
Fibrous and Fibrohistiocytic Proliferations of the Skin P.II
125
FIBROUS AND FIBROHISTIOCYTIC PROLIFERATIONS OF THE SKIN P.II WWW.FACEBOOK.COM/GROUPS/DERMATOLOGYCOURSEONLINE
-
Upload
ibrahim-mohammed -
Category
Health & Medicine
-
view
318 -
download
3
Transcript of Fibrous and Fibrohistiocytic Proliferations of the Skin P.II
FIBROUS AND FIBROHISTIOCYTIC PROLIFERATIONS OF THE SKIN P.IIWWW.FACEBOOK.COM/GROUPS/DERMATOLOGYCOURSEONLINE

DERMATOFIBROMA












It dimples inward with lateral pressure Dimple sign

On applying pressure around DF smooth, firm nodule can be palpated under the skin (black arrows) & a dimple can be seen in the center (blue arrow)



Cellular dermatofibroma

Polypoid nodular dermatofibroma

OVERVIEW
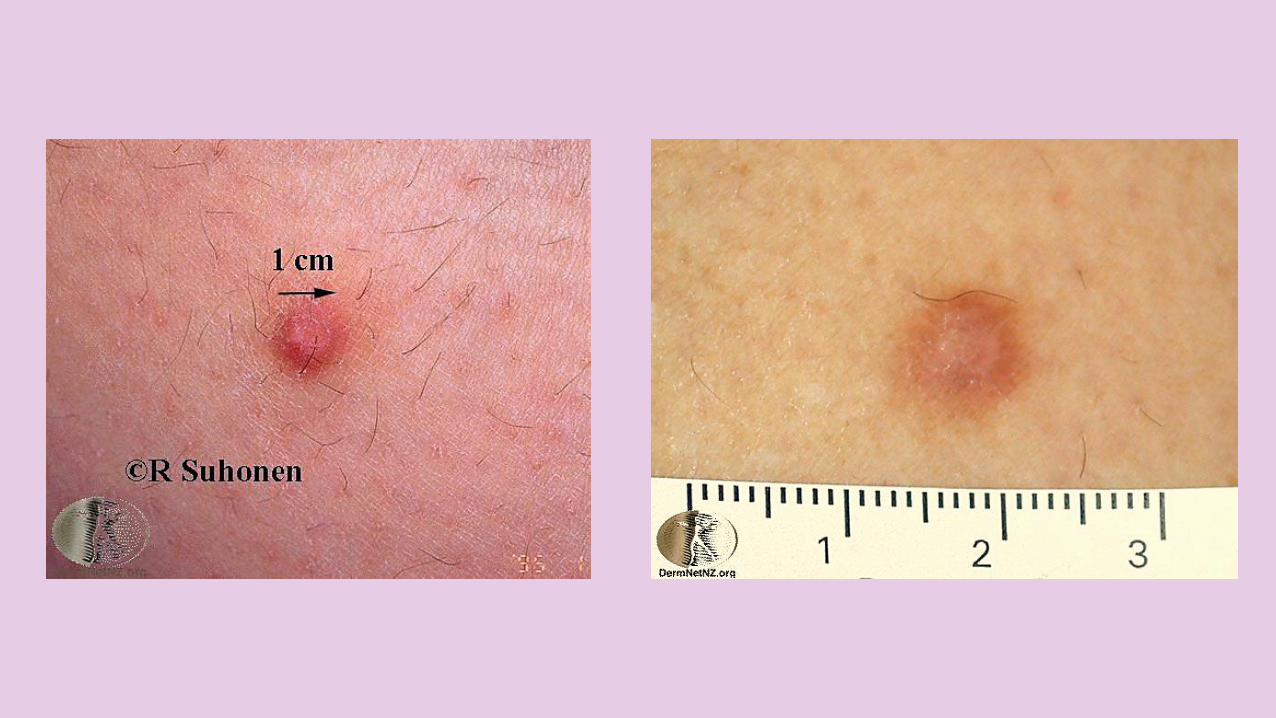
A dermatofibroma (DF) is a COMMON SLOWLY-GROWINGBENIGN FIBROHISTIOCYTIC skin lesion that usually has OVERLYINGHYPERPIGMENTATION on the LOWER EXTREMITIES.
Also called BENIGN FIBROUSHISTIOCYTOMA.
DERMATOFIBROMA
ETIOLOGY
The exact cause is UNKNOWN, but the lesions are thought to arise at sites of prior MINOR TRAUMA or as a late dermal dendritic HISTIOCYTIC REACTION to an ARTHROPOD BITE.
WHETHER it is due to a NEOPLASMor REACTIVE PROCESS is debated.
DERMATOFIBROMA
CLINICAL FEATURES
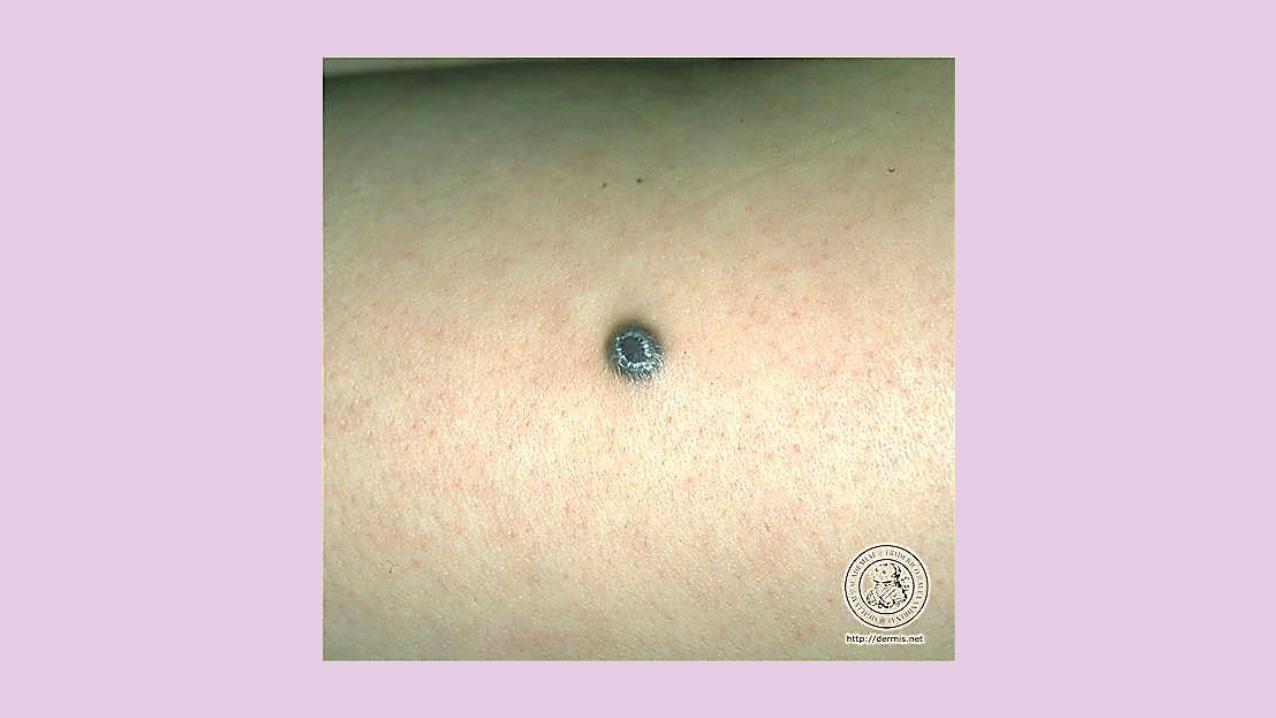
They appear as ROUND or OVOIDSINGLE FIRM DERMAL NODULES, often YELLOW-BROWN in colour, sometimes PINK (especially in fair skinned individuals) and sometimes quite DARK, (especially in dark colored skin).
POLYPOID, FLAT, DOME SHAPED or DEPRESSED.
DERMATOFIBROMA

CLINICAL FEATURES
If the skin over a dermatofibroma is SQUEEZED a DIMPLE (central depression) FORMS DIMPLESIGN or FITZPATRICK'SSIGN indicating TETHERING of the skin to the UNDERLYINGFIBROUS TISSUE.
DERMATOFIBROMA

