
Final paper-health 240
44
Running Head: U.S. BREASTFED INFANTS Proportion of Infants Breastfed in the United States Kaitlyn Greiner Health 2400-002 Clemson University
Transcript of Final paper-health 240

Running Head: U.S. BREASTFED INFANTS
Proportion of Infants Breastfed in the United States
Kaitlyn Greiner
Health 2400-002
Clemson University

U.S. BREASTFED INFANTS
HEALTH BEAHVIOR
The behavior of interest is to increase the amount of mothers engaging in breastfeeding in
the US. About one fourth of infants were never breastfed in their lives. Less than half of those
who were breastfed at one time were not breastfed the entire recommended duration (“Maternal”,
2013). In fact, it is recommended by the World Health Organization (WHO) that, “all babies be
exclusively breastfed for six months, then gradually introduced to appropriate family foods after
six months while continuing to breastfeed for two years or beyond” (“Breastfeeding”, 2013). The
proportion of infants that are breastfed exclusively is very small. It is unfortunate that more
infants are not breastfed because breastfeeding has been associated with many important health
benefits for the infant as well as the mother. Reasons that women give for deciding not to
breastfeed are that they didn’t like it, they have to go back to work or school, and that they have
other children to care for (Dimas & Wych, 2013). The number of breastfed infants would
increase if there were an increase in the number of mother’s rooms provided by employers.
Breastfeeding lowers the risks for many preventable diseases that currently inflict the US.
STATISTICS
The target population is the proportion of infants who are ever breastfed in the US. In this
country, 74 percent of infants born in 2006 were ever breastfed in their lives. This was reported
from 2007 to 2009. Graph 1 shows that the percent has increased very slightly over the years.
There are hopes that this number will continue to rise (“Maternal”, 2013). A more recent finding
showed that 77 percent of infants were breastfed at the start of their lives in 2013 (“Breastfeeding
report”, 2013). However, many mothers stop breastfeeding before the end of the recommended
duration period. 43.5 percent of these infants born in 2006 were breastfed at 6 months and only
14.1 percent were breastfed exclusively through these six months (“Maternal”, 2013). The
mother’s level of education is correlated with her decision to breastfeed. The higher the
education level, the more likely the mother is to breastfeed. For example, Graph 2 shows that 85
percent of mothers with a bachelor’s degree or higher have ever breastfed, while 65 percent of
mothers who graduated high school have ever breastfed (“Breastfeeding Rates”, 2014). Mothers
would be more inclined to breastfeed if they were able to work too. In 2009, 25 percent of
employers reported providing an onsite lactation/mother’s room. The goal is to increase this
number as well (“Maternal”, 2013). This would allow more women to breastfeed while ensuring
that infants are breastfed for the recommended duration of their early lives.
2

U.S. BREASTFED INFANTS
Graph 1: Infants ever Breastfed (percent) (“Maternal”, 2013)
3

U.S. BREASTFED INFANTS
Graph 2: Breastfeeding Rates by Duration and Education Level (“Breastfeeding Rates”, 2014)
HEALTH OUTCOMES
Breastfeeding provides a number of health benefits for the infant. Those infants who were
never breastfed have a higher risk of developing chronic diseases such as diabetes, infections,
sudden infant death syndrome (SIDS), obesity, and pediatric asthma as compared to those infants
who were breastfed (Dimas & Wych, 2013). For example, infants who were breastfed for 9
months had a 30 percent less chance of becoming overweight (“Does”, 2007). Breastfeeding can
4

U.S. BREASTFED INFANTS
protect your baby from developing allergies (“How”, 2014). It also helps the baby’s immune
system as breast milk contains many vitamins and minerals (“Breastfeeding vs.”, 2014). In
addition, it contains antibodies, or disease-fighting cells, which protect infants from germs and
illness. Breastfeeding is associated with a lower risk of ear infections, stomach viruses,
respiratory infections, atopic eczema, leukemia, and necrotizing enterocolitis (gastrointestinal
disease) in infants. Breast milk is easier to digest for infants because it takes time for their
stomachs to adjust to digesting the proteins in cow milk (“Breastfeeding fact”, 2013). Health
problems associated with a lack of breastfeeding can be more serious in emergent countries. The
lack of breastfeeding has been found to be associated with the risk for diarrhea, morbidity, and
mortality in developing countries (Lamerti, Walker, Noiman, Victora, and Black, 2011).
Therefore, it is clear that a lack of breastfeeding is often associated with stomach and digestive
system issues. Additionally, it is significant that breastfeeding has also been linked to
intelligence. Children who were exclusively breastfed during infancy have slightly higher IQ’s
than children who were given formula (“Breastfeeding vs.”, 2014).
Breastfeeding provides a number of health benefits for the mother as well. It lowers the
risk of cardiovascular disease and high blood pressure in mothers (“Breastfeeding vs.”, 2014). As
these are major health issues in the US, it is important to raise awareness of any measures that
could decrease these risks. Breastfeeding is associated with a lower risk of Type II diabetes,
breast cancer, ovarian cancer, and postpartum depression for the mother. (“Breastfeeding fact”,
2013). Breastfeeding can aid in the psychological health of the mother, too. Like the risk of
postpartum depression, stress levels are also decreased by breastfeeding (“How”, 2014). The
process provides warmth and closeness between the mother and child (“Why”, 2013). This
improves the mother’s psychological health and provides comfort for the infant. Therefore,
breastfeeding improves health outcomes in both the mother and infant.
HEALTHY PEOPLE 2020
Objective MICH-21 directly correlates with the behavior of interest, concerning the
amount of infants who are breastfed in the US. Objective MICH-21 states to increase the
proportion of infants who are breastfed. Objectives MICH-21.1 through MICH-21.5 state this
goal over certain time periods and differentiate whether the breastfeeding was exclusive or not.
For example, Objective MICH-21.5 states to increase the proportion of infants who were
breastfed exclusively through six months. This paper is mainly going to focus on Objective
5

