
File1
18
Hilik Levkovitz MD,MHA Professor Director Day Hospital & Cognitive and Emotional Lab. School of Medicine, Tel Aviv University, Israel. Deep Transcranial Magnetic Stimulation (TMS) for Tourette Syndrom
-
Upload
proffesolevkovic -
Category
Health & Medicine
-
view
922 -
download
4
Transcript of File1
Hilik Levkovitz MD,MHA
Professor
Director Day Hospital & Cognitive and Emotional
Lab.
School of Medicine, Tel Aviv University,
Israel.
Deep Transcranial Magnetic Stimulation (TMS) for Tourette
Syndrom
Dr. Levkovitz is a consultant and get a
regular consultant fee from Brainsway Ltd.
Disclosure
Previous rTMS Studies in Tourette Syndrome
• 12 subjects, 1Hz, 80% of MT, 3 gorupd : left premotor, left motor, left sham. No
improvement (Munchau et al. 2002, Orth et al. 2004)
• 8 subjects, 1 or 15 Hz, 110% of MT, 3 groups: left premotor, left motor, left sham.
6 days. Improvement in OC but not tic symptoms (Jeong-Ho et al. 2004)
• 5 subjects, 1 Hz, 100% of MT, SMA, 14 days. Significant improvement in Tics
(Mantovani et al. 2006)
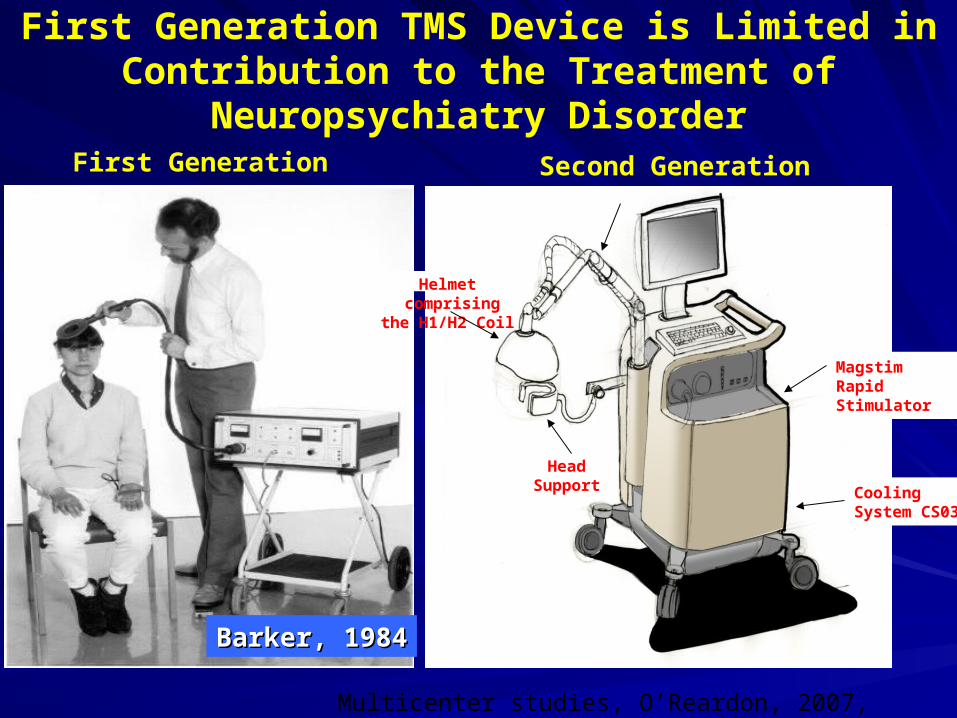
Barker, 1984Barker, 1984
Magstim Rapid Stimulator
Cooling System CS03
Head Support
Helmet comprising the H1/H2 Coil
First Generation Second Generation
First Generation TMS Device is Limited in Contribution to the Treatment of
Neuropsychiatry Disorder
Multicenter studies, O’Reardon, 2007, George, 2010
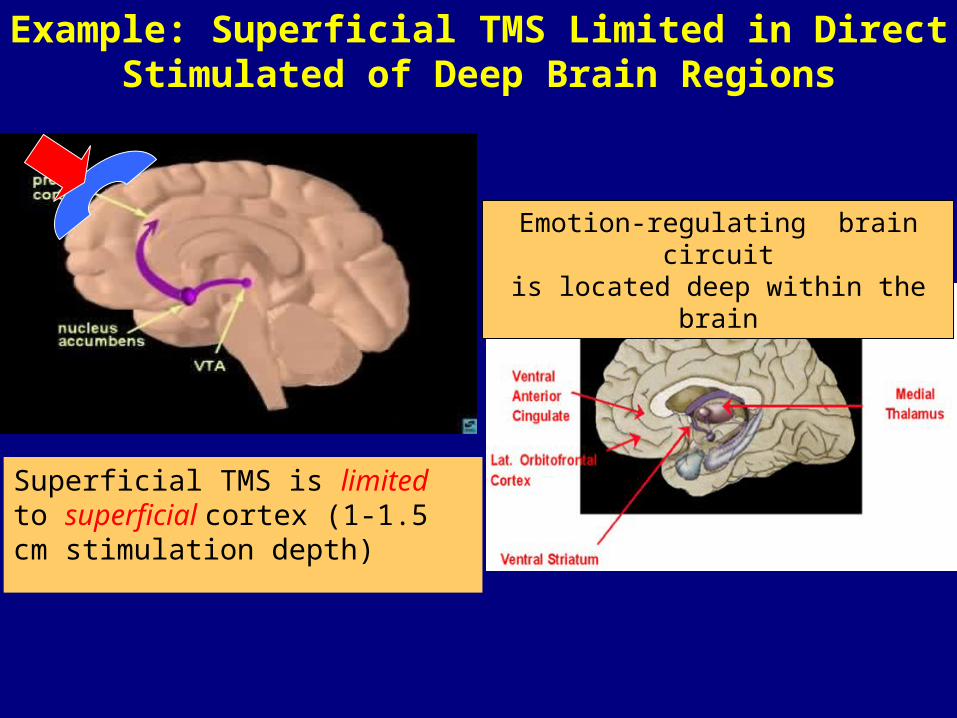
Example: Superficial TMS Limited in Direct Stimulated of Deep Brain Regions
Superficial TMS is limited to superficial cortex (1-1.5 cm stimulation depth)
