Final 2009 m sc thesis oliver vit cv
111
Oral MS therapy The coming revolution by Oliver Vit A CONFIDENTIAL DISSERTATION SUBMITTED IN PARTIAL FULFILMENT OF THE REQUIREMENTS FOR A MASTER’S DEGREE IN CLINICAL DRUG DEVELOPMENT (MSc in Clinical Drug Development) Queen Mary’s School of Medicine and Dentistry 2009
-
Upload
oliver-vit -
Category
Documents
-
view
301 -
download
0
Transcript of Final 2009 m sc thesis oliver vit cv

Oral MS therapy
The coming revolution
by
Oliver Vit
A CONFIDENTIAL DISSERTATION SUBMITTED IN PARTIAL FULFILMENT OF THE
REQUIREMENTS FOR A MASTER’S DEGREE IN CLINICAL DRUG DEVELOPMENT
(MSc in Clinical Drug Development)
Queen Mary’s School of Medicine and Dentistry
2009


i
Abstract
This dissertation reviews the oral therapies currently being developed for the treatment of
Multiple Sclerosis based on their strengths, weaknesses, opportunities, relative threats, and
predicts changes to the current market which can be expected upon respective launches.
Methods: A systematic review of publicly available information was initiated in an effort to
identify potential candidates and then to define the Mechanism of Action (MoA), the clinical
development plan (CDP) and the duration of market exclusivity. Where information
concerning the CDP or market exclusivity was found to be lacking, standard assumptions were
used to extrapolate forwards.
Results: No less than 11 candidates were identified across 4 separate MoAs spanning
clinical development phases from Phase I to registration: cladribine, teriflunomide, laquinimod,
fingolimod, BAF312, ACT-128800, CS-0777, ONO 4641, BG-12, Firategrast, CDP-323.
Conclusions: In 2010 Mylinax® (cladribine) and fingolimod will be the first oral therapies
ever launched to treat RRMS. MS therapy will adapt to the coming oral revolution according
to (1) time of approval (2) the risk:benefit profile each MS subtype supports, (3) the degree of
confidence neurologists acquire with these new agents, and (4) direct demands of MS patients
for convenient, efficacious and safe treatment of their disorder. Combination therapy will

ii
return however restricted to fringe use due to limited expectations and experience. Following
the launch in RRMS, Mylinax® and fingolimod will continue to expand into suspected early
stage MS (CIS) and progressive forms of MS (PPMS/SPMS) respectively. A 2nd wave of orals
consisting of teriflunomide, laquinimod and BG-12 may arrive in the market between 2013-
2014. This will be followed by BAF-312, ACT-128800 and firategrast in a 3rd wave offering a
range of additional differentiation in terms of both efficacy & safety which may arrive by 2017
well in advance of the 1st oral to lose IP protection (fingolimod in 2019).
Clever integration of MRI techniques along with monitoring of biomarkers and potentially
genetic screening may help to change the understanding of MS, its progression and the
therapeutic paradigm. Cost effectiveness as well as patient access will drive further
differentiation between clinically non-differentiated products. Biologics will suffer a dual
pronged assault from lower priced biosimilars and new oral agents as patent expiry and
competition from bio-similars looms; however the market will continue to support innovative
high priced therapy. Continued research into the non-inflammatory component of MS holds
the key to the next revolution.

iii
Table of Contents
Figures vi
Tables ix
INTRODUCTION
Etiology 1
Diagnostic tools 7
Current therapy 14
METHODS 19
RESULTS
Oral MS therapies; competitive environment 21
Anti-proliferative/replicant 23
Cladribine 23
Teriflunomide 32
S1P receptor agonists 37
Fingolimod 40
BAF312 55

iv
ACT-128800 60
CS-0777 63
ONO 4641 67
Up and coming S1P agonists 67
Nrf2 activation 69
BG-12 69
α4-integrin antagonists 74
Laquinimod 75
Firategrast 80
CDP-323 81
MS biologics; global market
Annual revenues 82
Market capitalization 83
Market exclusivity 84

v
DISCUSSION
(Mylinax®) Cladribine 86
Teriflunomide 88
Fingolimod 89
BAF312 90
ACT-128800 91
CS-0777 91
BG-12 92
Laquinimod 93
Firategrast 93
CONCLUSION 94
REFERENCES 99

vi
Figures
Figure 1 MS Disease subtypes p.3
Figure 2 Benign MS p.5
Figure 3 MS subtype segmentation p.5
Figure 4 MS subtype segmentation as reported by neurologists (USA) p.6
Figure 5 MS subtype segmentation as reported by patients p.6
Figure 6 MRI scans of T1 & T2 lesions with & without GD+ enhancement p.9
Figure 7 Full EDSS scoring p.11
Figure 8 EDSS scoring as shared with the patient p.12
Figure 9 Pipeline; oral MS agents in Phase II/III p.21
Figure 10 Competitive radar; oral MS agents p.22
Figure 11 Cladribine; chemical structure p.24
Figure 12 Cladribine MS development plan p.24
Figure 13 CLARITY trial design p.26
Figure 14 CLARITY; relapse rates at 2-years p.27
Figure 15 CLARITY; disease progression at 2-years p.27
Figure 16 Cladribine; selective reduction of lymphocytes p.29
Figure 17 Cladribine; registry trial design p.30
Figure 18 Teriflunomide & leflunomide; chemical structures p.32
Figure 19 Teriflunomide MS development plan p.33

vii
Figure 20 HMR1726D-2001 trial design p.34
Figure 21 Teriflunomide; combined unique lesions at 9-months p.35
Figure 22 Ceramide; generic chemical structure p.38
Figure 23 Sphingolipid biosynthetic pathway p.38
Figure 24 Fingolimod; parent and phosporylated metabolite p.40
Figure 25 Fingolimod MS development plan p.41
Figure 26 Fingolimod; SAD on top of Neoral® in renal transplant patients p.42
Figure 27 Fingolimod; SAD lymphocyte reductions p.42
Figure 28 Fingolimod; SAD Bradycardic effects p.43
Figure 29 Fingolimod; Phase IIb trial design p.44
Figure 30 Fingolimod; Phase IIb results at 6-months p.46
Figure 31 Fingolimod; tolerability profile at 6-months p.46
Figure 32 TRANSFORMS trial design p.48
Figure 33 Fingolimod; time to first confirmed relapse in 2-year extension study p.50
Figure 34 FREEDOMS I&II trial design p.52
Figure 35 Fingolimod; relapse rate at 2-years in FREEDOMS p.53
Figure 36 Fingolimod; disease progression at 2-years in FREEDOMS p.53
Figure 37 Fingolimod; Serious Adverse Events reported in FREEDOMS p.54
Figure 38 BAF312 MS development plan p.56
Figure 39 BAF312; BOLD trial design p.57
Figure 40 Mean Ventricular Heart Rate following administration of BAF312 p.58

viii
Figure 41 Absolute lymphocyte count reductions following administration of
BAF312
p.59
Figure 42 ACT-128800; SAD pharmacokinetics p.61
Figure 43 ACT-128800; SAD mean lymphocyte count reductions following
single administration
p.61
Figure 44 ACT-128800; SAD mean %Δ in lymphocyte count following single
administration
p.62
Figure 45 CS-0777P; SAD pharmacokinetics p.64
Figure 46 CS-0777; SAD reduction of lymphocyte sub-populations p.64
Figure 47 CS-0777; SAD peripheral lymphocyte counts p.65
Figure 48 CS-0777; Alanine aminotransferase levels p.65
Figure 49 CS-077-A-U102 trial design p.66
Figure 50 BG-12 MS development plan p.70
Figure 51 BG-12; Phase IIb MS trial design p.71
Figure 52 BG-12; Phase IIb GD+ enhanced lesions at 6-months p.72
Figure 53 Laquinimod; chemical structure p.75
Figure 54 Laquinimod MS development plan p.76
Figure 55 LAQ/5062 trial design p.77
Figure 56 Laquinimod; reduction of T1 GD+ enhanced lesions at 9-months p.78
Figure 57 Firategrast MS development plan p.80
Figure 58 Biologic MS therapy; annual revenues 2006-2008 p.82
Figure 59 Biologic MS therapy; market share 2006-2008 p.83

ix
Tables
Table I Biomarkers in Multiple Sclerosis p.13
Table II Properties of sphingosine-1-phosphates p.39
Table III CS-0777P; comparative S1P receptor selectivity p.63
Table IV Phase 0 development of S1P agonists p.68
Table V Protection of MS agents in clinical development (EU) p.85
Table VI Protection of MS agents in clinical development (US) p.85
Table VII Drug development success rates p.97

Page 1
INTRODUCTION
Etiology
Jean-Martin Charcot was the first physician to discover the lesions in both the brain’s white
matter and spinal cord upon autopsy, and named the disorder Multiple Sclerosis (MS) after
the localized & numerous scars he observed. Since 1868 strides have been made in the
diagnosis and treatment of MS in its varying degrees of severity, however the root cause of
the disorder remains unknown. MS is an autoimmune disorder in which trafficking
lymphocytes gain access to the normally immuno-privileged Central Nervous System (CNS)
following a primary insult to the blood-brain barrier (BBB) and permanent disability
accumulates following increased incidents of demyelination & eventual neuronal loss.
Inflammation plays a role in the earlier stages of the disease hence so it is speculated that as
a precursor to lymphatic attack lymphocytes encounter environmental antigens in the thymus
and incorrectly prime the immune system to falsely identify the myelin sheath as an external
threat to the body. Although not a hereditary disorder, genetic variations may leave certain
individuals more susceptible; likewise it has also been postulated that exposure to foreign
microbes such as the Epstein-Barr virus (EBV) may instigate MS [1][2].
Irrespective of the primary impetus, improperly conditioned T cells cross a compromised
blood-brain barrier (BBB) in the course of immuno-surveillance, attach to the myelin sheath
and release a cytokine cascade recruiting macrophages both from circulating blood and
locally in the form of microglials, inducing an incorrect onslaught against an axon’s
protective myelin sheath. The cytokines released by T cells are also suspect in recruiting and
activating local B cells which then promote an independent B cell attack [3]. Composed
primarily of lipids, the myelin surrounds and insulates a neuron’s elongated axon along
which electric stimuli travel. The brain’s white matter is comprised largely of neurons and

Page 2
the loss of the myelin sheath often results in the loss of conducting impulses and the
associated function, e.g. loss of gross & fine motor skills, speech, cognitive abilities, etc.
The more progressive subtypes of MS are characterized by a decreased inflammatory
component along with continual mounting neuronal degeneration & loss associated with
increased disability. Although MS is not fatal and does not significantly diminish the
average life-expectancy, progressive accumulation of disability incapacitates the afflicted
slowly stripping them of their cognitive abilities and mobility which eventually renders them
mute, disassociated from society and entirely dependent upon the care of others.
The incidence of MS is known to rise with increasing geographical latitude. Relapsing forms
of the disease most frequently affect young Caucasian females who reside within
industrialized nations. Prevalence has been estimated to be between 2 and 150 cases per
100,000 individuals [4].
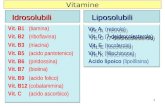
The US National Multiple Sclerosis Society (NMSS) defined four distinct subtypes of MS
based on the frequency of relapses driven by repeated inflammatory attacks and the pattern
of accumulation of permanent disability. These are referred to as Relapsing-remitting MS
(RRMS), Secondary Progressive MS (SPMS), Primary Progressive MS (PPMS) and
Progressive-relapsing (PRMS). Figure 1 depicts these four categories.

Page 3
Figure 1 – MS Disease subtypes Source: US National MS Society

Page 4
Relapsing-remitting MS (RRMS) By far the most common form of MS accounting for upwards of 80% of new diagnoses,
relapsing-remitting MS is characterized by distinct neurological disturbances followed by
periods of relative calm with potentially a temporal return of lost function alongside an
underlying gradual accumulation of permanent disability over time; patients are usually
women 20-40 years of age.
Progressive-relapsing MS (PRMS) Patients who suffer repetitive exacerbations of escalating severity & disability separated by
periods of remission are diagnosed with progressive-relapsing MS.
Secondary progressive MS (SPMS) After 10-20 years a RRMS patient who no longer experiences periods of remission between
symptomatic exacerbations of escalating severity is said to have advanced to secondary
progressive MS.
Primary progressive MS (PPMS) A continuous and steady loss of function not associated with intermittent exacerbations is
referred to primary progressive MS; patients of both sexes are equally affected and typically
middle aged.
In addition to the MS subtypes categories provided by the US National MS Society, so called
“benign” MS and clinically isolated syndrome (CIS) are frequently used terms.
“Benign” MS Patients diagnosed with benign MS experience irregular, sporadic attacks of variable
magnitude similar to RRMS which however do not result in the accumulation of disability
over time. See Figure 2.

Page 5
Figure 2 – Benign MS Adapted from: www.imaginginformatics.ca
Clinically isolated syndrome (CIS)
A diagnosis of CIS is based on the report of a neurological attack of at least 24 hours in
duration associated with MRI abnormalities suggestive of inflammatory demyelination. A
diagnosis of Clinically Definite MS (CDMS) cannot be ascertained as the occurrence and
location of lesions across both time and space remains uncertain, i.e. in the absence of a
relapse, the risk to subsequently develop CDMS is significantly higher than the general
population. This circumstance is defined as CIS.
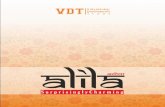
Figure 3 illustrates the distribution of MS subtypes as assessed by Net Resources
International. Figure 4 is assembled from a recent market research exercise conducted by
Decision Resources with 102 practicing neurologists in the United States of America.
Figure 5 represents how patients on a popular internet forum supported by <13,000 patients
classify themselves, albeit skewed by the fact that the responders’ condition permits internet
interaction.
Figure 3 – MS subtype segmentation Source: Drug Development Technology (2007)

Page 6
20% 19%
46%
15%
Figure 4 – MS subtype segmentation as reported by neurologists (USA) Source: Decision Resources (2009)
Figure 5 – MS subtype segmentation as reported by patients Source: www.patientslikeme.com
It is noteworthy that none of the three exercises used the same nomenclature when
approaching segmentation, and when there is overlap in the classification, e.g. RR MS, SP
MS, PP MS, the reported percentiles vary widely. Most significant is perhaps that 21% of
the patients who being internet active are most likely to have familiarized themselves with
their condition, are in fact unable to identify the MS subtype which afflicts them. Outside of
clinical parameters & measures little else in the MS community appears standard.
CIS
RR-MS
SP-MS
PP-MS
MS Population Breakdown By Subtype
20% 19%
46%
15%
CIS
RR-MS
SP-MS
PP-MS
MS Population Breakdown By Subtype

Page 7
Diagnostic tools
The signs and symptoms are varied and include any of the following alone or in
combination: loss of cognitive skills, loss of bladder control, fatigue, nystagmus, restricted or
loss of mobility, optic neuritis, pain, trigeminal neuralgia, Lhermitte’s sign, dysesthesias,
sexual dysfunction, spasticity, transverse myelitis, tremor and alaxia. A patient presenting
with one or more of these first signs symptomatic of MS may indeed be suffering from any
number of peripheral neuropathies, autoimmune disorders, demyelinating disorders, or in
fact nothing at all. The initial diagnosis of MS in any of its forms will be often difficult at
the start due to the vague, mild and transient nature of the symptoms, however no other
disease of the central nervous system (CNS) entirely mimics the debilitating progressive
assault of MS; progressive accumulated disability over time remains the decisive factor in
diagnosing MS.
McDonald criteria
The McDonald criteria were universally accepted by the US NMSS in 2001 and replaced
both Poser and Schumacher diagnostic criteria. Utilizing the knowledge gleaned from
decades of experience with both increasingly sensitive instrumentation and the disease itself,
the McDonald criteria make use of a description & frequency of attacks as reported by the
patient, the total number & dissemination in space and time of lesions detected with
magnetic resonance imaging (MRI) as well as the results from cerebrospinal fluid samples
(CSF) to diagnose the subtype of MS. The presence of multiple oligoclonal bands in CSF
samples is indicative of a recent or ongoing CNS inflammation inclusive of MS.

Page 8
Magnetic resonance imaging (MRI)
Hydrogen atoms when bound to oxygen produce water; however as the electrons are
unevenly distributed in covalent bonds favoring the oxygen atom and neutrons are not
present in the hydrogen nucleus, the two oxygen-bound hydrogen atoms in a molecule of
H20 behave very much like exposed protons. Aligning the nuclear magnetization of these
protons in the body with a strong magnetic field allows for precise interstitial images to be
taken. These are referred to as MRI scans and have proven invaluable to the diagnosis and
management of MS. MRIs allow practicing neurologists to evaluate the number, size, and
distribution of CNS lesions over time and so determine the extent and severity of the
inflammatory process throughout the lifetime of a MS patient.
The two types of MRI scan commonly used are called T1 and T2 scans. T1 imaging uses
gradient echo to maintain a <90° partial flip angle which allows for faster recovery of NMR
signal with a shorter Repetition time (TR)/ Echo time (TE); images taken within split second
of each other at varying degrees of magnetism can then be taken to produce a composite
image of higher resolution. This allows for better identification of edema and/or sites of
areas of extreme white matter loss otherwise referred to as “black holes”. T2 imaging makes
use of a longer TR/TE via two consecutive pulses prior to detection to refocus the
magnetization by 180° in a process called spin echo; as disturbances in the magnetic field are
lost by spin echo, the MRI resolution is thus enhanced. T2 imaging better identifies
inflammatory sites such as active lesions in the brain. Gadolinium (Gd+) is a contrast agent
which greatly increases MRI resolution of both T1 and T2 images.
Figure 6 illustrates the difference between axial T1 and T2 images with and without Gd+
enhancement.

