Fiber Reinforced Composites in Pediatric Dentistry
92
Fiber Reinforced Composites in Pediatric Dentistry Frc in Pediatric Dentistry Dr. Sunita Agarwalla, et al. Medical and Research Publications
Transcript of Fiber Reinforced Composites in Pediatric Dentistry
Fiber Reinforced Composites in
Pediatric Dentistry Frc in Pediatric Dentistry
Dr. Sunita Agarwalla, et al.
Medical and Research Publications
Fiber Reinforced Composites in Pediatric Dentistry
Contributing Authors
Dr. Gautam Kumar Kundu Prof & Ex -HOD.
Dr. Shabnam Zahir Prof & HOD.
Dr. Biswaroop Chandra Ass. Prof
Dr. Pratik Kumar Lahiri Ass. Prof.
Dr. Sudipta Kar Ass. Prof.
Dr. Rajib Saha Senior Lecturer.
Dr. Piyali Datta Senior Lecturer.

Fiber Reinforced Composites in Pediatric Dentistry
Medical and Research Publications
Copyright © 2021 Dr. Sunita Agarwalla, et. al.
All rights reserved. No part of this publication may be reproduced, distributed, or transmitted in
any form or by any means, including photocopying, recording, or other electronic or mechanical
methods, without the express written permission of the publisher except for the use of brief
quotations in a book review..
First printing, 2021.
Published by
Medical and Research Publications,
124SpencerRd,Stoke-on-TrentST42BE,
United Kingdom.
www.medicalandresearch.com
Email: [email protected]
ACKNOWLEDGEMENT
First and foremost, praises and thanks to the God, the Almighty, for His showers of
blessings throughout my work to complete the work successfully.
It is a humbling experience to acknowledge those people who have, directly or indirectly
contributed towards my work. I am indebted to so many for encouragement and support.
My sincerest thanks are extended to my mentor, Dr. Biswaroop Chandra (MDS) Reader, Dept of
Pediatric & Preventive Dentistry, GNIDSR for his encouragement and guidance. I shall forever
be grateful for the constant encouragement and fruitful criticism which he has bestowed upon me
in carrying out this work. His brilliant foresight and practical approach has been a guiding force
behind all my efforts in bringing this book to its ultimate goal.
I wish to convey my profound gratitude to Prof. (Dr.) Gautam Kumar Kundu Professor, Ex-Head
of the Department, Dept of Pediatric & Preventive Dentistry, GNIDSR and Prof. (Dr.) Shabnam
Zaheer (M.D.S), Professor, Head of the Department, Dept of Pediatric & Preventive Dentistry,
GNIDSR for their constant support and encouragement.
I owe a deep sense of gratitude to all my teachers Dr. Pratik Kumar Lahiri MDS, Dr. Sudipta
Kar MDS, Dr. Rajib Saha MDS, Dr. Piyali Datta MDS for their valuable guidance and
constructive criticism.
I am extremely grateful to my parents for their love, prayers, care and sacrifices for educating
and preparing me for my future. I am very much thankful to my husband and my daughter for
their love, understanding, prayers and continuing support to complete this work. Also I
express my thanks to my sisters, brother, and brother in law for their support and valuable
prayers.
Foreword
Let me start this writeup with a famous quote of C.S.Lewis
"You are never to old to set another goal or to dream a New Dream"
Its my privilege to say few words on this book.
Use of composite in restorative dentistry is constantly evolving. Reinforcement of Composite with
fibre has come up with variety of additional clinical applications.In this book Sunita has left
no stone unturned to update readers on different clinical possibilities which will help not only the
academicians but also the clinicians.
I wish all success of this endeavor though I believe in the famous quote of Winston Churchill
Success is not final,failure is not fatal: it is the" courage to continue " that counts.
Maintain this "Courage to continue".
Prof.(Dr)Gautam Kumar Kundu
Ex HOD,Dept.of Pediatric and Preventive Dentistry.
GNIDSR,KOLKATA
Dedicated to…
Gopal and Khanak who always inspire me and make me
so proud…
Without whom this work would not have been possible.
CONTENTS
S.No Chapter Pg.No
1. Introduction 1
2. History 6
3. Applications for Fiber Reinforced Composites Outside Dentistry
11
4. Definition and Classification of Fiber Reinforced Composites
12
5. Mechanical Properties of FRCs 16
6. Properties of Fibre Reinforced Composite 23
7. Biocompatibility 25
8. The Clinical Applications of Fiber Reinforced Composites in All Specialties of Dentistry
29
9. Clinical Applications in Conservative Dentistry 31
10. Fiber-Reinforced Composite as A Post and Core Material In A Pediatric Dentistry)
43
11. Clinical Procedure 62
12. Surgical Applications for Fiber Reinforced Composites
80
13. Bibliography 84

Fiber Reinforced Composites in Pediatric Dentistry
1
INTRODUCTION
The dental restorative materials are considered as a unique class of biomaterials with some
restrictions in physical, mechanical and biological properties like biocompatibility, aesthetics, and
material properties. Examples include Amalgam, composite resin, glass ionomer cement, resin
modified glass ionomer cement (RMGIC), compomers which fall under the direct restorative
materials. The indirect restorative materials include porcelain (ceramic), composite resin, ceramic-
resin hybrids, gold, other historical fillings such as platinum, aluminium, tin and iron, thorium,
lead and tungsten etc. In recent years the dental restorative materials are the main target of an
excellent deal of research with the goal of improving restoration performances by changing the
initiation systems (composite), fillers (GIC) and by developing novel polymerization strategies
(composites) etc.1
Despite better understanding of the materials and recent improvements in physical
properties, no material has been found that is ideal for any dental application. Silver amalgam has
been used for dental restoration for more than a century; however, there has been a serious concern
about mercury toxicity from the amalgam restorations for several years. Another major concern is
the color of amalgam for aesthetic considerations and alternative materials are being sought to
replace. The composite restorative materials have promising esthetics however these materials are
very technique sensitive and mechanical properties are not as good as of amalgam. Restorative
dentistry is constantly evolving as a result of innovative treatment procedures based on new
materials, treatment techniques and technologies, with composite materials being a key example.1
As popular and successful as these materials are, they exhibit shortcomings that frequently
cause clinical problems:2
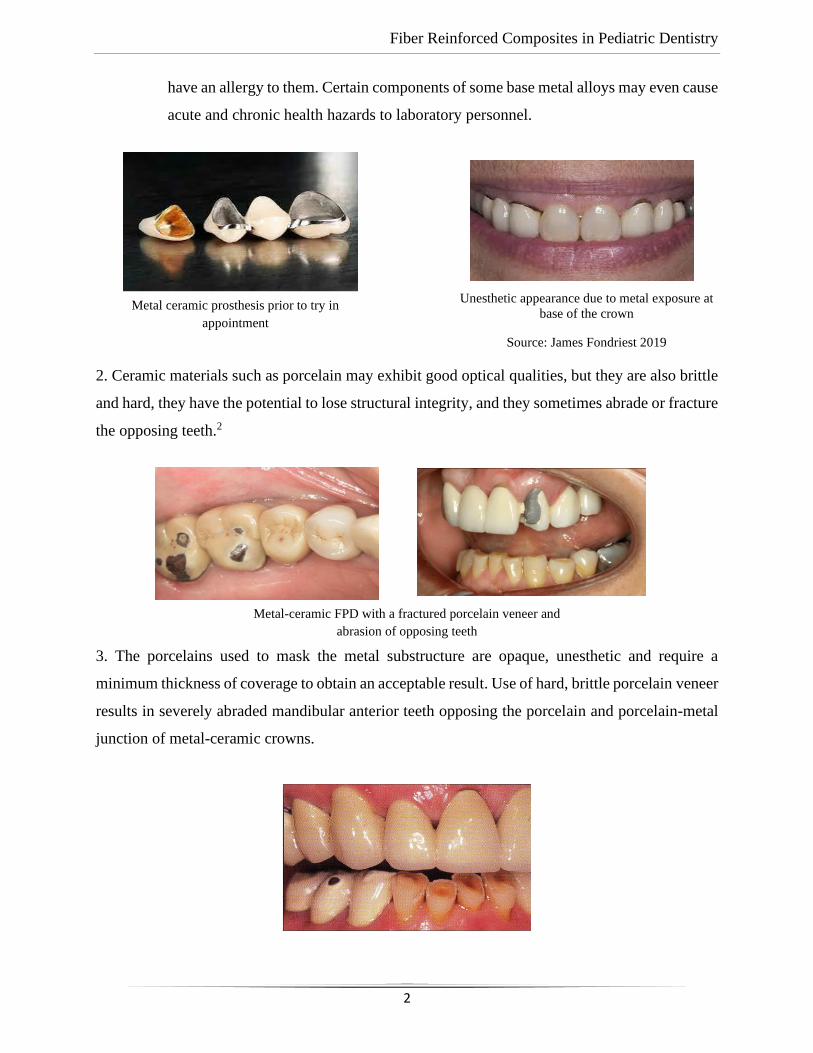
1. The metal alloys used to make substructures that reinforce crowns and fixed prostheses
are strong and rigid, but they are not esthetic as given in figure below. Furthermore, the
base metal alloys commonly utilized in clinical practice may corrode and a few patients
Fiber Reinforced Composites in Pediatric Dentistry
2
have an allergy to them. Certain components of some base metal alloys may even cause
acute and chronic health hazards to laboratory personnel.
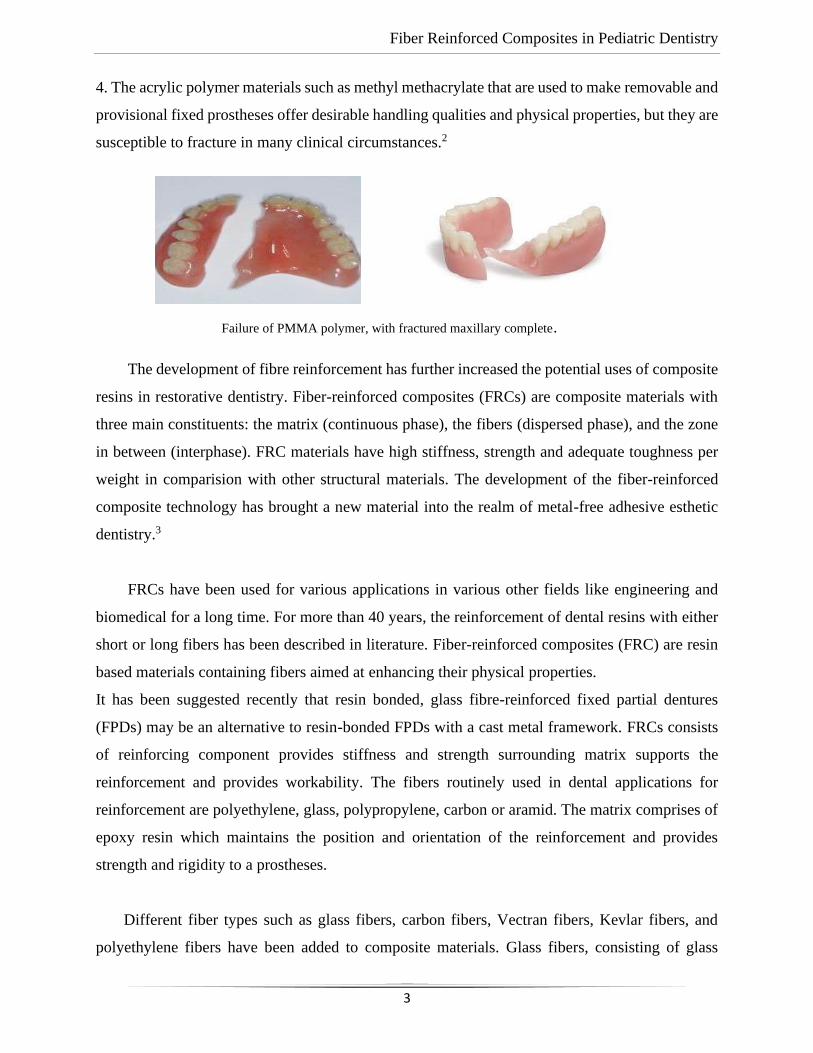
2. Ceramic materials such as porcelain may exhibit good optical qualities, but they are also brittle
and hard, they have the potential to lose structural integrity, and they sometimes abrade or fracture
the opposing teeth.2
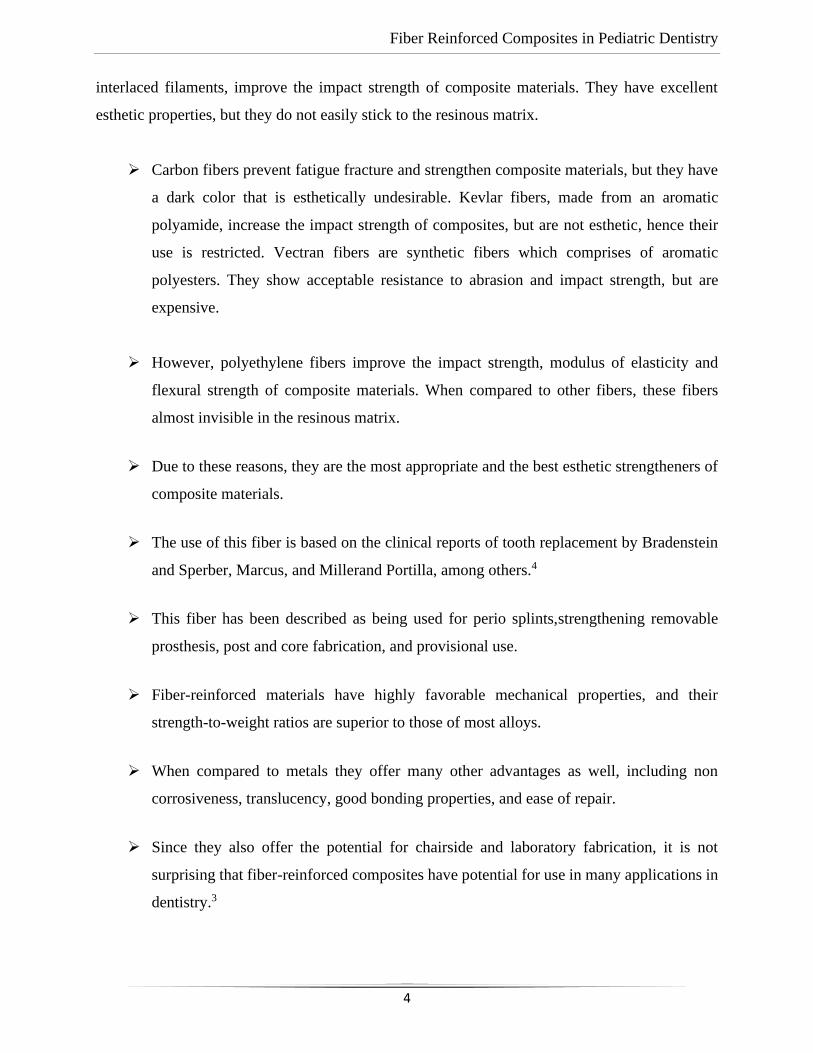
3. The porcelains used to mask the metal substructure are opaque, unesthetic and require a
minimum thickness of coverage to obtain an acceptable result. Use of hard, brittle porcelain veneer
results in severely abraded mandibular anterior teeth opposing the porcelain and porcelain-metal
junction of metal-ceramic crowns.
Unesthetic appearance due to metal exposure at
base of the crown
Source: James Fondriest 2019
Of te
Metal ceramic prosthesis prior to try in
appointment
Of te
Metal-ceramic FPD with a fractured porcelain veneer and
abrasion of opposing teeth
Fiber Reinforced Composites in Pediatric Dentistry
3
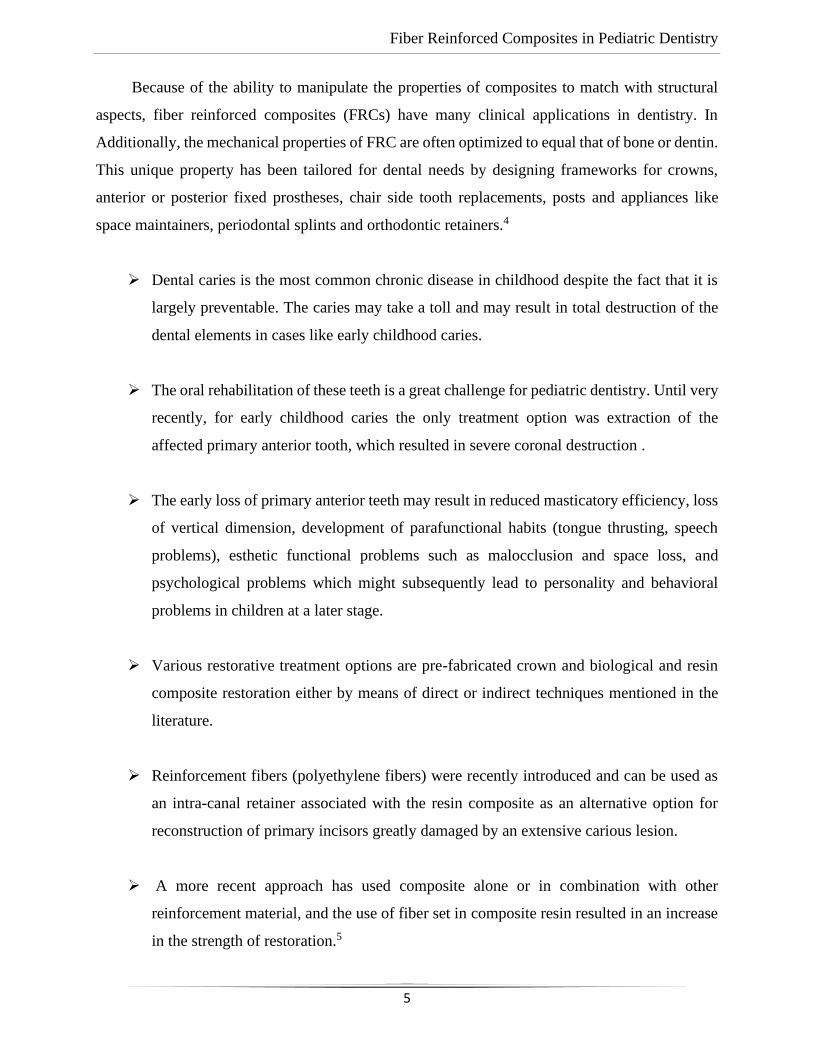
4. The acrylic polymer materials such as methyl methacrylate that are used to make removable and
provisional fixed prostheses offer desirable handling qualities and physical properties, but they are
susceptible to fracture in many clinical circumstances.2
The development of fibre reinforcement has further increased the potential uses of composite
resins in restorative dentistry. Fiber-reinforced composites (FRCs) are composite materials with
three main constituents: the matrix (continuous phase), the fibers (dispersed phase), and the zone
in between (interphase). FRC materials have high stiffness, strength and adequate toughness per
weight in comparision with other structural materials. The development of the fiber-reinforced
composite technology has brought a new material into the realm of metal-free adhesive esthetic
dentistry.3
FRCs have been used for various applications in various other fields like engineering and
biomedical for a long time. For more than 40 years, the reinforcement of dental resins with either
short or long fibers has been described in literature. Fiber-reinforced composites (FRC) are resin
based materials containing fibers aimed at enhancing their physical properties.
