Final 2nd TAG Meeting Report Designed-PK
35
Transcript of Final 2nd TAG Meeting Report Designed-PK


1
Ending Preventable Maternal, Newborn and
Child Mortality:
Regional Technical Advisory Group
Report and Recommendations of the Second Meeting of the South East Asia
Regional Technical Advisory Group (SEAR TAG)
New Delhi, India
8‐9 November 2016
SEA/CAH/131

2
© World Health Organization 2017
Some rights reserved. This work is available under the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo).
Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriately cited, as indicated below. In any use of this work, there should be no suggestion that WHO endorses any specific organization, products or services. The use of the WHO logo is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons licence. If you create a translation of this work, you should add the following disclaimer along with the suggested citation: “This translation was not created by the World Health Organization (WHO). WHO is not responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic edition”.
Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World Intellectual Property Organization.
Suggested citation. Ending Preventable Maternal, Newborn and Child Mortality: Regional Technical Advisory Group. New Delhi: World Health Organization, Regional Office for South-East Asia; 2017. Licence: CC BY-NC-SA 3.0 IGO.
Cataloguing-in-Publication (CIP) data. CIP data are available at http://apps.who.int/iris.
Sales, rights and licensing. To purchase WHO publications, see http://apps.who.int/bookorders. To submit requests for commercial use and queries on rights and licensing, see http://www.who.int/about/licensing.
Third-party materials. If you wish to reuse material from this work that is attributed to a third party, such as tables, figures or images, it is your responsibility to determine whether permission is needed for that reuse and to obtain permission from the copyright holder. The risk of claims resulting from infringement of any third-party-owned component in the work rests solely with the user.
General disclaimers. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of WHO concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted and dashed lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by WHO in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by WHO to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall WHO be liable for damages arising from its use.
3
Content
1. Objectives of the meeting
2. Introduction
3. Recommendations
4. Proceedings of the meeting
1
2
2
5
5. Annexes
Annex 1: Selected country updates
Annex 2: WHO Resolution SEA/RC69/R3
Annex 3: TAG Recommendations (Dec 2015)
Annex 4: List of Participants
Annex 5: Programme
12
25
27
28
29

1
Objectives of the meeting The second meeting of the SEAR‐TAG was organized at the WHO Regional Office for South‐East
Asia, New Delhi on 8‐9 November 2016 with the following objectives:
Review the progress in implementing recommendations from the previous meeting
Review the situation of maternal and child mortality in the Region
Discuss country‐specific high impact actions towards finishing the work of MDGs 4 and 5 in
priority countries
Plan for the next SEAR‐TAG meeting in 2017

2
Introduction
The Technical Advisory Group for Women’s and Children’s Health in the WHO South‐East Asia
Region (SEAR‐TAG) was established in 2015 as a mechanism to guide national governments,
implementing partners and other stakeholders on how best to accelerate implementation and
monitor strategies to advance the unfinished agenda of MDGs 4 and 5 and achieve progress
towards SDG targets.
In its first meeting, held in December 2015, the SEAR‐TAG focused on addressing neonatal
mortality and developed a set of recommendations for WHO, countries and partner agencies.
The subsequent WHO Resolution SEA/RC69/R3 ‘Ending preventable maternal, newborn and
child mortality in the SEAR with focus on newborn mortality’, adopted by the Regional
Committee in September 2016 provided an important basis for discussions during the current
meeting.
Urgent action is required to meet the MDG target levels for reducing maternal and under‐five
mortality by no later than 2018. For this, specific high impact approaches need to be agreed
and promoted in the priority countries in the Region: Bangladesh, India, Indonesia, Myanmar,
Nepal, and Timor Leste. Improving the healthy development, health, safety, and well‐being of
adolescents is also recognized as a high priority for the region.
The SEAR‐TAG meeting was accompanied by discussions among the H6 partners (UNFPA,
UNICEF, UNAIDS, UN Women, WHO and the World Bank). The H6 Regional Working Group was
created to institutionalize the regional interagency platform that would provide technical
assistance, promote multisectoral action, and coordinate partner and donor support to
countries for implementing the Global Strategy. This reflects the clear intent to respond to
governments’ request for less fragmentation and better alignment of efforts as well as the
importance of consistent regional recommendations across the spectrum of reproductive,
maternal, newborn, child and adolescent health, and across UN agencies.
Recommendations
The meeting resulted in recommendations to reinforce national commitment to the UN
Secretary‐General’s Global Strategy for Women’s, Children’s and Adolescents’ Health (“Global
Strategy”), develop a Regional monitoring framework for that strategy, define national technical
priorities, address implementation gaps, strengthen health systems, and intensify the focus on
adolescent health and development.
Reinforce national commitment to the UN Secretary‐General’s Global Strategy for Women’s,
Children’s and Adolescents’ Health (“Global Strategy”) and undertake urgent action towards
ending maternal, newborn and child mortality
1. WHO and other H6 partners will undertake advocacy on reducing maternal, newborn and
child mortality targeting heads of states, ministers of health and parliamentarians. This
includes high level missions to the priority countries to:

3
a. Strengthen national commitment to achieving mortality reduction levels of MDGs 4
and 5 by 2018, and to furthering progress towards Global Strategy and SDG3
targets.
b. Ensure resource mobilization from domestic and external sources.
2. Support countries to set intermediate targets for 2018, 2020, and 2025 towards achieving
the 2030 targets of the Global Strategy and SDG3, with an initial focus on reducing
mortality.
3. Strengthen interagency partnership and improve coordination at regional and country level
through the H6 and other mechanisms.
4. Undertake periodic joint H6 missions to high priority countries for follow‐up to review
progress and ensure technical assistance.
Develop and implement a regional monitoring framework for the Global Strategy
5. WHO and H6 partners will prepare a feasible monitoring framework to guide Member
States on reporting progress on implementing the Global Strategy.
Define technical priorities for maternal newborn and child health for the period 2016 to 2018.
6. Continue to take forward the 2015 TAG recommendations on reducing newborn mortality,
with a specific focus on scaling up recent interventions such as simplified antibiotic
treatment of newborn sepsis where referral is not possible.
7. Strengthen key interventions for maternal and newborn health in high priority countries to
ensure that the Region achieves the MDG level of maternal and newborn mortality
reductions by 2018:
a. Good quality intra‐partum care for mothers and new‐borns at health facilities
b. Good quality facility‐based care for small and sick newborn and for mothers with
complications, with efficient referral transport to facilities
c. Home‐based postnatal care for mothers and new‐borns
d. Prevention and management of adolescent pregnancies
8. Strengthen key interventions for child health in high priority countries to accelerate
mortality reduction to ensure that the Region achieves the MDG level of child mortality by
2018:
a. Strong IMNCI implementation at all three levels of care – home/community, first
level and referral level
b. Campaigns for the control of diarrhoea and pneumonia, aimed at improving
government ownership, public awareness and participation and availability of
essential supplies
c. Improved coverage of routine vaccines (e.g. measles, HiB) and introduction of new
vaccines (PCV, Rotavirus)
Address implementation gaps
9. WHO and H6 partners will collaborate with and support Member States to address
implementation gaps in coverage, quality, data collection and community engagement:

4
a. Coverage gap: build national capacity for effective planning to achieve high and
equitable coverage of the key intervention packages, targeting underserved
populations to ensure that no one is left behind.
b. Quality improvement: build national capacity for continuous quality
improvement methods, focusing initially on maternal and newborn care.
c. Data collection: strengthen the health information system, expand birth and
death registration (including stillbirths) as well as coverage data to monitor
progress, strengthen capacity to conduct Maternal, Perinatal Death Surveillance
and Response and Child Death Reviews.
d. Community engagement: expand activities for public awareness, engagement
and demand generation.
Strengthen health systems
10. Support high priority countries to identify health system bottlenecks and undertake actions
to address these:
a. Improve financing by increasing domestic investment for RMNCAH and
leveraging newer opportunities including GFF, GF, GAVI, and ensure financial
protection to minimize out‐of‐pocket expenses.
1. Strengthen the health workforce for RMNCAH
i. Adequate numbers and mix of staff, with a focus on midwives
ii. Strengthen pre‐service education
iii. Strengthen in‐service continuous professional development
iv. Strengthen capacity of programme managers for planning and
implementation at national and subnational levels
b. Strengthen the service delivery by addressing:
i. Gaps in the health infrastructure including basic amenities of WASH
and electricity
ii. Logistic management of essential supplies and equipment
iii. Definitions of minimum standards for functioning of birthing centres
(case load, staffing, physical infrastructure etc.)
iv. Rationalized and stronger BEmONC and CEmONC services
c. Improve health information system by strengthening birth and death registration
(including stillbirths) and coverage data to monitor progress.
Intensify the focus on adolescent health and development
11. Adolescent Health and Development' will be the theme of the next SEAR‐TAG meeting. This
recommendation is based on the recognition that
Primary care and hospital services have few or no specific provisions for
adolescents; has poor coverage and is generally of sub‐optimal quality
Universal health coverage (UHC) does not specifically address adolescents
Adolescent pregnancy is associated with higher neonatal mortality and maternal
morbidity
Numerous risk behaviours for non‐communicable diseases (NCDs) are initiated
during adolescence, indicating that NCD programmes should include adolescents as
specific risk group

5
There is a double burden of nutrition disorders, where under nutrition including
anaemia is common in boys and girls and overweight/obesity is gradually increasing
The innovative use of information technology and social media for life skills and
empowerment looks promising
School health programming is a good option and requires stronger collaboration
between the ministries of health and education
Proceedings of the meeting
Overview
Between 1990 and 2015, the global maternal mortality ratio (MMR) decreased by 44%.
Countries in the Region made significant progress, with a 69% drop in MMR, from 525 per
100 000 live births in 1990 to 164 in 2015. It is important to note that the burden of
maternal mortality and morbidity in the Region is dynamic, with uneven shifts in the
magnitude, causes, and distribution over time (see Table 1).
Table 1: Progress on MDGs 4 and 5 by country in the WHO South‐East Asia Region
Maternal Mortality Ratio (MMR)
Under‐5 Mortality Rate (U5MR)
MMR 2015
MDG 5 Target
U5MR 2015
MDG 4 Target
Bangladesh 176 142 38 48 [Achieved]
Bhutan 148 236 [Achieved]
33 45 [Achieved]
Democratic People’s Republic of Korea
82 19 25* 14
India 174 139 48 42
Indonesia 126 112 27 28 [Achieved]
Maldives 68* 169 [Achieved]
9* 31 [Achieved]
Myanmar 178 113 50 37
Nepal 258 225 36 47 [Achieved]
Sri Lanka 30* 19 10* 7
Thailand 20* 10 12* 12 [Achieved]
Timor Leste 215 270 [Achieved]
53 59 [Achieved]
South‐East Asia Region
164 131 (69% decline since
1990)
43 39 (64% decline since 1990)
Global 216 96 (44% decline since
1990)
43 30 (52% decline since 1990)
*Below SDG target, need to ensure equity across all population groups.
Source: Levels & Trends in Child mortality ‐ Report 2015: Estimates Developed by the UN Inter‐agency Group for Child Mortality Estimation: Trends in maternal mortality: 1990 to 2015: estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division.
During the SEAR‐TAG meeting, members reviewed the state of programmes and policies
towards achieving at least the MDG levels of mortality reduction in the six priority countries:

6
Bangladesh, India, Indonesia, Myanmar, Nepal and Timor Leste. The discussions aimed to
provide guidance in coherence with WHO to national governments, implementing partners and
other stakeholders on how best to accelerate key implementation strategies, and monitor these
and to move from the MDGs to the new SDG and Global Strategy agendas.
Maternal Health
Regional situation: Dr Elizabeth Mason stressed that the Region made the most progress in
MMR reduction among all the WHO regions during the MDG era. In 2015 the Region had 149
000 fewer maternal deaths than in 1990, with the number having plummeted to 61,000. This is
an unprecedented feat in maternal survival in the history of Member countries of South‐East
Asia However, a review of epidemiology and of policies shows that work remains to be done
(see Annex).
Lancet Maternal Health Series: Dr Wendy Graham presented the highlights of the ‘The Lancet
Series on maternal survival’. This series expands on the current knowledge of maternal health,
its epidemiology, successes, and failings, and comes at a crucial time in the sustainable
development framework to 2030. The series focused on analysing services that support safe
and healthy motherhood. It uses lessons from high‐income countries with low caesarean
section rates, yet good outcomes, and universally applicable low‐cost effective services such as:
o Team based care in maternity hospitals
o Low‐risk units alongside full scope maternity hospitals
o Free‐standing and home based midwifery
Dr Graham concluded with a call to action setting out five key targets to be met in the context
of the SDGs:
1. Prioritize good quality maternal health services that respond to local needs and meet
emerging challenges
2. Promote equity through universal coverage of quality maternal health services
3. Increase resilience and strength of health systems
4. Guarantee sustainable financing for maternal and perinatal health
5. Improve the availability and use of local evidence to inform quality improvement
processes
She proposed that SEAR countries focus on improving the quality of antenatal care and
intrapartum care, also how to link quality with continuous professional development of health
workers, both in their pre‐service and in‐service training. She also indicated that there needs to
be a greater focus on equity and also disaggregation of the data to better understand causality.
Child health
Regional situation: The progress in child survival has been another remarkable achievement of
the Region. With a 64% decline in child mortality, from 118 per 1000 live births in 1990 to 43
per 1000 live births in 2015, the reduction considerably exceeds the global rate of decline of
52%.