Page 9
Figure 6– MRI scans of T1 & T2 lesions with & without GD+ enhancement Source: Frey et al., 1999. Clinical Application of MRI Image Processing in Neurology, International Journal of Bioelectromagnitism, 1 (1)
Up to 80% of lesions detected on MRI scans may in fact be clinically silent [5]. MRI scans
are unable to detect axonal loss & neural degeneration, or sub-cortical demyelination of the
grey matter. Furthermore the utility as a predictive measure of eventual disability is
questionable as MRI scans are less sensitive to spinal lesions. Irrespective of these
drawbacks MRI scans are currently one of the best diagnostic tools at a neurologist’s
disposal.

Page 10
Annualized Relapse Rate (ARR)
A relapse is defined as a new neurological symptom or a worsening of a pre-existing
neurological condition whose duration is longer than 24 hours. Often used as a measure of
an agent’s efficacy, the annualized relapse rate (ARR) is simply the mean number of
reported clinical exacerbations over the mean time, hence it can be used for periods of less
than one year.
Expanded Disability Status Score (EDSS)
The Kurzke Expanded Disability Status Score (EDSS) was developed in 1983 to assist the
neurologist in quantifying the degree of disability in a given functional system (FS) for any
given MS patient. It divides the body into the following eight functional systems (FS):
pyramidal, cerebellar, brainstem, sensory, bowel & bladder, visual, cerebral, other. The
neurologist then assesses each FS on a scale from 0 (perfectly functional) to 10 (death) in a
series of 20 half steps. This is a commonly used disability score which in conjunction with
MRI scans helps to determine the progression of MS and the appropriate therapy. Figures 7
& 8 illustrate the full EDSS score from 0-10 and the EDSS score from 0-9 as explained to
patients & their families respectively.

Page 11
1.0: No disability, minimal signs on 1 FS
1.5: No disability, minimal signs on 2 of 7 FS
2.0: Minimal disability in 1 of 7 FS
2.5: Minimal disability in 2 FS
3.0: Moderate disability in 1 FS; or mild disability in 3 - 4 FS, though fully ambulatory
3.5: Fully ambulatory but with moderate disability in 1 FS and mild disability in 1 or 2 FS; or moderate disability in 2 FS; or mild disability in 5 FS
4.0: Fully ambulatory without aid, up and about 12hrs a day despite relatively severe disability. Able to walk without aid 500 meters
4.5: Fully ambulatory without aid, up and about much of day, able to work a full day, may otherwise have some limitations of full activity or require minimal assistance. Relatively severe disability. Able to walk without aid 300 meters
5.0: Ambulatory without aid for about 200 meters. Disability impairs full daily activities
5.5: Ambulatory for 100 meters, disability precludes full daily activities
6.0: Intermittent or unilateral constant assistance (cane, crutch or brace) required to walk 100 meters with or without resting
6.5: Constant bilateral support (cane, crutch or braces) required to walk 20 meters without resting
7.0: Unable to walk beyond 5 meters even with aid, essentially restricted to wheelchair, wheels self, transfers alone; active in wheelchair about 12 hours a day
7.5: Unable to take more than a few steps, restricted to wheelchair, may need aid to transfer; wheels self, but may require motorized chair for full day's activities
8.0: Essentially restricted to bed, chair, or wheelchair, but may be out of bed much of the day; retains self care functions, generally effective use of arms
8.5: Essentially restricted to bed much of the day, some effective use of arms, retains some self care functions
9.0: Helpless bed patient, can communicate and eat
9.5: Unable to communicate effectively or eat/swallow
10.0: Death due to MS
Figure 7 – Full EDSS scoring Source: http://www.mult-sclerosis.org/expandeddisabilitystatusscale.html.

Page 12
Figure 8 – EDSS scoring as shared with the patient Source: https://www.msactivesource.com 0.0: Normal Neurological Exam Multiple Sclerosis Functional Composite (MSFC)
In 1994 the US NMSS commissioned a task force to standardize the clinical evaluation of
the natural disease progression across meaningful parameters for use in clinical trials. It was
to be multidimensional to reflect the changes an MS patient undergoes over time, scoring of
each parameter was to be independent of any other parameters measured and cognitive
function was to be one of the parameters. In 1995 the results were made public and MSFC
was composed of three components: leg function/ambulation, arm/hand function and
cognitive function. First approved in 1995 the MSFC disability scoring tool has yet to
replace EDSS as a standard clinical endpoint in large registration trials despite favorable
reports from practicing neurologists [5].

Page 13
Biomarkers
Given the uncertainties associated with the etiology of MS, the genetic & environmental
factors which may predispose individuals to developing MS, the silent debilitating &
variable disease progression, and the ability of the current tools to properly diagnose,
monitor & support proactive treatment regimens, biomarkers are of particular interest. To
date no single biomarker has been successfully coupled with a specific outcome in MS;
however this precludes neither exploratory clinical research with existing biomarkers nor
further investigations in search of novel and predictive biomarkers. Table I summarizes
those biomarkers already identified and their potential significance towards diagnosis &
disease progression. Although more hazardous to procure, biomarkers found in the
cerebrospinal fluid (CSF) are more attractive than those acquired from the blood as the
samples are specifically reflective of the CNS environment.
Table I – Biomarkers in Multiple Sclerosis
Epstein-Barr Virus
(EBV)
Significantly higher levels of EBV antibodies found in MS patients as opposed to the populous at large
Blood serum TOBI Gene encoding transition factor responsible for the repression of T-cell proliferation; significantly down-regulated in CIS patients susceptible to rapid conversion to CDMS
Oligoclonal bands Immunoglobulins associated with active inflammation; subtraction of oligoclonal bands found in blood serum from those found in CSF indicates production within the CNS and along with MRI outcomes serves as a traditional MS diagnosis measure
Cytokines Pro & anti-inflammatory
Chemokines Regulate T&B cell recruitment to sites of active inflammation; not specific to MS
NO/NOS levels Indicative of increased oxidative stress, inflammatory activity & BBB breakdown
Cerebrospinal fluid
Fetuin-A Immune system regulatory protein; high levels in CSF are associated directly with demyelination & active MS
Adapted from: Harris and Sadiq, 2009, Disease Biomarkers in MS, Molecular Diagnosis & Therapy, 13 (4) p.225-244

Page 14
Current therapy
Intravenous corticosteroids are commonly used to relieve the localized swelling and pain of
acute inflammatory attacks and reduce the potential for accumulating further disability upon
remission. MS patients who have received a 3-5 day course of methylprednisolone often
rapidly regain function; unfortunately this improvement is usually not maintained and there
is no evidence that corticosteroids reduce the long-term risks of eventual relapse. Disease
modifying therapies (DMTs) are largely confined to injectable biologics targeting surface
proteins on lymphocytes which either impede the inflammatory cytokine cascade, adhesion
to endothelium & trafficking through the vascular wall or induce selective lysis of T cells.
All DMTs demonstrate varying degrees of increasing efficacy offset by escalating safety
concerns. Novantrone® is also used in MS patients who fail to respond to treatment with
traditional DMTs.
Betaferon® (interferon β-1b)
Betaferon® was the first non-steroidal DMT developed by Schering AG approved for MS
therapy; it was licensed in July 1993 indicated for use in reducing the frequency of clinical
exacerbations in relapsing forms of MS. Betaferon® is manufactured ex-vivo using
Escherichia coli. It mimics natural cytokines, cell signaling proteins released by
lymphocytes, which have been linked to the enhancement of suppressor T cell activity,
reduction of pro-inflammatory cytokine production, down-regulation of antigen presentation,
and inhibition of lymphocyte trafficking into the central nervous system (CNS) by improving
the integrity of the BBB. The Mechanism of Action (MoA) which provides direct benefit to
MS patients remains unknown. At 2-years, injections every other day with 0.25 mg
Betaferon® yielded a 32% reduction in Annualized Relapse Rate compared to placebo and

Page 15
no statistically significant reduction in disease progression as measured by EDSS.
Neutralizing antibodies (NABs) do develop over time. Side effects include injection site
reactions/necrosis and flu-like symptoms following administration. The current market
formulation is packaged as pre-filled syringes and commercialized by Novartis.
Copaxone® (glatiramer acetate) Glatiramer acetate was first licensed by Teva Pharmaceuticals in December 1996 as
Copaxone® for use in reducing the frequency of relapses in RRMS patients. Although the
MoA remains unknown it is likely that the chemical structure of glatiramer acetate mimics
that of myelin and so like a decoy circulating T cells bind to it rather than the protective
myelin. Copaxone® has been shown to have a modest effect of reducing the relapse rate
(~30% reduction) and delaying disease progression at 2-years compared to placebo.
However recent data has demonstrated that there may be significant benefit offered to
interferon-1β monotherapy treatment failures [7]. It is provided as a pre-filled syringe and
delivered via a daily 20 mg subcutaneous injection. NABs are known to develop with
repeated long-term use in almost all patients. The most common adverse events associated
with use are injection site reactions, vasodilatation, chest pain, asthenia, infection, pain,
nausea, arthralgia, anxiety, and hypertonia.
Avonex® (interferon β-1a)
Recombinant DNA techniques using Chinese Hamster Ovarian cells allowed Biogen Idec to
develop the first interferonβ-1a biologic, Avonex®. At 2-years 30 μg Avonex® delivered
once weekly via intramuscular injection demonstrated only an 18% reduction in ARR
compared to placebo; however Avonex® did achieve a relative 37% reduction in disability
progression. In May 1996 it was the first to be granted a license for reducing the frequency

Page 16
of clinical exacerbations and delay the accumulation of physical disability in relapsing MS
patients. In later clinical trials Avonex® was associated with up to a 38% reduction in ARR;
Avonex®’s increased efficacy is attributed to its ability to greatly improve the integrity of
the BBB as demonstrated in preclinical animal investigations. As with Copaxone® and
Betaseron® NABs develop over time, it is marketed as a pre-filled syringe and injection site
reactions/necrosis & flu-like symptoms upon administration persist along with anemia, fever,
chills, and muscle ache. However unlike all the rest, Avonex® is the market leader
accounting for 25-30% of market capitalization.
Rebif® (interferon β-1a)
Also manufactured using genetically engineered Chinese Hamster Ovarian cells Serono’s
Rebif® was the 3rd biologic developed for use in MS. At 2-years 44 μg delivered 3 times
weekly by subcutaneous injection demonstrated a 32% in annualized relapse rates and a 30%
reduction in disability progression against placebo. Furthermore in a second 6-month
clinical trial against Avonex® an absolute difference in ARR of 12% in Rebif®’s favor
translated into a 32% reduced risk of relapse. In May 1998 it followed Avonex® to be
granted a license for reducing the frequency of clinical exacerbations and delay the
accumulation of physical disability in relapsing MS patients. As with all biologic therapy
NABs specific to Rebif® develop over time. Injection site reactions/necrosis, flu-like
symptoms following administration, leucopenia, and increased liver enzymes are the most
common side effects.

Page 17
Tysabri® (α4-integrin antagonist)
First developed by Élan and co-developed with Biogen Idec, Tysabri® (natalizumab) was
the first fully humanized monoclonal α4-integrin antibody specifically antagonizing the very
late adhesion-4 (VLA-4) surface protein which enables the T cells to identify & bind to
vascular VCAM-1 and pass through the vessel wall; in effect it hinders lymphocyte
trafficking across the BBB and intestinal wall protecting these organs from potential
autoimmune attack by rogue T cells. Tysabri® is delivered by a 300 mg monthly
intravenous infusion and established a remarkable 69% reduction in ARR and 42% reduced
disease progression as compared to placebo at 2-years in clinical trials. Although
humanization of the antibodies reduced the proportion of patients in whom NABs develop,
NABs indeed develop and reintroduction of Tysabri® in these patients can promote allergic
reactions. This was the first revolution in MS therapy since Avonex®. Tysabri® is
currently penetrating the market at an impressive rate. First licensed in November 2004 it
was briefly removed from the market from 2005 to 2006 due to isolated cases of progressive
multifocal leukoencephalopathy (PML). Tysabri® carries a black box warning regarding
PML and as well as warnings regarding its immunosuppressive effects in the label.
Campath® (anti-CD52)
First developed at Cambridge University’s Pathology department, Campath® (alemtuzumab)
is an anti-CD52 monoclonal antibody licensed for use in the clinical treatment of chronic
lymphocytic leukemia (CLL) and cutaneous T cell lymphoma (CTCL) which is used off-
label in progressive MS patients. Campath® agonizes the surface protein CD-52 present
only on mature T cells and selectively induces lysis. Delivery of Campath® via intravenous
infusion results in an immediate death of circulating T cells and therapy is both complicated

Page 18
& restricted to hospital use. However in CAMMS223 a Phase IIb RRMS trial, annual
treatment with Campath® achieved a 74% decrease in ARR and a 72% decrease in disability
progression at 3-years compared to traditional Rebif® twice weekly subcutaneous injections.
At present CARE-I & CARE-II two Phase III Rebif®-controlled trials are underway and
scheduled to complete in 2011 and 2012 respectively. However therapy with Campath® is
not without risk; serious and fatal cytopenias, infusion reactions & infections are black-box
warnings in the current CLL label and therefore Campath® is primarily the agent of last
resort currently reserved for off-label use in the progressive forms of MS. Furthermore the
marketing potential of Campath® is in question as the compound loses patent protection in
July 2011 and the use in MS patent filed in 2007 was recently rejected on grounds of lack of
novelty.
Novantrone® (mitoxantrone)
A cytotoxic in the form of a small synthetic antineoplastic anthracenedione, Novantrone® is
typically reserved for cancer therapy, however delivered as a quarterly 12 mg/m2 intravenous
infusion it has proven effective in reducing the ARR and disease progression in both
secondary progressive MS (SPMS) and relapsing-remitting MS (RRMS) patients. As a type
II topoisomerase inhibitor it enters all dividing cells and actively prevents DNA replication
& repair. Novantrone® carries a black box warning as a teratogen with fatal cardiotoxic
potential and requires left ventrical ejection fraction (LVEF) monitoring prior to every
administration.

Page 19
METHODS
Given the highly competitive and secretive nature of drug development, retrieving reliable
information regarding potential oral therapies for the use in the treatment of Multiple
Sclerosis (MS) is ridden with misinformation and false leads. To best determine the scope of
this investigation, a thorough review of publically available resources was conducted
inclusive of, but not limited to, listings on the FDA website www.clinicaltrials.gov, annual
reports & press releases of pharmaceutical enterprises, and patent applications & grantings.
Thereafter further efforts were made to elucidate the Mechanism of Action (MoA) and the
clinical development plan of each indentified candidate; the results were eventually compiled
and plotted by MoA & estimated launch date. Where relevant information was not released
the following estimations were applied:
• 6-months between last Phase I trial and the start of a Phase II program
• 1 Phase IIb dose-finding trial assessing MRI and ARR at 6-months at minimum with
1-year of recruitment and 2 months of data cleaning prior to database closure
• 9-months between a dose-finding trial and the start of a Phase III program
• 2 confirmatory registration trials assessing disability at 2-years staggered by 3-months
with 18-months of recruitment and 3 months of data cleaning prior to database closure
• 6-months to submit a Manufacturer’s Authority Application (MAA) from the time of
the last registration trial’s last patient last visit/last data collection point
• 1-year review by the 1st Health Authority (HA) to grant Marketing Authorization
(MA), unless an expedited review was granted in which case 6-months was assumed
• 3-months between the MA and 1st launch

Page 20
The risk:benefit of each candidate was evaluated on the grounds of released efficacy, safety
and tolerability results either in the form of sponsored publications in renowned scientific
journals, e.g. Nature, The Lancet, Neurology, etc., or from presentations given at equally
reputable international conferences, The European Committee for Treatment and Research in
Multiple Sclerosis (ECTRIMS), The American Academy of Neurology (AAN).
The current market potential was established by extracting the annual revenues of each
product licensed for the treatment of MS as reported in the 2006, 2007, 2008 annual reports
published by the authorized manufacturer. A patent search for each compound was
conducted and finally the extent and duration of intellectual property (IP) protection periods
in the EU were determined based on the known and approximated MA dates.