It has been suggested recently that resin bonded, glass fibre-reinforced fixed partial dentures
(FPDs) may be an alternative to resin-bonded FPDs with a cast metal framework. FRCs consists
of reinforcing component provides stiffness and strength surrounding matrix supports the
reinforcement and provides workability. The fibers routinely used in dental applications for
reinforcement are polyethylene, glass, polypropylene, carbon or aramid. The matrix comprises of
epoxy resin which maintains the position and orientation of the reinforcement and provides
strength and rigidity to a prostheses.
Different fiber types such as glass fibers, carbon fibers, Vectran fibers, Kevlar fibers, and
polyethylene fibers have been added to composite materials. Glass fibers, consisting of glass
Failure of PMMA polymer, with fractured maxillary complete.
Fiber Reinforced Composites in Pediatric Dentistry
4
interlaced filaments, improve the impact strength of composite materials. They have excellent
esthetic properties, but they do not easily stick to the resinous matrix.
➢ Carbon fibers prevent fatigue fracture and strengthen composite materials, but they have
a dark color that is esthetically undesirable. Kevlar fibers, made from an aromatic
polyamide, increase the impact strength of composites, but are not esthetic, hence their
use is restricted. Vectran fibers are synthetic fibers which comprises of aromatic
polyesters. They show acceptable resistance to abrasion and impact strength, but are
expensive.
➢ However, polyethylene fibers improve the impact strength, modulus of elasticity and
flexural strength of composite materials. When compared to other fibers, these fibers
almost invisible in the resinous matrix.
➢ Due to these reasons, they are the most appropriate and the best esthetic strengtheners of
composite materials.
➢ The use of this fiber is based on the clinical reports of tooth replacement by Bradenstein
and Sperber, Marcus, and Millerand Portilla, among others.4
➢ This fiber has been described as being used for perio splints,strengthening removable
prosthesis, post and core fabrication, and provisional use.
➢ Fiber-reinforced materials have highly favorable mechanical properties, and their
strength-to-weight ratios are superior to those of most alloys.
➢ When compared to metals they offer many other advantages as well, including non
corrosiveness, translucency, good bonding properties, and ease of repair.
➢ Since they also offer the potential for chairside and laboratory fabrication, it is not
surprising that fiber-reinforced composites have potential for use in many applications in
dentistry.3
Fiber Reinforced Composites in Pediatric Dentistry
5
Because of the ability to manipulate the properties of composites to match with structural
aspects, fiber reinforced composites (FRCs) have many clinical applications in dentistry. In
Additionally, the mechanical properties of FRC are often optimized to equal that of bone or dentin.
This unique property has been tailored for dental needs by designing frameworks for crowns,
anterior or posterior fixed prostheses, chair side tooth replacements, posts and appliances like
space maintainers, periodontal splints and orthodontic retainers.4
➢ Dental caries is the most common chronic disease in childhood despite the fact that it is
largely preventable. The caries may take a toll and may result in total destruction of the
dental elements in cases like early childhood caries.
➢ The oral rehabilitation of these teeth is a great challenge for pediatric dentistry. Until very
recently, for early childhood caries the only treatment option was extraction of the
affected primary anterior tooth, which resulted in severe coronal destruction .
➢ The early loss of primary anterior teeth may result in reduced masticatory efficiency, loss
of vertical dimension, development of parafunctional habits (tongue thrusting, speech
problems), esthetic functional problems such as malocclusion and space loss, and
psychological problems which might subsequently lead to personality and behavioral
problems in children at a later stage.
➢ Various restorative treatment options are pre-fabricated crown and biological and resin
composite restoration either by means of direct or indirect techniques mentioned in the
literature.
➢ Reinforcement fibers (polyethylene fibers) were recently introduced and can be used as
an intra-canal retainer associated with the resin composite as an alternative option for
reconstruction of primary incisors greatly damaged by an extensive carious lesion.
➢ A more recent approach has used composite alone or in combination with other
reinforcement material, and the use of fiber set in composite resin resulted in an increase
in the strength of restoration.5
Fiber Reinforced Composites in Pediatric Dentistry
6
HISTORY
➢ Fiber reinforced composite (FRC) group of materials have been in use and tested since
1960s but for dental use developed and clinically approved materials are available more
extensively during the last 30 years and for the medical implant use during the 15 years.
➢ The initial attempts for using fiber reinforcement in clinical dentistry began more than
35 years ago. In the 1960s and 1970s, investigators sought to reinforce standard
polymethyl methacrylate dentures with glass or carbon fibers.
➢ In the 1980s, similar attempts were repeated, and initial efforts were made to fabricate
fiber-reinforced prosthodontic frameworks for implants, fixed prosthodontics
restorations, orthodontic retainers, and splints.2
➢ While these materials and techniques demonstrated improved mechanical properties,
they failed to achieve general clinical acceptance because of insufficient enhancement of
properties and awkward clinical manipulating procedures.
➢ Almost all the procedures advocated involved automatic manual placement of fibers into
dental resins that were otherwise processed with routine methods.
➢ But this approach was inconvenient because free fibers are difficult to handle and utmost
care must be taken to avoid either damaging or contaminating them.
➢ Even though the addition of fibers increased mechanical properties, the degree of
improvement achieved was far below other commercial applications.
➢ There were two main reasons for the lower-than-expected mechanical results.
➢ First, the actual amount of fiber incorporated into the dental resins was low, typically
less than 15% by volume. (Industrial products may contain 50% or even as much as 70%
fiber by volume.)
Fiber Reinforced Composites in Pediatric Dentistry
7
➢ Second, as stated in theory the fiber reinforcement was not very effective due to the poor
wetting of the fiber bundles by the resin which led to insufficient coupling and gaps
between the fibers and resin.
➢ During testing, it was found that effective coupling usually results in failure within the
matrix not at the fiber-matrix interface.
➢ Clinical uses and whether the fiber bundles are pre-impregnated with resin by the
manufacturer or resination is required by the dentist or laboratory technician. 2
➢ Though there is wide variation between products in fiber surface treatments, dental
manufacturers use only standard industrial fibers; methods for incorporating the fibers
into the polymeric resin, and chairside and laboratory processing methods.
➢ Towards the end of 1980s, dental researchers found the importance of effective coupling
and complete impregnation of the fiber bundles by the resin and started developing
techniques applicable for dentistry.
➢ Since then two approaches have evolved. In the first technique, manual application of a
low viscosity resin to the fiber bundles is done by the dentist or laboratory technician. It
provides complete wetting, Though it provides versatility in the selection of fibers and
resin, this approach can be cumbersome and requires an additional step in the procedure.
➢ The other approach is to use pre-impregnated fiber bundles during a controlled
manufacturing process.
➢ There are numerous manufacturing parameters which regulate the final fiber dimensions
and content, the viscosity of the resin, speed of the process, tension on the fiber bundles
etc.
Fiber Reinforced Composites in Pediatric Dentistry
8
➢ These complex process parameters allow for high fiber content, complete wetting,
minimum void content, and control of the cross-sectional dimensions in pre-impregnated
FRCs.2
➢ Some of the earliest of these experimental pre-impregnated FRCs designed for dental
applications were based on glass-reinforced thermoplastics.
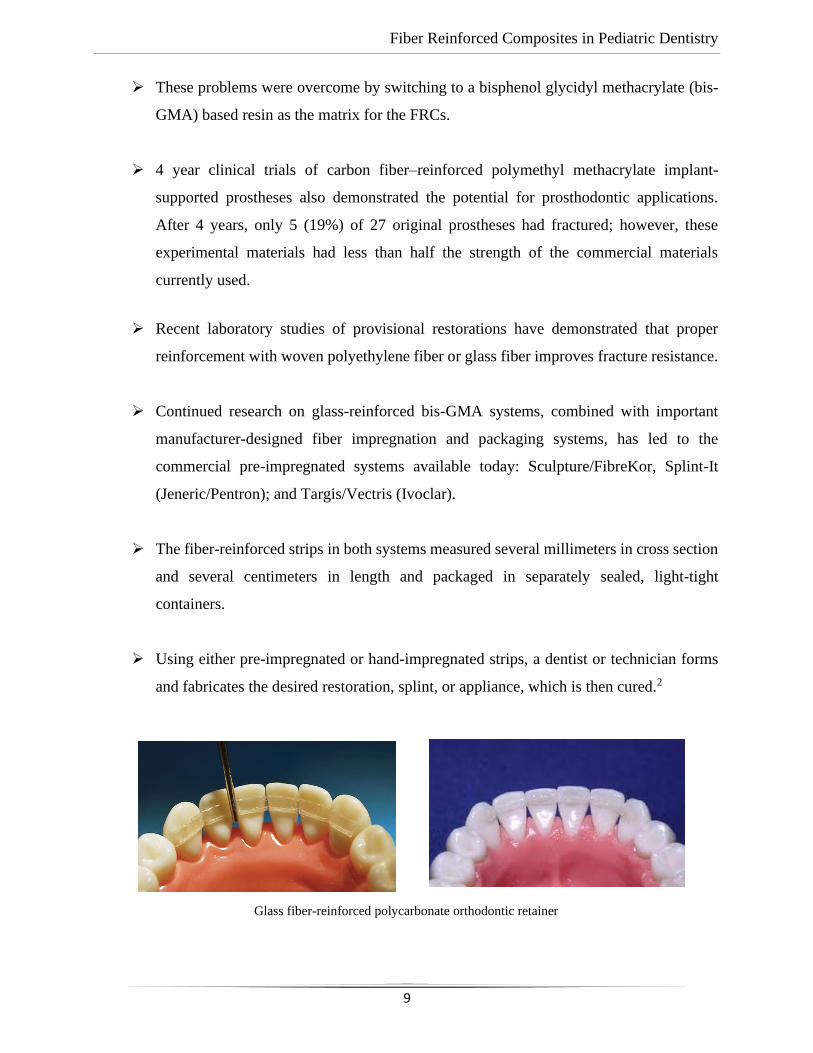
➢ Clinical trials were conducted using glass-reinforced polycarbonate as orthodontic
retainers. The function of esthetic retainers is satisfactory and the mean service life of
20.4 months.
➢ Most importantly, only 6% of those that failed were due to frank mechanical breakage of
the fiber composites, confirming that the physical properties of these materials are
adequate for this clinical application. The cause of most of the clinical failures was
debonding of the retainers from the tooth surface.
➢ A successive clinical trial evaluated the application of pre-impregnated glass-reinforced
polycarbonate as the framework for acid-etched fixed partial dentures (FPDs).
➢ 14 three unit restorations were placed both in anterior and posterior region using adhesive
techniques and without any tooth preparation.
➢ After 9 years, three restorations were still in place. Eleven failures were caused by
separation in the region of the tooth restoration interface and none was due to frank
mechanical breakage of the fiber-reinforced framework.
➢ The clinical failures mainly occurred at the adhesive-tooth interface, the adhesive–fiber
composite interface, or within the outer matrix of the fiber-reinforced composite.
➢ This study established the acceptable mechanical properties of FRCs for use in
prosthodontics and it also confirmed that it is difficult to manipulate the thermoplastic
resin matrix and offers poor bonding to tooth structures.2
Fiber Reinforced Composites in Pediatric Dentistry
9
➢ These problems were overcome by switching to a bisphenol glycidyl methacrylate (bis-
GMA) based resin as the matrix for the FRCs.
➢ 4 year clinical trials of carbon fiber–reinforced polymethyl methacrylate implant-
supported prostheses also demonstrated the potential for prosthodontic applications.
After 4 years, only 5 (19%) of 27 original prostheses had fractured; however, these
experimental materials had less than half the strength of the commercial materials
currently used.
➢ Recent laboratory studies of provisional restorations have demonstrated that proper
reinforcement with woven polyethylene fiber or glass fiber improves fracture resistance.
➢ Continued research on glass-reinforced bis-GMA systems, combined with important
manufacturer-designed fiber impregnation and packaging systems, has led to the
commercial pre-impregnated systems available today: Sculpture/FibreKor, Splint-It
(Jeneric/Pentron); and Targis/Vectris (Ivoclar).
➢ The fiber-reinforced strips in both systems measured several millimeters in cross section
and several centimeters in length and packaged in separately sealed, light-tight
containers.
➢ Using either pre-impregnated or hand-impregnated strips, a dentist or technician forms
and fabricates the desired restoration, splint, or appliance, which is then cured.2
Glass fiber-reinforced polycarbonate orthodontic retainer
Fiber Reinforced Composites in Pediatric Dentistry
10
➢ For most of the FRC procedures, a direct or indirect method can be used. Splints are
commonly fabricated with a direct approach and light-cured, while to minimize chair time
and to allow for optimum esthetic and mechanical results fixed prostheses are typically
fabricated by dental laboratories.
➢ Both hand-impregnated and pre-impregnated systems are commercially available to the
laboratory, although the latter are more widely used.
➢ Two commercial pre-impregnated systems are available for dental laboratories. Both use
fiber composites to fabricate the framework, and the final tooth shape is then built with
particulate reinforced restorative composite.
➢ One system, Sculpture/FibreKor (Jeneric/Pentron), uses hand fabrication to form the
framework and con-dense the strips .2
➢ The other system, Targis/Vectris (Ivoclar), uses custom-made matrices and special
equipment to apply pressure to the fiber strips during fabrication.
➢ The primary aim in the fabrication of the framework are to incorporate adequate amount
of fiber reinforcement, reduce voids and confirm strong bonding between both the layers
of pre-impregnated fiber strips and restorative composite and the fiber framework in both
systems,.
➢ Clinical trials of the commercial systems, now in their third year, demonstrate satisfactory
performance when appropriate designs, fiber volume, and manipulative procedures are
followed, although a loss of surface luster was often observed soon after placement.
➢ The initial designs of fiber-reinforced FPDs required substitution of the facings, however
repair techniques have been described to minimize or eliminate the need to replace the
complete restoration.
Fiber Reinforced Composites in Pediatric Dentistry
11
APPLICATIONS FOR FIBER REINFORCED
COMPOSITES OUTSIDE DENTISTRY:
➢ Fiber-reinforced composites (FRCs) have the potential to remedy many of the structural
andesthetic problems described above.
➢ Though the use of these materials is new to dentistry, but they have found application in
a number of industries outside dentistry because of their many advantageous properties.
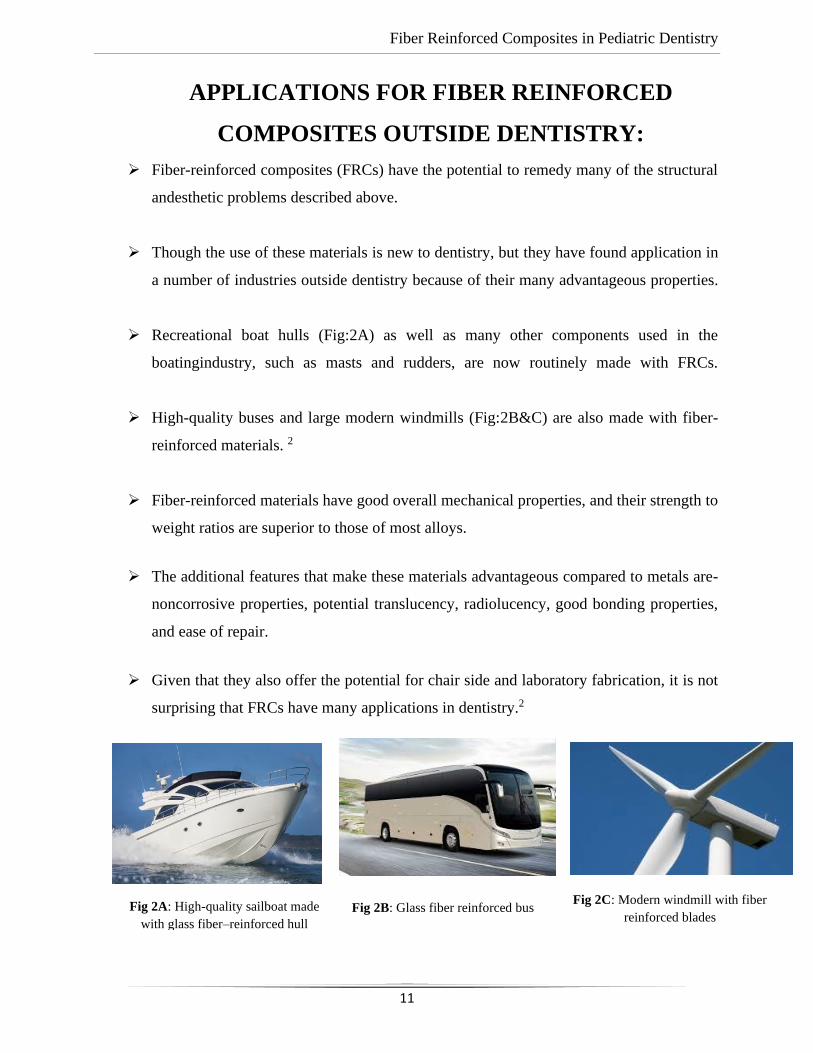
➢ Recreational boat hulls (Fig:2A) as well as many other components used in the
boatingindustry, such as masts and rudders, are now routinely made with FRCs.
