fifteen Elbow and Forearm - LiveConferences.com · Elbow and Forearm 309 bones in a manner that...
28
fifteen Edward D. Wang, MD Lawrence C. Hurst, MD Elbow and Forearm
Transcript of fifteen Elbow and Forearm - LiveConferences.com · Elbow and Forearm 309 bones in a manner that...

fifteen
Edward D. Wang, MDLawrence C. Hurst, MD
Elbow andForearm

Figure 15-1: Bones of Right Elbow Joint
Chapter 15
ANATOMYThe elbow is a functional link for position-
ing the hand in space, a fulcrum for the fore-arm lever, and a load-carrying joint. As such, itrequires a combination of mobility and stabil-ity. The three articulations of the elbow pro-vide flexion and extension, as well as forearmrotation (Figure 15-1). Control and stability offlexion and extension are provided primarilythrough the ulnohumeral (trochlea and ole-cranon) articulation and secondarily throughthe radiohumeral (capitellum and radial head)articulation. The trochlea is shaped like a
308
Humerus Humerus
Lateral
supracondylar ridge
Radial fossa
Lateral epicondyle
Capitulum
Head
Neck
Tuberosity
Radius Ulna
Tuberosity
Radial notch of ulna
Coronoidprocess
Trochlea
Medial epicondyle
Coronoidfossa
Medialsupracondylar ridge
Lateral epicondyle
Olecranon
fossaOlecranon
Head
Neck
Tuberosity
RadiusUlna
Humerus
Lateral epicondyle
Capitulum
Head
Neck
Radial tuberosity
Humerus
Medial epicondyle
Capitulum
Trochlea
HeadNeck
Radial tuberosity
Radius
UlnaRadial notch
Coronoid process
Trochlear notch
Olecranon
Coronoid processTrochlear notch
Olecranon
Groove forulnar nerve
of ulna
In extension: anterior view In extension: posterior view
In 90˚ flexion: lateral view In 90˚ flexion: medial view
Lateral condyle Medial condyle
spool and fits in the wrench-shaped trochlearnotch. This anatomic configuration, in con-junction with the collateral ligaments, pro-vides a stable hinge joint that can lift heavyobjects. Rotation of the forearm occursthrough the proximal and distal radioulnar ar-ticulations.
Distal to the radial head, the bone tapers toform the radial neck, then flares at the radialtuberosity—the insertion site of the biceps ten-don. Between the radius and the ulna is the interosseous membrane—a thickened, liga-mentous structure that connects the two

Elbow and Forearm
309
bones in a manner that provides stabilitywhile allowing forearm rotation.
Muscles that cross the elbow anteriorly in-clude the elbow flexors and the flexor-pronatorforearm muscles that originate from the medialepicondyle (Figure 15-2). In the forearm, thevolar muscles are arranged in three layers. Thesuperficial group includes the pronator teres,flexor carpi radialis, palmaris longus, and flexorcarpi ulnaris. The middle layer is the flexor dig-itorum superficialis. The deep layer comprisesthe supinator, flexor digitorum profundus,flexor pollicis longus, and pronator quadratus.The flexor-pronator muscle group primarilyprovides wrist flexion and forearm pronation.The biceps is a secondary flexor of the elbowand a strong supinator. Immediately deep tothe biceps lies the brachialis muscle—the majorflexor of the elbow.
Posterior elbow muscles include elbow ex-tensors, wrist and finger extensors, and thesupinator. Posterior forearm muscles are ar-ranged in two layers. The superficial grouporiginates from a common tendon at the lat-eral epicondyle and includes a lateral compo-nent (brachioradialis, extensor carpi radialislongus, and extensor carpi radialis brevis) anda medial subgroup (extensor digitorum, ex-tensor digiti minimi, extensor carpi ulnaris,and anconeus). The deep posterior forearmmuscles are the supinator, abductor pollicislongus, extensor pollicis brevis, and extensorpollicis longus (see Figure 15-2).
The brachial artery, the main artery of thearm and elbow, travels in the anterior com-partment of the arm adjacent to the mediannerve. Proximal to the elbow, it gives off collat-eral arteries that help form a rich plexus of ves-sels around the elbow. At the level of the radialhead, the brachial artery bifurcates into the ra-dial and ulnar arteries. The ulnar artery entersthe forearm posterior to the pronator teres,whereas the radial artery travels between thebrachioradialis and the supinator muscle.
The median nerve enters the forearm be-tween the humeral and ulnar heads of thepronator teres and travels inferior to the flexordigitorum superficialis muscle (Figure 15-3).The anterior interosseous nerve branches in-
nervate the index, and sometimes, the long,finger component of the flexor digitorum pro-fundus, the flexor pollicis longus, and thepronator quadratus. Because of the locationof its fibers in the median nerve, isolatedparalysis of the anterior interosseous nervemay occur with an elbow fracture. The rest ofthe median nerve innervates all the volar fore-arm muscles except the ulnar half of the flexordigitorum profundus (fourth and fifth fingers)and the flexor carpi ulnaris, both of which aresupplied by the ulnar nerve.
The ulnar nerve exits the anterior compart-ment of the arm, passing behind the medialepicondyle into the cubital tunnel at the el-bow, then enters the forearm between thetwo heads of the flexor carpi ulnaris (Figure15-4). It innervates the flexor carpi ulnarismuscle, the ulnar half of the flexor digitorumprofundus muscle, and, ultimately, the intrin-sic muscles of the hand.
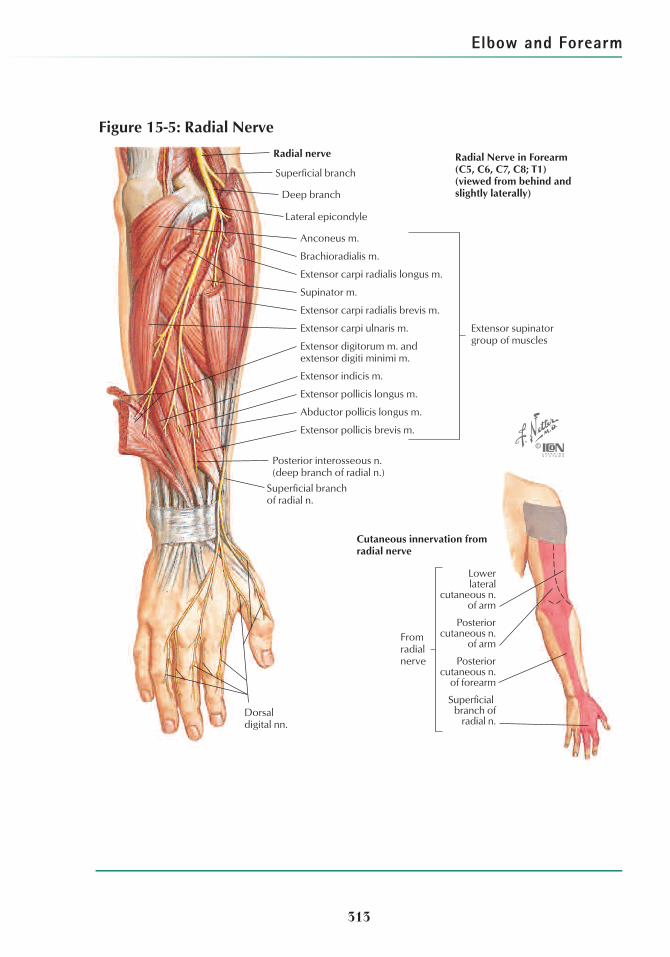
In the arm, the radial nerve travels within theposterior compartment, then enters the ante-rior compartment lateral to the humerus. Inthe antecubital fossa, the radial nerve inner-vates the brachioradialis and extensor carpi ra-dialis longus before dividing into superficial(sensory) and deep (mostly motor) branches(Figure 15-5). The superficial radial nerve pro-vides sensation to the radial dorsal wrist andhand. The deep branch innervates the remain-ing extensor muscles of the forearm. It travelsdeep and through the supinator muscle andexits this muscle as the posterior interosseousnerve. Distal to the radial tuberosity, the deepbranch of the radial nerve may lie “on thebone” and, as such, is vulnerable to injury infractures of the proximal radius or in opera-tions at this site.
PHYSICAL EXAMINATIONInspect the elbow for swelling and ecchy-
mosis, and determine the carrying angle (theaxial alignment of the humerus and the ulnawith the elbow extended). The normal carry-ing angle is 10° to 20°, with most studiesobserving slightly greater cubitus valgus infemales. Angular deformities may occur sec-ondary to previous trauma, growth distur-