Page 21
Cladribine, Mylinax (MS), Leustatin® (HCL)
Fingolimod, FTY720
BG-12, BG00012, FAG-102, Panaclar® (psoriasis)
Laquinimod, ABR-215062
Teriflunomide, A-771726
CDP-323
Firategrast, SB-683699, T-0047
BAF312
RESULTS
Oral MS therapies; competitive environment
In a field crowded with expensive parenterals, oral administration appears wanting, however
the pipelines of many pharmaceutical firms are expanding with a plethora of potential oral
agents promising therapeutic benefit to MS patients across all subtypes. Figure 9 illustrates
the oral compounds in Phase II/III development and the respective corporate sponsors.
Figure 10 depicts all oral compounds in clinical development split by MoA, phase of
clinical development and estimated launch date.
Figure 9 – Pipeline; oral MS agents in Phase II/III

Page 22
Figure 10 – Competitive radar; oral MS agents

Page 23
Anti-proliferative/replicant
Cladribine
Developed in the late 1970’s at the Scripps Research Institute as a therapeutic agent in the
treatment of lymphomas, cladribine is an adenosine deaminase-resistant purine nucleoside
analogue which is intracellularly phosphorylated to form an active mononucleotide which
then interferes with cell metabolism and DNA repair & replication. As a cytotoxic,
cladribine actively suppresses DNA repair which leads to increased deoxyribonucleotide
levels. This state then signals the activation of polyadenosine diphosphate (ADP) ribose
polymerase which subsequently exhausts cellular nicotinamide adenine dinucleotide (NDA)
levels and leads to eventual apoptosis [8]. Cladribine has demonstrated a good
bioavailability. It has been purported to selectively target only subpopulations of
lymphocytes due to a unique intracellular circumstance in which levels of deoxycytidine
kinase (DCK), an enzyme responsible for phosphorylation of the parent compound, largely
outnumber deoxynucleotide dephosphorylating enzymes in T cells. In nearly all other cells
of the body these enzymes are roughly equal in number which results in a continual
dephosphyrlation of the prodrug and renders it inactive [8]. Cladribine crosses the blood-
brain barrier (BBB) and accumulates with cerebrospinal fluid (CSF) levels exceed plasma
concentrations by up to 25% [9].

Page 24
Figure 11 – Cladribine; chemical structure Source: http://journals.prous.com/journals/dof/20042903/html/df290253/images/113529.gif
Clinical Development
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
RRMS/SPMS Onward
Clarity
CIS MS Oracle
Biocomparison i.v./tablet
Figure 12 – Cladribine MS development plan
CPMS i.v.
RRMS s.c.
SPMS/PPMS s.c.
On top of Rebif
MAA MA LaunchMAA MA Launch

Page 25
The clinical development of cladribine has spanned decades, indications and corporations. It
debuted as an experimental intravenous infusion therapy for use in lymphomas in the 1980’s.
This was followed by the licensing of a formulation supporting administration via
subcutaneous injection in the treatment of hairy cell leukemia (HCL) by Ortho Biotech in the
early 1990’s. Its lymphopenic properties marked it as a candidate not only for lymphomas
but also for autoimmune disorders where the immune system is suspected of mounting
attacks against otherwise healthy tissues. The Scripps Research Institute conducted 3
moderately sized Phase II clinical trials in chronic progressive Multiple Sclerosis (CPMS),
relapsing-remitting Multiple Sclerosis (RRMS) and Secondary/Primary Progressive Multiple
Sclerosis (SPMS/PPMS) with parenteral cladribine delivered by intravenous infusion or
subcutaneous injection in a total of 229 patients between 1992 and 1997 [9]. Large scale
investigations were not undertaken until the development of an oral tablet formulation which
demonstrated good bioavailability with a t½ of 6-8 hours. Renal excretion accounts for
~50% of systemic clearance with 21-32% of that being unaltered parent compound [9].
However the lymphopenic effects of cladribine last far beyond the 3-4 days it takes for
systemic clearance to be achieved. This supports the dosing schedule of 2-4 cycles of five-
day treatment annually which Merck Serono has implemented in the CLARITY, ONWARD
and ORACLE trials.
Following the favorable results from a short bioequivalence study comparing the
pharmacokinetic (PK) and pharmacodynamic (PD) profiles of the new tablet formulation
against the intravenous infusion regimen, differing regimens of oral cladribine were
evaluated in the MS population. In January 2005 Merck Serono’s single registration,
placebo controlled 2-year trial began to recruit 1,326 RRMS patients; recruitment completed
22 months later and preliminary results were released in January 2009. Figure 13 illustrates
the CLARITY trial.

Page 26
Jan Nov2005 2009
Figure 13 – CLARITY trial design Adapted from: ECTRIMS poster, Sep 2009 Primary endpoint
• qualifying relapse rate at 2 years based on Kurtzke Functional System (KFS) score
Secondary endpoints
• proportion of relapse-free patients
• total number of T1 Gd+ enhanced lesions per patient per scan
• total number of active T2 lesions per patient per scan
• combined unique (CU) lesions per patient per scan
Both the high and the low experimental doses of cladribine met each of these endpoints with
no statistical difference between the two doses. Annualized relapse rates were reduced by
55% and 58% (p<0.001) and progressive disability as measured by EDSS scores was slowed
by 33% and 31% compared to placebo at 2-years respectively. (see Figures 14 & 15)
Furthermore ~80% of the patients treated with either dose of cladribine were relapse-free as
opposed to 61% in the placebo cohort representing a odds ratio of 2.45 (p<0.001) [10].
Cladribine 3.5 mg/kg
5.25 mg/kg
lacebo
Rescue therapy 44 μgebif®)
scr 1 2 yr
P
(R
yr
MRI
Double blind core study Study extensionJan Nov2005 2009
x x
x x x x
X = 4/5-day course of administration
EDSS
x x
x x
Cladribine 3.5 mg/kg
5.25 mg/kg
lacebo
Rescue therapy 44 μgebif®)
scr 1 2 yr yr
MRI
Double blind core study Study extension
P
(R
x x
x x x x
X =
x x
x x
EDSS
4/5-day course of administration

Page 27
Figure 14 – CLARITY; relapse rates at 2-years Source: ECTRIMS poster, Sep 2009
Figure 15 – CLARITY; disease progression at 2-years Source: ECTRIMS poster, Sep 2009

Page 28
In line with expectations, T, B & NK cell counts in exposed patients decreased rapidly upon
administration with either the high or low dose; granulocytes and monocytes levels were
unaffected. Figure 16 depicts the time course of this effect on CD3+ and CD19 count levels.
Merck Serono has yet to release the full safety & tolerability findings inclusive of AEs,
SAEs and SUSARs per dose group; however cladribine appears to be well tolerated with
90% of the enrolled patients completing the trial. Generalized reports of lymphopenia and
leukopenia are in all likelihood attributable to the Mechanism of Action (MoA). In the high
dose group cardiorespiratory arrest in addition to pancytopenia pneumonia led to a fatality in
one patient who was later found to have had an active tuberculosis infection. Four cases of
malignancy including a fatality in the low dose group were reported in four individual
patients exposed to active treatment with cladribine in the CLARITY trial: ovarian,
pancreatic (†) & cervical cancers and a case of melanoma [11]. Individual cases of herpes
zoster, an opportunistic viral infection, were also noted in both active groups [11].

Page 29
Figure 16 – Cladribine; selective reduction of lymphocytes Source: ECTRIMS poster, Sep 2009

Page 30
ONWARDS is a Phase II 2-year trial evaluating the safety of oral cladribine in combination
with interferon-β; RRMS and SPMS patients entering the trial are randomized (1:1) to
receive either 2 short courses of cladribine or placebo annually on top of their current
therapy with either Rebif®, Avonex® or Betaseron®. This trial is not powered to evaluate
the difference in efficacy between these therapies.
Proactively an 8-year pharmacovigilance trial has been launched to survey the incidence of
safety related reports associated with the long term use of cladribine in MS patients. (see
Figure 17)
Figure 17 – Cladribine; registry trial design Source: ECTRIMS poster, Sep 2009
Primary endpoint
• cumulative incidence of severe and selected infections
• cumulative incidence of malignancies
• cumulative incidence of deaths
• time to resolution of cladribine-induced lymphopenia
• frequency and outcome of pregnancy
• time between seeking pregnancy and becoming pregnant

Page 31
Secondary endpoints
• cumulative incidence of myelodysplasic syndromes (MDS)
• cumulative incidence of haematological toxicity
• descriptive analyses of demographic and MS disease characteristics for all
participants
• hazard ratios for severe and selected infections
• hazard ratios for malignancies
• hazard ratios for deaths
• rate of recurrence of study events
• frequency of other clinically relevant events
Although there have been no comparator-controlled trials, Merck Serono issued two press
releases on July 23, 2009 and September 30, 2009 confirming the submission to the EMEA
and the FDA respectively of Manufacturing Authorization Applications (MAA) requesting
licensing for use of cladribine in RRMS. The FDA announced in 2006 that cladribine had
been awarded the status of “Fast Track” which designates an accelerated approval process
with a priority review of the dossier. If approved, cladribine will be the first highly effective
oral medication to meet the high and as of yet unmet medical need in MS.
Merck Serono is further establishing itself within the field of MS with the Phase III
ORACLE trial in which 200 newly diagnosed CIS patients at risk of progressing to
Clinically Definite MS (CDMS) will be randomized to receive either placebo or 1 or 2
courses of cladribine annually until conversion to CDMS.

Page 32
Teriflunomide
As a disease-modifying antirheumatic drug (DMARD) Arava® (leflunomide) inhibits the de-
novo pyramidine synthesis by hampering dihydro-orotate dehydrogenase (DHODH) and in
parallel exhibits anti-inflammatory properties. Arava® is licensed for use in Rheumatoid
Arthritis (RA) & psoriatic arthritis (PsA), and recently received orphan drug status for
transplant rejection from the FDA. Teriflunomide is the active metabolite of leflunomide;
both compounds belong to Sanofi-Aventis. The pro-inflammatory, activated T&B cells
which propagate brain lesions in MS are rapidly dividing and therefore targeting an enzyme
such as DHODH makes intuitive sense; teriflunomide arrests the division of the T&B cells
and renders them cytostatic. Resting lymphocytes are spared the effects of teriflunomide
through salvage pathways and continue with vital immuno-surveillance activities. Due to
the fact that teriflunomide’s target is an intracellular enzyme, it breaches the cell wall and
discontinuation of therapy is problematic requiring treatment with either cholestyramine or
activated charcoal.
Teriflunomide LeflunomideTeriflunomide Leflunomide
Figure 18 – Teriflunomide & leflunomide; chemical structures Source: http://journals.prous.com/journals/dof/20073211/html/df321007/images/fig13.gif

Page 33
Clinical Development
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
TEMSO
TOPIC (CIS MS)
HMR1726D-2001
Figure 19 – Teriflunomide MS development plan
In 2006 O’Connor et al. published the findings from the 9-month placebo-controlled dose-
finding Phase IIb trial with teriflunomide in 177 RR/SPMS patients recruited over 14 months
at 16 sites in France and Canada [11]. Patients were randomized to receive either daily doses
7 mg or 14 mg of experimental teriflunomide or placebo and MRIs were taken every 6
weeks. Figure 20 outlines the trial design.
HMR1726D-2002
On top of CopaxonePoC HMR1726D-2004
PoC TENEREOn top of interferon-β
TOWER
EFC6049
MAA
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
TEMSO
TOPIC (CIS MS)
HMR1726D-2001
MA Launch
HMR1726D-2002
On top of CopaxonePoC HMR1726D-2004
PoC TENEREOn top of interferon-β
TOWER
EFC6049
MAA MA LaunchMAA MA Launch

Page 34
Figure 20 – HMR1726D-2001 trial design Adapted from: O’Connor et al., 2006. , A Phase II Study of the Safety and Efficacy of Teriflunomide in Multiple Sclerosis with Relapses, Neurology, 66, p. 894-900 Primary endpoint
• total number of new and persisting combined unique (CU) lesions at 9 months
Secondary endpoints
• total number of lesions on T1 Gd+ enhancing MRI images
• total number of new & enlarging lesions on T2 Gd+ enhancing MRI images
• total number of patients with CU active, T1 and T2 Gd+ enhancing active lesions
• % change from baseline to endpoint in the burden of disease measured by T2 lesion
volume
Clinical endpoints
• number of patients experiencing a relapse
• annualized relapse rate
• number of relapsing patients requiring a course of steroids
• disability progression EDSS
Teriflunomide 7 mg
14 mg
lacebo
Double blind core study
scr x 1.5 3 4.5 6 7.5 9 mon 1 yr 2 yr 3 yr* 9 yr
Study extension
P
MRI
Apr Mar Nov 2001 2003 2011
//
EDSS
//
First week loading dose
* safety and efficacy readout
Teriflunomide 7 mg
14 mg
lacebo
Double blind core study
scr x 1.5 3 4.5 6 7.5 9 mon 1 yr 2 yr 3 yr* 9 yr
Study extension
MRI
Apr Mar Nov 2001 2003 2011
//
P
EDSS
//
First week loading dose
* safety and efficacy readout

Page 35
In this exploratory study in relapsing MS patients, doses of 7 mg OD and 14 mg OD
teriflunomide met the primary endpoint by reducing CU lesions by 60% (p<0.03) and 40%
(p<0.01) respectively compared to placebo. Treatment with teriflunomide significantly
reduced the number of T1 lesions per scan, new & enlarging T2 lesions per scan and new T2
lesions. Once daily 14 mg teriflunomide demonstrated statistically non-significant trends
towards lower ARRs, fewer relapsing patients, and the slowing of disability progression.
Figure 21 depicts the effect of teriflunomide on CU lesions over 9 months. The 14 mg OD
dose was associated with a non-statistically significant reduction in ARR of 32% and a 69%
reduction in the number of patients with a worsened disability state. The safety and
tolerability profile at 9-months was comparable between all groups.
Figure 21 – Teriflunomide; combined unique lesions at 9-months Source: O’Connor et al., 2006. , A Phase II Study of the Safety and Efficacy of Teriflunomide in Multiple Sclerosis with Relapses, Neurology, 66, p. 897
Following these encouraging results Sanofi-Aventis advanced teriflunomide into an
aggressive MS program encompassing monotherapy & combination therapy in relapsing MS
and the effects of monotherapy in early stage MS (CIS). The first RMS registration 2-year
placebo-controlled trial TEMSO began in September 2004 and has completed the

Page 36
recruitment of 1080 RR/SP/PPMS patients in 21 countries and is scheduled to report in
October 2010. TOWER is a 1-year placebo-controlled confirmatory trial in RMS patients
which began recruiting the targeted 1110 RR/SP/PPMS patients in August 2008 in 19
countries and is projected to complete by September 2011. In parallel to these registration
trials, Sanofi-Aventis launched TENERE a Proof-of-Concept (PoC) trial evaluating the
safety and efficacy of combination therapy with Rebif® (interferonβ-1a) in 300 RMS
patients and a second PoC trial comparing the safety of combination treatment with
Copaxone® (glatiramer acetate) at 6-months in 120 MS patients. TENERE is currently
recruiting whereas the 6-month combination trial with Copaxone® has completed
recruitment. Both PoC trials are expected to form a part of the Manufacturing Authority
Application (MAA).
Additionally TOPIC the 2-year placebo-controlled Phase III trial in an early stage/at risk
population began recruiting 780 CIS patients at 133 sites within 20 countries in February
2008.
Administration of either 7 mg OD or 14 mg OD teriflunomide is common to all of the above
mentioned trials.

Page 37
S1P receptor agonists
G protein-coupled receptors (GPCR) have come to the forefront of pharmacological research
as they transverse the cell wall and mediate intracellular signaling through the release of
specific messenger molecules. As a result a pharmacological agent need only interact with
the GPCR on the cell’s outer surface and need not necessarily penetrate the cell to induce or
exclude an intracellular response. Relying on the cell membrane’s innate protective
properties, undesired intracellular responses can thus be greatly reduced. Depending on the
conformational structure of and affinity between both target receptor & pharmacological
agent, a higher degree of specificity for the target receptor over other structurally similar yet
functionally different receptors can also potentially reduce many undesirable side effects.
Ceramides, a family of bioactive lipids present in the cell membrane of many cells, are
found predominantly in the skin; accounting for up to 50% of the lipid count in the stratum
corneum and in trace amounts throughout the rest of the body. Although ceramides are not
G protein-coupled receptors, following extensive research it was determined that similar to
GPCRs, they could also mediate intracellular responses inclusive of cell differentiation,
transformation, proliferation, and programmed cell death, i.e. apoptosis. The mechanism by
which these activities are achieved is still uncertain. Although de novo synthesis in animals
is possible, it is significantly faster for cells under stress to produce ceramide via the
hydrolyzing enzyme sphingomyelin phosphodiesterase (SMase).
Ceramides are composed of a fatty acid bound to sphingosine via an amide bond as shown in
Figure 22 beneath. The terminal hydroxyl group can be further conjugated to produce a
multitude of unique sphingolipids.

Page 38
Sphingosine
Fatty acid
Sphingosine
Fatty acid
Figure 22 – Ceramide; generic chemical structure Adapted from: http://www.lipidlibrary.co.uk/Lipids/ceramide/index.htm The process by which catabolism of ceramide yields sphingosine-1-phosphate (S1P), an
endogenous signaling sphingolipid found predominantly in the circulating blood supply, is
shown in Figure 23.
Figure 23 – Sphingolipid biosynthetic pathway Source: Rosen et al., 2009. Sphingosine 1-Phosphate Receptor Signaling, Annual Review of Biochemistry, 78, p. 745
S1P was shown to be an extracellular ligand released by both mast cells and platelets among
other cells which binds to S1P1-5, a family of lysophospholipid GCPRs. The known activity
of all known S1Px receptors, as determined by experiments with knock-out mice, in-vitro
assays or a combination of both, is listed beneath in Table I.