7
Reducing child survival is now increasingly dependent on reducing neonatal mortality, and Dr
Rajesh Mehta elaborated on the progress since the previous SEAR‐TAG meeting. Post‐neonatal
child deaths are still largely due to pneumonia, diarrhoea and malaria, with under nutrition
being as high as 60% in some South‐East Asian countries. This contributes significantly to
mortality, and is an area that the SEAR‐TAG must consider prioritizing. (See Annex)
IMNCI ‐ Convergence for Child Survival: Shifting epidemiology trends such as the double
burden of malnutrition, the proportion of child deaths during the newborn period,
environmental challenges to child health along with new technology and innovations like
mHealth, eHealth, new vaccines, diagnostic and treatment innovations indicate a need to a
make changes in IMNCI guidelines and implementation.
A global strategic review of IMNCI carried out in 2016 reflected on the lessons from 20 years of
implementation. With a view to provide state of the art care for all children, the review
included a ‘big picture’ of the best investments in child health. Thirty‐four unique data sources
were used and four SEAR countries were included in the review: Bangladesh, India, Myanmar
and Nepal. Renewed joint leadership by WHO and UNICEF is focusing on the following tasks:
• Planning for a new set of harmonized, flexible guidelines for child health, with a user‐
friendly online dissemination platform;
• Planning for a new global expert advisory group to standardize the systematic review of
care recommendations;
• Rethinking of positioning of child health to restore leadership and financing, and
achieve larger‐scale implementation in countries.
Adolescent Health: Strategic Guidance
A review of available documents and reports relating to WHO and other multilateral regional
strategies provided direction for developing Strategic Guidance on Adolescent Health for
countries in the South‐East Asia Region 2017 – 2020. Dr Bruce Dick presented the noteworthy
progress to date: adolescent health is now firmly and sustainably positioned in a number of
countries, and many activities are being undertaken to address both the unfinished MDG
agendas and the SDG challenges.
Taking advantage of the growing attention to adolescent health, and building on existing
successful partnerships and collaboration, the key components of the upcoming strategy (to be
endorsed by H6 partners) include:
• A life course approach: “triple dividend”
• An ecological model
• A human rights‐based approach
• The prominence of quality, equity and accountability
• Prioritizing, setting targets and implementing the evidence‐based interventions beyond
sexual and reproductive health (SRH)
• Adolescents as a positive force for change
The strategy will focus primarily on the role of the health sector. There is an increasing
awareness of the need to pay attention to a range of adolescent health issues that are often

8
inter‐related and frequently have common determinants. These include mental health
problems (suicide, depression and anxiety, stress and substance use), violence (interpersonal
and gender‐based), unintentional injuries (road traffic injuries and drowning), nutrition (both
under nutrition/anaemia and over‐weight/obesity); common endemic infectious diseases and
chronic conditions/non‐communicable diseases (NCDs). They also include a range of health‐
related behaviours and conditions that undermine adolescents’ health now and carry risks for
the future (tobacco and alcohol use, unhealthy diet and lack of exercise).
Moving the strategy from words to action will require an operational plan that defines
responsibilities for countries and for regional and national partners. The plan will need to cover
a spectrum of issues, from capacity strengthening to the sharing of programme support tools
and information about effective strategies for taking evidence‐based interventions to scale, in
ways that retain the quality that is required for effectiveness.
The SEAR‐TAG recognizes that:
Primary care has few or no specific provisions for adolescents in hospital services
and is of poor coverage and quality
Universal health coverage does not specifically address adolescents
Adolescent pregnancy is associated with higher neonatal mortality and maternal
morbidity
Numerous risk behaviours for non‐communicable diseases (NCDs) are initiated
during adolescence, indicating that NCD programmes should include adolescents as
specific risk group
There is a double burden of nutrition disorders, where under nutrition including
anaemia is common in boys and girls and overweight/obesity is gradually increasing
The innovative use of information technology and social media for life skills and
empowerment looks promising
School health programming is a good option and requires stronger collaboration
between the ministries of health and education
The strategic guidance will be further developed and will be the main focus of the next TAG
meeting.

9
UN Secretary‐General’s Global Strategy for Women’s, Children’s and Adolescents’ Health: New and under‐focused areas and country implications
Dr Vinod Paul described the Global Strategy in the context of the South‐East Asia Region.
Looking further into implications for individual countries, Dr Paul highlighted that countries with
high burdens require urgent action and commitment from the SEAR‐TAG and H6 partners
(above Table 2a and 2b).
Table 2a: WHO South‐East Asia Region: Estimates of maternal mortality ratio, number of deaths,
lifetime risk, and coverage of critical interventions in high priority countries
Maternal health indicators
Maternal Mortality Ratio (per
100 000 live births)
Births in health facility (%)
Caesarean section (CS) rates (%)
Number of
maternal deathsa
Life time Risk of maternal death
Bangladesh 176 37 23 5 500 240
India 174 47 8 45 000 220
Indonesia 126 63 12 6 400 320
Myanmar 178 36 Low 1 700 260
Nepal 258 35 5 1 500 150
Timor‐Leste
215 22 2 94 82
a Numbers of maternal deaths have been rounded according to the following scheme: < 100 rounded to nearest 1; 100–999 rounded to
nearest10; 1000–9999 rounded to nearest 100; and ≥ 10 000 rounded to nearest 1000
Source: Trends in maternal mortality: 1990 to 2015: estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division.

10
Table 2b: WHO South‐East Asia Region: Estimates of under‐five mortality rate and coverage of
interventions in high priority countries
Child health indicators
Under Five Mortality Rate (per 1000 live
births)
Children under 5 with suspected ARI given Ab (%)
Children under 5 with
diarrhoea given ORT (%)
Number of under‐five
deaths (thousands)
Bangladesh 38 71 84 119
India 48 83 54 1 201
Indonesia 27 39 47 147
Myanmar 50 34 66 46
Nepal 36 7 50 20
Timor‐Leste
53 45 78 3
Source: Levels & Trends in Child mortality ‐ Report 2015: Estimates Developed by the UN Inter‐agency Group for Child Mortality Estimation
The Global Strategy is guided by approaches that are country‐led, universal, sustainable, human
rights‐based, equity‐driven, gender‐responsive, evidence‐informed, partnership‐driven, people‐
centred, community‐owned and accountable. It draws its purpose and power from the SDGs.
The three cardinal objectives of the Global Strategy, Survive, Thrive and Transform, portray the
aspiration not only to end preventable mortality, but also to avert illnesses, ensure wellbeing,
and usher in a productive and empowered future. In this way the Global Strategy goes beyond
and is more aspirational than the MDGs.
Renewed commitment, new approaches and invigorated investments will be needed. Since the
interventions to save maternal and child lives are similar for all settings, it is the strength and
resilience of the health system that determines the coverage, equity and quality of
implementation. Each of the building blocks of the health system (infrastructure, human
resources, service delivery, commodities, finances, and governance and information system)
has to be in place to make an impact.
Monitoring the Global Strategy and SDG 3: Regional and
country implications
Monitoring implementation of the Global Strategy and tracking progress towards its
implementation requires a certain number of agreed indicators. After global technical reviews
and an open consultative process, a total of 60 indicators were selected to monitor the
implementation of the Global Strategy. These are published in the Unified Accountability
Framework. A sub‐set of sixteen key indicators were selected to give a snapshot of progress
towards the Global Strategy targets across maternal, newborn/child and adolescent health, and
the cardinal objectives of survive, thrive and transform.