Chapter 15
310
Ulna Radius
Brachioradialismuscle
Insertions
Origins
Flexor carpi ulnaris muscle
(humeral origin via common
flexor tendon)
Flexor digitorumprofundus muscle
Extensor carpi ulnarismuscle (ulnar origin)
Extensor pollicislongus muscle
Extensor indicismuscle
Extensor carpi radialislongus muscle
Extensor carpi radialisbrevis muscle
Brachioradialis muscle
Brachialis muscle
Biceps brachii muscle
Supinator muscle
Pronator teres muscle
Radius
Pronator quadratus muscle
Brachioradialis muscle
Ulna
Brachialis muscle
Flexor digitorumprofundus muscle
Flexor digitorumsuperficialis muscle
Extensor carpiulnaris muscle
Flexor carpiulnaris muscle
Flexor digitorumprofundus muscle
Pronator teres muscle(ulnar head)
Flexor digitorum superficialismuscle (humeroulnar head)
Pronator teres muscle(humeral head)
Flexor pollicislongus muscle
Flexor carpiradialis muscle
Abductor pollicislongus muscle
Flexor pollicislongus muscle
Flexor digitorum superficialismuscle (radial head)
Extensor carpi radialislongus muscle
Pronator teres, flexor carpi radialis, palmaris longus, flexor carpi ulnaris, flexor digitorum superficialis (humeroulnar head)
Commonflexortendon
Commonextensor
tendon
Extensor carpi radialis brevis, extensor digitorum, extensor digiti minimi, extensor carpi ulnaris muscles
Flexor carpi ulnarismuscle (ulnar origin)
Pronatorquadratusmuscle
Extensor carpiulnaris muscle
Extensor digitorummuscle (central bands)
Extensor digitiminimi muscle
Extensor digitorummuscle (lateral bands)
Triceps brachii muscle(medial head)
Triceps brachiitendon
Anconeus muscle
Biceps brachiimuscle
Supinator muscle
Abducor pollicislongus muscle
Pronator teresmuscle
Extensor pollicisbrevis muscle
Abductor pollicislongus muscle
Extensor pollicisbrevis muscle
Extensor pollicislongus muscle
Extensor indicismuscle
Anterior view
Posterior view
Note: Attachments of instrinsicmuscles of hand not shown
Figure 15-2: Bony Attachments of Muscles of Forearm

Elbow and Forearm
bances, or genetic syndromes. Ecchymosis,swelling, or both about the elbow indicate amuscle or tendon injury, fracture, or elbowsprain or dislocation.
Palpate subcutaneous landmarks for sites oftenderness, deformity, or effusion that indi-cate the site of occult fracture, tendinosis, lig-ament sprain, or tendon rupture. From lateralto medial, the structures in the antecubitalfossa are the biceps tendon, brachial artery,and median nerve. A palpable defect is key todiagnosing rupture of the distal biceps tendonor disruption of the triceps tendon. Joint effu-sion is best detected in the “soft spot” be-tween the lateral epicondyle, radial head, and
olecranon. Tenderness over the radial head orhumeral condyles may indicate an occult frac-ture that is not visible on radiographs.
The zero starting position for measurementof elbow motion is a straight extremity (Figure15-6). Young children commonly extend theelbow by 10° to 15°, but adults usually cannotextend the elbow past the zero starting posi-tion. The normal range of elbow flexion-extension is 0° to 145°. The plane of forearmrotation is pronation-supination. Pronation lit-erally means “the state of being prone” or, asit relates to the forearm, “the palm beingturned backward.” Likewise, supination liter-ally means “the state of being supine” (ie, the
311
Median nerve
Pronator teres m. (humeral head)
Flexor carpi radialis m.
Palmaris longus m.
Pronator teres m. (ulnar head)
Flexor digitorum superficialis m. (turned up)
Flexor digitorum profundus m.(lateral portion supplied via anterior
interosseous n.; medial portion by ulnar n.)
Anterior interosseous n.
Flexor pollicis longus m.
Pronator quadratus m.
Palmar branch
Then
arm
uscl
es Abductor pollicis brevis
Opponens pollicis
Cutaneous innervation
Anastomotic branch to ulnar n.
Flexorretinaculum
Common Proper
Palmar digital nn.
Articular branch
Flexor pollicis brevis(superficial head;
deep head suppliedby ulnar n.)
1st and 2nd lumbrical mm.
Branches to dorsum ofmiddle and distal phalanges
Figure 15-3: Median Nerve

Chapter 15
312
Ulnar Nerve (C8, T1)(only muscles innervated by ulnar nerve are depicted)
Cutaneous Innervation
Flexor pollicis brevis m.(deep head only; superficial
head and other thenar musclessupplied by median n.)
Adductor pollicis m.
Ulnar nerve(no branches above elbow)
Articular branch(behind medial condyle)
Flexor digitorum profundusm. (medial portion only;lateral portion supplied byanterior interosseousbranch of median n.)
Flexor carpi ulnaris m.(drawn aside)
Palmaris brevisAbductor digiti minimi Flexor digiti minimi brevisOpponens digiti minimi
Hypothenarmuscles
Common palmar digital n.
Palmar and dorsal interossei mm.
3rd and 4th lumbrical mm. (turned down)
Proper palmar digital nn.(dorsal digital nerves are from dorsal branch)
Branches to dorsum of middle and distal phalanges
Deep motor branch
Superficial cutaneous branch
Palmar branch
Dorsal branch
Figure 15-4: Ulnar Nerve
Elbow and Forearm
313
Radial Nerve in Forearm (C5, C6, C7, C8; T1)(viewed from behind and slightly laterally)
Radial nerve
Superficial branch
Deep branch
Lateral epicondyle
Anconeus m.
Brachioradialis m.
Extensor carpi radialis longus m.
Supinator m.
Extensor carpi radialis brevis m.
Extensor carpi ulnaris m. Extensor supinatorgroup of muscles
Extensor digitorum m. and extensor digiti minimi m.
Extensor indicis m.
Extensor pollicis longus m.
Abductor pollicis longus m.
Extensor pollicis brevis m.
Posterior interosseous n.(deep branch of radial n.)
Superficial branchof radial n.
Fromradialnerve
Lowerlateral
cutaneous n.of arm
Posteriorcutaneous n.
of forearm
Posteriorcutaneous n.
of arm
Superficial branch of
radial n.Dorsal digital nn.
Cutaneous innervation from radial nerve
Figure 15-5: Radial Nerve