Emotion-regulating brain circuitis located deep within the brain
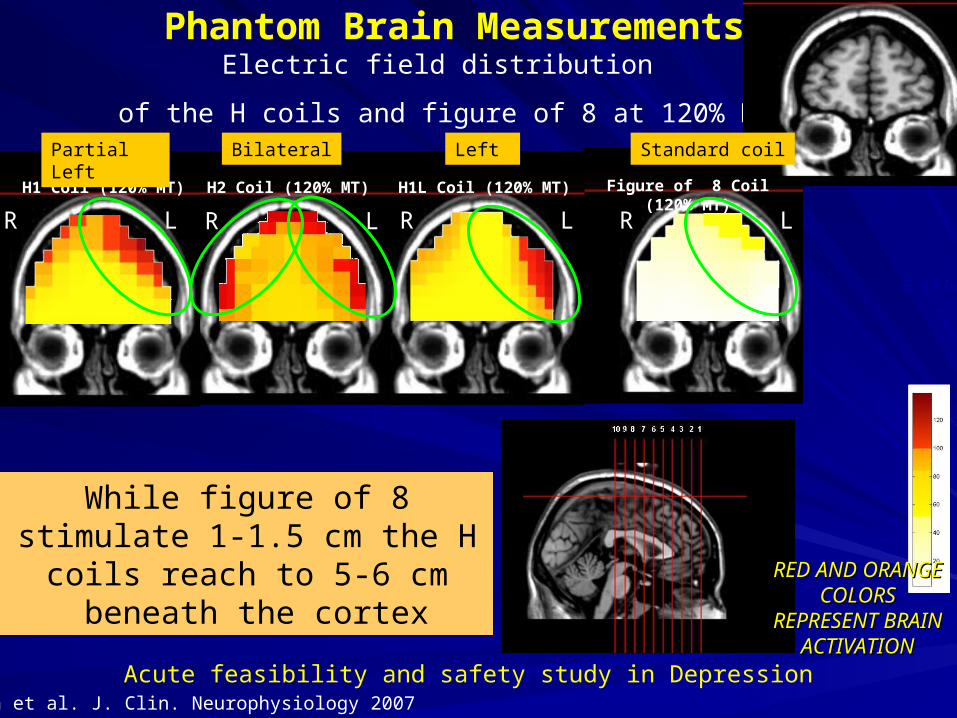
H1L Coil (120% MT)H1 Coil (120% MT)
E [V/m]
H2 Coil (120% MT)
RED AND RED AND ORANGE ORANGE COLORS COLORS
REPRESENT REPRESENT BRAIN BRAIN
ACTIVATIONACTIVATION
Phantom Brain MeasurementsElectric field distribution
of the H coils and figure of 8 at 120% MT
Figure of 8 Coil (120% MT)
While figure of 8 stimulate 1-1.5 cm the H coils reach to 5-
6 cm beneath the cortex
Roth et al. J. Clin. Neurophysiology 2007
Acute feasibility and safety study in Depression
LR LR LR LR
Left BilateralPartial Left Standard coil
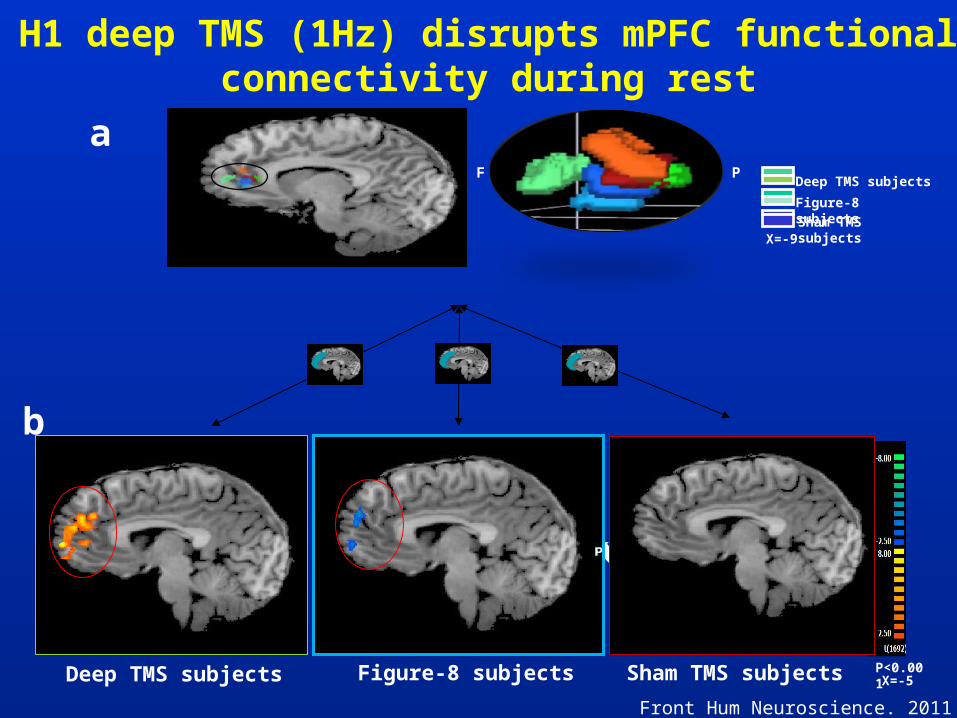
H1 deep TMS (1Hz) disrupts mPFC functional connectivity during rest
b
P<0.001Sham TMS subjects
Figure-8 subjectsDeep TMS subjects X=-5
PF
aDeep TMS subjects