➢ High-quality buses and large modern windmills (Fig:2B&C) are also made with fiber-
reinforced materials. 2
➢ Fiber-reinforced materials have good overall mechanical properties, and their strength to
weight ratios are superior to those of most alloys.
➢ The additional features that make these materials advantageous compared to metals are-
noncorrosive properties, potential translucency, radiolucency, good bonding properties,
and ease of repair.
➢ Given that they also offer the potential for chair side and laboratory fabrication, it is not
surprising that FRCs have many applications in dentistry.2
Fig 2A: High-quality sailboat made
with glass fiber–reinforced hull
Fig 2B: Glass fiber reinforced bus Fig 2C: Modern windmill with fiber
reinforced blades
Fiber Reinforced Composites in Pediatric Dentistry
12
DEFINITION AND CLASSIFICATION OF FIBER
REINFORCED COMPOSITES:
• Fibre-reinforced composite restorations are resin-based restorations containing
fibres aimed at enhancing their physical properties.
• The nature of the fibre, the geometrical arrangement of the fibres and the overlying resin
used makes this group of materials is very heterogeneous
• An adhesive interface allows the fibres within the composite matrix to bond to the resin.
The main factors that influence the physical properties of FRC structures are listed as follows:
• Fibre loading (volumetric fraction) within the restoration;
• The fibre-resin interface bond efficacy;
• Fibre orientation relative to load;
• Fibre position in restoration3
Fiber Reinforced Composites in Pediatric Dentistry
13
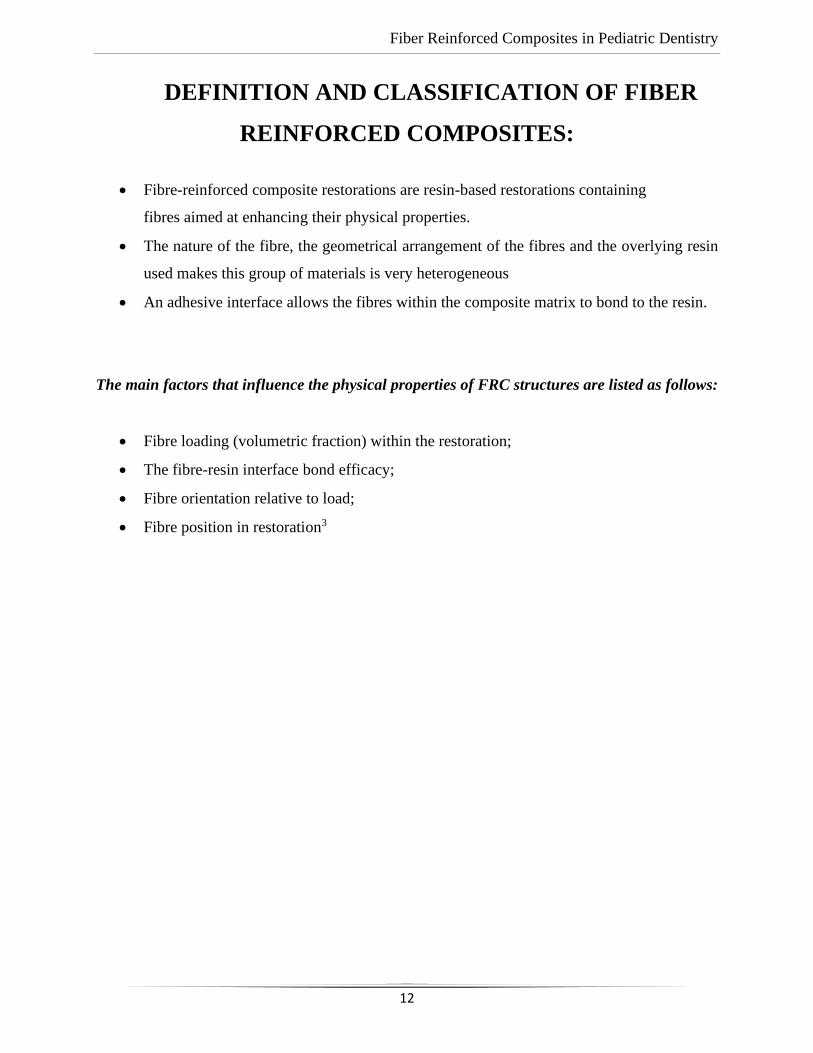
CLASSIFICATION:2 Fiber reinforced composites can be
classified as follows:
ADVANTAGES AND DISADVANTAGES OF FRCs:
ADVANTAGES
• Lower treatment costs.
• Single visit immediate tooth replacements.
• Appropriate for long-term and transitional provisional restorations.
• Readily repaired.
• Suitable for young patients (developing dentition) and elderly (time saving).
• Metal free restoration.
• Improved aesthetics.
• Can be produced in a simple manner in the laboratory without the need for waxing,
investing and casting.
Fiber Reinforced Composites in Pediatric Dentistry
14
• Can be routinely used with minimal or no tooth preparation.
• Minimize abrasion of the opposing teeth in comparison to conventional metal-ceramic
restorations.
DISADVANTAGES
• Potential wear of the overlying veneering composite especially in patients with significant
parafunction.
• May lack sufficient rigidity for long span bridges.
• Excellent moisture control required for adhesive technique.
• To allow sufficient room for fibres and adequate bulk for veneering composite overlay,
space requirements are greater in posterior occlusal situations in comparison to metal
occlusal surfaces.
• Uncertain longevity in comparison to traditional techniques.3
COMPOSITION, ARCHITECTURE, AND MECHANICAL PROPERTIES
OF FIBER-REINFORCED COMPOSITES4
• Fiber-reinforced composites (FRCs) are structural materials that have at least two distinct
constituents.
• The reinforcing component imparts stiffness and strength, whereas the encompassing
matrix supports the reinforcement and provides workability.
• In dental applications, one of the constituents may be metal, ceramic, or polymer,
polymeric or resin matrices reinforced with glass, polyethylene, or carbon fiber are most
common.
• Usually, fibers are 7 to 10 pm in diameter and span the length of the prosthesis or appliance.
The particle size used in standard restorative dental composites are 1 to 5 pm in diameter,
or submicron. The fibers may be arranged in various configurations: unidirectional fibers
—continuous, long and parallel—are the most popular, followed by braided and woven
fibers.

Fiber Reinforced Composites in Pediatric Dentistry
15
• The type of fiber used to make an FRC depends on how it is intended to be used and the
characteristics that are needed for that purpose.
• Glass fibers of various kinds are commonly used in dental laboratory products, while
polymeric reinforcements, such as polyethylene, are often used for chairside applications.
Posts are made of carbon or glass fibers.
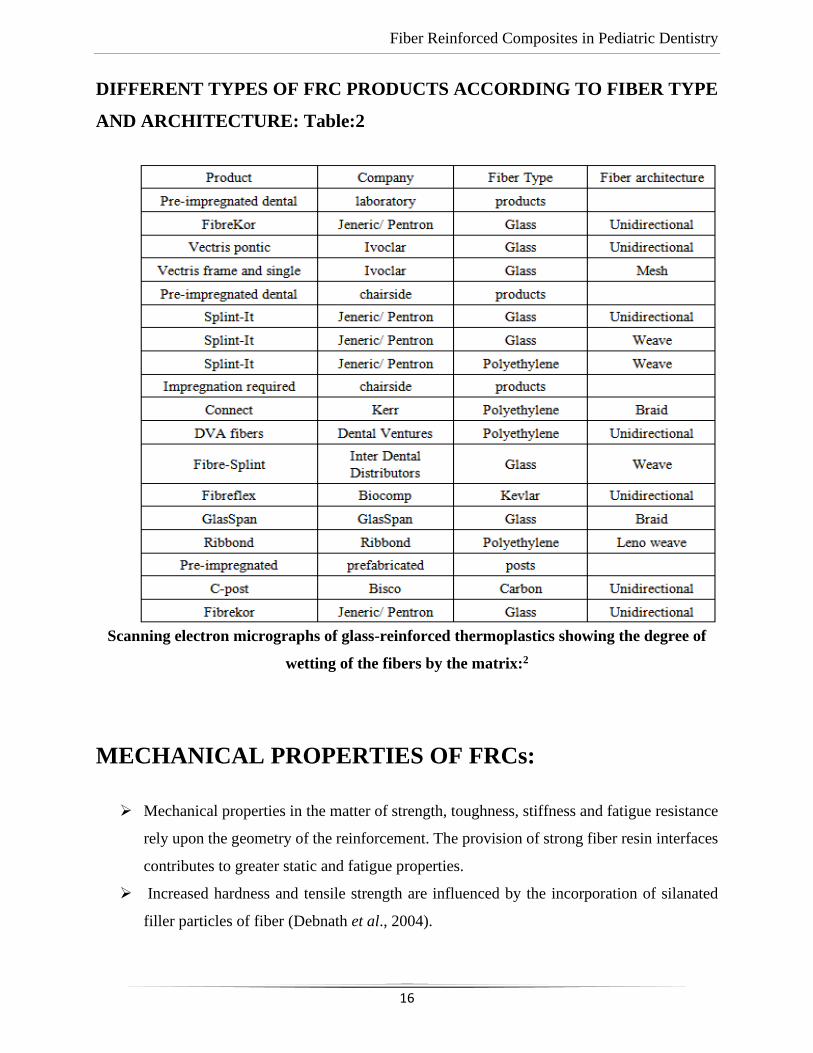
• Table below (table:2) lists different types of fiber and the important mechanical and
physical characteristics of each. The types of fiber and architecture found in various
products products are classified according to their clinical uses and whether the fiber
bundles are pre-impregnated with resin by the manufacturer or resination is required by the
dentist or laboratory technician.4
Fiber Reinforced Composites in Pediatric Dentistry
16
DIFFERENT TYPES OF FRC PRODUCTS ACCORDING TO FIBER TYPE
AND ARCHITECTURE: Table:2
Scanning electron micrographs of glass-reinforced thermoplastics showing the degree of
wetting of the fibers by the matrix:2
MECHANICAL PROPERTIES OF FRCs:
➢ Mechanical properties in the matter of strength, toughness, stiffness and fatigue resistance
rely upon the geometry of the reinforcement. The provision of strong fiber resin interfaces
contributes to greater static and fatigue properties.
➢ Increased hardness and tensile strength are influenced by the incorporation of silanated
filler particles of fiber (Debnath et al., 2004).
Fiber Reinforced Composites in Pediatric Dentistry
17
➢ The effectiveness of the fiber reinforcement, as described on theKrenchel’s factor, differs
according to the length and fiber orientation.
➢ The reinforcing efficiency factor for the fiber reinforcement goes against the known
direction of stress (Krenchel 1963).
➢ Many other parameters contribute to the reinforcing efficiency offibers, between them
interfacial adhesion, fiber volume fraction and elongation of fibers (Murphy, 1998).
➢ Fiber-reinforced composites are classified as short discontinuous and long continuous
FRCs. They show differences in their mechanical properties even when their fiber volume
fraction is similar (Kardos 1993).
➢ For instance, if continuous unidirectional fibers are replaced by longitudinally oriented
discontinuous short fibers of lower aspect ratio, a reduction of the ultimate tensile strength
of the composite will be the result (Vallittu, 2015).4
➢ The isotropicity-anisotropicity of the material plays a role. Continuous and discontinuous
FRCs are anisotropic and they become isotropic when the orientation of short fibers is
random, with the outcome of reducing the tensile strength.
➢ In a polymeric structure the provision of fiber reinforcement increase its modulus of
elasticity or stiffness and toughness (Wright et al., 1997).
➢ The modulus of elasticity (E) is a measure of the stiffness, defined by the slope of the
stress-strain curve linear segment before plastic deformation.
➢ According to that, a direct influence exists between the E and the stiffness, providing that
the higher the E, the stiffer the material will be.
➢ The greater the E, the less the elastic deformation will be as a resultant of the stress
application.
➢ Toughness is the ability of a material to absorb energy and have the capacity to plastically
deform without fracturing (Callister, 1991). Some investigations have been focused on the
effects of fracture toughness and E on FRCs.
➢ One of them found that the E of particulate reinforced composites increases when cross-
sectional designs included 1 or more fiber reinforcements located at the compression side
(Dyer et al 2005).4
Fiber Reinforced Composites in Pediatric Dentistry
18
ADHESIVE INTERFACE:
➢ The adhesive interface transfers the load from the polymer matrix to the reinforcing fibers,
which positions this interface as a key aspect for the durability of FRCs (Bouillaguet et al.,
2006).
➢ A chemical bond is achieved between the polymer matrix and the exposed glass fibers due
to the use of silane coupling agents.
➢ The abilities of silanes to enhance the surface wettability of the glass fibers, resulting in
chemical bridges formation and an increased physical attachment of the resin to the surface
of glass have been reported in some studies. (Goracci et al., 2005).
➢ Some other aspects have an effect on the durability of FRC restorations, for instance, the
properties of the fibers; resin matrix; the quantity of fibers; the direction, orientation,
distribution, construction and position of the fibers and the impregnation of the fibers with
the resin (Pensler etal., 1997).
➢ Two types of resins are used in FRCs, forming a cross-linked (thermoset) Polymer matrix,
or a linear (thermoplastic) polymer matrix. Multifunctional or dimethacrylate resins are
involved in the formation of the cross-linked matrix, contrary to the non-crosslinked
polymer matrix where monofunctional methacrylates are included (Vakipartaet al., 2007).
➢ A combination of thermoset and thermoplastic resins has been used as impregnation
methods. In this case, the polymer matrix is a semi-interpenetrating polymer network (semi-
IPN), where a cross-linked polymer and a linear polymer are merged(Kallio et al., 2001). 6
➢ Cross-linked polymer matrix results in FRCs with higher modulus of elasticity than the
achieved by thermoplastic or semi-IPN polymers (Lassila et al.,2002).
➢ Additionally, higher toughness is one of the advantages that thermoplastic and semi-IPN
polymer matrices contribute over FRCs manufactured from highly cross-linked thermosets.
➢ The semi-IPN polymer matrix of FRC provides some benefits over crosslinked
dimethacrylate regarding its handling properties and the adhesion of indirectly made
restorations to resin luting cements and veneering composites (Kallio et al.,
2001).Polyethylene (PE), polyetheretherketone (PEEK), polyacetal (PA), and polyurethane
(PU) are examples of thermoplastics that are used in medical applications of thermosets are
epoxy polymer, bis-GMA, and TEGDMA copolymer (Tuusa et al.,2007).
Fiber Reinforced Composites in Pediatric Dentistry
19
Rule of Mixtures
➢ In prosthodontic applications, the two most important mechanical properties for FRCs are
strength and stiffness. The modulus of elasticity refers to stiffness or rigidity of the material.
➢ For fiber-reinforced FPD frameworks a high modulus is necessary because they must
support the more brittle overlying restorative composite. This situation is comparable to
metal frameworks supporting porcelain in a metal-ceramic prosthesis.
➢ In an ideal unidirectional FRC, the modulus as well as the strength in the fiber direction is
proportional to the volume and individual properties of the fiber and the matrix. This
relationship is known as the rule of mixtures.2
➢ The rigidity and strength of a unidirectional fiber composite are significantly dependent on
the properties and volume of the fiber as the properties of the fiber are generally much
greater than those of the matrix,
➢ Large volumes of high-strength unidirectional fibers are desirable when the highest
mechanical properties are desired in a single direction, as in a post or in the pontic region
of an FPD framework,
➢ Areas where esthetics may not be of concern, carbon fibers may be used. Glass fibers are
generally preferred where translucency is required along with good mechanical properties.
➢ Fiber volumes are generally limited to less than 50% because of the necessity of having all
fibers fully wetted by the resin. Classic pre-impregnated unidirectional dental fiber
composites incorporating approximately 45% glass fibers have a flexure modulus in the
range of 28 to 34 GPa and flexure strengths of about 600 to 1,000 MPa.
➢ These values are about 10 times greater than those for dental resin alone, and they represent
the primary mechanical benefit of using fiber reinforcement in dentistry.
Fiber Reinforced Composites in Pediatric Dentistry
20
How FRC Materials Work
➢ Several parameters influence the mechanical performance of FRC. Increasing fiber volume
leads to a greater increase in mechanical strength. The fiber architecture: unidirectional
fibers long, continuous, and parallel followed by braided and woven fibers also increase
flexural strength b van Hueman.4
➢ Typically, fibers are 7 to 10 μm in diameter and span the length of the prosthesis or appliance
whereas the size of the particles used in standard restorative dental composites are 1 to 5
μm in diameter, or submicron in size.
➢ Glass fibers of various kinds are commonly used in dental laboratory products, while
polymeric reinforcements, such as ultra high molecular weight polyethylene, are often used
for chair-side applications. Posts are made of carbon or glass fibers.
• Woven fiber has lesser flexural strength and is less technique-sensitive, and easy to manipulate
thus conforming to the desired shape and maintains its adaptation during placement and is the ideal
choice while making an appliance for rotated or malpositioned teeth.
• Unidirectional fiber has greater flexure strength and rigidity and is the better choice for high
stress situations as in prosthodontic frameworks.4
Fiber Reinforced Composites in Pediatric Dentistry
21
The Two Approaches have Evolved Namely Non-Impregnated and
Pre-Impregnated
Non Impregnated :
Non-impregnated are the fibers that needs to be wetted with an unfilled fourth or fifth
generation bonding resin at chairside. A partially filled bonding resin is not recommended to wet
the Ribbond as they are more viscous and hence are not self wetting. While it provides complete
wetting, this approach can be cumbersome, requires an additional step in the procedure and
displays limited service as splints. However, this method can be considered versatile.
Pre-Impregnated Fibers :
➢ Clinical longevity of non-impregnated fibers is compromised as it lack good adhesion
between the fiber and resin matrix compromising and freshly drawn glass fibers exhibit
higher strength than ordinary glass fibers but are rapidly degraded on exposure to moisture
and humidity.4
➢ As these fibers with resin maintains the high strength values if coated immediately, the
concept of pre-impregnation of glass fibers evolved (Splint-it). This procedure is
accomplished by pre-impregnating the fiber bundles with resin during the manufacturing
process.