CLINICAL FEATURES
More commonly in FEMALES.
Most commonly on the LOWEREXTREMITIES (most common growth below the knee in young adults) & ARMS, but may be seen in any location.
Once developed, they usually PERSIST FOR YRS.
DERMATOFIBROMA


A white centre (blue arrows) and a peripheral pigment network (black arrows)


CLINICAL VARIANTS
1. MULTIPLE ERUPTIVE DERMATOFIBROMAS may be seen in normal individuals but also associated within immunosuppression or SLE.
2. CELLULAR DERMATOFIBROMA- 5% of all dermatofibromas and is clinically larger than more typical lesions.
3. POLYPOID NODULAR DERMATOFIBROMA
DERMATOFIBROMA


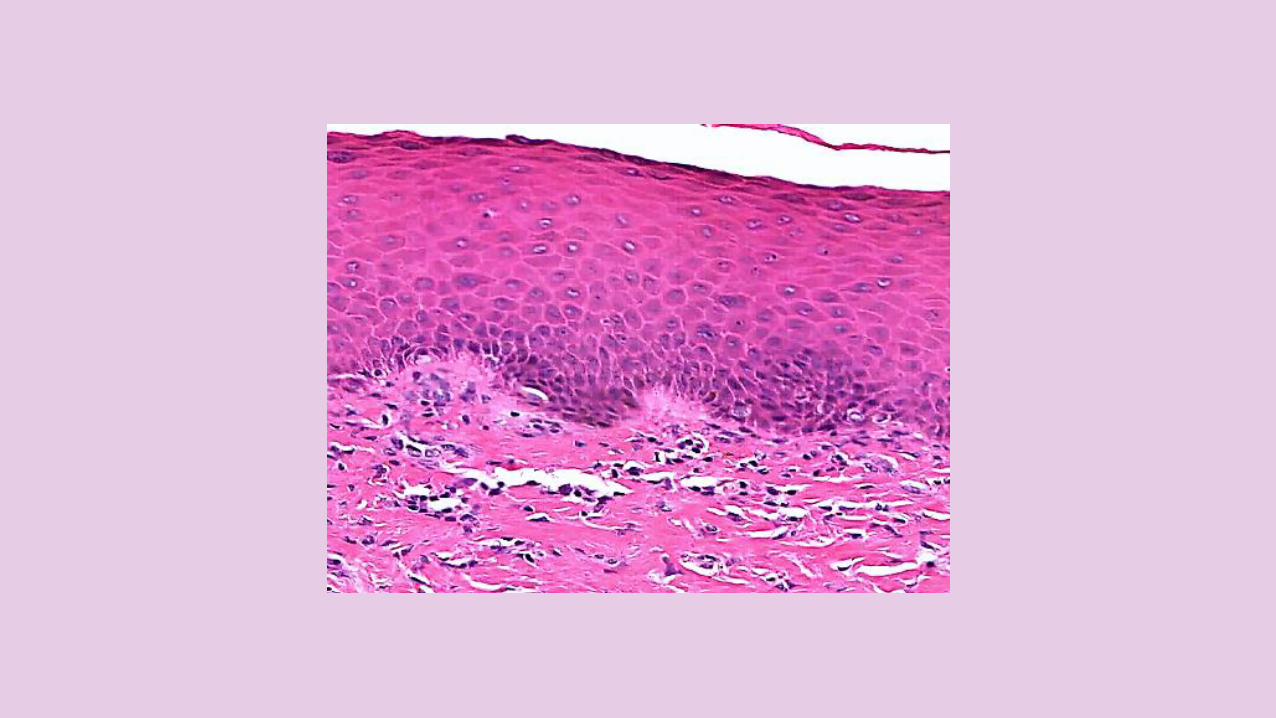
Typical epidermal change of dermatofibroma-induced hyperkeratosis, acanthosis and basal layer hyperpigmentation

