Financial Assistance Form Active English
4
SUMMIT AREA YMCA Y CARES FINANCIAL ASSISTANCE APPLICATION FORM Berkeley Heights YMCA Summit YMCA The Learning Circle YMCA Y Cares Financial Assistance for YMCA Members and Program Participants The Summit Area YMCA is a nonprofit organization committed to providing memberships and programs that enhance the lives of people in the community. Through the Y Cares Financial Assistance Program, we are able to reach out to those in need of financial support so that they may benefit from all the Y has to offer. Frequently Asked Questions About Financial Assistance Who is eligible to receive financial assistance? Individuals and families who show they are in need of financial assistance to help pay for their programs or memberships. Please Note: financial assistance for child care will not be offered unless both parents are employed. The applicant must reside in the Summit Area YMCA service area including: Springfield, Mill- burn, Short Hills, Summit, New Providence, Berkeley Heights, Gillette and Stirling. How are Financial Assistance Awards determined? The Y has a sliding fee scale based on total household income and number of dependents, which assists in determining the support amount. Repeat requests may result in less financial assistance awarded. How long will the financial assistance continue? The need for financial assistance will be reassessed every six months for memberships and programs. Please Note: financial assistance for membership begins the date acceptance letter is received. Lack of timely response to request for updated information will result in termination of financial assistance. It is the applicant’s responsibility to furnish updated finan- cial information at the end of 5 months of member- ship/enrollment for redetermination if continuation of membership/enrollment is requested. Continued on next page......
-
Upload
summit-area-ymca -
Category
Documents
-
view
212 -
download
0
description
Summit Area YMCA financial assistance form in English
Transcript of Financial Assistance Form Active English
SUMMIT AREA YMCAY CARES FINANCIAL ASSISTANCE APPLICATION FORM
Berkeley Heights YMCA
Summit YMCA
The Learning Circle YMCA
Y Cares Financial Assistance for YMCA Members and Program Participants
The Summit Area YMCA is a nonprofit
organization committed to providing
memberships and programs that enhance
the lives of people in the community.
Through the Y Cares Financial Assistance
Program, we are able to reach out to those
in need of financial support so that they may
benefit from all the Y has to offer.
Frequently Asked Questions
About Financial Assistance
Who is eligible to receive financial assistance? Individuals and families who show they are in need of financial assistance to help pay for their programs or memberships. Please Note: financial assistance for child care will not be offered unless both parents are employed. The applicant must reside in the Summit Area YMCA service area including: Springfield, Mill-burn, Short Hills, Summit, New Providence, Berkeley Heights, Gillette and Stirling.
How are Financial Assistance Awards determined? The Y has a sliding fee scale based on total household income and number of dependents, which assists in determining the support amount. Repeat requests may result in less financial assistance awarded.
How long will the financial assistance continue? The need for financial assistance will be reassessed every six months for memberships and programs. Please Note: financial assistance for membership begins the date acceptance letter is received. Lack of timely response to request for updated information will result in termination of financial assistance. It is the applicant’s responsibility to furnish updated finan-cial information at the end of 5 months of member-ship/enrollment for redetermination if continuation of membership/enrollment is requested.
Continued on next page......

Questions Cont’d.....
Is financial assistance available at all four branches of the Summit Area YMCA? Yes. However, because subsidies are branch specific, financial assistance is not transferable and may vary from branch to branch. If you would like information on multi branch assistance please contact each branch individually.
What is the responsibility of the scholarship recipient?The YMCA expects that the recipient will make timely scheduled payments. It is our hope that participants will also volunteer whenever possible. Since our funds are limited and there are others in the community in need of financial assistance, we expect to be notified one month in advance if you no longer need our sup-port or are unable to use the services we provide.
How are scholarships funded?The YMCA raises money through the ongoing work of volunteers and staff. Funds are available as a result of gifts received from individuals, corporations, founda-tions and through the Annual Campaign.
Return completed application form and all applicable documents to your branch YMCA.
Berkeley Heights YMCA 908-464-8373550 Springfield AvenueBerkeley Heights NJ 07922
Summit YMCA 908-273-333067 Maple StreetSummit NJ 07901
The Learning Circle YMCA 908-273-704095 Morris AvenueSummit NJ 07901
www.thesay.org
2
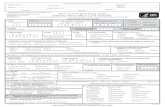
DOCUMENTS REQUIRED FOR APPLICATIONWe require verification of your income and residence before we can offer you Y Cares Financial Assistance. All information will remain confidential.
CHOOSE FROM A OR B BELOW
GROUP AProvide all of the following documents:__ Most Recent Tax Return (1040 and W2).__ Last 4 paycheck stubs or last 4 unemployment stubs.__ Child support documentation. __ List of all income received from public assistance including assistance for housing.
GROUP BOne of the following documents:__ Current lease or property tax bill.__ Notarized letter from Landlord. Letter must state location of residence and monthly rental amount and include land lord’s name, address, and phone number. (Landlord may be contacted).__ Copy of utility bill from previous month (phone, gas, electric).__ Copy of car insurance card (if applicable). -- Copy of cell phone bill from previous month. AND all the following documents:__ Notarized letter from current employer stating hours, wages and including employers contact information. (Employer may be contacted).__ Child support documentation. __ List of all income received from public assistance including assistance for housing.
OR
We reserve the right to verify your information with employers, landlords, agencies and references.