U.S. BREASTFED INFANTS
MICH-21.1, which is to increase the proportion of infants who are ever breastfed. Specifically,
the goal of Objective MICH-21.1 is to increase the proportion of infants who are ever breastfed
from 74 percent to 81.9 percent.
Although it is important to breastfeed exclusively and extensively, there is still a large
proportion of the population of US infants who have never been breastfed. This population
should be targeted first because it is at the highest risk for developing the above health problems.
Awareness of the benefits of breastfeeding and a higher accessibility to breastfeeding should be
implemented. Access is a large barrier to this problem though. Objective MICH-22 states to
increase the proportion of employers that have worksite lactation support programs. The goal of
Objective MICH-22 is to increase the proportion of employers that have worksite lactation
support programs from 25 percent to 38 percent (“Maternal”, 2013). This would allow more
working mothers who do not breastfeed at all a chance to breastfeed exclusively and extensively.
One of the top reasons that women do not breastfeed is the inability of going back to work while
breastfeeding. Objective MICH-22 provides women with this option and, in effect, would
increase the proportion of infants who are breastfed in the US.
BELIEFS AND KNOWLEDGE
The intrapersonal factors of breastfeeding involve the individual mother’s beliefs, values,
attitudes, and knowledge about the issue. A mother’s personal opinion concerning breastfeeding
can vary considerably. Some mothers may feel that breastfeeding is too much of a hassle and
inappropriate to do in public. A mother may also feel embarrassed to breastfeed in public.
Mothers may not know the health benefits of breastfeeding or how to breastfeed correctly.
Breastfeeding can be learned in a hospital after having given birth. Some women may fear that
breastfeeding hurts and causes discomfort to the breast. Another common worry mothers have is
that they won’t produce enough milk for the baby. These personal concerns can cause mothers to
steer away from breastfeeding. On the other hand, a mother may feel that breastfeeding is a
positive action because it establishes a bond with her child. Mothers who feel comfortable with
breastfeeding anywhere and can easily do it in their daily lives will feel less embarrassed or
stressed about the process. Also, a mother would be more inclined to overcome any stress or
embarrassment if she was well informed of the health benefits of breastfeeding for the baby as
well as for herself. Knowledge and personal skills can influence one’s attitudes and beliefs about
breastfeeding. If a mother knew how to breastfeed without any problems, this would increase her
6

U.S. BREASTFED INFANTS
chances of deciding to carry out the process. Another personal concern is money. A mother may
realize that breastfeeding is a free option and this may sway her decision as well. These internal
factors can have a large impact on the mother’s decision to breastfeed.
DEMOGRAPHICS
Traits, such as beliefs and knowledge, are not the only factors associated with the
decision to breastfeed. Personal demographics correlate to breastfeeding as well. The
relationship between race and breastfeeding has been determined. Foreign-born, Hispanic
mothers are more likely to breastfeed overall (Heck, Braveman, Cubbin, Chavez, & Kiely,
2006). It was found that Hispanics were more likely to breastfeed in Eastern states, while whites
were more likely to breastfeed in Western states (Scanlon et al., 2010). Breastfeeding rates are
positively correlated with the mother’s age. For example, mothers aged 30 and over have the
highest rates of breastfeeding. Young mothers have less knowledge about the health benefits of
breastfeeding so their breastfeeding rate is lower (Department of Health, Social Services and
Public Safety, 2004). A mother’s education level is also positively correlated to breastfeeding
rates (“Breastfeeding Rates”, 2014). Therefore, women with a higher family income are more
likely to breastfeed than women with a low family income (Heck, Braveman, Cubbin, Chavez, &
Kiely, 2006).
PERSONALITY CHARACTERISTICS
Psychological factors can make or break a mother’s decision to breastfeed. A mother may
choose and continue to breastfeed because of the psychological bond she forms with the baby.
She is able to nourish and protect her baby in a natural way. Correctly carrying out the process
can increase the mother’s confidence in her ability of being a mother. Another psychological
aspect is guilt. A mother could feel guilty that she does not breastfeed if she knows that she is
depriving the child of health benefits or a deeper bond with herself. Certain personality types are
more likely to breastfeed than others. A study in the Journal of Advanced Nursing showed that
outgoing mothers are more likely to breastfeed and continue breastfeeding for a longer period of
time. Introverted and anxious mothers who lacked emotional stability were more self conscious
about the process and were less likely to breastfeed (Brown, 2013). Extroverted, outgoing
women are more likely to feel comfortable breastfeeding in public and less embarrassed about
the process. A woman with an easygoing personality would be less stressed by the process,
therefore would be more inclined to breastfeed. However, a woman who worries often would
7
U.S. BREASTFED INFANTS
constantly be concerned that she was not providing enough milk for the baby or that she was
doing the process wrong. A money conscious woman would be more likely to breastfeed for
conservation reasons. Many different factors just involving the mother’s personality will impact
her decision to breastfeed.
SOCIAL SUPPORT
Interpersonal factors of breastfeeding involve how the mother is influenced by her
relationships with others and their own behaviors and attitudes. Social support is a major
contributing factor to a successful process of breastfeeding (Plitcha & Raj, 1998). People with
whom one has close relationships, such as family, can usually provide the best support system.
The support of a spouse can make or break one’s decision to continue breastfeeding or to
breastfeed at all. For example, a spouse may have an introverted personality and be embarrassed
for his wife to breastfeed in public. A spouse can provide emotional support, which can be very
important in the process. A woman also needs informational or instrumental support from others.
The woman’s mother can provide this by teaching her daughter what she knows from experience
or by aiding in the actual process. Families, especially mothers, can be vital in this health
behavior because it is a private, delicate matter that is usually only shared with those very close
to the new mother. Grandmothers or mothers-in-law can offer informational or instrumental
support as well.
SOCIAL INTERACTIONS
While family and close friends can provide the strongest social support in the
breastfeeding process, a mother’s relationship with others can be influential as well. A mother’s
social interactions can have an important impact on the breastfeeding process. Friends,
neighbors, one’s doctor, one’s nurse, classmates, co-workers, and bosses are all examples of
influential social interactions in a new mother’s life. Of course, social interactions include family
and close friends as well. A woman’s friends can influence the breastfeeding process by
understanding that breastfeeding will affect a large part of the woman’s daily life. The friends
could aid in the process by offering informational support if they have experience. If a woman’s
friend is a new mother as well, she could offer support by attending breastfeeding classes with
the woman. A mother’s social interactions in the learning process of breastfeeding can be a
deciding factor for one’s continuation of the behavior. It has been proven that social support
largely influences a mother’s breastfeeding self-efficacy (McCarter-Spaulding & Gore, 2012).
8