➢ Pretreatment of glass fibers are done with organo-silanes and polyethylene fibers are
subjected to cold gas plasma treatment to increase their wettability and chemical bond. E-
glass and S-glass are two types of glass fibers of which E-glass is employed in dental
materials. Another type used is C-glass mainly used in chemical applications that requires
greater corrosion resistance to acids than is provided by E-glass.
Fiber Reinforced Composites in Pediatric Dentistry
22
IMPREGNATION OF FIBERS:
➢ Resin impregnation allows an optimal reinforcement and transfer of stresses from the
polymer matrix to the reinforcing fibers (Vallittu, 1998b).
➢ Effective impregnation is a requirement to achieve a good contact between the matrix and
each fiber, which isoften performed using various monomers. Some of these monomers are
bis-GMA,UDMA, urethane tetramethacrylate (UTMA), poly(methylmethacrylate) (PMMA)
ortriethylene glycol dimethacrylate (TEGDMA) (Lastumäki et al., 2003).
➢ The use of only monomers for the impregnation of fibers brings as a consequence a high
polymerization shrinkage, which may affect the mechanical properties of the FRC (Vallittu,
1996).
➢ Then, pre-impregnated FRC systems have been developed, which facilitates the handling
properties.
➢ Deficiencies in the impregnation of fibers increase the water sorption in FRC, reducing their
strength and modulus of elasticity (Miettinen et al., 1999).
➢ The use of high viscosity resin systems and the polymerization shrinkage of the resin can
have as consequence an inadequate degree of impregnation of fibers (Vallittu 1995a; Vallittu
1995b).
➢ This enhances water sorption through voids leading to decreased mechanical properties of
FRC (Miettinen & Vallittu, 1997). In addition, voids originated due to poorly impregnated
fibers serve as oxygen reservoirs that inhibit the radical polymerization of the polymer matrix
(Vallittu, 1999).
➢ Pre-impregnated FRCs also show good mechanical properties due to the reduction in voids
and cracks in its composition, which can limit water sorption. Water sorption due to poor
impregnation can have detrimental consequences in the bond strength and lead to hydrolytic
degradation of polysiloxane network of FRC (Miettinen & Vallittu, 1997).5

Fiber Reinforced Composites in Pediatric Dentistry
23
PROPERTIES OF FIBRE REINFORCED COMPOSITE
Water sorption:
➢ Water sorption of a material includes water absorbed into the body and water adsorbed on
the surface of the material during preparation and while the material is in service.
➢ Poly (methyl methacrylate) absorbs water because of the polarity of the water molecule
and because it is smaller than the inter chain distance in the polymer.
➢ The volume of water uptake by a polymeric material is determined by polymer structure,
content of various polar and hydrophilic groups in the polymer structure, temperature,
concentration of various additives, presence of voids within the matrix, Physicochemical
and mechanical properties can be affected by absorbed water.5
Flexure Strength:
➢ These materials are often tested in the laboratory, although the mode of failure and many
other properties affect clinical performance.
➢ Investigators accentuate the importance of fatigue and fracture toughness in predicting
clinical performance of several classes of dental materials, including fibre composites.
➢ It is important to note that test methods, procedures for preparing the samples, and, in
particular, the geometry of the test specimens all affect the calculated flexure strength.
➢ Flexure strength for commercial laboratory–processed fibre-reinforced composites may
range from approximately 300 to 1,000 MPa, depending on the specimen preparation and
geometry.
Fracture toughness:
➢ The fracture toughness of a material reflects the resistance of a material to fracture and
represents the energy required to propagate a crack through the material to complete
fracture.
Fiber Reinforced Composites in Pediatric Dentistry
24
➢ Fracture toughness of polymer composites depends on the type of polymer and
reinforcement. Fracture toughness of a monomethacrylate-based material is lower than in
a dimethacrylate-based material.
➢ Generally, “intrinsic” physical aging and/or storage in a humid environment at elevated
temperatures can decrease fracture toughness, as well as other mechanical properties.
However, an increase in fracture toughness can be achieved by adding reinforcing fibres
to a polymer to prevent or slow down crack growth.5
Linear coefficient of thermal expansion:
➢ The variation of the coefficient of thermal expansion between different materials is
important because a mismatch can lead to strains, resulting in stress formation and adverse
effects on the interface.
➢ Therefore, thermally induced strains and stresses adversely affect long-term stability of
intraoral multiphase materials. By adding fibres to a polymer, the coefficient of thermal
expansion decreases.
➢ Usually, the thermal coefficient varies with the direction of the fibres. The matrix is forced
to expand in the transverse direction as in a composite rigid fibres appear to prevent
expansion of the matrix in the longitudinal direction.
➢ One of the major concerns in the development of dental materials is physical and chemical
durability.
Fiber Reinforced Composites in Pediatric Dentistry
25
BIOCOMPATIBILITY
Solubility:
➢ Stabilizers, plasticizers, monomers, residuals of initiators and degradation products are the
components that may be released into the oral environment over time.
➢ Therefore, the amount of such components should be as small as possible to ensure that no
components adversely influence biocompatibility and the polymer retains its characteristic
properties.
Residual monomer:
➢ Biological features, as well as mechanical properties, of polymeric materials are highly
influenced by the monomer-polymer conversion.
➢ Residual monomer will alter the property and may leach out to pulp if a protective layer of
base is not given.5
Cytotoxicity:
➢ Some substances released from materials are cytotoxic and residual monomers leached out
into the oral environment may induce toxic and allergic reactions.
Polymerization shrinkage:
➢ The increased awareness among clinicians to protect and reinforce the remaining sound tooth
structure and gradual improvement in adhesive systems resulted in the increased use of
particulate filler composite resin materials (PRFC) both at the anterior and posterior regions.
➢ Despite the continuous improvement through modifications in formulation, polymerization
shrinkage seems to be a problem for the PRFC.
Various steps have been undertaken to evaluate and improve restorative composite resin against
wear and lower the polymerization shrinkage. Attempts have been made to change type and size
of filler and their silanization. Also attempts to change the polymerization kinetics of resins and to
influence to degree of monomer conversion. Reinforcing the resin with glass fibres with fibre-
reinforced composite (FRC) substructure and optimization of filler content are among the methods
that have been studied.
Fiber Reinforced Composites in Pediatric Dentistry
26
THE MATRIX IN FRCS
➢ The fibers in the composite structure are held together by the polymeric plastic matrix
composed of polymerised monomers. It protects the fibers from the external environment such
as moisture, chemicals and mechanical shocks and transfers stresses between fibers.
➢ Therefore the matrix may have an impact on the compressive strength, interlaminar shear and
in-plate shear properties, interaction between the matrix and the fiber and defects in the
composite. 6
➢ Two types of resins namely the cross-linked or linear, are used in FRCs. The cross-linking
polymer referring to multifunctional or dimethacrylate resins is also called a thermoset
polymer. The linear polymer referring to monofunctional methacrylate polymers is also called
a thermoplastic polymer.
➢ The matrix consists of a cross-linking polymer, a linear polymer and a photo-initiator
with an interpenetrating polymer network (IPN) structure in FRCs. Polymerization
reactions and cross-linking reactions are the setting reactions in the resin matrix. Sequential
addition of monomeric units leading to the formation of a polymer by is a polymerization
reaction.
➢ Addition (including free-radical addition polymerisation) and condensation polymerizations
are the main polymerization reactions. The cross-linking reaction in a polymer is the
formation of a cross-link where chains are bonded together either through direct connection
or an intermediary atom, ion, molecule or chain. This produces a 3D strongly cross-linked
system.
FIBER:
➢ A fiber may be described as an elongated uniform material with a more or less equiaxed and
uniform transverse cross sectional diameter or thickness less than 250 μm, and with an aspect
ratio, i.e. length to cross-sectional diameter or thickness ratio, which is usually greater than
about 100.
➢ However, in some cases, such as short fibers, chopped fibers, or staple fibers, the fibers’ aspect
ratio can be smaller than 100.
Fiber Reinforced Composites in Pediatric Dentistry
27
➢ For the reinforcement and clinical success the fiber orientation, content, distribution and the
ability to maintain these parameters are significant.
➢ The type, length, orientation and volume fraction of the fiber influence the following
properties of the FRC: their tensile strength and modulus, compressive strength and modulus,
fatigue strength and fatigue failure mechanism, density, electrical and thermal conductivity,
and finally their cost. 6
➢ Glass, polyester, polyethylene, carbon/graphite, aramid, quartz and ceramic fibers are the
commonly used fibers.
ADHESION BETWEEN FIBER AND MATRIX
➢ Silanes are hybrid inorganic-organic chemical compound in which a carbon is directly attached
to silicon, eg. ≡Si–C≡. These silicon esters are used as coupling agents in silanization
treatment, often called as silanation. This refers to bonding of dissimilar matrices together with
surface treatment.
➢ Preimpregnation means that the fibers are impregnated with the matrix resin before further
steps in the fabrication of the final restoration in dentistry. Highly porous linear polymers are
used to preimpregnate the fibers as described in of the current preimpregnation based fiber
reinforcement system.
➢ This is why the high-viscous denture base resin is subjected to further impregnation.
➢ The use of natural rubber and thereafter synthetic polymers as denture base polymers had
already started in the 1860s.
➢ With the introduction of crosslinking thermoset monomers in dentistry by Bowen, crosslinking
dimethacrylate monomers became available also for monomer liquids of denture base resins
and, thus, in multiphase denture base polymers—the start of the use of interpenetrating
polymer network (IPN)-like structures in dentistry.
➢ As a concept, an IPN is a combination of two or more polymers in network form that are
synthesized injuxta position. IPNs are composed of finely divided phaseswith a thickness of
approximately 5–10 nm.6
➢ They differ from polymer blends which are rougher in structure, and also differ from
copolymers which are based on chemical reactions of monomer units and polymer backbones.
➢ Several adhesive interfaces between natural and synthetic biomaterials and adhesive resins by
means of primers or coupling agents can also be considered as IPNs.
Fiber Reinforced Composites in Pediatric Dentistry
28
➢ Some other interfaces are a dentine bonding hybrid layer, silane promoted adhesive interphases
between metal and ceramics and adhesive resins.
➢ On the other hand, the so-called semi-IPN refers to the impregnation methods based on using
a combination of thermoset and thermoplastic types of resins. Here, the polymer matrix is a
multiphase material.
➢ The semi-IPN is formed during the polymerization of the dimethacrylate monomers with a
swelled linear polymer, PMMA.
➢ In addition to the above methods, plasma-etching has also been applied to enhance
polyalkanefiber’s adhesion to the matrix.
➢ It is also noteworthy that durable adhesion between fiber and matrix provides good load
transfer between the two, which ensures that the load is transferred to the stronger fiber and
this is how the fiber works as a reinforcement.
➢ Hardness is a surface phenomenon influenced by yield strength, true tensile strength, work
hardening, elastic modulus and so on.
➢ Brinell, Vickers, Knoop, Rockwell, Rockwell superficial and Shore scleroscope are various
standard testing methods for hardness.
➢ Flexural strength refers to the maximum stress and strain at the surface of the specimen and a
measure of the stiffness during the first or initial step of bending a body (material) is flexural
modulus.
➢ It is calculated according to an ASTM D-790 standard: mathematically it is the slope of the
initial straight line portion on the stress–strain curve.
➢ In laboratory experiments, several factors have effects on the flexural properties. Previous
research shows that thermo-cycling, the brand of the FRC material and diameter of the
specimen may have a significant effect (p<0.001) on flexural strength of FRC root canal posts.
Furthermore, fatigue strength refers to the stress that causes failure after some specified
number of loading cycles.
➢ In the aspect of fatigue strength, FRCs are considerably stronger than typical cast metal alloys
used in dentistry.
➢ In clinical use, biomechanical properties of dental materials vary depending on which
application the material is utilized. For instance, in a direct fibre-reinforced resin-bonded
dental bridge, the weakest region exists across the pontic–abutment interface.
Fiber Reinforced Composites in Pediatric Dentistry
29
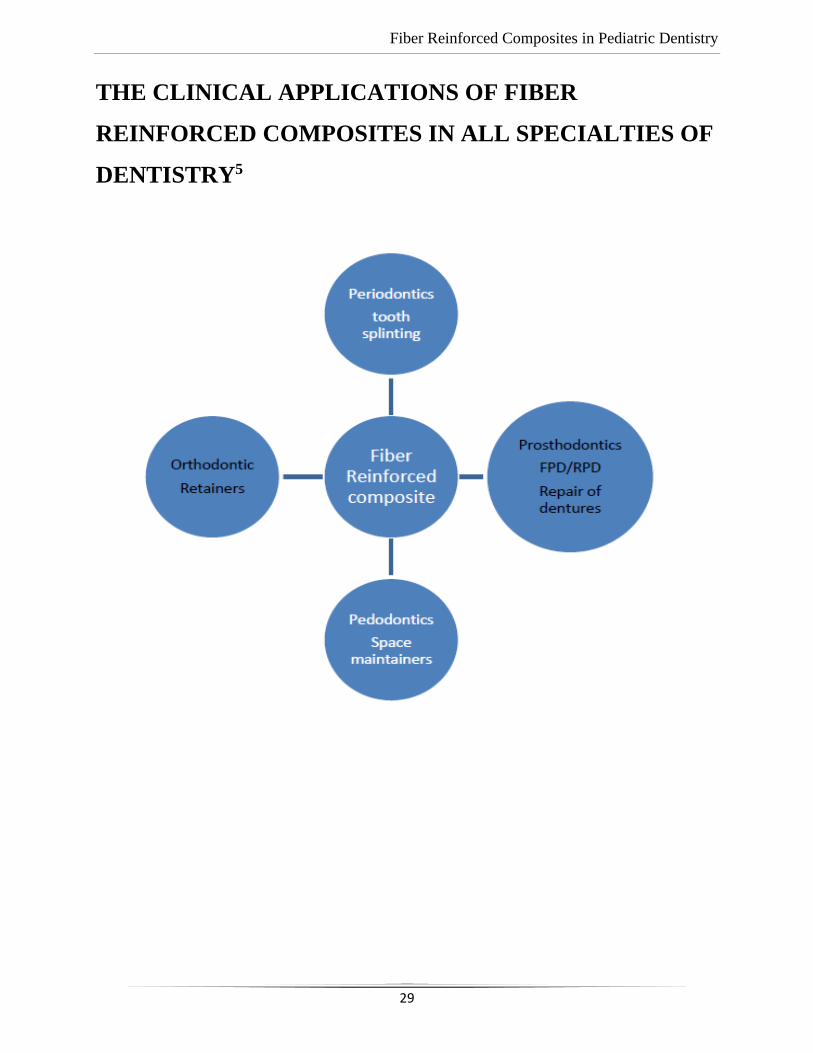
THE CLINICAL APPLICATIONS OF FIBER
REINFORCED COMPOSITES IN ALL SPECIALTIES OF
DENTISTRY5
Fiber Reinforced Composites in Pediatric Dentistry
30
VERSATILITY OF FRC IN VARIOUS DENTAL
SPECIALITIES
➢ The properties of fibre-reinforced composites (FRCs) that make them well suited for
various clinical applications include strength; desirable aesthetic characteristics; ease of
adaptability to various shapes; and potential for direct bonding to tooth structure.
Restoration:
➢ Modern adhesives successfully bond to tooth tissue in the short as shown in laboratory
reports. Adhesives that provide strong and durable bonding to the remaining sound enamel
and dentin ensures restoring teeth with minimal loss of sound tooth structure.
➢ Marginal deterioration of composite restorations remains major disadvantage in the long
term and still is the major reason to replace adhesive restorations clinically.
➢ The initial and residual polymerization stresses that are present along the cavity walls may
result in gap formation, leakage, recurrent caries and pulp irritation when resin composite
is bonded to tooth structure.
➢ Along with aesthetics, the physical properties of restorative material should also be
considered for long-lasting restoration. Fibre reinforcement has been introduced as a newer
technique with the aim of improving the physical properties of composite materials.
➢ High fracture resistance of the restorative material is required in the clinical situations
where the high impact stresses are experienced and incisal angle restoration is one such
demand.
➢ Attempts have been made to improve the fracture resistance of restoration by using
different bonding agents, adhesive resins and different restorative techniques using fibre
reinforced technique.7
Fiber Reinforced Composites in Pediatric Dentistry
31
CLINICAL APPLICATIONS IN CONSERVATIVE
DENTISTRY
➢ The applications of FRCs in conservative dentistry mainly consist of direct composite
restorations. The advantages of the use of FRCs over conventional filling materials are
related to their biomimetic properties.
➢ In fact, the dental restorations ideally would be as minimally invasive as possible and
substitute the missing hard dental tissues resembling mechanical features and properties
of natural teeth.
➢ Research has shown that the FRC substructure supports the composite restoration and acts
as a crack-prevention layer when a bilayered approach has been proposed in which lost
dentin is replaced by though short FRCs and enamel by surface layer of particulate filler
composite resin in dental restorations.
➢ In addition, FRCs have been reported to have superior physical properties and fracture
toughness compared to unreinforced composites and depth of cure and polymerization
shrinkage of FRCs have been reported to be superior to conventional resin composites.
➢ On the other hand, bilayered biomimetic technique is recommended for direct coronal
restorations of teeth with large cavities in high stress-bearing areas.7
Fiber Reinforced Composites in Pediatric Dentistry
32
CLINICAL APPLICATIONS IN ENDODONTICS
➢ The use of FRCs in endodontics is mainly reported as root canal anchoring system.
Research on both prefabricated and individualized FRC posts demonstrated that root canal
walls restored with individually formed FRC posts displayed higher fracture resistance
than those restored with only resin composite.
➢ FRC posts both used in combination with self-adhesive and glass ionomer cements showed
promising bond strength to flared root canal dentin and FRCs achieved better
performances, even in combination with bulk fill resin composite.
➢ Mechanical properties of posts significantly decreased when compared with values at
baseline after aging as shown in various studies.
