Final Case Study Sl

of 17
-
Upload
charmie-mei-paredes -
Category
Documents
-
view
223 -
download
0
Transcript of Final Case Study Sl
-
8/4/2019 Final Case Study Sl
1/17
BIOGRAPHICAL DATA
Name: Baby AC Sex: Female
Birthdate: August 02, 2010 Age: 9 months old
Address: Dona Faustina II Machaca Camp Cul, Quezon City
Religion: Roman Catholic
Nationality: Filipino
Fathers Name: Mr. PC
Mothers name: Mrs. EC
Admission: May 07, 2011 (05:20 AM)
Admitting Diagnosis: Infected Varicella
Attending Physician: Dr. Rachelle A Grafil
HEALTH HISTORY
CURRENT HEALTH PROBLEMS
The condition of the patient started on May 03, 2011, when the mother noticed
vesiculomaculo rash starting from the head going to lower extrimities with
accompanying symptoms of fever and vomiting. They went to Barangay Health Center
and prescribed with Paracetamol and Immunosin. There was no relief of the symptoms
of the patient.
May 06, 2011, persistence of Bullous lesion prompted consult at East Avenue
Medical Center then referred to San Lazaro Hospital hence admitted.
-
8/4/2019 Final Case Study Sl
2/17
PAST HEALTH PROBLEMS
It was her 2nd hospitalization. Her 1st confinement was due to Sepsis Neonatorum
8 months ago. Her common illness includes cough, colds, and fever. Her mother usually
gave her a Paracetamol to relieve her fever. She received 1 dose of BCG, 1 dose Hepa
B, 3 doses of OPV, 3 doses of DPT except for measles. She had no known allergies to
drugs, foods, and agents.
OBSTETRICAL HISTORY
During Mrs. ECs pregnancy, she always go for check- ups in their Barangay
Health Center and was completed her Tetanus Toxoid Vaccine. Baby AC delivered in a
Normal Spontaneous Delivery without any known complications. Baby AC is a breastfed
baby until now but also eats soft foods such as crashed potato and cereals.
FAMILY RISK FACTORS
The family is residing at Bucaue, Bulacan. Mrs. EC verbalized that one of her
cousin had chicken pox. Their common illnesses are cough, colds, headache and fever.
They usually take OTC meds to relieve their illness such as Robitusin for cough and
colds, Alaxan for headache and Paracetamol for Fever. There is no known diseases
noted that runs in their family. There are no known allergies noted in their family.
MEDICATION
Paracetamol drops q4hours for fever
Zinc Oxide to apply in diaper rash
Cloxacillin 250mg/ 5mL QID
-
8/4/2019 Final Case Study Sl
3/17
PERSON ASSESSMENT
PSYCHOSOCIAL Lives at Bucaue, Bulacan with her mother and 2 sisters, ages 5
years old and 3 years old. Her mother and her father separated 5
months ago due to failure to provide the needs of their family. Her
grandmother was the one who provide their needs even her
hospital bills. Her mother is a house wife. She is a Roman Catholic.
She was baptized when she was 5 months old. Her mother usually
brought her to Barangay Health Center for health consultation.
Before hospitalization, she weighs 8.7kgsand now she weighs
7.4kgs. She is active and playful upon assessment.
ELIMINATION She consumed two diapers per day if there is no stool present. She
defecates once a day, sometimes the color is yellow and
sometimes green in color.
REST ANDACTIVITY
She has 16 hours of sleep. Her sleeping time is usually around 7pm
and usually wakes up around 11am. Sometimes she wakes up in
the midnight due to needs to be breastfed. She usually take a naps
around 1pm.
-
8/4/2019 Final Case Study Sl
4/17
SAFEENVIRONMENT
She has no known allergy in medications and foods. She has dry
skin, presence of crust and macules. The mucous membrane is
normal in color and there is no presence of dryness. Her present
temperature is 37C. On admission her temperature is 39.4C.
Medicated with paracetamol, oxacillin and zinc oxide. Medicated at
home with paracetamol for her fever. Upon admission her WBC is
17.19 due presence of infection.
OXYGEN There is no presence of murmur sound. No accessory muscles
being used. Her respiratory rate is 29 cpm. Her cardiac rate is 11O
bpm. No presence of edema. ( - ) homans sign. Upon admission
her Hb: 10.48, Hct: 37.79, and RBC of 402. Blunch test done;
capillary refill immediately back to its normal color.
NUTRITION Still on breast feed, but sometimes her mother gives her soft foods
e.g. crashed biscuits. She is also a bottlefed baby, uses bearbrand
and consumed 1L of milk per day. She has good appetite. She
weighs 7.4, weight loss of 1.3 kgs. over past 4 days. IV: D5 IMB
500cc @ 21 gtts/hour. She is on diet according to age as ordered.