Page 39
Table II – Properties of sphingosine-1-phosphates
Distribution Cellular function and consequences S1P1 brain
heart spleen liver lung thymus kidney skeletal muscle lymphoid
Astrocyte: migration B-cell: blockade of egress, chemotaxis Cardiomyocyte: increased β-AR positive inotropy Endothelial cell: early vascular system development, adherens junction assembly, APC-mediated increased barrier integrity Neural stem cell: increased migration Pericyte: early vascular system development (VSMC) T-cell: blockade of egress, chemotaxis, decreased late-stage maturation VSMC
S1P2 brain heart spleen liver lung thymus kidney skeletal muscle
Cardiomyocyte: survival to ischemia-reperfusion Epithelial cell (stria vascularis): integrity/development Epithelial hair cells (cochlea): integrity/development Endothelial cell (retina): pathological angiogenesis, adherens junction disruption Hepatocyte: proliferation/matrix remodeling Fibroblast (MEF) Mast cell: degranulation VSMC: decreased PDGF-induced migration
S1P3 brain heart spleen liver lung thymus kidney skeletal muscle testis
Cardiomyocyte: survival to ischemia-reperfusion Dendritic cell (hematopoietic): worsening experimental sepsis lethality/inflammation/coagulation
S1P4 lung lymphoid
T-cell: migration/cytokine secretion
S1P5 brain skin spleen
NK cell: trafficking Oligodendrocyte: survival OPC: glial process retraction; inhibition of migration
Source: Rosen et al., 2009. Sphingosine 1-Phosphate Receptor Signaling, Annual Review of Biochemistry, 78, p. 749
This sequestration of peripheral blood lymphocytes via S1P1 agonism is thought to offer
primary therapeutic benefit in MS, effectively reducing the chances of further immunological
attacks on myelinated brain tissue.

Page 40
Fingolimod
The discovery of these 5 lysophospholipids and the elucidation of their expression &
function has presented the pharmaceutical industry with an entirely new and novel set of
target receptors. The first and most well known non-selective S1P1,3-5 agonist to reach
clinical trials was Novartis’ fingolimod, also known as FTY720. Fingolimod is an analogue
to a naturally occurring Myriocin metabolite ISP-1 produced by the fungus Isaria sinclairii
which has been used for centuries in traditional Chinese medicine [13]. Fingolimod was first
synthesized in 1992 by Kunitomo Adachi & Kenji Chiba, two Japanese medicinal chemists.
Long after its entry in the 1990’s into clinical testing as a novel immunomodulator,
fingolimod was found to be a sphingosine-like prodrug in 2002. Fingolimod-phosphate
(fingolimid-P), the active metabolite produced via phosphorylation by sphingosine kinase, is
a potent agonist at all S1P receptors with the exception of S1P2 and selectively reduces both
peripheral T&B cell counts in the blood [14]. There is also evidence that fingolimod-P acts
as a cannabinoid antagonist, cPLA2 inhibitor, and ceramide synthase inhibitor [15][16][17].
Figure 24 depicts the structure of both the parent compound fingolimod and its prodrug
fingolimod-P.
fingolimod fingolimod-P
Sphingosinekinase
fingolimod fingolimod-P
Sphingosinekinase
Figure 24 – Fingolimod; parent and phosporylated metabolite Adapted from: http://journals.prous.com/journals/dof/20073211/html/df321007/images/fig12.gif

Page 41
Lymphocytes naturally migrate from secondary lymphoid tissues and the thymus, where the
concentration of sphingosine-1 phosphate (S1P) is low, to the blood where the aggregation is
significantly higher. It has been postulated that the immunosuppressive effect witnessed
with fingolimod-P is due its ability as a “functional antagonist” to internalize the S1P1
receptors on the surface of the T&B cells and so by desensitize them to the gradient of S1P
leaving them sequestered in the lymphatic system [18]. Fingolimod-P does not affect the
activation, proliferation or effector functions of these lymphocytes nor does it affect levels of
natural killer cells, monocytes or granulocytes in the blood.
Clinical Development
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 Figure 25 – Fingolimod MS development plan
The 1st administration of fingolimod in single ascending doses on top of Neoral® in human
renal transplant patients was reported in 2002 by Budde et al. [19]. Figure 26 depicts the
study design.
RRMS/SPMS
Freedoms I
Freedoms II
Informs (PPMS)
Transforms
Ethnic sensitivity
MAA MA Launch
Asthma
end 2011
1998 MAD199X SAD
2013
Avonex controlled
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
199X SAD
RRMS/SPMS
Freedoms I
Freedoms II
Informs (PPMS)
Transforms
Ethnic sensitivity
Asthma
end 2011
1998 MAD
2013
Avonex controlled
MAA MA Launch

Page 42
Figure 26 – Fingolimod; SAD on top of Neoral® in renal transplant patients Adapted from: Budde et al., 2002. First human trial of FTY720 a novel immunomodulator in stable renal transplant patients, Journal of the American Society of Nephrology, 13(4), p.1073-83
All doses showed a reversible transient lymphopenia as shown in Figure 27. Whereas the
variability in response to the 0.25 – 2.0 mg doses failed to yield clear dose-dependent
relationship, 3.5 mg fingolimod demonstrated a dramatic mean decrease of 73% from
baseline values within 8 hours of administration.
Figure 27 – Fingolimod; SAD lymphocyte reductions Source: Budde et al., 2002. First human trial of FTY720 a novel immunomodulator in stable renal transplant patients, Journal of the American Society of Nephrology, 13(4), p.1077
FTY720 0.25 mg0.5 mg
0.75 mg1.0 mg2.0 mg3.5 mg
ebo
-21d -2d -1d -1hr x 0.5 1 2 6 12 24 48 72 96hr
Plac
administration
FEV1, FVC, DLCO, exercise
undisclosed timepoints
FTY720 0.25 mg0.5 mg
0.75 mg1.0 mg2.0 mg3.5 mg
ebo
-21d -2d -1d -1hr x 0.5 1 2 6 12 24 48 72 96hr
Plac
administration
FEV1, FVC, DLCO, exercise
undisclosed timepoints

Page 43
Single administration was considered to be safe and well tolerated with no serious adverse
effects. However the most common adverse event was dose-dependent transient
asymptomatic bradycardia. As the treatment arms contained few and occasionally shared the
same subjects, the pulse rate data was combined to produce a low dose group of 0.25 & 0.5
mg and a high dose group of 0.75, 1, 2 & 3.5 mg. A more pronounced effect is associated
with the higher dose groups. Figure 28 clearly illustrates this effect.
Figure 28 – Fingolimod; SAD Bradycardic effects Source: Budde et al., 2002. First human trial of FTY720 a novel immunomodulator stable renal transplant patients, Journal of the American Society of Nephrology, 13(4), p.1077
Encouraged by these results, Novartis engaged in further development of fingolimod
culminating in the decision to enter full scale development in two indications where the
sequestration of lymphocytes could plausibly provide therapeutic promise: renal transplant
and Multiple Sclerosis.
In 2006 Salvadori et al. reported on a 1-year Phase III registration trial in renal transplant
which began in May 2003 and recruited 668 patients in 42 sites worldwide [20]. This trial
established no benefit for either a course of 2.5 mg fingolimod plus a full-dose of
cyclosporine or 5 mg fingolimod plus a reduced-dose of cyclosporine over the standard care:
mycophenolate mofetil plus a full-dose of cyclosporine. The safety findings of note

Page 44
FTY720 1.25 mg
5 mg
Placebo
Double blind core study
scr x 1d 7d 1 mon 2 3 4 5 6 mon 9 mon 1 yr
FEV1, FVC, DLCO
Study extension
consisted of the expected transient first dose bradycardia as well as lower creatinine
clearance levels and a dose-dependent, increased incidence of macular edema.
Also in 2006 Kappos et al. reported on the placebo controlled 6-month Phase IIb dose
finding study in MS which began in May 2003 and recruited 281 patients in 26 sites ex-US
[21]. This study explored the efficacy of fingolimod doses 5 mg and 1.25 mg against
placebo at 6-months in patients which presented with either relapsing-remitting MS (RRMS)
or secondary progressive MS (SPMS); thereafter an open label extension was offered to all
patients who desired to continue on treatment with fingolimod until either the eventual
registration or termination of the clinical development program. Figure 29 illustrates the
study design.
Figure 29 – Fingolimod; Phase IIb trial design Adapted from: Kappos et al., 2006. Oral fingolimod (FTY720) for relapsing Multiple Sclerosis, New England Journal of Medicine, 335), p.1124-41
Following the heart rate disturbances and reports of dyspnea witnessed in the SAD trial,
monitoring measures, i.e. electrocardiogram (ECG), Holter monitoring, forced expiratory
volume in 1 second (FEV1), forced vital capacity (FVC) and diffusing capacity of the lung
for carbon monoxide (DLCO), were implemented in the protocol to ensure the patient’s
ECG
EDSS, MSFC
MRI
x x xx = 24hr Holter
at select sites
May October April May2003 2004 2005 2010
//
5 mg dose shows no moreefficacy than 1.25 mg andall remaining patients areswitched to 1.25 mg @month 15
FTY720 1.25 mg
5 mg
Placebo
Double blind core study
scr x 1d 7d 1 mon 2 3 4 5 6 mon 9 mon 1 yr
FEV1, FVC, DLCO
Study extension
ECG
EDSS, MSFC
MRI
x x xx = 24hr Holter
at select sites
May October April May2003 2004 2005 2010
//
5 mg dose shows no moreefficacy than 1.25 mg andall remaining patients areswitched to 1.25 mg @month 15

Page 45
safety as well as to better describe the occurrence, course & severity of these events. The
endpoints were:
Primary endpoint
• reduction in the number of Gd+ enhanced lesions/patient at 6 months on T1-weighted
MRI images
Secondary endpoints
• total volume of Gd+ enhanced lesions per patient
• proportion of patients with Gd+ enhanced lesions
• total number of new lesions/patient on T2-weighted MRI images
• brain volume from baseline to month 6
Clinical endpoints
• number of patients remaining free of relapse
• annualized relapse rate
• time to first relapse
• Expanded Disability Status Score (EDSS) at 12 months
Both experimental doses of fingolimod met all of the endpoints above with the exception of
brain volume from baseline to month 6 and EDSS at 12 months. As shown in Figure 30 the
higher dose of 5 mg failed to differentiate itself from the effects witnessed with 1.25 mg at 6-
months. After the 5 mg dose continued to provide no increased clinical benefit compared to
the 1.25 mg dose at 12-months, it was discontinued as an experimental dose in subsequent
MS trials.

Page 46
Proportions of patients who were free of Gd-enhanced lesions on T1 weighted MRI at month 0 and 6 Estimated time to a first confirmed relapse
Proportions of patients who were free of Gd-enhanced lesions on T1 weighted MRI at month 0 and 6 Estimated time to a first confirmed relapse
Figure 30 –Fingolimod; Phase IIb results at 6-months Source: Kappos et al., 2006. Oral fingolimod (FTY720) for relapsing Multiple Sclerosis, New England Journal of Medicine, 335), p.1132
Both experimental doses of fingolimod were judged to be well tolerated in the patient
population. The majority of the SAEs were associated with the 5 mg dose. Figure 31 lists
the most common reported SAEs and AEs associated with both doses at 6-months. Raised
levels of liver enzyme levels (>3 x ULN) of both alanine transaminase (ALT) and aspartate
transaminase (AST) were noted at 6-months. No clinical symptoms were observed and the
levels normalized equally either over time without a down-titration or upon discontinuation
of treatment altogether.
Figure 31– Fingolimod; tolerability profile at 6-months Adapted from: Kappos et al., 2006. Oral fingolimod (FTY720) for relapsing Multiple Sclerosis, New England Journal of Medicine, (335), p.1134-37

Page 47
This Phase IIb dose-finding study established neither a full dose response curve nor any
improvement on the disability score observed with either dose at 6-months; however the
45% reduction in Annualized Relapse Rate (ARR) against placebo was already a tremendous
improvement on the ~ 30% ARR reductions achieved with currently marketed biologics.
Furthermore it could be argued that 6-months was far too short a period to measure the delay
to disease progression in an indication whose time course spans more than a decade on
average - and fingolimod held the promise of convenient oral once daily administration.
Novartis abandoned the renal transplant program and invested in a substantial MS Phase III
program which began with two registration trials TRANSFORMS & FREEDOMS and
eventually expanded to include FREEDOMS II. TRANSFORMS was a 1-year trial with 2
doses of 1.25 mg and 0.5 mg against Avonex® the market leading interferon β-1a which
began in May 2006 and recruited 1,292 patients with 141 clinical sites in 18 countries.
Figure 32 depicts the trial design as disclosed at the World Congress on Treatment and
Research in Multiple Sclerosis. Holter monitoring was dropped as a requirement. Many of
the remaining safety monitoring measures were the same, i.e. MRI, ECG, FEV1, FVC and
DLCO. New monitoring requirements included ophthalmological exams, chest x-ray and
high resolution CT scan (HRCT). Ophthalmological exams could be warranted given the
increased incidence of macular edema in the renal transplant program. Chest x-rays might
have been used to exclude patients with latent tuberculosis infections which could be
reactivated under therapy. HRCT was introduced presumably to determine the etiology of
the dyspnea reported in the Phase IIb study. Given the 1-year duration of this trial and the
decrease in FEV1 observed in the Phase IIb trial, it is possible that the use of HRCT scans
was used to detect potential fibrotic changes which could result in constriction of the
bronchial passages and eventually lead to difficulty in breathing.

Page 48
TY720 0.5 mg
1.25 mg
onex® 30 μg
scr x 1 yr
FEV1, FVC, DLCO
May Sep Apr 2006 2008 2011Double blind core study Study extensionMay Sep Apr 2006 2008 2011Double blind core study Study extension
FF Av
Figure 32 – TRANSFORMS trial design Adapted from: WCTRIMS poster, Sep 2008
This trial was conducted in the patients with relapsing-remitting MS (RRMS). The
endpoints were as follows:
Primary endpoints
• monthly MRI lesion parameters
• safety & tolerability at 6-months
Secondary endpoints
• time to first relapse at 6-months
• proportion of relapse-free patients at 6-months
ECG
EDSS, MSFC
MRI
Chest X-ray or HRCT
Ophthalmological exam
??
??
??
??
??
??
TY720 0.5 mg
1.25 mg
onex® 30 μg
scr x 1 yr
FEV1, FVC, DLCO
Av
ECG
EDSS, MSFC
MRI??
??
??
??
Chest X-ray or HRCT
Ophthalmological exam
??
??

Page 49
On December12, 2008 Novartis issued a press release disclosing the initial results from the
TRANSFORMS trial. Strikingly the lower dose of 0.5 mg demonstrated a better clinical
response than the higher 1.25 mg dose; 52% reduction in ARR as opposed to 38%
respectively (p<0.001). Fingolimod was once more considered to be well tolerated as 87%
of the patients completed the study. Also of note was the ARR of 0.33 relapses/year
determined from the 431 Avonex® treated patients. The registration trial as reported in the
Avonex® Manufacturing Authorization Application (MAA) submitted to the FDA did not
report a clinical benefit to patients in the first year of administration; it reported an ARR of
1.03 in the active 65 patient arm against 0.8 reported in the 45 patient placebo arm at 1-year
with a therapeutic benefit manifesting itself only at the 2-year timepoint. In the
TRANSFORMS data Avonex® appears to already have an effect at 6-months. This
however may be due to the change in clinical practice since 1996 when the MAA was
submitted. Curiously enough Novartis decided against releasing data pertaining to disease
progression as measured by EDSS.
The astounding efficacy was off-set by the long term safety profile however. Transient
bradycardia remained a common safety finding, AST & ALT levels ≥ 3 x ULN were
reported in some patients, along with 7 cases of macular edema. New findings included
increased blood pressure (BP), 7 cases of skin cancer and 2 fatal viral infections: primary
disseminated varicella (†) and herpes encephalitis (†). Malignancies and opportunistic
infections are two well known risks associated with long term immunosuppression.
Shortly after the December 2008 press release, O’Connor et al. published the results of the
Phase IIb 2-year extension study [22]. 250 (89%) of the patients from the core study entered
the optional open-label extension study where those patients initially receiving placebo
therapy were re-randomized to receive long term treatment with either 1.25 mg or 5 mg
fingolimod. O’Connor et al. reported on the outcomes from the remaining 189 (75.6%)
patients as they completed 2-years of continuous treatment. As previously mentioned within
3 months of the study start the 5 mg dose group was discontinued due to an increased safety

Page 50
burden combined with a lack of increased efficacy compared to 1.25 mg at 6-months.
Patients re-randomized to either dose of fingolimod exhibited a similar reduction on
inflammatory markers as detected by MRI, i.e. T2 weighted Gd+ enhanced images, as
previously witnessed in the active groups in the core study. Those patients continuing with
either 1.25 mg treatment or down-titrating from 5 to 1.25 mg improved or remained stable
and these groups demonstrated a 55% or 53% relative reduction in ARR respectively after 1-
year of continuous treatment including the core study exposure. Figure 33 illustrates the
proportion of patients remaining relapse-free over time.
Figure 33 – Fingolimod; time to first confirmed relapse in 2-year extension study Source: O’Connor et al., 2009. Oral fingolimod (FTY720) in Multiple Sclerosis, Neurology (72), p.76
AEs and withdrawal of consent were the two most common reasons for treatment
discontinuation. The majority of the AEs were mild to moderate in nature with
nasopharyngitis, headache, influenza and lymphopenia being the most prevalent. 10% of the
patients experienced at least one SAE: unconfirmed macular edema, peripheral edema,
hepatitis, jaundice, MS relapse, hirsutism, flushing, neutropenia, adrenal mass, acute
abdomen, inguinal hernia, salpingitis, drug exposure during pregnancy and hypertension.
ALT elevations >3 x ULN were reported in 12-16% of the patient population.