Chapter 15
palm turned forward, or anteriorly). In forearmrotation measurement, the patient’s arm is sta-bilized against the chest wall, and the elbow isflexed to 90° (Figure 15-7). The zero startingposition occurs with the thumb aligned withthe humerus. Normal motion in adults is 75°pronation and 85° supination. Mild elbowcontractures are of limited functional conse-quence, as most activities of daily living are ac-complished in an arc of motion from 30° to130° flexion and 50° each of pronation andsupination.
DEGENERATIVE DISORDERS OF THEELBOWArthritis
Primary osteoarthritis of the elbow is rela-tively uncommon and accounts for 2% to 7%of elbow arthritis. These patients often work ata job or hobby that repetitively loads the el-bow. Males and the dominant extremity aremore commonly affected. Manifestationsinclude stiffness, loss of motion, and painwith activity. Terminal extension typicallyincreases pain. Secondary osteoarthritis ofthe elbow most often follows intra-articularfractures. Rheumatoid arthritis is by far themost common cause of inflammatory arthritis
of the elbow. Of patients with rheumatoidarthritis, 20% to 50% eventually have elbowinvolvement.
Most patients with elbow arthritis can betreated with standard nonoperative modali-ties. Arthrotomy or arthroscopy may be indi-cated for loose body removal, osteophyteresection and capsular resection, or synovec-tomy. Elimination of locking and decreasedpain are more predictable after removal of aloose body than is increased motion. Injury toneurovascular structures is a potential risk ofelbow arthroscopy, but complications are gen-erally minimal, and recovery time is shortercompared with open procedures.
Resection ulnohumeral arthroplasty that in-cludes resection of the tip of the olecranon,débridement of the olecranon fossa, and re-section of osteophytes from the coronoid maybe used to treat patients with extensivehumeral osteophytes and disabling pain at theextremes of motion, but no pain at rest or inthe mid arc of motion. Patients should havegood elbow stability and normal musculature.Concomitant transposition of the ulnar nerve isindicated for patients with symptoms of en-trapment. Increased motion and decreasedpain have been reported in 85% of patientswho undergo this procedure. Symptoms often
314
0˚
10˚15˚
90˚
140˚
Flexion
Extension
Adult extension to 0˚
In children, normal elbowextension is 10˚–15˚
Figure 15-6: Measurement of Flexion/Extension

Elbow and Forearm
return; however, the interval improvement anddelay in the need for total joint arthroplasty arehelpful. Resection arthroplasty that includesthe distal humerus and radial head may becombined with interposition of autogenousfascia or dermis between the bone surfaces forpatients with more severe arthritis.
Arthrodesis of the elbow is seldom indi-cated because no single position provides rea-sonable function. The rare indications include(1) incurable sepsis or (2) the need for a strong,stable joint in a young manual laborer who hasa normal shoulder and contralateral limb.
Total elbow arthroplasty provides consis-tent short-term results. A semiconstrainedprosthesis that depends on both the compo-nent and the surrounding soft tissues for jointstability provides the best compromise forfunction and the highest long-term survivalrates (approximately 95% at 7 years) (Figure15-8). Loosening of the implant with resultantinstability and recurrent pain is the most com-
mon long-term complication. At the elbow,the rate of loosening is higher and prostheticrevision is less predictable and more compli-cated than at other sites of joint replacement.In general, total elbow arthroplasty is pre-ferred in the older patient, whereas resectionor interposition arthroplasty is preferred inthe younger patient. Because of severe ero-sion and joint instability, total elbow arthro-plasty is indicated in nearly all patients withrheumatoid arthritis.
Lateral EpicondylitisLateral epicondylitis, commonly known as
“tennis elbow,” occurs secondary to a tendi-nosis of the extensor carpi radialis brevisorigin immediately distal to the lateral epi-condyle. The name is misleading because thelateral epicondyle is not the site of involve-ment, inflammation is not present, and mostpatients are not active tennis players. The typ-ical patient is 35 to 50 years of age and expe-
315
0˚
SupinationPronation
0˚0˚
0˚
85˚
75˚
75˚
Thumb in linewith humerus
85˚
Pronation Supination
Arm stabilized against chest wall with elbow flexed at 90˚
Figure 15-7: Measurement of Pronation-Supination

Chapter 15
riences an insidious or acute lateral elbowpain that is exacerbated by activities that in-volve forceful wrist extension. Motions suchas turning a screwdriver or opening a doorcan aggravate the symptoms. Over time, thepain can become severe and may interferewith routine activities.
Examination shows pain just distal and pos-terior to the lateral epicondyle that is exacer-bated when the extensor carpi radialis brevisis stressed in an elongated position (wristextension against resistance with the elbowextended) (Figure 15-9). Elbow motion andradiographic findings are normal. The differ-ential diagnosis includes radial nerve (poste-rior interosseous branch) entrapment, arthritisinvolving the radiohumeral articulation, lateralelbow instability, and referred pain from cervi-cal radiculopathy.
Nonoperative treatment consists primarilyof patience, modification of activities, and
progressive strengthening exercises. Patientsshould be taught to “grasp and lift only insupination.” A counterforce strap wornaround the proximal forearm may decreasepain during lifting activities. Corticosteroid in-jections at the site of maximum tendernessshould be infrequently used. Operative treat-ment, which is infrequently required, involvesexcision of the pathologic area of degener-ated tendon. It results in an 85% to 90% returnto full activity without pain. Persistent painusually occurs secondary to an incomplete re-section or an incorrect diagnosis.
Medial EpicondylitisMedial epicondylitis, commonly known as
“golfer’s elbow,” occurs secondary to tendi-nosis of the flexor-pronator origin. Examina-tion demonstrates tenderness just distal andanterior to the medial epicondyle. Pronationand wrist flexion against resistance exacer-
316
Inherent stability by mechanical locking of components with hinge arrangement
Design of prosthesis allows 5˚–7˚ of rotation about flexion-extension,
varus-valgus and axial rotation
Three types of total elbow arthroplasty have been used. The constrained design replaced the elbow joint with a hinged prosthesis. All stability of the joint was dependent on the prosthesis which was not built to accommodate the rotational demands of the elbow joint. Due to an unacceptably high failure rate, this prosthesis has been abandoned. Results were better with an unrestrained prosthesis but with 5%–20% incidence of postoperative instability, most patients are now treated with a semi-constrained prosthesis, which has inherent stability by linking of the component usually with a hinge (shown above) or a snap-fit axis arrangement.
Figure 15-8: Prosthesis for Total Elbow Arthroplasty

Elbow and Forearm
bate the pain. As in lateral epicondylitis, elbowmotion and radiographic findings are usuallynormal. The differential diagnosis includes ul-nar nerve entrapment, medial elbow instabil-ity, and cervical radiculopathy. Treatmentprinciples for the noncompetitive athlete aresimilar to those used for lateral epicondylitis.
NERVE ENTRAPMENT SYNDROMESUlnar Nerve Entrapment
Compression of the ulnar nerve at the el-bow, or cubital tunnel syndrome, is the mostcommon cause of peripheral nerve entrap-ment after carpal tunnel syndrome (Figure 15-10). The cubital tunnel extends from 8 cmabove the medial epicondyle, where the ulnarnerve passes from the anterior to the posteriorcompartment of the arm, to 5 cm distal to theelbow, where the ulnar nerve enters the ante-rior compartment of the forearm. Compres-sion of the nerve may occur at any site withinthis tunnel. A hypermobile or subluxating ul-nar nerve also may produce symptoms, andthis condition may be aggravated by in-creased mobility and snapping of the medialtriceps.
Symptoms vary with the duration and theseverity of compression. Aching on the medialaspect of the elbow and numbness on the dor-
sal and palmar surfaces of the fingers inner-vated by the ulnar nerve that is aggravated byelbow flexion are typical (see Figure 15-4). Ex-amination shows a positive Tinel sign and al-tered ulnar nerve sensation in the fingers thattypically is exacerbated by flexion of the elbowand pressure on the ulnar nerve. Loss of sensa-tion on the dorsoulnar aspect of the wrist andhand and weakness of the intrinsic musclescausing decreased pinch and grip strengthmay or may not be present. The differential di-agnosis includes ulnar nerve entrapment at thewrist, cervical radiculopathy, thoracic outletsyndrome, and medial epicondylitis.
Nonoperative treatment may include night-time splinting to keep the elbow in a relativelyextended position, as well as avoidance ofprolonged leaning on the elbow, use of vi-brating tools, or activities that repetitively flexthe elbow. Operative treatment is recom-mended for persistent moderate or severesymptoms. The procedure most commonlyused is decompression and transposition ofthe nerve anterior to the medial epicondyle.
Median Nerve EntrapmentAt the elbow, entrapment of the median
nerve can occur at several locations, includ-ing an anomalous supracondylar process ofthe humerus and the lacertus fibrosus (Figure15-11). Fibrous constriction arches also mayentrap the nerve as it passes beneath the twoheads of the pronator teres or flexor digito-rum superficialis. The most common locationof entrapment is the pronator teres—hence,the alternative name, pronator syndrome.
Typical symptoms include an aching pain inthe mid to proximal forearm that is aggra-vated by repetitive lifting activities. Numb-ness and weakness in the median nerve distribution are variable and may be absent.Aggravation of symptoms after 90 seconds ofresisted pronation or resisted activity of theflexor digitorum superficialis of the long fingersuggests median nerve entrapment. Nerveconduction tests are less useful in this syn-drome but should be performed. A lidocaineand corticosteroid injection may be benefi-cial and diagnostic.
317
Epicondylitis (tennis elbow)Exquisite tenderness approximately1 cm distal to the lateral epicondyle
Figure 15-9: Epicondylitis