Figure-8 subjectsSham TMS subjects
X=-9
Front Hum Neuroscience. 2011

• Deeper penetration leads to activate brain circuit located deep within the brain• Different coils target to different brain area
H-coil Transcranial Magnetic Stimulation (TMS)
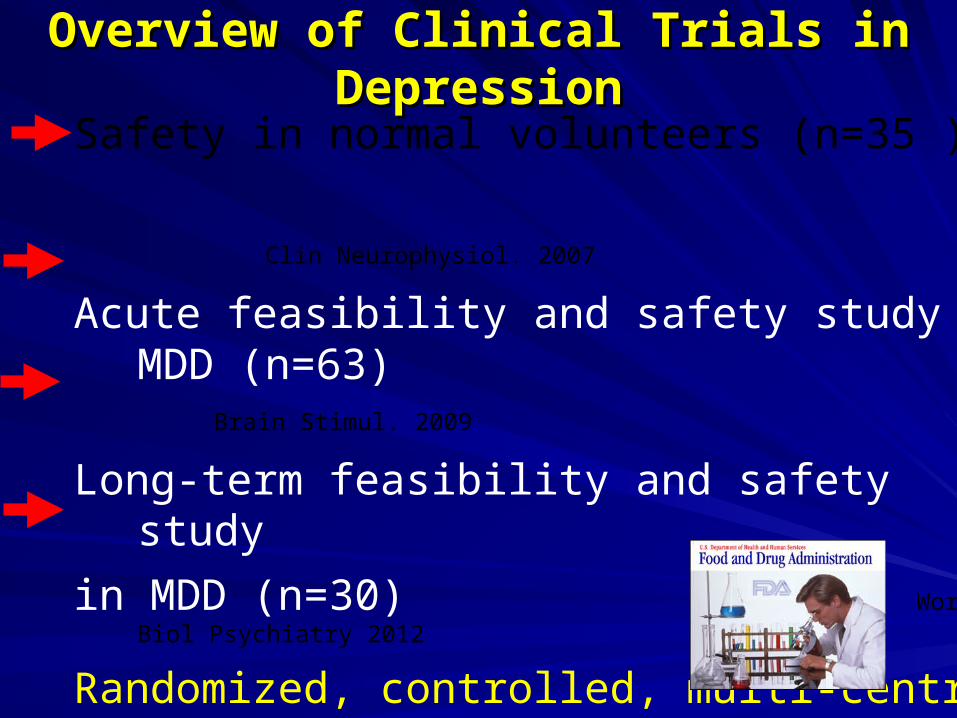
Overview of Clinical Trials in Overview of Clinical Trials in DepressionDepression
Safety in normal volunteers (n=35 )
Clin Neurophysiol. 2007
Acute feasibility and safety study in MDD (n=63) Brain Stimul. 2009
Long-term feasibility and safety study
in MDD (n=30) World J Biol Psychiatry 2012
Randomized, controlled, multi-centre study
(efficacy) (n=230)
21 sites (15 from North America , 2 from Europe and 4 from Israel) participate in the study and this was one of
the biggest studies in the field of TMS.