U.S. BREASTFED INFANTS
The teacher of the classes can help the mother hone her skills for the process and therefore
provide a sense of self-efficacy for the mother. The mother can also be reassured that she is not
the only one having difficulty with the behavior and she can communicate with others who have
had similar experiences. The learning process can also be affected by interactions in the hospital
directly after birth. This is the time when nurses teach the mothers about breastfeeding. If a
mother hasn’t attended any birthing classes, this may be the first time that she has heard anything
about the process. This makes these interactions during teaching periods all the more vital to the
success of the behavior. For example, if a mother is in a fragile state after having given birth and
does not have a good relationship with her nurse, she may give up on the behavior if she fails the
first couple of times. A supportive and informative nurse is very important to have because he or
she could also provide the mother with a sense of self-efficacy as well. A positive relationship
between the mother and her physician is essential for many of the same reasons. A physician can
offer informative support throughout the process of breastfeeding if the mother reaches out. A
woman’s social interactions with people at her workplace can be a crucial factor in determining
if she continues or even begins the behavior of breastfeeding. If a boss does not allow much time
off of work or for a mother to bring her baby to work, lack of access could be the sole reason for
the decision to not breastfeed. If, on the off chance, a woman’s workplace does offer lactation
support programs, she may choose not to breastfeed because her co-workers may not support the
behavior. In contrast, the people at a woman’s workplace may be in full support of the behavior
and provide the access and emotional support that she needs to decide to carry out the process.
There are many social interactions at a workplace that can determine the execution of this
behavior. The attitudes and behaviors of others and the mother’s relationship with these people
are all influential in the behavior of breastfeeding in the U.S.
ORGANIZATIONS
The main organizational factor related to breastfeeding is the workplace. Workplaces can
provide services to their employees, such as lactation support programs. According to Healthy
People 2020, 25 percent of employers reported providing an onsite lactation or mother’s room in
2009 (U.S. Department of Health and Human Services, 2013). The goal for Healthy People 2020
is for 38 percent of workplaces to offer this opportunity. Workplaces can also set standards for
their employees related to breastfeeding. Many workplaces will provide maternity leave but no
further standards after this to promote continued breastfeeding. One’s church is another
9

U.S. BREASTFED INFANTS
significant organizational factor that can affect breastfeeding. The support of an organization
such as this can affect if the mother chooses to continue the behavior in other organizations. For
example if a church encouraged breastfeeding, a mother may be more inclined to also perform
this behavior at her workplace as long as her workplace offered lactation rooms. A school is
another factor at the organizational level that can have an influence on breastfeeding. If students
are educated about the advantages of breastfeeding, this could increase breastfeeding rates in the
future. For instance, information about breastfeeding could be further incorporated into health
classes in middle schools, high schools, or colleges. Since breastfeeding rates and the percentage
of lactation rooms at the workplace are lower than desired, changes need to occur to increase
these numbers. Organizations can actually make changes when they come together. Change in
factors influencing the behavior of breastfeeding for the population as a whole begins at the
community level. It is here that power shifts and coalitions start to form.
COMMUNITIES
At the community level, a system of networks influences the behavior of breastfeeding.
At this level organizations, such as workplaces, may come together and attempt to develop a
solution to the health behavior problem. An example of this effort to promote change is for these
organizations to request funding for more lactation rooms at work. This system of networks
requires civic participation. An example of civic participation is for the employed mothers to
voice their desires to keep their newborns healthy by breastfeeding them at work. The system
also demands leadership. An example of leadership is for the bosses of these workplaces to come
together to determine a plan to accommodate the needs of their employees. There are currently
many state coalitions that function within the United States Breastfeeding Committee (U.S.
Breastfeeding Committee, 2013). The goal of these coalitions is to increase the breastfeeding rate
in the United States. A conference for health care providers would be another example of a
system of networks gathering to share information and promote a change. Here, the health
professionals could be refreshed on how to provide guidance for breastfeeding properly. They
could also be reminded to tell every patient who is a new mother about the health benefits of
breastfeeding. Coalitions may choose to target schools. Representatives of pro-breastfeeding
coalitions could travel from school to school and provide information about breastfeeding. This
could also be further incorporated and emphasized in medical schools. Advocates for
breastfeeding may target the media. Through the media, one can promote awareness of the
10

U.S. BREASTFED INFANTS
behavior, provide information to the public about breastfeeding, and keep breastfeeding relevant
and memorable. The media can easily sway a community of people. If community coalitions and
advocates can gain enough support or develop beneficial and significant solutions to
breastfeeding rates, their notions could be made into law.
PUBLIC POLICY
Public policy factors can create major changes in the behavior of breastfeeding for the
population if local, state, or federal laws are implemented and enforced. While change in public
policy is significant, it is harder to accomplish because it requires a broad consensus. An
example of public policy intervention is that the Women, Infant, and Children Organization
(WIC) provides federal grants to states for resources that promote breastfeeding. Some of this
funding offers nutritional education for low income pregnant or breastfeeding women and aid to
infants who are at nutritional risk (U.S. Department of Agriculture Food and Nutrition Service,
2014). According to the US Department of Labor, the Affordable Care Act states that the current
federal law concerning nursing mothers in the workplace requires employers to provide a break
time for mothers to nurse for one year after birth. Employers also must provide a comfortable
place, other than a bathroom for breastfeeding to occur (U.S. Department of Labor, 2013). This
law is beneficial for mothers to have access to breastfeeding while at work. Breastfeeding rates
should increase as a result of this law. The law does not require mothers to breastfeed at work
but allows access so they can make a choice to carry out this behavior. Some states have a
workplace pumping law, while others do not. For example, California employers are encouraged
to make efforts to provide an appropriate break time and room for the employee. South Carolina
currently has no workplace pumping law. Both states share a common public law that a mother
can breastfeed her child in any location, even a public location, if they are authorized to be there
(Marcus, 2014).
PHYSICAL ENVIRONMENT
Often mothers will feel the most comfortable breastfeeding in their own home, but this is
not always an option. The physical environment can affect the behavior of breastfeeding directly
through exposure. For example, a mother may choose not to or be unable to breastfeed her child
in a crowded, loud environment. The public policy level could change this by passing laws to
create healthier environments. If a law passed for there to be an increase in the number of open,
clean parks in a community, women would most likely feel more comfortable and safe to
11