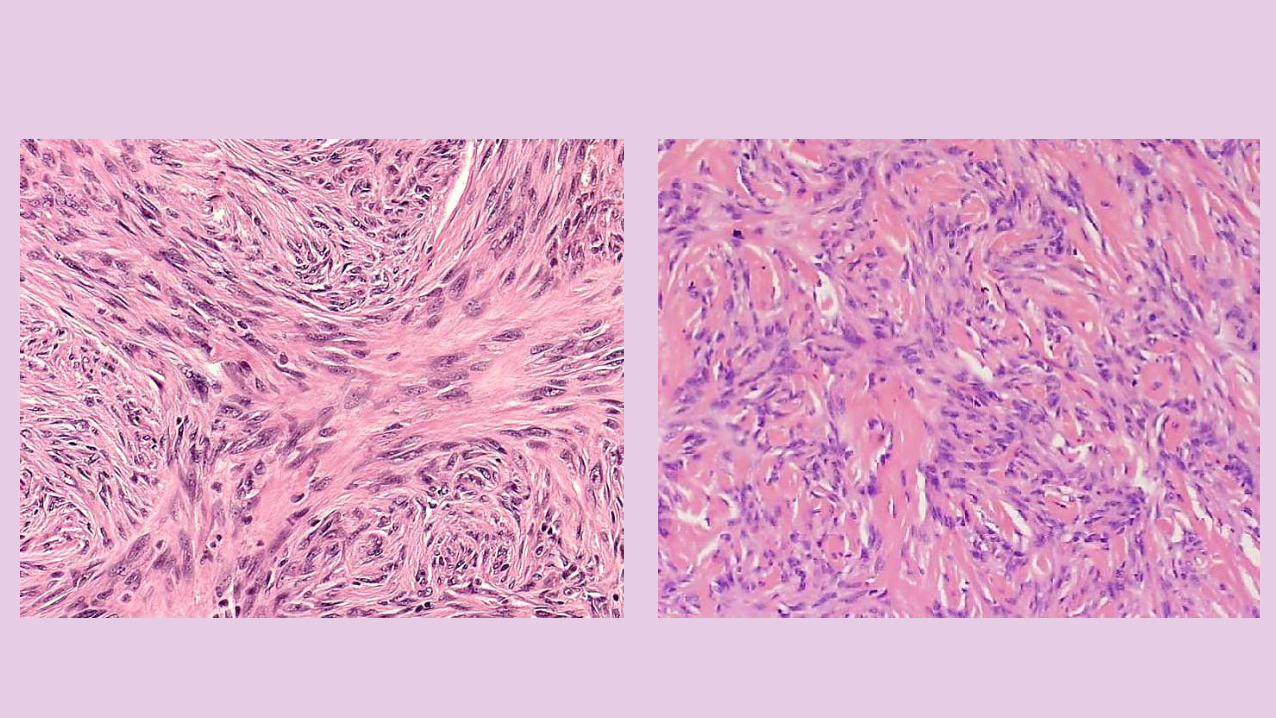
Collagen trapping



Tumor cells with vacuolated cytoplasm (foam cells)
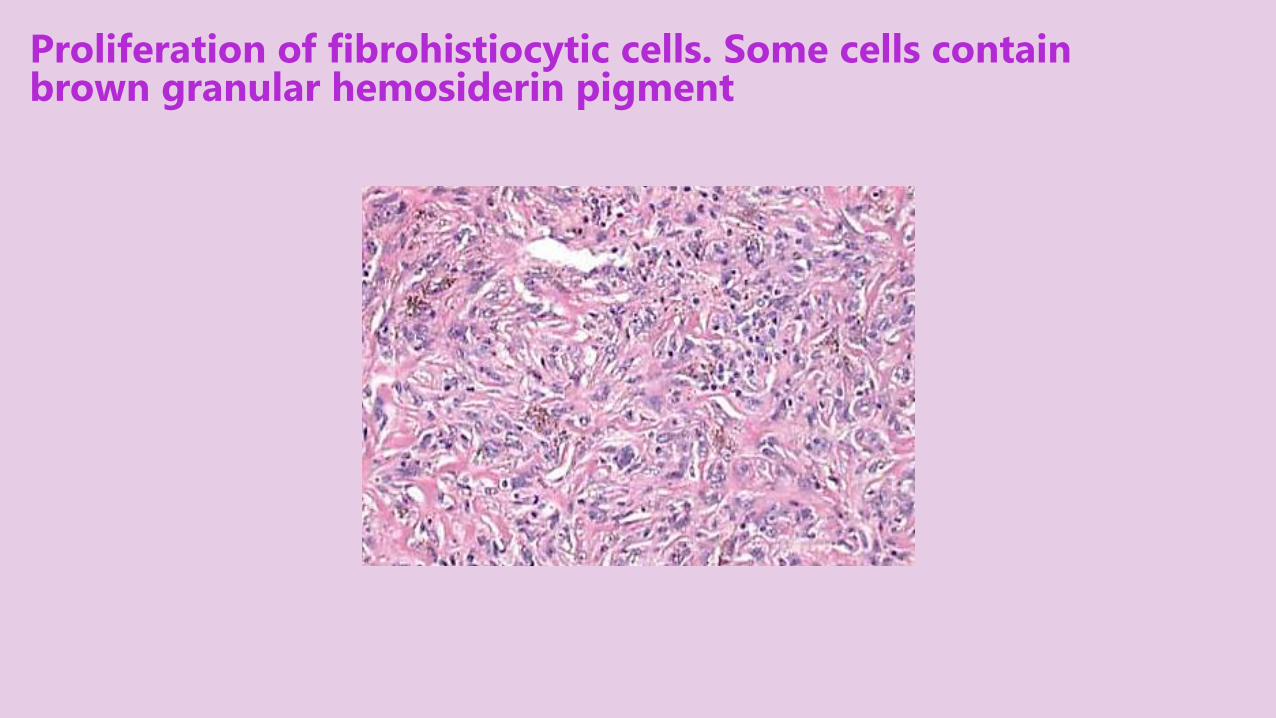
Proliferation of fibrohistiocytic cells. Some cells contain brown granular hemosiderin pigment