International sites include:
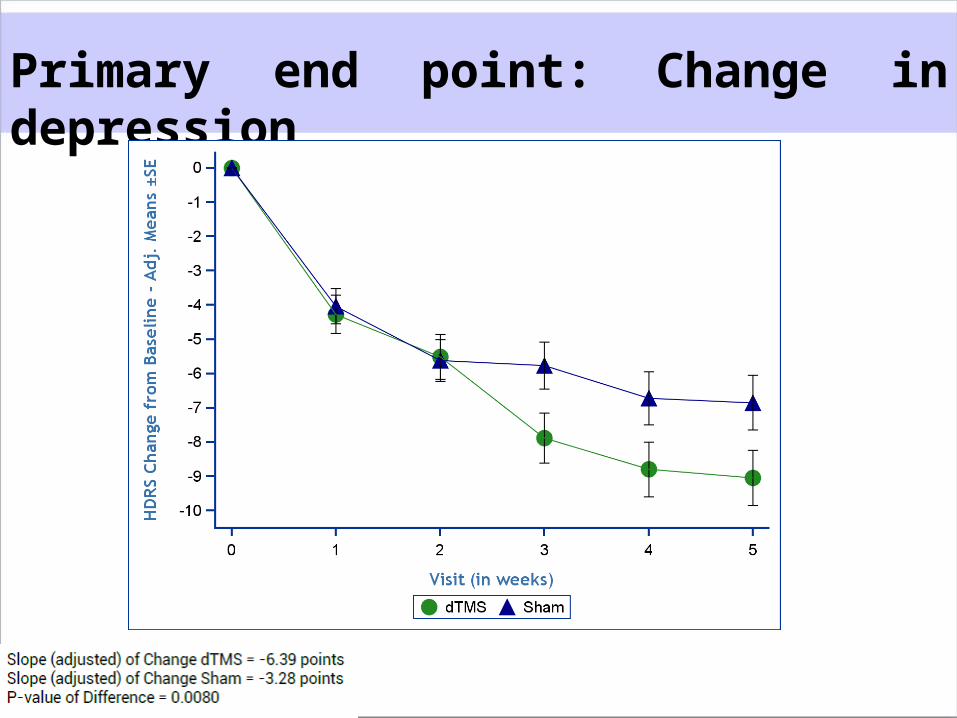
Primary end point: Change in depression
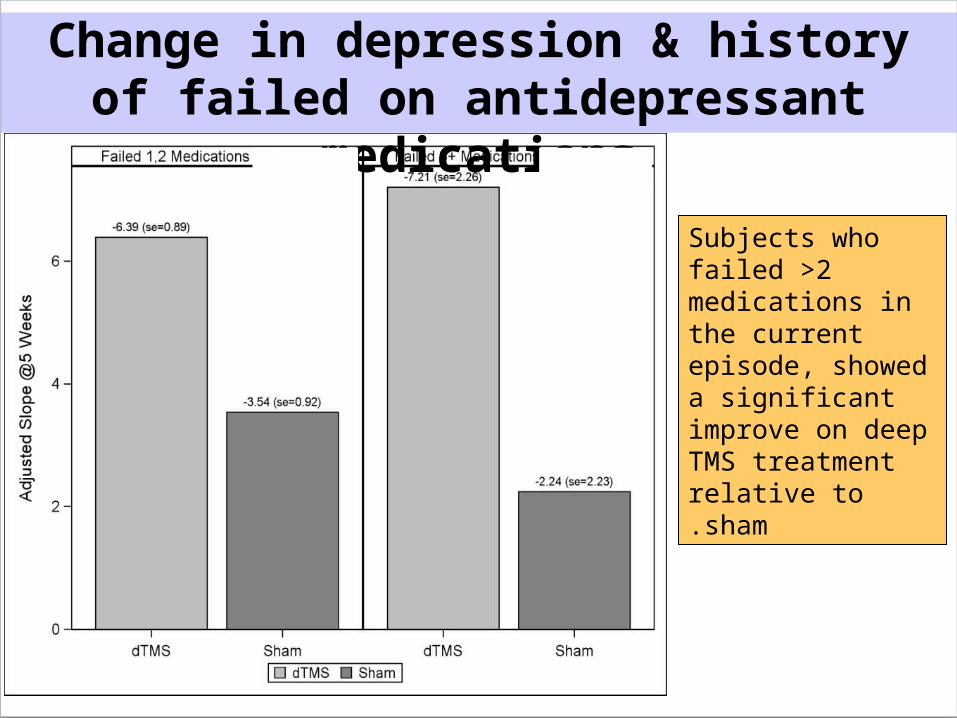
Change in depression & history of failed on antidepressant
medications
Subjects who failed >2 medications in the current episode, showed a significant improve on deep TMS treatment relative to sham.