U.S. BREASTFED INFANTS
breastfeed outside of the home. The breastfeeding rate would be likely to increase if lactation
rooms were included in public places, such as restaurants and stores. These would provide clean,
safe, and convenient options for new mothers. The risk of germs and exposure to the risky
general public would decrease with the provision of such resources. The physical environment
can also affect the behavior indirectly by influencing the mother’s perceptions of safety and risk.
A woman may have a number of discernments about carrying out this behavior in the physical
environment. For example, a mother may be nervous to breastfeed her child in an unsanitary
public place, such as a public restroom, for fear of exposure to germs. Also, they may be in a
completely safe environment with harmless people, but be too apprehensive to carry out the
behavior. The physical environment and one’s perception of it can be a major barrier to the
behavior of breastfeeding for a woman.
PREDISPOING FACTORS
The predisposing factors of breastfeeding include one’s knowledge, confidence, and
attitude toward the behavior. They determine whether or not a woman will initially decide to
breastfeed. These factors stem from within the mother, therefore are intrapersonal factors.
Knowledge is an important root in determining one’s attitude and confidence toward
breastfeeding. A mother may not know the health benefits that accompany breastfeeding.
Women often have concerns about breastfeeding because they lack information about the
behavior. Mothers commonly worry that breastfeeding is painful and they fear that they won’t
produce enough milk for the baby. This lack of information can decrease one’s confidence
toward the behavior. A decrease in confidence can make a mother feel embarrassed and
unmotivated to breastfeed in public or at all. A woman may also not be aware that breastfeeding
can establish a bond with her baby and that it provides other healthy benefits. If a mother does
not know if breastfeeding is necessarily a healthy behavior, then she could feel that the behavior
is not very important or have a negative attitude toward the behavior. Women may feel that
breastfeeding is too much of a hassle or inappropriate to do in public. Some mothers consider
breastfeeding to be stressful. One would be more inclined to overcome these attitudes of stress
and embarrassment if one was well informed of the health benefits of breastfeeding for both the
baby and mother. Money may be a personal value for a mother. The realization that
breastfeeding is a free option could sway her decision to engage in the behavior. There are
12

U.S. BREASTFED INFANTS
several preceding internal factors at play can have a large impact on the mother’s decision to
breastfeed.
ENABLING FACTORS
An enabling factor is a factor that allows a woman to engage in the behavior of
breastfeeding. A woman’s skill for breastfeeding is an example of these factors. Skill is
intrapersonal and, in the case of this behavior, requires a learning process. A new mother will
most likely not know how to breastfeed correctly. If she had these skills, she would be more
inclined to carry out the behavior. A woman’s mother can be a key player in helping her to hone
her skills. A woman’s grandmother and mother-in-law can teach skills as well. They can all offer
valuable and instrumental information to the mother. The new mother’s friend can share her
knowledge in the process as well. She could aid by offering information about breastfeeding if
she has experience. Breastfeeding classes could be a beneficial medium to gaining skill.
Acquiring the skills in these classes before giving birth to the child can provide a sense of self-
efficacy for the woman. This confidence could improve her ability to breastfeed when the child
comes. Skill is also acquired from the teachings of a nurse in the hospital after birth. Physicians
can also impart skills on the mother. A woman’s access and availability to breastfeeding are also
examples of enabling factors. Access can be a major barrier to carrying out the behavior. If a
boss does not allow much time off of work or for a mother to bring her baby to work, lack of
access could be the sole reason for the decision to not breastfeed. Workplaces can set standards
for their employees related to breastfeeding. Many workplaces will provide maternity leave but
no further standards after this to promote continued breastfeeding. A woman may be unable to
engage in the behavior because of decreased availability to workplace lactation support
programs. According to Healthy People 2020, 25 percent of employers reported providing an
onsite lactation or mother’s room in 2009 (U.S. Department of Health and Human Services,
2013). The goal for Healthy People 2020 is for 38 percent of workplaces to offer this
opportunity. Also, a safe and sanitary place to breastfeed in public may not be offered in a
community. Mothers are unlikely to breastfeed in crowded, loud environments. Laws serve as
powerful enabling factors. The public policy level could change environments by passing laws to
create healthier environments. If a law passed for there to be an increase in the number of open,
clean parks in a community, women would most likely feel more comfortable and safe to
breastfeed outside of the home. There are currently many state coalitions that function within the
13

U.S. BREASTFED INFANTS
United States Breastfeeding Committee (U.S. Breastfeeding Committee, 2013). The goal of these
coalitions is to increase the breastfeeding rate in the United States. Public policy has intervened
through the Women, Infant, and Children Organization (WIC). This provides federal grants to
states for resources that promote breastfeeding. Some of this funding offers nutritional education
for low income pregnant or breastfeeding women and aid to infants who are at nutritional risk
(U.S. Department of Agriculture Food and Nutrition Service, 2014). According to the US
Department of Labor, the Affordable Care Act states that the current federal law concerning
nursing mothers in the workplace requires employers to provide a break time for mothers to
nurse for one year after birth. Employers also must provide a comfortable place, other than a
bathroom for breastfeeding to occur (U.S. Department of Labor, 2013). This law is beneficial for
mothers to have access to breastfeeding while at work. Some states have a workplace pumping
law, while others do not. For example, California employers are encouraged but not required to
make efforts to provide an appropriate break time and room for the employee. South Carolina
currently has no workplace pumping law. Both states share a common public law that a mother
can breastfeed her child in any location, even a public location, if they are authorized to be there
(Marcus, 2014).
REINFORCING FACTORS
A mother’s decision to continue in the behavior of breastfeeding relies heavily on
reinforcing factors, or feedback for the behavior from others. When this feedback is positive and
encouraging, the mother will feel rewarded for engaging in the behavior. These reinforcing
factors will generally come from people who are close with the mother, like her family and
friends. Social support is a major contributing factor to a successful process of breastfeeding
(Plitcha & Raj, 1998). The support of a spouse can determine the mother’s decision to continue
breastfeeding. If the spouse feels embarrassed for his wife to breastfeed in public, for example,
the mother will most likely decide to stop engaging in the behavior because she does not feel
rewarded. The positive emotional support of a spouse can be very rewarding for the woman. The
attitude of the woman’s mother can also be a significant determinant. If the mother supports and
instructs the woman in the behavior, this would reinforce the woman’s confidence and decision
to breastfeed. A woman’s friends can provide reinforcement by offering helpful advice from
experience, admiring the mother’s behavior, and praising her decision to engage in the behavior.
If the friend is participating in the behavior as well, the two new mothers can celebrate the
14

