Fibroids by mavish
54
Prepared by: Mahwish Gul Roll # 08-089 Final yr MBBS FIBROIDS
-
Upload
ayub-medical-college -
Category
Health & Medicine
-
view
83 -
download
2
Transcript of Fibroids by mavish

Prepared by:
Mahwish GulRoll # 08-089
Final yr MBBS
FIBROIDS

What is fibroid?Its epidemiology?its gross & microscopic features? Its types?What causes fibroid?What are its signs and symptoms?Its treatment options?Its complications?Its differential diagnosis?Effect of fibroids on pregnancy & pregnancy on
fibroids?
Basic considerations during the presentation:

• Actually fibroid is a misnomer because there is very little connective tissue in it.
• Its other name is LEIOMYOMA or MYOMA. • It is chiefly composed of the smooth muscle fibers
& contains fibrous tissue in small amount.• Tumor arises from the muscle tissue and NOT
from the fibrous tissue of the uterus.• It is a BENIGN in nature.• Predominantly occurs in the body of the uterus
and less commonly in the cervix.
What is fibroid?

Most common tumor not only of the uterus but of the whole female body!
Present in 20-30% of the women of reproductive age.
Disease of the reproductive age, never occurs before menarche & regresses after menopause.
Commonly occurs in infertile & women with low parity.
Incidence is more common in black women where it presents at a younger age as well.
Family history +
epidemiology


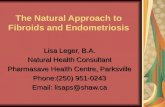
Nodular outgrowth which causes enlargement of the uterus and distortion of its normal structure.
Could be single but are usually multiple.Size varies from a few millimeters to the size
of the football.Oval or rounded in shape.Firm in consistency.Characteristic whorled appearance on cut
surface which becomes convex.Its colour is generally lighter than surrounding
myometrium.Could be surrounded by the pseudo-capsule.
GROSSLY we see:
Multiple leiomyomas in the same uterus

