIEW
Second,first-aid programmes and guidelines should be designed to fit the specific context in which they are to be implemented and the actors con-cerned.ICRCfirst-aiddelegatesandotherICRCpersonnelworkingintheareaoffirstaidmustassessandunderstandbothcurrentconflict-specificneeds(blastinjuries,gunshotwounds,burns,massivehaemorrhage,etc.)andthepre-existingneeds,diseases,constraintsandhealthinequitiesinthecontextinwhichtheyareoperating.Understandingconflict-specificneedsandthesocio-cultural context is crucial fordesigningefficientandeffectivefirst-aid programmes or emergency-care response systems for specific actors.Inadequatecontextualization(contextandactor)canresult in improperorerroneousprioritiesbeingsetforhealthservices;itcanalsohavedamagingconsequencesforemergency-caresystemsandsocialdynamics.
ICRCfirst-aidpersonnelalsoneedtoassessandunderstandexistingstruc-tures,servicesorlocalmethodsofresponse.Experiencehasshownthatwecanoftenassumetheexistenceofsomeleveloffunctioningbasichealthinfrastruc-turethatwecanconnectto,buildonorsupport.Itisessentialforeveryfirst-aidprogrammetocontinuallyevaluatetheservicesavailable,asthecontextsinquestionareusuallyinastateofflux.Inmostconflict-affectedcontexts,offi-cialhealthservicesbreakdownshortlyaftertheonsetoftheconflict;andcom-munity-based(informal)healthservices,whichoftensupplementorevenfullyreplaceofficialhealth-careservices,arefrequentlydisruptedbythefighting.
Ingeneral,standardizedinternationalapproachestofirstaidarenotsuffi-cientlyflexibleoradaptable.Theyare largelyWesternorWesternized;andeventheneedsassessmentsconductedwithintheseframeworkstendtobeone-offsnapshotsthatdonottakelocalcircumstancesintoaccount.TheICRCcontinuestograpplewiththechallengeofprovidingadequateandappropriate,andhencecontext-specific,emergencycareforconflict-affectedpopulations:for instance, itpushes formore localizedefforts.Localizationhasbecomesomethingofabuzzword:it isevenincludedinthenewICRCinstitutionalstrategy–butithasmanydimensionsandisinterpretedinmanydifferentways.Theconceptoriginatedintherecognitionthattherearelocalcapacitiesthatcanbetappedintoandbuilton;thatlocalactors,especiallytheNationalSocieties,aretherebefore,during,andafteranarmedconflict;andthattheseactorsunderstand the context and culture inquestion. Localized action isthereforepotentiallycapableofrespondingmoreeffectivelytotheneedsofpeopleaffected,assistingintheimplementationofservices,andstrengthen-ingtheresilienceofpeopleaffected.

FIRST-AID TRAINING PROGRAMME: AN OVERVIEW 5
Pleasenotethattheseguidelinesforfirst-aidtrainingprogrammeshavebeendevelopedprimarilyforICRCred-linemanagers,ICRCcoordinators(health,cooperation,protection,etc.),ICRChealth-programmemanagersand/orotherICRCpersonnelworkingintheareaoffirstaid–tohelpthemreachafullerunderstandingof theICRC’sfirst-aidtrainingprogrammes.Therefore, theguidelinesdonotcontainspecificclinicalguidanceforfirstaid.Pleasecon-tactyourfirst-aiddelegatesorthefirst-aidcoordinationteamfortechnicalorclinicalguidance.
Thomas WilpPre-hospitalEmergencyCareandFirst-AidCoordinatorInternationalCommitteeoftheRedCross

6 FIRST-AID TRAINING PROGRAMME: AN OVERVIEW
ABBREVIATIONS
EMS Emergencymedicalservices
EMT Emergencymedicaltechnicians
HCiD HealthCareinDanger
ICRC InternationalCommitteeoftheRedCross
IFRC InternationalFederationofRedCrossandRedCrescentSocieties
IHL Internationalhumanitarianlaw
IT Informationtechnology
MHPSS Mental-healthandpsychosocialsupport
NGO(s) Non-governmentalorganization(s)
OCHA UnitedNationsOfficefortheCoordinationofHumanitarianAffairs
PAHO PanAmericanHealthOrganization
PHEC Pre-HospitalEmergencyCare
RBM Results-basedmanagement
ToR Termsofreference
UN UnitedNations
UNDSS UnitedNationsDepartmentofSafetyandSecurity
WHO WorldHealthOrganization

FIRST-AID TRAINING PROGRAMME: AN OVERVIEW 7
1. GENERAL INTRODUCTION
1 Theterm‘sensitiveandinsecurecontexts’coversabroadrangeofcircumstances,includingthefollowing:situationsthatinvolvenoviolencebutthatnonethelesspresentemergency-careresponderswithperceptionoracceptanceissues;violentdemonstrations,riotsorspontaneousactsofrebellion(alsoreferredtoas‘internaldisturbances’or‘internaltensions’);armedconflict;andmanyothersituationscharacterizedbyvariouskindsofdisorder.Inaddition,naturaldisasters,andsituationswherebanditry,gangviolenceorotherformsofcriminalityarepervasive,cangiverisetosecurityandaccessissues.
ThefollowingoverviewoftheICRC’sfirst-aidtrainingprogrammesumma-rizesyearsoffirst-aid-relatedplanning,implementationandfieldobservation–operationaland/oreducational–invariouscircumstancesandcontexts,especiallyinsensitiveandinsecurecontexts1orthosewithlimitedresources(fragile/austereenvironments).Thefirst-aidtrainingprogrammeisaflexibleandadaptableprogrammeconsistingofseveraldifferentelements.Basicfirst-aidtrainingforfirstaidersandemergency-carerespondersisoneofthemostcommonactivitiesundertakenbytheICRC.Itequipsthepersonnelconcernedwiththeskillsandknowledgenecessarytorespondeffectivelyduringtimesofcrisis.TheICRCfirst-aidprogrammemayalsoofferotherservicesthatarenotalwaysregardedaspartofitsbrief:forinstance,workingwithlegalofficialstodevelopalegalframework–theso-called“GoodSamaritanlaw”–thatprovideslegalprotectionforpeopledeliveringfirstaidtothewoundedandthesick;theprotectionisintendedtoreassurefirst-aiderswhomaybehesitanttoprovidehelpbecausetheyareafraidofbeingsuedorprosecutedforcaus-ingunintentionalinjuryorwrongfuldeath.Thisfirst-aidtrainingprogrammeoverviewaimstoprovideapracticaloverviewofwhat,howandwherefirst-aidtrainingprogrammescanbeofferedbytheICRC.
Thisdocumentprovidesanoverviewonly of the ICRC first-aid training activ-ities.Separateoperationalguidelinesforfirstaidareavailableforfirst-aiddelegatesandotherICRCpersonnelworkingintheareaoffirstaid;andasep-arateoverviewoftheICRC’sPre-HospitalEmergencyCareprogramme(PHEC)anditsactivitieswillbeavailablein2021.

8 FIRST-AID TRAINING PROGRAMME: AN OVERVIEW
To ensure a coherent andmultidisciplinary approach, the following ICRC referenceframeworksshouldalsobeconsulted:
• referenceframeworksforotherhealth-caresub-programmes(AssistanceMedical,AssistanceOrthopaedics;WaterandHabitat–continuityofpatientcare):firstlevelofhealthcare;hospitalcare;physicalrehabilitationprogrammes;mental-healthandpsychosocialsupport(MHPSS);healthcareindetention
• referenceframeworkforforensicservices • referenceframeworkforweaponcontaminationandthecivilianpopulation • referenceframeworkforcooperation(NationalSociety/Movement–partneringandcapacitybuilding)
• referenceframeworkforprotectingthecivilianpopulationandthewoundedandthesick
• referenceframeworkforprotectingthecivilianpopulation(displacedpeople)
• Preventionreferenceframework–keyarea:acceptancefortheICRC.
FIRST-AID TRAINING PROGRAMME: AN OVERVIEW 9
2. THE ICRC FIRST-AID PROGRAMME: WHAT WE DO
2 “Red”supportreferstothespecifickindsofassistanceprovidedbytheMovement.
2.1 PROVISION OF FIRST AID
TheoverallgoaloftheICRC’sfirst-aidprogrammeistoensurethatduringemergencies(wars,conflictand/orviolence),woundedandacutelysickpeoplebenefitfromhumane,impartial,effectiveandsecureprovisionoffirstaid.Thiscareshouldbeprovidedbyconfident,skilledandproperlysupportedemergen-cy-carerespondersabidingbyhumanitarianvaluesandprinciples.Sometimes,casualtiesmayhavetobeevacuatedfordefinitivecare.ItmustbekeptinmindthattheICRC’sfirst-aidprogrammerarelysendsinICRCpersonnel–doctors,nurses,paramedics,etc.–toprovidedirecthelptovictimsofarmedconflictorothersituationsofviolence.ItisequallyimportanttonotethattheICRC’sfirst-aidprogrammemostoftenseekstoempowerindividuallocalfirst-aiders.
Toachievetheoverallgoalofprovidingfirstaid,thefollowingissuesmustalwaysbekeptinmind:
• TheICRCismandatedtooperateinsituationsofarmedconflictandotherviolence.These situations reveal the true degree of acceptance and effectiveness achieved by the emergency-care responders and the organization they represent.Acceptanceandeffectivenessaredependentonthedailyattitudesandworkoftherespondersandtheirorganization.
• Effectivemanagementofrisksandsecuritydependsonmanydifferentfactors:itshouldresultineverywoundedoracutelysickperson,andeveryemergency-careresponder,gettingtherespectandsupporttheyneed.
• Buildingfirst-aidcapacitieswillenablepeople to “make a difference”: the added or distinctive value that “Red” support2canprovidewillenablethemtodosoinawaythatisstronger,bigger,betterandmoredurable.Itishopedthatthisdistinctivenesswillberepaidthroughincreasedrespect,valueandappreciationfromthecommunity,patientsandtheirfamilies.
ThegeneralICRCapproachtofirstaidactivitiesduringemergenciesandforfirstaidempowermenthasthreeelements:people,context,andneedsandresults.

10 FIRST-AID TRAINING PROGRAMME: AN OVERVIEW
People - Experiences related to emergencies - Desire for involvement and level of confidence in responding
to emergencies - Practices, knowledge and perceptions related to emergencies,
and to preventing them - Practices, beliefs, and knowledge of the religious and cultural context
with regard to preventing and responding to emergencies
Context - Security - Resources available - Community resilience - Emergency-response system (who does what, where, when, and how) - Access to and performance of the people/facilities to whom or to which
emergency cases are referred for further care
Needs and Needs:results - Who is injured or acutely sick? How, when, where? - Nature, cause, and number of emergency situations and cases - Consequences of emergencies - Support for emergency preparedness and response
Results (care and humanitarian outcomes): - Immediate care; referral for further care; recovery - Social fabric: the relationships and connections between first aid
responders and the community - Humanitarian assistance (access to casualties, access to health care)
2.2 RESPONDING TO CONTEXT-SPECIFIC NEEDS
AllPHECservices(frombasicfirstaidtoprofessionalambulancecare)must becontext-specific.Thisensuresthateverypriorityneedisaddressedade-quatelyandappropriately;anditrequiresourfirst-aidprogrammesincon-flict-affectedsettingstobesufficientlyflexible.Basic,simpleandrealisticfirstresponsesmustbedeveloped–orwheretheystillexist,strengthened–toensurethemeaningfulparticipationoflocalactorsinthedevelopmentandimplementationofsuchresponses.Thefinalobjectiveistoensurethattheselocalactorsarewillingandabletofullytakeoveranfirst-aidresponse.Tothatend,ourlocalcounterpartsshouldbepermittedorenabledtoinfluenceandshapethefirst-aidresponsesystem–forexample,bytakinganactivepartinsettingprioritiesforourprogrammes(seealso:ICRC,Accountability to Affected
People – Institutional Framework).