Chapter 15
318
Clinical signsInterosseousmusclewasting
Motorweaknessand musclewasting insevere cases
Nonsurgical management
Elbow pad
Furniture pad
Padding of elbowor of furniture mayprevent compression
Night splinting of elbowin mild flexion preventsnocturnal paresthesias
Tinelsign
Paresthesias indistribution ofulnar nerve
Elbow flexion test
Submuscular transposition of ulnar nerve
Biceps brachii m.
Brachialis m.
Medialintermuscular
septum
Tricepsbrachii m.
Medialepicondyle
Olecranon
Anterior transpositionof ulnar nerve
Divided tendonof origin
Lengthened and repairedflexor-pronator overtransposed nerve
Flexor carpiulnaris m.
Flexor-pronatormuscle mass
90˚ Z-plasty incision andlengthening of flexor-pronatorExposure of
ulnar nerve
Figure 15-10: Cubital Tunnel Syndrome

Elbow and Forearm
319
Pronator syndrome
Pain location
Hypesthesia andactivity-induced
paresthesias
Provocative maneuvers
Compression by flexordigitorum superficialismuscle
Flexion ofmiddle fingeragainstresistance
Compression bypronator teres muscle
Pronationagainstresistancewith forearmin supination
Compressionby lacertusfibrosus
Flexion ofwrist againstresistance
Supra-condylarprocess
Ligament ofStruthers
Medialepicondyle
Lacertusfibrosus
Pronator teres muscleHumeral head
Ulnar head
Flexor digitorum superficialismuscle and arch
Flexor pollicis longus muscle
Anterior interosseous syndrome
Normal Abnormal
Anterior interosseous n.
Mediannerve
Figure 15-11: Proximal Compression of Median Nerve

Chapter 15
320
The differential diagnosis includes muscletears in the proximal forearm and carpaltunnel syndrome. Carpal tunnel syndromecan be ruled out if there is loss of sensation atthe thenar eminence (supplied by the palmarbranch originating proximal to the wrist) orweakness of the flexor pollicis longus. Ifavoidance of inciting activities does not re-lieve the symptoms, surgical decompressionis indicated. All areas of possible compressionshould be explored.
Radial Nerve EntrapmentRadial nerve entrapment at the elbow typ-
ically involves compression of the posteriorinterosseous branch of the radial nerve, mostcommonly as it passes beneath the proximaledge of the supinator muscle at the arcadeof Frohse (Figure 15-12). Because the poste-rior interosseous nerve is purely motor, theposterior interosseous syndrome affects onlymotor function of the thumb, finger exten-sors, and extensor carpi ulnaris (see Figure15-5). Symptoms and signs of motor weak-ness are often vague in the early phase of thecondition, and radial tunnel syndrome some-times masquerades as a resistant lateral epi-condylitis.
Diagnosis is based on history and an exam-ination that typically shows tenderness overthe proximal supinator muscle (approxi-mately 5 cm distal to the lateral epicondyle).Pain is typically exacerbated by extension ofthe long finger against resistance with the el-bow extended.
Surgical decompression with release of theimpinging fibrous bands of the supinator mus-cle is usually helpful if symptoms are severe ordo not resolve after a period of observation.The course of the posterior interosseousnerve through the full extent of the supinatormuscle should be explored because entrap-ment also may occur in the midsubstance ofthe muscle and in its distal margin.
MISCELLANEOUS CONDITIONSAcute Sprains
The medial collateral ligament (MCL) com-plex includes the anterior bundle, the poste-
rior bundle, and the transverse ligament (Fig-ure 15-13). The anterior bundle of the MCLoriginates at the midportion of the medial epicondyle and inserts onto the coronoid tu-bercle of the ulna. The anterior bundle is theprimary restraint to valgus stress. Its eccentriclocation provides valgus restraint throughoutthe full arc of flexion-extension. With the el-bow in full extension, stability to valgus stressis conferred equally by the MCL, anterior cap-sule, and bony articulation. With the elbow in90°of flexion, the MCL provides 55% of val-gus stability. The contribution of the radio-capitellar articulation to valgus stability is sec-ondary and significant only when the anteriorbundle is disrupted.
The lateral collateral ligament (LCL) com-plex includes the radial collateral ligament, the annular ligament, the accessory lateralcollateral ligament, and the lateral ulnar collateral ligament. The lateral ulnar collateralligament originates from the anteroinferiorportion of the lateral epicondyle, inserts onthe supinator crest of the proximal ulna, and isthe primary lateral stabilizer. The annular liga-ment serves as a checkrein for the radial head.
Patients with acute sprains report a historyof acute pain after a fall or forceful throwinginjury. Valgus distraction injuries transmitloads primarily to the MCL complex and themedial flexor-pronator muscular origin. In-juries to the LCL typically occur with a varusstress to the elbow joint when it is in exten-sion and the forearm is in pronation. In acuteinjuries, the global swelling and tenderness,as well as the unreliability of stress maneu-vers, make it virtually impossible for the clin-ician to determine precisely which ligamentcomponents are injured. Avulsion fracturesmay be seen on radiographs. Short-term im-mobilization and gradual resumption of ac-tivities are successful in treating most acute elbow sprains.
Chronic Medial Elbow Pain andInstability
Medial elbow pain and MCL instability typ-ically develop in athletes involved in repeti-tive throwing activities. Pain is usually gradual

Elbow and Forearm
321
Motor signs
Posterior interosseoussyndrome
Proximal compression. Lossof wrist and finger extension
Pain locations in radial tunnel syndrome
Pain andtenderness
Painradiation
Provocative tests for radial tunnel syndrome
Supination against reisistance
Resist extension of longfinger with elbow extended
Provocative tests elicit painover radial tunnelSuperficial
radial nerveVascular
leash of Henry
Fibrous arcadeof Frohse
Posterior interosseousnerve
Innervation ofextensor muscles
Tendon ofbrachioradialis muscle
Superficial radialnerve at wrist
Radial nerveRecurrentradial artery
Posteriorinterosseousnerve
Extensorcarpi radialisbrevis muscle
Supinatormuscle
Figure 15-12: Radial Nerve Compression

