Final Image Evaluation: Left Lateral Lumbar Spine
24
Oral Presentation #10 Nicole Blankenhorn Lateral Lumbar Spine
Transcript of Final Image Evaluation: Left Lateral Lumbar Spine

Oral Presentation #10
Nicole Blankenhorn
Lateral Lumbar Spine

• The image is HIPAA compliant as it does not display any information that violates HIPAA compliancy
Is the image HIPAA compliant?

• There is no anatomical side marker visible on the image
• There is no marker visible that indicates whether a marker was used • Cannot determine
whether a marker was placed beside the anatomical part prior to or following the exposure
Marker & Patient ID

• NOW the anatomical marker correctly marks the side being imaged
• The marker does not superimpose over pertinent anatomy
• There are no additional markers needed/ used for this image• Upright (or a weight-bearing)
marker could be used if patient imaged in that position
• Based on marker placement, the image is correctly displayed • “if a patient’s left side is positioned
closer to IR for a lateral lumbar vertebrae projection, place an L marker on the IR”

• Proper beam restriction requires the presence of at least three sides of collimation on the image
• There are no sides of beam restriction present• Does not mean that BR was not used
• There does not appear to be evidence to prove primary shielding (closest to gonads) was used• For male patients, gonadal shielding
can be employed
• Gonadal shielding must be provided if gonads are within 5 cm of primary beam
Radiation Hygiene

Routine Radiographic Projections Performed:• AP (or PA)• 45 ̊Obliques • AP Obliques• RPO/LPO
• PA Obliques• RAO/LAO
• Lateral (R or L)• Lateral L5-S1 “Spot”
Other Projections May Include:• Erect (Weight-Bearing)• “With bending”
• Flexion• Extension*can be done upright/supine*
• AP/PA Axial – Ferguson Method• Cross Table Lateral “Shoot thru”
Lateral

AP Lumbar
Ferguson Method
Flexion
Extension
“Spot” Lateral
LPO
RPO
AP Obliques (typically done) Projections differ based
on institutional/ departmental
protocol

• This image does comply w/routine position(s)/projection(s)• Routine Projection
• Left Lateral Projection• All anatomical parts correctly visualized

Artifact Identification
• There appears to be no preventable physical artifacts visible • Gas patterns• Soft tissue folds
• There appears to be no body parts superimposed that should not be
• There appears to be no hospital paraphernalia visible
• no patient clothing/belongings visible
• There appears to be no indwelling artifacts/foreign bodies visible

Artifact Identification/ Image Sharpness
• There does not appear to be excess fog that could degrade overall image contrast/visibility of recorded detail & there are no visible CR/DR artifacts
• There appears to be no “gross” voluntary motion visible
• There is no excessive quantum mottle (or image noise) visible
• There is no evidence of a double exposure
• There are no grid lines, grid artifact &/or grid cut-off
• Grids should be used when:• Body parts measure more than 10cm in
thickness• Whenever applied kVp is > 70 to 80
(some sources >60)• Merrill’s recommends a 16:1 grid
NB

Image Sharpness
• Size distortion does not appear greater than expected
• The CR should enter perpendicular to the level of the crest of the ilium (L4)
• Off-centering appears to be less than 1 cm, causing minimal shape distortion

Accurate Part Positioning • The part is adequately aligned to
the longitudinal axis of the imaging media
• The part is slightly off-centered to the image media• Patient should have been moved down
slightly, back JUST A BIT (very minimal)
• The CR does appear to be centered less than 1 cm of anatomical part
• The CR adequately aligned with the imaging media
• The CR’s alignment does conform to an accepted IR exposure field recognition template/field• Collimation not visible

A Note About Lumbar Spines…• Sometimes the center of the vertebral column
may sag, due to lateral flexion, or may be straight but tilted at an angle with the IR• Occurs in patients with broad shoulders & narrow hips
(and vice versa)• Slight sagging is acceptable, as it will better align
the disk spaces with the beam, but excessive sagging will distort vertebral bodies and close disc spaces
THIS is why a radiolucent sponge is placed superior to the crest on some patients!