➢ Special considerations should be taken while bonding of luting cement and core-built-up
composite to FRC post: only FRC post with interpenetrating polymer network containing
polymer matrix can provide reliable bonding to resin luting cements and resin based
materials in general.
➢ Generally, FRCs present limited radio-opacity due to the low concentration of radio-
opaque elements. This shortcoming of E-glass fiber would limit its application in dentistry
as sufficient radio opacity is highly desirable for dental materials.
➢ The addition of synthesized iodine containing a new methacrylate monomer HMTIB has
been tested to increase the radio opacity of FRCs with the results showing that FRCs
present higher radiopacity than natural tooth enamel.
➢ Finally, in the field of endodontics, FRCs showed excellent integration with other new
technologies such as laser applications and CAD/CAM.7
Fiber Reinforced Composites in Pediatric Dentistry
33
Endodontic Fibre Reinforced Composite Posts:
➢ FRC posts are a recent addition to the systems traditionally used to retain a core in severely
broken down, endodontically treated teeth: custom-made metal or cast posts and cores and
prefabricated metal and zirconium posts.
➢ The FRC posts offer greater flexure and fatigue strength, a modulus of elasticity close to that
of dentin, the ability to form a single bonded complex within the root canal for a unified root
post complex, and improved aesthetics when used with all-ceramic or FRC crowns as
compared to custom-made cast or metal-prefabricated posts.
➢ The properties of this post design have the potential to reinforce a compromised root and to
distribute stress more uniformly on loading to prevent root fracture moreover, the FRC post
will yield prior to catastrophic root failure better than will custom- made cast metal or
prefabricated metal post systems.
➢ Two categories of FRC posts are available: chair side-fabricated and prefabricated. Chair side
fabricated posts are custom designs that use polyethylene non pre-impregnated woven fibres
(Ribbond, Connect) or glass fibres (Glass Span) to reinforce the root and hold a composite
core.
➢ Prefabricated posts are constructed of two kinds of fibre: carbon fibres embedded in an epoxy
matrix (C-Post, U-M CPost, and Aestheti-Post) and S-type glass fibres embedded in a filled
resin matrix (FibreKor Post).
➢ Fibre-reinforced composite posts consist of a resin matrix, in which structural reinforcing
carbon fibres or quartz/glass fibres are embedded.
➢ Black carbon fibre-reinforced composite posts are, on the one hand, poorly suited for
combination with translucent full ceramic restorations due to their unfavourable optical
properties. On the other hand, carbon fibre posts also have unfavourable biomechanical
properties.7
Fiber Reinforced Composites in Pediatric Dentistry
34
CLINICAL APPLICATIONS IN PROSTHODONTICS
• The main application of FRCs in dentistry is related to provisional or definitive prosthodontics.
By using FRCs, FDPs and veneers can be realized in a minimal invasive fashion, utilizing
combinations of various kinds of adhering and retentive elements.
• A resin bonded FRC prosthesis may contain inlays/onlays, surface bonding wings, and
crowns. Direct and indirect frameworks can be made also immediately after extraction of tooth
[Cramer et al., 2011].
• FRC FDPs could be fabricated as surface-retained, inlay-retained, or full coverage crown
retained prostheses.
• The fabrication could be realized directly in the mouth or can include prefabricated pontics,
simplifying the fabrication technique and providing more predictable outcomes.
The results of mechanical and adhesion properties of FRC frameworks appear to be
encouraging. In addition, FRCs can be used in the repair of existing conventional prosthetic
devices. Repairs of veneers of porcelain-fused-to-metal restorations with resin composite veneers
can be made using woven glass fiber reinforcement, thus increasing the strength of the repair. In
addition, removable devices could be reinforced using FRCs. Finally, FRCs can be used in indirect
pontic fabrication, also in combination with CAD/CAM based technologies.7
Conservative treatment of missing tooth replacement:
• Chair side tooth replacement is an excellent application for fibre reinforcement composite
technology. 2
• Previous attempts at chair side tooth replacement involved the use of pontics derived from
extracted teeth, acrylic resin denture teeth with or without lingual wire reinforcement, and resin
composite.
• These were attached to abutment teeth with acid-etched bonded particulate composite. The
abutment teeth used for these approaches were usually not prepared; most often, tooth
replacement was only for the anterior region and the procedure was considered a short-term
solution.
Fiber Reinforced Composites in Pediatric Dentistry
35
• The chair side fibre reinforced composite prosthesis offers a fast, minimally invasive approach
for tooth replacement that combines all of the benefits of the fibre reinforced composite
material for an esthetic, functional, and potentially durable result.
• A denture tooth or a natural tooth (in the case of an extraction of a periodontally involved
incisor) can be used as the pontic.
Selection criteria for this tooth replacement approach include:
1. A patient who desires an immediate, minimally invasive approach
2. A patient who requires an extraction in an esthetic area and desires an immediate replacement
3. Abutment teeth with a questionable long term prognosis
4. Anterior disarticulation during mandibular protrusive movements
5. A non-bruxing patient
6. Cost considerations 2
Repair of Acrylic Resin Prosthesis
• Both unidirectional and woven light-polymerized FRC strips can be used effectively for chair
side repairs of fractured acrylic resin prostheses. As mentioned earlier, FibreKor (Jeneric/
Pentron) and Vectris (Ivoclar/ Williams) are unidirectional materials available for laboratory
use.
• Splint-It (Jeneric/Pentron), another chairside material, is available either as a unidirectional or
a woven fibre. All of these materials have significantly greater flexural properties than
unreinforced resin.
• Woven FRC has a shorter memory than unidirectional FRC, which makes it easier to handle;
however, unidirectional FRC has superior flexural properties and will likely provide a stronger
repair.
Fiber Reinforced Composites in Pediatric Dentistry
36
Indications for Chair side Repairs with Light-polymerized FRC
Virtually any acrylic resin prosthesis or appliance can be repaired with light-polymerized FRC:
1. Complete dentures
2. Acrylic bases of partial dentures
3. Provisional removable partial dentures
4. Provisional FPDs
5. Obturators
6. Palatal lift appliances
7. Orthodontic retainers
8. Occlusal splints and night guards4
CLINICAL APPLICATIONS IN PERIODONTOLOGY
➢ Periodontal or posttraumatic FRC splints have been reported in clinical periodontology. Splints
are used to stabilize teeth, which have become loose as a result of supporting bone loss as a
consequence of periodontal disease.
➢ The main advantage of stabilization splints is the reduction of tooth mobility. FRC periodontal
or posttraumatic splints have been reported to have reliable long term stability.
➢ In fact, fiber reinforced frameworks showed higher flexural forces when compared with
conventional metallic wires.
➢ Moreover, FRC splints showed high flexural resistance also when polymerized directly with
polymerization lamp without laboratory oven post polymerization, thus reducing the number
of clinical steps and number of appointments for the patients.
➢ The common failure types are debonding and fractures. In fact, the splinting with FRC
materials of periodontally compromised teeth that have different mobility grade is prone to
debonding, with the mobility grade as main causative factor.
➢ However, FRC splints can be easily repaired, so in many cases it is not necessary to completely
debond the framework with the substitution with a new one.7
Fiber Reinforced Composites in Pediatric Dentistry
37
Tooth Stabilization and Splints:
➢ Fibre reinforced composite materials are an excellent choice for the stabilization of mobile
teeth due to periodontal reason or due to any trauma.
➢ Chair side-fabricated fixed splints have previously been made from material combinations that
have included resin composites, wire, wire mesh, wire embedded in amalgam and resin and
fibre mesh embedded in composite.
➢ All of these materials suffered from various problems like Poor handling characteristics, Over
bulking ,Insufficient bonding of the internal structural materials to the dental resins, Poor
esthetic outcome, Fibre splints overcome these drawbacks and provide ease in tooth splinting.
Splinting can be done on palatal/lingual surfaces, labial surface or both the surfaces.4
CLINICAL APPLICATIONS IN ORTHODONTICS
➢ The main use of FRCs in clinical orthodontics is as fixed retention. After orthodontic treatment,
the need for maintaining the teeth in correct position is crucial for long term stability of clinical
results.
➢ These bonded retainers appear to be both relatively independent of patient cooperation and
well accepted by patients.
➢ Bond strength is reported to be sufficient both on enamel and on dentin. Clinical reliability is
also reported to be successful for moderate time.
➢ A great advantage of FRC splints over conventional metallic retention is aesthetics. Fibers are
barely invisible and do not affect the translucency of teeth [Karaman et al., 2002]. This aspect
is important, considering the higher number of adult patients who request an orthodontic
therapy.
➢ Finally, FRCs are metal-free and are indicated for adult and young patients screened by
Nuclear Magnetic Resonance or in subjects allergic to metals. On the other hand, FRC splints
are more rigid than conventional metallic splints, thus leading to a higher ankyloses risk of
teeth involved.
Fiber Reinforced Composites in Pediatric Dentistry
38
➢ However, the application of FRC with a spot-bonding technique has been proposed, in order
to reduce framework rigidity, thus allowing physiologic tooth movement.
➢ Clinical success of FRC resins has been reported also for space maintainer purpose. The early
loss of deciduous molars is a frequently encountered problem in dentistry and, if untreated, it
could evolve in various orthodontic problems. Space maintainers are developed to prevent the
loss of the space.
➢ FRC space maintainers can be prepared on plaster models of patients and fixed directly to the
adjacent teeth. In addition to stabilization uses, in orthodontics, FRCs have been proposed also
for active tooth movement. 4
➢ Groups of two or more teeth can be splinted with FRCs and moved “en masse” with sectional
mechanics. One other application of FRCs has been proposed as innovative materials for
fabrication of brackets and wires; yet only a few research papers have been conducted on the
topic.
Applications of fibre reinforced composite in orthodontic practice
1. Fixed orthodontic retention appliance
2. Fixed space maintainer
3. Temporary esthetic retention appliance
4. Posttraumatic stabilization splint 7
Fiber Reinforced Composites in Pediatric Dentistry
39
CLINICAL APPLICATIONS IN ORAL AND
MAXILLOFACIAL SURGERY
➢ The use of FRCs has been recently reported also in oral and maxillofacial surgery. These
materials can be applied in oral implantology for bone replacing and bone anchoring
implants.
➢ The rationale for this application is that, although metal implants have successfully been
used for decades, devices made out of metals do not meet all clinical requirements.
➢ Metal objects may interfere with some medical imaging systems, while their stiffness also
differs from natural bone and may cause stress shielding and overloading of bone.
➢ Glass fibers are responsible for the load-bearing capacity of the implant, while the
dissolution of bioactive glass particles supports bone bonding and provides antimicrobial
properties for the implant.
➢ Moreover, FRCs materials can be used in maxillofacial discipline for orbital floor implants,
cranioplasty implants, and craniofacial bone reconstruction.7
Fiber Reinforced Composites in Pediatric Dentistry
40
CLINICAL APPLICATIONS IN PAEDIATRIC
DENTISTRY
➢ In paediatric dentistry FRCs can be used in almost all the fields as described above:
restorations, space maintainers, splints, or other frameworks. The main difference is that
the enamel of primary teeth is significantly different compared to permanent enamel.
➢ The differences have been mainly detected in composition, mechanical characteristics,
bond strength, and clinical performance. However, the FRC devices used in paediatric
dentistry showed acceptable clinical performance, durability, and ease of use.7
CLINICAL USE OF DENTAL FRCS AS FILLING RESIN
COMPOSITES (POSTERIOR BULK FILLING
MATERIAL)
➢ Although amalgam has shown its many benefits as dental restorative material its use is
ending due to environmental reasons. Direct resin composite restorations are used used
for the treatment of damaged tooth structure allowing high cost-effect ratio for the
treatment outcome.
➢ Particulate filler resin composites have fulfilled direct application requirements in terms
of material cost but often failed in terms of longevity of restorations made by general
practitioners.
➢ One reason for the limited longevity of restorations is low mechanical strength of the
particulate filler resin composite as material and inadequately adjusted occlusion, which
can cause high local stress concentrations and damage the restoration.
➢ Resin composite restorations and ceramic restorations do not become adjusted to the
occlusion like amalgam restorations did during long lasting setting reaction. Occlusal
Fiber Reinforced Composites in Pediatric Dentistry
41
adjustments of the resin composite and ceramic restorations must be made by the dentist
with high precision.
➢ Utilization of reinforcing fibers in filling composites to toughen the material has been
tested for years but not until recently, the reinforcing effect by fibers has been proved.
➢ Reasons for the poor success of previous FRC filling materials have been of selecting of
too short discontinuous fibers, which were not even in theory able to increase strength
and toughness of the resin composite.
➢ The current concept of using FRC in fillings is based on the bilayered composite system
in which FRC base is made of discontinous fibers with length of the fibers exceeding the
critical fiber length in the dimethacrylate polymer matrix.
➢ Fibers in the FRC increase toughness and other physical properties of the material
compared to regular filling composites.
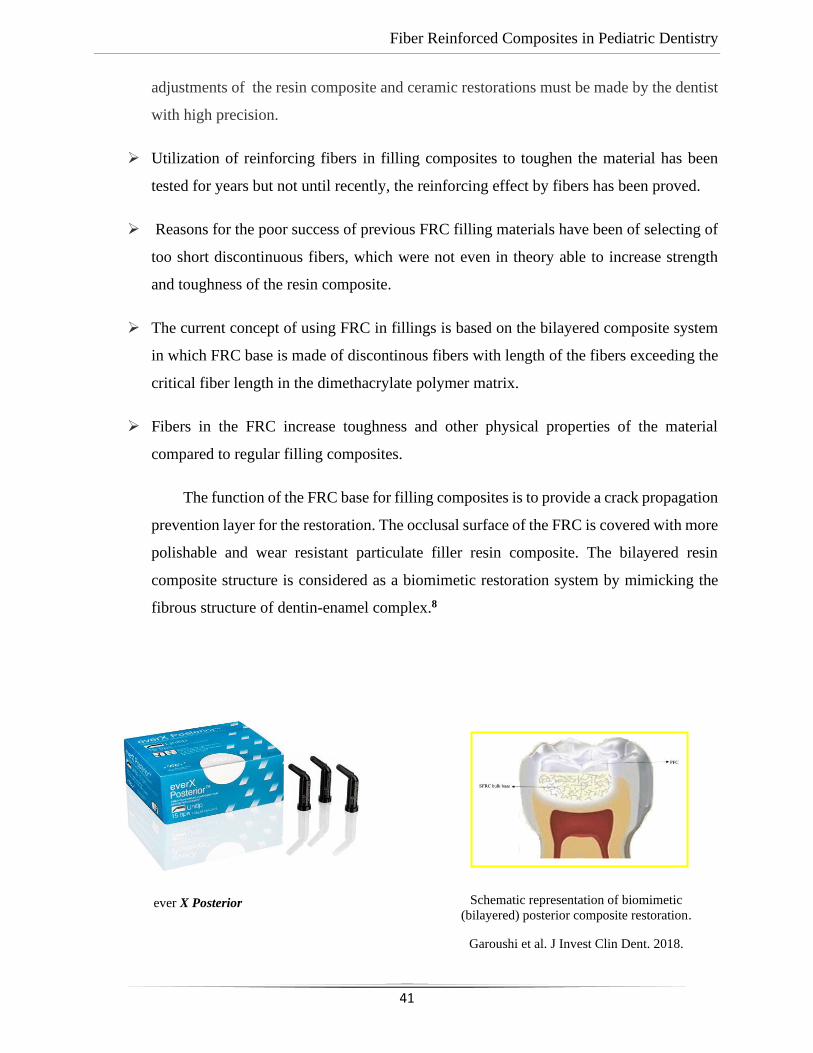
The function of the FRC base for filling composites is to provide a crack propagation
prevention layer for the restoration. The occlusal surface of the FRC is covered with more
polishable and wear resistant particulate filler resin composite. The bilayered resin
composite structure is considered as a biomimetic restoration system by mimicking the
fibrous structure of dentin-enamel complex.8
ever X Posterior Schematic representation of biomimetic
(bilayered) posterior composite restoration.
Garoushi et al. J Invest Clin Dent. 2018.
Fiber Reinforced Composites in Pediatric Dentistry
42
➢ The failures of composite resins are due are typically due to secondary caries and bulk
fractures of the composite. These relate to the material’s properties; particulate filler
composites are prone to crack propagation and therefore have low damage tolerance,
causing bulk fractures to occur. On the other hand, particulate fillers keep the composite
isotropic in terms of its many properties, including polymerisation shrinkage.
➢ Shrinkage causes gaps between the filling and the tooth and creates a predisposition to
secondary caries. Research studies using FRCs in tooth filling applications have shown
how the structure of a restored tooth can be more biomimetic. everX Posterior is a short
fibre-reinforced composite which is used to replace tissue in damaged teeth, especially
dentine.