FINANCIAL ASSISTANCE APPLICATION
Choose the branch where you are applying for financial assistance:
_____Berkeley Heights YMCA _____ Summit YMCA _____The Learning Circle YMCA
Please contact the branch directly for assistance.
Applicant Information: Adult (or parent/ legal guardian if applicant is a youth)
Last Name___________________________________________________________First Name _____________________________________ M F DOB______________
Street___________________________________________________________________________________ City______________________ State __________ Zip___________________
Phone (H)________________________________________________ (W)_____________________________________________ (C)________________________________________________
Email ___________________________________________________________________________________________________________________________________________________________
If different - Participant’s (Child’s) Name _________________________________________________________________________________DOB_______________________
I am applying for financial assistance for the following area:
____Membership: Adult Family Teen Youth
____ Program: Please indicate which program _________________________________________________________________
____ Child Care YMCA ____ Child Care TLC YMCA ____ Camp Other:_____________________________________________
List family members noted as dependents for tax purposes:
Spouse (or other adult, if applicable) ________________________________________________________________________________________________
Name________________________________________________________________________________ DOB_______________ Relationship___________________________________
Name_________________________________________________________________________________ DOB_________________ Relationship__________________________________
Name_________________________________________________________________________________ DOB_________________ Relationship__________________________________
Name________________________________________________________________________________ DOB_________________ Relationship__________________________________
3

Employment Information: Please complete ALL information
Applicant (or parent/guardian of youth) Spouse (or other adult, if applicable)
Employer’s Name and Address Employer’s Name and Address
_________________________________________________________________________ ___________________________________________________________________
Address ____________________________________________________________ Address________________________________________________________
________________________________________________________________________ __________________________________________________________________
Phone_______________________________ How long employed_______ Phone__________________________ How long employed_______
Monthly Income Worksheet - Applications will be processed only after all information is submitted and the application is filled out completely. Applicants may be asked to provide documentation to verify their expenses.
Income: Monthly Amounts only
$______________Gross Monthly Income $______________Other Adult’s Gross Monthly Income
$______________Child Support $______________Social Security or Disability
$______________Welfare (submit copy of card) $______________Food Stamps $______________Unemployment $_______________Other ( please explain)
Are there any extraordinary circumstances that should be taken into consideration when reviewing this application?
__________________________________________________________________________________________________________________________________________________________________
__________________________________________________________________________________________________________________________________________________________________
Are you interested in volunteering at the Y? ______ Yes _________Not at this time I (we) certify that all of the information provided to the Summit Area YMCA is true and correct. I (we) certify that all income, including income from self-employment, is reported to the Summit Area YMCA. I (we) understand that child care is provided during my working hours only. I (we) understand that any change in family size, family income or any other circumstances that may change eligibility must be reported to the Summit Area YMCA within 2 weeks.I (we) understand that the Summit Area YMCA may contact the numbers provided by me to verify information and I (we )autho-rize the representatives at those numbers listed to release information for the purpose of verification.
For office use only
Date Received__________________ Date of Award_________________Percent Awarded_______________Annual Income ____________________
Signature ________________________________________________________________________________________________________________ Date ____________________________
Signature ________________________________________________________________________________________________________________ Date ____________________________
4Revised 1.3.12