Note, Continued• IF patient has SCOLIOSIS, place them in the
ERECT POSITION• Place patient in a R or L lateral position• Whichever lateral places the sag (convexity) of the
spine down (better opens intervertebral spaces)
Alignment of CR andScoliotic lumbar vertebra

Positioning • IR Size: 14x17 LW• 40”SID (a 42-46” SID reduces magnification)
Position of Patient• Use same body position (recumbent or upright)
as for PA/AP projection• Ensure patient is dressed in an open-backed
gown so spine can be exposed for adjustment of position
Position of Part• Ask patient to turn onto affected side & flex
hips/knees to a comfortable position• Thin patients require pad under dependent hip
to relieve pressure• Align MCP to midline of grid & ensure that it is
vertical• With the patients elbows flexed, adjust the
dependent arm at right angles to body• To prevent rotation, superimpose knees exactly
& place small sponge/sandbag between them• Place a suitable radiolucent support under lower
thorax & adjust it so that the long axis of the spine is horizontal
• Collimate to 8x17• Suspend at the end of respiration

Central Ray• Enters MCP perpendicular to the level of the crest
of the ilium (L4)• When spine cannot be adjusted so that it is
horizontal, angle the CR caudad so that it is perpendicular to the long axis• Degree of angulation depends on angulation of the
lumbar column& breadth of the pelvis• Typically: 5º for men & 8º for women

Improving Radiographic Quality• The quality of a radiographic image can be
improved if a sheet of leaded rubber is placed on the table behind the patient• kVp is increased for lateral projections due to the
increased part thickness• Lead absorbs scatter
• Scatter decreases radiographic quality• With AEC, scatter coming from patient can
terminate exposure timer prematurely & create an underexposed image• Close collimation necessary

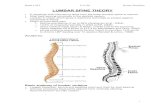
Evaluation Criteria• Area from the lower thoracic
vertebrae to the coccyx• 12th thoracic vertebra, 1st -5th vertebrae
& L5-S1 intervertebral disk spaces included in field
• Open intervertebral disk spaces & intervertebral foramina
• Superimposed posterior margins of each vertebral body
• Vertebrae aligned down the middle of the image
• Nearly superimposed crests of the ilia when the x-ray beam is not angled
• Spinous processes in profile• Evidence: proper collimation

IMAGE EVALUATION
Is the anatomical part correctly positioned? YES
Area from the lower thoracic vertebrae to the coccyx
12th thoracic vertebra, 1st -5th vertebrae & L5-S1 intervertebral disk spaces included in field
Although included, it is difficult to visualize L5S1 joint space
Open intervertebral disk spaces & intervertebral foramina
Superimposed posterior margins of each vertebral body
Vertebrae aligned down the middle of the image
Nearly superimposed crests of the ilia when the x-ray beam is not angled
Spinous processes in profile
Evidence: proper collimation


Exposure Technique • The most radiolucent structures are
the patient soft tissue & air/ gas patterns
• The most radiopaque structures are the bony trabecular markings
• Given that there is no EI value, it is difficult to determine as to whether the image is underexposed, overexposed or adequately exposed
• Upon further observation of the image, I believe that the image was adequately exposed & the EI value was likely within normal range• Long Scale Contrast
• Shade of grey• Adequate amount of brightness
Appears to be sufficient brightness

Accept or Reject?
• This image meets the standards for acceptance criteria
• It is of diagnostic quality
• I would accept this image
• I would change a few things…

• Include marker PRIOR TO the exposure
• Improve BR to having 4 sides- or an acceptable 3 sides!• Include a leaded strip
behind patient • Improves contrast
• Ensure that CR enters at the correct location
• Patient should have been brought back more toward the radiographer • Places spine at center of
field, aligning to longitudinal axis IR

References• Frank,E.D.,Long B.W.,Smith,B.J.,Merrill,V.,&
Ballinger, P.W. (2007). Merrill’s atlas of radiographic positioning & procedures. St Louis,MO: Mosby/Elsevier
• McQuillen-Martensen (2015). Radiographic Image Analysis. Vol 4 St. Louis, MO: Elsevier