FIRST-AID TRAINING PROGRAMME: AN OVERVIEW 11
All actors concerned need to ensure that emergency health responses areguidedstrictlybyacomprehensive, impartial, andevolvingassessmentofneeds.This requires the involvementofour local counterparts, thepeopleaffectedandtheICRC’sfirstaidandPHECteam.Itisimportanttoavoidpri-oritizingcertainactivitiesjustbecauseitiseasytodevelopthemandmeas-uretheireffectiveness,andtofocusprogrammesandresourcesonthemainemergencyhealthissuesineachparticularcontext.Localcopingmechanismsandlocalfirst-aidresponsesystemsneedtobebetterassessed,understood,andaddressedbymeansofa jointlyconducted–andeffective–first-aidprogramme.Giventhenumberofprotractedcrisesorrecrudescent/recurringconflicts, there isalsoaneedtothinkabouthowlocalfirst-aidguidelinesandprocedurescanbeadaptedandupdatedasnecessary,ratherthanseektoimplementstandardizedandmostlyWesternizedapproaches.Thisover-viewdescribestheICRC’sapproachtofirstaidtraining,theflexibilityofthisapproach, and the importance of conducting a proper assessment beforeundertakinganyfirstaidactivities(notonlytraining);italsoexplainswhywestronglyrecommendfollowingtheresults-based management(RBM)model.
2.3 EMPOWERMENT OF THE EMERGENCY-CARE RESPONDER
Anemergency-care responderissomeonewhoislikelytobepresentatthesceneofanemergency,andwhohasenoughconfidenceandtheskillsnec-essarytotendtopeopleaffected.Emergency-careresponderscanbedividedintofourcategories:
• first-aiders(trainedinbasicfirstaid)–inthecommunity,andamongweaponbearers,demonstrators,workers,etc.
• first responders(qualifiedinadvancedfirstaid)–membersofanemergency-responseorganization,suchasaNationalSociety,andcivildefencestaff,ambulance-servicepersonnel(includinginformalserviceproviders),healthministryofficials,etc.
• volunteer ambulance-service personnel(trainedinbasicambulancecare)–ambulancelayresponderswhocanbeembeddedinavarietyoforganizations/set-upsfromalargerorganizationlikeaNationalSocietyorjustfunctiononaverysmall/individuallevelascommunity-basedambulanceresponders.
• others(suchaspeoplewhoareevenmorequalified:professionalambulanceresponders,EMTsandparamedics)–thisgroupistrainedandsupportedthroughtheICRC’sPHECprogramme,butwillalsohavetoundergofirst-aidtraining.

12 FIRST-AID TRAINING PROGRAMME: AN OVERVIEW
Emergency-careresponderscanbeanyofthefollowing:
• membersofthegeneralpopulation,communityandinfluentialortrustedpersons(e.g.political,religiousorfinancialleaders)
• weaponbearers(stateandnon-state) • Movementstaffandvolunteers • publicandprivateemergency-serviceproviders • certaingroupsofpeople(e.g.demonstrators,journalists,religiousassemblies,NGOstaff,demininggroups,migrants/refugees,womenandyouthclubs,communitycooperatives,shopkeepers,hotelstaff,workers)
• ambulancepersonnel,taxi-drivers,andothersmobilizedtotransport/evacuatewoundedoracutelysickpeople
• community-basedhealth-careworkers,health-carepersonnel(dispensaries,clinics,hospitals),traditionalhealers.
An emergency-care responder should not regard themselves as “a saviour,
managing or resolving the situation by themselves”orconductthemselvesinsuchamanner.Instead,theyshouldseektorealizethefollowingobjectives:
• security:byinvolvingthecrowdofbystanders,relatives,and/orfriends,inordertolimitchaosandmitigatepotentialrisks
• humanity:byensuringdialogue,basicpsychosocialsupportandrespectfortheprivacyanddignityofthepeopleatthesceneoftheemergency,andrespectalsoforhumanitarianvaluesandprinciples
• efficiency:bymobilizingpeopleand,whenevernecessary,bymakingeffectiveuseoftheresourcesavailable
• resilience:byensuringthatpeoplepresentatthesceneofanemergencycanexercisetheirowncapacitytoactinsuchcircumstances
• continuum of care:bymakingsurethatwoundedorsickpeoplearecaredfor,fromthesceneoftheemergencyuntiltheirrecoveryorwhiletheyareevacuated/transportedelsewhereforfurthercare
• respect:thatis,ensuringrespectforthewoundedorsickpersonandforthepeopletendingtothemallalongthepatientjourney;andensuringrespectfortheprotectiveredcross,redcrescentandredcrystalemblemsaswell.Respondersshouldbeawarethatthepatientcouldbetheirlovedones,oreventhemselvesinthefutureandshouldtreatthemastheywouldwishtobetreated.
Theconsequencesoftheseachievementsmightbecomeapparent laterandelsewhere:forinstance,theymayleadpeopletobecomefirstaidersintheircommunities,orevenNationalSocietyfirstaidvolunteers.

FIRST-AID TRAINING PROGRAMME: AN OVERVIEW 13
Empowermentoftheemergency-carerespondershould:
• includerespondingtotheneedsexpressedbytheemergency-careresponders,andthecapabilitiesidentifiedbyothers
• beendorsedbytheauthorities/leadersconcernedorotheractors and sources of influence3
• beadaptedtothecharacteristics of that specific emergency-care responder4
• neverlosesightofthefactthatfirst aid seeks to preserve life,andthuspreservationoflifeshouldbeamatterofpriorityinwhateversupportoradviceisoffered.
Inordertoensurethatcasualtiesgettheassistancetheyneed,theemergen-cy-carerespondershouldbemotivated,andconfident.Theyshouldhavetheabilitytoperformalltheirtasksinasafe, humane and efficientway.Finally,theyshouldbeabletodisplayallthesecharacteristicsattheplaceandtimeofemergencysituations.Trainingintheseareaswillbringtheemergency-carerespondersclosertotherealitiestheymayfaceduringemergencies.Themain elementstoincorporateinanyprogrammeorprojecttodevelopandstrengthennecessaryskillsarelistedbelow:5
• safetyandsecuritymanagement6(managementofthesceneofanemergency,self-managementofstressandwhenrelevant,dealingwithweaponcontaminationorinfectiousdiseases)
• basiclife-savingandstabilizingmeasures(wounddressing,provisionofphysicalandpsychologicalcareforawoundedperson)
• basicpsychosocialsupport(reassurance,empathy,communication/explanationofstepstakentoprovideimmediatemedicalattentionandwhatthewoundedpersoncanexpecttohappennext,andseektheirconsent)
• mobilizationofbystandersanduseoflocalresources • transport/evacuation(forfurthercarewhennecessaryandpossible)
3 Actorsfromvariousspheres(political,religious,financial,etc.);‘meansofinfluence’ referstothevarioussources,suchassocialmediaandcommunities,thatareinfluentialinthatcontext.
4 Actorsfromvariousspheres(political,religious,financial,etc.);‘meansofinfluence’ referstothevarioussources,suchassocialmediaandcommunities,thatareinfluentialinthatcontext.
5 Theseelementsmustbeadaptedtolocalcircumstances,asthesewilldependuponmanyfactors,includingpossibilitiesforevacuation,qualityandfunctioningofreferralhealthstructures,etc.
6 WithguidancefromtheSaferAccessFrameworkaswell:http://saferaccess.icrc.org.

14 FIRST-AID TRAINING PROGRAMME: AN OVERVIEW
• ensuringrespectfortheredcross,redcrescentandredcrystalemblemsandforeverycasualtyandcareprovider,includingtheemergency-careresponder
• ensuringthewell-beingofthecareprovider(whichincludesreassuringhisorherrelativesandfriends)
• wheneverrelevant,thebasicelementsofdead-bodymanagement.
Empowermentofemergency-carerespondersthereforeentailsprovisionofa comprehensive package of knowledge, attitudes and skills, foruse inaholisticwayduringanemergency.
2.4 CHAIN OF CASUALTY CARE
As thefirst link in thecasualty care chain,first aid is crucial foranotherreason:itisalsothefirstpointofaccesstothehealth-caresystem.Optimalmanagementofthewoundedrequiresacontinuum of carefromthepointofwoundingorinjurytotheirstayinhospital,anduptowhenthepatientsarebackintheircommunities.Hospitalswouldlikepatientstohavebeenproperlystabilizedbeforetheirarrival,inatimelymannerandinorderofpriority.Tolearnhowthiscanbeachieved,itisnecessarytokeepthisinmind:firstaidistheinitialassistancegiventoaninjuredorsickpersonuntilhisorhercondi-tionhasbeenstabilizedorremedied,orahigherlevelofcare–forinstance,ahospital–canbereached,orprofessionalmedicalhelpismadeavailable.
Whatleveloffirstaidisavailableandhowfirstaidisdeliveredvariesaccord-ing to security conditions; thenumberandconditionof thewounded; theresourcesthatcanbemobilized;transportcapacity;theavailabilityofemer-gencymedicalservices(EMS);accesstofurthercare,ortheavailabilityofsuchcare,andthecapacitiesofsecondary-carefacilities.
Sinceitsinception,theMovementhasbeenassociatedmainlywithfirstaidprovision. Itpioneeredtheconceptofprovidingan immediateresponse totheconsequencesofwars,disastersandepidemics,byfirst-aidersandlocalcommunities.
ThegoalsofanICRCfirst-aiderare:
• tointervenesafelyandsecurely • topreservelifebysupportingvitalsystemsofthebody

FIRST-AID TRAINING PROGRAMME: AN OVERVIEW 15
• tolimittheeffectofinjuryandtopreventfurtherinjuries • topreventcomplicationsanddisability • toprovidepsychosocial/moralsupportandalleviatesuffering • topromoterecovery • toensureproperhandoveroftheinjuredandthesicktothenextlevel ofcareortohealth-careprofessionals.
First-aiderscanalsohelpmobilizetheircommunitytoprepareforandrespondtodailyemergenciesortothosethatariseduringcrisessuchasarmedconflictorotherviolence.DecadesofICRCexperiencehaveshownthatthepre-hos-pitalphaseisvitallyimportantindeterminingthefateofthewar-wounded.It is an irrefutable truth that first aid saves lives and decreases morbidity. Effectivefirstaidreducestheburdenonhospitalsbymakingiteasierforthemtoprovidesurgeryandotherformsofmedicalattention.
Firstaidprovisionisoneofthefundamentalresponsibilitiesofmilitarymed-ical services, National Societies and, increasingly in contemporary armedconflicts,ofmedicalstaffinbothruralandurbanpublichospitals.Localcom-munitiesplayanessentialroleinprovidingassistanceonthespot,aswit-nessedbyHenryDunantafterthebattleofSolferinoon24June1859.DunantwasoneofthefoundersoftheRedCrossandtheinspirationfortheoriginalGenevaConventionof1864.
Consequently,supportforbasicfirst-aidtraining–bothinitialandrefresher–shouldbeprovidedto:
• thegeneralpopulation(community-basedfirstaid) • soldiersandmembersofsecurityforces • non-Statearmedgroupsandoppositiongroups • community-basedhealthworkers(includingambulancepersonnel) • militaryandothermilitarymedicalservices.
Itissafetoassumethatmilitarycommanderswillnotwanttodiminishtheirfightingcapacitybyusinghealthytroopstotransfertheirwoundedcomrades,onlybecauseoftheinadequacyoffirstaidservicesinthefield.
Advancedfirst-aidtrainingcanbeaddedtothecurriculumofthosealreadytrainedinbasicfirstaidandwhosespecifictaskitistoprovidefirstaidinthefield,suchasmilitarymedicsandNationalSocietyfirst-aidteams.