Whorled appearance on cut surface

Colour lighter than the surrounding myometrium
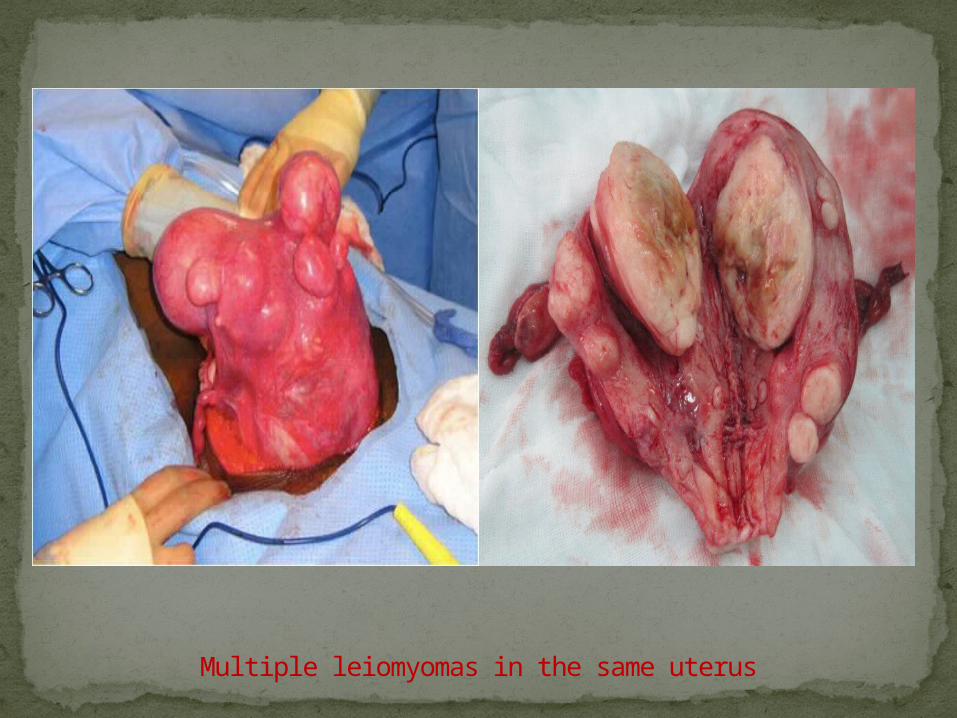
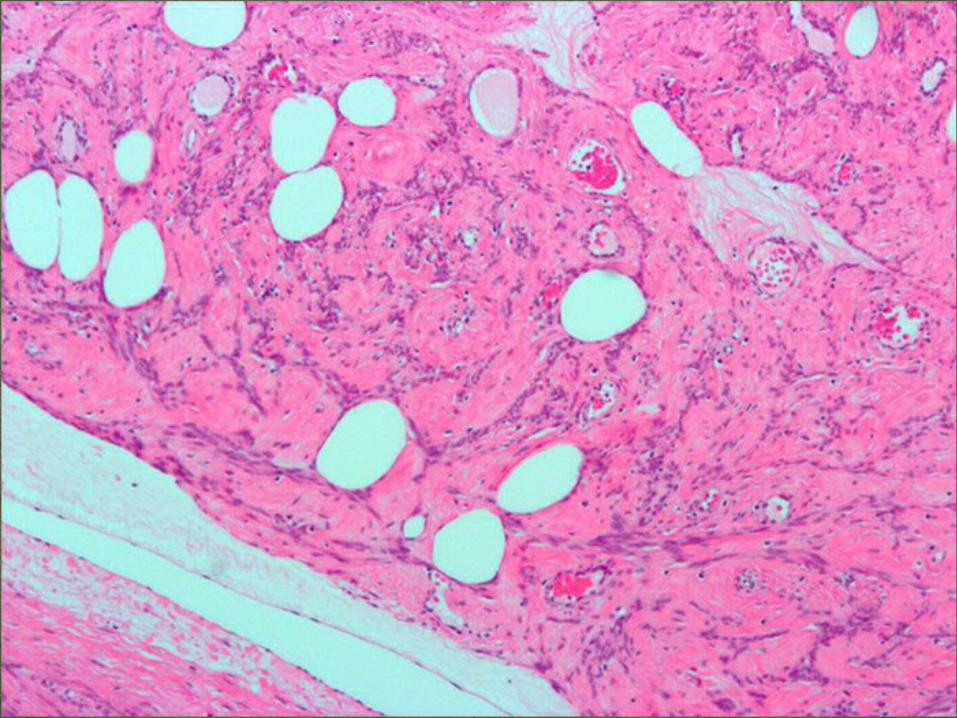
Bundles on muscle cells seen running in all directions.
Nuclei of these cells are rod shaped and uniform in shape and size.
Variable amount of connective tissue present in between.
Microscopically:

Female hormonesMechanical stressRacial factorsGenetic factorsParity
Aetiology

Receptors Does not occur before menarche & regresses
after menopause In size when treated with GnRH
analogues In size in response to oral contraceptives Incidence in obese women Incidence in smokers
What is the role of estrogens & progesterone?

•subserous
•Intramural
•submucous
body
cervical
intraligamentary
CLASSIFICATION


Originates from the outer
myometrium & projects
outwards from the
uterine surface covered
with the peritoneum.
May attain a large size
because of unrestricted
growth.
May become
pedunculated.
Subserous type

Lies within the uterine
wall & is surrounded by
the normal myometrium
on all sides.
May be surrounded by
pseudo-capsule.
Large intramural fibroid
may distort the uterine
cavity & increase its
surface area.
Intramural type

Arises from the inner
myometrium & is
covered by the
endometrium.
Projects inwards into
the uterine cavity &
may become
pedunculated.
Submucous type