Basaloid induction
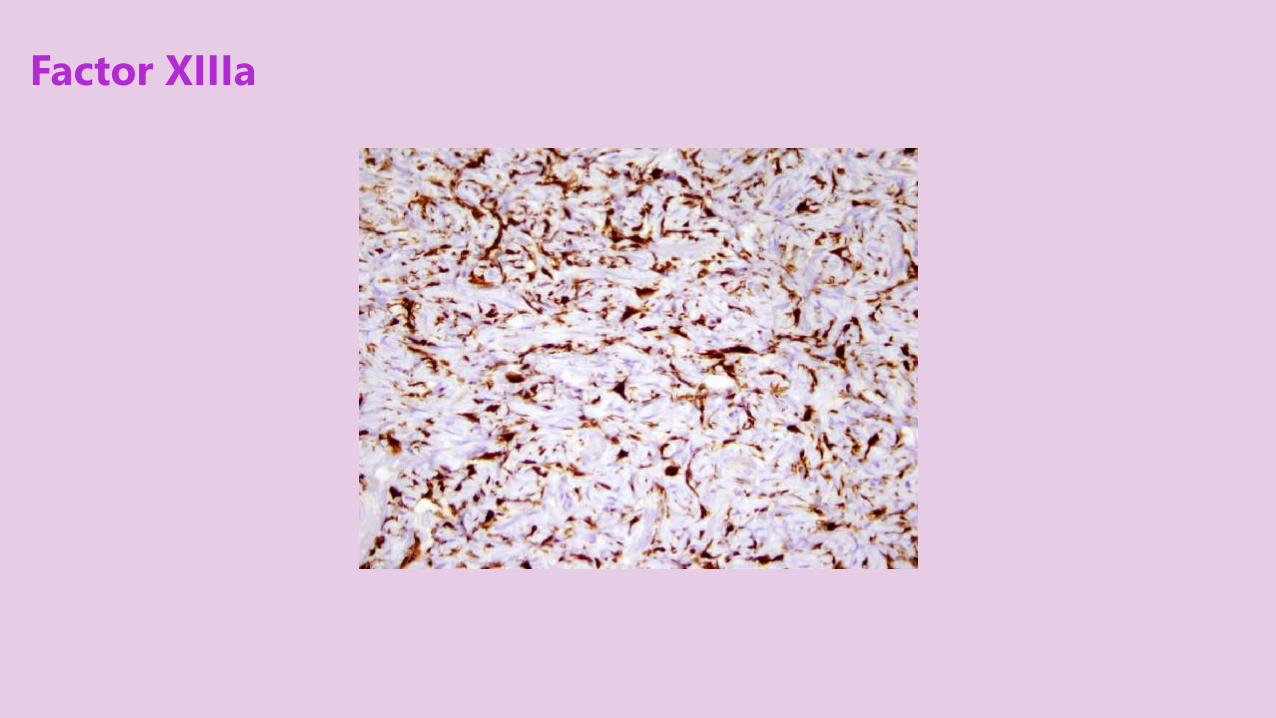
Factor XIIIa

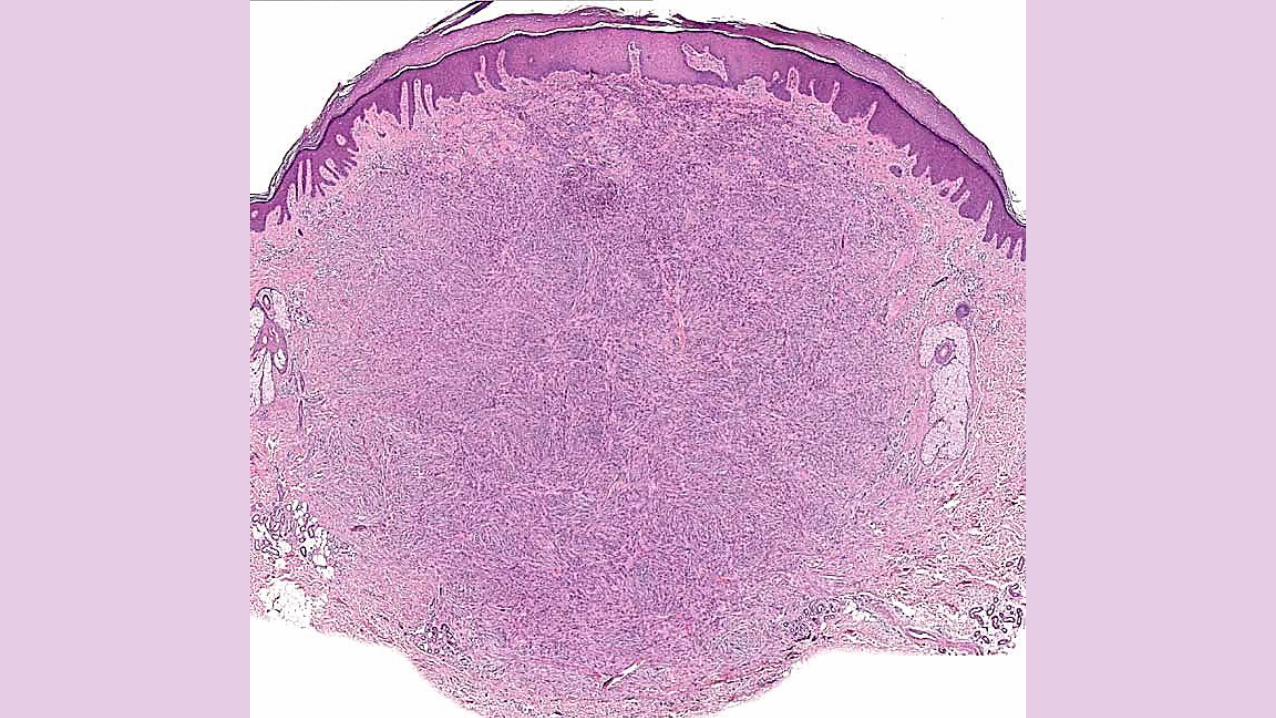
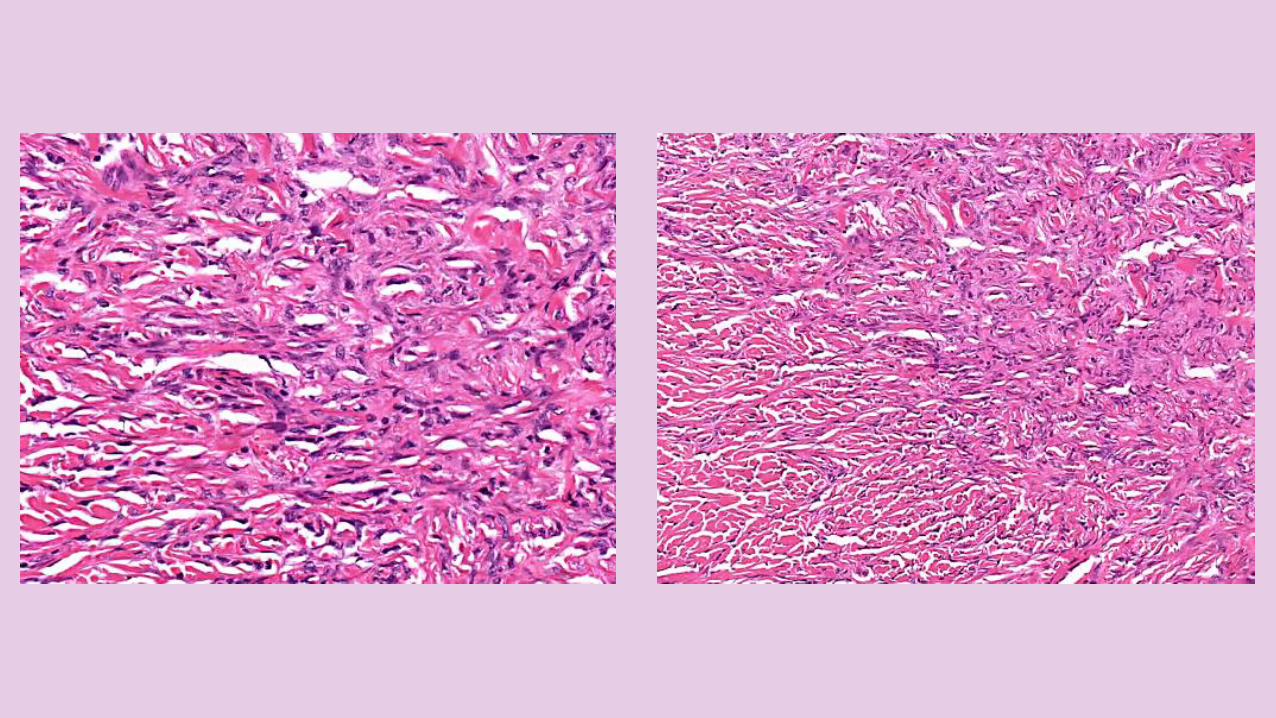
HISTOPATHOLOGY
Large BUNDLESof KELOIDALCOLLAGEN.proliferation of SPINDLEDFIBROBLASTS around the collagen bundles “COLLAGEN TRAPPING” at the PERIPHERY.LIPID LADEN HISTIOCYTES, and MULTINUCLEATE GIANT CELLS sometimes the cells contain HEMOSIDERIN pigment.
DERMATOFIBROMA
HISTOPATHOLOGY
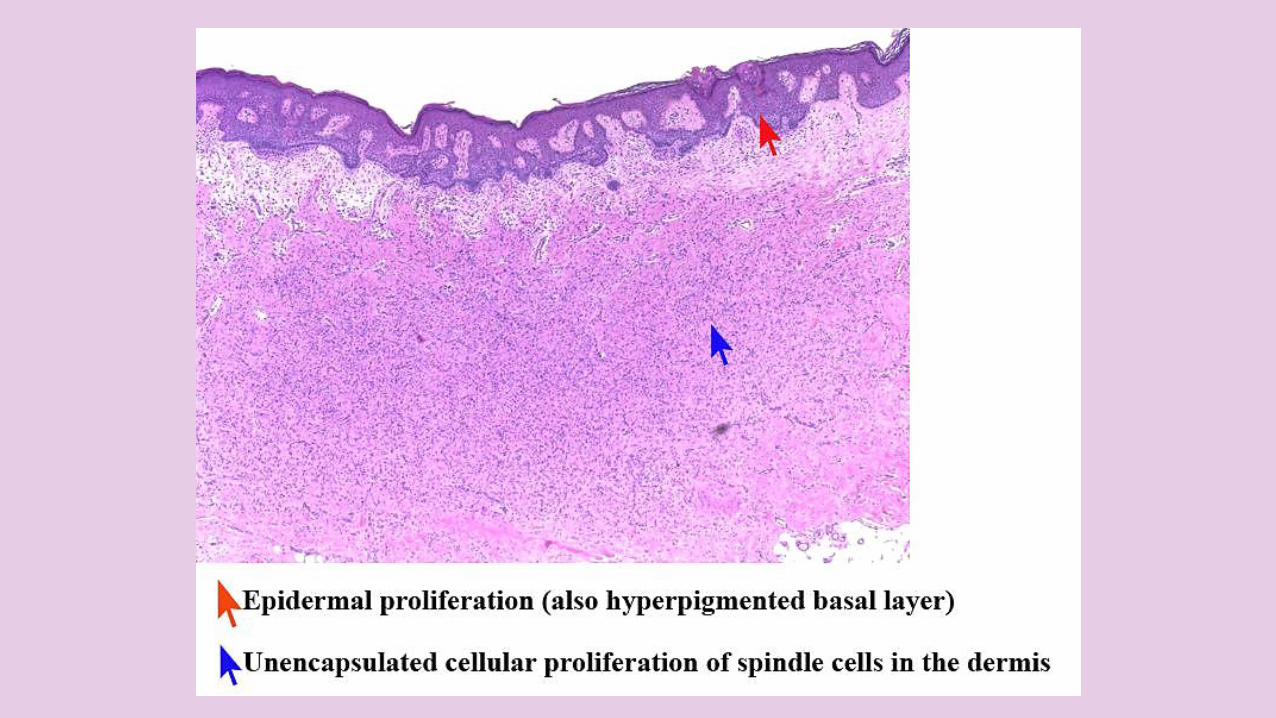
These benign dermal proliferations can induce overlying EPIDERMALPROLIFERATION.
The BASAL epidermal LAYER is classically HYPERPIGMENTED.
May cause BASALOIDINDUCTION.
DERMATOFIBROMA

HISTOPATHOLOGICAL VARIANTS
1. Fibrocollagenous (most common)2. Cellular3. Aneurismal4. Epithelioid5. Atypical6. Lipidized7. Palisading8. Cholesterotic
DERMATOFIBROMA

TREATMENT
A dermatofibroma is of COSMETICSIGNIFICANCE only and although it tends to persist long term, it seldom causes any symptoms.
Usually only REASSURANCE is needed. Sometimes its dark color can raise anxiety about melanoma; if there is any doubt about its nature, the lesion can be excised for histology.
DERMATOFIBROMA

TREATMENT
TREATMENT TECHNIQUES include;1. SURGICAL EXCISION may leaves scars
that are evident and sometimes more noticeable than the original lesion.
2. CRYOTHERAPY - rarely completely successful and may leave a hypopigmentation.
3. INTRALESIONAL STEROIDS.
DERMATOFIBROMA

a Small reddish cutaneous nodule on the right leg, consistent with DF. b Appearance of the scar 1.5 years after surgery.


DERMATOFIBROSARCOMAPROTUBERANS




A broad, pink-brown, multinodular, firm plaque on the back

42-year-old woman presented with a 3-cm, firm, violaceous, multinodular mass located on the left upper abdomen







DFSP on lower abdomen right side




OVERVIEW
RARE SLOWLY GROWINGINTERMEDIATE-GRADE LOCALLYAGGRESSIVE FIBROBLASTICMALIGNANT skin tumor arising from the DERMIS & RARELY METASTASIZES.
DFSP

ETIOLOGY
Most DFSPs (>90%) have ABNORMAL CHROMOSOMESwithin the tumor cells either TRANSLOCATION ORSUPERNUMERARY RINGCHROMOSOMES.
DFSP

ETIOLOGYDFSP
CHROMOSOMAL TRANSLOCATION EXPRESSION
NEW
FUSION
GENE
HIGH
LEVELS
OF
PDGF
PROLIFERA
-TION OF
FIBRO-
BLASTS
DFSP

ETIOLOGY
This chromosomal TRANSLOCATIONfuses the alpha chain type 1 of COLLAGEN of CHROMOSOME 17 and PLATELET-DERIVED GROWTH FACTORgenes at CHROMOSOME 22 PDGF β-CHAIN gene is now UNDER the CONTROLof the COLLAGEN 1A1 PROMOTEREXPRESSION of this FUSION GENE high levels of PDGF stimulates PROLIFERATION of FIBROBLASTS DFSP.
DFSP