16 FIRST-AID TRAINING PROGRAMME: AN OVERVIEW
First aid in the chain of casualty careFirstaidstartsatthepointofwoundingorinjury,canbegiventhroughoutthecasualtycarechain,untilthesiteofdefinitivetreatment.
Point of woundingOn-the-spotfirstaidisoftenadministeredonthebattlefielditself;combat-antsandotherweaponbearersmaygiveittothemselvesortotheircomrades,iftheyhavereceivedtheappropriatefirst-aidtraining.Otherwise,firstaidisprovidedbymilitarymedicsandNationalSocietyfirst-aidersorothercivilians.
Collection pointItiscommonpractice,andconvenient,tobringallthewoundedtoonespot,whenthesituationpermitsit.Thisgatheringtogetherofcasualtiesenablesthefollowing:effectiveevaluationoftheircondition;firstaidprovisionifthathasnotalreadyhappened;stabilizationforthoseforwhomlife-savingmeas-ureshavealreadybeentaken;andfinally,themakingofdecisionsaboutwhoneedstobeevacuatedforfurthertreatment–inaccordancewithtriageprior-ities.Afirst-aidpostisneededforthisprocesstobemosteffective:therefore,instructioninsettingupandrunningafirst-aidpostmayalsoformapartoffirstaidtraining.
EvacuationThe decision to transport awounded person should be taken only after adetailedassessment,becauseofthedangersanddifficultiesinherentinsit-uationsofarmedconflict.Regardlessofthemeansoftransportusedalongthecasualtycarechain,firstaidmeasuresshouldbemaintainedthroughout.Patientreferralistaughtinadvancedfirst-aidtrainingandinbasictrainingforambulancepersonnel.
Hospital emergency roomIntheruralareasofpoorcountriesandduringurbanwarfare,thefirstplacewhereanyprofessionalcareisavailableisoftentheemergencyreceptionofanestablishedhospital.Evenwhenthereisanefficientemergencytransportser-vice,familiesandneighboursoftendonotwaitforit;theyprefertotransporttheirwoundedrelativeorneighbourdirectlytoahospital,wheretheemer-gencyroomthenservesasafirst-aidpost.
FIRST-AID TRAINING PROGRAMME: AN OVERVIEW 17
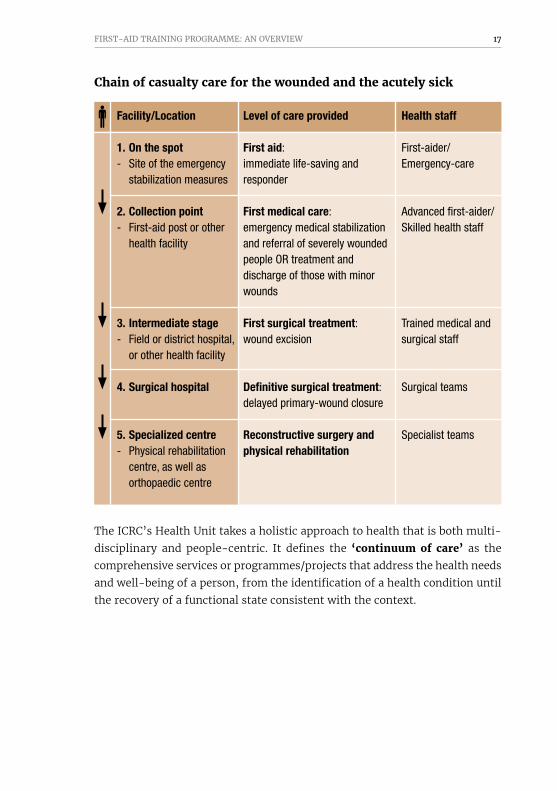
Chain of casualty care for the wounded and the acutely sick
Facility/Location Level of care provided Health staff
1. On the spot First aid: First-aider/ - Site of the emergency immediate life-saving and Emergency-care stabilization measures responder
2. Collection point First medical care: Advanced first-aider/ - First-aid post or other emergency medical stabilization Skilled health staff health facility and referral of severely wounded people OR treatment and discharge of those with minor wounds
3. Intermediate stage First surgical treatment: Trained medical and - Field or district hospital, wound excision surgical staff or other health facility 4. Surgical hospital Definitive surgical treatment: Surgical teams delayed primary-wound closure 5. Specialized centre Reconstructive surgery and Specialist teams - Physical rehabilitation physical rehabilitation centre, as well as orthopaedic centre
TheICRC’sHealthUnittakesaholisticapproachtohealththatisbothmulti-disciplinary andpeople-centric. It defines the ‘continuum of care’ as thecomprehensiveservicesorprogrammes/projectsthataddressthehealthneedsandwell-beingofaperson,fromtheidentificationofahealthconditionuntiltherecoveryofafunctionalstateconsistentwiththecontext.

18 FIRST-AID TRAINING PROGRAMME: AN OVERVIEW
ICRC Continuum of care
Thecontinuum-of-careapproachdrawsonexpertisefromeveryhealthpro-gramme,includingfirstaid,andconnectswithareasbeyondhealth,suchasinfrastructure,waterandsanitation,economicsecurity,andprotection.
Thehealthstatusofpopulationsistheresultofseveralinterlinkedfactors,andunderstandingitrequiresamultidisciplinaryassessmentoftheneedsandrisks,theresourcesavailable,andprotectivefactors.Itfollowsfromthisthatoperationalprogrammesthattargetcriticalgaps,andaddressarangeofsocialdeterminantsforagivenhealthissue,willhavethemostimpact.TheICRC’sfirstaidandpre-hospitalemergencycareprogrammestrivestoclosegapsinaccesstoheathcare,inpre-hospitalemergencycare,andinreferralservices. Continuum of caredoesnotmeanacontinuumofICRCoperations.TheICRCdoesnotthereforeneedtobeactiveinallareasofitsprogrammingineachgivencontext.Itmust,however,beabletoidentifyandlinkactorsthatsupportthecontinuumofcareforthetargetpopulation.
Traditional birth attendants
Red Cross and Red Crescent Psychosocial focal pointsfirst responders
Persons with disabilities
Detainees and their families
Primary health care
Physical rehabilitation
Health carein detention
Prehospitalemergency
care
Traumafirst aid
Mental health and
psychosocial support
Continuum
Continuum
Tert
iary
Seco
ndar
yPr
imar
y
Community
Leve
ls o
f car
e
Economic Security - Water & Habitat
Protection

FIRST-AID TRAINING PROGRAMME: AN OVERVIEW 19
Firstaidandpre-hospitalemergencycarehavebecome,inconflict-affectedcontexts,somethingofafrontlinefornumerouscriticalinternationalhuman-itarianlaw(IHL)andpolicyissues:thedenialoffirstaidorpre-hospitalcareasatacticofwar;theabrogationofneutralitybymilitaryfirstresponders;the involvementof theprivate sector in frontlinepre-hospital emergencyresponses;anddisregardfortheprinciplesofprecaution,distinctionandpro-portionalityintheconductofhostilities.
OneofthekeyobjectivesoftheICRC’sHealthUnit,andthereforeakeyobjec-tiveofthepre-hospitalandfirstaidprogrammeaswell,istocontributetoprotectingtherighttohealthofpeopleinneed.Progressionalongthecasualtycarechainstartswithaccesstobasicfirstaidfromlaypersonsand/oraccesstoareferralsystemforpre-hospitalemergencycare.Inconflict-affectedcon-texts,between40and60%ofallinjuredciviliansandweaponbearersdonotrequirehospitalization:basicfirstaidandsimpleoralantibioticsandanalge-sicsarealltheyneed.Simpleandeffectivefirstaidsystemscanandshouldthereforebeattheforefrontofanyhealth-careresponseforconflict-affectedpeople.

20 FIRST-AID TRAINING PROGRAMME: AN OVERVIEW
3. THE ICRC FIRST-AID PROGRAMME: WHAT WE OFFER
FirstaidintheICRCcontextshouldnotbeunderstoodtomeanjustasetofbandagesorlistsofequipment,oraseriesoftrainingcourses.Itsperspec-tive ismuchbroader: it includesoperational issues(contingencyplanning,lawsandregulations,securitymanagement,developingresponseandrefer-ralsystemswiththefieldactors,logistics,follow-upandmonitoring,etc.)andmulti-dimensionalhumanvalues(copingresources,engagementspirit,psychosocialissues,resourcefulnessetc.).Thefirst-aidtrainingprogrammeseekstofurtherdevelopand/orstrengthenpeopleandorganizationsinvolvedinemergencypreparednessandresponse,especiallyincontextsthataresen-sitiveandinsecureorwhereresourcesarelimited.Itispreparedtoaugment,supportand/orcarryouttheactivitiesdescribedbelow.
Analysis ofand participationin the casualty
care chain
Supportand coaching
for teams
Deliveryof first-aid
trainingcourses
Adviceon technical
and/oroperational
matters
Provisionof materials
and equipment
Sharingand reviewingexperiences
Developingand reviewing
contingency plans
Deliveryof first-aid
trainingcourses
Provisionof materials
and equipment

FIRST-AID TRAINING PROGRAMME: AN OVERVIEW 21
3.1 DELIVERY OF TRAINING COURSES
Beforeundertakinganyactivitiesinaparticularcontext,theICRCcarriesoutaneedsassessmentandanalysis;thisisthecasethroughouttheorganization.Aftertheneedsassessmentandanalysisitwillseektoundertakeorsupportthoseactivitiesthatcanbeadaptedtotheneedsofthetargetgroup(s).Oneoftheseactivitieswillusuallybeeducational,suchastraininginbasicand/oradvancedfirstaid.Forthepurposeofthisoverview,thetrainingactivitiesmentionedbelowareforfirst-aid training only:PHECtrainingforqualifiedpre-hospitalhealthpersonnel(e.g.paramedics,EMTs,ambulancenursesand/orpre-hospitalemergencyphysicians)andotherskilledhealthprofessionalswillbeoutlinedinthePHECguidelines.
Thedecisiontoofferbasicoradvancedfirst-aidtrainingwilldependontheknowledgeandproficiencyofparticipants.Thismustbeevaluatedduringthefirstaidneedsassessmentthatiscarriedoutbeforeimplementinganyfirstaid-relatedactivities.Advancedfirst-aidtrainingcanbeofferedonlytopartic-ipantswhohavemasteredallaspectsofbasicfirstaid;theymustalsohaveabackgroundinformalorinformalmedicine.Passingacourseinbasicfirstaiddoesnotautomaticallyqualifysomeoneforadvancedfirst-aidtraining.
Peopleinvolvedinthecontinuumofcareforthewoundedandtheacutelysickwillencounternumerouschallengeswhentreatingandtransportingcasualtiesfromsceneofanemergencytoacollectionpointorsiteofintermediatecare.Theymustbeempoweredtothinkcreatively(thehowandwhy)andfocusonessentialaction-relatedprinciplesandlimits(thewhat).Thiswillenablethemtomakedecisionsthataresafeandeffective–before,during,andaftertheemergencyresponse.
StandardICRCtraininginbasicfirstaidaimstoempowerthefirst-aidertobemotivated,confidentandskilledtoperformallaspectsofbasicfirstaidinamannerthatissafe, humane and efficient.Thisgoalcanbeachievedonlyiftheapproachtotrainingispragmatic, realistic and eclectic.ICRCtrainingworkshopsinfirstaid(forallserviceproviders)aregroundedinpracticeratherthantheory:theyinvolvesimulations/practicesthatarecloselyalignedtotherealitiesthatparticipantshavetodealwith.CasesimulationsaredesignedandpreparedbytheICRCfirst-aiddelegateand/orfirst-aidfieldofficer;andICRCfirst-aidtrainingusuallyfocusesontraumaandtraumatic injuries,whicharetypicalofthecontextsinwhichtheorganizationworks.
22 FIRST-AID TRAINING PROGRAMME: AN OVERVIEW
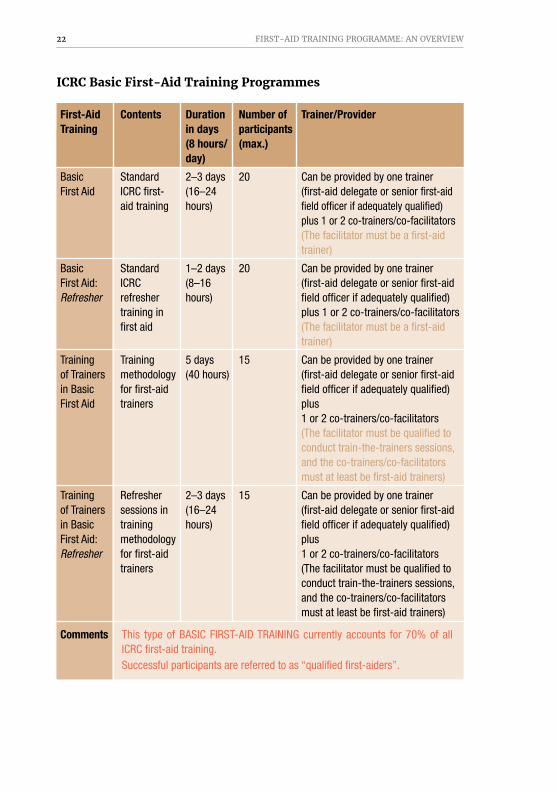
ICRC Basic First-Aid Training Programmes
First-Aid Contents Duration Number of Trainer/Provider Training in days participants (8 hours/ (max.) day)
Basic Standard 2–3 days 20 Can be provided by one trainer First Aid ICRC first- (16–24 (first-aid delegate or senior first-aid aid training hours) field officer if adequately qualified) plus 1 or 2 co-trainers/co-facilitators (The facilitator must be a first-aid trainer)
Basic Standard 1–2 days 20 Can be provided by one trainer First Aid: ICRC (8–16 (first-aid delegate or senior first-aid Refresher refresher hours) field officer if adequately qualified) training in plus 1 or 2 co-trainers/co-facilitators first aid (The facilitator must be a first-aid trainer)
Training Training 5 days 15 Can be provided by one trainer of Trainers methodology (40 hours) (first-aid delegate or senior first-aid in Basic for first-aid field officer if adequately qualified) First Aid trainers plus 1 or 2 co-trainers/co-facilitators (The facilitator must be qualified to conduct train-the-trainers sessions, and the co-trainers/co-facilitators must at least be first-aid trainers)
Training Refresher 2–3 days 15 Can be provided by one trainer of Trainers sessions in (16–24 (first-aid delegate or senior first-aid in Basic training hours) field officer if adequately qualified) First Aid: methodology plus Refresher for first-aid 1 or 2 co-trainers/co-facilitators trainers (The facilitator must be qualified to conduct train-the-trainers sessions, and the co-trainers/co-facilitators must at least be first-aid trainers)
Comments This type of BASIC FIRST-AID TRAINING currently accounts for 70% of all ICRC first-aid training. Successful participants are referred to as “qualified first-aiders”.