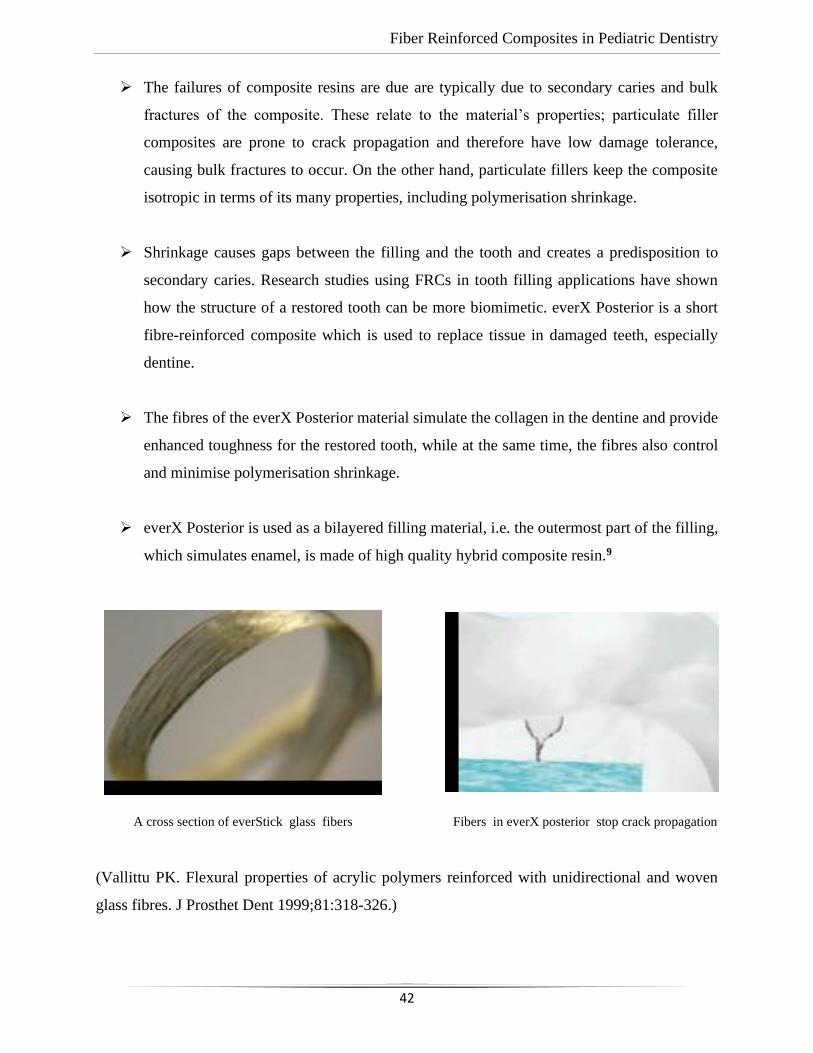
➢ The fibres of the everX Posterior material simulate the collagen in the dentine and provide
enhanced toughness for the restored tooth, while at the same time, the fibres also control
and minimise polymerisation shrinkage.
➢ everX Posterior is used as a bilayered filling material, i.e. the outermost part of the filling,
which simulates enamel, is made of high quality hybrid composite resin.9
(Vallittu PK. Flexural properties of acrylic polymers reinforced with unidirectional and woven
glass fibres. J Prosthet Dent 1999;81:318-326.)
A cross section of everStick glass fibers Fibers in everX posterior stop crack propagation
Fiber Reinforced Composites in Pediatric Dentistry
43
FIBER-REINFORCED COMPOSITE AS A POST AND
CORE MATERIAL IN A PEDIATRIC DENTISTRY
➢ Management of fractured teeth have always presented a challenge to the dentists. Today,
the predictability of root canal therapy states that it can retain almost indefinitely, even
very badly broken teeth.
➢ One of the widely accepted techniques involving restoration of extensively carious or
badly fractured teeth is the fabrication of a post and core, utilizing the root canal space for
anchorage.
➢ Thus far, the only materials that have been available to the dentists for thisprocedure have
been a variety of metallic alloys. Hard and unyielding, these metals haveto be cast in the
precise shape of the prepared canals and cemented into place.10
➢ Today, materials are available, which eliminate all the intermediate steps, and control is
rendered in the hands of the dentists, to fabricate on the chair, a resilient, esthetic and
bonded post and core. One such material is fiber reinforced composites (FRCs).
➢ A recently developed bondable reinforcement fiber, Ribbond, (Ribbond THM, Ribbond
Inc., Seattle, WA) is reported to be an alternative to conventional post materialsbecause
of its aesthetic qualities, mechanical properties, and the neutral color of the reinforcing
material.
➢ First introduced to the market in 1992, Ribbond consists of bondable, reinforced ultra-
high-strength polyethylene fibers.
➢ The open and lace like architecture of Ribbond allows it to adapt closely to the teeth and
dental arch. This is an advantage over prefabricated fiber posts where adaptability to root
canals is difficult.
Fiber Reinforced Composites in Pediatric Dentistry
44
➢ Apart from this feature the Ribbond can be condensed properly in the canals with little
microleakage. The application of a fiber layer increases the load bearing capacity of the
restoration and prevents crack propagation from the restoration to the tooth.
➢ When prefabricated fiber post is placed in flexure, cracks appear on the tensile face and
due to brittleness of the material rapidly propagates causing failure.10
STEPS INVOLVED IN THIS PROCEDURE ARE:
• The tooth should be adequately obturated and the canal space should be prepared.
• The use of Ribbond does not require additional tooth preparation as is required for metal
posts.
• Isolation of the tooth using rubber dam, high suction evacuation with cotton rolls.
• Gutta percha to be removed using gutta percha solvent until the desired length for the post
was achieved.
• The post hole shaped using gates glidden drills,cleaned with 5% sodium hypochlorite and
dried.
• The width of Ribbond (Ribbond THM, 2, 3 or 4 mm, Ribbond Inc., Seattle WA) is decided
on the root canal space available.
Radiograph showing post space
Source: Pic courtesy Acharya S. and Tandon S. srmjrds 2015
Fiber Reinforced Composites in Pediatric Dentistry
45
• The depth of the post space measured using a periodontal probe, and a 3mm wide Ribbond
cut using special scissors provided with the kit (Ribbond starter kit, Ribbond THM,
Seattle), measuring twice the depth of the post space and 3-4 times the height of the core
build-up and placed in dual cure adhesive resin and set aside in light protected container.
• The root canal wall etched for 15 s, washed for 30 s and then gently air-dried.
• Excess water removed from the post space using paper points (Spident, SPI Dental Mfg.
Inc., Korea).
• The dual cure adhesive resin (Ed Primer II A and B) applied using a microbrush in 2
consecutive coats and gently air-driedto evaporate the solvent.10
• Dual cure resin cement (Panavia F,Kuraray, Japan) is injected in the canal space.
• The Ribbond removed from the resin and the excess resin was removed using a hand
instrument, folded in a V-shape and coated with dual-curing resin cement (Panavia,
Kuraray MedicalInc., Japan).
• The piece of ribbon then placed in the postspace in a facial-lingual direction with an
endodontic plugger.
• Excess resin cement removed, and the cement cured for 20s.
• The two protruding ends of the Ribbond strips formed the reinforcement for the core build-
up to replace the lost coronal portion of the tooth.
• The remaining resin mix from the syringe extruded onto this framework to create a core
resembling almost like the shape of a lower central incisor.
• The space between the protruding ribbon ends was filled with resin so as not to leave any
voids.
Fiber Reinforced Composites in Pediatric Dentistry
46
• Composite resin should also be placed so as to cover the ribbond ends completely and leave
none of them exposed on the outer surface of the core.
• All the material thoroughly light cured to create a set surface.
• The material left in the mouth for a couple of hours to ensure complete set of the self curing
component of the resin mix.
• The result of this procedure came out to be a single piece post and core, which was bonded
onto the root, creating a solid structure without any wedging effect on the root. There were
no voids and resin conforming to the inside shape of the canal space ensured that the fitting
problems normally associated with cast posts were eliminated.10
• The bands of Ribbond reinforced the resin material and made it extremely strong and
durable.
• The restorative procedure completed by building up the tooth using dual cure hybrid
composite resin following technique of small progressive build up.
• If the development of occlusion is not completed a crown should be advised at a later stage
when occlusion development is complete.
In recent times the number of endodontic procedures have increased with extremely good results
and restoration of teeth after endodontic treatment is becoming an integral part of the restorative
practice in dentistry even when the teeth have gross lesion. Fibre-reinforced composites emerges
as a boon to the esthetic dentistry.
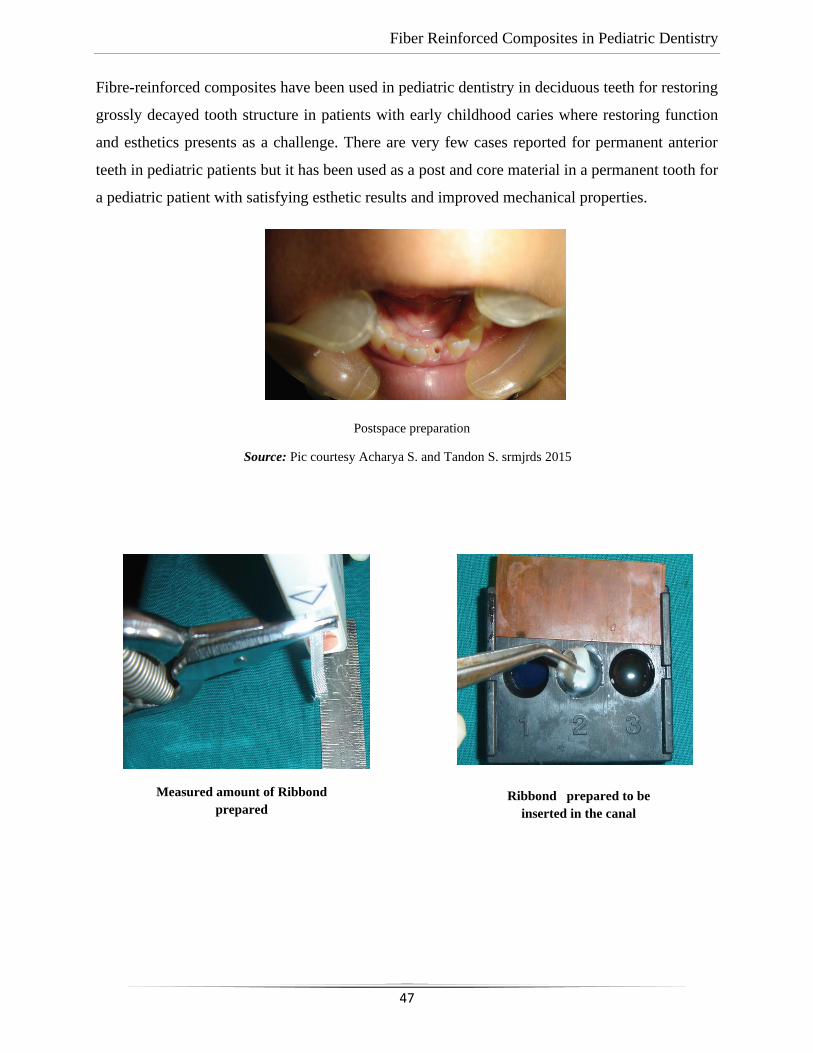
Fiber Reinforced Composites in Pediatric Dentistry
47
Fibre-reinforced composites have been used in pediatric dentistry in deciduous teeth for restoring
grossly decayed tooth structure in patients with early childhood caries where restoring function
and esthetics presents as a challenge. There are very few cases reported for permanent anterior
teeth in pediatric patients but it has been used as a post and core material in a permanent tooth for
a pediatric patient with satisfying esthetic results and improved mechanical properties.
Postspace preparation
Source: Pic courtesy Acharya S. and Tandon S. srmjrds 2015
Measured amount of Ribbond
prepared Ribbond prepared to be
inserted in the canal
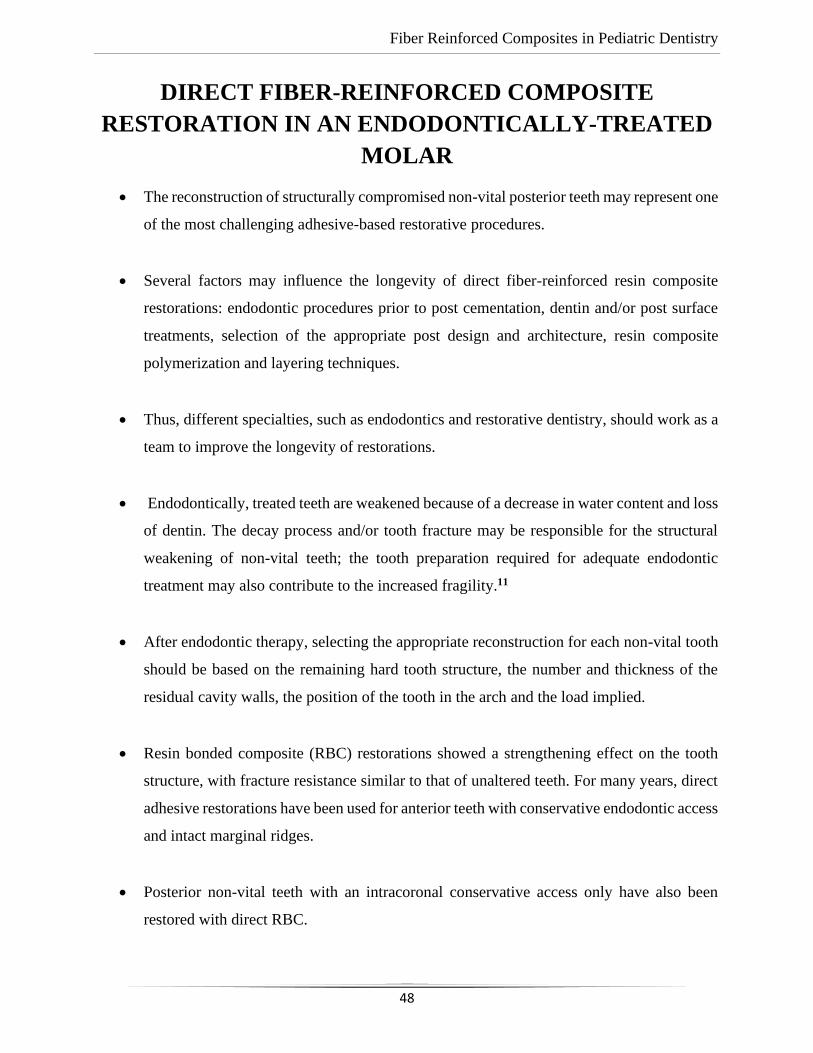
Fiber Reinforced Composites in Pediatric Dentistry
48
DIRECT FIBER-REINFORCED COMPOSITE
RESTORATION IN AN ENDODONTICALLY-TREATED
MOLAR
• The reconstruction of structurally compromised non-vital posterior teeth may represent one
of the most challenging adhesive-based restorative procedures.
• Several factors may influence the longevity of direct fiber-reinforced resin composite
restorations: endodontic procedures prior to post cementation, dentin and/or post surface
treatments, selection of the appropriate post design and architecture, resin composite
polymerization and layering techniques.
• Thus, different specialties, such as endodontics and restorative dentistry, should work as a
team to improve the longevity of restorations.
• Endodontically, treated teeth are weakened because of a decrease in water content and loss
of dentin. The decay process and/or tooth fracture may be responsible for the structural
weakening of non-vital teeth; the tooth preparation required for adequate endodontic
treatment may also contribute to the increased fragility.11
• After endodontic therapy, selecting the appropriate reconstruction for each non-vital tooth
should be based on the remaining hard tooth structure, the number and thickness of the
residual cavity walls, the position of the tooth in the arch and the load implied.
• Resin bonded composite (RBC) restorations showed a strengthening effect on the tooth
structure, with fracture resistance similar to that of unaltered teeth. For many years, direct
adhesive restorations have been used for anterior teeth with conservative endodontic access
and intact marginal ridges.
• Posterior non-vital teeth with an intracoronal conservative access only have also been
restored with direct RBC.
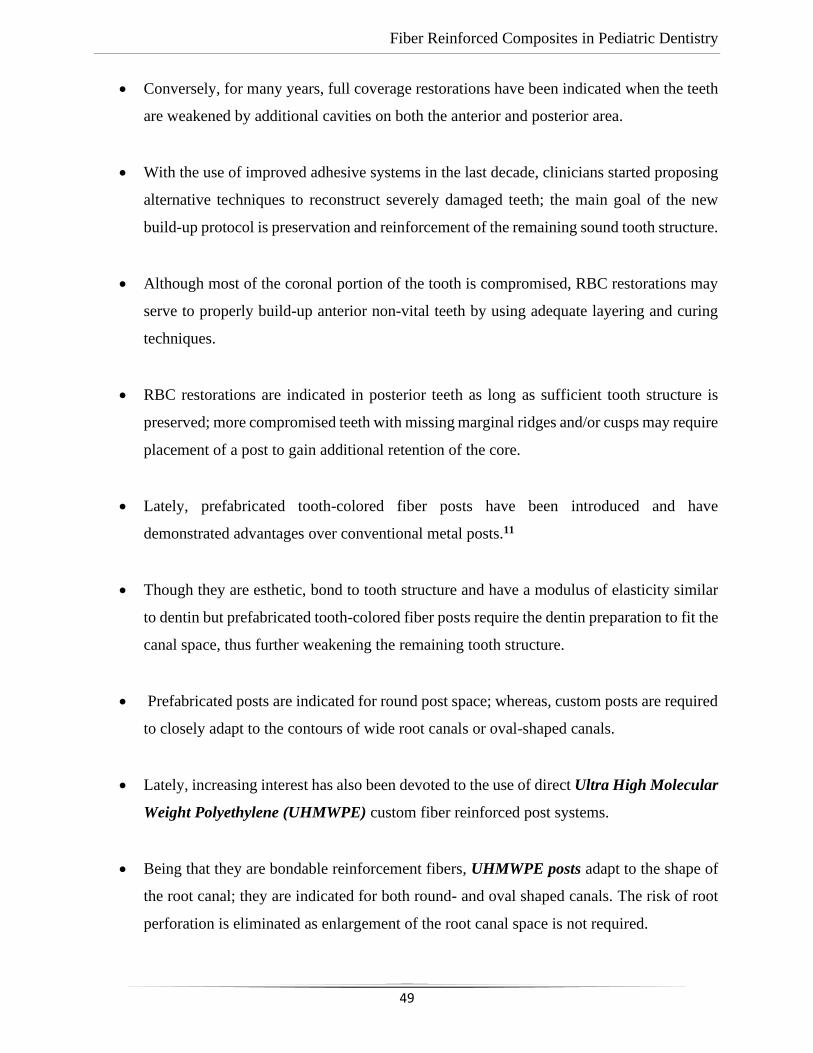
Fiber Reinforced Composites in Pediatric Dentistry
49
• Conversely, for many years, full coverage restorations have been indicated when the teeth
are weakened by additional cavities on both the anterior and posterior area.
• With the use of improved adhesive systems in the last decade, clinicians started proposing
alternative techniques to reconstruct severely damaged teeth; the main goal of the new
build-up protocol is preservation and reinforcement of the remaining sound tooth structure.
• Although most of the coronal portion of the tooth is compromised, RBC restorations may
serve to properly build-up anterior non-vital teeth by using adequate layering and curing
techniques.