ETIOLOGY
—t(17;22)(q22;q13) fusion the fused PROTO-ONCOGENE COL1A1-PDGFβ.
DFSP

CLINICAL FEATURES
Usually presents in EARLY or MIDDLE ADULT life between 20 and 59 years of age, but all ages can be affected.
MALES are affected slightly more frequently than females.
DFSP

CLINICAL FEATURES
Usually ASYMPTOMATIC this often leads to a DELAY in DIAGNOSIS.
Often “INFECTED KELOID” appearance.It usually grows VERY SLOWLY over MONTHS to YEARS.
May range in size from 1 TO 25 CM in diameter.
DFSP

CLINICAL FEATURES
PAINLESS FIRM indurated RED-BROWN or SKIN COLORED PLAQUEand/or nodules (CHARACTERISTICALLYMULTINODULAR) FIXED to the UNDERLYING TISSUE.
50-60% arise on the TRUNK often in the SHOULDER and CHEST area.
DFSP

CLINICAL FEATURES
DFSP is OFTEN DIAGNOSED LATER ON when it enters a MORERAPID GROWTH PHASE giving rise to larger lesions.
May METASTASIZE (<5%), possibly to LUNGS.
DFSP

DDx
1. KELOID
2. LARGE DERMATOFIBROMA
3. DERMATOMYOFIBROMA
4. MORPHEA
DFSP

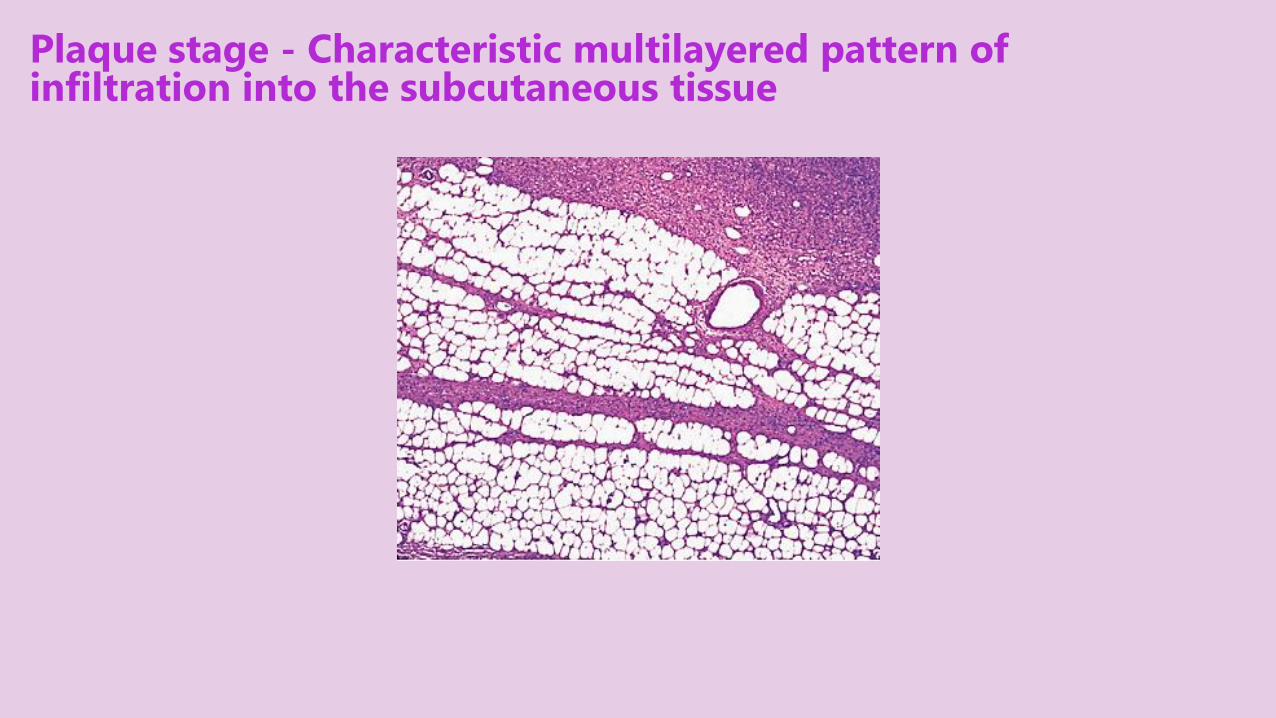
Plaque stage - Characteristic multilayered pattern of infiltration into the subcutaneous tissue

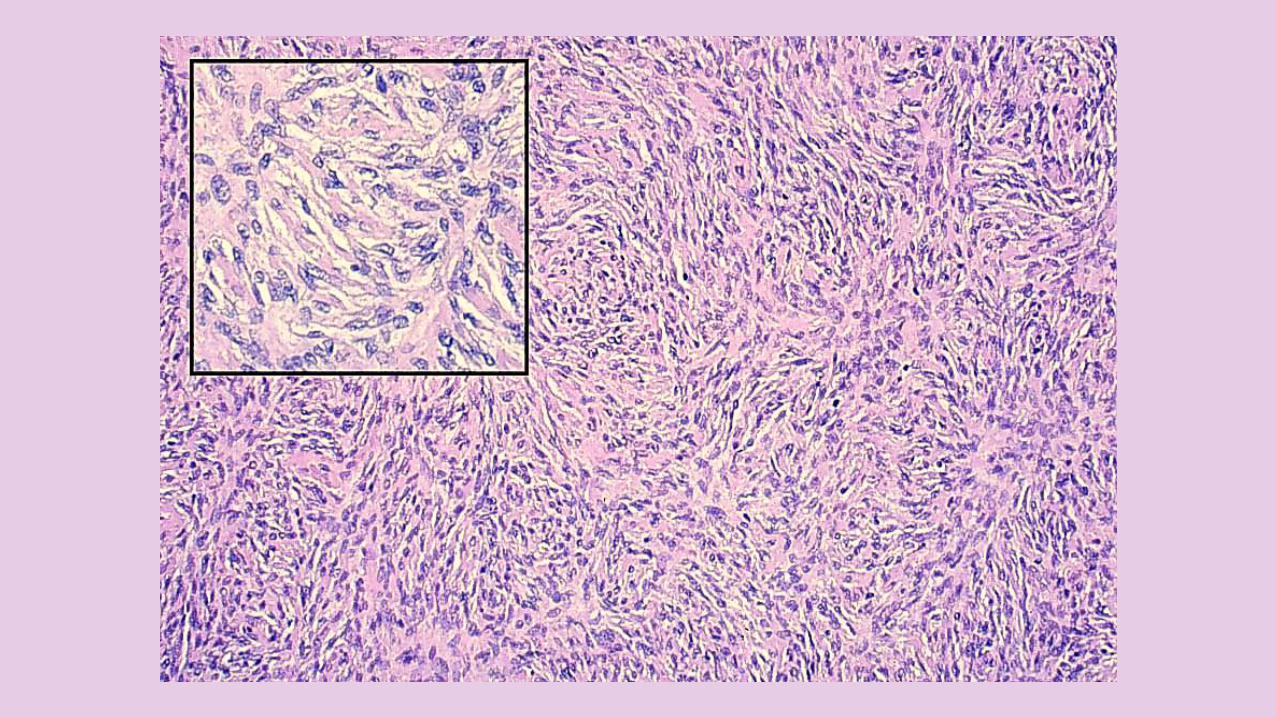
Storiform or cartwheel arrangement of tumor cells in a DFSP



Tumor cells enveloping the adnexal structures and invading the dermal collagen, subcutaneous tissues