Less common.
1-2% of the cases.
Often single.
Usually confined to
supravaginal portion of
cervix.
Either intramural or
subserous.
Cervical type
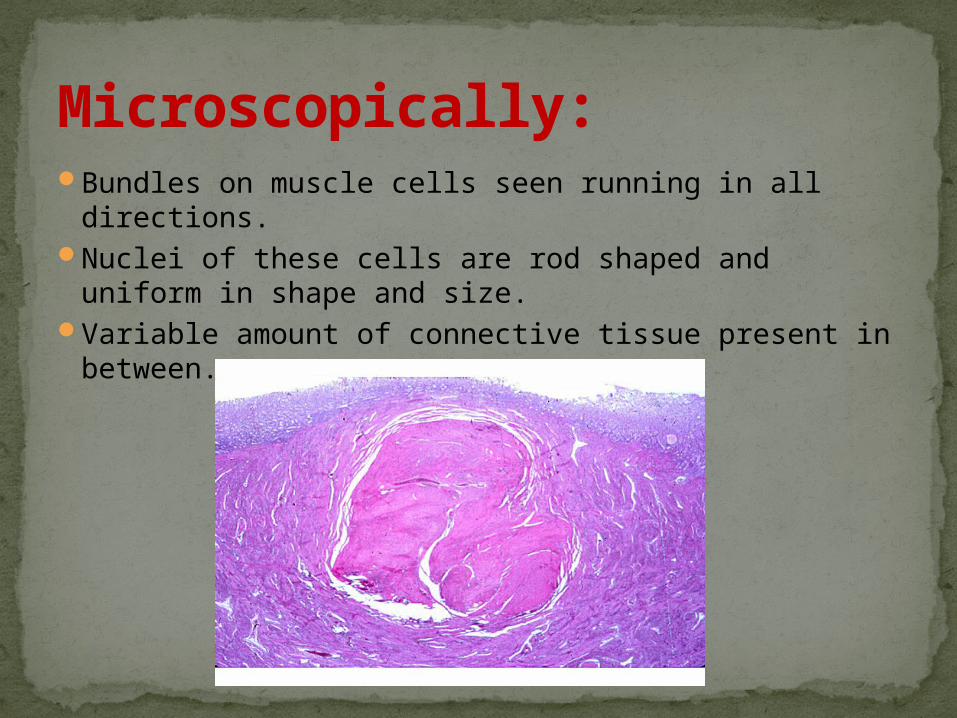
Rare
Arises from smooth muscle
fibres within the broad
ligament.
Should be differentiated
from the subserous fibroid.
Intraligamentary type

Usually silent (in more than 50% of the cases)Menstrual problems e.g I. Menorrhagia > surface area >
endometrium becomes ulcerated covering the submucous type > vasularity
II. Intermenstrual bleedingIII. Postcoital bleedingIV. Irregular bleeding
SYMPTOMS

Abdominopelvic mass (in the absence of pregnancy)Subfertility
occurs in 30% of the patients with fibroid (unclear whether fibroid is a cause of subfertility or an effect) possible explanations: > delay in child bearing & interfere with implantation of the fertilized ovum.
Heaviness in the lower abdomenPainUrinary retentionUrinary frequencyDyspepsiaDyspneaIntestinal obstructionConstipationHaemorrhoidsEdema of the legsVaricosities of the legs

General physical examinationNo specific findingsExcessive loss of blood may cause anemia ,presenting
with pallor and in extreme cases with breathlessness Edema and varicosities of limbs are rare findings with
large fibroids .Abdominal examination :Uterus palpable abdominally
Single fibroid -- uterus with smooth surfaceMultiple fibroids – irregular mass maybe shifted to a sideFibroids – firm ,non tender unless undergone
degeneration.Pelvic examination :
Protruding fibroids easily seen
Signs