• RBC restorations are indicated in posterior teeth as long as sufficient tooth structure is
preserved; more compromised teeth with missing marginal ridges and/or cusps may require
placement of a post to gain additional retention of the core.
• Lately, prefabricated tooth-colored fiber posts have been introduced and have
demonstrated advantages over conventional metal posts.11
• Though they are esthetic, bond to tooth structure and have a modulus of elasticity similar
to dentin but prefabricated tooth-colored fiber posts require the dentin preparation to fit the
canal space, thus further weakening the remaining tooth structure.
• Prefabricated posts are indicated for round post space; whereas, custom posts are required
to closely adapt to the contours of wide root canals or oval-shaped canals.
• Lately, increasing interest has also been devoted to the use of direct Ultra High Molecular
Weight Polyethylene (UHMWPE) custom fiber reinforced post systems.
• Being that they are bondable reinforcement fibers, UHMWPE posts adapt to the shape of
the root canal; they are indicated for both round- and oval shaped canals. The risk of root
perforation is eliminated as enlargement of the root canal space is not required.
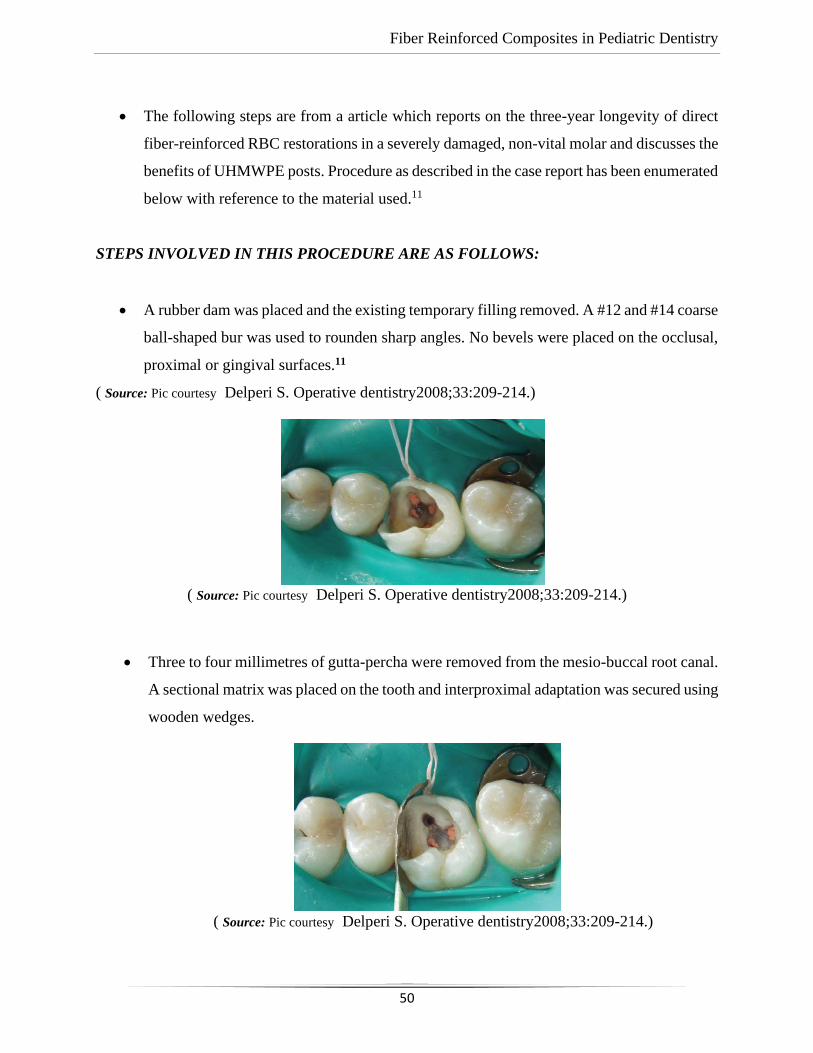
Fiber Reinforced Composites in Pediatric Dentistry
50
• The following steps are from a article which reports on the three-year longevity of direct
fiber-reinforced RBC restorations in a severely damaged, non-vital molar and discusses the
benefits of UHMWPE posts. Procedure as described in the case report has been enumerated
below with reference to the material used.11
STEPS INVOLVED IN THIS PROCEDURE ARE AS FOLLOWS:
• A rubber dam was placed and the existing temporary filling removed. A #12 and #14 coarse
ball-shaped bur was used to rounden sharp angles. No bevels were placed on the occlusal,
proximal or gingival surfaces.11
( Source: Pic courtesy Delperi S. Operative dentistry2008;33:209-214.)
( Source: Pic courtesy Delperi S. Operative dentistry2008;33:209-214.)
• Three to four millimetres of gutta-percha were removed from the mesio-buccal root canal.
A sectional matrix was placed on the tooth and interproximal adaptation was secured using
wooden wedges.
( Source: Pic courtesy Delperi S. Operative dentistry2008;33:209-214.)
Fiber Reinforced Composites in Pediatric Dentistry
51
• Enamel and dentin were etched for 30 seconds using 35% phosphoric acid; etchant was
removed, and the cavity was washed for 30 seconds with water spray, being careful to
maintain a moist surface.
( Source: Pic courtesy Delperi S. Operative dentistry2008;33:209-214.)
• A fifth generation 40% filled ethanol based adhesive system was placed in the preparation,
gently air-thinned to evaporate solvent and light cured for 20 seconds at 800 mW/cm2
from the occlusal surface using an LED curing light.
• A particular composite placement technique was selected to build-up the restoration.11 The
combination of RBC wedge-shaped increments and the UHMWPE fiber-reinforcement
system was considered to be of paramount importance to further reduce polymerization
shrinkage, better support the RBC, reinforce the remaining tooth structure and reduce total
composite volume mass An UHMWPE triaxial fiber (Ribbond) was selected, and the
dental assistant started to manipulate it according to the manufacturer’s instructions.
• Triaxial fibers were wetted with an unfilled resin, excess resin was removed andthe fibers
were completely covered with a B1 light cured flowable resin composite and placed in the
central area of the restoration.
• UHMWPE triaxial fibers were folded and each end wasplaced into the root canal using a
thin composite spatula.
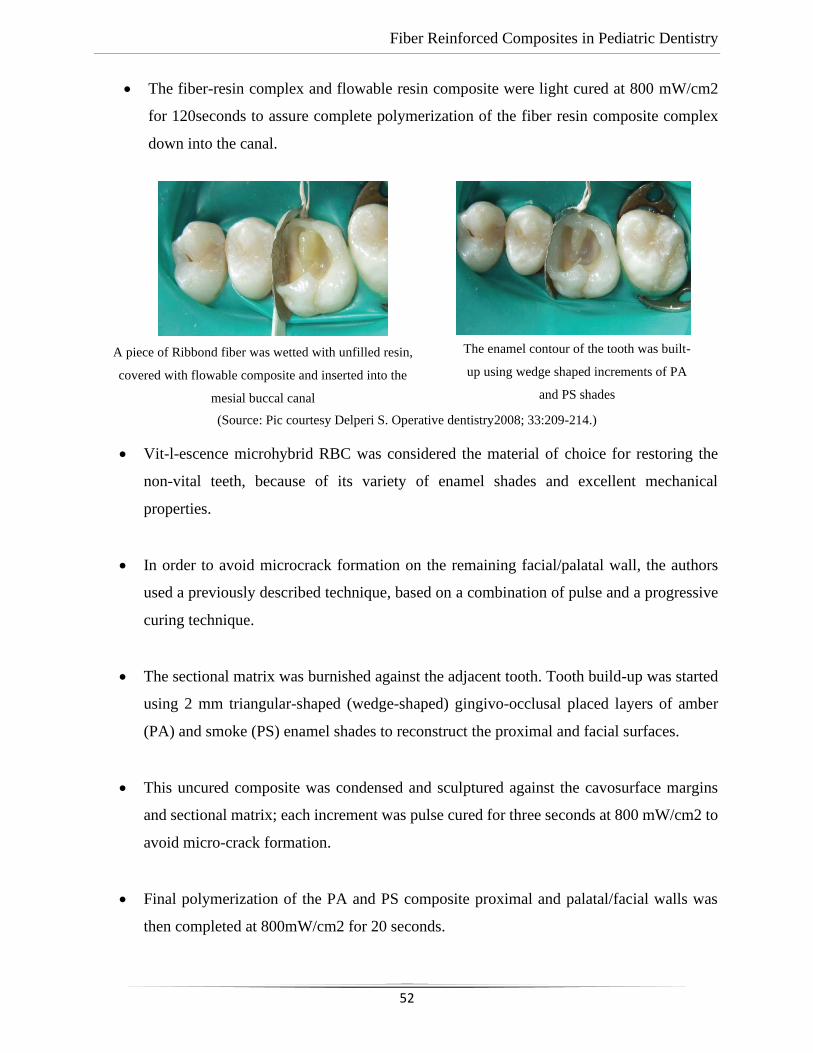
Fiber Reinforced Composites in Pediatric Dentistry
52
• The fiber-resin complex and flowable resin composite were light cured at 800 mW/cm2
for 120seconds to assure complete polymerization of the fiber resin composite complex
down into the canal.
(Source: Pic courtesy Delperi S. Operative dentistry2008; 33:209-214.)
• Vit-l-escence microhybrid RBC was considered the material of choice for restoring the
non-vital teeth, because of its variety of enamel shades and excellent mechanical
properties.
• In order to avoid microcrack formation on the remaining facial/palatal wall, the authors
used a previously described technique, based on a combination of pulse and a progressive
curing technique.
• The sectional matrix was burnished against the adjacent tooth. Tooth build-up was started
using 2 mm triangular-shaped (wedge-shaped) gingivo-occlusal placed layers of amber
(PA) and smoke (PS) enamel shades to reconstruct the proximal and facial surfaces.
• This uncured composite was condensed and sculptured against the cavosurface margins
and sectional matrix; each increment was pulse cured for three seconds at 800 mW/cm2 to
avoid micro-crack formation.
• Final polymerization of the PA and PS composite proximal and palatal/facial walls was
then completed at 800mW/cm2 for 20 seconds.
A piece of Ribbond fiber was wetted with unfilled resin,
covered with flowable composite and inserted into the
mesial buccal canal
The enamel contour of the tooth was built-
up using wedge shaped increments of PA
and PS shades
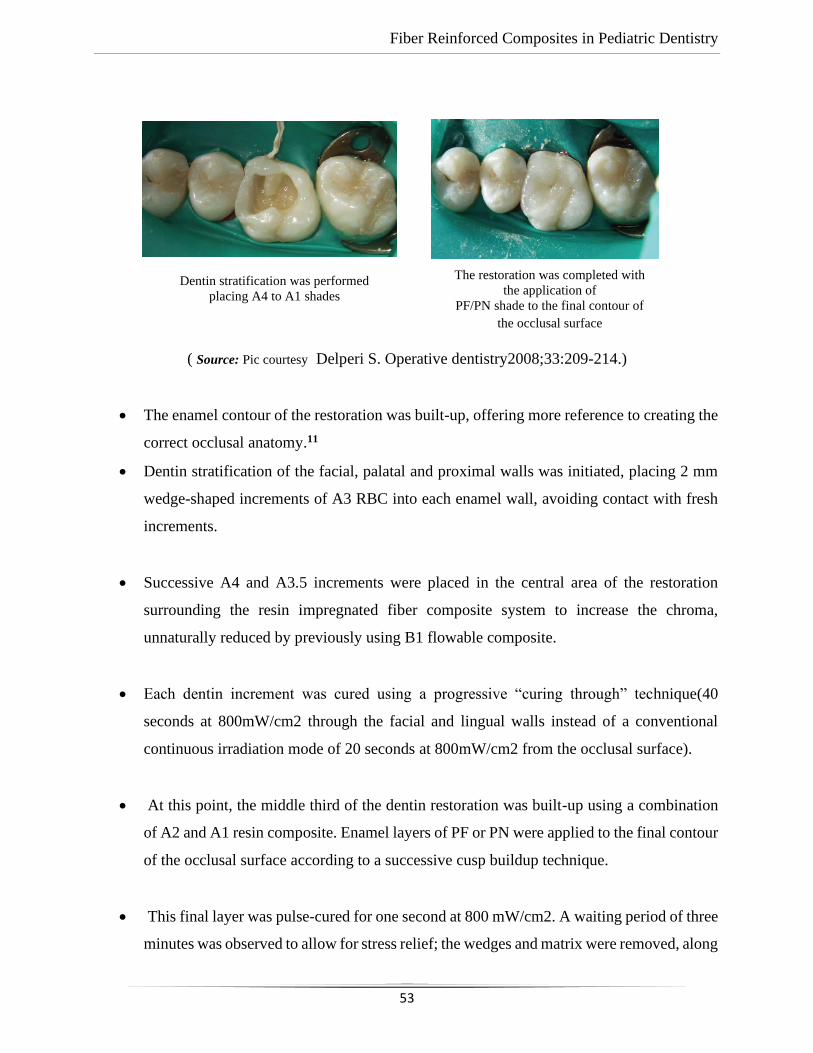
Fiber Reinforced Composites in Pediatric Dentistry
53
( Source: Pic courtesy Delperi S. Operative dentistry2008;33:209-214.)
• The enamel contour of the restoration was built-up, offering more reference to creating the
correct occlusal anatomy.11
• Dentin stratification of the facial, palatal and proximal walls was initiated, placing 2 mm
wedge-shaped increments of A3 RBC into each enamel wall, avoiding contact with fresh
increments.
• Successive A4 and A3.5 increments were placed in the central area of the restoration
surrounding the resin impregnated fiber composite system to increase the chroma,
unnaturally reduced by previously using B1 flowable composite.
• Each dentin increment was cured using a progressive “curing through” technique(40
seconds at 800mW/cm2 through the facial and lingual walls instead of a conventional
continuous irradiation mode of 20 seconds at 800mW/cm2 from the occlusal surface).
• At this point, the middle third of the dentin restoration was built-up using a combination
of A2 and A1 resin composite. Enamel layers of PF or PN were applied to the final contour
of the occlusal surface according to a successive cusp buildup technique.
• This final layer was pulse-cured for one second at 800 mW/cm2. A waiting period of three
minutes was observed to allow for stress relief; the wedges and matrix were removed, along
Dentin stratification was performed
placing A4 to A1 shades
The restoration was completed with
the application of
PF/PN shade to the final contour of
the occlusal surface
Fiber Reinforced Composites in Pediatric Dentistry
54
with the rubber dam; occlusion was checked and the restoration was finished using the
Ultradent Composite Finishing Kit.
• The final polymerization cycle was completed by irradiating the restored tooth through the
facial, palatal and occlusal surface, respectively, for 20 seconds at 800mW/cm2.
• Final polishing was performed using Jiffy polishing cups and points (Finale, Ultradent).11
The reconstruction of severely damaged non-vital teeth requires knowledge of both curing and
adhesive techniques. Fiber-reinforced resin composite restorations allow for the utilization of
conservative tooth preparation, preservation and reinforcement of sound tooth structure. Selection
of the appropriate fiber-post design and architecture is paramount to achieving this goal.
The rigidity of traditional metal posts and novel ceramic posts is a major concern, because
the rigidity may pose a risk of root fracture (Torbjörner et al 1996, Schmitter et al. 2007). A stiff
post transmits the occlusal forces to the surrounding dentin. Tension stress at the apical regions of
the post cause microscopic fatigue fractures, which, with time, may lead to macroscopic fractures
of the root.
➢ There are two ways of reducing the tension stress that causes fatigue fracture of the root.
➢ The traditional approach is prolonging the post preparation of a stiff post. This principle,
which is called the moment compensation principle, is in practice, very difficult and not
always possible to carry out.
➢ Another current approach, called the modulus compensation principle, is to use a post
material which is biomechanically more suitable, e.g. a post material which is strong
enough but also flexible so that it can behave like tooth structure inside the root under the
occlusal forces.
➢ The flexibility or stiffness of a material may be described by the so-called modulus of
elasticity or elastic modulus (Young’s modulus, E-modulus).
Fiber Reinforced Composites in Pediatric Dentistry
55
➢ The E-modulus is the constant that relates the stress and the strain in the linear elastic
region where elastic deformation of a material occurs (Gutmann 1992, Van Noort 2002).
A group of materials which offers stiffness equal to that of dentin, as well as high durability
is the group of fibre-reinforced composites (FRC).11
FIBER REINFORCED COMPOSITE- FIXED FUNCTIONAL SPACE MAINTAINERS
➢ Premature loss of the primary teeth is a common occurrence in children. A space maintainer
is the safest and effective method in preventing malocclusions pertaining to early loss of a
primary tooth and is durable and economical.
➢ Among the various space maintainers used in pediatric dentistry, band and loop is the most
commonly used fixed space maintainer.
➢ However, the construction of band and loop requires three steps, it involves a clinician as
well as a laboratory technician, and therefore it is expensive.
➢ With the advances in the technology and materials, there is a need to search for an
alternative to overcome various disadvantages of the band and loop space maintainer.
➢ Fiber-reinforced composite resin (FRCR) provides new opportunities to us in this regard.
In addition to their mechanical properties, FRCR materials are now being used in many
areas of dentistry due to their advantages, such as the possibility to be prepared by the
dentist chairside, the number of visits are decreased, adherence to teeth structures by way
of adhesive applications along with improved aesthetic properties.
➢ Fabrication of SMs with fiber reinforced composite (FRC) possesses the advantages of
being easily manipulated and directly chair-side applied. Moreover, they are fixed,
minimally invasive, aesthetic, readily repaired, reversible, biocompatible, and of relatively
lower treatment costs. However, their longevity is still a controversial issue.