11
These indicators will be relevant for tracking Regional progress on the Global Strategy and for
evidence‐informed advocacy and accountability for resources, results and rights. Equity (SDG
17.18.1) was a cross‐cutting theme. Furthermore, this framework can be used to support
national SDG and health monitoring, with countries adding contextual indicators as relevant.
Regional intermediate targets aligned with the SDG targets and the Global Strategy need to be
set early on, with special emphasis on data availability and regularity. The SEAR‐TAG agreed
that WHO, together with the H6 and other partners, would review and update relevant
Regional data.
Table 3: Proposed Regional intermediate targets on mortality indicators
SEAR 2015 2018 2020 2025 2030
Maternal Mortality Ratio (SDG 3.1.1)
164 Set intermediate Regional targets to
achieve MDGs 4 & 5 levels
135 100 70
Under 5 Mortality Rate (SDG 3.2.1)
43 37 31 25
Neonatal Mortality Rate (SDG 3.2.2)
24 20 16 12
Stillbirth Rate 24 20 16 12
Adolescent Mortality Rate
‐ ‐ ‐ ‐
Source: Accountability in the 2015 Global Strategy for Women’s, Children’s and Adolescents’ Health BMJ 2015; 351 doi: https://doi.org/10.1136/bmj.h4248; Stillbirths: rates, risk factors, and acceleration towards 2030, Lawn et al, Lancet DOI: http://dx.doi.org/10.1016/S0140‐6736(15)00837‐5
Conclusion
The 2030 targets for SDG 3 and the Global Strategy include and go beyond the unfinished
agenda of maternal, newborn and child survival. They require a global maternal mortality ratio
of 70 per 100,000 live births or less, and all countries to achieve neonatal mortality rate of 12
per 1000 live births or less and an under‐five mortality rate of 25 per 1000 live births or less.
Realizing the importance of accelerating reductions in neonatal mortality, where the least gain
was made during the MDG era, the Regional Flagship “Ending preventable maternal, newborn
and child deaths with focus on neonatal deaths” was developed to provide the focus and
resources needed.
The SEAR‐TAG meeting provided a significant opportunity for members and experts to meet
with H6 partners and discuss priorities for the Region. With over 350 million adolescents in the
Region, the meeting aptly put adolescent health and development back on the agenda. The
next SEAR‐TAG meeting is planned to be held in Bhutan in July 2017, and will focus on the
Regional strategic directions for adolescent health.

12
Annex‐1
Selected country updates Bangladesh
MDG SDG
Target Progress from1990 to 2015
Target Situation in 2016
Women’s Health
Maternal mortality ratio
Target 5.A Reduce by three quarters, between 1990 and 2015, the maternal mortality ratio
Significant progress with 69% reduction
SDG 3.1: By 2030, reduce the global maternal mortality ratio to less than 70 per 100 000 live births
176 per 100 000 live births
Proportion of births attended by skilled health personnel
More than 60% increase in the last decade but coverage remains low
42%
Antenatal care coverage (at least one visit)
Target 5.B Achieve, by 2015, universal access to reproductive health
SDG 3.7 and 5.6: By 2030, ensure universal access to sexual and reproductive health care services and rights
64%
Contraceptive prevalence rate
62%
Unmet need for family planning/ Demand unsatisfied for family planning
12%
Children’s Health
Under‐5 mortality rate
Target 4.A Reduce by two‐thirds, between 1990 and 2015, the under‐five mortality rate
Achieved MDG 4 with 74% Reduction in under‐5 mortality
SDG 3.2: By 2030, reduce under‐5 mortality to at least as low as 25 per 1 000 live births
38 per 1000 live births
Infant mortality rate
Newborn interventions prioritized 44% of neonatal deaths due to preterm birth
SDG 3.2: By 2030, reduce neonatal mortality to at least as low as 12 per 1000 live births
31 per 1000 live births
Proportion of 1 year‐old children immunized against measles
Immunization coverage increased equitably
‐
80%
Stillbirth rate ‐ Global Strategy target: By 2030, reduce stillbirths to single digits
25.4 per 1000 total births
Adolescents’ Health
Adolescent birth rate Indicator 5.4
under Target
5.B
More than 50% of girls are married by 18 years of age, thus adolescent pregnancy continues to be very high
SDG 2.2: End all forms of malnutrition and address the nutritional needs of adolescent girls, pregnant and lactating women and children
113 per 1000 girls aged 15‐19
years
Adolescent Mortality
Rate
- ‐ ‐
Source:‐ Levels & Trends in Child mortality ‐ Report 2015: Estimates Developed by the UN Inter‐agency Group for Child Mortality Estimation: Trends in maternal mortality: 1990 to 2015: estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division: World Health Statistics, WHO Publication, 2016; Bangladesh DHS 2014

13
Bangladesh‐ lessons learnt and key actions: (Observations by Shams El Arifeen)
1. Prioritized newborn interventions for common causes of neonatal deaths:
o Infections‐ Chlorhexidine for cord care and emergency management of newborn
infections
o Birth asphyxia‐ resuscitation of new‐borns
o Prematurity‐ Units set up for special care of newborn and for newborn stabilization;
Antenatal corticosteroids provided; Kangaroo Mother Care prominent
2. To achieve SDGs we need to:
o Make every effort possible to achieve, and possibly exceed, the “optimistic” coverage
targets for the interventions:
i. Substantially increase facility deliveries
ii. Focus on a few well‐functioning facilities for providing delivery services
iii. Make “smart” choices on selection of strategies for newborn interventions
iv. Multiple communication channels to reinforce behaviour change
o Invest in improving the quality of services to ensure expected or higher levels of
effectiveness
3. We need to now move beyond the neonatal period and address critical child health problems:
i. Stagnating rates of ORS use for childhood diarrhoea
ii. Uncontrolled use of antibiotics for treatment of pneumonia
iii. Preventing childhood deaths due to drowning

14
India MDG SDG
Target Progress since 1990 in 2015
Target Situation in 2016
Women’s Health
Maternal mortality ratio
Target 5.A Reduce by three quarters, between 1990 and 2015, the maternal mortality ratio
Significant progress with 69 % reduction
SDG 3.1: By 2030, reduce the global maternal mortality ratio to less than 70 per 100 000 live births
174 per 100 000 live births
Proportion of births attended by skilled health personnel
56% increase in delivery with SBA but fewer than half (47%) of childbirths occur in facilities
67%
Antenatal care coverage (at least one)
Target 5.B Achieve, by 2015, universal access to reproductive health
More than 75% covered but still one in four women missed
SDG 3.7 and 5.6: By 2030, ensure universal access to sexual and reproductive health‐care services and rights
75%
Contraceptive prevalence rate
55%
Unmet need for family planning/ Demand for family planning
21%
Children’s Health
Under‐5 mortality rate
Target 4.A Reduce by two‐thirds, between 1990 and 2015, the under‐five mortality rate
With 62 % reduction, missed MDG 4
SDG 3.2: By 2030, reduce under‐5 mortality to at least as low as 25 per 1,000 live births
48 per 1000 live births
Infant mortality rate
Highest number of newborn deaths (748 000 per year) 34% of newborn deaths are due to preterm birth
SDG 3.2: By 2030, reduce neonatal mortality to at least as low as 12 per 1,000 live births
38 per 1000 live births
Proportion of 1 year‐old children immunized against measles
‐
74%
Stillbirth Rate ‐ Global Strategy target: By 2030, reduce stillbirths to single digits
23 per 1000 total births
Adolescents’ Health
Adolescent birth rate
Indicator 5.4
under Target 5.B
43% girls married by 18 years and among them one in three have begun childbearing by 19 years
SDG 2.2: End all forms of malnutrition and address the nutritional needs of adolescent girls, pregnant and lactating women and children
28 per 1000 girls
15‐19years
Adolescent
Mortality Rate
-
‐
Source:‐ Levels & Trends in Child mortality ‐ Report 2015: Estimates Developed by the UN Inter‐agency Group for Child Mortality Estimation: Trends in maternal mortality: 1990 to 2015: estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division: World Health Statistics, WHO Publication, 2016.