-
8/4/2019 Final Case Study Sl
5/17
DRUG STUDY
NAME OF DRUG/GENERICDRUG CLASIFICATION
ACTION
RATIONALE
SIDE EFFECT NURSING IMPLICATION
OXACILLIN (PINICILLIN)
BETA-LACTAMASEINHIBITOR
DOSAGE:90 mg/kg/day P.OQ 12 hours for 10 days
BACKTERICIDAL
INHIBITS THE ENZYME INCELL WALL SYNTHESIS
NAUSEA, VOMITING,
DIARRHEA, RASH,STOMATITIS,HERPENSENSITIVITYRANGING FROM RASH,UNRTICARIA
SUPER INFECTIONSIGN/SYNTOMS,BLACK,FURRY TONGUE,THRUSH, AND VIGINALDISCHARGE
MONITOR V/S
MONITOR WBC MONITOR I&O
CHECK FORBLEEDING OF HIGHDOSE OFPENICILLIN.
CULTURE &SENSITIVITY
REPORTS RENALFUNCTION TEST
PARACETAMOL(ACETAMINOPHEN)
PARA-AMINOPHENNOLDERIVATIVE
DOSAGE:80 mg P.OQ 4 to 6 hours P.R.N
PRODUCE ANALGESIABY BLOCKING PAIN
IMPULSES BY INHIBITINGSYNTHESIS OFPROSTAGLANDIN IN THECNS
HEMATOLOGIC:HEMOLYTIC ANEMIA,
LEUKOPENIA,NEUTROPENIA,PANCYTOPENIA
HEPATIC: JAUNDICE
METABOLIC:HYPOGLYCEMIA
SKIN: RASH & URTICARIA
MONITOR V/S
MONITOR I&O
MONITOR WBC,RBC CHECK FOR
GLUCOSE ANDHEMOGLOBIN
-
8/4/2019 Final Case Study Sl
6/17
CHICKEN POX
Chickenpox is a highly contagious illness caused by
primary infection with varicella zoster virus (VZV). It
usually starts with vesicular skin rash mainly on the
body and head rather than at the periphery and
becomes itchy, raw pockmarks, which mostly heal
without scarring.
Chickenpox is an airborne disease spread easily
through coughing or sneezing of ill individuals or
through direct contact with secretions from the rash. A
person with chickenpox is infectious from one to five
days before the rash appears. The contagious period continues for 4 to 5 days after the
appearance of the rash, or until all lesions have crusted over. Immunocompromised
patients are probably contagious during the entire period new lesions keep appearing.
Crusted lesions are not contagious. It takes from 10 to 21 days after contact with an
infected person for someone to develop chickenpox.
The onset of illness with chickenpox is often characterized by symptoms
including myalgia, nausea, fever, headache, sore throat, pain in both ears, complaints of
pressure in head or swollen face, and malaise in adolescents and adults. In children,
the first symptom is usually the development of a papular rash, followed by
development of malaise, fever (a body temperature of 38 C (100 F), but may be as
high as 42 C (108 F) in rare cases), and anorexia. Typically, the disease is more
severe in adults. Chickenpox is rarely fatal, although it is generally more severe in adult
males than in adult females or children. Non-immune pregnant women and those with a
suppressed immune system are at highest risk of serious complications. Chickenpox is
believed to be the cause of one third of stroke cases in children. The most common late
complication of chickenpox is shingles, caused by reactivation of the varicella
zoster virus decades after the initial episode of chickenpox.
http://en.wikipedia.org/wiki/Infectious_diseasehttp://en.wikipedia.org/wiki/Infectionhttp://en.wikipedia.org/wiki/Varicella_zoster_virushttp://en.wikipedia.org/wiki/Vesicle_(dermatology)http://en.wikipedia.org/wiki/Rashhttp://en.wikipedia.org/wiki/Pockmarkshttp://en.wikipedia.org/wiki/Airborne_diseasehttp://en.wikipedia.org/wiki/Myalgiahttp://en.wikipedia.org/wiki/Nauseahttp://en.wikipedia.org/wiki/Feverhttp://en.wikipedia.org/wiki/Malaisehttp://en.wikipedia.org/wiki/Papulehttp://en.wikipedia.org/wiki/Malaisehttp://en.wikipedia.org/wiki/Feverhttp://en.wikipedia.org/wiki/Herpes_zosterhttp://en.wikipedia.org/wiki/Herpes_zosterhttp://en.wikipedia.org/wiki/Feverhttp://en.wikipedia.org/wiki/Malaisehttp://en.wikipedia.org/wiki/Papulehttp://en.wikipedia.org/wiki/Malaisehttp://en.wikipedia.org/wiki/Feverhttp://en.wikipedia.org/wiki/Nauseahttp://en.wikipedia.org/wiki/Myalgiahttp://en.wikipedia.org/wiki/Airborne_diseasehttp://en.wikipedia.org/wiki/Pockmarkshttp://en.wikipedia.org/wiki/Rashhttp://en.wikipedia.org/wiki/Vesicle_(dermatology)http://en.wikipedia.org/wiki/Varicella_zoster_virushttp://en.wikipedia.org/wiki/Infectionhttp://en.wikipedia.org/wiki/Infectious_disease -
8/4/2019 Final Case Study Sl
7/17
DIAGNOSIS
The diagnosis of varicella is primarily clinical, with typical early "prodromal" symptoms,
and then the characteristic rash. Confirmation of the diagnosis can be sought through
either examination of the fluid within the vesicles of the rash, or by testing blood for
evidence of an acute immunologic response.