Spindle cells infiltrate SC fat in honeycomb pattern
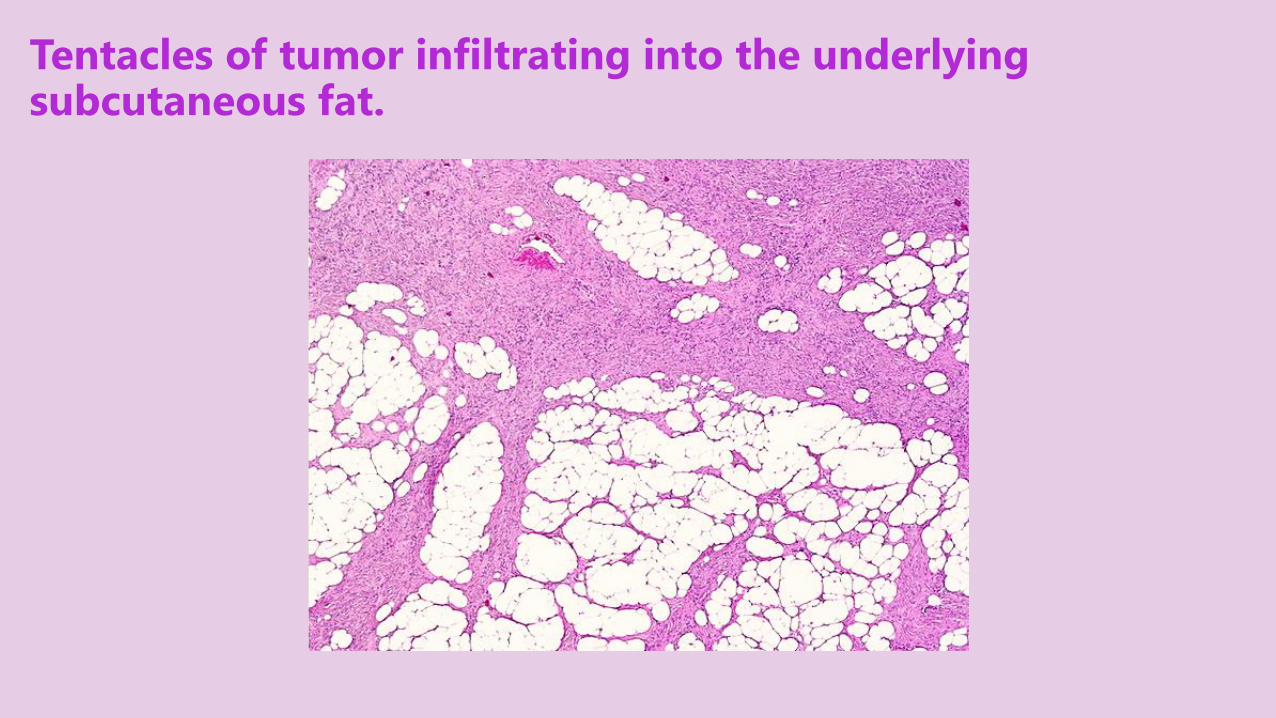
Tentacles of tumor infiltrating into the underlying subcutaneous fat.
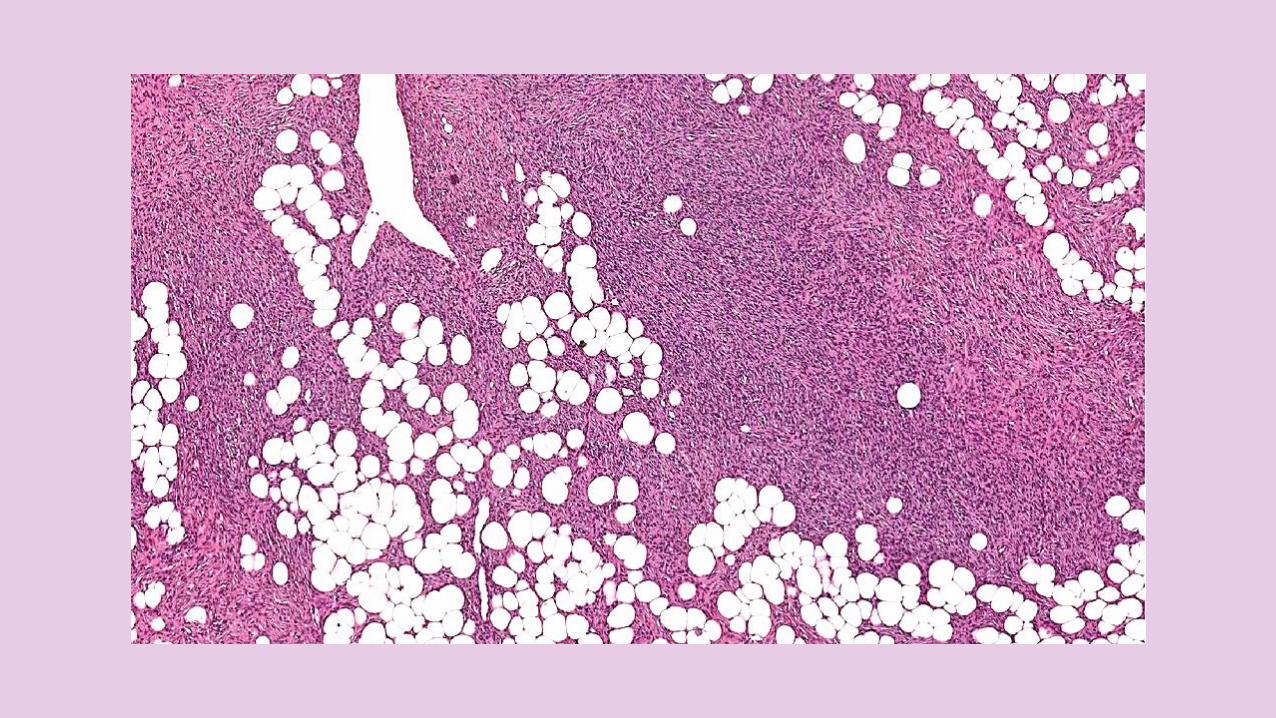


HISTOPATHOLOGY
NON CIRCUMSCRIBED, HIGHLYCELLULAR DERMAL proliferation of SPINDLE CELLS in distinct STORIFORM or CARTWHEELPATTERN.
DFSP
HISTOPATHOLOGY
Spindle cells are THINMONOMORPHIC with MINIMALATYPIA and spindly with SCANTEOSINOPHILIC CYTOPLASM and ELONGATED HYPERCHROMATICNUCLEI and LITTLE or NOPLEOMORPHISM & MITOTIC figures are RARE but EASILY IDENTIFIEDLATER in NODULAR stage.
DFSP

HISTOPATHOLOGY
ADNEXAL STRUCTURES are INFILTRATED and obliterated. The spindle cells infiltrate into the SUBCUTANEOUS TISSUE, very often in a MULTILAYERED PATTERN EARLYin PLAQUE STAGE & entraps fat cells to form characteristic HONEYCOMB pattern LATER in NODULAR STAGE.
DFSP

HISTOPATHOLOGY
INVASION of MUSCLE may occur.
Usually NO/RARE HISTIOCYTES, no HISTIOCYTE-LIKE cells, no FOAM CELLS, no GIANT CELLS or other INFLAMMATORY CELLS.
DFSP

HISTOPATHOLOGY
May show areas of FIBROSARCOMATOUSTRANSFORMATION
It is important to identify this fibrosarcomatous DFSP, which is MORE AGGRESSIVE tumor, that requires MORE AGGRESSIVETREATMENT.
DFSP