15
India‐lessons on approaches for reduction in maternal mortality provision of safe delivery:
(Observations by Nozer Sheriar) 1. Continue the shift to institutional deliveries
o Optimize safer utilization of existing facilities with basic mandatory standards of care and
resources
o Invest in human resource and others including accessible safe blood banks and storage facilities
2. Embark on the Mother/Baby Friendly hospital initiative
o WASH as one of the core indicators of quality
3. Develop and provide facilities for grass roots access
o Basic maternity care to be available close to women
o Enlist services of public and private sector
o Defined role, training and respect for skilled birth attendants
4. Time to create a cadre of dedicated qualified midwifes
o Independent providers of basic maternity care
o Expected to be more sensitive to women and less likely to medicalize childbirth
5. Provide Emergency Obstetric and Neonatal Care facilities
o Recognize significant role in mortality reduction
o Provision of adequate technical resources
6. Increase facilities providing critical obstetric care
o Develop replicable models of advanced critical care facilities for obstetrics
o Map available facilities to identify unserved area
7. Build a system of transport for maternity care
o Emergency response vehicles using toll free number,
o Government and private ambulances
o Referral transport for pregnant women and new‐borns
o Reimbursement or subsidization of transport cost if necessary
8. Communication to women regarding health messaging and entitlements
o Use mobile sms and voice based messaging
o Role for grass root workers such as ASHAs in messaging and advocacy
9. Dissemination and implementation of guidelines
o Standardize guidelines and protocols related to maternal health & childbirth
o Develop a national credible and robust system to create guidelines
o Work to disseminate and implement in partnerships including professional organizations
10. Create an ongoing system of guideline dissemination and upgrades
o Healthcare delivery Checklists
o Adoption of the WHO Safe Childbirth Checklist at all levels of maternity care
16
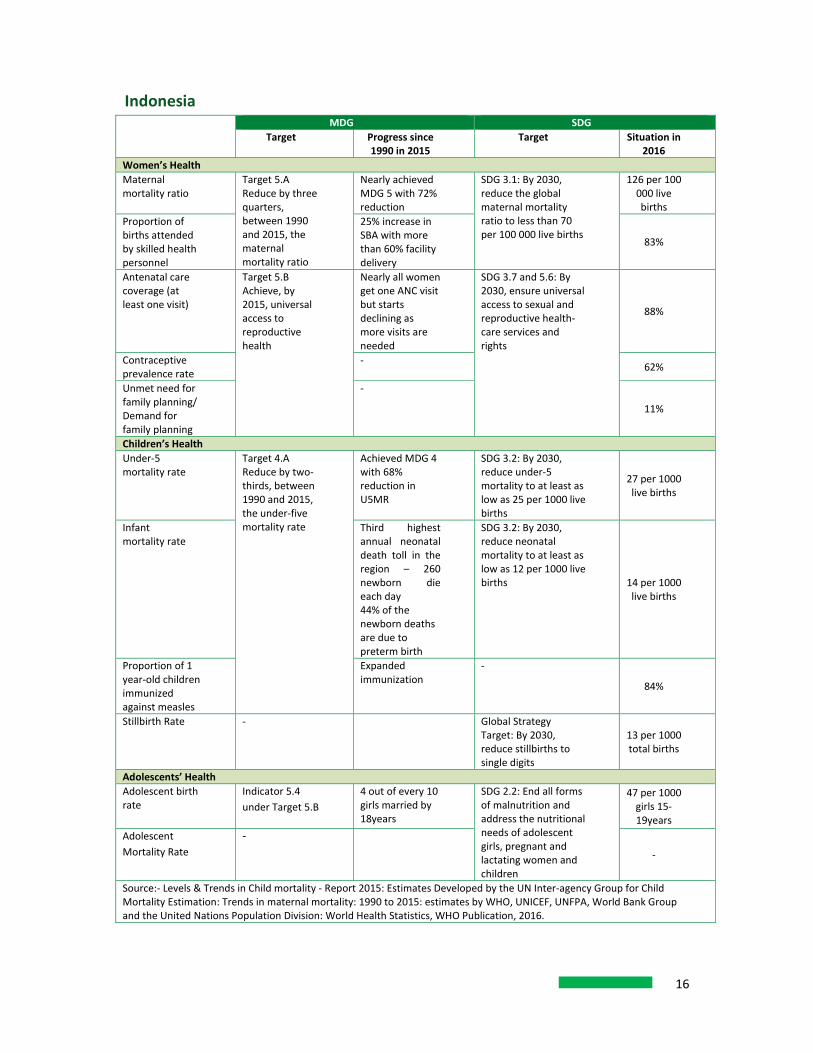
Indonesia MDG SDG
Target Progress since 1990 in 2015
Target Situation in 2016
Women’s Health
Maternal mortality ratio
Target 5.A Reduce by three quarters, between 1990 and 2015, the maternal mortality ratio
Nearly achieved MDG 5 with 72% reduction
SDG 3.1: By 2030, reduce the global maternal mortality ratio to less than 70 per 100 000 live births
126 per 100 000 live births
Proportion of births attended by skilled health personnel
25% increase in SBA with more than 60% facility delivery
83%
Antenatal care coverage (at least one visit)
Target 5.B Achieve, by 2015, universal access to reproductive health
Nearly all women get one ANC visit but starts declining as more visits are needed
SDG 3.7 and 5.6: By 2030, ensure universal access to sexual and reproductive health‐care services and rights
88%
Contraceptive prevalence rate
‐ 62%
Unmet need for family planning/ Demand for family planning
‐
11%
Children’s Health
Under‐5 mortality rate
Target 4.A Reduce by two‐thirds, between 1990 and 2015, the under‐five mortality rate
Achieved MDG 4 with 68% reduction in U5MR
SDG 3.2: By 2030, reduce under‐5 mortality to at least as low as 25 per 1000 live births
27 per 1000 live births
Infant mortality rate
Third highest annual neonatal death toll in the region – 260 newborn die each day 44% of the newborn deaths are due to preterm birth
SDG 3.2: By 2030, reduce neonatal mortality to at least as low as 12 per 1000 live births 14 per 1000
live births
Proportion of 1 year‐old children immunized against measles
Expanded immunization
‐
84%
Stillbirth Rate ‐ Global Strategy Target: By 2030, reduce stillbirths to single digits
13 per 1000 total births
Adolescents’ Health
Adolescent birth rate
Indicator 5.4
under Target 5.B
4 out of every 10 girls married by 18years
SDG 2.2: End all forms of malnutrition and address the nutritional needs of adolescent girls, pregnant and lactating women and children
47 per 1000 girls 15‐19years
Adolescent
Mortality Rate
-
‐
Source:‐ Levels & Trends in Child mortality ‐ Report 2015: Estimates Developed by the UN Inter‐agency Group for Child Mortality Estimation: Trends in maternal mortality: 1990 to 2015: estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division: World Health Statistics, WHO Publication, 2016.