Vesicular fluid can be examined with a Tsanck smear, or better with examination
for direct fluorescent antibody. The fluid can also be "cultured", whereby attempts are
made to grow the virus from a fluid sample. Blood tests can be used to identify a
response to acute infection (IgM) or previous infection and subsequent immunity (IgG).
Prenatal diagnosis of fetal varicella infection can be performed using ultrasound, though
a delay of 5 weeks following primary maternal infection is advised. A PCR (DNA) test of
the mother's amniotic fluid can also be performed, though the risk of spontaneous
abortion due to the amniocentesis procedure is higher than the risk of the baby
developing foetal varicella syndrome.
EPIDEMIOLOGY
Primary varicella is an endemic disease. Cases of varicella are seen throughout the
year but more commonly in winter and early spring. Varicella is one of the classic
diseases of childhood, with the highest prevalence in the 410 year old age group.
Like rubella, it is uncommon in preschool children. Varicella is highly communicable,
with an infection rate of 90% in close contacts. Most people become infected before
adulthood but 10% of young adults remain susceptible.
Historically, varicella has been a disease predominantly affecting young school-aged
children. In adults the pock marks are darker and the scars more prominent than inchildren.
http://en.wikipedia.org/wiki/Prodromehttp://en.wikipedia.org/wiki/Rashhttp://en.wikipedia.org/wiki/Tzanck_testhttp://en.wikipedia.org/wiki/Direct_fluorescent_antibodyhttp://en.wikipedia.org/wiki/Ultrasoundhttp://en.wikipedia.org/wiki/Polymerase_chain_reactionhttp://en.wikipedia.org/wiki/Amniotic_fluidhttp://en.wikipedia.org/wiki/Spontaneous_abortionhttp://en.wikipedia.org/wiki/Spontaneous_abortionhttp://en.wikipedia.org/wiki/Amniocentesishttp://en.wikipedia.org/wiki/Endemic_(epidemiology)http://en.wikipedia.org/wiki/Rubellahttp://en.wikipedia.org/wiki/Rubellahttp://en.wikipedia.org/wiki/Endemic_(epidemiology)http://en.wikipedia.org/wiki/Amniocentesishttp://en.wikipedia.org/wiki/Spontaneous_abortionhttp://en.wikipedia.org/wiki/Spontaneous_abortionhttp://en.wikipedia.org/wiki/Amniotic_fluidhttp://en.wikipedia.org/wiki/Polymerase_chain_reactionhttp://en.wikipedia.org/wiki/Ultrasoundhttp://en.wikipedia.org/wiki/Direct_fluorescent_antibodyhttp://en.wikipedia.org/wiki/Tzanck_testhttp://en.wikipedia.org/wiki/Rashhttp://en.wikipedia.org/wiki/Prodrome -
8/4/2019 Final Case Study Sl
8/17
PATHOPHYSIOLOGY
Exposure to VZV in a healthy child initiates the
production of host immunoglobulin
G (IgG),immunoglobulin M (IgM), and immunoglobulin
A (IgA) antibodies; IgG antibodies persist for life and
confer immunity. Cell-mediated immune responses are
also important in limiting the scope and the duration of
primary varicella infection. After primary infection, VZV
is hypothesized to spread
frommucosal and epidermal lesions to local sensory
nerves. VZV then remains latent in the dorsal ganglion cells of the sensory nerves.
Reactivation of VZV results in the clinically distinct syndrome of herpes
zoster (i.e., shingles), and sometimes Ramsay Hunt syndrome type II.
INFECTION IN PREGNANCY AND NEONATES
For pregnant women, antibodies produced as a result of immunization or previous
infection is transferred via the placenta to the fetus. Women who are immune to
chickenpox cannot become infected and do not need to be concerned about it for
themselves or their infant during pregnancy.
Varicella infection in pregnant women could lead to viral transmission via the placenta
and infection of the fetus. If infection occurs during the first 28 weeks of gestation, this
can lead to fetal varicella syndrome (also known as congenital varicella syndrome).