U.S. BREASTFED INFANTS
behavior together by going to classes and learning more about breastfeeding. A positive
relationship with the teacher of these breastfeeding classes, while the mother learns to hone her
skills and therefore obtain a sense of self-efficacy, can be a very encouraging factor for the
behavior. A woman’s experience with other students in the class, if positive and relatable, can be
another source of reassurance. Health professionals can serve as reinforcement factors for the
mother as well. The most important interactions in the hospital related to breastfeeding occur
directly after birth. This is the time when the nurse teaches the mothers about breastfeeding. If a
mother hasn’t attended any birthing classes, this may be the first time that she has heard anything
about the process. This makes these interactions during teaching periods all the more vital to the
success of the behavior. For example, if a mother does not have a good relationship with her
nurse, she may give up on the behavior if she fails the first couple of times and if the health
professional is unsupportive. A supportive and informative nurse is a very important reinforcing
factor because he or she would fortify the mother’s decision to breastfeed even further. The same
applies for the relationship with the physician. A physician can offer informative support and
praise throughout the process of breastfeeding if the mother reaches out. A woman’s social
interactions with people at her workplace can be a crucial factor in determining if she continues
the behavior of breastfeeding. The behavior may not be is not socially accepted or admired by
co-workers or bosses. This lack of emotional support from peers and one’s leader would be a
significant negative reinforcement. The positive or negative feedback from others is a major
determinant in one’s adherence to breastfeeding.
INTERACTION OF FACTORS
Predisposing factors determine if a woman will decide to breastfeed in the first place. An
example is a woman’s belief that breastfeeding is a hassle. Knowledge and confidence about
breastfeeding are major aspects of these factors as well. If a mother’s predisposing factors cause
her to decide to breastfeed, enabling factors actually allow her to carry out this behavior. Her
personal skills for the behavior and access to breastfeeding determine whether or not she can
physically breastfeed. For example, if she does not know how to breastfeed properly or if her
workplace does not provide lactation support programs, she is unable to breastfeed. If a woman
is able to breastfeed, reinforcing factors will determine if she adheres to the behavior. If a mother
is rewarded with encouraging words from her spouse and close family, she is likely to continue
15

U.S. BREASTFED INFANTS
to breastfeed. All of these factors working together determine if a mother will engage and
continue engaging in the behavior of breastfeeding.
16

U.S. BREASTFED INFANTS
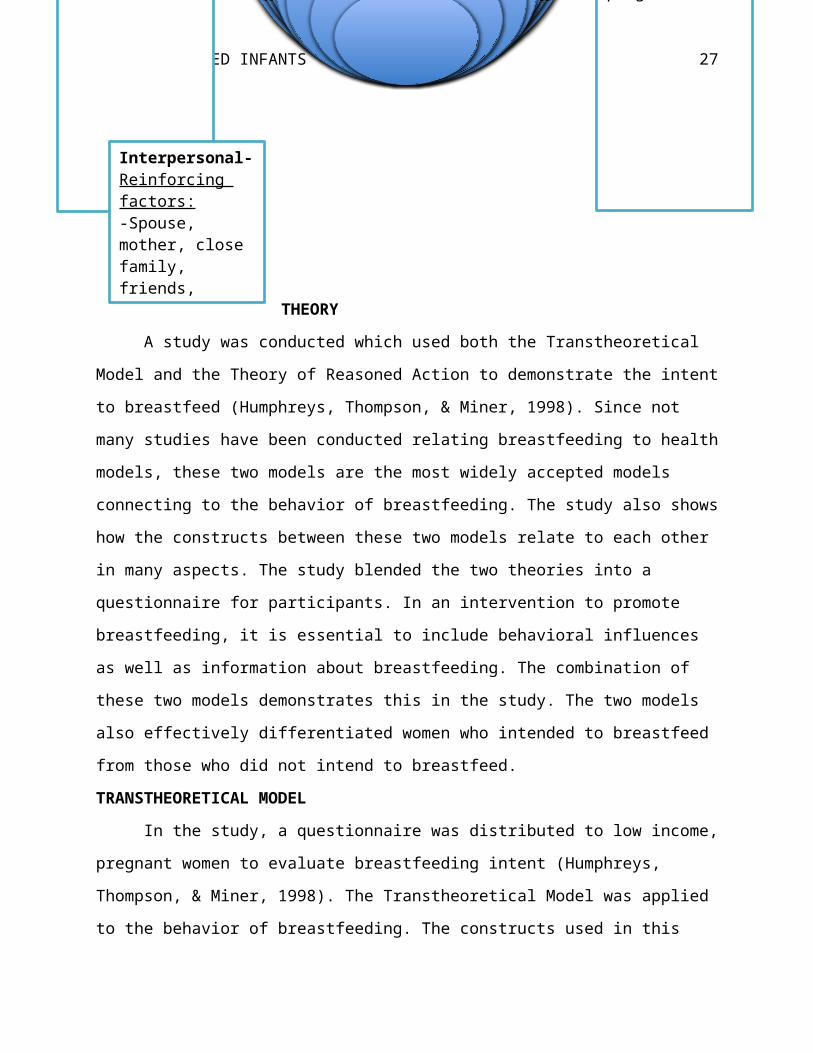
Figure 1: Applied Social Ecological Model Graphic
THEORY
A study was conducted
which used both the Transtheoretical Model and the
Theory of Reasoned Action to demonstrate the intent to
breastfeed (Humphreys, Thompson, & Miner, 1998).
Since not many studies have been conducted relating
breastfeeding to health models, these two models are the most widely accepted models
connecting to the behavior of breastfeeding. The study also shows how the constructs between
these two models relate to each other in many aspects. The study blended the two theories into a
questionnaire for participants. In an intervention to promote breastfeeding, it is essential to
include behavioral influences as well as information about breastfeeding. The combination of
Culture
Physical Environment
Public Policy
Community
Organizational
Interpersonal
Intrapersonal
Culture-Predisposing factor:-Importance of breastfeeding (social norm)
Physical environment-Enabling Factor:-Safe and sanitary public place to breastfeed (access and availability)
Public Policy-Enabling Factors: -Lactation support programs at the workplace (access and availability)-ACA: break time and comfortable place -WIC: federal grants to states for resources that promote breastfeeding- Some states have a workplace pumping law, while others do not
Organizational-Reinforcing factors:-Workplace support of breastfeedingEnabling factor (access and availability):-Workplace maternity leave -Workplace lactation support programReinforcing and Enabling factor:-Breastfeeding class
Interpersonal-Reinforcing factors:-Spouse, mother, close family, friends, classmates, teacher, doctor, nurse, co-workers, boss
Community- Enabling Factor:-State coalitions function to promote breastfeeding
17