• ultrasound
investigations

Hysteroscopy & curettage

• laproscopy
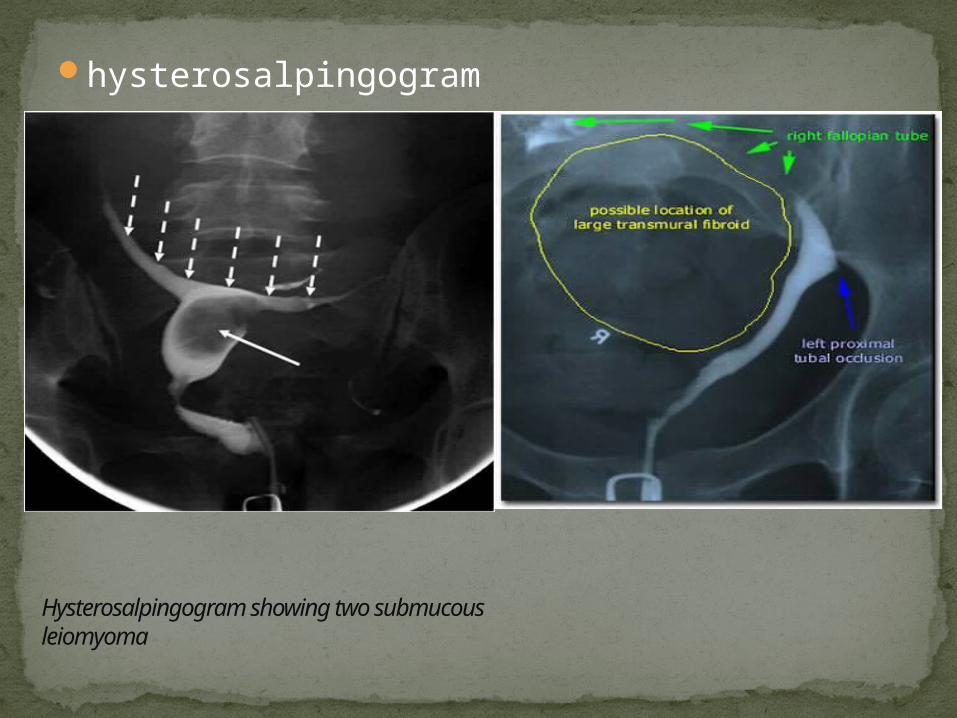
hysterosalpingogram
Hysterosalpingogram showing two submucous leiomyoma

CT scan

MRIComplete blood picture >Hb >associated polycythemia

conservative treatment
Medical treatment
Surgical treatment
depends on symptoms, size & site of tumor, age of patient & her reproductive status + patients choice
Treatment

kept under observation, repeated follow ups done
>approaching menopause + no
symptoms + small tumor + no complications
(should be examined every 4-6 months interval till menopause)
1. Expectant treatment

Correct anemiaGnRH analogues (prescribed for 3-6months duration)
*IM injection> monthly *SC injection> 12 hourly *nasal spray> 6hourly
-- reduce size & vasularity > by causing pseudo-monopause > by supression of ovaries
(menorrhagia is improved upto 80% & size reduced by 50%)
-- temporary treatment -- only used now a days to prepare the patient for surgery >
causes less bleeding DISADVANTAGES:1. Expensive2. Effects last for the duration of treatment3. Causes postmenopausal symptoms (hot flushes, night sweats,
psychological disturbances) 4. If used for >6months– osteoporosisOther drugs:Danazol, antiprogestogens
2. Medical treatment

Occlude uterine artery by
particulate emboli (polyvinyl
alcohol)
Approached by trans femoral route
Causes ischemic necrosis of
fibroids & reduce their size
COMPLICATIONS:
>failure to canalize
>hematoma formation
>infection
>pain
3.Surgical treatment >uterine artery embolism (UAE)

(removal of the myomas & conservation of the uterus)
Preferred treatment for the following circumstances:
*age <40*symptomatic fibroid*patient wishing to have more children*patient with recurrent abortions*Infertile patients*patient wishing to conserve her uterus
> myomectomy

Contraindications:>associated carcinoma *treatment should be directed against
malignancy>Suspicion of sarcomatous change>pregnancy * myomectomy should be postponed till
3months after delivery > cuz of increased congestion of uterus
* pedunculated subserous must be removed however to prevent torsion in puerperium
Cont…..

Preparation: >Hb corrected >rule out endometrial carcinoma or any other
abnormality by D & C before myomectomy >X-ray abdomen >IVU
Routes:>abdominal>vaginal>endoscopic
Cont…

COMPLICATIONS:>sepsis>recurrence (5-10%)>persistant symptoms>oozing from uterine wound>intra peritoneal adhesions>haemorrhage *heavy intraoperative bleeding (atleast 2units blood
should be available prehand)Minimized by applying bonney’s myomectomy clamp or
simple rubber tourniquet
Bonney’s myomectomy clamp
Cont…

(removal of the uterus)Treatment of choice under following conditions:*age>40*multiple fibroids*completed her family*severe symptoms
Carried out by:>abdominal route >vaginal route
>hysterectomy

complications
degeneration
torsion
Sarcomatouschange
infection

(cuz of reduced blood supply to the tumor) types:>atrophic>hyaline>cystic>calcific>septic>red>myxomatous(fatty)
DEGENERATION