Effects on the fetus can range in severity from underdeveloped toes and fingers to
severe anal and bladder malformation. Possible problems include:
Damage to brain: encephalitis, microcephaly, hydrocephaly, aplasia of brain
Damage to the eye: optic stalk, optic cup, and
lens vesicles, microphthalmia, cataracts,chorioretinitis, optic atrophy
Other neurological disorder: damage to cervical and lumbosacral spinal cord,
motor/sensory deficits, absent deep tendon reflexes, anisocoria/Horner's syndrome
http://en.wikipedia.org/wiki/Immunoglobulin_Ghttp://en.wikipedia.org/wiki/Immunoglobulin_Ghttp://en.wikipedia.org/wiki/Immunoglobulin_Mhttp://en.wikipedia.org/wiki/Immunoglobulin_Ahttp://en.wikipedia.org/wiki/Immunoglobulin_Ahttp://en.wikipedia.org/wiki/Antibodyhttp://en.wikipedia.org/wiki/Cell-mediated_immunityhttp://en.wikipedia.org/wiki/Mucosahttp://en.wikipedia.org/wiki/Epidermis_(skin)http://en.wikipedia.org/wiki/Sensory_nervehttp://en.wikipedia.org/wiki/Sensory_nervehttp://en.wikipedia.org/wiki/Dorsal_root_ganglionhttp://en.wikipedia.org/wiki/Herpes_zosterhttp://en.wikipedia.org/wiki/Herpes_zosterhttp://en.wikipedia.org/wiki/Ramsay_Hunt_syndrome_type_IIhttp://en.wikipedia.org/wiki/Ramsay_Hunt_syndrome_type_IIhttp://en.wikipedia.org/wiki/Antibodyhttp://en.wikipedia.org/wiki/Placentahttp://en.wikipedia.org/wiki/Fetushttp://en.wikipedia.org/wiki/Virushttp://en.wikipedia.org/wiki/Transmission_(medicine)http://en.wikipedia.org/wiki/Gestationhttp://en.wikipedia.org/wiki/Encephalitishttp://en.wikipedia.org/wiki/Microcephalyhttp://en.wikipedia.org/wiki/Hydrocephalyhttp://en.wikipedia.org/wiki/Aplasiahttp://en.wikipedia.org/wiki/Optic_stalkhttp://en.wikipedia.org/wiki/Optic_cup_(ophthalmology)http://en.wikipedia.org/wiki/Vesicle_(dermatology)http://en.wikipedia.org/wiki/Microphthalmiahttp://en.wikipedia.org/wiki/Cataractshttp://en.wikipedia.org/wiki/Chorioretinitishttp://en.wikipedia.org/wiki/Optic_atrophyhttp://en.wikipedia.org/wiki/Spinal_cordhttp://en.wikipedia.org/wiki/Tendon_reflexhttp://en.wikipedia.org/wiki/Anisocoriahttp://en.wikipedia.org/wiki/Horner%27s_syndromehttp://en.wikipedia.org/wiki/File:Checkenpox_Adult_back.jpghttp://en.wikipedia.org/wiki/Horner%27s_syndromehttp://en.wikipedia.org/wiki/Anisocoriahttp://en.wikipedia.org/wiki/Tendon_reflexhttp://en.wikipedia.org/wiki/Spinal_cordhttp://en.wikipedia.org/wiki/Optic_atrophyhttp://en.wikipedia.org/wiki/Chorioretinitishttp://en.wikipedia.org/wiki/Cataractshttp://en.wikipedia.org/wiki/Microphthalmiahttp://en.wikipedia.org/wiki/Vesicle_(dermatology)http://en.wikipedia.org/wiki/Optic_cup_(ophthalmology)http://en.wikipedia.org/wiki/Optic_stalkhttp://en.wikipedia.org/wiki/Aplasiahttp://en.wikipedia.org/wiki/Hydrocephalyhttp://en.wikipedia.org/wiki/Microcephalyhttp://en.wikipedia.org/wiki/Encephalitishttp://en.wikipedia.org/wiki/Gestationhttp://en.wikipedia.org/wiki/Transmission_(medicine)http://en.wikipedia.org/wiki/Virushttp://en.wikipedia.org/wiki/Fetushttp://en.wikipedia.org/wiki/Placentahttp://en.wikipedia.org/wiki/Antibodyhttp://en.wikipedia.org/wiki/Ramsay_Hunt_syndrome_type_IIhttp://en.wikipedia.org/wiki/Herpes_zosterhttp://en.wikipedia.org/wiki/Herpes_zosterhttp://en.wikipedia.org/wiki/Dorsal_root_ganglionhttp://en.wikipedia.org/wiki/Sensory_nervehttp://en.wikipedia.org/wiki/Sensory_nervehttp://en.wikipedia.org/wiki/Epidermis_(skin)http://en.wikipedia.org/wiki/Mucosahttp://en.wikipedia.org/wiki/Cell-mediated_immunityhttp://en.wikipedia.org/wiki/Antibodyhttp://en.wikipedia.org/wiki/Immunoglobulin_Ahttp://en.wikipedia.org/wiki/Immunoglobulin_Ahttp://en.wikipedia.org/wiki/Immunoglobulin_Mhttp://en.wikipedia.org/wiki/Immunoglobulin_Ghttp://en.wikipedia.org/wiki/Immunoglobulin_G -
8/4/2019 Final Case Study Sl
9/17
Damage to body: hypoplasia of upper/lower extremities, anal and
bladder sphincter dysfunction
Skin disorders: (cicatricial) skin lesions, hypopigmentation
Infection late in gestation or immediately following birth is referred to as "neonatal
varicella".Maternal infection is associated with premature delivery. The risk of the baby
developing the disease is greatest following exposure to infection in the period 7 days
prior to delivery and up to 7 days following the birth. The baby may also be exposed to
the virus via infectious siblings or other contacts, but this is of less concern if the mother
is immune. Newborns that develop symptoms are at a high risk of pneumonia and other
serious complications of the disease.