Chapter 15
in onset, localized to the medial aspect of the elbow, and most severe during the accelera-tion phase of pitching (ie, the phase of pitch-ing in which maximum valgus stress is trans-mitted to the elbow). MCL disruption orattenuation is most often noted at the mid-substance of the anterior bundle. Concomi-tant symptoms of lateral elbow pain mayoccur secondary to the valgus overload, caus-ing compression, shear injury, and osteo-chondral fragments and/or osteochondritisdissecans of the capitellum.
Examination reveals tenderness on the me-dial aspect of the elbow. Valgus instability isassessed with the elbow in 25°of flexion to re-lax the ulnohumeral articulation. The patientshould be evaluated for the presence of aconcomitant ulnar entrapment neuropathy.Radiographs should be inspected for signs ofosteochondral loose bodies, medial osteo-phytes, and osteochondritis dissecans. Mag-netic resonance imaging (MRI) can be helpfulin preoperative planning.
Nonoperative treatment includes activitymodification followed by a gradual rehabilita-tion program. For persistent symptomatic instability, operative treatment includes recon-struction of the MCL with a tendon graft, re-moval of any associated osteophytes or loosebodies, and decompression of ulnar neuritis.
Posterolateral Rotatory ElbowInstability
Posterolateral rotatory instability developsafter injury to the ulnar collateral componentof the LCL. With a lax or attenuated ligament,patients report lateral elbow pain and catch-ing or giving way of the elbow. The lateralpivot test may be difficult to perform exceptwhen the patient is completely relaxed underanesthesia. MRI studies often identify the liga-ment disruption. Reconstruction of the lateralulnar collateral ligament with a tendon graft isrequired for treatment of persistent and dis-abling symptoms.
Rupture of the Distal Biceps TendonRupture of the distal biceps brachii tendon is
uncommon; however, timely diagnosis ofthese injuries is important because failure torecognize and repair the lesion before the onset of irreversible muscle contraction de-creases the strength of elbow flexion and fore-arm supination by 30% to 50%. Predisposingfactors include a male older than 40 years andthe presence of preexisting degenerativechanges in the tendon. Rupture typically oc-curs at the insertion of the biceps tendon intothe radial tuberosity (see Figure 15-13).
Injury results from an extension force on apartially flexed and contracting biceps muscle.
322
Humerus HumerusAnterior bundle ofulnar collateral ligament
Radius
Ulna
Joint capsule
Annular ligament of radius
Biceps brachii tendon
Oblique cord
Tricepsbrachiitendon
Joint capsuleAnterior collateral ligament
Annular ligament of radius
Biceps brachii tendonTricepsbrachiitendon
Sub-cutaneousolecranon
bursa
Lateral ulnar collateral ligament Transverseligament
Posterior bundle ofulnar collateral ligament
Subcutaneousolecranonbursa
In 90˚ flexion: lateral view In 90˚ flexion: medial view
Figure 15-13: Ligaments of Right Elbow Joint

Elbow and Forearm
Patients frequently report the acute onset ofsharp pain in the anterior aspect of the elbow,followed by a chronic, dull ache that is exac-erbated by lifting activities. Examinationshows tenderness and a defect in the antecu-bital fossa resulting from absence of the nor-mally prominent bicipital tendon. If theaponeurosis remains intact, the defect is notas obvious. If the tendon rupture is incom-plete, no defect is obvious, but the patient ex-periences pain and weakness on flexion of theelbow against resistance. Radiographs areusually normal. MRI may be helpful in evalua-tion of equivocal cases.
Partial ruptures can be managed withsplinting and activity modifications. Com-plete ruptures are treated more successfullywith operative repair. Injury to the radialnerve is a possible complication of surgicalrepair.
Olecranon BursitisThe olecranon bursa is easily irritated
because of its superficial location (see Figure15-13) and the tendency for people to leanon their elbows. Precipitating factors includefalls or direct blows, an inflammatory arthritissuch as rheumatoid arthritis or gout, and oc-cupations and avocations that cause pro-longed irritation. Olecranon bursitis also maydevelop in patients with chronic lung diseasewho lean on their elbows to aid breathing.Septic bursitis (infection) may occur primarily,but it is more likely to develop as a secondarycomplication of aseptic olecranon bursitis.
The onset of pain and swelling is relativelyrapid when caused by trauma or infectionbut is indolent when caused by other condi-tions. Pain is variable, exacerbated by elbow flexion, and more intense with infection. Ex-amination reveals a boggy swelling over theolecranon process. Erythema and increasedwarmth are common in patients with acutebursitis and universal in individuals with septicbursitis. Tenderness is less marked in chronic,recurrent aseptic bursitis.
If the olecranon bursitis is small and onlymildly symptomatic, treatment should includeobservation, avoidance of direct pressure,
and, occasionally, short-term splinting withthe elbow extended. Patients with more symp-tomatic bursitis should have the bursa aspi-rated for Gram stain and culture. Patients with-out infection should have the elbow protectedand immobilized in relative extension with afoam or compressive dressing. Patients withseptic bursitis require limited surgicaldrainage or daily aspiration and antibiotic ad-ministration that covers penicillin-resistantStaphylococcus aureus. Excision of a chroni-cally inflamed olecranon bursa should beavoided if at all possible because recurrence iscommon and operative treatment may lead tochronic infection.
FRACTURESGeneral Considerations
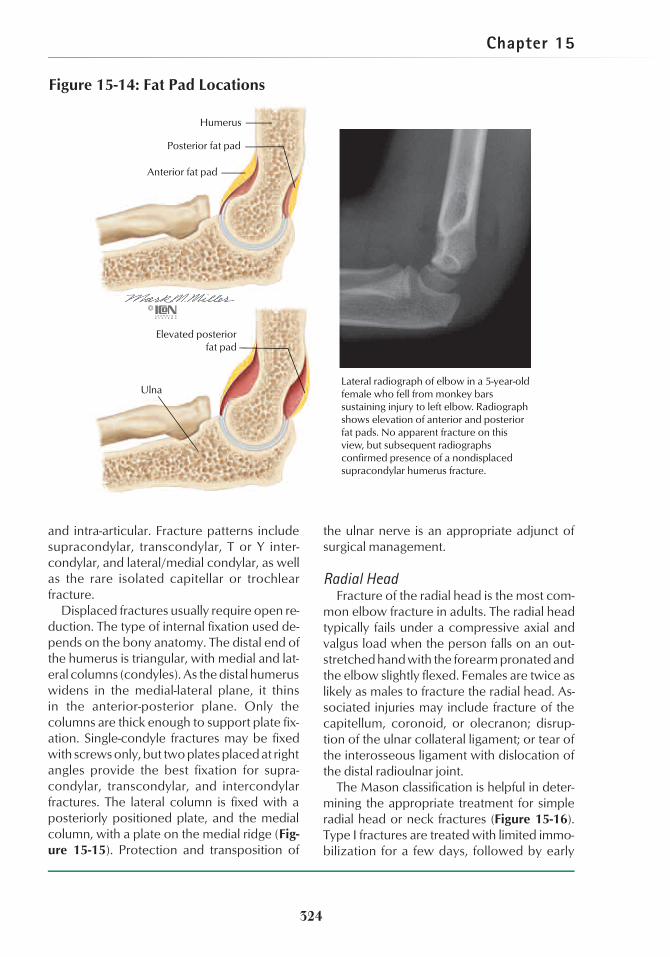
When a patient reports an injury to the el-bow or forearm, inspect for swelling, ecchy-mosis, deformity, and open wounds. Palpatethe area of maximum tenderness, and assessjoint swelling and distal pulses. Assess func-tion of the median, radial, and ulnar nerves.Anteroposterior and lateral radiographs ofthe elbow are adequate for assessing most el-bow injuries, but complicated intra-articularinjuries may necessitate oblique views andcomputed tomographic (CT) scans. The radialhead should point to the capitellum in bothanteroposterior and lateral views; otherwise,a dislocation or subluxation is present. Lookfor a fat pad sign if no fracture is obvious. In anormal elbow, the anterior fat pad can beseen on a lateral radiograph, but the posteriorfat pad is not visualized. Any process thatcauses an elbow effusion elevates both ante-rior and posterior fat pads (Figure 15-14).Forearm injuries necessitate anteroposteriorand lateral radiographs that visualize bonyanatomy from the elbow to the wrist.
Fractures about the Elbow in AdultsDistal Humerus
In adults, fractures of the distal humerus areusually caused by high-speed injuries withthe elbow flexed more than 90°. As a result,these fractures are frequently comminuted
323
Chapter 15
and intra-articular. Fracture patterns includesupracondylar, transcondylar, T or Y inter-condylar, and lateral/medial condylar, as wellas the rare isolated capitellar or trochlearfracture.
Displaced fractures usually require open re-duction. The type of internal fixation used de-pends on the bony anatomy. The distal end ofthe humerus is triangular, with medial and lat-eral columns (condyles). As the distal humeruswidens in the medial-lateral plane, it thinsin the anterior-posterior plane. Only thecolumns are thick enough to support plate fix-ation. Single-condyle fractures may be fixedwith screws only, but two plates placed at rightangles provide the best fixation for supra-condylar, transcondylar, and intercondylarfractures. The lateral column is fixed with aposteriorly positioned plate, and the medialcolumn, with a plate on the medial ridge (Fig-ure 15-15). Protection and transposition of
the ulnar nerve is an appropriate adjunct ofsurgical management.
Radial HeadFracture of the radial head is the most com-
mon elbow fracture in adults. The radial headtypically fails under a compressive axial andvalgus load when the person falls on an out-stretched hand with the forearm pronated andthe elbow slightly flexed. Females are twice aslikely as males to fracture the radial head. As-sociated injuries may include fracture of thecapitellum, coronoid, or olecranon; disrup-tion of the ulnar collateral ligament; or tear ofthe interosseous ligament with dislocation ofthe distal radioulnar joint.
The Mason classification is helpful in deter-mining the appropriate treatment for simpleradial head or neck fractures (Figure 15-16).Type I fractures are treated with limited immo-bilization for a few days, followed by early
324
Anterior fat pad
Posterior fat pad
Elevated posteriorfat pad
Humerus
UlnaLateral radiograph of elbow in a 5-year-old female who fell from monkey barssustaining injury to left elbow. Radiograph shows elevation of anterior and posterior fat pads. No apparent fracture on this view, but subsequent radiographsconfirmed presence of a nondisplaced supracondylar humerus fracture.
Figure 15-14: Fat Pad Locations