Page 51
As expected peripheral lymphocyte counts decreased by up to 75% from baseline and
remained between 500 - 600 cells/m3. Furthermore there were no reported instances of
opportunistic infections or malignancies as one might expect with the continuous use of a
compound which so effectively reduces circulating lymphocytes.
Transient bradycardia continued to be witnessed in naïve patients switching from placebo to
active treatment within the first hour of dosing and resolved without further medical
intervention after a maximal 4-5 hours. Comparison with pre-treatment values at 2-years
revealed no further instances of bradycardia.
A decrease in systolic blood pressure was observed in the first 6 hours of dosing which
returned to baseline values by Day 7 without intervention. At 2-years a mean increase of 4.1
- 6.3 mm Hg in sitting BP from the baseline values measured in the core study was noted.
Pulmonary function was not explicitly monitored in the long term extension study; however
reports of asthma and dyspnea were associated with both dose groups.
In contrast to the core study and TRANSFORMS, there were no instances of confirmed
macular edema.
The FREEDOMS trials are two identical 2-year placebo-controlled studies investigating the
doses of 1.25 mg and 0.5 mg fingolimod. FREEDOMS I began in January 2006 and
recruited 1,272 RRMS patients with 115 clinical sites in 19 countries ex-US. FREEDOMS
II began later in June 2006 and recruited 1,080 RRMS patients with 107 clinical sites
predominantly in the US but also included sites from another 7 countries. Figure 34 depicts
the FREEDOMS I&II trial design as disclosed at the World Congress on Treatment &
Research in Multiple Sclerosis and an independent press release in September 2009.

Page 52
Jan Aug Apr 2006 2009 2011Double blind core study Study extensionJan Aug Apr 2006 2009 2011Double blind core study Study extension
FTY720 0.5 mg
1.25 mg
lacebo
scr x 6 mon 1 yr 2 yr
FEV1, FVC, DLCO
FTY Figure 34 – FREEDOMS I&II trial design Adapted from: WCTRIMS poster, Sep 2008 / FREEDOMS press release, Sep 2009 Both of these trials were conducted in the patients with relapsing-remitting MS (RRMS).
The endpoints were as follows:
Primary endpoint
• Annualized relapse rate at 2-years
Secondary endpoints
• Proportion of relapse-free patients treated at 2-years
• Safety & tolerability of fingolimod at 2-years
• Burden of disease and inflammatory activity as measured by MRI lesion parameters
at 2-years
On September 30, 2009 Novartis released the first results from the FREEDOMS trial.
Compared to placebo daily oral dosing with 0.5 and 1.25 mg led to a reduction in
Annualized Relapse Rates (ARR) by 54% and 60% (p<0.001) and slowing of disease
P
ECG
EDSS, MSFC
MRI
x x = MSFC
Chest X-ray
Ophthalmological exam
??
??
??
??
??
720 0.5 mg
1.25 mg
lacebo
scr x 6 mon 1 yr 2 yr
FEV1, FVC, DLCO
P
ECG
EDSS, MSFC
MRI
??
??
??x x = MSFC
Chest X-ray
Ophthalmological exam
??
??

Page 53
progression as measured by EDSS scores of 30% and 32% respectively at 2-years. (see
Figures 35 & 36)
The 0.5 mg dose appears to have been safer and better tolerated than the 1.25 mg dose. In
contrast to placebo and 1.25 mg groups, no cases of heart rhythm disorders, macular edema,
melanoma, breast cancer or deaths were reported with this dose. Figure 37 provides the
SAE listings.
Figure 35– Fingolimod; relapse rate at 2-years in FREEDOMS Source: FREEDOMS press release, Sep 2009
Figure 36 – Fingolimod; disease progression at 2-years in FREEDOMS Source: FREEDOMS press release, Sep 2009

Page 54
Figure 37 – Fingolimod; Serious Adverse Events reported in FREEDOMS Source: FREEDOMS press release, Sep 2009
Novartis plans to submit a Manufacturer’s Authorization Application (MAA) to the EU and
a New Drug Application (NDA) to the FDA by the end of 2009; the FDA has not granted
Fast Track status to fingolimod.
Novartis has initiated INFORMS, a 3-year study comparing the effects of 1.25 mg
fingolimod against placebo in 654 patients with primary progressive MS (PPMS). There is
no licensed treatment for PPMS. Currently there are no on-going trials exploring the
efficacy and safety of combination therapy with other licensed products in RRMS. Neither
clinically isolated syndrome (CIS) nor secondary progressive MS (SPMS) are presently
under investigation with fingolimod.

Page 55
BAF312
The natural process of remyelination begins with the migration of oligodendrocyte precursor
cells (OPC) to sites of axonal trauma and ends with the development of mature
oligodendrocyte cells which re-sheath the damaged neurons with myelin. As S1P5 is
predominantly expressed in oligodendrocytes and the white matter tracts of the brain, it
presented itself as an interesting target to researchers investigating demyelinating disorders.
Novgorodov et al. published work which links the inhibition of OPC migration to agonism of
S1P5 using S1P in cultured cells from neonatal rat cortices; however other studies show an
increased survival rate of mature oligodendrocytes in cytotoxic environments [23][24].
Although fingolimod, a non-selective S1P1,3-5 agonist, demonstrated a high degree of clinical
efficacy as measured by reduced GD+ enhanced lesions, ARR & disability progression,
differentiation between the therapeutic benefits derived from remyelination as a direct result
of S1P5 agonism or otherwise, and lymphocyte sequestration will remain highly speculative;
comparative outcomes from clinical trials in patients suffering demyelinating disorders are
the sole means to investigate this mechanism and even then the conclusions will not be
decisive.
In 2004, during the conduct of the fingolimod Phase IIb program, Germana Sanna et al.
published an article which linked S1P3 agonism with bradycardia using S1P3 knock-out mice
[25]. Novartis developed a dual S1P1/5 agonist BAF312 which was >1,000 fold more
selective for S1P1 than S1P3 and began the first pharmacological study with 63 human
subjects in October 2006.

Page 56
Clinical Development
Figure 38 – BAF312 MS development plan
In December 2008 Novartis disclosed the initiation of the BOLD Phase IIb trial in RRMS
patients. The experimental dosing range of 0.5 to 10 mg against placebo was constructed
based on the PK/PD data from the BAF312 SAD trial and the mean lymphocyte count
reductions associated with a clinical improvement in the previous fingolimod MS Phase IIb
trial. An interim analysis at 3-months will allow the introduction of up to 2 additional doses
for the remainder of the 6-month treatment period in an effort to hone in on the doses most
likely to be efficacious in the Phase III program. The BOLD trial is currently recruiting 275
RRMS patients at 82 investigational sites in 12 countries and is scheduled to conclude
treatment in October 2010. This was an apparent leap-frogging of the standard MAD trial in
human subjects. Figure 39 depicts the study design of the BOLD trial.
CBAF312A2201 IIb
2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 2018
CBAF312A2101 SAD
MAA MA LaunchMAA MA LaunchMAA MA Launch
X
LPLV
CBAF312A210X MAD ?

Page 57
Figure 39 – BAF312; BOLD trial design Source: ECTRIMS, Sep 2009
BOLD is conducted exclusively in relapsing-remitting MS (RRMS) patients. The endpoints
are as follows:
Primary endpoint
• Dose dependent relationship among five doses of BAF312 and placebo as measured
by the number of combined unique active MRI lesions at 3-months
Secondary endpoints
• Safety & tolerability of BAF312 at 3 & 6 months
• Number of relapses, annualized relapse rate (ARR), and proportion of relapse-free
patients
• Correlation between the course of lymphocyte count with MRI activity & clinical
outcomes
• Additional MRI parameters
• Steady state plasma concentrations

Page 58
However in September 2009 Novartis released the first results from a hitherto undisclosed
MAD study in human subjects at the annual ECTRIMS conference. Contrary to
expectations a first dose effect of transient bradycardia was still observed in a dose
dependent manner with the use of an S1P1 selective agonist in humans in first 24 hours of
exposure; maximum mean decrease was observed at ~2 hours with every dose tested.
Curiously the highest dose group, 20 mg, largely overshoots the baseline heart rate values as
it recovers on Day 1. (see Figure 40)
Figure 40 – Mean Ventricular Heart Rate following administration of BAF312 Source: ECTRIMS poster, Sep 2009
Figure 41 depicts the expected dose dependent reductions of average lymphocyte counts
(ALC). BAF312 decreased both blood borne CD+3 T cells and B cells, preferentially
depletes CD+4 over CD+8 and has no effect on natural killer cells, monocytes or granulocytes.
In contrast to fingolimod the ALC levels in each cohort excepting 20 mg were rapidly
restored to baseline values within 2-weeks.

Page 59
Figure 41 – Absolute lymphocyte count reductions following administration of BAF312 Source: ECTRIMS poster, Sep 2009
With a half-life of approximately 30 hours and steady state achieved within 6 days, BAF312
lends itself to once daily administration.

Page 60
ACT-128800
In July 2006 Actelion Pharmaceuticals Ltd and F. Hoffmann-La Roche entered into a
collaboration to develop and commercialize Actelion’s S1P1 selective receptor agonist,
ACT-128800. At the American Society for Clinical Pharmacology and Therapeutics
(ASCPT) conference in March 2009, the first results from the placebo-controlled SAD trial
with this compound in 48 healthy male subjects were presented [26]. Doses of 1, 3, 8, 20,
50, and 75 mg were given in a fasted state to 8 subjects randomized to active drug or placebo
(3:1) with the 20 mg dose group receiving a 2nd dose after a standardized meal 7-days later.
ACT-128800 demonstrated well defined dose-proportional pharmacokinetics profile with a
t½ of 22-33 hours supporting once daily oral dosing (see Figures 42). No relevant food
effect was observed nor were any serious adverse events (SAEs) reported; however a
transient bradycardia peaking along with Cmax at 2.5 hours post-dose and returning to normal
between 6-10 hours after administration was witnessed with doses ≥ 8 mg. The maximal
lymphocyte reduction was associated with the highest dose tested, 75 mg, and reached a
mean value of 70% from baseline. Furthermore the immunomodulatory effect was rapidly
reversible as noted in Figures 43 & 44.

Page 61
AC
T-12
8800
(ng/
mL)
AC
T-12
8800
(ng/
mL)
Figure 42 – ACT-128800; SAD pharmacokinetics Source: ASCPT poster, Mar 2009
Figure 43 – ACT-128800; SAD mean lymphocyte count reductions following single administration Source: ASCPT poster, Mar 2009

Page 62
Figure 44 – ACT-128800; SAD mean %Δ in lymphocyte count following single administration Source: ASCPT poster, Mar 2009
A Proof of Concept (PoC) 6-week study in psoriasis another auto-immune disorder began in
October 2008 and completed recruitment in July 2009; results are expected to be announced
by year-end.
On 08 October 2009 both companies announced the first patient in a Phase IIb dose-finding
study in Multiple Sclerosis.

Page 63
CS-0777
Daiichi Sankyo has developed a prodrug CS-0777 which is selective for the S1P1 receptor
and phosphorylated in-vivo to CS-0777P. The EC50 of CS-0777P and FTY720P
(phosphorylated fingolimod) were determined for S1P1,2,3,5 receptors using cultured rat and
human cell lines. CS-0777P demonstrates an affinity which is 311 fold higher for the S1P1
receptor over S1P3 than its predecessor FTY720-P (see Table II). In an apparent
confirmation of this selectivity asymptomatic bradycardia was limited to the first exposure
with the highest dose of 2.5 mg and resolved without intervention within 24 hours in the
SAD trial.
Table III – CS-0777P; comparative S1P receptor selectivity
Source: ECTRIMS poster, Sep 2009
Plasma concentrations of CS-0777P increased in a well defined dose-dependent fashion and
as expected the absolute lymphocyte counts in exposed subjects reduced overtime in a
similar fashion (see Figure 45). CS-0777P preferentially reduces the plasma concentrations
of T&B cells, exhibits no debilitative effects on either of these cells, i.e. apoptosis or

Page 64
necrosis, and shows no effect on NK cells or neutrophils (see Figure 46). Maximal
lymphocyte reductions were witnessed with the higher dose groups of 1 and 2.5 mg;
however on the last blood sampling 12 days following single administration significant
concentrations of CS-0777P were still present and lymphocyte counts had yet to return to
baseline values (see Figure 47).
Figure 45 – CS-0777P; SAD pharmacokinetics Source: ECTRIMS poster, Sep 2009
Figure 46 – CS-0777; SAD reduction of lymphocyte sub-populations

Page 65
Source: ECTRIMS poster, Sep 2009
Figure 47 – CS-0777; SAD peripheral lymphocyte counts Source: ECTRIMS poster, Sep 2009
Aside from transient bradycardia (nadir ~30-40 bpm at ~1 hr), single administration of CS-
0777 was associated with a >3xULN rise in ALT levels in healthy subjects. This effect was
most notable in the 2.5 mg dose group (see Figure 48).
Figure 48 – CS-0777; Alanine aminotransferase levels Source: ECTRIMS poster, Sep 2009

Page 66
In March 2008, a 12-week open label Phase I trial exploring the safety & tolerability and
MRI outcomes of escalating doses of CS-0777 in 18 MS patients began recruiting in five US
sites (see Figure 49).
Figure 49 – CS-077-A-U102 trial design Source: ECTRIMS poster, Sep 2009
Mar Jan2008 2010
CS-0777 0.1 mg
0.3 mg
0.6 mg
ministration
MRI
X = ad
X X X X X X X X X X X X
X X X X X X X X X X X X
X X X X X X X X X X X X
X X X X X X
X X X X X X
Mar Jan2008 2010
CS-0777 0.1 mg
0.3 mg
0.6 mg
ministration
MRI
X = ad
X X X X X X X X X X X X
X X X X X X X X X X X X
X X X X X X X X X X X X
X X X X X X
X X X X X X

Page 67
ONO-4641
Ono Pharmaceuticals, a Japanese firm, announced the start of a US-based Phase I trial with
ONO-4641 a low molecular weight, orally available S1P receptor agonist in November
2007. ONO-4641 is purported to reduce peripheral lymphocyte counts through sequestration
and so by reduce inflammation in auto-immune disorders. One year later ONO-4641
remained in Ono’s pipeline with the target indication of MS, however to date the selectivity
of this compound remains undisclosed as do the results from the Entry into Man (EIM) study
and any intentions to continue with clinical development.
Up and coming S1P agonists
In 2009 no less than 8 companies announced S1P agonists in development. This represents
an 11 fold increase from 2005 when Novartis was the only pharmaceutical company to lay
claim to the therapeutic effects of the S1P receptors. Table III demonstrates this growing
industrial interest.

Page 68
???, S1P1 selective agonist
???, S1P1 selective agonist
???, S1P1 selective agonist
PPI-4955, S1P1 selective agonist
???, S1P1 selective agonist
???, S1P1 selective agonist
???, S1P agonist
???, S1P agonist
Table IV – Phase 0 development of S1P agonists
Moreover MS is not the sole indication where inactivation of active inflammation promises
therapeutic benefit. Rheumatoid Arthritis, Crohn’s disease, Ulcerative Colitis, Psoriatic
Arthritis, Plaque psoriasis, Juvenile idiopathic arthritis, and Ankylosing spondylitis are all
autoimmune disorders successfully treated by administration of TNF-α antagonists such as
Humira® (adalimumab), Enbrel® (entanercept), Remicade® (infliximab). Over time
patients develop neutralizing antibodies and the efficacy of these biologics wanes allowing
the disease to relapse and persist. Due to the large protein structures of antibodies, biologics
by nature will always remain nettlesome parenterals. Still the annual revenue of the three
above mentioned TNF-α antagonists reached 11.8 bio USD in 2008. With these stakes, the
search for convenient oral agents will continue vigorously.

Page 69
Nrf2 activation
Nuclear factor 2 (Nrf2) is an intracellular transcription factor whose function has not been
completely elucidated. At present it has been implicated in cytoprotection via regulating the
expression of detoxification or antioxidant enzymes, tissue repair and plays a role in the
inflammatory response [26][27][28]. Targeting an intracellular process complicates the
search for a prospective agent as it must (1) be transported across the cell wall and (2)
remain selective for the desired pathway.
BG-12
Fumaderm® was first licensed in 1994 for use in the treatment of moderate-to-severe plaque
psoriasis exclusively in Germany however it was associated with undesired gastrointestinal
effects, i.e. diarrhea and nausea. Fumaderm® is primarily composed of a mixture of
dimethylfumarate and ethylhydrogenfumarate; in an effort to improve the tolerability profile
of fumarate therapy, BG-12 was designed as an oral presentation of dimethylfumerate ester
alone and is presently marketed in Germany as Panaclar® for use in the treatment of
psoriasis. In October 2003, Biogen Idec licensed the rights to develop and market BG-12
outside of Germany from Fumapharm AG following a successful Phase IIb study in
psoriasis. Immediately thereafter, Biogen Idec announced the start of a Phase IIb study in
MS. The Mechanism of Action (MoA) by which an oral fumerate offers therapeutic benefit
in either psoriasis or MS remains a mystery however it is claimed that BG-12 is a novel
immunomodulator which activates the Nrf2 pathway and so defends against oxidative-stress
induced by neuronal death, protects the blood-brain barrier, and supports maintenance of
myelin integrity in the central nervous system [30]. Work by Lukashev et al. in mice with
the experimental autoimmune encephalomyelitis (EAE) model appears to support the claim
[31].