SHINGLES
After a chickenpox infection, the virus remains dormant in the body's nerve tissues.
The immune system keeps the virus at bay, but later in life, usually as an adult, it can be
reactivated and cause a different form of the viral infection called shingles.
PREVENTION
HYGIENE MEASURES
The spread of chicken pox can be prevented by isolating affected individuals. Contagion
is by exposure to respiratory droplets, or direct contact with lesions, within a period
lasting from three days prior to the onset of the rash, to four days after the onset of the
rash. The chicken pox virus (VZV) is susceptible to disinfectants, notably chlorine
bleach (i.e., sodium hypochlorite). Also, like all enveloped viruses, VZV is sensitive to
desiccation, heat and detergents. Therefore these viruses are relatively easy to kill.
VACCINE
Main article:Varicella vaccine
A varicella vaccine was first developed by Michiaki Takahashi in 1974 derived from the
Oka strain. It has been available in the U.S. since 1995 to inoculate against the disease.
Some countries require the varicella vaccination or an exemption before entering
elementary school. Protection from one dose is not lifelong and a second dose is
necessary five years after the initial immunization, which is currently part of the routine
http://en.wikipedia.org/wiki/Horner%27s_syndromehttp://en.wikipedia.org/wiki/Horner%27s_syndromehttp://en.wikipedia.org/wiki/Horner%27s_syndromehttp://en.wikipedia.org/wiki/Hypoplasiahttp://en.wikipedia.org/wiki/Sphincterhttp://en.wikipedia.org/wiki/Cicatricialhttp://en.wikipedia.org/wiki/Hypopigmentationhttp://en.wikipedia.org/wiki/Pneumoniahttp://en.wikipedia.org/wiki/Immune_systemhttp://en.wikipedia.org/wiki/Shingleshttp://en.wikipedia.org/wiki/VZVhttp://en.wikipedia.org/wiki/Bleachhttp://en.wikipedia.org/wiki/Bleachhttp://en.wikipedia.org/wiki/Sodium_hypochloritehttp://en.wikipedia.org/wiki/Viral_envelopehttp://en.wikipedia.org/wiki/Varicella_vaccinehttp://en.wikipedia.org/wiki/Varicella_vaccinehttp://en.wikipedia.org/wiki/Varicella_vaccinehttp://en.wikipedia.org/wiki/Varicella_vaccinehttp://en.wikipedia.org/wiki/Viral_envelopehttp://en.wikipedia.org/wiki/Sodium_hypochloritehttp://en.wikipedia.org/wiki/Bleachhttp://en.wikipedia.org/wiki/Bleachhttp://en.wikipedia.org/wiki/VZVhttp://en.wikipedia.org/wiki/Shingleshttp://en.wikipedia.org/wiki/Immune_systemhttp://en.wikipedia.org/wiki/Pneumoniahttp://en.wikipedia.org/wiki/Hypopigmentationhttp://en.wikipedia.org/wiki/Cicatricialhttp://en.wikipedia.org/wiki/Sphincterhttp://en.wikipedia.org/wiki/Hypoplasia -
8/4/2019 Final Case Study Sl
10/17
immunization schedule in the US. The chickenpox vaccine is not part of the routine
childhood vaccination schedule in the UK. In the UK, the vaccine is currently only
offered to people who are particularly vulnerable to chickenpox.
TREATMENT
Varicella treatment mainly consists of easing the symptoms as there is no actual cure of
the condition. Some treatments are however available for relieving the symptoms while
the immune system clears the virus from the body. As a protective measure, patients
are usually required to stay at home while they are infectious to avoid spreading the
disease to others. Also, sufferers are frequently asked to cut their nails short or to
wear gloves to prevent scratching and to minimize the risk of secondary infections.
The condition resolves by itself within a couple of weeks but meanwhile patients must
pay attention to their personal hygiene. The rash caused by varicella zoster virus may
however last for up to one month, although the infectious stage does not take longer
than a week or two. Also, staying in a cold surrounding can help in easing the itching
as heat and sweat makes it worse.
Although there have been no formal clinical studies evaluating the effectiveness of
topical application of calamine lotion, a topical barrier preparation containing zinc
oxide and one of the most commonly used interventions, it has an excellent safety
profile. It is important to maintain good hygiene and daily cleaning of skin with warm
water to avoid secondary bacterial infection. Scratching may also increase the risk of
secondary infection.
To relieve the symptoms of chicken pox, people commonly use anti-itching creams and
lotions. These lotions are not to be used on the face or close to the eyes.
An oatmeal bath also might help ease discomfort.