Elbow and Forearm
325
Fracture of lateral condyle of humerus. Fracture of medial condyle less common
Fractured condyle fixed with one or two compression screws
Articular surface of distal humerus reconstructed and fixed with transverse screw and buttress plates with screws. Ulnar nerve may be transposed anteriorly to prevent injury. Lateral column fixed with posterior plate and medial column fixed with plate on the medial ridge.
Olecranon reattached with longitudinal Kirschner wires and tension band wire wrapped around them and through hole drilled in ulna
Olecranon osteotomized and reflected proximally with triceps brachii tendon
Open (transolecranon) repair. Posterior incision skirts medial margin of olecranon, exposing triceps brachii tendon and olecranon. Ulnar nerve identified on posterior surface of medial epicondyle. Incisions made along each side of olecranon and triceps brachii tendon
Intercondylar (T or Y) fracture of distal humerus
Medial epicondyle of humerus
Triceps brachii tendon
Extensor carpi radialislongus muscle
Anconeusmuscle
Olecranon
Ulnar nerveLateral
epicondyle
Figure 15-15: Elbow Fractures

Chapter 15
range-of-motion exercises. Type II fractureswith acceptable fracture patterns should betreated with open reduction and internal fixa-tion. In equivocal situations, particularly if thepatient has a low-demand occupation, type IIinjuries can be treated nonoperatively, with de-layed excision of the radial head if persistentpain or significant limitation of forearm rota-tion occurs. Uncomplicated type III fracturesshould be treated with excision of the radialhead. When radial head fractures are associ-ated with dislocation of the elbow and severeligament injury or disruption of the forearm
interosseus, the fragments should be removedand the radial head replaced by a prosthesis.
Results of treatment are uniformly good fortype I fractures and often satisfactory for sim-ple type II and type III fractures. Potentialcomplications include loss of motion, elbowinstability, posttraumatic arthritis, myositis os-sificans, and distal radioulnar symptoms.
Olecranon FracturesOlecranon fractures are caused by a direct
blow or an indirect avulsion injury (eg, a fallon an outstretched hand with the elbow
326
Type I: nondisplaced or minimally displaced.
Type II: displaced single fragment (usually >2 mm) of the head or angulated (usually >30°) of the neck.
Type III: severely comminuted fractures of the radial head and neck.
Excision of fragment or entire radial head via posterolateral incision. Radial head should be replaced with a prosthesis in patients with certain complex fractures.
Comminuted fracture of radial head with dislocation of distal radioulnar joint, proximal migration of radius, and tear of interosseous membrane (Essex-Lopresti fracture)
Figure 15-16: Fracture of Head and Neck of Radius

Elbow and Forearm
slightly flexed while the triceps is contracting).Avulsion injuries create a transverse or slightlyoblique fracture pattern. Direct blows typi-cally are associated with some degree ofcomminution. A palpable defect is presentwith displaced fractures. The skin should beevaluated carefully for possible open injury.Radiographs should be scrutinized for detec-tion of associated fractures of the radial heador coronoid process.
Nondisplaced fractures can be treated witha splint or cast (Figure 15-17). The elbow ispositioned in approximately 45°of flexion torelax the pull of the triceps. Displaced frac-tures require open treatment. Tension bandwiring, which transforms distraction forcesinto compression, is the most common formof fixation. Plate fixation is required for frac-tures that extend to the coronoid or ulnarshaft. Comminuted fractures can be managedby excision of the fragments and repair of thetriceps tendon. If the collateral ligaments areintact, as much as 70% of the proximal ole-cranon can be excised without resultant in-stability.
Monteggia Fractures/DislocationsThe Monteggia fracture/dislocation is a
fracture of the ulna that is associated withdislocation of the radial head (Figure 15-18).Bado classified these injuries into four types.The radial head is dislocated anteriorly intype 1, posteriorly in type 2, and laterally in
type 3, and the ulnar fracture is angulated inthe direction of the radial head dislocation.In a type 4 injury, the proximal radius andulna are fractured, and the radial head is dis-located anteriorly. Type 1 and type 2 ac-count for 70% to 90% of Monteggia injuries.Type 1, the most common, may be causedby a direct blow or a fall on the outstretchedhand with the forearm in full pronation. Type2 injuries occur most often in adults. Radialnerve injury, often isolated to the posteriorinterosseous branch, is relatively common inMonteggia lesions.
These injuries are frequently misdiagnosed,particularly in children, in whom palpation ofan anteriorly displaced radial head is more difficult. Another common mistake is to rec-ognize the fracture of the ulna but miss thedislocated radial head, either because the ra-diograph did not adequately show the elbowor because the evaluator did not understandthat on both anteroposterior and lateral ra-diographs, a line through the axis of the prox-imal radius and the radial head should passthrough the capitellum.
If recognized early, Monteggia injuries inchildren usually can be treated by closed re-duction and cast immobilization. Adults re-quire open reduction and internal fixation ofthe ulnar fracture. When the ulna is anatomi-cally reduced, the radial head typically re-duces and becomes stable without additionalsurgical intervention.
327
Displaced fracture of olecranon requires open reduction and internal fixation
Open reduction of olecranon fracture. Fracture secured with two Kirschner wires plus tension band wire passed around bent ends of Kirschner wires and through drill hole in ulna
Figure 15-17: Olecranon Fracture