Page 70
Clinical Development
Figure 50 – BG-12 MS development plan
In October 2008 Kappos et al. reported the findings of the 1-year Phase IIb MS trial in the
Lancet [32]. 257 RRMS patients were recruited into the study in the 5 months between
November 2004 and March 2005 at 26 sites within 11 countries ex-US and randomized to
receive either BG-12 at experimental doses of 120 mg once daily, 120 mg three times daily,
240 mg three times daily or placebo for the 1st six months. Thereafter the patients in the
placebo arm were re-randomized to the 240 mg TID group after an initial 2-week up-titration
period of 120 mg TID. Figure 51 depicts the trial design.
MAA MA LaunchMAA
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
C-1900
Define
Confirm
MA Launch
QTc study??
PoC
Avonex rescue therapy
Copaxone controlled

Page 71
BG-12 120 mg OD
120 mg TID
240 mg TID
Placebo
Double blind core study
scr x 3 4 5 6 mon 9 mon 1 yr
Study extension Nov Sep Mar 2004 2005 2006
Figure 51– BG-12; Phase IIb MS trial design Adapted from: Kappos et al., 2008. Efficacy and Safety of Oral Fumarate in Patients with Relapsing-Remitting Multiple Sclerosis: a Multicentre, Randomised, Double-blind, Placebo-controlled Phase IIb Study, The Lancet, 372 (9648), p. 1463-73
Primary endpoints
• total number of new Gd+ enhanced lesions at 3,4,5 & 6 months
Secondary endpoints
• total number of Gd+ enhanced lesions between 1-6 months
• total number of new & enlarging lesions on T2-weighted MRI images
• total number of new lesions on T1-weighted MRI images
Clinical endpoints
• annualized relapse rate
Only the 240 mg TID dose met the MRI endpoints showing a 69% reduction of the total
number of new Gd+ enhanced lesions, 44% reduction in the total number of Gd+ enhanced
lesions, 48% reduction in the total number of new & enlarging lesions on T2-weighted MRI
ECG
EDSS
MRI
//
up-titration step2 weeks @ 120 mg TID
BG-12 120 mg OD
120 mg TID
240 mg TID
Placebo
Double blind core study
scr x 3 4 5 6 mon 9 mon 1 yr
Study extensionNov Sep Mar
2004 2005 2006
//
ECG
EDSS
MRI up-titration step2 weeks @ 120 mg TID

Page 72
images and 53% reduction in the total number of new lesions on T1-weighted MRI images.
Although the study was not powered to detect a difference in annualized relapse rate (ARR)
between the active doses and placebo, a 32% reduction with the BG-12 240 TID dose group
was observed at 6-months. A progressive decrease in relapse rates was witnessed in all
groups in the 6-month extension phase potentially indicative of a delayed onset of action.
Figure 52 – BG-12; Phase IIb GD+ enhanced lesions at 6-months Source: Kappos et al., 2008. Efficacy and Safety of Oral Fumarate in Patients with Relapsing-remitting Multiple Sclerosis: a Multicentre, Randomised, Double-blind, Placebo-controlled Phase IIb Study, The Lancet, (372), p.1467
Reports of flushing, headache, nasopharyngitis, nausea, diarrhea, pruritus, and upper
abdominal pain were reported as adverse events (AE) in all dose groups with a higher
incidence in the 240 TID dose group. Increased liver enzyme levels of >2xULN were
reported in 19% of the patients in the highest dose group. More disturbing however were the
reports of MS relapse in up to 19% of patients in the highest dose group while on treatment.
No serious opportunistic infections or malignancies were reported.

Page 73
Following the closure of the Phase IIb trial, Biogen Idec initiated a robust registration
program with 2 confirmatory Phase III registration studies: DEFINE & CONFIRM.
DEFINE is a 2-year placebo-controlled trial evaluating the efficacy of BG-12 at 120 mg TID
versus 240 mg TID as measured by ARR, EDSS & MFSC scores and MRI endpoints.
DEFINE began to recruit the targeted 1,011 RRMS patients at 210 sites within 38 countries
in January 2007 – only 9 months after the Phase IIb results were available. CONFIRM is an
equally ambitious study which will compare the results of 2-year treatment with
experimental BG-12 doses of 240 mg BID or 240 mg TID against a daily subcutaneous
injection of 20 mg Copaxone® (glatiramer acetate) as defined by ARR, EDSS & MFSC
scores and MRI endpoints. This 1,232 patient study started to recruit in June 2007 at 209
sites within 35 countries worldwide. DEFINE and CONFIRM are projected to end in
December 2010 and June 2011 respectively.
To date Biogen Idec has not released any statement declaring intention to explore further MS
trials outside of RRMS, i.e. CIS, SPMS or PPMS, nor combination therapy in any of the MS
subtypes.
In December 2008 a Proof-of-Concept (PoC) trial began evaluating the effect of BG-12 at
240 mg BID and 240 mg versus placebo at 12 weeks in 150 Rheumatoid Arthritis patients at
24 sites within 6 countries ex-US.

Page 74
α4-integrin antagonists
Intergrins are receptors expressed on the exterior of the cell wall which mediate the cell
adhesion to other tissue surfaces. As lymphocytes must recognize and adhere to tissues in
the process of passing through the blood-brain barrier (BBB), antagonism of integrins
specific to trafficking T&B cells makes for logical targets in the search for safe & effective
MS therapies.
Tysabri® (natalizumab) a humanized monoclonal antibody which binds to α4-integrin
present on the exterior of lymphocytes, monocytes and eosinophils specifically hindering the
traffic of these cells inclusive of damaging T cells implicit in MS neuronal degeneration
across the BBB by antagonizing the VLA-4 receptor and thereby hindering the lymphocyte’s
ability to recognize & bind to vascular cell adhesion molecule-1 (VCAM-1) present on
vascular endothelial cells and is delivered by a monthly intravenous infusion. Launched in
late 2004 with a remarkable efficacy profile Tysabri® was recalled from the market within 6
months of launch due to 3 reports of progressive multifocal leukoencephalopathy (PML), a
potentially lethal infection of the brain’s white matter caused by the reactivation of latent
viral infection present in >80% of the population, while used in combination with Avonex®
an interferon-β. Re-launched in 2006 after restricting use to monotherapy and putting in
place a patient registry with rigorous monitoring & reporting requirements, Tysabri® has
grown from 21,000 patients exposed with 14,000 patients on treatment in 2007 to 43,300
patients exposed with 31,200 patients on treatment by the end of 2008; this represents a
growing retention rate from 66% to 72% at a time when four more cases of PML were
associated with Tysabri® monotherapy. Still the risk of PML after 18 months of continuous
monotherapy with Tysabri® has been estimated to be 1 in 1,000 whereas the prospect of
unrelenting debilitating progressive disability mounts with each day in an MS patient
irrespective of the treatment [33]. To date there have been 24 independent cases of PML
reported in association with Tysabri® treatment in either MS or Crohn’s disease.

Page 75
Laquinimod
Following the discontinuation of MS Phase III trials with LinomideTM (roquinimex) in 1997
by Pharmacia and Upjohn Inc. due to 2 reported cases of myocardial infarction, Active
Biotech AB partnered with Teva Pharmaceutical Industries Ltd to develop the successor
compound laquinimod. There are differing reports as to laquinimod’s MoA, as with
LinomideTM, it may induce a TH-1/TH-2 shift in the cytokines released by activated T cells
so by reversing the release of pro-inflammatory cytokines and encouraging proliferation of
cytokines which inhibit inflammation or as suggested by Teva in a release presented at the
American Academy of Neurology in 2009 data from a murine model laquinimod may act as
a very late adhesion-4 (VLA-4) antagonist [34][35]. This would make laquinimod the 1st
oral VLA-4 antagonist with the promise of Tysabri®-like efficacy. Laquinimod is a
quinolonecarboxamide which is associated with neither cardiac nor pulmonary disturbances.
Figure 53 – Laquinimod; chemical structure Source: http://journals.prous.com/journals/dof/20042903/html/df290253/images/282472.gif

Page 76
Clinical Development
Figure 54 – Laquinimod MS development plan
In 2008 Comi et al. reported on the outcomes of the dose-finding placebo-controlled 9-
month Phase IIb trial in 306 RRMS patients recruited at 51 centers within 9 countries [36].
Patients were randomized to receive either experimental doses of 0.3 mg OD or 0.6 mg OD
laquinimod or placebo. Figure 55 depicts the trial design.
MAA
2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
BRAVO
ALLEGRO
MA Launch
LAQ/5062
LAQ/5063 OL
Avonex & placebo controlled
LAQ/5061 ? PoC
CD-LAQ-201PoC Crohn‘s disease
MAA
2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
BRAVO
ALLEGRO
MA Launch
LAQ/5062
LAQ/5063 OL
Avonex & placebo controlled
LAQ/5061 ? PoC
CD-LAQ-201PoC Crohn‘s disease

Page 77
aquinimod 0.3 mg
0.6 mg
lacebo
Double blind core study
scr x 1 3 4 5 6 7 8 9 mon
Study extension
L P Figure 55 – LAQ/5062 trial design Adapted from: Comi et al., 2008. Effect of Laquinimod on MRI-monitored Disease Activity in Patients with Relapsing-remitting Multiple Sclerosis: a Multicentre, Randomised, Double-blind, Placebo-controlled Phase IIb Study. , Lancet, 371 (9630), p. 2085-92
Primary endpoint
• total number of Gd+ enhanced lesions at months 6, 7, 8 & 9
Secondary endpoints
• total number of Gd+ enhanced lesions at months 3, 4, 5, 6, 7, 8 & 9
• total number of new T2 lesions at months 6, 7, 8 & 9
• total number of confirmed relapses
Exploratory endpoints
• total number of new T1 lesions at months 6, 7, 8 & 9
• proportion of patients with no Gd+ enhanced lesions at months 7, 8 & 9
• proportion of relapse free patients
• time to first confirmed relapse
• disability progression (EDSS score)
• dynamics of MRI activity at months 3, 4, 5 & 6 compared to months 7, 8 & 9
MRI
Mar Aug Jun 2005 2006 2011
//
Double blind core study
scr x 1 3 4 5 6 7 8 9 mon
Study extension
EDSS
//
ECG
Laquinimod 0.3 mg
0.6 mg
laceboP
MRI
Mar Aug Jun 2005 2006 2011
//
Double blind core study
scr x 1 3 4 5 6 7 8 9 mon
Study extension
EDSS
//
ECG
MRI
Mar Aug Jun 2005 2006 2011
////
EDSS
ECG

Page 78
Only the 0.6 mg OD dose met the primary endpoint demonstrating a 40.4% (p=0.0048)
reduction compared to placebo in the cumulative number of Gd+ enhanced lesions as
measured from baseline and the last 4 MRI scans (see Figure 56). The high dose continued
to show a statistically significant reduction of 51% (p=0.0001) in the total number of Gd+
enhanced lesions when the MRI scans from months 3, 4 & 5 were included in the analysis.
A 44% reduction (p=0.0013) in the total number of new T2 lesions at months 6, 7, 8 & 9 was
also reported with daily administration of 0.6 mg laquinimod. A non-statistically significant
reduction of 32.5% at 6-months was reported with 0.6 mg OD with further trends also
observed with this dose in the outcomes of all exploratory endpoints with the exception of
disability progression as measured by EDSS scores. Chest pain, viral infections and elevated
liver enzymes were reported in patient on active treatment, however the use of laquinimod
was generally considered safe and well-tolerated.
Figure 56 – Laquinimod; reduction of T1 GD+ enhanced lesions at 9-months Source: 2008 Active Biotech AB, Rodman & Renshaw 10th annual healthcare conference

Page 79
In September 2007 ALLEGRO a 2-year placebo-controlled Phase III registration trial to
evaluate the efficacy & safety of 0.6 mg laquinimod began to recruit its targeted 1,000
RRMS patients at 152 sites within 25 countries worldwide. Shortly thereafter in April 2008
BRAVO the 2nd confirmatory Phase III 2-year controlled trial comparing the efficacy &
safety of 0.6 mg laquinimod against both Avonex® (interferonβ-1a) and placebo began to
recruit 1,200 RRMS patients at 137 sites within 18 countries. Both ALLEGRO and BRAVO
have completed recruitment and results are expected in March 2011 and June 2011
respectively.
At present no prospective trials with laquinimod either in combination with other therapies
or as monotherapy in other MS subtypes are planned.

Page 80
Firategrast Mitsubishi Tanabe partnered with Glaxo Smith Kline to develop Firategrast, a prodrug and
low molecular weight oral very late adhesion-4 (VLA-4) antagonist. An open label four-way
crossover trial in 37 MS patients comparing the pharmacokinetic profile of 900 mg
firategrast in 3 different tablet formulations was conducted between April and November
2007 at 4 sites within 3 countries. In parallel an open label Phase II trial which evaluated the
effect of an undisclosed dose of firategrast on the lymphocyte levels in the cerebrospinal
fluid (CSF) of 47 MS patients began in July 2007. Neither of these trials alone can be
considered critical to the development of firategrast, however they are representative of the
stage of development which firategrast has achieved. Figure 57 illustrates firategrast’s
estimated development path assuming that the later Phase II trial in combination with the
results from a larger controlled Phase IIb trial will be essential in determining the
experimental doses evaluated in two 2-year Phase III registration trials.
Clinical Development
Figure 57 – Firategrast MS development plan
MAA
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
A4M1XXXXX ?
A4M108119
MA Launch
A4M109079
A4M1YYYYY ?
683699/003
A4M105038
MAA MA LaunchMAA
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
A4M1XXXXX ?
A4M108119
A4M109079
MA Launch
A4M1YYYYY ?
683699/003
A4M105038

Page 81
In fact a Phase IIb trial in 350 RRMS patients comparing firategrast experimental doses of
150 – 900/1,200 mg BID against placebo is reportedly being conducted in 13 countries ex-
US with results available at the end of 2009. The same source cites a completed massive
Phase I trial conducted in 194 healthy volunteers exploring doses up to 1,600 mg BID for 28
days; firategrast apparently has a t1/2 supporting BID dosing with no accumulation of either
the parent compound or the active metabolite [37].
CDP-323
UCB and Biogen Idec collaborated to develop CDP-323, another low molecular weight,
orally available agent α-4 integrin antagonist which later demonstrated no gender effect,
successfully hampered the traffic of T cells, and was well tolerated at up to 1,000 mg BID
administered for 7 days with an adverse event profile comparable to placebo. In July 2009
UCB announced that the Phase IIb dose-finding study in 279 RRMS was stopped due to a
lack of efficacy at the 1st interim analysis. No cases of PML were reported. Given the
relative success of Tysabri® the failure of CDP-323 is somewhat counterintuitive, however
the results of the firategrast Phase IIb RRMS trial may shed light on the feasibility of oral α-
4 integrin antagonists.

Page 82
MS biologics; global market
0
0.5
1
1.5
2
2.5 Figure 55– Biologic MS therapy; annual revenues 2006-2008 Adapted from: Annual reports 2006-2008; Teva Pharmaceutical Industries Ltd, Biogen Idec Inc, Bayer AG, Merck KGaA
2006 2007 2008
CopaxoneAvonexRebif BetaseronTysabri
BillionUSD
Annual revenues(with year-on-year growth %)
638
156
19
3218
9
10
9
92
11
0
0.5
1
1.5
2
2.5
CopaxoneAvonexRebif BetaseronTysabri
BillionUSD
Annual revenues(with year-on-year growth %)
638
156
19
3218
9
10
9
92
11
2006 2007 2008

Page 83
Copaxone
Figure 56 – Biologic MS therapy; market share 2006-2008 Calculated from: Annual reports 2006-2008; Teva Pharmaceutical Industries Ltd, Biogen Idec Inc, Bayer AG, Merck KGaA
AvonexRebifBetaseronTysabri
CopaxoneAvonexRebifBetaseronTysabri
2006
CopaxoneAvonexRebifBetaseronTysabri
2007
2008
8.7 bio USD
6.83 bio USD
5.37 bio USD
26%32%27%14%~1%
25%28%24%20%
3%
26%25%22%19%7%
Market capitalization
CopaxoneAvonexRebifBetaseronTysabri
CopaxoneAvonexRebifBetaseron
CopaxoneAvonexRebifBetaseronTysabri
2006
Tysabri
2007
2008
8.7 bio USD
6.83 bio USD
5.37 bio USD
26%32%27%14%~1%
25%28%24%20%
3%
26%25%22%19%7%
Market capitalization

Page 84
Market exclusivity
Supplementary Patent Certificate (SPC)
To partially compensate the pharmaceutical industry in the EU for the patent time lost
between the filing of a patent and the eventual approval for sale the EEC passed COUNCIL
REGULATION No 1768/92 on the 18th June, 1992 which allowed for a maximum extension
protection period of 5-years in addition to the first protective patent to expire; the combined
patent life and the SPC extension is not to exceed a total of 15 years of market exclusivity.
Both the SPC and period of market exclusivity can be extended a further 6 months in the
case that the sponsor completes the actions outlined in an approved Paediatric Investigational
Plan (PIP).
Patent Term Extension (PTE)
The US Patent and Trademark Office offers a patent term extension of any patent which
provides protection for the 1st approval of a new chemical entity (NCE) and is equivalent to
½ the IND period plus the NDA review period and capped at a maximum of 5 years in total;
the PTE shall also not result in more than 14 years of protection from the time of the 1st MA.
As in the EU a 6-month patent extension is offered for the development of a licensed
paediatric formulation.
Data exclusivity
The EMEA also provides a period of 10 years from the approval of the 1st Marketing
Authorization Application (MAA) to compensate industry for the time lost in the review
periods associated with each individual Clinical Trial Application (CTA) and the MAA. In
this time the EMEA will not allow any other company other than the Marketing
Authorization Holder (MAH) to make reference to the data contained within the MAA. This
usually results in market exclusivity as a standard bio-equivalence bridging study would no
longer be sufficient to launch a generic; an entire clinical development program would have
to be conducted to generate sufficient data for filing. In a similar spirit the FDA provides