FIRST-AID TRAINING PROGRAMME: AN OVERVIEW 23
ICRC Advanced First-Aid Training Programmes
First-Aid Contents Duration Number of Trainer/Provider Training in days participants (8 hours/ (max.) day)
Advanced Advanced 2–3 days 15 Can be provided by one trainer First Aid (medically (16–24 (first-aid delegate or senior first-aid based) first- hours) field officer if adequately qualified) aid training plus 1 co-trainer/co-facilitator (The facilitator must be a first-aid trainer and have a medical background)
Advanced Refresher 1–2 days 15 Can be provided by one trainer First Aid: training (8–16 (first-aid delegate or senior first-aid Refresher (medically hours) field officer if adequately qualified) based) in plus 1 co-trainer/co-facilitator advanced (The facilitator must be a first-aid first aid trainer and have a medical background)
Training Training 5–7 days 10 Can be provided by one trainer of Trainers methodology (40–56 (first-aid delegate or senior first-aid in Advanced for trainers hours) field officer if adequately qualified) First Aid in advanced plus 1 co-trainer/co-facilitator first aid (The facilitator must be a qualified master trainer in first aid, and the co-trainer/co-facilitator must be at least a trainer of trainers; both should have a medical background)
Training Refresher 2–3 days 10 Can be provided by one trainer of Trainers sessions (16–24 (first-aid delegate or senior first-aid in Advanced in training hours) field officer if adequately qualified) First Aid: methodology plus 1 co-trainer/co-facilitator. Refresher for trainers (The facilitator must be a qualified in advanced master trainer in first aid, and the first aid co-trainer/co-facilitator must be at least a trainer of trainers; both should have a medical background)
Comments To be delivered only to medical/emergency-medical-care professionals and/or to people with long-standing involvement in first aid, like senior National Society first aid volunteers or trainers capable of managing all aspects of basic first aid. Successful participants are referred to as “qualified first responders”.
24 FIRST-AID TRAINING PROGRAMME: AN OVERVIEW
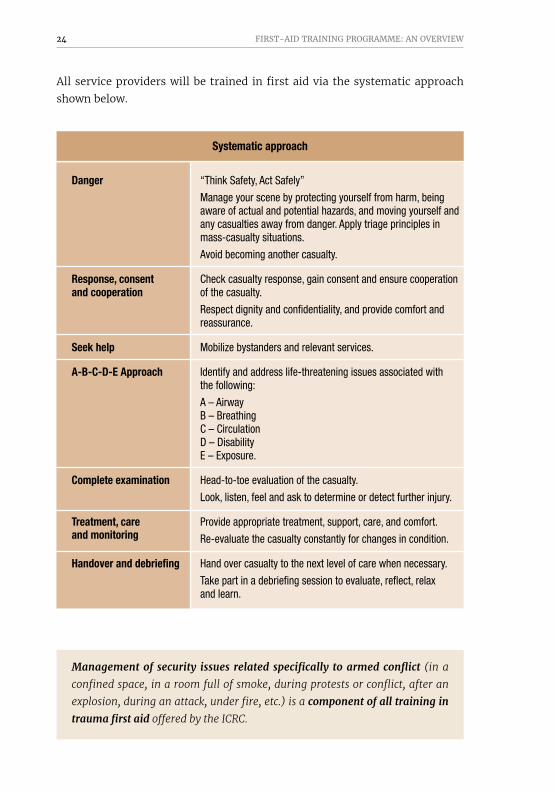
Allserviceproviderswillbetrainedinfirstaidviathesystematicapproachshownbelow.
Systematic approach
Danger “Think Safety, Act Safely”
Manage your scene by protecting yourself from harm, being aware of actual and potential hazards, and moving yourself and any casualties away from danger. Apply triage principles in mass-casualty situations.
Avoid becoming another casualty.
Response, consent Check casualty response, gain consent and ensure cooperation and cooperation of the casualty.
Respect dignity and confidentiality, and provide comfort and reassurance.
Seek help Mobilize bystanders and relevant services.
A-B-C-D-E Approach Identify and address life-threatening issues associated with the following:
A – Airway B – Breathing C – Circulation D – Disability E – Exposure.
Complete examination Head-to-toe evaluation of the casualty.
Look, listen, feel and ask to determine or detect further injury.
Treatment, care Provide appropriate treatment, support, care, and comfort.and monitoring Re-evaluate the casualty constantly for changes in condition.
Handover and debriefing Hand over casualty to the next level of care when necessary.
Take part in a debriefing session to evaluate, reflect, relax and learn.
Management of security issues related specifically to armed conflict (in a
confined space, in a room full of smoke, during protests or conflict, after an
explosion, during an attack, under fire, etc.) is a component of all training in trauma first aid offered by the ICRC.

FIRST-AID TRAINING PROGRAMME: AN OVERVIEW 25
First-aidtrainingbytheICRCwillalsoinvolvetraininginmanagingcertainkindsofcontext-specificcases.However,thiswillgenerallyinvolvesomeofthefollowingsituations:
Managing a situation where a person is:
• unresponsive(topicsmayincludemanagementofheadtrauma,babies/children,absenceofspontaneousbreathing,etc.)
• bleeding(topicsmayincludemanagementoflargebleedingareas,compressivebandaging,deep-woundpacking,dizziness,amputation,tourniquet,post-deliverybleeding,etc.)
• sufferingfromburns(topicsmayincludemanagementofvictims’clothesthatarestillonfire,clothesclingingtoburntareasofskin,burnsondifferentpartsofthebody,burnsofdifferentkinds,etc.)
• sufferingfromafracture(topicsmayincludemanagementofopenfractures,fracturesassociatedwithbleedingorunconsciousness,useofsuchthingsastreebranchesorcardboardforsplinting)
• sufferingfromawound(topicsmayincludemanagementofanimalbites,weapon-relatedinjuries,infectedwounds,shortagesofwound-dressingmaterials,etc.).
Everysession7isstructuredaroundfoursuccessivestages:
• EXPLORATION–Sharingofexpectations,experiencesandideasamongalltheparticipants(includingthefacilitator)throughreal-lifescenariosandstorytelling
• HARMONIZATION–Identificationoftheelementsessentialforprovidingasafe,humaneandeffectiveresponse8
• CONSOLIDATION–Consolidationoflearningexperiencesandconsolidationofclinicaltechniquesthroughavarietyofsituations/scenariosinvariouscontexts
7 Eachsessionofatrainingcourseistitled“Themanagementofanemergencysituationwhereapersonsuffersfrom…”,andnot“Thetechniquetoapplyincaseofinjury…”:theformergivesaclearerdescriptionofthesession’saims.
8 Thisreferstotheintendedresultofanactionbasedonsignsthatarevisibleandcanbeevaluated.Forinstance,withregardtoburns,itmeanscontrollingthepainandavoidinginfection,withoutdoingharmorbeingharmed.Inothercasesthiswillmean:unconsciousness(passageoftheair),bleeding(visibleblood),fracture(localizedpain),wound(openedskin).Furthermore,partofthebuildingoftheconfidenceandtheefficiencyistonotdistinguishbetweenthedifferentbleedingsandburndegrees,astheactionisthesameforanybleedingandforanyburn.

26 FIRST-AID TRAINING PROGRAMME: AN OVERVIEW
• CONCLUSION–Conclusioncompletedwithacommitmentforcontinuationandsomeaspectsrelatedtoprevention.
Thedurationofafirst-aidtrainingcourseanditscontentdependon:
• theavailabilityoftheparticipants(poorsecurityconditionsmightlimitparticipation),andtheirneedsandcapacities
• thebestoutcomesfeasible.
Thetrainingshouldnotbeanendinitself.MobileappsorWeb-basedsup-port,orvirtual-realitytools,cannotcoverallneeds,expectationsandreali-ties.Trainingshouldberegardedasonecomponentofacontinuous efforttoreinforcetheconfidenceandskillsnecessarytoprovideaneffectiveresponse,andtotakeadvantageofthegainsmade–thatis,theresultsachieved–andthelessonslearned.Various methods, channels and resources must be used, at different times, to raise awareness and empower people and never create dependence on just one training method.
AnysupportprovidedbytheICRCshould:
• respectthelevelofaccess(e.g.withorwithoutIT)9 • reflectwhatgenerallyattractspeopleandholdstheirattentionorinterest,andkeepsthemactive(e.g.game-like,interactivity)
• beinalanguageandformthatthetargetaudiencecangraspeasily • addressthemainaspectsofpreventingandrespondingtoanemergency(notjusttheskillsandmaterialsused).
Someexamplesofeducation/trainingsupportarelistedbelow:
• groupdiscussions,theatre,songs,radiospots,TVshows,drawings,photos • media,publicevent,placeswhererelativesandfriendswaitinginreferralhealth-carefacilities
• firstaidservices/posts(e.g.duringaresponsetoanemergency,aNationalSocietyfirst-aidercanactasanintermediaryorgo-betweenforthecasualtyandbystanders)
• regularmeetings,briefinganddebriefingsessions(coveringoperationalandemotionalaspects),lessons-learntexercises,meetingswithothersinthechainofemergencycare
9 Rememberthatpeoplewithaninternetconnectionlookforinformationmainlyviainternetsearchenginesandsocialmedia.Thatmayleadtosomeconfusionorcauseconfrontations,becausetheirsourcesofinformationmaybecontradictoryorunreliable(evenwhentheyclaimtobescientific).

FIRST-AID TRAINING PROGRAMME: AN OVERVIEW 27
• simulationexercises,updatesandupgrades–basedontheexperiencesgained,andcarriedoutregularly
• dedicatedmobileappsandwebpages • virtual-realitytools.
Management of dead bodiesIftheneedsassessmentfindsthatitisnecessary,managementofdeadbodies10 canbeincludedinbasicandadvancedfirstaid-relatededucationalactivities.First-aidtrainingwillcoverthemainaspects:collectingdeadbodies;protect-ingthebodiesandtheemergency-careresponders;recordingallpertinentinformationobtainablefromthebodies;andtrackingthebodies.Thetrain-ingwillalsocoversuchmattersashealthandsafetymeasures,securitypre-cautions,andrespectingandensuringrespectforthedeadandthebereaved. Thefollowingwillbeemphasized:
• bodiesdonotcreateepidemics;avoid/preventhastydisposal (burial/cremation)ofdeadbodies
• thedeadandthebereavedshouldalwaysbeshowndueregard • knowyourlimitsanddon'tbeafraidofthem:knowwhentorespondandwhentostop
• ambulancesmustnotbeusedtomovehumanremains,astheyarebestemployedtotransportthewoundedandtheacutelysick.
Please refer to the manual recommended in footnote 10 for further details.
3.2 TECHNICAL SUPPORT
TheICRCmustensurethatitisagileandthatitsprogrammesremainrelevant,up-to-dateandwherepossible,evidence-basedandwidelyaccepted.There-fore,akeycomponentoftheICRC’sfirst-aidtrainingprogramme,andakeyfunctionoftheICRC’sfirst-aiddelegatesandfieldofficers,andofthefirst-aidcoordinationteamatheadquarters,istheprovisionoftechnicalguidanceandadvicefortheactorswithwhomwework.Provisionoftechnicalsupportwillbeathreadrunningthroughtheprogramme,buttheremaybespecificareasoffocus,suchas:
10 Adetaileddescriptionoftheproceduresthatmustbefollowed,togetherwithnumerousrecommendations,canbefoundinthisguide:PAHO/WHO,ICRC,IFRC,Management of Dead Bodies after Disasters: A Field Manual for First Responders, Geneva,2016:https://shop.icrc.org/management-of-dead-bodies-after-disasters-a-field-manual-for-first-responders-pdf-en

28 FIRST-AID TRAINING PROGRAMME: AN OVERVIEW
• analysisofthecasualtycarechainandthecontinuumofcare • developmentand/orreviewofcontingencyplans(includingplansfordealingwithmajorincidents/masscasualties)
• trainingandcurriculumdevelopment(revieworprovisionofadvice) • materialsandequipment(revieworprovisionofadvice) • updatesforbestpractices • datacollection,analysisandmapping • adviceformattersrelatedtocommunication • HealthCareinDanger(HCiD)andtheSaferAccessFramework.
Analysis of the casualty care chainToensurethat there isaneffective, functioningandfullyunderstoodcarepathway,theICRCfirst-aidteammaywishtoundertakeananalysisofthecasualtycarechain,thecontinuumofcare,andreferralsystems.Thisanalysiswilllookatthecasualtycarechainfrompointofincidenttodefinitivecare(see2.4)andwillassessthepopulationsaffected,keystakeholders,facilitiesavailableandexistingcapabilities,andanygapsinthecontinuumthatmayneedtobeaddressed.
Contingency planningTogetherwiththewiderhealthteam,otherICRCspecialistsandkeyactors,the ICRCfirst-aid teammayprovidesupportandadvice fordevelopingorreviewingcontingencyplanning.Thismayincludeadviceonemergencypre-paredness,disasterplanning,andmanagementofmajor incidentsormasscasualties.
Training and curriculumTheICRCfirst-aidteammaybeinvolvedindeveloping,reviewingorupdatingfirst-aidtrainingstandards,curriculaandteaching/educationalpracticesusedbyactorsintheirvariouscontexts.Theseupdateswillreflecttheneedsofthepopulationandtheskillsofserviceproviders,andincorporatethelatestwidelyacceptedpracticesandguidelineswhereappropriate.TheICRCfirst-aidteamwillremainconnectedtoawidernetworktoensuretheirawarenessofthelatestdevelopmentsintheirfield.
Materials and equipmentTheICRCfirst-aidteammaybeinvolvedinreviewing,updatingormakingrecommendationsinconnectionwithfirstaidmaterialsandequipment(foroperationsand/ortraining)beingusedbyactorsintheirvariouscontexts,or