CHILDREN
If oral acyclovir is started within 24 hours of rash onset it decreases symptoms by one
day but has no effect on complication rates. Use of acyclovir therefore is not currently
recommended for immunocompetent individuals (i.e., otherwise healthy persons without
known immunodeficiency or on immunosuppressive medication). Children younger than
12 years old and older than one month are not meant to receive antiviral medication if
they are not suffering from another medical condition which would put them at risk of
developing complications.
http://en.wikipedia.org/wiki/Curehttp://en.wikipedia.org/wiki/Immune_systemhttp://en.wikipedia.org/wiki/Bodyhttp://en.wikipedia.org/wiki/Gloveshttp://en.wikipedia.org/wiki/Infectionshttp://en.wikipedia.org/wiki/Hygienehttp://en.wikipedia.org/wiki/Heathttp://en.wikipedia.org/wiki/Sweathttp://en.wikipedia.org/wiki/Calamine_lotionhttp://en.wikipedia.org/wiki/Zinc_oxidehttp://en.wikipedia.org/wiki/Zinc_oxidehttp://en.wikipedia.org/wiki/Human_skinhttp://en.wikipedia.org/wiki/Bacterial_infectionhttp://en.wikipedia.org/wiki/Oatmealhttp://en.wikipedia.org/wiki/Acyclovirhttp://en.wikipedia.org/wiki/Rashhttp://en.wikipedia.org/wiki/Antiviral_medicationhttp://en.wikipedia.org/wiki/Antiviral_medicationhttp://en.wikipedia.org/wiki/Rashhttp://en.wikipedia.org/wiki/Acyclovirhttp://en.wikipedia.org/wiki/Oatmealhttp://en.wikipedia.org/wiki/Bacterial_infectionhttp://en.wikipedia.org/wiki/Human_skinhttp://en.wikipedia.org/wiki/Zinc_oxidehttp://en.wikipedia.org/wiki/Zinc_oxidehttp://en.wikipedia.org/wiki/Calamine_lotionhttp://en.wikipedia.org/wiki/Sweathttp://en.wikipedia.org/wiki/Heathttp://en.wikipedia.org/wiki/Hygienehttp://en.wikipedia.org/wiki/Infectionshttp://en.wikipedia.org/wiki/Gloveshttp://en.wikipedia.org/wiki/Bodyhttp://en.wikipedia.org/wiki/Immune_systemhttp://en.wikipedia.org/wiki/Cure -
8/4/2019 Final Case Study Sl
11/17
Treatment of chicken pox in children is aimed at symptoms whilst the immune system
deals with the virus. With children younger than 12 years cutting nails and keeping them
clean is an important part of treatment as they are more likely to deep scratch their
blisters.
Aspirin is highly contraindicated in children younger than 16 years as it has been related
with a potentially fatal condition known as Reye's syndrome.
ADULTS
Infection in otherwise healthy adults tends to be more severe and active; treatment with
antiviral drugs (e.g. acyclovir) is generally advised, as long as it is started within 2448
hours from rash onset. Remedies to ease the symptoms of chicken pox in adults are
basically the same as those used on children. Moreover, adults are often prescribed
antiviral medication as it is effective in reducing the severity of the condition and the
likelihood of developing complications. Antiviral medicines are not however aimed to kill
the virus, but to stop it from multiplying. Adults are also advised to increase water intake
to reduce dehydration and to relieve headaches. Painkillers such as paracetamol and
ibuprofen are also recommended as they are effective in relieving itching and other
symptoms such as fever or pains. Antihistamines may be used in cases when thesymptoms cause the inability to sleep, as they are efficient for easing the itching and
they are acting as a sedative. As with children, antiviral medication is considered more
useful for those adults who are more prone to develop complications. These
includepregnant women or people who have a poor immune system. Sorivudine, a
nucleoside analogue has been found in few case reports effective in the treatment of
primary varicella in healthy adults. Larger scale clinical trials are needed to demonstrate
the efficacy of this medication.
PROGNOSIS
The duration of the visible blistering caused by varicella zoster virus varies in children
usually from 4 to 7 days, and the appearance of new blisters begins to subside after the
5th day. Chickenpox infection is milder in young children, and symptomatic treatment,
with sodium bicarbonate baths or antihistamine medication may ease itching.
Paracetamol (acetaminophen) is widely used to reduce fever. Aspirin, or productscontaining aspirin, should not be given to children with chickenpox as it can
cause Reye's syndrome.
http://en.wikipedia.org/wiki/Nail_(anatomy)http://en.wikipedia.org/wiki/Aspirinhttp://en.wikipedia.org/wiki/Reye%27s_syndromehttp://en.wikipedia.org/wiki/Infectionhttp://en.wikipedia.org/wiki/Therapyhttp://en.wikipedia.org/wiki/Drugshttp://en.wikipedia.org/wiki/Acyclovirhttp://en.wikipedia.org/wiki/Sleephttp://en.wikipedia.org/wiki/Sedativehttp://en.wikipedia.org/wiki/Pregnant_womenhttp://en.wikipedia.org/wiki/Sorivudinehttp://en.wikipedia.org/wiki/Sodium_bicarbonatehttp://en.wikipedia.org/wiki/Antihistaminehttp://en.wikipedia.org/wiki/Paracetamolhttp://en.wikipedia.org/wiki/Aspirinhttp://en.wikipedia.org/wiki/Reye%27s_Syndromehttp://en.wikipedia.org/wiki/Reye%27s_Syndromehttp://en.wikipedia.org/wiki/Aspirinhttp://en.wikipedia.org/wiki/Paracetamolhttp://en.wikipedia.org/wiki/Antihistaminehttp://en.wikipedia.org/wiki/Sodium_bicarbonatehttp://en.wikipedia.org/wiki/Sorivudinehttp://en.wikipedia.org/wiki/Pregnant_womenhttp://en.wikipedia.org/wiki/Sedativehttp://en.wikipedia.org/wiki/Sleephttp://en.wikipedia.org/wiki/Acyclovirhttp://en.wikipedia.org/wiki/Drugshttp://en.wikipedia.org/wiki/Therapyhttp://en.wikipedia.org/wiki/Infectionhttp://en.wikipedia.org/wiki/Reye%27s_syndromehttp://en.wikipedia.org/wiki/Aspirinhttp://en.wikipedia.org/wiki/Nail_(anatomy) -
8/4/2019 Final Case Study Sl
12/17
In adults, the disease is more severe, though the incidence is much less common.