Page 85
01-Apr-14not eligible26-Mar-2401-Jun-1026-Mar-04
US 2007065492US 2007/0197468
(oral formulation,not yet granted)Cladribine
01-Apr-1801-Feb-2715-Apr-2201-Apr-1301-Apr-02US 6794410Teriflunomide
01-Feb-1801-Nov-2322-Apr-1901-Feb-1322-Apr-99US 6077851Laquinimod
01-Apr-1701-Jan-2318-May-2001-Apr-1229-Oct-99US 7320999BG-12
01-Dec-1518-Feb-1918-Feb-1401-Dec-1018-Oct-93US 5604229FTY-720
Dataexclusivity(estimated)
PTE(estimated)
Use in MS
patentexpiry
Parentpatentexpiry
Market authorisation(estimated)
Use in MS
patentfiling
Use in MS
patent #
ParentpatentfilingParent patent #Compound
01-Apr-14not eligible26-Mar-2401-Jun-1026-Mar-04
US 2007065492US 2007/0197468
(oral formulation,not yet granted)Cladribine
01-Apr-1801-Feb-2715-Apr-2201-Apr-1301-Apr-02US 6794410Teriflunomide
01-Feb-1801-Nov-2322-Apr-1901-Feb-1322-Apr-99US 6077851Laquinimod
01-Apr-1701-Jan-2318-May-2001-Apr-1229-Oct-99US 7320999BG-12
01-Dec-1518-Feb-1918-Feb-1401-Dec-1018-Oct-93US 5604229FTY-720
Dataexclusivity(estimated)
PTE(estimated)
Use in MS
patentexpiry
Parentpatentexpiry
Market authorisation(estimated)
Use in MS
patentfiling
Use in MS
patent #
ParentpatentfilingParent patent #Compound
01-Apr-2118-Feb-1801-Jun-1018-Feb-93EP 0626853Cladribine
01-Apr-2304-Apr-2704-Apr-2201-Apr-1304-Apr-02EP1935416
(not yet granted)Teriflunomide
01-Feb-2326-Apr-2426-Apr-1901-Feb-1326-Apr-99EP 1073639Laquinimod
01-Apr-22not eligible29-Oct-1901-Apr-1229-Oct-99EP 1131065BG-12
01-Dec-2018-Oct-1818-Oct-1301-Dec-1018-Oct-93EP 0627406FTY-720
Dataexclusivity(estimated)
SPC(estimated)
Use in MS
patentexpiry
Parentpatentexpiry
Market authorisation(estimated)
Use in MS
patentfiling
Use in MS
patent #
ParentpatentfilingParent patent #Compound
01-Apr-2118-Feb-1801-Jun-1018-Feb-93EP 0626853Cladribine
01-Apr-2304-Apr-2704-Apr-2201-Apr-1304-Apr-02EP1935416
(not yet granted)Teriflunomide
01-Feb-2326-Apr-2426-Apr-1901-Feb-1326-Apr-99EP 1073639Laquinimod
01-Apr-22not eligible29-Oct-1901-Apr-1229-Oct-99EP 1131065BG-12
01-Dec-2018-Oct-1818-Oct-1301-Dec-1018-Oct-93EP 0627406FTY-720
Dataexclusivity(estimated)
SPC(estimated)
Use in MS
patentexpiry
Parentpatentexpiry
Market authorisation(estimated)
Use in MS
patentfiling
Use in MS
patent #
ParentpatentfilingParent patent #Compound
five-years data exclusivity for any NCE receiving its 1st Marketing Authorization (MA) and
3 additional years of any subsequent indications.
Table V – Protection of MS agents in clinical development (EU)
Table VI – Protection of MS agents in clinical development (US)
The ability of pharmaceutical firms to regenerate the billions spent in the development of a
pipeline relies on the respect of intellectual property (IP) rights and these extension periods
can encourage further investment in projects whose Net Present Value (NPV) would not
make them attractive enough to warrant the considerable expense otherwise.

Page 86
DISCUSSION
Mylinax® (Cladribine) Clearly the leader in the race to license oral therapy for the treatment of MS, Merck Serono
has filed MAAs at both the EMEA and the FDA with an impressive efficacy read-out
(reductions of 58% ARR and 31% disease progression at 2-years with the low dose);
however with four malignancies in different tissue types reported including a fatality, there is
cause to revisit the safety findings with an eye to both the Mechanism of Action (MoA) and
pharmacokinetic/pharmacodynamic (PK/PD) profile.
Given the reported t½ of 6 to 8 hours, systemic clearance would be achieved within 2 days
however the lymphocyte reductions are maintained over a period long enough to warrant an
annual dosing regimen in MS. This could only be the case if intracellular accumulation of
cladribine spared the parent compound from metabolism and renal clearance. Is it at all
plausible to presume that although cladribine breaches the cell wall of countless cell types in
the body, its active metabolite uniquely inhibits DNA repair & replication exclusively in
lymphocytes due to the exceptional circumstance of a favorable balance between
deoxycytidine kinase (DCK) levels and those of deoxynucleotide dephosphorylating
enzymes?
Furthermore cladribine has been shown to deplete not only the T&B cell populations but also
the natural killer cell levels as well. NK cells are a part of the innate immune system and not
associated with a misdirected attack on neurons by T&B cells as witnessed in MS; however
NK cells play a distinct role in the body’s general immuno-surveillance & defense against
pathogens, e.g. opportunistic viral infections and malignancies.

Page 87
Lastly cladribine is poorly reversible; it is a matter of fire and forget for the next year. All
four cases of malignancies and the one case of reactivated tuberculosis infection were
attributed to active treatment with cladribine; no events of a similar nature were reported in
the placebo arm.
Although the FDA guidance calls for a minimum of 2 confirmatory Phase III trials prior to
registration and the EMEA prefers at least 1 of these trials to be comparator-controlled, it is
possible to register with only a single trial when compelling statistical significance and a
favorable risk:benefit profile is achieved within a patient population appropriately large
enough to detect infrequent safety signals. Merck Serono has taken a significant risk in
filing with a single Phase III RRMS trial; however the clinical efficacy demonstrated by
cladribine far exceeds that achieved by standard therapy with interferonβ, the patient
exposure-years requirements have been met and with p values <0.001 the statistical
significance of the results can be considered sound. Moreover to satisfy pharmacovigilance
expectations and better ascertain the risks associated with opportunistic infections,
malignancies and teratogenicity in exposed patients, Merck Serono has proactively put in
place a registry study which will monitor for emergent safety signals. Regulators are likely
to grant cladribine approval in 2010.
Should cladribine prove effective in delaying the time towards disease progression in both
CIS & RRMS as well as safe in combination with interferon-β therapy in RRMS & SPMS,
cladribine will establish itself as a formidable therapeutic agent in the treatment of Multiple
Sclerosis.
The question remains to what degree practicing neurologists will feel comfortable
prescribing a cytotoxic to young fertile women, and to what degree their patients will
demand cladribine as routine therapy.

Page 88
Teriflunomide With only the Phase IIb data from 177 RRMS patients available the long term efficacy and
safety profile of teriflunomide will remain difficult to assess. Certainly achieving a 40 to
60 % reduction in combined unique lesions at 9-months with 7 mg and 14 mg once daily
active treatment along with the 32% and 69% reductions in ARR and worsened disability
with the 14 mg OD dose places teriflunomide in a favorable light, yet the statistical
significance of these results remains to be substantiated in the larger 2-year Phase III trials
TEMSO & TOWER.
As the active metabolite of leflunomide, teriflunomide shares a similar MoA which is also
not without suspicion. Teriflunomide targets rapidly dividing cells and inhibits de-novo
DNA repair & replication; like cladribine the target is an intracellular process common to all
dividing cells and also like cladribine, teriflunomide is a cytotoxic. The safety & tolerability
of teriflunomide at 9-months was reported to be indistinguishable from placebo; however as
9-months is too short a period to monitor the long term immunosuppressive or mutagenetic
effects, a glance at the safety & tolerability profile of Avara® (leflunomide) may be justified.
Avara® has been associated with hepatotoxicity (inclusive of fatalities), haematotoxicity,
opportunistic infections (inclusive of tuberculosis), interstitial lung disease, gastrointestinal
tract disorders and allergic reactions. The long term efficacy and safety & tolerability profile
of teriflunomide will only become available after the completion of TEMSO in 2011.
It is important to note that following the Phase IIb trial, Sanofi-Aventis did not prune either
of the doses and that all of the ongoing clinical investigations are evaluating both the 7mg
and 14 mg OD doses. This may further complicate registration in terms of determination of
lowest effective dose, and the cumulative patient exposure years & associated safety signals
at the suggested marketed dose.

Page 89
If positive the PoC trials assessing the safety & tolerability and efficacy in combination with
Rebif® and Copaxone® will form a part of the submission package for registration; not only
might these trials assist to overcome any shortcomings in terms of patient exposure,
combination therapy help teriflunomide to penetrate what will be a crowded and small
market. TOPIC the Phase III CIS trial it is unlikely to form a part of the initial MAA
package, however if positive this trial could prove to be the first line-extension for
teriflunomide.
Fingolimod Certainly the reductions of 54% in ARR and 30% in disability progression achieved with 0.5
mg fingolimod at 2-years are stunning; however the therapeutic promise appears to be
largely comparable with that offered by cladribine. The safety & tolerability profiles, e.g.
comparative incidence of opportunistic infection, malignancy (inclusive of etiologies),
macular edema, cardiac & pulmonary disturbances and death, will differentiate these two
agents. At first glance fingolimod’s MoA speaks for a greater degree of safety as the
function of sequestered T&B cells is not affected and fingolimod does not enter and
interfere with DNA repair & replication processes in multiple cell types in the body.
Fingolimod like cladribine crosses the BBB, per contra fingolimod’s efficacy may partly be
related to remyelinating properties purported with S1P5 agonism. Also in contrast to
cladribine, fingolimod does not affect the levels of peripheral NK cells.
Having overcome the hurdle first dose transient bradycardia posed, the lower fingolimod
dose has consistently demonstrated comparable efficacy with a favorable safety profile over
the higher doses. It would be safe to assume that 0.5 mg fingolimod will be the MAA’s
recommended dose. The safety profile of the 0.5 mg dose in the 2-year FREEDOMS trial
paradoxically appears to improve from what was previously reported in the 1-year
TRANSFORMS trial. In the absence of the FREEDOMS II trial results the true hazards

Page 90
posed by the safety concerns of macular edema, opportunistic infections and malignancies
will remain difficult to quantify. Although malignancies and opportunistic infections are
resilient disorders and fingolimod’s average t½ of 8.8 days does little to assist in providing a
rapid restoration of functioning lymphocytes upon diagnosis, it may offer a distinct benefit
as compared to the time it takes to systemically clear cladribine under similar circumstances.
Increased mean arterial blood pressure has been reported with 0.5 mg fingolimod persistent
at 2-years; this may lead to contraindications and/or warnings for patients at higher risk
which in today’s society may not be such a negligible number.
Given the safety findings and the fact that throughout the clinical development program the
lowest efficacious dose was not identified, the granting of Marketing Authorization (MA)
may still prove problematic. However as fingolimod is the only compound in development
with a safety database consisting of 1,000’s of patient years based on its clinical experience
in transplant rejection and three Phase III trials in MS, it is likely that Novartis may have a
speedier approval than Merck Serono and fingolimod could reach the market alongside
cladribine; its shorter t½ may prove a sincere boon should clever use of diagnostics and
undulating therapy regimens allow physicians to remove patients from the risks of
immunosuppression and still maintain a high degree of efficacy. Currently Novartis has yet
to put in place a high profile pharmacovigilance registry but it can be assumed that the
pooled safety findings from the various open label extension trials will serve the purpose and
that as a post-approval obligation such a registry is likely to be established.
BAF312 The so called “son of fingolimod” may indeed live up to its reputation as its dual S1P1/5
selectivity has already proven effective in limiting first dose transient bradycardia, reducing
T&B cell lymphocyte subsets without affecting NK cells, monocytes or granulocytes and the
rapid return of the diminished lymphocytes to the peripheral blood supply due to the greatly

Page 91
reduced t½ (~30 hrs). Novartis has unburdened the dose determination of BAF312 and
challenged conventional view of linear clinical development. However basing the doses on
fingolimod’s efficacy and tolerability profile may prove foolhardy if in fact direct effects on
the brain tissues and not the sequestration of lymphocytes are directly responsible for the
clinical benefits in MS.
ACT-128800 Jointly developed with Roche since 2006, Actelion’s selective S1P1 receptor agonist has just
entered the clinical arena. Following fingolimod’s lead it selectively sequesters T&B cells
through the same MoA and neck-in-neck with BAF312 it nonetheless remains a serious
contender. Nothing is known about its effects upon multiple dosing or over extended periods
of time, however as the first patient in a Phase IIb MS trial has successfully been enrolled the
safety & tolerability profile must be sufficient to warrant further development in a disorder
whose treatment is lifelong. Should direct actions in the brain prove to contribute to the
success of a non-selective S1P agonist in MS, it remains to be seen what advantages ACT-
128800’s profile as a selective S1P1 agonist would offer; that said Tysabri®’s unequalled
efficacy in MS is derived entirely from hindering the traffic of lymphocytes across the BBB.
CS-0777 Daiichi Sankyo’s fist selective S1P1 receptor agonist has a 300 fold greater S1P1>S1P3
selectivity than fingolimod, however BAF312 lays claim to a >1,000 fold S1P1>S1P3
selectivity. How can it be that BAF312 has a >3 fold higher selectivity profile and reports
bradycardia at every dose yet with CS-0777 first dose bradycardia is limited to the top dose
of 2.5 mg? Paradoxical as it may seem, cross-investigational comparisons are discouraged;
it is quite likely that the assays used to determine these sensitivities vary from each other and

Page 92
therefore although the results of fingolimod vs. either BAF312 or CS-0777 are valid,
comparisons of BAF312 vs. CS-0777 should not be avoided. Given that the t½ of CS-0777
was determined to be 7.3 days complete systemic clearance could be expected to take more
than 1 month. Although CS-0777 does not appear to affect the function of lymphocytes, a
rapid and full restoration of the immune system does not appear promising; lymphocyte
counts remained below baseline 13 days following the administration of a single dose.
The small patient population will restrict these findings to an exploratory MAD trial in MS
patients, however if followed by an aggressive Phase IIb/III registration trial, CS-0777 could
indeed spring forward ahead of its peers
BG-12 Neither an anti-proliferant/replicant nor a lymphocyte sequestering agent, BG-12 and its
MoA continue to mystify the inquisitive. Biogen Idec asserts that neuroprotection is
mediated by Nrf2 activation with BG-12; however no such pathway has been identified to
explain the immunomodulation claims set forth by Biogen Idec. Irrespective from all of the
oral therapies in development, BG-12 appears to be the most benign offering a meager 32%
reduction in relapse rate at 6-months with a more acceptable safety & tolerability profile with
240 mg TID. Although there is speculation that 6-months is insufficient for BG-12’s full
therapeutic benefit to manifest, the sense of optimism should be balanced by the reports of
relapses while on treatment. Three times daily administration is not as convenient as annual
treatment with cladribine or once daily fingolimod, however to date there have been no
reports of opportunistic infections or malignancies. As with Fumaderm® reports flushing
and GI tract disturbances continue to shadow BG-12 and long-term efficacy and safety &
tolerability have yet to be established. As two large 2-year registration trials comparing the
use of BG-12 against placebo and Copaxone® respectively, DEFINE & CONFIRM will
only begin to define BG-12’s long term safety profile.

Page 93
Laquinimod Another successor molecule and yet another uncertain MoA, laquinimod either initiates a
Th1-Th2 shift in the same manner as Linomide® (roquinimex) before it, or it is a VLA-4
antagonist which inhibits lymphocyte trafficking across the endothelial layer of blood vessels
like Tysabri®. Phase III clinical investigations with Linomide® in MS patients were
terminated due to serious cardiopulmonary toxicities, pancreatitis, and fatalities within the 1st
month of conduct [38]. Laquinimod passed the 1-month hurdle and was generally well
tolerated in a 9-month Phase IIb trial. Daily administration of 0.6 mg, the highest dose of
laquinimod demonstrated a 51% reduction in the total number of Gd+ enhanced lesions at 9-
months against placebo and a non-statistically significant 32.5% reduction in relapse rate at
9-months. Long term efficacy and safety & tolerability data are presently being accumulated
with ALLEGRO and BRAVO, two large 2-year registration trials against placebo and
Avonex® respectively.
Laquinimod may prove an effective therapy in the treatment of RRMS, however without
further trials to assess the safety and efficacy of combination therapy and explore the
therapeutic benefit in other MS subtypes both market entrance and penetration may be
hindered.
Firategrast An oral α4-integrin antagonist would be a welcome addition to the cornucopia of potential
oral candidates for use in the treatment of MS. It is simply too early to evaluate firategrast’s
chances, however with the recent failure of another oral α4-integrin antagonist, CDP-323,
firategrast’s prospects are not unusually bright at the moment.