Chapter 15
328
Type 1 Monteggia fracture/dislocation with anterior dislocation of radial head and anterior angulation of proximal or middle third ulna fracture
Less common type 2 Monteggia fracture/dislocation with ulna fracture angulated posteriorly and radial head
dislocated posteriorly
Fracture of ulna treated with open reduction and internal fixation using compression plate
and screws. After reduction of ulna, radial head spontaneously reduced
Preoperative radiograph shows Type I Monteggia fracture/dislocation
Postoperative radiograph shows compression plate in place
Anconeus m.
Annular ligament(sutured)
Extensor carpi ulnaris m.
If radial head does not reduce after angulation of ulna is corrected, open reduction of radial head dislocation and repair of annular ligament are needed. Typically, this is done through a separate incision between the anconeus and extensor carpi ulnaris muscles
Radius
Supinator m. (incised)
Ulna
withC.A. Luce
Figure 15-18: Monteggia Fracture/Dislocation

Elbow and Forearm
Fractures of the Diaphysis of the Radiusand Ulna
In adults, motor vehicle accidents or fallsfrom a considerable height usually causeboth-bone forearm fractures. Displacement,angulation, and shortening are commonwhen both the radius and the ulna are frac-tured. A direct blow usually fractures onlyone bone—typically the ulna, as the forearmis positioned to stop the oncoming injury(“nightstick” fracture). Because only onecomponent of the “structural rectangle”has been disrupted, direct-blow injuries ofthe ulna or radius are minimally displacedand usually can be treated by nonopera-tive methods. However, a fall on the out-stretched hand with the forearm pronatedcan cause a fracture at the middle/distalthird junction of the radius with associateddisruption of the distal radioulnar ligaments(Galeazzi fracture). In this injury, two sidesof the structural rectangle are injured; there-fore, the fracture of the radius is displacedand unstable.
Displaced forearm fractures in adults arebest treated by open reduction and internalfixation. This procedure minimizes the rela-tively high rates of malunion, nonunion, andloss of forearm rotation associated with man-agement by closed techniques. Bone graftingshould be considered with comminution ofmore than a third of the diameter of the boneor with a segmental fracture.
Fractures About the Elbow inChildren
Fractures about the elbow are more com-mon in children than in adults, and treatmentin children often differs from treatment of in-juries at similar locations in adults. Occultfractures are more common in children, par-ticularly young children, in whom low-impactfalls are common. A significant portion of thebone in young children has not ossified, sosome fractures are more difficult to visualizeon initial radiographs. A child who has a his-tory of injury, tenderness about the elbow,and a positive posterior fat pad sign should beassumed to have an occult fracture andshould be immobilized for 3 weeks.
Supracondylar FracturesFracture of the supracondylar humerus is
the most common elbow fracture in children.The typical age group is 2 to 12 years—a timewhen a child is able to hyperextend the el-bow. The typical mechanism of injury is a fallon the outstretched arm with the elbow in fullextension. The distal fragment is displacedposteriorly (Figure 15-19). The less commonflexion injuries cause anterior displacementof the distal humerus and are more commonin the adolescent years.
Supracondylar fractures are associatedwith a relatively high incidence of neurovas-cular injury. Usually only one nerve is injured.The median, radial, or ulnar nerve may be
329
Extension typePosterior displacement of distal fragment (most common). In general, supracondylar fractures occur more frequently in children
Flexion typeAnterior displacement of distal fragment (uncommon in children)
Figure 15-19: Supracondylar Fracture of the Humerus

Chapter 15
involved. Median nerve injury, the most com-mon type, may be limited to the anterior in-terosseous branch. Compartment syndromeof the forearm may occur, and failure to treatthis problem in a timely fashion may result inVolkmann ischemic contractures of the wristand fingers. Malunion with resultant cubitusvarus is another potential complication.
To minimize the risk of complications, dis-placed fractures typically are treated withclosed manipulation and percutaneous pin-ning. If the radial and ulnar pulses are absent,the fracture is reduced. Frequently, the pulsereturns after the fracture is reduced and theproximal fragment no longer stretches thebrachial vessels. If the pulse does not returnbut the capillary refill is normal and there areno signs of compartment syndrome, the pa-tient may be treated with observation withcareful monitoring. If the pulse does not re-turn after the fracture has been reduced andthe fingers or forearm show signs of ischemia,the vessels should be explored.
Cubitus varus, the “gunstock deformity,” re-sults from malrotation and the resultant tilt ofthe distal fragment. The thin, spadelike shapeof the distal humerus, in combination with aswollen arm and the small size of a child’sbone, is a predisposing factor. The deformityis primarily a cosmetic rather than a functionalproblem.
Transphyseal Fracture Separation of theDistal Humerus
Transphyseal separations of the distalhumerus typically occur in infants and youngchildren as a result of child abuse. Radio-graphs may be difficult to interpret becausethe secondary centers of ossification have notdeveloped in children this young. Typically,the proximal forearm is displaced mediallyand posterior to the humeral shaft. Arthrogra-phy, MRI studies, or ultrasonography may benecessary to distinguish this lesion from an el-bow dislocation or lateral condylar fracture.
Lateral and Medial Condyle FracturesFracture of the lateral condyle of the distal
humerus is the second most common elbow
injury in children. Lateral condyle fractures re-sult from a fall on a varus, supinated elbow,with the condyle avulsed by attached exten-sor muscles. Medial condyle fractures are un-common, but the treatment principles are thesame as for lateral condyle fractures. Whenthese fractures cross the articular surface, dis-placement .1 mm at the joint requires re-duction and pinning to minimize associatedproblems of nonunion, cubitus valgus, tardyulnar nerve palsy, and traumatic arthritis.
Lateral and Medial Epicondyle FracturesLateral epicondyle fractures are uncommon
in children, but avulsion of the medial epi-condyle by forceful contraction of the flexor-pronator muscles with the elbow in valgus isthe third most common pediatric elbow frac-ture. The injury typically occurs in a 10- to 15-year-old child. A concomitant posterior dislo-cation of the elbow may occur. In this situation,open reduction should be performed if the me-dial epicondyle fragment is incarcerated in thejoint. Otherwise, medial epicondyle fractures,even when markedly displaced, do not com-monly cause residual disability and can betreated with short-term splinting.
Radial Neck FracturesIn children, fracture of the proximal radius
typically involves the physis, with extensioninto the neck of the radius (Peterson II orSalter II). The typical age group is 7 to 12years. Associated injuries may include frac-ture of the olecranon or medial epicondyle, aswell as dislocation of the elbow. Isolated frac-tures result from a fall on an extended elbowwith valgus stress.
Treatment depends on the age of the childand the degree of angulation. Tilt of morethan 30° may result in loss of forearm rota-tion. With more than 30° angulation, closedreduction with or without percutaneous ma-nipulation of the fracture should be at-tempted with the goal of reducing angulationto less than 30°. Open reduction may be re-quired but has a greater risk of osteonecrosisof the radial head and synostosis between the radius and ulna. Premature fusion of the
330