17
Indonesia‐ lessons from Expanding Maternal and Newborn Survival (EMAS) Programme
(Observations by Mohammad Baharuddin)
The USAID supported EMAS programme is a five year cooperative agreement aimed at
contributing to the reduction of maternal and newborn deaths in Indonesia. Within this focus,
EMAS has several overarching objectives:
‐ Contributing to 25% national reduction in maternal and newborn mortality;
‐ Improving quality of emergency care in at least 150 hospitals;
‐ Improving life‐saving clinical interventions and effectiveness of referrals in at least 300
puskesmas
Key findings from EMAS implementation include:
‐ At provincial, district, and facility levels EMAS appears to be contributing to positive
changes in quality, organization, and management of MNH services.
‐ One of EMAS’ most important results has been turning a fragmented referral system
into a functional network, and developing relationships, connection, and
communication within that network.
Evaluation findings related to achieving impact and sustainability at scale include:
‐ Data available from EMAS and from health services do not allow connections between
the observed and reported changes in processes with changes in health worker or
system performance, nor with maternal and newborn mortality.
‐ Because of this lack of certainty about performance and mortality, it will be crucial to
determine the actual operational and clinical causes of continuing maternal and
newborn deaths.
‐ There are important changes happening in Indonesia that could override efforts to increase the effectiveness of maternal and newborn services.

18
Myanmar MDG SDG
Target Progress since 1990 in 2015
Target Situation in 2016
Women’s Health
Maternal mortality ratio
Target 5.A Reduce by three quarters, between 1990 and 2015, the maternal mortality ratio
61% reduction but burden remains high
SDG 3.1: By 2030, reduce the global maternal mortality ratio to less than 70 per 100,000 live births
178 per 100 000 live births
Proportion of births attended by skilled health personnel
40% increase in SBA but only 36% deliver in facilities
78%
Antenatal care coverage (at least one visit)
Target 5.B Achieve, by 2015, universal access to reproductive health
More than half the women who get one visit do not get a second one
SDG 3.7 and 5.6: By 2030, ensure universal access to sexual and reproductive health‐care services and rights
83%
Contraceptive prevalence rate
46%
Unmet need for family planning/ Demand for family planning
n/a
Children’s Health
Under‐5 mortality rate
Target 4.A Reduce by two‐thirds, between 1990 and 2015, the under‐5 mortality rate
With 55% reduction insufficient progress towards achieving MDG 4
SDG 3.2: By 2030, reduce under‐5 mortality to at least as low as 25 per 1000 live births
50 per 1000 live births
Infant mortality rate
‐ SDG 3.2: By 2030, reduce neonatal mortality to at least as low as 12 per 1,000 live births
40 per 1000 live births
Proportion of 1 year‐old children immunized against measles
‐ ‐
86%
Stillbirth Rate ‐ ‐ Global Strategy Target: By 2030, reduce stillbirths to single digits
20 per 1000 total births
Adolescents’ Health
Adolescent birth rate Indicator 5.4
under Target
5.B
72% adolescents began child bearing by 19 years
SDG 2.2: End all forms of malnutrition and address the nutritional needs of adolescent girls, pregnant and lactating women and children
30 per 1000
girls 15‐19 years
Adolescent Mortality
Rate
- ‐
‐
Source: Levels & Trends in Child mortality ‐ Report 2015: Estimates Developed by the UN Inter‐agency Group for Child Mortality Estimation: Trends in maternal mortality: 1990 to 2015: estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division: World Health Statistics, WHO Publication, 2016.

19
Myanmar‐ lessons learnt and accomplishments made: (Observations by Katherine Ba‐Thike)
1. Transition of MDR to MDSR ‐ started in November 2015 (UNFPA and WHO support)
2. Technical and training guidelines of Child Death Surveillance and Response (CDSR) with
advocacy meetings, TOT and multiplier trainings for CDSR done for 2016 and 2017
3. Health workforce initiative on Midwifery‐ ASEAN Regional Guideline for Minimum
Requirements for Training and Accreditation of SBA endorsed by ASEAN, released June 20144.
4. Hospital Equity Fund to support reduction MMR and under‐5 mortality (NMR, IMR, U5MR)
according to national targets of the programme
But efforts still needed:
o Advocacy for investment in RMNCAH at different levels
o Focus on ending preventable maternal and neonatal mortality
o Implement plans that have been developed – Every Newborn Action Plan, Strategic
Plan for Reproductive Health
o Address health system issues to support above plans
o For WHO – to help RMH/MoH to focus on a few issues and “do‐it‐well”

20
Nepal MDG SDG
Target Progress since 1990 in 2015
Target Situation in 2016
Women’s Health
Maternal mortality ratio
Target 5.A Reduce by three quarters, between 1990 and 2015, the maternal mortality ratio
Just missed despite 71% reduction but number of deaths very high
SDG 3.1: By 2030, reduce the global maternal mortality ratio to less than 70 per 100,000 live births
258 per 100 000 live births
Proportion of births attended by skilled health personnel
69% increase but still only one third population catered to for institutional deliveries
36%
Antenatal care coverage (at least one visit)
Target 5.B Achieve, by 2015, universal access to reproductive health
Only half the population covered with very high geographic/social inequities
SDG 3.7 and 5.6: By 2030, ensure universal access to sexual and reproductive health‐care services and rights
58%
Contraceptive prevalence rate
‐ 50%
Unmet need for family planning/ Demand for family planning
‐ 28%
Children’s Health
Under‐five mortality rate
Target 4.A Reduce by two‐thirds, between 1990 and 2015, the under‐five mortality rate
Achieved MDG 4 but 57% of under‐five deaths are due to newborn conditions
SDG 3.2: By 2030, reduce under‐5 mortality to at least as low as 25 per 1000 live births
36 per 1000 live births
Infant mortality rate
SDG 3.2: By 2030, reduce neonatal mortality to at least as low as 12 per 1000 live births
29 per 1000 live births
Proportion of 1 year‐old children immunized against measles
‐ 88%
Stillbirth Rate Global Strategy Target: By 2030, reduce stillbirths to single digits
18 per 1000 total births
Adolescents’ Health
Adolescent birth rate Indicator 5.4 under Target 5.B
40% of the girls are married by 18 years and begin childbearing by 19 years
SDG 2.2: End all forms of malnutrition and address the nutritional needs of adolescent girls, pregnant and lactating women and children
71 per 1000 girls 15‐19years
Adolescent Mortality Rate
Source:‐ Levels & Trends in Child mortality ‐ Report 2015: Estimates Developed by the UN Inter‐agency Group for Child Mortality Estimation: Trends in maternal mortality: 1990 to 2015: estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division: World Health Statistics, WHO Publication, 2016.