Prospective, Multicenter, Double-Blind, Randomized, Sham Controlled Trial
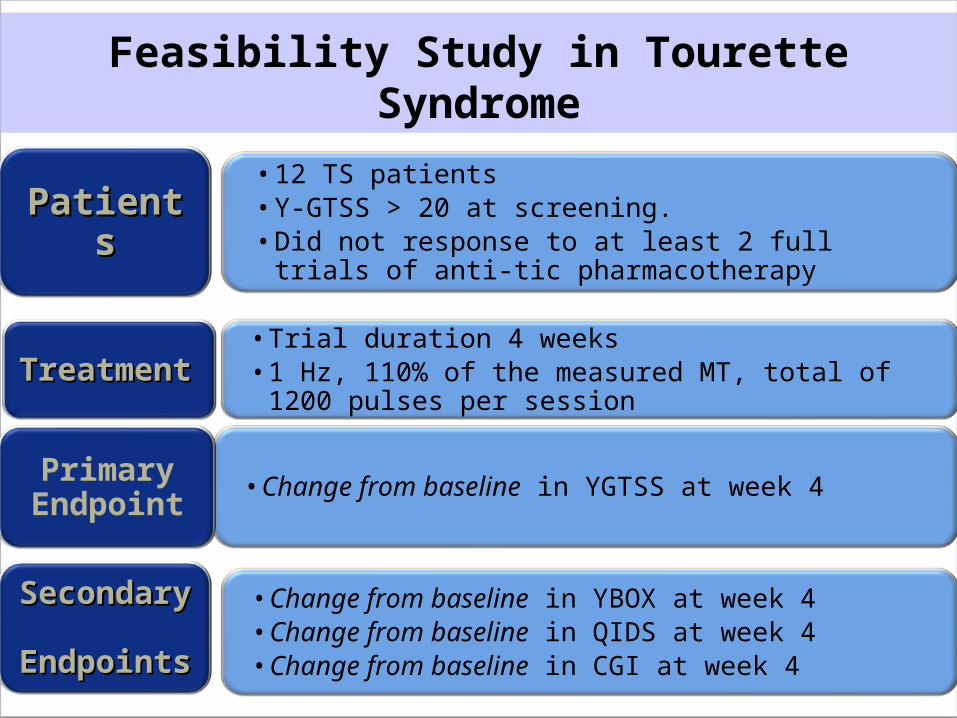
•12 TS patients•Y-GTSS > 20 at screening.• Did not response to at least 2 full trials of anti-
tic pharmacotherapy
•Trial duration 4 weeks•1 Hz, 110% of the measured MT, total of 1200
pulses per session
•Change from baseline in YGTSS at week 4
• Change from baseline in YBOX at week 4•Change from baseline in QIDS at week 4•Change from baseline in CGI at week 4
PatientsPatients
TreatmenTreatmentt
Primary Endpoint
SecondarSecondary y
EndpointEndpointss
Feasibility Study in Tourette Syndrome
Yale-Brown Obsessive Compulsive Disorder Scale
(YBOCS)
Yale Global Tic Severity rating Scale (YGTSS)