U.S. BREASTFED INFANTS
these two models demonstrates this in the study. The two models also effectively differentiated
women who intended to breastfeed from those who did not intend to breastfeed.
TRANSTHEORETICAL MODEL
In the study, a questionnaire was distributed to low income, pregnant women to evaluate
breastfeeding intent (Humphreys, Thompson, & Miner, 1998). The Transtheoretical Model was
applied to the behavior of breastfeeding. The constructs used in this model were
precontemplation, contemplation, preparation, action, and maintenance. Precontemplation is the
stage in which the individual has no intention of changing in the near future. The mother has not
even considered breastfeeding her child at this point. Contemplation is the stage in which the
individual intends to take action within the next six months. The mother thinks she is going to
breastfeed her child at this stage. Preparation is the stage in which the individual has planned and
taken steps toward the action. At this stage, the mother is going to classes to learn about
breastfeeding and acquiring further information about the behavior. Action is the stage in which
the individual has taken part in the behavior. The mother is breastfeeding at this point. Finally,
maintenance is the stage in which the individual has continued the behavior for more than six
months. Therefore, the mother has breastfed her baby for more than six months. The optimal
duration to breastfeed is for the first twelve months. The amount of information about
breastfeeding an individual needs changes at each stage. Each participant’s stage was determined
through statements on a questionnaire. Another study found that social support from the father of
the baby was a major predictor of the mother’s intent to breastfeed (Risica, 2008). It was found
in this newer study that as the individual progressed through these stages, their social support
increased because the subjective norms score in the Theory of Reasoned Action section
increased. Also, attitude toward breastfeeding from the Theory of Reasoned Action became more
positive in these later stages of breastfeeding. This shows that the two theories correlate to each
other when analyzing the behavior of breastfeeding. The number of processes of change for each
stage was also determined through a questionnaire. More processes of change obviously
occurred in the later stages of change. In addition, the study also used the decisional balance
construct. This construct “represents the relative weighing of positive and negative perceptions
associated with the behavior” (Humphreys, Thompson, & Miner, 1998). Decisional balance was
examined through a questionnaire using positive and negative statements. A challenge in the
study was applying the time frame of the stages of change to the pregnancy time frame. The
18

U.S. BREASTFED INFANTS
study only focused on intention to breastfeed, not the action of behavior. This means only the
first three constructs of the Transtheoretical Model were analyzed. Though, the study stated that
intention is correlated with the action of the behavior. The maintenance construct was not fully
analyzed because the behavior of breastfeeding does not occur throughout one’s entire life. This
was a gray area. The goal of the study was to establish a formula that helps practitioners shift the
woman’s decision toward breastfeeding, encourage women to breastfeed for the appropriate
duration of time, and support the woman’s breastfeeding decisions.
INTERVENTIONS USING TRANSTHEORETICAL MODEL
Factors of the Transtheoretical Model were applied to intervention ideas. The lack of
breastfeeding interventions may be the reason that breastfeeding rates have not changed in the
recent years (Humphreys, Thompson, & Miner, 1998). Currently, the goal of breastfeeding
interventions is simply to convey information about breastfeeding, but this is not enough to
promote the action of the behavior. Most women in the study already knew that breastfeeding
was the healthiest choice of feeding. It was found that behavioral influences needed to be
integrated into the informational education of breastfeeding as well. The study found that, in
order to establish a successful educational intervention, the factors leading to the intention and
ultimate decision of breastfeeding must be completely clarified. The Transtheoretical Model
shows that interventions should be based on the individual’s stages of change. The study
suggests that breastfeeding education should be centered on these stages. That means that each
stage would be targeted in the intervention through education. This would allow the intervention
to reach the individual more effectively because the focus would be on the individual, rather than
just forcing general educational information on them. The individual would understand the
factors needed to move forward to the next stage of change. This is an essential factor in the
promotion of breastfeeding through the Transtheoretical Model. If the behavior is successfully
carried out through this model, this would allow further research to be conducted and for the
development of media campaign designs to promote breastfeeding.
THEORY OF REASONED ACTION
The Theory of Reasoned Action was also applied to the behavior of breastfeeding.
Behavioral intention is the key construct of this theory because it directly leads to the behavior.
This intent to breastfeed correlates with the action of breastfeeding. Intention was determined for
each individual through the questionnaire. The constructs used in the study that lead to intention
19

U.S. BREASTFED INFANTS
are attitudes toward the behavior and subjective norms. The attitude construct is an outcome of
behavioral beliefs and the evaluation of behavioral outcomes. This construct was analyzed
through a questionnaire using positive and negative statements about breastfeeding. In this
section of the study, the women identified beliefs that are most important to them. The subjective
norms construct is a result of normative beliefs and the motivation to comply with other’s
beliefs. This construct was measured through a questionnaire to determine the significance of
five close people in the mother’s life, the mother’s perceptions about the people’s breastfeeding
attitudes, and the mother’s likelihood of compliance with the perceived beliefs of the people.
INTERVENTIONS USING THEORY OF REASONED ACTION
The Theory of Reasoned Action can provide a basis to breastfeeding interventions by
distinguishing between women who intend to breastfeed and those who do not by analyzing
attitudes and subjective norms. Through the educational process of the promotion of
breastfeeding, educators can emphasize the belief that differentiates the women who intend to
breastfeed from the women who do not intend to breastfeed. This is important because attitudes
and norms can be greatly affected by the particular behavior and the population. The behavior
and population may change the relative importance of each construct in relation to intention.
Knowing how heavily each construct weighs on the intention to breastfeed is beneficial in
improving educational interventions for breastfeeding (Humphreys, Thompson, & Miner, 1998).
SUGGESTED INTERVENTION PLANS
Many strategies for interventions that have been used and suggested for the behavior of
breastfeeding can be found through research. Formal breastfeeding education, support of the
behavior from people in one’s social group, and an educated professional staff have been proven
to be very effective intervention techniques. These interventions should occur before and after
birth. Suggested interventions at a large-scale level include peer support, social marketing,
workplace initiatives, and public policy initiatives (U.S. Preventive Services Task Force, 2008).
More specifically, maternity care practices have proven to be very effective in the promotion of
breastfeeding. For some of these practices, there is a written policy to promote the behavior.
Examples of these practices are the restriction of pacifiers for infants and the maintenance of
contact between the mother and child after birth. The behavior of breastfeeding is greatly
dependent on timing. It should occur for the baby within the first portion of its life. The
education of breastfeeding for the mother is an essential technique to include in an intervention.
20