CD34 immunostaining in DFSP

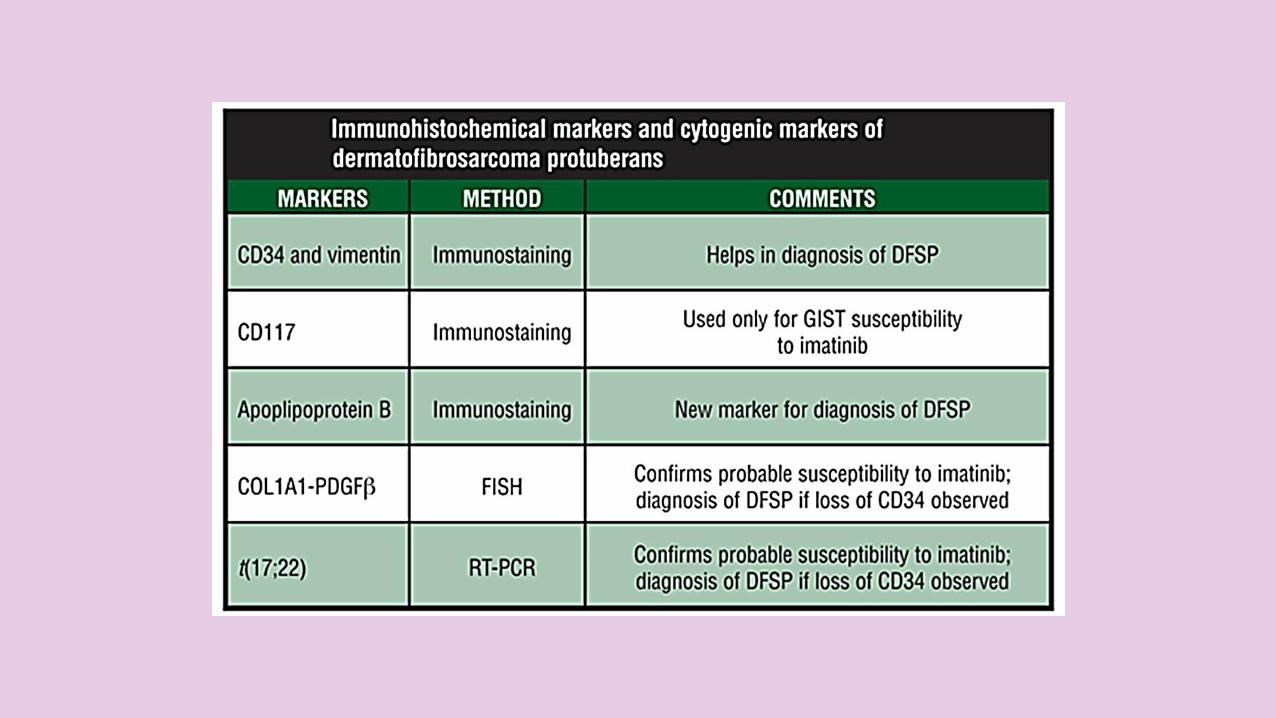
IMMUNOHISTOCHEMISTRY
STRONGLY POSITIVE STAINING FOR CD34.
DFSP

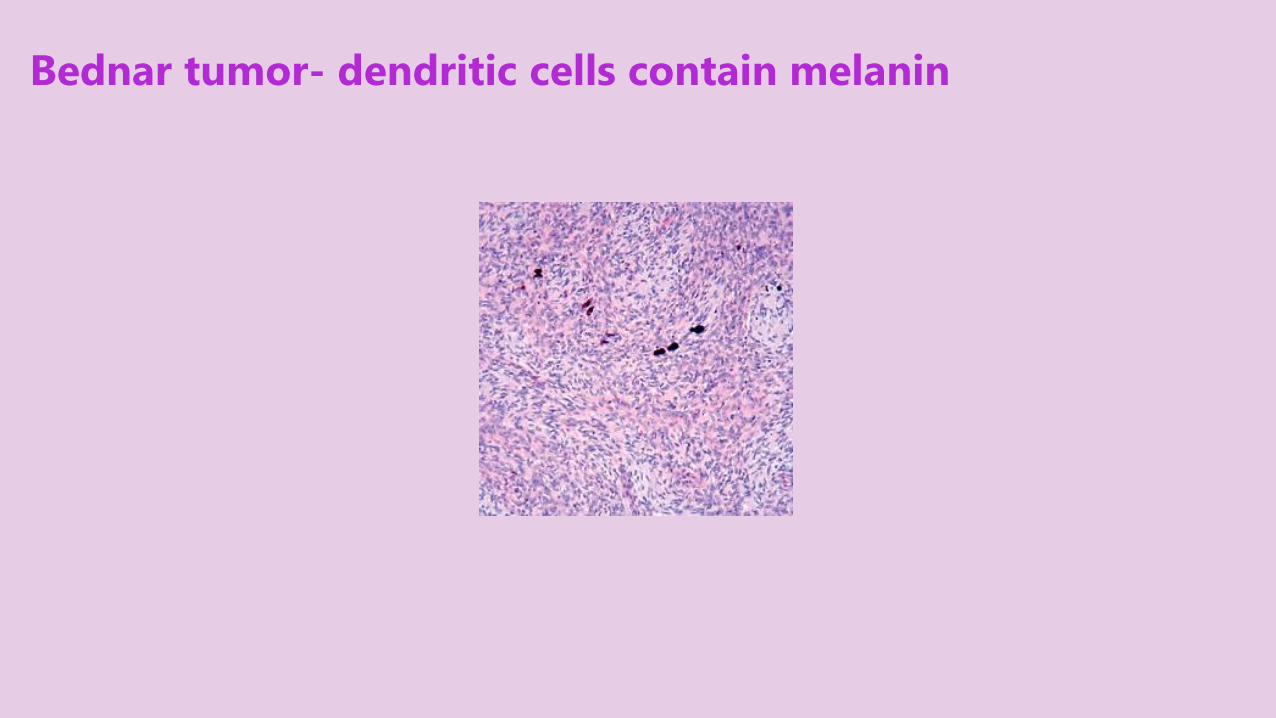
Bednar tumor- dendritic cells contain melanin

INVESTIGATIONS
LAB
FISH
RT-PCR
RADIOGRAPHY
CT
MRI
DFSP
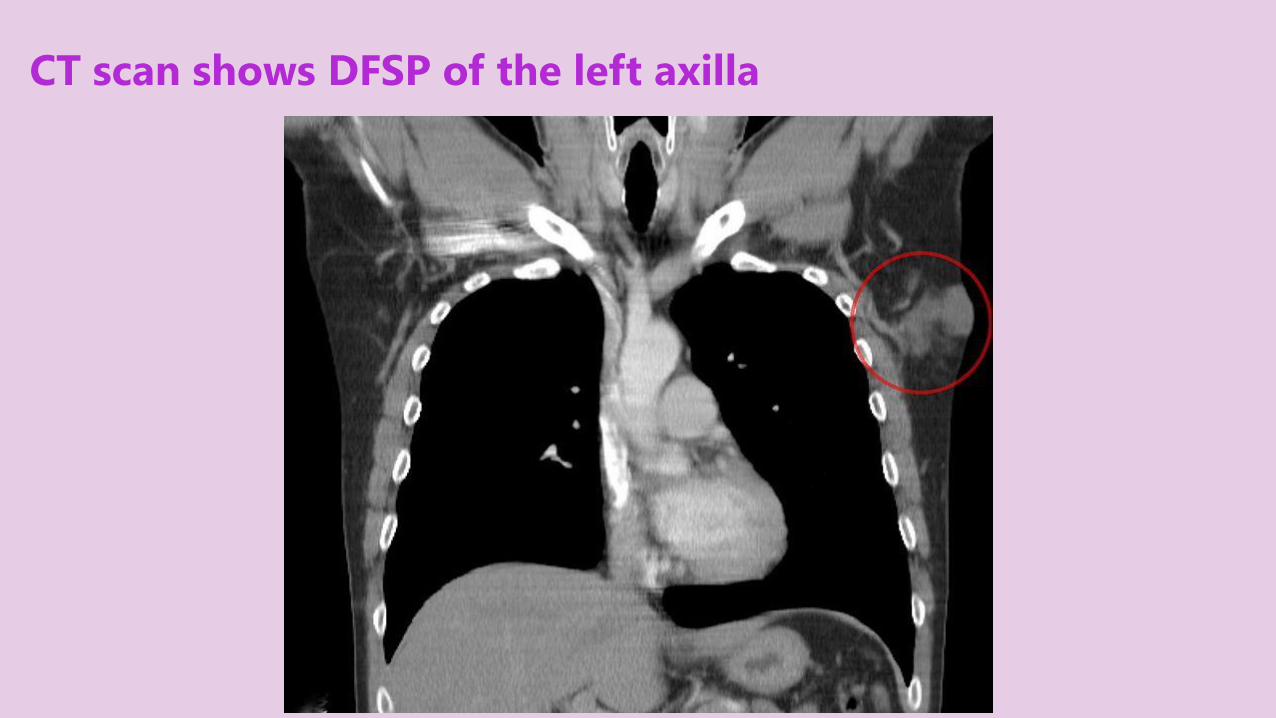
CT scan shows DFSP of the left axilla

TREATMENT
COMPLETE SURGICAL EXCISION, including Mohs micrographic surgery is considered the STANDARD TREATMENT.
Chemotherapy is ineffective.
DFSP

TREATMENT
1. WIDE LOCAL EXCISION 2-3 cm margins Local recurrence so follow-up is important.
2. MOHS MICROGRAPHIC SURGERYrecurrence ~1%
3. POST-OPERATIVE RADIOTHERAPY may be used as an adjunct to surgery. when resection is incomplete.
4. IMATINIB MESYLATE an oral PDGF receptor tyrosine kinase inhibitor. FDA-approved for unresectable, recurrent or metastatic cases in adults.
DFSP

(A) Baseline view of advanced, primary dermatofibrosarcomaprotuberans of the chest wall, (B) the partial response after 12 weeks of imatinib therapy, and (C) 2 years after resection of the tumor.