FIRST-AID TRAINING PROGRAMME: AN OVERVIEW 29
withregardtoplansforobtainingsuchmaterialsandequipment.Thesup-portand/orrecommendationsprovidedbytheICRC’sfirstaidexpertswillreflectthecontext(resourcesavailable),theskillsofserviceproviders,andtheneedsofthepopulationaffected.Itmayincludeadviceonfuture,sustainableplanning.
Best practices The ICRC’sfirst-aid teamseeks to ensure that everybodywhoneedsfirstaidwillgetit.Torealizethisobjectivewestrivetomakesurethatthefirst-aidtrainingweprovideisuptodateanddeliveredbyqualifiedtrainers.TheICRC’sfirst-aidprogrammealsostrivestoensureadequatefirstaidprovisioninarmedconflictandtheexistenceofcontext-specificequipmentandcom-petentindividualswithinthepopulationaffected.AtICRCheadquarterstheprogrammeintraumafirstaidisevaluatedandmodifiedperiodically,tokeepituptodate:thisincludesperiodicassessmentsoftheICRC’sfirst-aidtrain-ingcourses.TheICRC’sfirst-aidguidelinessetouttheelementsnecessaryforfirst-aidprogrammestobefeasible,effective,andsustainableforeachgivencontext.
Data collection and analysisTosupportthedeliveryofservicesandtoensureefficiencyandpertinence,theICRC’sfirst-aidteammaycollectandanalysedatatomakechangesinprogrammesorsetprioritiesforthem.Itmayusestatisticsandotherdatato:
• providecost-benefitandcost-efficiencyanalyses • ensurethatpeopleaffectedarebeingadequatelyserved(i.e.monitoringandfollow-up)
• understandtrendsinpublichealth • mapstakeholdersandfacilities • understandpopulationsanddemographics • collectresponse-andreferral-relatedinformation • improvethequalityofaparticularservice.
CommunicationTosupporttrainingandservicedelivery,theICRC’sfirst-aidteammaypro-videtechnicalassistanceoradvice,inconjunctionwiththecommunicationsteam,forraisingawarenessofprogrammesandservicesandpromotingthem.Thismayincludeassistanceindevelopingawarenesscampaignsand/orpro-motionalactivities,andmayevenextendtoprovidingadviceforformulatingoperationalcommunicationanddispatchprotocols(andservices).

30 FIRST-AID TRAINING PROGRAMME: AN OVERVIEW
Health Care in Danger (HCiD) and the Safer Access FrameworkTogetherwiththewiderhealthteamandotherICRCspecialists,theICRC’sfirst-aidteamwillensurethatraisingawarenessofHCiD,andreportingonmattersrelatedto it,remainsapriorityandthatpeopleaffectedhavesafeaccesstohealthcareandthesupportprovidedbythefirst-aidprogramme.HCiDstatisticsarereportedaspartofthefirstaid’smonthlysubmissionofdatatothemedicalactivitydatabase.
3.3 SHARING AND REVIEWING EXPERIENCES
RepresentativesoftheICRCfirst-aidteamwillusetheirexpertiseandnet-workofcontactstoshareandreviewexperiencesamongcontextsandprojectsaroundtheworld,withaviewtoreviewingpractices,exchangingideasandofcourse,applyinglessonslearned.
Putsimply,lessonslearnedisatermusedtodescribethegeneralprocessoflearningfromexperiencetomakeimprovementstosomethingorsomeone.Successforalessonslearnedprocesscanbedefinedmoreelaboratelylikethis:anincreaseincapacitiesorperformance–confirmedwhennecessary–asaresultoftheimplementationofoneormoreremedialactionsforaclearlyidentifieddeficiency.
Foranorganization,theideaisthat,throughaformalapproachtolearning–lessonslearned–individualsandtheorganizationcanreducetheriskofrepeatingmistakesandimprovefutureprocesses.InthefirstaidandPHECcontextthismeansreducingoperationalerrors,makingcaremoreeffective,increasingcostefficiency,andfocusingonimprovingpatientoutcomes.
Lessonslearnedmeansmorethanjustlearningfromexperience.Thepurposeofalessonslearnedprocessistolearnefficientlyfromexperienceandprovidejustificationforchangingtheexistingwayofdoingthings,inordertoimprovefirstaidprovision.Thisrequiresthatthelessonsbemeaningfulandbroughttotheattentionofthedecisionmakersconcerned.
• Everyonewithinthetargetgroupneedstobeinvolvedforalessonslearnedprocesstobesuccessful.
• Alessoncannotbesaidtohavebeenlearntuntilsomethingchangesinthewayweoperate;andtheoneswhoneedtochangearetheonesimplicatedinanissue:thestakeholders.

FIRST-AID TRAINING PROGRAMME: AN OVERVIEW 31
• Operationalvolunteers/staff(first-aidersandfirstresponders)mustbetheoneswholearn.
• First-aidersandfirstrespondersareusuallythefirst,andoftentheonlyoperationalpersonnellikelytobeawareofthelessonstobelearnt,becausetheyaretheonesmostcloselyinvolvedwiththeissueinquestion.
• Unlessthesepotentiallessonsaresubmittedviaaclearlydefinedlessonslearnedprocess,itisunlikelythatanymanagerialoroperationalstaffwillbeabletodiscovertheirexistenceinordertoevenbeginthelearningprocess.
• Allstakeholdersmustsharethelessonstheyhaveidentified.
Everyoneinanorganizationhasadutytolearnlessons,sotospeak,butales-sonslearnedworkinggroupisvitallyimportantroletoplayinensuringthateverybodyunderstandshowvaluablethelessonslearnedprocessis.TolearnmoreaboutthetechnicalaspectsoftheICRC’srecommendedlessonslearnedexercise,contactanfirst-aiddelegateorthefirst-aidcoordinationteamatICRCheadquarters.
3.4 PROVISION OF MATERIALS, EQUIPMENT AND FUNDS
TheICRCmayneedtoprovidematerialorfinancialsupporttoensureeffectivedeliveryoffirstaid.Donationsmaybeprovidedtosupporttrainingcoursesorsessions,respondersandresponseteams,andevencertainpromotionalactiv-ities.Provisionofsupplieswillbebased on need,andwilltakeintoaccountrequisite skills, sustainability and availability.Adetailedlistofallthesup-plyoptionswillbeavailablefromthefirst-aiddelegateconcerned.Thechartbelowprovidesanumberofexamples.

32 FIRST-AID TRAINING PROGRAMME: AN OVERVIEW
Activity Material support Financial or other support
Training and - First aid kits (equipped with - Per diem allowances
response basic first aid materials) - Meals or refreshments
- Basic medicines - Travel costs
- Stretchers - Funds for hiring venues
- Mannequins - External training and certification
- Moulage items - MHPSS
- Uniforms - Exposure missions and internship opportunities
Operations - Vehicles - Fuel costs
- Communication equipment - Mechanical, engineering and IT
and infrastructure support
- Cleaning and decontamination - Fleet advice
supplies - External training and certification
- Safety equipment - Exposure missions and intern
opportunities
Administration - IT equipment - Budgetary support
- Office supplies - Printing (certificates)
Promotion - Booklets and flyers - Advertising
- Emblems and decals

FIRST-AID TRAINING PROGRAMME: AN OVERVIEW 33
4. THE ICRC FIRST-AID PROGRAMME: WITH WHOM WE WORK
11 ForalistofNationalSocietiesandtheircontactdetails,pleasesee: http://www.ifrc.org/en/what-we-do/where-we-work/
4.1 FIRST AID FOR WEAPON BEARERS
Caringforwoundedweaponbearersduringarmedconflictandothersituationsofviolenceis a foundational element of the ICRC’s identity.ICRCandNationalSocietyfirst-aidersareamongthefewactorswhocanprovideassistanceinsuchcircumstances. Inaccordancewith itsmandate, the ICRCworkswithother organizations– andwith governments,weapon bearers, non-statearmedgroupsandcivilsociety–toprotectandassistvictimsonallsidesofanarmedconflict.IHLobligesallpartiestoconflicttocollectandcareforthesickandthewounded,andtotreatthemhumanely.Woundedweaponsbearerswhoarenolongerdirectlyparticipatinginhostilitiesmustalsobeprotectedandassisted.
Today,thereareNationalSocietiesinmostcountries,11andweaponbearersof different kinds oftenhavewell-developedmedical corps to assist theirwoundedintimesofconflict.Therearemanyfirst-aiders,medicalcorps,anddomesticandinternationallawstrainedordevelopedspecificallytoassistandprotectwoundedweaponbearers;however,theICRCmayneedtoprovidefirstaidandothersupportforwoundedweaponsbearerswhen:
• firstaidorotherservicesforwoundedweaponbearersareinadequateornon-existent,orwhenaccesstotimelycivilianservicesislimitedornon-existentbecauseoftheterrainorowingtopoliticalcircumstancesorsecurityconditions
• theneedsofthewoundedareunmet,andwhentheyareinaccessibletoNationalSocietyfirst-aidersforvariousreasons:theterrain;politicalcircumstances;securityconditions;orscepticismabouttheneutralityandimpartialityoftheNationalSocietyinquestion
• medicalstaff–stretcher-bearers,first-aiders,medics,nurses,doctorsorsurgeonsfromoneormorepartiestoconflict–arefacedwithinjuriesorwoundsthatarenewtothem;shortagesofsupplies;orunexpectedsurgesinthecasualtyrate

34 FIRST-AID TRAINING PROGRAMME: AN OVERVIEW
• first-aidersorothermedicalpersonnelfromoneormorepartiestoconflict,theirmedicalfacilities,orthewoundedintheircareareattacked(seethesectiononHCiDin3.2.)
• suchsupportisrequiredtoimprovethequalityofcare(becauseoftheemploymentofharmfulmethodssuchasprolongedtourniquetuse;incorrecttreatment;littleornotriage;inefficientreferralsystems;littleornoemergencypreparednessand/orplans)and/ortoimprovethequalityofinstructionortraininginfirstaid
• knowledgeofvariousvitalmattersislacking:forinstance,therespectandprotectiondue,underIHL,tomedicalstaff,facilitiesandvehiclesnotinvolvedinhostilities;theroleoftheICRC;andmeasuresthatprovidemoreeffectivephysicalprotectionforfirst-aidersandothermedicalpersonnel,theirpatients,andtheirassets.
Fromamedicalperspective,thesearethemostimportantaspectsofcarepro-visionforweaponbearerswoundedduringhostilities:prompt and adequate trauma first aid and stabilization measures at the point of injury or in the safest place near the battlefield (e.g. first aid posts), and rapid evacuation. Anefficientcasualtycarechainforthewoundedwillofferthesemeasures;they save lives, reduce complications and disability, and facilitate surgery. Withregardtocivilianswoundedduringurbanviolence,timelylife-savingandsta-bilizationmeasures,plusasimpleoralantibioticandpainkiller,aresufficienttotreatmorethan50%ofallthoseadmittedtohospital.12
Anefficientcasualtycarechain13forthewoundedcansavelives,reducecom-plications,preventdisability,and/orfacilitatesurgery.Dependingonthecon-text,weaponbearerscanplayapartthroughoutthecontinuumofcareforwoundedoracutelysickpeople,includingcivilians.Traumafirstaidfocusesmostofthetimeonthebattlefieldandoncollectionpoints;butotherkindsofcare–PHEC,intermediatecare,surgicalcareathospitalsandspecialistcare–mustalsobeconsideredwhentakingdecisionsaboutsupportfortraumafirstaid.ICRCsupportforallthesedifferentkindsofcareisgenerallyman-agedseparatelyfromfirst-aidprogrammes.Itisnecessarythatprovidersofthesevariouskindsofcarealsobetrainedinfirstaid;itisthereforenecessaryforustocoordinatewithourcolleaguesinotherhealthprogrammesandto
12 C.GiannouandM.Baldan,War Surgery: Working with Limited Resources in Armed Conflict and Other Situations of Violence,2nded.,Vol.1,ICRC,Geneva,2019.
13 Thechainofcasualtycareistheroutefollowedbythewoundedfromthepointofinjurytospecializedcare.