Infection in adults is associated with greater morbidity and mortality due to pneumonia,
hepatitis, and encephalitis. In particular, up to 10% of pregnant women with chickenpox
develop pneumonia, the severity of which increases with onset later in gestation. In
England and Wales, 75% of deaths due to chickenpox are in adults. nflammation of the
brain, or encephalitis, can occur in immunocompromised individuals, although the risk is
higher withherpes zoster. Necrotizing fasciitis is also a rare complication.
Secondary bacterial infection of skin lesions, manifesting as impetigo, cellulitis,
and erysipelas, is the most common complication in healthy children. Disseminated
primary varicella infection usually seen in the immunocompromised may have high
morbidity. Ninety percent of cases of varicella pneumonia occur in the adult population.
Rarer complications of disseminated chickenpox also include myocarditis, hepatitis,
andglomerulonephritis.
Hemorrhagic complications are more common in the immunocompromised or
immunosuppressed populations, although healthy children and adults have been
affected. Five major clinical syndromes have been described: febrile purpura, malignantchickenpox with purpura, postinfectious purpura, purpura fulminans, and anaphylactoid
purpura. These syndromes have variable courses, with febrile purpura being the most
benign of the syndromes and having an uncomplicated outcome. In contrast, malignant
chickenpox with purpura is a grave clinical condition that has a mortality rate of greater
than 70%. The etiology of these hemorrhagic chickenpox syndromes is not known.
http://en.wikipedia.org/wiki/Pneumoniahttp://en.wikipedia.org/wiki/Hepatitishttp://en.wikipedia.org/wiki/Encephalitishttp://en.wikipedia.org/wiki/Encephalitishttp://en.wikipedia.org/wiki/Herpes_zosterhttp://en.wikipedia.org/wiki/Necrotizing_fasciitishttp://en.wikipedia.org/wiki/Impetigohttp://en.wikipedia.org/wiki/Cellulitishttp://en.wikipedia.org/wiki/Erysipelashttp://en.wikipedia.org/wiki/Myocarditishttp://en.wikipedia.org/wiki/Hepatitishttp://en.wikipedia.org/wiki/Glomerulonephritishttp://en.wikipedia.org/wiki/Anaphylactoid_purpurahttp://en.wikipedia.org/wiki/Anaphylactoid_purpurahttp://en.wikipedia.org/wiki/Anaphylactoid_purpurahttp://en.wikipedia.org/wiki/Anaphylactoid_purpurahttp://en.wikipedia.org/wiki/Glomerulonephritishttp://en.wikipedia.org/wiki/Hepatitishttp://en.wikipedia.org/wiki/Myocarditishttp://en.wikipedia.org/wiki/Erysipelashttp://en.wikipedia.org/wiki/Cellulitishttp://en.wikipedia.org/wiki/Impetigohttp://en.wikipedia.org/wiki/Necrotizing_fasciitishttp://en.wikipedia.org/wiki/Herpes_zosterhttp://en.wikipedia.org/wiki/Encephalitishttp://en.wikipedia.org/wiki/Encephalitishttp://en.wikipedia.org/wiki/Hepatitishttp://en.wikipedia.org/wiki/Pneumonia -
8/4/2019 Final Case Study Sl
13/17
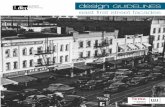
ANATOMY AND PHYSIOLOGY OF RESPIRATORY SYSTEM
-
8/4/2019 Final Case Study Sl
14/17
The nose consists of the visible external nose and the internal nasal cavity. The
nasal septum divides the nasal cavity into right and left sides. Air enters two
openings, the external nares (nostrils; singular, naris), and passes into the
vestibule and through passages called meatuses. The bony walls of the
meatuses, called concha, are formed by facial bones (the inferior nasal concha
and the ethmoid bone). From the meatuses, air then funnels into two (left and
right) internal nares. Hair, mucus, blood capillaries, and cilia that line the nasal
cavity filter, moisten, warm, and eliminate debris from the passing air.
The pharynx (throat) consists of the following three regions, listed in order
through which incoming air passes:
The nasopharynx receives the incoming air from the two internal nares.
