Figure 1 - medscistudents
14
1 THE KIDNEY (Fig. 1 & 2) The kidney is a bean-shaped, reddish-brown organ of the urinary system located retroperitoneally in the upper part of the paravertebral gutter of the abdominal cavity, padded by pararenal extraperitoneal fat. There are normally two kidneys per individual, each possessing anterior and posterior surfaces, lateral and medial borders and upper and lower poles. The indented aspect of the medial border, which is called the hilus (hilum), impacts the bean-shaped appearance on the kidney. This area also serves as the route of passage of structures in and out of the organ. Measuring about 10cm in length, 5cm in width and 2.5cm in depth, each kidney lies lateral to the vertebral column between T12 and L3 vertebral bodies. Weighing about 150gms in the male and 135gms in the female, each kidney lies obliquely with the upper pole nearer the midline than the lower pole. Furthermore, the right kidney is lower, wider and shorter than the left one and lies further away from the midline than the latter. Figure 1
Transcript of Figure 1 - medscistudents

1
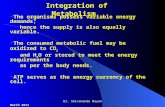
THE KIDNEY (Fig. 1 & 2)
The kidney is a bean-shaped, reddish-brown organ of the urinary system located retroperitoneally in the upper
part of the paravertebral gutter of the abdominal cavity, padded by pararenal extraperitoneal fat.
There are normally two kidneys per individual, each possessing anterior and posterior surfaces, lateral and
medial borders and upper and lower poles. The indented aspect of the medial border, which is called the hilus
(hilum), impacts the bean-shaped appearance on the kidney. This area also serves as the route of passage of
structures in and out of the organ.
Measuring about 10cm in length, 5cm in width and 2.5cm in depth, each kidney lies lateral to the vertebral
column between T12 and L3 vertebral bodies.
Weighing about 150gms in the male and 135gms in the female, each kidney lies obliquely with the upper pole
nearer the midline than the lower pole. Furthermore, the right kidney is lower, wider and shorter than the left one
and lies further away from the midline than the latter.
Figure 1

2
Figure. 2

3
Surface Anatomy of the Kidney Fig. 3:
The kidneys are located on the posterior abdominal wall and hence the surface anatomy of the kidney is
projected to the posterior surface of the body in the abdominal region.
The upper pole of each kidney lies 2.5cm from the midline at the level of T12 while the lower pole lies 7.5cm
from the midline at the level of L3. The hilar of each kidney lies 5cm from the midline.
The transpyloric plane (L1), which passes along the tip of the ninth costal cartilage, traverses the upper part of
the right hilum and the lower part of the left hilum. The lower pole of the right kidney is 1.25cm above the iliac
crest while that of the left kidney is 2.5cm above the iliac crest.
Figure. 3
Structures Closely Associated with the Medial Border of the Kidney:
The Renal Sinus: This is the 2.5 cm-deep cavities in the medial aspect of the kidney, which opens into the hilus
of the kidney. It is lined by the fibrous renal capsule (The deepest layer of the renal coverings) and contains:
1. Rostral part of the renal pelvis
2. Major calyces (calices)
3. Minor calyces (calices)

4
4. Blood vessels
5. Nerves
6. Lymphatics and
7. Adipose tissue
The Renal pelvis: This is a funnel-shaped tube located partly in the renal sinus and in the hilum. It projects
beyond the hilum to continue caudally with the ureter. In its rostral part within the sinus, it divides to form 2-3
major calyces, which in turn divide to form 7-14 minor calyces
Relations of the Kidneys (Fig. 4):
The structure entering and leaving the kidney at the hilus constitute its medial relations. These include:
1 The renal vein (Lies anterior)
2 The renal artery (Lies posterior to the vein)
3 The renal pelvis (Lies posterior to the artery)
The suprarenal glands are located in the anteromedial aspect of the superior poles of the kidneys.
Figure 4
Posterior Relations (Fig. 5):
With the exception of the eleventh rib, which is the highest posterior relation of the left kidney, the posterior
relations of both kidneys are similar. They include:
1. The muscular bed comprising:

5
a. The thoracoabdominal diaphragm, which separates the kidney from the base of the lung, the pleura
and the 12th
/11th
rib/11th
intercostal space.
b. The psoas major muscle on the medial aspect
c. The quadratus lumborum lateral to the psoas muscle and
d. The transversus abdominis lateral to the quadratus lumborum muscle
e. The medial and lateral arcuate ligaments of the diaphragm above the psoas and quadratus muscles
2. The subcostal nerve (T12) and vessels
3. The iliohypogastric nerve (L1) and
4. The ilioinguinal nerve (L1)
Figure 5
Anterior Relations:
These are listed in the table below: (See Diagram)
RIGHT KIDNEY LEFT KIDNEY
Inferior surface, right lobe of the Liver The stomach
Hepatorenal recess The pancreas
Duodenum The splenic vein
Right colic flexure The splenic artery
Loops of the small intestine ( Ileum) The spleen
Loops of the small intestine (Jejunum)
Splenic flexure and descending colon
The omental bursa (Lesser sac)

6
Blood Supply of the Kidney (Fig: 6):
Renal arteries of corresponding sides supply the kidneys. Both are branches of the abdominal aorta arising at the
level of L1/L2. The right renal artery which is longer than the left one passes to the right hilum, posterior to the
inferior vena cava. The shorter left artery passes directly into the left hilum.
In 30% of the population, assessory renal arteries may arise from the aorta above or below the origin of the main
renal artery. On entering the kidney, each artery divides to give rise to about 5 segmental arteries within the
sinus. The segmental arteries give rise to lobar arteries, which in turn give rise to interlobar arteries.
Interlobar arteries enter the column of Bertin and continue as arcuate arteries at the junction of the cortex and
the medulla of the kidney. The arcuate arteries give rise to interlobular arteries, which form the basis of the
subdivision of the kidney into lobules. Large-diameter afferent arterioles arise from the interlobular arteries to
supply the glomeruli (Glomerular capillaries), which are drained by Small-diameter efferent arterioles. These in
turn form peritubular capillary network around the proximal and distal convoluted tubules. Peritubular capillaries
drain into interlobular veins which, in turn drain into the arcuate vein of the corticomedullay junction.
The efferent arterioles associated with Juxtamedullary nephrons form straight capillary network referred to as the
Vasa Recta around the corresponding Henle’s loops in the renal medulla. The vasa recta invariably drain into
the arcuate veins.
Venous drainage of the Kidney:
The venous drainage of the kidney commences with the stellate veins, which drain the renal capsule and the
outer cortex into interlobular veins. From this point on the vein pursue the pattern of the arterial distribution and
finally drain into the inferior vena cava via the renal veins. The left renal vein, which passes anterior to the
abdominal aorta, is longer than the right renal vein.
Lymphatic drainage of the Kidney:
Renal lymphatic vessels run with the veins and drain into lumbar (Lateral aortic) lymph nodes.
Innervation of the Kidney:
The kidney receives sympathetic and parasympathetic fibers from the renal nerve plexus, which is formed from
fibers arising from the lesser and least (lowest or renal) splanchnic nerves (T10-L1). The renal plexus is located
along the renal arterial tree and it possesses an aorticorenal ganglion on each side of the aorta.

7
Figure 6

8
THE URETER
The ureter is the thick-walled, highly expandable muscular tube, which propels urine in boluses by peristaltic
contraction from the renal pelvis to the urinary bladder. It is a direct continuation of the renal pelvis and it
terminates by traversing the wall of the base (Fundus) of the urinary bladder. Measuring about 25cm in length, it
descends retroperitoneally anterior to the medial aspect of the psoas major muscle along the tips of the lumbar
transverse processes and crosses the pelvic brim anterior to the bifurcation of the common iliac artery.
The ureter has a narrow lumen, about 3mm** in diameter and is subdivided into two parts, viz.
a. The abdominal part (12.5cm), which lies in the abdominal cavity above the pelvic brim and
b. The pelvic part (12.5cm), which lies in the pelvic cavity below the pelvic brim.
The ureter is constricted in three areas along its course from the abdomen to the pelvis. These areas are:
1. At the pelviureteric region (Not junction)
2. At the pelvic brim and
3. At the part which, traverses the base of the urinary bladder. This is the narrowest part of the ureter,
which is also referred to as the intramural (intravesical) part of the ureter. This part also projects into
the lumen of the urinary bladder as the Ureteric fold.
Course of the Abdominal Ureter (Figure 7):
The abdominal ureter passes along the medial aspect of the psoas major muscle, from the tip of the transverse
process of the first lumbar vertebra bone to the pelvic brim.
Relations of the abdominal ureter
The relations of the abdominal ureter are similar in the male and female but differ from one side to the other.
Posterior Relations: These are similar on both sides and include:
1. Psoas major muscle
2. Tips of the lumbar transverse processes
3. Genitofemoral nerve
Anterior Relations (Right side):
1. Descending part of the duodenum
2. Right colic vessels
3. Iliocolic vessels
4. The root of the mesentery
5. The terminal ileum
6. The gonadal vessels
7. The peritoneum
Anterior Relations: Left side:
1. Left colic vessels
2. Sigmoid colon
3. Sigmoid mesocolon
4. Gonadal vessels
5. The peritoneum
Medial Relations: These exist only on the right side and include:
1. The inferior vena cava
2. The lumbar lymph nodes
3. The sympathetic trunk