FIRST-AID TRAINING PROGRAMME: AN OVERVIEW 35
stayabreastofotherICRCassistanceactivitiesthatwillhaveanimpactonthecasualtycarechainforthewounded.
4.2 FIRST AID FOR COMMUNITIES
Communitiesarethebackboneoffirst-aidresponseandserviceprovisioninalmostallcontexts;theyfacilitateandsupportallstagesofthecontinuumofcareforwoundedandacutelysickpeople(seefigureonp.31).Whenacrisisoremergencypresentsitself,itisthecommunitythatfirstprovidesessentialaid–likestoppingtheflowofbloodfromawoundorofferingmuch-neededcom-fort.TheICRC–aloneorwithpartners–deliversfirst-aidtrainingincom-munitiesthroughouttheworld,toensuretheyareequippedwithlife-savingknowledgeandskills,andtheconfidencetoactwhenneeded.Communities–particularlyinthosecontextswheretheICRCoperates–canplayapivotalroleinreducingmorbidityandmortalityamongwoundedandacutelysickpeople.Communitiesare,bydefinition,groupsofpeoplewholiveinproximitytooneanotherorsharecertaincharacteristics(suchassufferingtheconsequencesofthesameeventorincident).Wehopethatcommunitiesempoweredinfirstaidwillworktowardsacommonobjective:toalleviatepainandsufferingandactastruehumanitarians,duringconflictand/orotheremergencies.Itisalsothecasethatappropriatefirst-aidtraininghelpscommunitiesandorganizationsprepareforcrisesanddealwiththemmoreeffectively.
Members of the communitiesinwhichtheICRCoperates–relatives,comrades-in-arms,ordinarybystanders,and/orNationalSocietyvolunteers–areusuallythefirstpersonsatthesceneofanemergencyandaresubsequentlythefirst to be able to provide immediate assistancetothewoundedortheacutelysick.
Communityempowermentinfirstaidhelpssavelivesandalleviatesuffering;butitcanalsobroadenawarenessandacceptanceoftheredcross/redcres-cent/redcrystalemblemandhealth-carepersonnelingeneral.14Inaddition,thesustainabilityofactivitiesrelatedtodisasterpreparedness,andtheresil-ienceofcommunitiesduringemergencies,canbestrengthenedthroughwelldesigned,andproperlytargetedandimplemented,firstaidaction(educationalandoperational).Adetailedknowledgeofallthoseinvolvedinaresponse–includingwoundedandacutelysickpeople–iscrucialforensuringthattheICRC’sfirstaidsupportreachesthosepeopleandgroupswhoneeditmost.
14 InlinewiththeHCiDinitiative:www.healthcareindanger.org

36 FIRST-AID TRAINING PROGRAMME: AN OVERVIEW
ICRC vs IFRC/National Societies in Community First Aid Action
1 TheIFRCanditsNationalSocietypartnersprovidetrainingincom-munity-basedhealthandfirstaid(CBHFA).
2 TheICRCworksprimarilyintrauma-relatedfirstaidanddoesnotincludecurativehealthcareinitsfirst-aidtraining.
3 Theirworkingmethods(or‘operatingprocedures’,ifyoupreferthatphrase)arenotthesame.
4.3 FIRST AID FOR AMBULANCE PERSONNEL
Ambulanceandothertransportservicesfacilitatetheevacuationofsickandwoundedpeople.ParticularlyinthecontextsinwhichtheICRCoperates,thesetransportservicescoverabroadrange,fromlayambulanceservices(e.g.rap-id-taxiservices)tomedicalshipsand/orhelicoptersandplanes.TheICRC’sfirstaidandPHECprogrammesmustincorporatealllayambulanceservicesinordertoensurethebestpossiblecareandoutcomesforthoseaffectedbyarmedconflictorotherviolenceand/orotheremergencies.Asthefirstemer-gency-carerespondersqualifiedtoprovideadvancedfirstaidand/orbasicemergencymedicalcare,ambulancepersonnel–duringarmedconflict–areoftenalsoinvolvedinsettingupfirstaidpostsormedicalposts(thatis,any-thingfromapatient-collectionpointtoamedicalpostwheresomeformofadvancedcareisavailable).Detailedknowledgeoftheenvironmentandofthepersonnelthatwillbeinvolvedinevacuatingsickandwoundedpeople,andestablishingmedicalposts,isanecessity:withoutsuchknowledgeitwillbedifficult,ifnotimpossible,toensurethatinformalfacilitiesprovidingfirstaidareidentifiedandgiventhenecessaryICRCsupportforfirstaid.
The level of training received by these emergency-care responders– fromhighlyskilledservicesandprofessionallyrecognizedstafftodriver-onlysys-temswithnodirectpatientcareduringreferral–varieswidelyfromonecountrytoanother.Effectivepre-hospitalcareisunavailableinmanysettings:oneofthemainreasonsforthisistheinabilityofresponderstoprovidefirstaidforcasualties.15Theevidenceshowsthatemergency-carerespondersandambu-lancepersonnelcanbenefitfromcontextualizedandappropriatefirst-aidtrain-
15 ICRC,First Aid in Armed Conflicts and Other Situations of Violence,ICRC,Geneva,2006.

FIRST-AID TRAINING PROGRAMME: AN OVERVIEW 37
ing,particularlyinsettingswherethereisnoformallystructuredandregulatedpre-hospitaleducation.16Suchfirst-aidtrainingcouldalso leadto improvedoutcomesforpatientsinthecriticalphasebetweeninjuryanddefinitivecare.
TheICRC’sfirst-aidprogramme’sactivitiestobenefitambulancerespondersandservicesmayincludeotherthingsbesidesfirst-aidtraining,suchas:
• providingsafeaccessandaddressingbarrierstocareandreferral(forthewounded/sickandthecareprovider)
• ensuringtheavailabilityofthenecessaryresourcesofgoodquality • monitoringandevaluatingtransportandreferralsystems • contingencyplanningand/oremergencypreparedness.
Ambulance and transport services should not have to restrict themselvestoevacuatingsickandwoundedpeople;theyshouldalsobemotivatedandempoweredtoprovideemergency medical care.
4.4 FIRST AID FOR NATIONAL SOCIETY VOLUNTEERS AND STAFF
Together, theNationalSocieties, the IFRC, and the ICRCmakeavailable auniquepool offirst-aiders,first responders andhealthprofessionalswhoworkallovertheworldinacommunity-basednetwork.17First-aidersandfirstrespondersareactivenotonlyduringdisastersandarmedconflictorotherviolence;theyalsohavedailytasks.Appropriatefirst-aidtraininganddailyactivitiesprovide thebasis foraneffectiveandwell-preparedresponsebyNationalSocietiesintheeventofdisastersorarmedconflict/otherviolence.Involvingthepeopleconcernedindesigningandimplementingprogrammesensures:
• responsivenesstoneeds • preparednessandthecapacitytopreventormanageemergencies(injuries,diseases)
• respectforlocalsocio-culturalpracticesandreligiousbeliefs.
Thepresenceontheground,andthedailywork,offirst-aidersandfirstrespond-ers–orofemergency-carerespondersingeneral–makesastatementaboutthehumanitarianspirit linkingpeoplesandcommunities.Bydemonstrating
16 S.Suryanto,V.Plummer,VandM.Boyle,“EMSsystemsinlower-middleincomecountries:Aliteraturereview”,Prehospital and Disaster Medicine,32(1).
17 JenniferL.Pigogaetal.,(2017).“AdaptingtheemergencyfirstaidrespondercourseforZambiathroughcurriculummappingandblueprinting”,BMJ Open,7(12).

38 FIRST-AID TRAINING PROGRAMME: AN OVERVIEW
that“peoplehelpotherpeople”allemergency-careresponderssetanexample.TheICRChasanobligation–inspiredbyhumanitarianprinciplesandvalues–toensurethatallNationalSocietieshavethesupporttheyneedtoprovidetimely,impartialandeffectivefirstaidduringconflictandotheremergencies.
Duringarmedconflictorotheremergencies,emergency medical care can often be inaccessible or unavailabletocasualties.Therearevariousreasonsforthis,suchas:insecurity;threatstohealth-carepersonnel;damagetothehealth-caresystem;andthedestructionofambulances.Anyimmediateassis-tanceortransport/evacuationofcasualtiesisprovidedbypeoplepresentatthescene:relatives,comrades-in-arms,ordinarybystandersand/orlocalhealth-carepersonnel.Thisassistance,thoughessential,isoftenofpoorquality:thepersonsconcernedlacktheknowledgeortheabilitytorespondtoemergen-ciesofthiskind;andthesystemsorstructuresinplaceareunpreparedandunder-resourcedandunabletoprovidetheservicesnecessary.
Furthermore, it isoftenthecasethatemergency services (public,private,NationalSocieties,NGOs)do not have the capacities necessary torespondin contexts characterized by a lack of securitymanagement; unprepared-nessinhandlingemergencies;inabilitytoworkwithlimitedresourcesandin isolation;shortageofsupplies;andsoon.National Society first-aiders/first respondersareoftenthefirstorganizedrespondersonthescene,anddepend-ingon the context, sometimes, for awhile, theonlyones there.Very fewNational Societies are adequately prepared or equippedtocopewitharmedconflict/otherviolence,andotheremergencies:theyarealmostalwaysunabletoensureaccessfortheirfirst-aidteamsortoguaranteetheireffectiveness.TheNationalSocietiesthatrecentlybecameinvolvedfrequentlyfind it diffi-cult to incorporate lessons learnedintheirstrategies,contingencyplansandroutineworkinconnectionwithemergencypreparednessandresponse.
Inaddition, thesystemfor collecting, transportingandstoringdeadbod-iesoftenbreaksdownorisdisrupted.Therefore,the task of managing dead bodiesisoftenlefttothosepresentatthescene:ambulancepersonnelorotherfirstrespondersand,almosteverywhere,NationalSocietyfirstresponders/first-aiders;thesepeoplecarryoutthistaskeitherbecausetheyarerequiredbylawtodosoorbecausetheirhelphasbeensolicitedforthatoccasion.Inthis connection, local sourcesof reference, awareness and skills areofteninadequateornon-existent;thisisalsotrueofthematerialsandequipmentrequiredformanagingdeadbodies.

FIRST-AID TRAINING PROGRAMME: AN OVERVIEW 39
The ICRC'sfirst-aidprogrammecan incorporate allNational Society staffandvolunteersinoperationalcontexts,toensurethebestpossiblecareandoutcomesforthoseaffectedbyemergencies.NationalSocietiescanbecom-plicatedorganizationswithvariousaffiliations.ClosecollaborationwiththeICRC’sCooperationDivisionandwiththered-linemanagementatdelegationsisrequiredtoensurethattheICRC’sfirst-aidprogrammesandactivitiesarerelevantandwellreceived.Dependingonthecontext,aNationalSocietycanbeinvolvedinand/orresponsiblefortheentirecontinuumofcareforawoundedoracutelysickperson.Asperthecontinuumofcare,NationalSocietiescanbeinvolvedinorresponsiblefor:
• firstresponseatthesceneofanemergency(NationalSocietyvolunteers) • immediatecare(NationalSocietyhealthpostsandhealthfacilities) • transportation(NationalSocietyambulanceservices) • preparedness(NationalSocietyprogrammesineducationandpreventionforcommunitiesandothers).
4.5 FIRST AID FOR HEALTH PROFESSIONALS
Duringconflictandotheremergencieshealthprofessionalsmaybethefirstqualifiedpeopleonthescene.Itisthereforeessentialthattheyhaveabasicknowledge of the life-savingmeasures, outside the clinical context, thatarecurrently inuse.Appropriatefirstaidtraininganddailyexercisespre-parehealthprofessionalstorespondeffectivelyintheeventofdisastersorarmedconflict/otherviolence.Involvingthehealthprofessionalsconcernedindesigningandimplementingprogrammesensures:
• responsivenesstoneeds • preparednessandthecapacitytopreventormanageemergencies(injuries,diseases)
• respectforlocalsocio-culturalpracticesandreligiousbeliefs.
Dependingontheir training,experience,capacitiesandmotivation,skilledhealth professionals can, in principle, be first-aiders or emergency-careresponders.Thepresenceontheground,andthedailywork,offirst-aidersandemergency-carerespondersmakesastatementaboutthehumanitarianspiritlinkingpeoplesandcommunities.Bydemonstratingthat“peoplehelpotherpeople”,first-aidersandemergency-careresponderssetanexample.Inafunctioninghealthsystem,healthprofessionalsprovidehealth-careservicesinordinarytimes;thisgivesthemauniquepositionoftrustandrespectincommunities.Duringemergencies,healthprofessionals–communityhealth