U.S. BREASTFED INFANTS
An educated hospital staff is, therefore, significant for the behavior to be successful. This would
enhance maternity care practices. In order to maintain an informed hospital staff, it is
recommended that a written breastfeeding policy is communicated to them on a normal basis and
that they be trained in the skills needed to implement the policy. The staff should know how to
aid the mother in initiating breastfeeding directly after birth and how to show mothers that they
can continue the behavior even when not around the child. The staff should focus on counseling
the mother, encouraging her, and helping in a lactation crisis. Education about the behavior is
important as well but should mainly be obtained through educational programs outside the
hospital. Health care providers should, therefore, refer mothers to breastfeeding support groups
after leaving the hospital. This education of the staff could be accomplished by government
payment for training courses in breastfeeding for the health professionals (Shealy, Li, Benton-
Davis, & Grummer-Strawn, 2005).
Research also suggests that interventions should occur in the workplace. There should be
an increase in employee services, such as corporate policies, to support the behavior, education
about the behavior, a designated space for the behavior to take place at the workplace, flexible
scheduling, and the provision of child care and breast pumps. Breaks and job sharing could help
employees carry out breastfeeding. It was already found that the behavior of breastfeeding
increased when mothers had access to breast pumps and support groups. Public policy is needed
for these interventions to occur in the workplace and to ensure a woman’s right to breastfeed.
Legislation must be passed for workplaces to provide lactation support programs. Public policy
could be influential in promoting the behavior at the workplace by educating employers on the
benefits of supporting breastfeeding employees, creating a model lactation support program for
state employees, and honoring employers who support the behavior in their employees. Public
policy could even expand beyond the workplace. Programs could be implemented to increase
acceptance of the behavior in public places, such as restaurants. The government could also
incorporate designated breastfeeding areas for these same public places (Shealy, Li, Benton-
Davis, & Grummer-Strawn, 2005).
Peer support is an encouraging channel through which intervention can occur. This
support includes emotional support, education about breastfeeding, and aid in the behavior. This
could be individual or could occur through peer support groups. The education that a mother can
gain through this support or through other means is essential to her decision to breastfeed. For
21

U.S. BREASTFED INFANTS
my intervention, education is the most important key. However, education is not limited to the
mother. Others in the mother’s peer support group could participate as well. Social marketing is
an important intervention technique that can boost peer support. Peer support can be increased
and enhanced by increasing public acceptance of the behavior. Advertising can promote
breastfeeding by using images to portray it as a regular, accepted behavior. Examples of slogans
that portray breastfeeding in a positive light and that encourage the behavior include, “Babies
Were Born to Be Breastfed” and “Loving Support Makes Breastfeeding Work”. This
advertisement can be channeled through television stations or billboards. Endorsements and
events encouraging breastfeeding can also occur through social marketing (Shealy, Li, Benton-
Davis, & Grummer-Strawn, 2005).
INTERVENTION PLAN
The strategy that I would use to design an intervention to promote breastfeeding is to,
first, target the predisposing factors that affect a mother’s initial decision to carry out the
behavior. This intervention will focus on the intrapersonal level of the mother from the Social
Ecological Model. Education about breastfeeding is key in my intervention and will continue
throughout the entire process of breastfeeding. Education will be adjusted to accommodate to
whichever phase of the Transtheoretical Model that the mother is in. A mother’s knowledge is
important in determining her initial decision to breastfeed. Knowledge about breastfeeding could
shift a mother from the pre-contemplation to the contemplation stage of the Transtheoretical
Model. Educational programs about breastfeeding will alter the mother’s attitudes and
confidence about the behavior. This attitude toward the behavior can have a direct effect on the
mother’s intention to carry out the behavior has portrayed in the Theory of Reasoned Action.
Distinguishing between a woman who intends to breastfeed and one who doesn’t is very
important in the educational process of my intervention. Knowing this can show which stage of
the Transtheoretical Model the woman is in and the curriculum should, therefore, be altered
depending on her stage. Learning about the health benefits of breastfeeding is an essential
component of intervention. By deciding to actually attend these classes, the mother is moving
into the preparation stage of the Transtheoretical Model. In addition to learning about health
benefits, a mother needs to learn the necessary skills. This intrapersonal enabling factor can have
a huge impact on the mother’s confidence in the behavior. The educational aspect of my
intervention will mainly consist of information about the benefits of breastfeeding and about the
22

U.S. BREASTFED INFANTS
skill of the behavior. Once the mother has moved from the preparation stage to the action stage
of the Transtheoretical Model, my intervention will then focus on providing comfort for her
action of the behavior so that she can reach the maintenance stage. Other enabling factors that I
would target are a mother’s access to the behavior of breastfeeding in the workplace and in other
public places. These factors fall into the organizational, community, public policy, and physical
environment levels of the Social Ecological Model. I would ensure that every mother has an
appropriate maternity leave duration in the workplace and that a policy passes that guarantees
lactation support programs in every workplace. The mothers would also be allotted break times
to breastfeed at work. The workplace pumping law would be required to be used by every state,
not just a select few. Beyond the workplace, I want to enable women to breastfeed, if necessary,
in public. I would create a policy that assures the availability of safe and sanitary breastfeeding
lounges in places, such as stores and parks. The reinforcing factors that I would focus on in my
intervention are the mother’s significant others. These factors all occur at an interpersonal level
of the Social Ecological Model. The subjective norms from these people also have a direct effect
on the mother’s intent to carry out the behavior according to the Theory of Reasoned Action. My
intervention will educate these important people on how to provide positive feedback and
support of the mother’s breastfeeding behavior. They will attend breastfeeding classes with the
mother but learn these encouraging skills in a separate section of the classroom, while the mother
focuses on the information concerning the behavior of breastfeeding. These people will learn to
support the mother in her action until termination of the behavior is appropriate to take place.
This is where the Transtheoretical Model stages will end in the process. While the mother is
attending breastfeeding classes, she will gain social support from her peers who are also learning
the same process. My other way method of promoting positive reinforcing factors in the
mother’s life is to require that health professionals be adequately trained in the encouragement
and act of breastfeeding in order to assist the mother. It is imperative that this interaction with the
health professional to go smoothly for the mother, so that she will feel confident and rewarded
about the behavior. Positive reinforcing factors are important in the workplace as well. Not only
would the mother have access to proper breastfeeding facilities, she would also have the support
of her employer. I would create programs that reward employers for providing these services to
their female employees. These reinforcing factors also affect the cultural level of the Social
Ecological Model. With the implementation of all of these breastfeeding-promoting programs,
23