21
Nepal‐ lessons learnt but challenges remain: (Observations by D S Manandhar)
a. Financial‐‐ High out of pocket expenditure. The policy is for free newborn care but funding is
inadequate; cost of capacity building /strengthening infrastructure and equipment is
large
b. Programmatic ‐ Inconsistent use of antenatal corticosteroids; inadequate coverage of
Kangaroo Mother Care; quality care issues e.g. use of partograph, inadequate institutional readiness for new born resuscitation, skilled human resource constraint particularly for newborn care, unavailability of services 24/7 for 365 days for both
mother and neonates including postnatal care, inconsistent use of national protocols/guidelines, newborn component is not well addressed in MNCH training,
and monitoring /quality information issues
Way forward:
• Focus on upgrading existing birthing centres to birthing and newborn care centres
• Scale up community mobilization initiatives
• Strengthening referral mechanisms for all children
• Partnerships with private sector in newborn and child health programme
• Local context‐specific planning and support by all partners
• Operational research
• Continuum of quality services to newborn and children
22
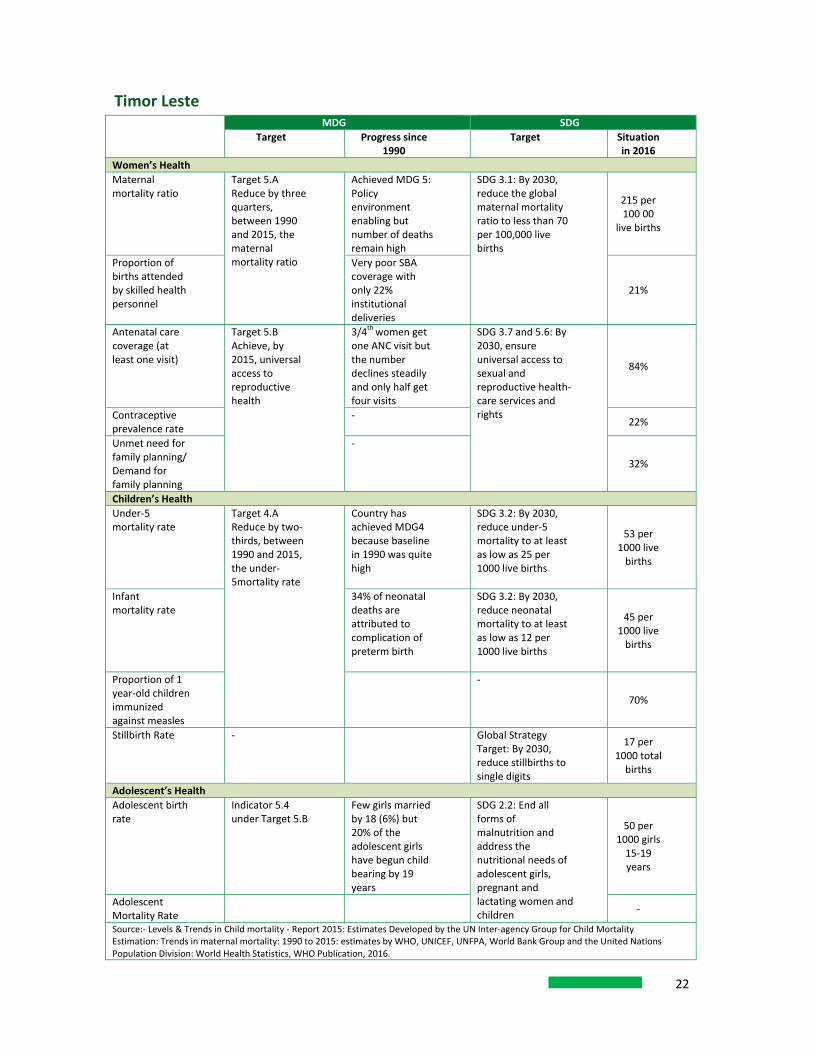
Timor Leste MDG SDG
Target Progress since 1990
Target Situation in 2016
Women’s Health
Maternal mortality ratio
Target 5.A Reduce by three quarters, between 1990 and 2015, the maternal mortality ratio
Achieved MDG 5: Policy environment enabling but number of deaths remain high
SDG 3.1: By 2030, reduce the global maternal mortality ratio to less than 70 per 100,000 live births
215 per 100 00
live births
Proportion of births attended by skilled health personnel
Very poor SBA coverage with only 22% institutional deliveries
21%
Antenatal care coverage (at least one visit)
Target 5.B Achieve, by 2015, universal access to reproductive health
3/4th women get one ANC visit but the number declines steadily and only half get four visits
SDG 3.7 and 5.6: By 2030, ensure universal access to sexual and reproductive health‐care services and rights
84%
Contraceptive prevalence rate
‐ 22%
Unmet need for family planning/ Demand for family planning
‐
32%
Children’s Health
Under‐5 mortality rate
Target 4.A Reduce by two‐thirds, between 1990 and 2015, the under‐5mortality rate
Country has achieved MDG4 because baseline in 1990 was quite high
SDG 3.2: By 2030, reduce under‐5 mortality to at least as low as 25 per 1000 live births
53 per 1000 live births
Infant mortality rate
34% of neonatal deaths are attributed to complication of preterm birth
SDG 3.2: By 2030, reduce neonatal mortality to at least as low as 12 per 1000 live births
45 per 1000 live births
Proportion of 1 year‐old children immunized against measles
‐
70%
Stillbirth Rate ‐ Global Strategy Target: By 2030, reduce stillbirths to single digits
17 per 1000 total births
Adolescent’s Health
Adolescent birth rate
Indicator 5.4 under Target 5.B
Few girls married by 18 (6%) but 20% of the adolescent girls have begun child bearing by 19 years
SDG 2.2: End all forms of malnutrition and address the nutritional needs of adolescent girls, pregnant and lactating women and children
50 per 1000 girls 15‐19 years
Adolescent Mortality Rate
‐
Source:‐ Levels & Trends in Child mortality ‐ Report 2015: Estimates Developed by the UN Inter‐agency Group for Child Mortality Estimation: Trends in maternal mortality: 1990 to 2015: estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division: World Health Statistics, WHO Publication, 2016.

23
Timor Leste: Lessons learnt and key actions taken: (Observations by Sujeewa Amarasena) Timor‐Leste started with very high maternal and child mortality, which many thought was
impossible to tackle. But a high degree of political will, initiatives to strengthen the health
system and evidence‐based interventions taken to scale, to reach every woman ever child, have
led to dramatic reductions in maternal and child mortality, and ultimately helping them achieve
MDGs 4 and 5.
Since 2000 the Government has publicized its commitment to the MDGs 4 and 5, and
demonstrated very positive improvements.
Increased coverage of skilled care at birth and institutional deliveries
Improved quality of care around childbirth, including resuscitation
Strengthened management of preterm labour and preterm babies
Improved essential newborn care, and early postnatal care at home
Strengthened care of sick and small new‐borns in hospitals

24
Thailand Country has already achieved SDG targets
Maternal mortality ratio at 20 is less than SDG Target (70 per 100 000 live births)
Neonatal mortality at 7 is lower than the expected 12 per 1000 live births
Under‐5 mortality at 7 is already below 25 per 1000 live births
Lessons from Thailand’s success: (Observations by Sawasdivorn Siraporn)
1. Successful centralized health care coverage plan must be made at the central level but
implemented at the local level
2. Coordination of planning and utilization of human resources must consider both providing
health services (demand) and training qualify health care personnel (supply)
3. Owing to conscious capacity building on health care financing, Thailand gradually moved
from an out of pocket payment to a prepayment system