DIFFERENCES BETWEEN DF & DFSP
DF DFSP
NATURE OF THE TUMOR benign Intermediate-grade malignancy
ETIOLOGY ? Minor trauma, insect bite mutations
PREVALENCE common rare
CLINICALLY
SEX female Males (slightly more)
DIMPLE SIGN + -
SITE OF
PREDILECTIONLower extremities or arms Trunk especially shoulder or chest
SIZE generally < 1 cm 1-25 cm
MORPHOLOGYSingle Static well-defined
hyperpigmented firm nodule
Expanding keloidal plaque
characteristically multilobulated
red-blue to brown color

DIFFERENCES BETWEEN DF & DFSP
DF DFSP
HISTO-
PATHOLOGY
TUMOR CELLS Fibrohistiocytic proliferationSpindle cells in storiform
pattern
COLLAGEN
BUNDLESKeloidal & may be entrapped thin
SC INVOLVEMENT in a radial pattern Multilayered Honeycomb
ATYPICALITY No minimal
HISTIOCYTES lipid laden histiocytes no/rare
GIANT CELLS present no
IMMUNO-
STAINING
S100 – or + –
CD34 – +
FXIIIA ++ –
STROMELYSIN-3 + –
RxREASSURANCE /Surgical/
cryotherapy/intralesional steroids
WLE/ Mohs MS/ adjuvant
radioRx/ Imatinib mesylate

FIBROMATOSES

FIBROMATOSIS
Fibromatosis is a condition where FIBROUS OVERGROWTHSof DERMAL and SUBCUTANEOUSCONNECTIVE TISSUE develop tumors called FIBROMAS. These fibromas are usually BENIGN.
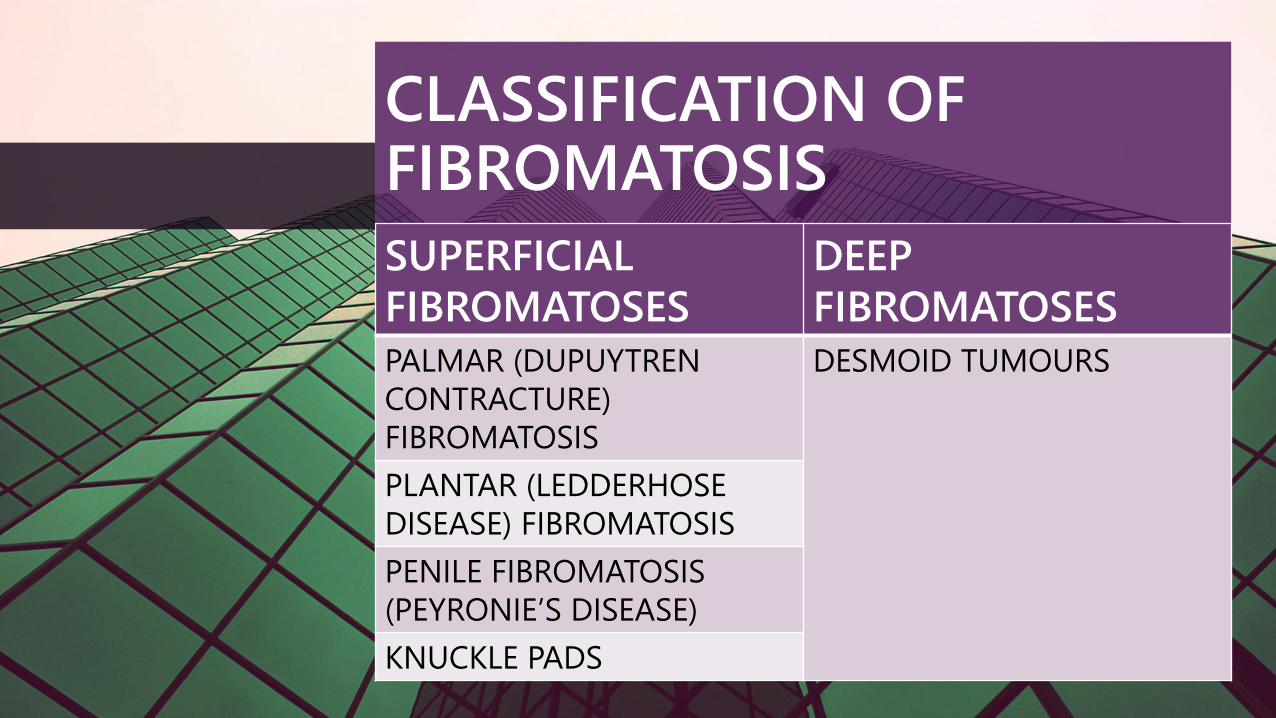
CLASSIFICATION OF FIBROMATOSIS
SUPERFICIAL
FIBROMATOSES
DEEP
FIBROMATOSES
PALMAR (DUPUYTREN
CONTRACTURE)
FIBROMATOSIS
DESMOID TUMOURS
PLANTAR (LEDDERHOSE
DISEASE) FIBROMATOSIS
PENILE FIBROMATOSIS
(PEYRONIE’S DISEASE)
KNUCKLE PADS

OVERVIEW
Knuckle pads are WELL DEFINEDTHICKENINGS over the dorsum of FINGER OR TOE JOINTS more likely develop from REPETITIVEPRESSURE or FRICTION related to SPORTS or OCCUPATION.
KNUCKLE PADS








ETIOLOGY
1. IDIOPATHIC2. GENETIC as part of an inherited
syndrome e.g. epidermolyticpalmoplantar keratoderma, may run in families together with other forms of fibromatosis.
3. ACQUIRED as a response to repetitive trauma, or associated with several other acquired conditions.
KNUCKLE PADS

CLINICAL FEATURES
Most commonly become apparent after the age of 30YEARS.
Usually ASYMPTOMATIC WELL-DEFINED, SMOOTH, FIRM SKIN-COLORED dome-shaped PAPULES, NODULES, or PLAQUES.
KNUCKLE PADS

CLINICAL FEATURES
More commonly located over DORSAL ASPECTS of the PROXIMALINTERPHALANGEAL JOINTS than over the KNUCKLES(METACARPOPHALANGEALjoint/”misnomer”) or DISTALINTERPHALANGEAL joints.Over SINGLE or MULTIPLE joints.In most cases, PERSIST INDEFINITELYwith little change.
KNUCKLE PADS

HISTOPATHOLOGY
HYPERKERATOSIS and mild ACANTHOSIS of the epidermis.
THICKENING of the DERMIS and thickened, IRREGULAR COLLAGENBUNDLES.
Slight PROLIFERATION of FIBROBLASTS and capillaries in the papillary dermis.
KNUCKLE PADS

HISTOPATHOLOGY
When associated with a KERATIN 9 GENE MUTATION, as in EPIDERMOLYTICPALMOPLANTAR KERATODERMA, SUPRABASAL EPIDERMOLYSIS is also seen.
KNUCKLE PADS

TREATMENT
In general TREATMENT is NOTREQUIRED.
AVOIDANCE of a REPETITIVEBEHAVIOR if possible may improve the situation e.g. CHANGING OCCUPATION or WEARING PROTECTIVE GLOVES.
KNUCKLE PADS
TREATMENT
1. MOISTURIZERS & KERATOLYTICSmay be useful if the knuckle pads are hyperkeratotic.
2. INTRALESIONAL INJECTIONS of CORTICOSTEROIDS or FLUOROURACIL.
3. SURGERY has been used, but may be complicated by the development of keloid scars, tendon tethering or Recurrence.
KNUCKLE PADS

REFERENCES
BOLONGIA DERMATOLOGY ESSENTIALS
BOLONGIA 3rd ed
WEEDON’S SKIN PATHOLOGY ESSENTIALS
GOOGLE IMAGES
DERMNETNZ.ORG
EMEDICINE.MEDSCAPE.COM
DERMIS.NET

THANK YOU


