9
Figure 7
Course of the Pelvic Ureter
The pelvic ureter is retroperitoneal throughout its course. The first segment of the pelvic ureter passes
posteroinferiorly from the pelvic brim to the lateral pelvic wall resting on the obturator fascia along the anterior
border of the greater sciatic notch. The second segment turns anteromedially at the level of the ischial spine and
runs on the levator ani muscle (the pelvic diaphragm) to reach the base of the urinary bladder.

10
Relations of the Pelvic Ureter
Posterior Relations (First segment): These are similar in both sexes and on both sides. They include:
1. The internal iliac artery and vein
2. The lumbosacral nerve trunk
3. The sacroiliac joint
Lateral relations (First segment):
1. Obturator fascia
2. Umbilical artery
3. Obturator vessels
4. Obturator nerve
5. Inferior vesical vessels
6. Middle rectal artery
7. The uterine artery in the Female
Anterior relations (First segment):
1. The ovary in the Female
Relations of The second Segment
In the Male:
1. Vas deferens – Anteromedially
2. Seminar vesicle – Inferiorly
In the Female:
1. Uterine artery – superiorly
2. Broad ligament of the Uterus – superiorly
3. Lateral fornix of the vagina – medially
4. Uterine cervix – medially
5. Vagina – posteriorlly
Blood supply of the ureter
The ureter receives blood supply from all the vessels along its course from the abdomen to the pelvis. These
arteries establish anastomotic network on the wall of the ureter. The vessels from above downwards are:
1. Renal artery
2. Abdominal aorta
3. Gonadal arteries
4. Common iliac artery
5. Internal iliac artery
6. Superior vesical artery
7. Inferior vesical artery in the Male
8. Uterine artery in the Female
Venous Drainage of the ureter

11
The veins of the ureter run along corresponding arteries and invariably drain into the inferior vena cava or the
renal veins.
Nerve Supply of the Ureter
The smooth muscles and the blood vessels of the ureter receive autonomic supply from the following plexuses:
1. Renal plexus
2. aortic plexus
3. Superior hypogastric plexus
4. Inferior hypogastric plexus
Afferent fiber for pain and awareness of distention traverse T11-L2. Areas of referred pain for the ureter are:
Inguinal region
Scrotum
Medial femoral region and the cremasteric muscle.
Histology of the Ureter
The mucous membrane which is urothelium is supported by a connective tissue layer of lamina propia. The
luminal cells of the urothelium are cuboidal in shape, the middle layer are polyhedral while the basal layer are
columnar/cuboidal in shape.
In the upper 1/3 the smooth muscle fibers of the tunica muscularis are arranged in helical and longitudinal axis.
The middle 1/3 consists of smooth muscles arranged in outer circular and inner longitudinal layers, while the
lower 1/3 consists of smooth muscles arranged in inner longitudinal middle circular and outer longitudinal
layers.
The tunica adventitia consists of fibroelastic and adipose tissue in which are embedded nerve fibers, blood
vessels and lymphatics.
Applied Anatomy of the Kidney and the Ureter
The Kidney:
1. Tract of internal bleeding from a ruptured kidney
2. Pus from a perinephric abscess.
3. The kidney and respiratory movements
4. Surgical exposure of the kidney
5. Nephroptosis “dropped kidney”
6. Renal transplant
The Ureter:
1. The ureter and the peritoneum
2. Constricted sites of the ureter and obstruction by Ureteric stone (Calculus):
Consequences of obstruction:
a. Colicky pain due to hyperperistalsis of the ureter
b. Ureteric distention by urine (Uroureter or Hydroureter)
c. Renal Pelvis distensions by urine (Hydronephrosis or Uronephrosis or Nephrohydrosis)
3. Radiological investigations of the ureter:
a. Plain X-ray
b. Administration of radiopaque materials Pyeloghraphy
4. Endourology – Cystoscope insertion
5. Lithotripsy – Fragmentation of stones using shock waves
6. Palpation of a Ureteric stone

12
7. Common sites of injury to the ureter in obstetrics practice are
At the Pelvic brim where it is close to the ovarian vessels.
At the lateral aspect of the cervix where it is crossed by the uterine artery.

13

14