25
Annex 2
SEA/RC69/R3
ENDING PREVENTABLE MATERNAL, NEWBORN AND CHILD MORTALITY IN THE SOUTH‐EAST ASIA
REGION IN LINE WITH THE SUSTAINABLE DEVELOPMENT GOALS (SDGS) AND GLOBAL STRATEGY ON WOMEN’S, CHILDREN’S AND ADOLESCENTS’ HEALTH
The Regional Committee, Recalling its resolutions SEA/RC53/R9 on Maternal mortality, SEA/RC56/R9 on Health of the
newborn1 and SEA/RC58/R2 on Skilled care at every birth, as well as the recent World Health Assembly resolution WHA69.2 on Committing to implementation of the Global Strategy for Women’s, Children’s and Adolescents’ Health. Newborn period is first 28 days of life after birth
Recognizing the significant progress made towards achieving MDGs 4 and 5 in countries of the South‐East Asia Region with a regional decline in child mortality rate of 64% and a decline of 69% in the maternal mortality ratio, between 1990 and 2015, and the need to further build upon these achievements,
Noting that these figures fall short of the MDG targets of a two thirds reduction in child mortality and a three fourths reduction in maternal mortality, and that neonatal mortality has declined less rapidly than child mortality, that there are significant disparities in achievements across and within countries, and that maternal, newborn and child mortality continue to remain high in some countries in the Region,
Acknowledging that the UN Secretary‐General’s Global Strategy on Women’s, Children’s and Adolescents’ Health (2016‐2030), and the Sustainable Development Goals provide new opportunities and have set new targets for countries on reducing maternal mortality and ending preventable, newborn and child deaths, Further acknowledging that Universal Health Coverage is the overarching umbrella for taking forward the SDG Goal 3 on health, and that the SDGs provide an excellent framework to accelerate efforts to narrow equity gaps in accessing quality care, ensure adequate health financing and sufficient numbers and appropriate skill‐mix and deployment of health workforce,
Appreciating the Regional Flagship Priority on ending preventable maternal, newborn and child mortality with a focus on newborn deaths, and the partnership commitment as exemplified by the joint statement by H6 agencies (WHO, UNICEF, UNFPA, UNAIDS, UN WOMEN and World Bank) on ending preventable maternal, newborn and child mortality,
Considering that this resolution supersedes the three previous resolutions on related subjects namely, SEA/RC53/R9, SEA/RC56/R9 and SEA/RC58/R2;
1. URGES Member States: a) To achieve universal access to and coverage of essential intervention packages for reproductive, maternal, newborn, child and adolescent health (RMNCAH) across the continuum of care, with focus on good quality care of mothers and newborns at the time of childbirth and, including mothers and newborns with risks and complications, b) To review and strengthen national health systems, as appropriate, to identify gaps and solutions in relation to the needs of RMNCAH, including by investing in midwifery skills and development of sustainable health financing mechanisms to reduce out‐of‐pocket expenses for safe child birth and care of mothers and newborns, c) To strengthen the quality and use of data for programme improvement in line with the indicators and disaggregation in the SDGs and Global Strategy including still births and cause of death related to maternal, neonatal, child and adolescent health, and

26
d) To reinforce multisectoral and multi‐stakeholder partnerships and commitments to address underlying social determinants of women’s, children’s and adolescents’ health such as early marriage2, nutrition, education, poverty, water‐sanitation, and to promote early childhood development, 2. REQUESTS the Regional Director: a) To intensify technical collaboration with, and support to, Member States to update their national RMNCAH strategies and plans to address the coverage gaps for essential interventions for RMNCAH, with specific guidance on organizing, planning and setting up quality services for child birth and newborn care, b) To support Member States to strengthen the quality and use of data for programme improvement in line with the indicators and disaggregation in the SDGs and Global Strategy including still births and cause of death related to maternal, neonatal, child and adolescent health, c) To support Member States, upon request, for developing national RMNCAH investment case3and encourage adequate national and international investments for ending preventable maternal, newborn and child mortality and improving health and wellbeing of women, children and adolescents, and d) To report progress on implementation of this resolution to the Regional Committee in 2018, 2022, 2026 and 2030.
9 September 2016

27
Annex 3
SEAR TAG Meeting December 2015‐ Overarching recommendations
(1) WHO to secure the buy‐in to the recommendations from all the national governments through the
Regional Committee deliberations on Women’s, Children’s and Adolescents Health, with a focus on
reduction in newborn mortality in September 2016.
(2) To facilitate dissemination, buy‐in and adoption of the recommendations in countries, countries
should be encouraged to replicate the Regional TAG, through national processes, e.g. multi‐speciality
National Task Force. Each country is encouraged to undertake a strategic consultation with the support of
H4+ and partners in the country.
‐ Countries to create/strengthen National Task Force or similar mechanism and share progress at the next
SEAR‐TAG meeting.
(3) Countries to focus on expansion of good quality care for mothers and new‐borns around the time of
childbirth (including late antenatal care) and first few days thereafter including facility‐based and home‐
based care of small and sick babies.
‐ Countries to prioritize this and operationalize plans e.g. within ENAP immediately and share progress at
the next SEARTAG meeting.
(4) WHO to inform the intervention packages that will be required for reducing the NMR to low levels of
12 per 1000 live births or less (secondary and tertiary care and other interventions).
(5) WHO, UNH4+ and partners to support high priority countries for development of investment cases, to
engage with Global Finance Facility and mobilise domestic resources for RMNCAH.
‐ WHO, UNH4+ and partners to prepare a strategic approach and support country level dialogue for
development of investment cases in 2‐3 priority countries in 2016
(6) WHO with H4+ to create a SEAR web‐based repository of best practices in RMNCAH and increase
opportunities for cross learning and share innovative experiences.
‐ WHO with UNH4+ to create SEAR repository and inform of progress.

28
Annex 4
List of Participants
SEAR‐TAG Members
1. Vinod Paul: Chair
2. Nozer Sheriar (India)
3. Mohammad Baharuddin Hasanudin (Indonesia)
4. Katherine Ba‐Thike (Myanmar)
5. Dharma Saran Manandhar (Nepal)
6. Sujeewa Amarasena (Sri Lanka)
7. Siraporn Sawasdivorn (Thailand)
8. Wendy Graham (connected through skype)
H6 Partners:
1. UNCEF ROSA: Sufang Guo
2. UNICEF EAPRO: Kyoko Shimamoto
3. UNFPA: Wame Baravilala
4. UN WOMEN: Ms Subhalakshmi Nandi
5. World Bank: Dr Sheena Chhabra
Consultants:
1. Elizabeth Mason
2. Bruce Dick
3. Krishna Bose
Secretariat (WHO Regional Offic3):
1. Pem Namgyal, Director, Family Health, Life Course and Gender
2. Neena Raina, Coordinator, Health Through Life Course
3. Rajesh Mehta, Medical Officer, Child and Adolescent Health
4. Neelamani Hewageegana, Maternal and Reproductive Health
5. Priya Karna, Junior Public Health Professional

29
Annex 5
Programme 1. Opening Session
2. Progress in implementation of TAG recommendations
Report on implementation
Perspective from H6 agencies 3. Maternal Health: Finishing the MDG5 work
Maternal Health ‐ Lancet Series
Regional situation
Country‐specific Reflections: (Bangladesh, India, Indonesia, Myanmar, Nepal, TLS)
Recommendations for regional and country level actions
4. Child Health: Finishing the MDG4 work
Regional situation
Child Health‐ Strategic Review
Country‐specific Reflections: (Bangladesh, India, Indonesia, Myanmar, Nepal, TLS)
Recommendations for regional and country level actions
5. Regional strategic guidance on Adolescent Health
Setting the stage for new regional priority
6. Global Strategy:
New and under‐focused areas and country implications
7. Monitoring Global Strategy and SDG3: Regional and Country
8. Plan for the next TAG Meeting (2017)
9. Conclusion of the meeting