Elbow and Forearm
physis usually is of little significance, because80% of the growth of the radius occurs at thedistal physis.
Olecranon Fractures and DiaphysealFractures of the Radius and Ulna
Olecranon fractures are uncommon inchildren and are likely to be nondisplaced. Dis-placed fractures usually require open reduc-tion and tension band wire and pin fixation.
Most diaphyseal forearm fractures in chil-dren can be managed by closed techniques.Proximal and middle third forearm fracturesaccount for only 15% to 20% of pediatricforearm fractures, but these injuries are morelikely to develop complications such as com-partment syndrome, malunion, or synostosis.
Dislocation of the ElbowThe elbow is the most commonly dislo-
cated joint in children and the second mostcommon site of dislocation in adults (Figure15-20). Posterior dislocations are most com-mon. Anterior dislocation is rare because ofthe shape of the olecranon process. Diver-gent dislocation with separation of the radiusand the ulna results from severe disruption ofthe soft tissues.
Posterior dislocations typically occur in afall on the outstretched hand with the shoul-der abducted. Axial compression at the el-bow combined with an external and valgusstress at the elbow (the body internally ro-tates) results in a continuum of ligamentousinjury that typically starts laterally and moves
331
Posterior dislocation. Note prominence of olecranon posteriorly and distal humerus anteriorly
Fracture of coronoid process of ulna with posterior dislocation of elbow. Coronoid fracture may occur occasionally without dislocation
Divergent dislocation, anterior-posterior type (rare). Medial-lateral type may also occur (extremely rare)
Posterior dislocation with fracture of both coronoid process and radial head. Rare but serious; poor outcome even with good treatment. May require total elbow replacement
Figure 15-20: Dislocation of Elbow Joint

Chapter 15
medially. The first stage tears the ulnar portionof the lateral collateral ligament (LCL), fol-lowed by disruption of the entire LCL com-plex, then the anterior and posterior capsules,then the posterior band of the medial collat-eral ligament (MCL), and lastly, the anteriorband of the MCL. Associated injuries may include avulsion of the medial and lateral epicondyles, radial head and radial neck frac-tures, and coronoid fractures. These addi-tional injuries increase instability and may necessitate internal fixation.
Isolated dislocation of the elbow is treatedby closed reduction. Distal traction is appliedwith the elbow in extension and the forearmin supination. After reduction, elbow stabilityis assessed with the forearm in pronation. Ifligament disruption involves the anteriorband of the medial collateral ligament, insta-bility is noted with the elbow in extension.This injury will need 3 to 6 weeks of protec-tion, starting with the elbow in pronation and90°of flexion. More stable injuries should beimmobilized for a short time (1 to 2 weeks) toprevent the complications of elbow stiffnessand loss of extension. Other complications,such as heterotopic ossification, brachialartery injury, ulnar nerve injury, and compart-ment syndrome, are associated with high-energy injuries and concomitant fractures.
Subluxation of the Radial HeadSubluxation of the radial head, also called a
“pulled elbow” or “nursemaid’s elbow,” isthe most common elbow injury in childrenyounger than 5 years. Subluxation occurswith a pull on the forearm when the elbow isextended and the forearm pronated. The an-nular ligament (see Figure 15-13) slips proxi-mally and becomes interposed between theradius and the ulna. This injury is associatedwith ligamentous laxity, a condition that is al-most universal in young children and typicallyoccurs when a young child is “helped along”or lifted by pulling on the forearm.
Immediately after the injury, the child willcry, but the initial pain quickly subsides. There-after, the child is reluctant to use the arm butotherwise does not appear to be in great dis-
tress. The extremity is held with the elbowslightly flexed and the forearm pronated. Ten-derness over the radial head and resistance onattempted supination are the only consistentfindings. Radiographic findings are normal.
Reduction is accomplished by applyingpressure over the radial head, followed byquick supination. If this maneuver fails to pro-duce the snap of reduction, the elbow shouldbe flexed. Resistance is perceived just beforefull flexion. As the elbow is pushed throughthat resistance, the annular ligament will re-duce, and a snap will be perceived as the ra-dial head is reseated. If the reduction is suc-cessful, the child will resume use of theextremity in a few minutes. In a child who pre-sents for evaluation 1 to 2 days after injury,however, swelling may obscure the snap ofreduction and deter the immediate resump-tion of normal function. If the elbow has fullflexion and supination, the radial head hasbeen reduced. Immobilization is ineffectiveas slings are quickly discarded.
PEDIATRIC DISORDERSCongenital Dislocation of the Radial Head
Isolated congenital dislocation of the radialhead, although present at birth, is usually notdiagnosed until a child is 2 to 5 years of age,when the parents note mild limitation ofelbow extension and an abnormal promi-nence (Figure 15-21). The dislocation may be bilateral or unilateral. Most dislocations areposterior or posterolateral, but they may beanterior. The limitation of motion is rarely dysfunctional, and most patients are asymp-tomatic. Excision of the radial head, after com-pletion of growth, is indicated for relief of painfrom joint incongruity; however, elbow mo-tion does not improve after the procedure.
Congenital Radioulnar SynostosisCongenital radioulnar synostosis is an un-
common congenital abnormality caused byfailure of separation of the proximal radiusand ulna during fetal development. As a re-sult, forearm rotation is lost. The synostosisis frequently an isolated event but may be
332

Elbow and Forearm
associated with other conditions. Most casesinvolve some degree of fixed pronation. Thedegree of disability depends on the amountof fixed pronation and whether the conditionis unilateral or bilateral. Patients with bilateralinvolvement and forearms fixed in greaterthan 60°of pronation have the greatest diffi-culty with activities such as holding a fork,dressing, and maintaining good personal hy-giene after bowel movements. Patients withless fixed pronation often can substituteshoulder motion.
Surgery to resect the synostosis and restoremotion has not been successful. Rotationalosteotomy through the synostosis to changethe position of the forearm varies accordingto the amount of functional impairment. Typi-
cally, the dominant forearm is positioned in0° to 20°of pronation. Compartment syn-drome is the most common postoperativecomplication.
Osteochondrosis of the ElbowChildren involved in repetitive throwing ac-
tivities or gymnastics repetitively overload theelbow into valgus with tension on the medialepicondyle and compression on the capitel-lum. Traction apophysitis of the medial epi-condyle, better known as “little leaguer’s elbow,” may develop. The resultant pain re-sponds well to a relatively short period of rest.
Chronic lateral elbow pain in pediatric ath-letes usually occurs secondary to osteonecro-sis of the capitellum and is more problematic.
333
Anteroposterior and lateral radiographs reveal posterior dislocation of radial head, most evident on elbow flexion.Note also hypoplastic capitulum of humerus.
Lateral view of upper extremity reveals posterior bulge of head of radius and inability to fully extend elbow
Figure 15-21: Congenital Dislocation of Radial Head

Chapter 15
When osteonecrosis occurs in childrenyounger than 10 years, the condition is calledPanner disease and has a good prognosis forhealing with a period of rest and, sometimes,immobilization. When the condition occursduring adolescence, it is called osteochondri-tis dissecans of the capitellum and has a moreguarded prognosis.
Adolescents with osteonecrosis of thecapitellum report the insidious onset of lateralelbow pain that is aggravated by throwing ac-tivities. Examination shows tenderness overthe lateral elbow, tenderness at the extremesof passive elbow motion, and a flexion con-tracture of 10° to 30°. Typical radiographicchanges include lucency and fragmentation of
the anterior central capitellum (Figure 15-22).Osteochondral loose bodies may be present.An MRI study often helps define the extent ofosteonecrosis. Treatment for patients in thisage group includes activity modification, exci-sion of osteochondral fragments, and occa-sionally, drilling of the defect to stimulate afibrocartilaginous response.
ADDITIONAL READINGSChen FS, Rokito AS, Jobe FW. Medial elbow problems in
the overhead-throwing athlete. J Am Acad OrthopSurg. 2001; 9:99–113.
Morrey BF, ed. The Elbow and Its Disorders, 2nd edition.Philadelphia, Pa: Saunders; 2000.
Staheli LT, ed. Pediatric Orthopaedic Secrets, 2nd edition.Philadelphia, Pa: Hanley and Belfus; 2003.
334
Characteristic changes in capitulum of left humerus (arrow) compared with normal right elbow
Bone resorption seen as radio-lucent areas and irregular surface of capitulum of humerus
Figure 15-22: Osteochondrosis of the Capitellum