40 FIRST-AID TRAINING PROGRAMME: AN OVERVIEW
workers,traditionalhealersandotherhealth-carepersonnel(dispensaries,clinics/hospitals)-willbeexpectedtoprovidebasicbuteffectivecaretothewoundedandacutelysick,andtheyshouldbeabletodoso.
Duringarmedconflictorotheremergencies,emergency medical care can often be inaccessible or unavailabletocasualties.Therearevariousreasonsforthis,suchas:insecurity;threatstohealth-carepersonnel;damagetothehealth-caresystem;andthedestructionofambulances.Anyimmediateassis-tanceortransport/evacuationofcasualtiesisprovidedbypeoplepresentatthescene:relatives,comrades-in-arms,ordinarybystandersand/orlocalhealth-carepersonnel.Thisassistance,thoughessential,isoftenofpoorquality:thepersonsconcernedlacktheknowledgeortheabilitytorespondtoemergen-ciesofthiskind;andthesystemsorstructuresinplaceareunpreparedandunder-resourcedandunabletoprovidetheservicesnecessary.
Furthermore, it isoftenthecasethatemergency services (public,private,NationalSocieties,NGOs)do not have the capacities necessarytorespondincontextscharacterizedbyalackofsecuritymanagement;unpreparednessinhandlingemergencies;inabilitytoworkwithlimitedresourcesandinisola-tion;shortageofsupplies;andsoon.Healthprofessionalsareoftenthefirstprofessionalrespondersonthescene(infirst-aidpost,advancedmedicalpost,casualtyclearingstation,etc.);anddependingonthecontext,theyarealsooften,forawhile,theonlyoneswithknowledgeofemergencymedicineonthescene.Healthprofessionalswhoarenothospitalstaffarefrequentlyunpre-paredorunequippedtocopewitharmedconflict/otherviolence,andotheremergencies:theyarealmostalwaysunabletoensureaccesstopre-hospitalemergencymedicalcareortoguaranteeitseffectiveness.Theythereforeneedtohaveclearlydefinedfirstaidstrategiesandcontingencyplanswithregardto theircapacities inemergencypreparednessandresponse,especially forout-of-hospitaloroff-dutysituations.
TheICRC’sfirstaidandPHECprogrammescanincorporatehealthprofes-sionalsatalllevels,toensurethebestpossiblecareandoutcomesforthoseaffectedbyemergenciesinout-of-hospitalsettingsofanykind.Dependingonthecontext,healthprofessionalscanbeinvolvedinand/orresponsiblefortheentirecontinuumofcareforawoundedoracutelysickperson.Asperthecontinuumofcare,NationalSocietiescanbeinvolvedinorresponsiblefor:

FIRST-AID TRAINING PROGRAMME: AN OVERVIEW 41
• firstresponseatthesceneofanemergency(allhealth-carepersonnel,includingtraditionalhealers)
• immediatecare(healthprofessionals(doctors/nurses/EMTs/paramedics,etc.)
• transportation(EMSservices) • furthercare(includesabroadrangeofproviders,fromtraditionalhealerstohospitalstaff;further-careoptionsarecontext-dependent)
• preparedness(healthprofessionals(clinicstaff,dispensaries,doctors,nurses,traditionalhealers,etc.;programmesineducationandpreventionforcommunitiesandothers).

42 FIRST-AID TRAINING PROGRAMME: AN OVERVIEW
Continuum of care for the wounded and the acutely sick.
BEFORETo be empowered
DURINGTo find solutions at the time and at the place of the emergency (creative thinking + limits)
• Motivated/ Confident
• Confident
• Safe
• Effective and coordinated
• Humane
AFTERTo see results
To learn from experience
COMMUNITY
WOUNDED
(Wea
pon bearer or civilian)
BASIC CARE
SENDBACK
TO
TRANSPORT/EVACUATIONAMBU
LANC
E SE
RVIC
ESED
UCAT
ION/
PREV
ENTI
ON
CONNECTION TO FURTHER CARE
DEFINITIVE CARE(if required)
BEST POSSIBLE CARE & PATIENT
OUTCOMES
FIRST-AID TRAINING PROGRAMME: AN OVERVIEW 43
5. THE ICRC FIRST-AID PROGRAMME: HOW WE IMPLEMENT OUR PROGRAMMES
TheICRC’sfirst-aidprogrammesandprojectsaredevelopedaccordingtotheneedsofthepeopleaffectedandfollowtheRBMprocess.Thisensuresthateveryprogrammeisnecessary;properlyplanned;evaluatedforeffectiveness;andcontinuouslyimproved.TheICRC’sfirst-aidteamworkswithmanydif-ferentgroupsofpeopleaffectedandactorstoensurethatgapsincare,equip-ment,knowledgeorskillsareadequatelyaddressedinamannerthatfitsthecontext,andiseffectiveandaccountable.
5.1 RESULTS-BASED MANAGEMENT
TheICRC’sRBMcycleisdividedintofourstages:
• assessandanalyse • formulateandplan • implementandmonitor • review/evaluateandlearn.
Thiscycleimpliesthenecessityofhavingaclearunderstandingofthecon-textinwhichwework(assessandanalyse);definingtheobjectivesthatwilladdresstheneedsidentifiedthroughourassessment(formulateandplan);carryingouttheactionsrequiredtoachieveourobjectivesandkeepingtrackofprogress(implementandmonitor);andassessingifourobjectivesarelikelytobeachieved/havebeenachieved,whilealsonotingthereasonsforoursuccessorfailure(review/evaluateandlearn).FirstaidprogrammingshouldfollowtheRBMapproach,inordertostrengthenitsperformanceanditsabilitytodemonstratetheeffectsofitsactivities.

44 FIRST-AID TRAINING PROGRAMME: AN OVERVIEW
EVAL
UATE
AND
LEA
RN
IMPLEMENT AND MONITOR
FORMULATE AND PLAN
ASSESS AND ANALYSE
Module 1: Assessing Economic Security
Module 2: EcoSec Planning, Monitoring and Evaluation
Module 3: The EcoSec Response – Implementing the Project
I CRC M
I S S I O N , M A N D AT E , A N D P R I NC IPLES
I CR C I N S T I T U T I O N A L M A N A G E M E N T P R I O
R I TI E
S
AllICRCassistanceactivitiesmustfollowtheRBMcycleinordertoensureprojectaccountabilityandprogress.FurtherinformationonthespecificsoftheRBMcyclecanbefoundontheICRCHealth Wiki.
5.2 NEEDS ASSESSMENTS
Aneeds assessment isthefirstofthefourphasesofanRBMprocess.Itiscarriedouttogainanunderstandingofthesituationandtheproblems–theircausesandconsequences–andtodeterminewhetherthereisaneedforICRCactionandifso,whatformthatactionshouldtake.Anassessmentoftheneedforfirstaidandrelatedsupportprovides:
• abaselineforinformedICRCdecision-making • abaselineformonitoringandevaluatingprogrammeoutcomes • anunderstandingofstakeholders’rolesandinterests • opendialoguewithactorsinvolvedinhealth-relatedmatterstofacilitateongoingassessmentsormonitoringofevolvingneeds,andanopportunitytoestablishanetworkofhealth-relatedcontacts
• informationonthegeneralsituationandhealthburdenofthewoundedandthesick
• informationonthecasualtycarechain,includingreferralsystemsandcontingencyplans.

FIRST-AID TRAINING PROGRAMME: AN OVERVIEW 45
Afirstaidneedsassessmentmayhaveaspecificobjectiveoritmaybepartofageneralhealthassessment.Inbothcases,anassessmentexaminesallstagesofthecontinuumofcareforthewoundedandtheacutelysick.Itshould:
• estimatetheneeds(incidentsrelatedtothewoundedandthesick) • identifyresourcesavailable:existingfirstaidactivities,referralpossibilitiesandcapacityofkeyhealthfacilities
• determineifminimumservicesareavailable • determinetheunmetneedsandprioritiesofthewoundedandthesick • analysewhethertheICRCshouldassistthewoundedandthesick,andhowitshoulddoso.
In areas to which the ICRC has only limited access,itmaynotbepossibletodoa‘bird’s-eye-view’assessmentinthefield.Afirstaidassessmentmaythenhavetobebasedoninterviewswithkeystakeholders,suchas;villagechiefs;healthstaff;woundedpeople;armedandotheroppositiongroups;stateforces(themilitary,securityforces,civil-defencepersonnel,thepolice,etc.);andothermembersofthepartiestoconflict.
Informationcanalsobeobtainedfromreferralhospitalsandotherstakeholdersresponsibleforthoseworkingintheareaaffected.Regularconfidentialdialogue–betweentheICRCandhealthpersonneltendingtowoundedandacutelysickpeople–isessentialwhentheICRChaslittleornoaccess.Suchdialoguehelpstodevelopafullerandmorereliablepictureofexistingemergencymedicalsys-temsandsupportneeds.Suchassessment-relatedconfidentialdialoguecanbeundertakenduringICRCassistanceactivitiessuchasfirst-aidtrainingforhealthprofessionals;provisionofemergencymedicalsupplies;ormonitoring.
Data fromother sources–media reports; reportspreparedbyother, reliableorganizations;andphotographsoftheareatakenbyICRCcontacts–canbecom-binedwiththedatagatheredbytheICRCduringitsinterviews.Thisallowstri-angulationofinformationandincreasesconfidenceinthereliabilityofthedata.
TheICRCcarriesoutthreemaintypesofassessment:rapid,in-depthandcon-tinuous.Itschoiceofassessmentwilldependoncertainfactors:thecontextanditsaccessibility;theICRC’sobjectives;theavailabilityofinformationfrompreviousassessments;andthetimeandresourcesavailable.
• Arapidassessmentisalwaysthestartingpointforestablishingorre-establishingICRCassistanceforfirstaidservices;additionalinformationcanbeaddedlatertocompleteanin-depthassessment.

46 FIRST-AID TRAINING PROGRAMME: AN OVERVIEW
• Anin-depthassessmentenablesmorecomprehensivecollectionofinformationtosupportlonger-termplanningofICRCsupportandtoassesscriticalareasidentifiedduringarapidassessment.
• Acontinuousassessmentisnecessarybecauseconflictsituationsandemergenciesarecomplexandconstantlychanging.Theseassessmentshelptoidentifyadjustmentstofirst-aidprogrammesandactivitiesthatmaybenecessary.
AnICRCneedsassessmentshouldinvolvefourstages,asshowninthetablebelow.Confirmthelevelofsupportthedelegationcanofferbeforeplanninganassessment.Themoredetailedtheinformationgatheredthroughathoroughassessment,theeasieritwillbetodesign,planandimplementarelevantandappropriatefirst-aidprogramme.
Conducting an ICRC assessment
Steps What has to be done
1. Purpose - Define the objectives of the assessment - Determine the type of assessment: rapid, in-depth or continuous - Select the team: personnel from ICRC departments and others
2. Preparation - Perform/review/update stakeholder mapping and analysis– Before visit - Review existing information/data: ICRC and other sources - Decide areas and structures to visit, and key stakeholders to meet - Determine the type of data needed and where/ from whom to get it - Organize data collection - Make logistical and other arrangements for the assessment
3. Information - Document initial observations during visits to the area affected collection - Meet with stakeholders as arranged or create opportunities for – During visit meetings, review all relevant information that may be available at health facilities or other sites of medical care, within communities and among weapon bearers - Visit specific site as planned, including surgical wards, triage areas, morgues, cemeteries and other pertinent areas - Identify and assess existing health surveillance systems - Establish network of key health- and transportation-related contacts
4. Analysis - Determine urgent needs during visit, including any life-saving – During and assistance that may be required, and provide immediate support after visit (first aid supplies or transportation) - Map services and stakeholder networks - Determine needs and potential ICRC response - Develop recommendations, reporting