U.S. BREASTFED INFANTS
widespread public acceptance, from people such as the mother’s co-workers, will eventually
begin to increase as the behavior becomes more prevalent in everyday life. Breastfeeding will
ultimately be well integrated into the United States culture.
References
Breastfeeding-deciding when to stop. (2013). Better Health Channel. Retrieved from
http://www.betterhealth.vic.gov.au/bhcv2/bhcarticles.nsf/pages/
Breastfeeding_deciding_when_to_stop
Breastfeeding fact sheet. (2013). Women’shealth.gov. Retrieved from
http://www.womenshealth.gov/publications/our-publications/fact-sheet/
breastfeeding.html#a
24

U.S. BREASTFED INFANTS
Breastfeeding rates by duration and education. (2014). CollegeBoard. Retrieved from
http://trends.collegeboard.org/education-pays/figures-tables/breastfeeding-rates-duration-
and-education-level
Breastfeeding report card. (2013). CDC. Retrieved from
http://www.cdc.gov/breastfeeding/pdf/2013BreastfeedingReportCard.pdf
Breastfeeding vs. formula feeding. (2014). KidsHealth. Retrieved from
http://kidshealth.org/parent/growth/feeding/breast_bottle_feeding.html#
Brown, A. (2013). Personality may affect a new mother’s decision to breastfeed. Journal
of Advanced Nursing. Retrieved from http://www.wiley.com/WileyCDA/
PressRelease/pressReleaseId-109293.html
Department of Health, Social Services and Public Safety. (2004). Health and social
wellbeing: Young mothers & breastfeeding rates. Equality and Inequalities in Health and
Social Care: A Statistical Overview. Retrieved from
http://www.dhsspsni.gov.uk/breasfeedingratesyoungmothers.pdf
Dimas, H., & Wych, S. (2013). Implementing worksite lactation support programs. Health
Connect One. Retrieved from http://www.cookcountypublichealth.org/files/community-
toolbox/ImplementingWorksiteLactationSupportPrograms_Wych_Dimas.pdf
Does breastfeeding reduce the risk of pediatric overweight? (2007). CDC. Retrieved from
http://www.cdc.gov/nccdphp/dnpa/nutrition/pdf/breastfeeding_r2p.pdf
Heck, K. E., Braveman, P., Cubbin, C., Chavez, G. F., & Kiely, J. L. (2006).
Socioeconomic status and breastfeeding initiation among California mothers. Public
Health Reports, 121(1), 51-59.
How breastfeeding benefits you and your baby. (2014). Babycenter. Retrieved from
http://www.babycenter.com/0_how-breastfeeding-benefits-you-and-your-baby_8910.bc?
page=3
Humphreys, A. S., Thompson, N. J., & Miner, K. R. (1998). Assessment of breastfeeding
intention using the Transtheoretical Model and the Theory of Reasoned Action. Health
Education Research, 13(3), 331-341. Retrieved from http://her.oxfordjournals.org/
content/13/3/331.full.pdf
25

U.S. BREASTFED INFANTS
Lamberti, L. M., Walker, C. L., Noiman, A., Victora, C., & Black, R. E. (2011). Breastfeeding
and the risk for diarrhea morbidity and mortality. BMC Public Health. Retrieved from
http://www.biomedcentral.com/1471-2458/11/S3/S15
Marcus, Jake. (2014). Breastfeeding law: Know your legal rights. Retrieved from
http://breastfeedinglaw.com/
Maternal, infant and child care. (2013). HealthyPeople.gov. Retrieved from
http://www.healthypeople.gov/2020/Data/SearchResult.aspx?
topicid=26&topic=Maternal,%20Infant,%20and%20Child%20Health&objective=MICH-
21.1&anchor=102124
McCarter-Spaulding, D., & Gore, R. (2012). Social Support improves breastfeeding self-efficacy
in a sample of black women. Official Journal of the United States Lactation Consultant
Association. 3(3), 114-117. Retrieved from
http://www.clinicallactation.org/content/social-support-improves-breastfeeding-self-
efficacy-sample-black-women
Plichta, S.B., & Raj, V.K. (1998). The role of social support in breastfeeding promotion: a
literature review. NCBI. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/9543958
Risica, P. M. (2008). Application of behavioral theory to breastfeeding: An opportunity to
optimize counseling and public health interventions. American Public Health
Association. Retrieved from http://www.apha.org/membergroups/newsletters/
sectionnewsletters/food/winter08/
Application+of+Behavioral+Theory+to+Breastfeeding+--
+An+Opportunity+to+Optimize+Counseling+and+Publi.htm
Scanlon, K. S., Grummer-Strawn, L., Li, R., Chen, J., Molinari, N., & Perrine, C. G.
(2010). Racial and ethnic differences in breastfeeding initiation and duration by state.
Morbidity and Mortality Weekly Report, 59(11), 327-334. Retrieved from
http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5911a2.htm
Shealy, K. R., Li, R., Benton-Davis, S., & Grummer-Strawn, L. M. (2005). The CDC guide to
breastfeeding. U.S. Department of Health and Human Services, Centers for Disease Control
and Prevention. Retrieved from
http://www.cdc.gov/breastfeeding/pdf/breastfeeding_interventions.pdf
U.S. Breastfeeding Committee. (2013). Directory of state/territorial/tribal breastfeeding
26
U.S. BREASTFED INFANTS
coalitions. Retrieved from http://www.usbreastfeeding.org/Coalitions/
CoalitionsDirectory/tabid/74/Default.aspx
U.S. Department of Agriculture Food and Nutrition Service. (2014, February 28). Women,
infants, and children. Retrieved from http://www.fns.usda.gov/wic/women-infants-and-
children-wic
U.S. Department of Health and Human Services. (2013, August 28). Maternal, infant, and child
health: Morbidity and mortality. Retrieved from http://www.healthypeople.gov/2020/
topicsobjectives2020/objectiveslist.aspx?topicId=26
U.S. Department of Labor. (2013, August). Wage and hour division. Retrieved from
http://www.dol.gov/whd/regs/compliance/whdfs73.htm
U.S. Preventive Services Task Force. (2008). Primary care interventions to promote breastfeeding:
U.S. Preventive Services Task Force Recommendation Statement. Ann Intern Med. Retrieved
from http://www.uspreventiveservicestaskforce.org/uspstf08/breastfeeding/brfeedrs.htm
Why breastfeed? (2013). Healthychildren.org. Retrieved January 24, 2014, from
http://www.healthychildren.org/English/ages-stages/baby/breastfeeding/pages/Why-
Breastfeed.aspx
27


