Page 94
CONCLUSION
Multiple Sclerosis is divided into subtypes varying in severity and supporting a range of
differing risk:benefit profiles. Agents best suited to each subtype will comprise the future
neurologist’s arsenal. None of the compounds reviewed will be used in every form of MS at
every stage in a patient’s life. Efficacy in reducing relapses and preventing disease
progression along with the associated safety & tolerability profile will serve to aggregate the
future market into three categories: (1) lower broadband efficacy with a more acceptable
safety profile, (2) resounding efficacy in reducing inflammation, relapses and disease
progression with a heavier safety burden inclusive of extensive, regular monitoring, and
finally (3) outstanding efficacy associated with general systemic risks.
The low efficacy broadband orals will challenge the interferonβ therapies of today in the
twilight of their respective IP protection periods and offer equal efficacy with low risks to
the patient’s general well-being and convenient oral formulations. Compounds such as
Mylinax® (cladribine) and fingolimod will compete with Tysabri® offering the future
neurologist with an effective means to control relapsing forms of MS, hinder disability
progression and potentially halt the diagnosis of CDMS in CIS patients. Finally agents such
as Campath® will be the last resort when all else fails and disease progression cannot be
controlled by any other means.
At nearly 9 bio USD per annum the market value is high and the market entrance of
Tysabri® attests to the elasticity of the MS market; in the 3 years following its re-
introduction Tysabri®’s market share increased from below 1% to 3% and finally 7% in face
of reports of escalating cases of confirmed PML associated with monotherapy. Efficacy
drives the MS market and the patients indeed place pressure on their neurologists for the
therapy they believe to be best suited to their current therapeutic needs.

Page 95
Exempting the circumstance in which new and as of yet unidentified MoAs promise better or
safer clinical efficacy against the currently identified therapies, further trials assessing the
comparative efficacy of combination therapy will be confined to the outer fringes of a
MS subtype when clinical exacerbations are building in magnitude and frequency, i.e. the
patient’s disease progresses.
With Betaseron®, Rebif®, Avonex® and most recently Copaxone® already licensed for the
treatment of Clinically Isolated Syndrome (CIS) and Mylinax® (cladribine) & teriflunomide
actively recruiting patients into CIS trials, the oral treatment paradigm will also broaden to
start with early and potentially aggressive therapy. As 33-50% of CIS patients reach a
diagnosis of clinically definite MS and 80% of RRMS patients were previously diagnosed
with CIS, oral agents which have been proven to be effective in controlling the inflammatory
component of RRMS could prove efficacious in preventing a CDMS diagnosis or delaying
the time to onset. Once the long term safety profiles of both Mylinax® (cladribine) &
teriflunomide are established, orals may again infiltrate an exclusively parenteral market
offering equal or better efficacy without the pin prick.
Mylinax® (cladribine) and fingolimod will be the first oral agents approved for the treatment
or relapsing MS in 2010. Should the Phase III programs of teriflunomide, laquinimod and
BG-12 support licensing, a 2nd wave of oral products would enter between 2013-2014 and
further crowd a tight market. Assuming that the preliminary efficacy in terms of ARR &
EDSS scores do not improve, i.e. remain below that achieved with Mylinax® (cladribine) &
fingolimod, they will form the low efficacy broadband component and compete exclusively
with all forms of interferonβ therapy.
BAF312, ACT-128800 and firategrast are projected to form the 3rd phase of the oral
revolution exempting unforeseen safety events and arrive perhaps in 2017. Novelty,
efficacy, safety & differentiation determined in their Phase III programs will drive this lot
more than any of their predecessors in an effort to carve a niche in what may be a rather

Page 96
congested marketplace just prior to 2019 when fingolimod will be the first oral to lose IP
protection. The clinical development programs of these agents in particular may drive the
use of novel MRI scanning techniques along with monitoring for biomarkers and potentially
genetic screening in the effort to better identify & diagnose high risk patients in every stage
of MS and offer the best corresponding treatment. These marketing claims could further
differentiate new oral MS therapies from those previously launched. Furthermore cost
effectiveness and patient access may also prove effective in strategically positioning
clinically non-differentiated products.
However these predictions would be made ignoring the hurdle of recruitment and the results
of historical drug development. Neither the prevalence of MS nor the annual incidence of
exacerbations & disease progression is growing as rapidly as the number of agents promising
therapeutic benefit. Recruitment is based on the availability of patients who are either
treatment naïve, dissatisfied with or unable to afford their current therapy. As novel,
convenient and effective therapies become commercially available, there will be less
incentive for satisfied patients to enter clinical trials which may require them to switch
treatment to an agent which may prove potentially less effective, tolerated or safe, or risk
being randomized to a placebo arm in a double-blind study. The recruitment approximations
used to guide this analysis may indeed be too optimistic to meet with expectations.
Historically just half of the CNS compounds in Phase II enter Phase III where only two
thirds successfully submit Manufacturing Authorization Applications (MAA) with the
Health Authorities (HA) worldwide, and from these roughly one quarter fail to receive
Manufacturing Authority (MA). This comes to an overall success rate of 50% for those
reaching Phase III and only 22% for those compounds entering Phase II. From this analysis
teriflunomide, laquinimod, BAF312, & ACT-128800 show the highest probability of success
with BG-12, firategrast and CS-0777 currently ranking the lowest. Although clinical results
will eventually confirm or contradict this prediction, it can still be assumed that between a

Page 97
quarter and one half of the all 10 remaining candidates identified will never reach the
pharmacopeia.
Table VII – Drug development success rates
Disease Group Clinical Phase I
Clinical Phase II
Clinical Phase III
Marketing Approval
Cumulative %
Arthritis/Pain 76.9% 38.1% 78.1% 89.1% 20.4% CNS 66.2% 45.6% 61.8% 77.9% 14.5% CV 62.7% 43.3% 76.3% 84.4% 17.5% GIT 66.8% 49.1% 71.0% 85.9% 20.0% Immunology 64.8% 44.6% 65.2% 81.6% 15.4% Infections 70.8% 51.2% 79.9% 96.9% 28.1% Metabolism 47.8% 52.0% 78.9% 92.8% 18.2% Oncology 64.4% 41.8% 65.4% 89.7% 15.8% Ophthalmology 66.0% 39.0% 64.0% 92.0% 15.2% Respiratory 63.4% 41.1% 59.9% 76.9% 12.0% Urology 50.0% 38.0% 67.0% 79.0% 10.1% Women’s Health
39.0% 42.0% 48.0% 59.0% 4.6%
Source: DeMasi 2001, Kola 2004, Avance cited in Valuation in Life Sciences, 2007, p.14)
The IP protection of all the compounds reviewed does rule out generic competition at launch
for any of the potential candidates which are granted a license. As witnessed from the recent
EU condoned joint venture between Teva Pharmaceutical Industries and Lonza Group
biologics will face tough competition from biosimilars [39]. Novartis, the first
pharmaceutical company to launch its own biosimilar for use in MS, Extavia® (Betaseron®;
interferon β-1b), has demonstrated that the market price of a biosimilar can be expected to
retain ~80% of the sale price of the patented originator [40]. This will allow all the oral
compounds in clinical development today for the treatment of MS reaching the market to
demand a high return and further drive the R&D efforts to identify, develop and
commercialize even better compounds.

Page 98
This however is not the final revolution in MS therapy. The agents licensed for therapy and
those in development all concentrate on the inflammatory component of MS which can be
evaluated by means of MRI. MRI is used in Phase IIb trials to identify the “correct” dose;
however this is simply because the compound’s target happens to be the inflammatory
component of MS. Looking back at Figure 1 it is clear that the peaks represent clinical
exacerbations which are related to inflammatory flares and that preventing their recurrence
impedes disability progression; in effect it merely reduces the slope of the line over time.
Recent studies have shown that a degree of inflammation may indeed be required to promote
the migration of monoculear phagocytes to sites of neuronal damage and remyelination [41].
It may be that a MS patient is best served by a balance between the neuroprotection provided
by immunomodulation and natural neuroregeneration processes.
Significant inroads have already been made in propagating the neuroregeneration promise of
remyelination. Targeting the migration, proliferation, and differentiation of oligodendrocyte
precursor cells (OPC) through receptors expressed on OPC, e.g. interleukin 8 receptor β
(CXCR2), is one such option. Hyaluronan is a non-sulfated glycosaminoglycan produced by
astrocytes and found in higher concentrations in demyelinated lesions. As lower rates of
OPC maturation are noted in the presence of hyaluronan, reduction or inactivation of
hyaluronan offers another opportunity to enhance remyelination [42]. Lastly investigations
in the rat have demonstrated positive results with intravenously administered neural stem
cells; adhesion molecules specific to neuronal damage present on these cells allow them to
circulate systemically and selectively attach to lesions where their therapeutic benefit can
hopefully be harnessed [43].
The true revolution will follow in the wake of scientific reason’s harsh discernable light
exposing the insidious component which principally instigates neuronal degradation in MS
patients.

Page 99
REFERENCES
1. Dyment et al., 2004. Genetics of Multiple Sclerosis, Lancet Neurology, 3 (92), p. 104-10 2. Ascherio A & Munger KL, 2007. Environmental Risk Factors for Multiple Sclerosis. Part I: the Role
of Infection, Annals of Neurology, 61 (4), p. 288-99 3. Pöllinger et al., 2009. Spontaneous Relapsing-remitting EAR in the SJL/J Mouse: MOGreactive
Transgenic T Cells Recruit Endogenous MOG-specific B Cells, Journal of Experimental Medicine, 206 (6), p. 1303-16
4. Rosati G, 2001. The Prevalence of Multiple Sclerosis in the World: an Update, Neurological Sciences, 22 (2), p. 117-39
5. Barkhof F, 2002. The Clinico-radiologicla Paradox in Multiple Sclerosis Revisited, Current Opnion Neurology, 15 (3), p. 239-45
6. Cohen J et al., 2001. Use of the Multiple Sclerosis Functional Composite as an Outcome Measure in a Phase 3 Clinical Trial, Archives of Neurology, 58, p. 961-7
7. http://www.tevapharm.com/pr/2008/pr_747.asp; accessed on 25Sep2009 8. Sipe JC, 2005. Cladribine for Multiple Sclerosis: Review and Current Status, Expert Review
Neurotherapeutics, 5 (6), p. 721-27 9. Leist & Vermersch, 2007, The Potential Role of Cladribine in the Treatment of Multiple Sclerosis;
Clinical Experience and development of an Oral Tablet, Current Medical Research and Opinion, 23 (11), p. 2667-76
10. http://www.medscape.com/viewarticle/702193; accessed on 25Sep2009 11. http://www.bloomberg.com/apps/news?pid=20601100&sid=aFPM5GZtruUU&refer=germany;
accessed on 02Feb2009 12. O’Connor et al., 2006. A Phase II Study of the Safety and Efficacy of Teriflunomide in Multiple
Sclerosis with Relapses, Neurology, 66, p. 894-900 13. Im, 2003. Linking Chinese medicine and G-protein-coupled receptors, Trends in Pharmacological
Sciences, 24 (1), p. 2 14. Adachi, K. Chiba, K., 2007. Perspectives in Medicinal Chemistry, 1, p. 11-23 15. Paugh SW et al., 2006. Sphingosine and Its Analog, the Immunosuppressant 2-amino-2-(2-[4-
octylphenyl]ethyl)-1,3-propanediol, Interact with the CB1 Cannabinoid Receptor, Molecular Pharmacology 70, p. 41-50.
16. Payne SG et al., 2007. The Immunosuppressant Drug FTY720 Inhibits Cytosolic Phospholipase A2 Independently of Sphingosine-1-phosphate Receptors, Blood, 109, p.1077–85
17. Berdyshev EV et al., 2009. FTY720 Inhibits Ceramide Synthases and Up-regulates Dihydrosphingosine 1-phosphate Formation in Human Lung Endothelial Cells, Journal of Biological Chemistry, 284 (9), p. 5467–77
18. Chiba, 2005. FTY720, a new class of immunomodulator, inhibits lymphocyte egress from secondary lymphoid tissues and thymus by agonistic activity at sphingosine 1-phosphate receptors, Pharmacology and Therapeutics, 108 (3), p. 308-19.
19. Budde K et al., 2002. First human trial of FTY720, a novel immunomodulator, in stable renal transplant patients, Journal of the American Society of Nephrology, 13(4), p.1073-83.
20. Salvadori M et al., 2006. FTY720 versus MMF with Cyclosporine in de novo Renal Transplantation: A 1-Year, Randomized Controlled Trial in Europe and Australasia, American Journal of Transplantation, 6 (12), p. 2912-21
21. Kappos et al., 2006. Oral fingolimod (FTY720) for relapsing Multiple Sclerosis, New England Journal of Medicine, (335), p.1124-41
22. O’Connor et al., 2009. Oral fingolimod (FTY720) in Multiple Sclerosis, Neurology, (72), p.73-79

Page 100
23. Novgorodov et al., 2007. Activation of Sphingosine-1-Phosphate Receptor S1P5 Inhibits Oligodendrocyte Progenitor Migration, FASEB Journal, (21), p.1503-14
24. Miron et al., 2008. Central Nervous System-Directed Effects of FTY720 (fingolimod), Journal of Neurological sciences (2008), doi: 10.1016/j.jns.2008.06.031
25. Germana Sanna et al., 2004. Sphingosine 1-Phosphate (S1P) Receptor Subtypes S1P1 and S1P3, Respectively, Regulate Lymphocyte Recirculation and Heart Rate, Journal of Biological Chemisty, (279), p. 13839-48
26. Brossard et al., 2009. Entry-into-humans study with ACT-128800, a selective S1P1 receptor agonist: tolerability, safety, pharmacokinetics, and pharmacodynamics, American Society for Clinical Pharmacologists and Therapeutics, Abstract
27. Bayer et al., 2008. The Cytoprotective Nrf2 Transcription Factor Controls Insulin Receptor Signaling in the Regenerating Liver, Cell Cycle, 7 (7), p.874-8
28. Braun et al., 2002. Nrf2 Transcription Factor, a Novel Target of Keratinocyte Growth Factor Action Which Regulates Gene Expression and Inflammation in the Healing Skin Wound, Molecular and Cellular Biology, 22 (15), p. 5492-5505
29. Maruyama & Itoh, 2007. The Role of Nrf2 in the Protection Against Inflammation and Innate Immunity, Hiroaski Medical Journal, 59 (Suppl.), p. S167-71
30. http://investor.biogenidec.com/phoenix.zhtml?c=148682&p=irol-newsArticle&ID=1216902&highlight=, accessed on 07Nov2008
31. Lukashev M, Zeng W, Goetz S, et al., 2007. Activation of Nrf2 and Modulation of Disease Progression in EAE models by BG00012 (dimethyl fumarate) Suggests a Novel Mechanism of Action Combining Anti-inflammatory and Neuroprotective Modalities. Program and abstracts of the ECTRIMS 2007: 23rd Congress of the European Committee for Treatment and Research in Multiple Sclerosis; October 11-14, 2007; Prague, Czech Republic. Poster 503.
32. Kappos et al., 2008. Efficacy and Safety of Oral Fumarate in Patients with Relapsing-Remitting Multiple Sclerosis: a Multicentre, Randomised, Double-blind, Placebo-controlled Phase IIb Study, The Lancet, 372 (9648), p. 1463-73
33. Yousry TA et al., 2006. Evaluation of Patients Treated with Natalizumab for Progressive Multifocal Leukoencephalopathy, New England Journal of Medicine, 354(9), p. 924-33
34. Yang J et al., 2004. Laquinimod (ABR-215062) Suppresses the Development of Experimental Autoimmune Encephalomyelitis, Modulates the Th1/Th2 balance and Induces the Th3 Cytokine TGF-β in Lewis Rats, Journal of Neuroimmunology, 156 (1-2), p. 3-9
35. http://www.tevapharm.com/pr/2009/pr_844.asp; accessed on 13July2009 36. Comi et al., 2008. Effect of Laquinimod on MRI-monitored Disease Activity in Patients with
Relapsing-remitting Multiple Sclerosis: a Multicentre, Randomised, Double-blind, Placebo-controlled Phase IIb Study. , Lancet, 371 (9630), p. 2085-92
37. http://www.gsk.com/investors/presentations/2007/neurosciences-seminar-dec07/jingwu-zang.pdf; accessed 01October2009
38. Noseworthy J et al., 2000. Linomide in relapsing and secondary progressive MS, Neurology, 54, p. 1726-33
39. http://www.reuters.com/article/mergersNews/idUSBFA00093220090514; accessed 08October2009 40. http://www.europharmatoday.com/2009/01/new-brand-same-ms-drug-novartis-launches-extavia-in-
europe.html; accessed 08October2009 41. Foote AK, Blakemore WF, 2005. Inflammation Stimulates Remyelination in Areas of Chronic
Demyelination, Brain, 128, p. 528-39 42. Back SA et al., 2005. Hyaluronan Accumulates in Demyelinated Lesions and Inhibits
Oligodendrocyte Progenitor Maturation, Nature Medicine, 11, p. 966-72 43. Pluchino S et al, 2005. Injection of Adult Neurosphere-derived Multiponent Precursors Promote
Neuroprotection by an Immunomodulatory Mechanism, Nature, (436), p. 266-71