FIRST-AID TRAINING PROGRAMME: AN OVERVIEW 47
ThepurposeofconductinganassessmentforanICRCfirst-aidprogrammemaybeto:
• learnmoreaboutthecontext • determinetheneedforICRCsupport • establishdialoguewithcontacts • developassistanceplanforfirst-aidprogrammes • identifyorexplorepossibilitiesfor“vector”activities,whicharesetupmainlytoengagewithstakeholders.
Terms of reference (ToR)aredevelopedforeachassessmentandwilldescribeindetailwhytheassessmentisbeingdone,andwhere,howandbywhom.TheToRshouldinclude:
• backgroundinformationonthesituation • justificationforICRCinvolvement • mainpurposeandobjectivesoftheassessment • compositionoftheteamandrolesandresponsibilities.
Alldelegatesshouldprepare foraneedsassessmentby reviewingexistinginformationandconductingastakeholder-mappingexercise.
Stakeholder mapping and analysis:ICRCmanagementmayhavealreadycon-ductedstakeholdermappingandanalysis,forhelpinunderstandingtherolesandpowerof thevariousactors intheareaaffected. It isessential tomapstakeholdersbeforeanassessment;ICRCmanagement’smappingwillincludeweaponbearers,actorsinvolvedinhealth-relatedmatters,andothersofper-tinenceinthearea.Stakeholdermappingwillbeupdatedaftertheassessment,andupdatedalsoinstepwithchangesinthecontext.Itwillassistinplanningtheassessment;decidingonlocations,andonkeystakeholderstomeet;deter-miningsecurityrisksandaccessibilityofthearea.
Reviewing existing information:Theinformationavailablemustbereviewedbeforegoingtotheareaaffected.Thisishelpfulforunderstandingthesitu-ation,identifyingstakeholders,anddeterminingwhatinformationhastobecollected.Existingsourcesofinformationincludeliterature,websites,data-bases,reportsandmapsrelatingtotheareaaffected.
Sourcesofvaluableandinformationmayinclude:
• ICRCmanagementteamandICRCdepartments • Movementpartners:NationalSocieties,IFRC
48 FIRST-AID TRAINING PROGRAMME: AN OVERVIEW
• UNbodies,includingOCHA,UNDSSandWHO • Donors,embassies • Defenceandhealthministries,governmentdepartments(i.e.statisticaloffices)
• Weaponbearers(thewebsitesofsomearmedgroupshavecasualtyreports) • NGOs,privateorganizations(i.e.ambulanceservices)andothersinvolvedinprovidingfirstaidandhealth-relatedassistanceinthearea.
Itmightbehelpfultomeetwithseniorrepresentativesoftheorganizationsmentionedabove–andseniorgovernmentofficials–beforevisitingthefield.Thismayfacilitateaccesstotheareaandmayalsohelpinsettingupmeet-ingswithkeystakeholdersto,forinstance,identifykeysitessuchashealthfacilitiesundertheirmanagement.Allthismayyieldadditionalinformation,suchas:
• assistancepolicies,activityreports,detailedmapsandstatistics • contactdetailsforkeyfiguresinthearea,suchaslocalauthorities,directorsofhealthservices,hospitaldirectors,projectmanagers
• overviewofthecontext:demographics,infrastructureandbaselinehealthdata
• detailsaboutthecurrentsituation,securityconditions,needs,currentresponseandgaps.
Planningandcoordination–inadvance,andwithallstakeholders–arenec-essarytoreduceriskandpreventproblemsduringtheassessment.
Decide what areas – and health and other facilities – to visit, and which key stakeholders to meet:Securityconditionsandaccessibilitywilldeterminewhatareascanbevisitedforassessment.
Theplacestovisitmayinclude:
• areasreportedtobeaffectedbyarmedconflictorotherviolence • areaswhere,accordingtostakeholders,unmetneedsamongthewoundedarehigh
• healthfacilitiesintheareaaffected,particularlyfacilitiestreatingwoundedpeople
• officesofauthorities,militarycommandersandleadersofarmedgroups • officesofthosemanagingorprovidingassistancetowoundedpeople • siteswherethedeadarelikelytobefound(i.e.graveyards,morgues).

FIRST-AID TRAINING PROGRAMME: AN OVERVIEW 49
During the stakeholdermapping and analysis, and the review of existinginformation,itwillbecomeevidentwhichkeystakeholdersshouldbemet.Itisadvisabletomeetauthoritiesfirst,togetherwithICRCmanagement,asamarkofrespectandtodiscusssecurityandaccessissues.ICRCmanagementcanalsorequesttheleadersofarmedgroupstointroducethemtothepersonorpersonsinchargeofhealth-relatedmatters,sothatICRChealthteamscanmeetwiththemtodiscussthecareavailabletotheirwoundedpersonnel.
Determine the type of data required and where/from whom to get it:Ifnopreviousassessmentoftheareahasbeendone,itwillbenecessarytocollectinformationonthegeneralsituationaswellasonhealth.Thisinformationisalsonecessaryforlearningabouttheservicesintheareaaffectedandneedsamongthepeopleaffected.However,useofdatacollectedmustalwaysbejus-tifiable,andsometimesrestricted:thisisessential.Itisalsoworthnotingthatinformationonthenumberandtypesofcasualtiesmaybeofgreatvaluetomil-itaryintelligence;sobeawareofthesensitivityofthedatayouarecollecting.
Data for assessing first aid and related purposes
General and health data
• Security, general context and geographical data
• Demographic data (population, gender, displaced people, vulnerable groups, etc.)
• Health situation:- Health ministry policies and procedures (list of essential drugs, treatment protocols)- Health-related actors and health facilities in area (functional/non-functional, resources,
ambulances, non-governmental)- Access to health services (considerations include topography, security conditions, cost) - Morbidity and mortality patterns, epidemics - Mine-related and other risks - Health concerns and priorities of beneficiaries, and health staff and others- Pre-hospital set-up (lay and professional response)
• Protection of health care: Incidents affecting provision of care - Incidents affecting health workers, and facilities and vehicles used solely for medical
purposes- Incidents affecting patients and their relatives - Management of incidents
• Access for ICRC to area- Distance from ICRC delegation/office, state of roads; types of vehicle needed- Security and other concerns - Communication: Coverage for mobile phones, satellite phone, high-frequency radio

50 FIRST-AID TRAINING PROGRAMME: AN OVERVIEW
First-aid data
• Medical systems and casualty care chain - Who administers first aid? National Society volunteers, military medical services,
health ministry, untrained weapon bearers, NGOs, private ambulance services - Where do the wounded go? Types and location of health facilities, and services
provided at each stage of the chain (first aid, emergency medical stabilization, wound excision, surgical care)
- What capacities are available – at all levels – to treat wounded people? Staff skills and resources (staff, training, equipment, medical supplies)
- People who depend on services- Transport, evacuation and referral procedures and systems- Contingency plans, as well as number and types of incidents and response- How effective or efficient is the casualty care chain, including evacuation?
• Caseload and epidemiology of the wounded- Number of wounded people, number of dead people, main causes of death- Types (burns, gunshot), sites (head, limb) and causes of wounds (shell, mine) - Origin of wounded people- Age, gender - Who is wounded? Civilians, weapon bearers (police stretcher-bearers, trained soldiers,
members of armed groups)
• Unmet needs of wounded people- Problems faced by wounded people and actors involved in providing care- Incomplete assistance or support provided by other actors - Gaps in assistance and plans for support
• Protection of health care: - Any arrests of wounded weapon bearers (with possible interruption of health care), or
denial of health care to certain wounded people- Delayed referral of wounded people (e.g. delays at checkpoints)- Denial of access to first-aiders seeking to assist wounded people - Lack of respect and protection for first-aiders, stretcher-bearers or other health staff
assisting wounded people
- Awareness: identification used or other preventive measures

FIRST-AID TRAINING PROGRAMME: AN OVERVIEW 51
5.3 RESULTS, REVIEW AND EVALUATION
TheresultsoftheICRC’sfirstaidactivitiesmustbetracked,notonlyafterameetingortrainingcourse,butmainly after the management of emergency situations,as that is the goal of first aid empowerment.Theseoutcomes canbemeasuredatthesceneofanemergency.Theycanalsobemeasuredelsewhere:atthehomeofthewoundedandtheacutelysickpersoninques-tion,iftheywerenotinneedoffurthercare;attheplacetowhichthatpersonwastransportedforfurthercare;and/orduringdebriefingsessionsandles-sons learned exerciseswiththerespondersandotherstakeholdersconcernedor involved intheemergencyresponse(e.g. thegeneralpopulationand itsleaders).
Lessons learned Thelessonslearnedanalysisshouldseekto improve the first aid activities in question – operational or educational – that is, make them stronger, safer and more durable.Accordingly,thedatatobecollected,andtheoverallprocess,shouldbesimpleandeasilyconvertedintomeaningfulandusableinformation.Reactions or responsestothisanalysismustbeprovidedwithoutunduedelay(shortlyaftertheactivityundertakenorthecollectionofdata).Thoseatthereceivingendincludethefollowing:peopledirectlyinvolvedintheactivityordatacollection;peoplerequiredtorespectthecasualties;peo-pleinvolvedinensuringrespectandprovidingsupportforcasualties;andtheemergency-carerespondersandfirst-aidersconcerned.Thepurposeistocon-solidatethemotivationandtheassets,andtohelptotackledoubts,concernsanddeficiencies.Evidenceofsuccessorfailure–andthereasonsforeither–shouldbepresentedanddiscussed.
Themostimportantmatterstoassessinthelessonslearnedprocessare:
• relatedtotheprimarygoal:livessavedandsufferingalleviated,andtheresultsofthecareprovidedalongthecasualtycarechain
• thepossibleeffectsamongthefollowing: – weaponbearersandpeoplelikelytobepresentatthesceneofanemergency:theirresilience,theirinvolvementandparticipationintheresponsetoemergencies,theirtrustinemergency-careresponders,theiracceptanceofthatparticularNationalSociety,etc.
– emergency-careresponders:theirconfidenceandmotivation,theirperformance,theirwell-being,howtheyvaluethesupportoffered,etc.

52 FIRST-AID TRAINING PROGRAMME: AN OVERVIEW
– humanitarianassistance:readieraccesstopeopleinneedandtoreferralfacilities,greaterrespectfortheredcross,redcrescentandredcrystalemblemsandfortheprovisionofhealthcare,etc.
– NationalSocietiesandotherorganizationsreceivingsupport:e.g.improvementinstructure,functioning;coordinationandcollaboration;greateracceptance;broaderaccesstopeopleinneed;expandedemergency-responsecapacities.
Forprogrammesthatareremotelydeliveredandmonitored–currentlythemainoperationalmodelforICRCfirst-aidprogrammesinhigh-conflictareas–qualitative informationfromvarioussources18isanecessity.Dataofthiskind are useful for evaluating the relevance of a programmewhen directsupervision,andconventionalquantitativemonitoringandevaluation,isnotpossible(orreliable).Collectingqualitativedatashouldbepossibleinmostplaces ifdoneaftersecuringthenecessaryconsentor inanon-interroga-tivemannerduringmeetingsortours.Someintervieweesmaybeunwillingtopartwithsuchinformationbecausetheyregarditassensitiveandpotentiallydamaging(e.g.weaponbearersoftenconsidersuchinformationtobevaluablemilitaryintelligence,andlocalhealthauthoritiesmaynotwanttohaveanyattentiondrawntotheirshortcomings).
Asformonitoringandevaluatingfirstaidactivities(operationalandeduca-tional),abaselinemustbeestablishedbeforethedeliveryofsupport,withsimpleandmeaningfulindicators,andduringthefirststageofimplementa-tionoffirstaidsupportifitwasnotdoneduringtheassessmentphase.
18 Triangulationoftestimonies,public-servicesdata,mediareports,interviews,etc.

FIRST-AID TRAINING PROGRAMME: AN OVERVIEW 53
6. FINAL NOTE
Thisdocumentisanoverview only of the first-aid training programme, its components and beneficiaries(populationaffected/woundedorsickpeoplearedirectbeneficiaries;emergency-careresponders/careprovidersareindirect
beneficiaries),andcanserveasabriefguidetoconsultbeforedevelopingandimplementingfirstaidtrainingactivities.Programmesandprojectshavethebestchancetobeeffective,efficientandcollaborativewhentheirdevelopmentisprecededbyadetailedneedsassessmentandwhentheyfollowaresults-basedapproach.
Thefirst-aid coordination teamat ICRCheadquarters canprovide specifictechnicalguidanceforprogrammedevelopment,adviceontheavailabilityofhumanresources(i.e.first-aiddelegates,firstaidspecialists,first-aidfieldofficers,etc.)orcontactsatconcurrentprojectsinsimilarcontextsorloca-tions.Itisimportanttoconsultthefirst-aidteamatICRCheadquartersbeforeimplementinganyof thecomponentsofafirstaidtrainingprogrammeordevelopinganfirstaidprojectofanykind—toensurethatdelegationsandpopulationsaffectedcanbenefitfromalltheexpertiseandexperiencethatisavailable.

4517
/002
11
.202
0
Cove
r ph
oto:
ICR
C
facebook.com/icrc
twitter.com/icrc
instagram.com/icrc
International Committee of the Red Cross19,avenuedelaPaix1202Geneva,SwitzerlandT +41 22 734 60 01shop.icrc.org©ICRC,November2020
The ICRC helps people around the world affected by armed conflict and other violence, doing everything it can to protect their lives and dignity and to relieve their suffering, often with its Red Cross and Red Crescent partners. The organization also seeks to prevent hardship by promoting and strengthening humanitarian law and championing universal humanitarian principles.
People know they can count on the ICRC to carry out a range of life-saving activities in conflict zones and to work closely with the communities there to understand and meet their needs. The organization’s experience and expertise enables it to respond quickly and effectively, without taking sides.