The two auditory (Eustachian) tubes that equalize air pressure in the
middle ear also enter here. The pharyngeal tonsil (adenoid) lies at the back
of the nasopharynx.
The oropharyrnx receives air from the nasopharynx and food from the oral
cavity. The palatine and lingual tonsils are located here.
The laryngopharynx passes food to the esophagus and air to the larynx.
The larynx receives air from the laryngopharynx. It consists of the following nine
pieces of cartilage that are joined by membranes and ligaments.
The epiglottis, the first piece of cartilage of the larynx, is a flexible flap thatcovers the glottis, the upper region of the larynx, during swallowing to
prevent the entrance of food.
The thyroid cartilage protects the front of the larynx. A forward projection of
this cartilage appears as the Adam's apple.
-
8/4/2019 Final Case Study Sl
15/17
The paired arytenoids cartilages in the rear are horizontally attached to the
thyroid cartilage in the front by folds of mucous membranes. The upper
vestibular folds (false vocal cords) contain muscle fibers that bring the folds
together and allow the breath to be held during periods of muscular
pressure on the thoracic cavity (straining while defecating or lifting a heavy
object, for example). The lower vocal folds (true vocal cords) contain
elastic ligaments that vibrate when skeletal muscles move them into the
path of outgoing air. Various sounds, including speech, are produced in
this manner.
The cricoid cartilage, the paired cuneiform cartilages, and the paired
corniculate cartilages are the remaining cartilages supporting the larynx.
The trachea (windpipe) is a flexible tube, 10 to 12 cm (4 inches) long and 2.5 cm
(1 inch) in diameter, whose wall consists of four layers, as shown in Figure2 :
The mucosa is the inner layer of the trachea. It contains mucusproducing
goblet cells and pseudostratified ciliated epithelium. The movement of the
cilia sweep debris away from the lungs toward the pharynx.
The submucosa is a layer of areolar connective tissue that surrounds the
mucosa.
Hyaline cartilage forms 16 to 20 C-shaped rings that wrap around the
submucosa. The rigid rings prevent the trachea from collapsing during
inspiration.
The adventitia is the outermost layer of the trachea. It consists of areolar
connective tissue.
The primary bronchi are two tubes that branch from the trachea to the left and
right lungs.
Inside the lungs, each primary bronchus divides repeatedly into branches of
smaller diameters, forming secondary (lobar) bronchi, tertiary (segmental)
bronchi, and numerous orders of bronchioles (1 mm or less in diameter),
including terminal bronchioles (0.5 mm in diameter) and microscopic respiratory
bronchioles. The wall of the primary bronchi are constructed like the trachea, but
as the branches of the tree get smaller, the cartilaginous rings and the mucosa
are replaced by smooth muscle.
http://www.cliffsnotes.com/study_guide/Structure-of-the-Respiratory-System.topicArticleId-22032,articleId-21997.html#pack3734c17-fig-0002http://www.cliffsnotes.com/study_guide/Structure-of-the-Respiratory-System.topicArticleId-22032,articleId-21997.html#pack3734c17-fig-0002 -
8/4/2019 Final Case Study Sl
16/17
Alveolar ducts are the final branches of the bronchial tree. Each alveolar duct has
enlarged, bubblelike swellings along its length. Each swelling is called an
alveolus, and a cluster of adjoining alveolar is called an alveolar sac. Some
adjacent alveoli are connected by alveolar pores.
The respiratory membrane consists of the alveolar and capillary walls. Gas
exchange occurs across this membrane. Characteristics of this membrane follow:
Type I cells are thin, squamous epithelial cells that constitute the primary
cell type of the alveolar wall. Oxygen diffusion occurs across these cells.
Type II cells are cuboidal epithelial cells that are interspersed among the
type I cells. Type II cells secrete pulmonary surfactant (a phospholipidbound to a protein) that reduces the surface tension of the moisture that
covers the alveolar walls. A reduction in surface tension permits oxygen to
diffuse more easily into the moisture. A lower surface tension also prevents
the moisture on opposite walls of an alveolus or alveolar duct from
cohering and causing the minute airway to collapse.
Alveolar macrophage (dust cells) wander among the other cells of the
alveolar wall removing debris and microorganisms.
A thin epithelial basement membrane forms the outer layer of the alveolar
wall.
A dense network of capillaries surrounds each alveolus. The capillary walls
consist of endothelial cells surrounded by a thin basement membrane. The
basement membranes of the alveolus and the capillary are often so close
that they fuse.
-
8/4/2019 Final Case Study Sl
17/17
PATHOPHYSIOLOGY OF CHICKEN POX
PREDISPOSING FACTOR PRECIPITATING FACTOR
>childhood >herpes virus varicellae>occur at any age>socio economic status>environment>occupation
Invasion of virus or microorganism in the upper respiratory tract
Viral proliferation occurs in regional lymph nodes
Primary viremia (post infection 4-6 days)
Second round of viral replication occurs in the bodys internal organ (liver & spleen)
Secondary Viremia (14-16 days post infection)
Diffuse viral invasion of capillary endothelial cell and the epidermis
Intracellular edema intercellular edema
Macule
Papule
Vesicle
Crust