ATROPHIC: >size of tumor decreases after menopause or after
pregnancy>due to withdrawl of estrogens>size decreases but the myoma does not disappear
HYALINE:>commonest of all(except for tiniest tumors)>homogenous & glassy areas on microscopy>fibrous tissue gets involved first &then the Ms fibres
CYSTIC:>hyaline degeneration(if extensive) may progress into cystic
degeneration>liquifaction of hyalinized areascystic cavities>walls of cavity irregular>cavity filled withgelatinous material>whole tumorone large cystic cavitysimulate pregnancy or
ovarian cyst

CALCIFIC:>carbonate &phosphate salts deposited in the
tumor>seen as radioopaque shadows>more commonly in subserous myomas

SEPTIC:>necrosis in the center of large myoma
MYXOMATOUS:>rare>Fatty change occurs in the fibroid >Require differentiation from uterine lipoma
RED:>most commonly seen durong pregnancy & puerperium but may occur
without pregnancy as well>due to thrombosis of the veins ischemia & necrosis>soft, on section looks red or pink with areas of necrosis in the center
>microscopically structureless>onset of symptoms sudden*pain *increased size(mistaken for torsion of myoma or ovarian cyst,concealed accidental
haemorrhage etc)>TREATMENT: analgesics, bed rest & observation(usually settle down within a week or so)


>very rare (0.2% of cases)>usually starts in the center of the tumor
*if myoma enlarges rapidly or becomes painful &tender malignant change should be suspected
INFECTION>more common during puerperium &after abortion>more common in myomas that have undergone necrosis
TORSION>pedunculated subserous>more commonly seen during pregnancy &puerperium>sudden pain, enlarges in size & becomes tender
*difficult to differentiate from red degeneration & torsion of ovarian cyst
SARCOMATOUS CHANGE

Usually easily diagnosedExclude pregnancyExclude other pelvic masses -Ovarian Ca -Tubo-ovarian abscess -Endometriosis -Adenexa, omentum or bowel adherent to the uterus Exclude other causes of uterine enlargement: -Adenomyosis -Myometrial hypertrophy -Congenital anomalies -Endometrial Ca
DIFFERENTIAL DIAGNOSIS
Exclude other causes of abnormal bleeding Endometrial hyperplasia Endometrial or tubal Ca Uterine sarcoma Ovarian CaPolypsAdenomyosisEndometriosisExogenous estrogens*Endometrial biopsy or D&C is essential in the
evaluation of abnormal bleeding

1. adenomyosis
• Disease of multiparous women
• Menorrhagia is associated with severe dysmenorrhea
• Uterus : uniformly enlarged ,tender
• Ultrasound : thickened myometrium with swiss cheese appearance
• Cut surface : lacks whorled appearance and capsule.
2.Ovarian tumor
• Confused with pedunculaed sub serous tumor
• Menorrhagia often absent
• Mass feels separate from the uterus while fibroids has limited mobilty
• Ultrasound may be helpful but diagnosis is not confirmed until laproscopy or laprotomy is performed

3. Pregnancy with or without myomas >amenorrhea +>uterus soft nd cystic>clinical signs of pregnancy>pregnancy test +>U/S
4. PID & endometriosis>tenderness on bimanual examination>adhesions on pelvic examination
5. Myohyperplasia>in response to excessive or prolonged unopposed
estrogen influence e.g metropathia haemorrhagica

EFFECTS OF MYOMAS>On pregnancy 1.abortion*distortion of uterine cavity*interference in accommodation & increase in
size*defective placentation*impacted myomas in pelvis
2.premature onset of labour
3.malpresentations*interfere with descent of the presenting part

During labour 1. Abnormal uterine contractions
prolonged labour 2. Cervical dystocia*interfere with dilatation of the cervix 3. Obstructed labour*usually with cervical & broad ligament
myomas 4. Retained placenta*interfere with its separation 5. PPH*cuz of retained placenta & abnormal uterine
contractions

During puerperium 1. Sepsis*submucous myomas may get infected 2. Delayed involution of uterus

Effects of pregnancy on myomas
1. increase in size• Due to congestion & odema of tumor• After pregnancy return to their original size2. Change in consistency• Become soft• Due to congestion & odema of tumor3. Red degeneration• More common during pregnancy & puerperium• Due to increased tendency for thrombosis4. Torsion & infection• These complications are more common during
pregnancy & puerperium