Clinical Global Impression (CGI)
Social Adaptation Self-evaluation Scale (SASS)
Hamilton Anxiety Rating Scale (HARS-14)
Level of depression (HDRS-21)
Subjective improvement (IDS-SR)
Efficacy rating scales used in the study
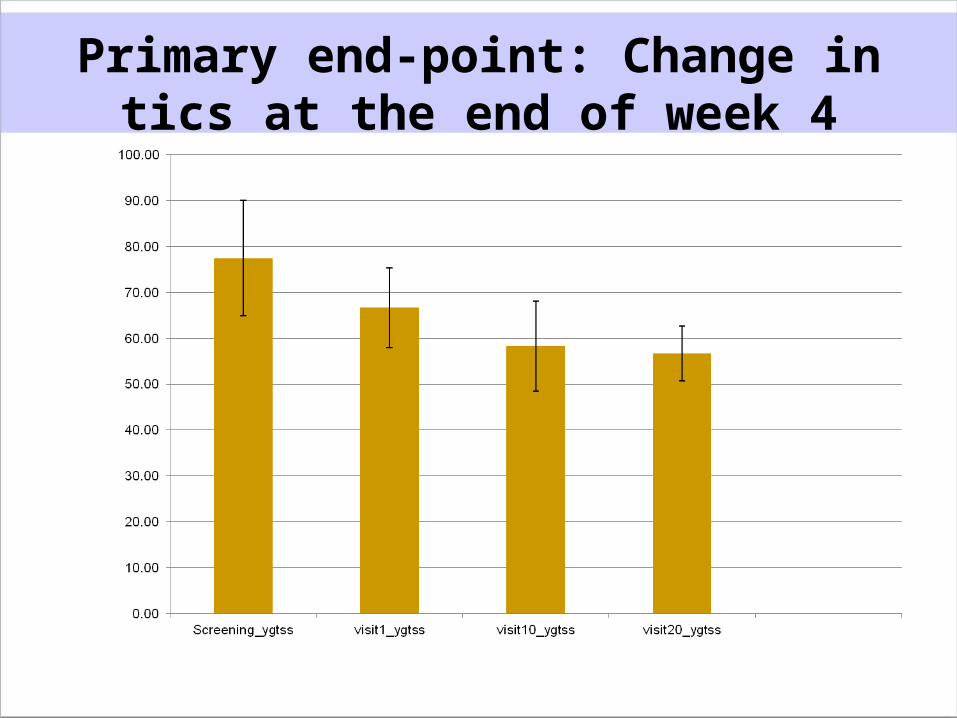
Primary end-point: Change in tics at the end of week 4
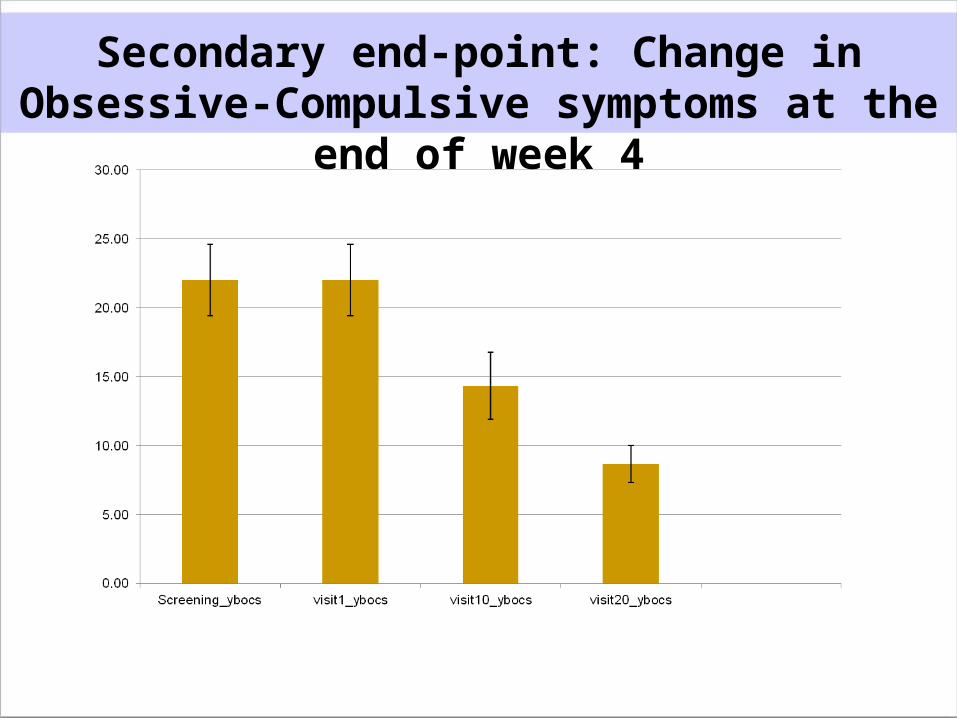
Secondary end-point: Change in Obsessive-Compulsive symptoms at
the end of week 4
Primary end-point: change in tics at the end of week 4
For sub-group of patients suffered from Tourette & OCD :
Tics improved significantly (p=0.047) OC symptoms a trend for
improvement on YBOCS (p= 0.065)

Thanks !Thanks !


