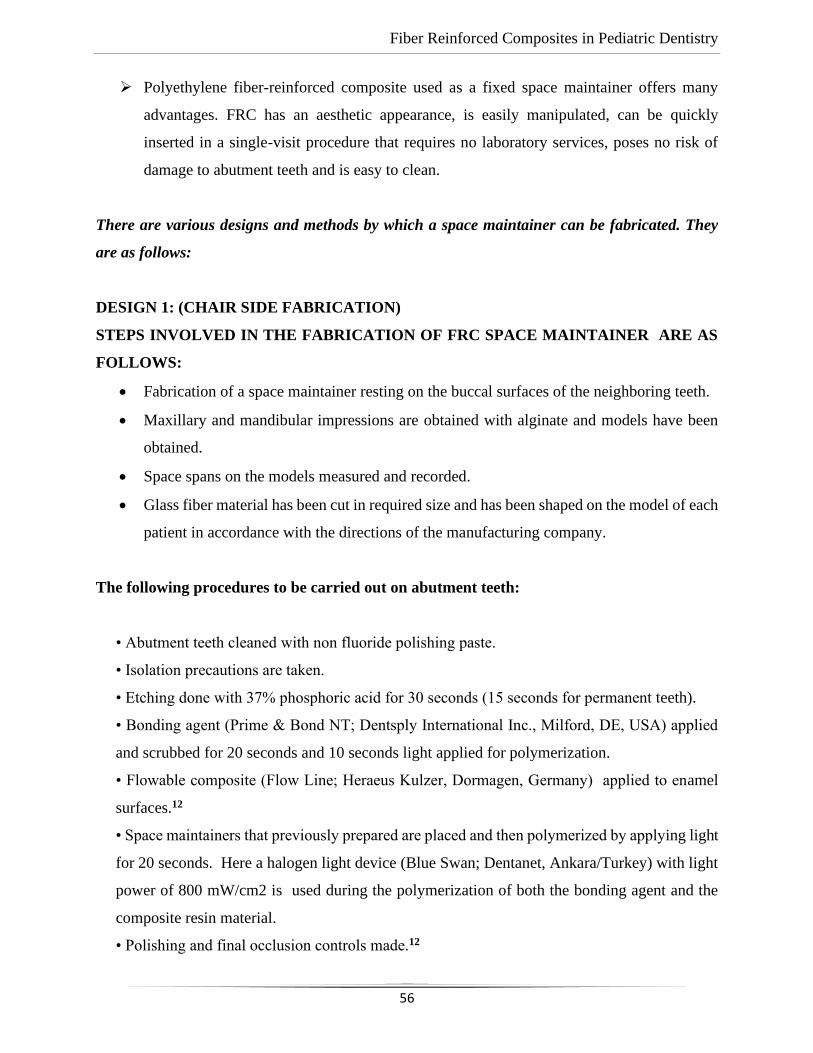
Fiber Reinforced Composites in Pediatric Dentistry
56
➢ Polyethylene fiber-reinforced composite used as a fixed space maintainer offers many
advantages. FRC has an aesthetic appearance, is easily manipulated, can be quickly
inserted in a single-visit procedure that requires no laboratory services, poses no risk of
damage to abutment teeth and is easy to clean.
There are various designs and methods by which a space maintainer can be fabricated. They
are as follows:
DESIGN 1: (CHAIR SIDE FABRICATION)
STEPS INVOLVED IN THE FABRICATION OF FRC SPACE MAINTAINER ARE AS
FOLLOWS:
• Fabrication of a space maintainer resting on the buccal surfaces of the neighboring teeth.
• Maxillary and mandibular impressions are obtained with alginate and models have been
obtained.
• Space spans on the models measured and recorded.
• Glass fiber material has been cut in required size and has been shaped on the model of each
patient in accordance with the directions of the manufacturing company.
The following procedures to be carried out on abutment teeth:
• Abutment teeth cleaned with non fluoride polishing paste.
• Isolation precautions are taken.
• Etching done with 37% phosphoric acid for 30 seconds (15 seconds for permanent teeth).
• Bonding agent (Prime & Bond NT; Dentsply International Inc., Milford, DE, USA) applied
and scrubbed for 20 seconds and 10 seconds light applied for polymerization.
• Flowable composite (Flow Line; Heraeus Kulzer, Dormagen, Germany) applied to enamel
surfaces.12
• Space maintainers that previously prepared are placed and then polymerized by applying light
for 20 seconds. Here a halogen light device (Blue Swan; Dentanet, Ankara/Turkey) with light
power of 800 mW/cm2 is used during the polymerization of both the bonding agent and the
composite resin material.
• Polishing and final occlusion controls made.12
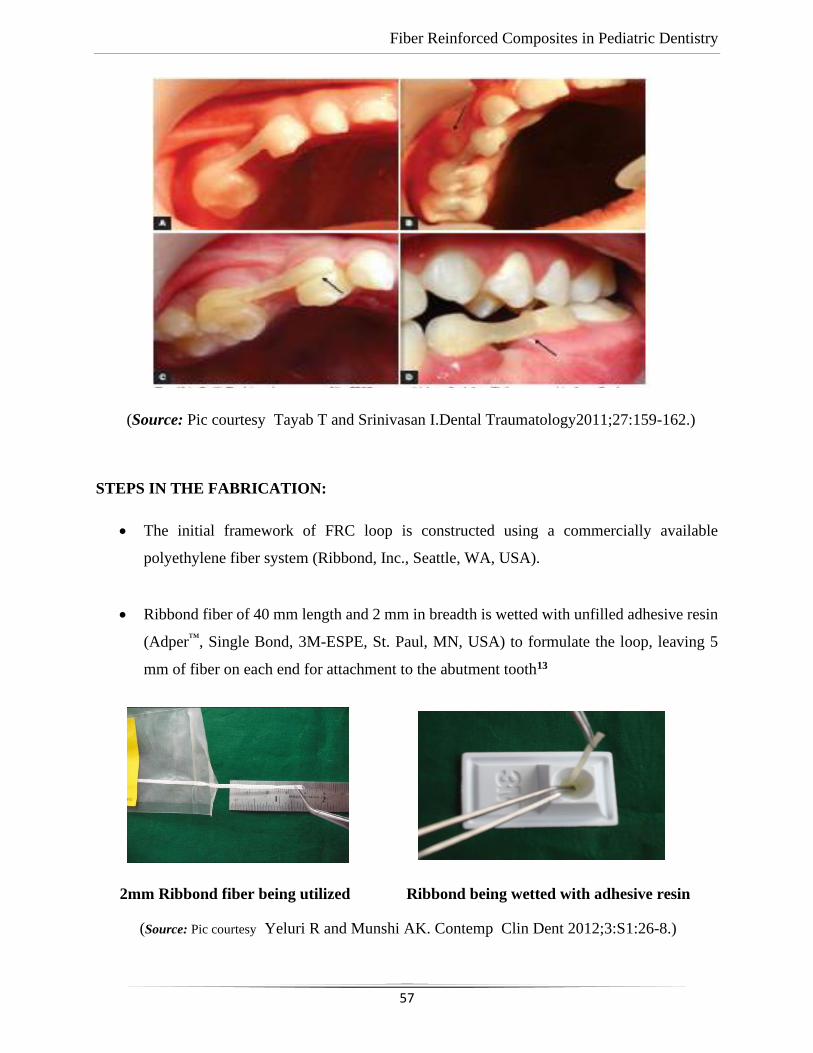
Fiber Reinforced Composites in Pediatric Dentistry
57
(Source: Pic courtesy Tayab T and Srinivasan I.Dental Traumatology2011;27:159-162.)
STEPS IN THE FABRICATION:
• The initial framework of FRC loop is constructed using a commercially available
polyethylene fiber system (Ribbond, Inc., Seattle, WA, USA).
• Ribbond fiber of 40 mm length and 2 mm in breadth is wetted with unfilled adhesive resin
(Adper™, Single Bond, 3M-ESPE, St. Paul, MN, USA) to formulate the loop, leaving 5
mm of fiber on each end for attachment to the abutment tooth13
2mm Ribbond fiber being utilized Ribbond being wetted with adhesive resin
(Source: Pic courtesy Yeluri R and Munshi AK. Contemp Clin Dent 2012;3:S1:26-8.)
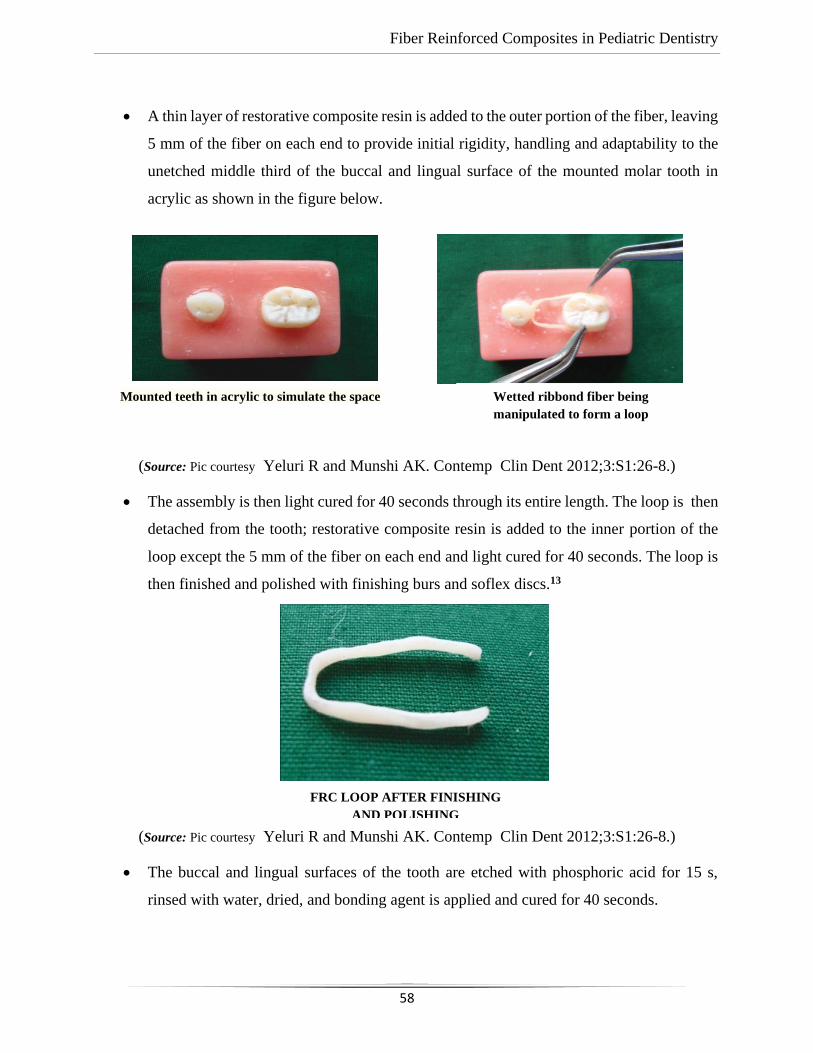
Fiber Reinforced Composites in Pediatric Dentistry
58
• A thin layer of restorative composite resin is added to the outer portion of the fiber, leaving
5 mm of the fiber on each end to provide initial rigidity, handling and adaptability to the
unetched middle third of the buccal and lingual surface of the mounted molar tooth in
acrylic as shown in the figure below.
(Source: Pic courtesy Yeluri R and Munshi AK. Contemp Clin Dent 2012;3:S1:26-8.)
• The assembly is then light cured for 40 seconds through its entire length. The loop is then
detached from the tooth; restorative composite resin is added to the inner portion of the
loop except the 5 mm of the fiber on each end and light cured for 40 seconds. The loop is
then finished and polished with finishing burs and soflex discs.13
(Source: Pic courtesy Yeluri R and Munshi AK. Contemp Clin Dent 2012;3:S1:26-8.)
• The buccal and lingual surfaces of the tooth are etched with phosphoric acid for 15 s,
rinsed with water, dried, and bonding agent is applied and cured for 40 seconds.
Mounted teeth in acrylic to simulate the space
Wetted ribbond fiber being
manipulated to form a loop
FRC LOOP AFTER FINISHING
AND POLISHING
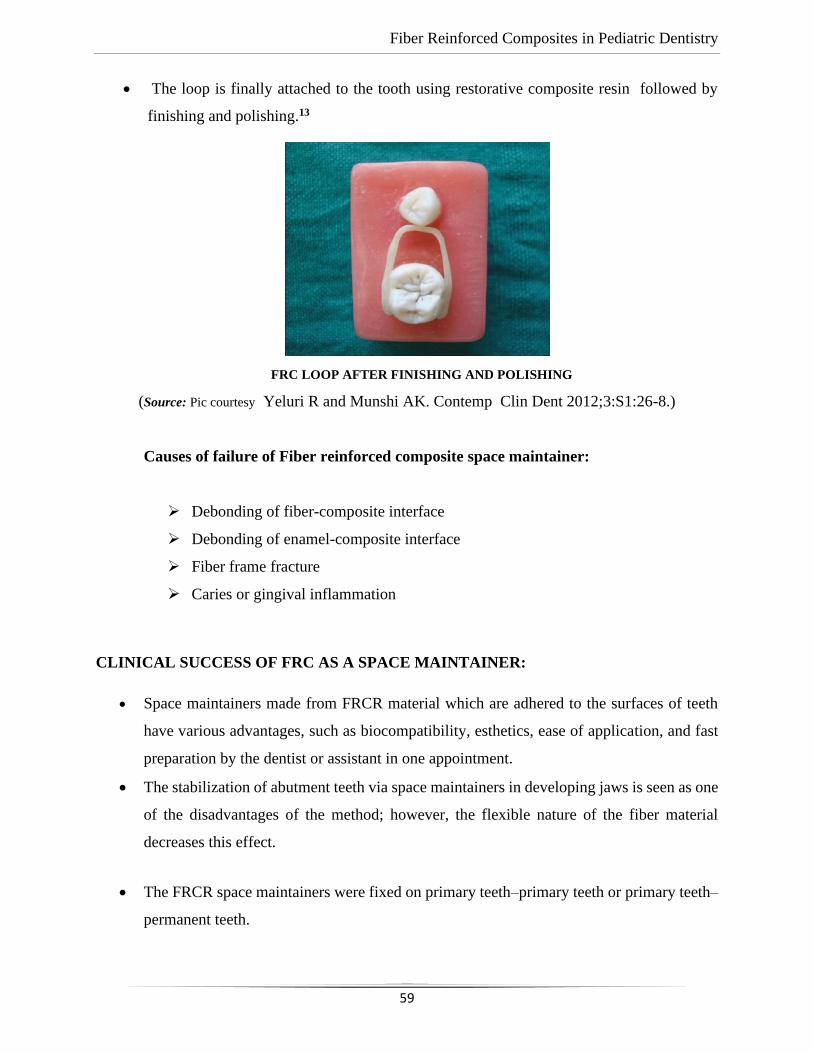
Fiber Reinforced Composites in Pediatric Dentistry
59
• The loop is finally attached to the tooth using restorative composite resin followed by
finishing and polishing.13
(Source: Pic courtesy Yeluri R and Munshi AK. Contemp Clin Dent 2012;3:S1:26-8.)
Causes of failure of Fiber reinforced composite space maintainer:
➢ Debonding of fiber-composite interface
➢ Debonding of enamel-composite interface
➢ Fiber frame fracture
➢ Caries or gingival inflammation
CLINICAL SUCCESS OF FRC AS A SPACE MAINTAINER:
• Space maintainers made from FRCR material which are adhered to the surfaces of teeth
have various advantages, such as biocompatibility, esthetics, ease of application, and fast
preparation by the dentist or assistant in one appointment.
• The stabilization of abutment teeth via space maintainers in developing jaws is seen as one
of the disadvantages of the method; however, the flexible nature of the fiber material
decreases this effect.
• The FRCR space maintainers were fixed on primary teeth–primary teeth or primary teeth–
permanent teeth.
FRC LOOP AFTER FINISHING AND POLISHING
Fiber Reinforced Composites in Pediatric Dentistry
60
• When such space maintainers are fixed on primary teeth, the prismless enamel surface
structure of primary teeth may have negative effects on the retention of resin material.
• It has been stated in previous studies that space maintainers prepared similarly using fiber
material are more stable when fixed on permanent teeth.
• Swaine and Wright have carried out a study during which they determined the failure rate
as 18% in cases when primary teeth are used as abutment and as 60% in cases when
application is made between primary and permanent teeth.
• Researchers think this is due to isolation problems in addition to the fact that
polymerization light cannot reach the back region sufficiently.
• Researchers have suggested etching at the area to where space maintainers will be applied
to decrease the external prismless layer of the enamel.14
• The failure rate of wire-composite space maintainers during the first 6 months varies
between 4 and 30%, whereas the failure rate at the end of the first 6 months in our study is
2.3%, which is quite low.
• Studies during which the retention of FRCR space maintainers was compared for 12
months with those of band-loop space maintainers have indicated the success ratios as 53
and 33% respectively.
• Baroni et al. emphasize that occlusal stresses are more important for the long-term use of
space maintainers instead of their design. Furthermore, in another study made by Kara et
al. to compare the biomechanics of space maintainers, it is found that load distributions of
band-loop, direct bonded, and fiber-reinforced space maintainers seem comparable.
• It has also been put forth that children mostly use the right side of the jaw when chewing
and hence, space maintainers fixed to the right side of the jaw experience more occlusal
stress and are thereby lost earlier.
Fiber Reinforced Composites in Pediatric Dentistry
61
• Kirzioğlu and Ertürkhave stated that the FRC space maintainers they placed to the right
side of the arc are less successful in comparison with those placed to the left side.
• It has been determined during the study carried out by Subramaniam et al. that 46% of
the space maintainers applied to the right side of the jaws are unsuccessful.
• On the contrary, Santos et al. have determined a high failure rate in the left maxilla region,
whereas Kirzioğlu and Yilmaz,Baroni et al. have determined no statistically significant
difference during their studies in which they compared wire-composite space maintainers
placed to the right and left sides of the jaw.14
• Studies in the literature carried out in this topic are generally in the form of either a case
report or the evaluation of a method. The number of studies examining the long-term
success of such space maintainers is rare.
ANTERIOR FIBER-REINFORCED RIBBON COMPOSITE RESIN BRIDGE:
• Different therapeutic options can be considered for the replacement of a congenitally or
traumatically missing permanent incisor in young children and adolescents. One of the
greatest challenges that the dentist faces is the esthetic and functional rehabilitation of a
missing anterior tooth.
• The procedure becomes difficult when the missing tooth cannot be replaced by an implant-
supported prosthesis or a conventional fixed dental prosthesis due to a local bony defect,
inadequate volume of bone in the edentulous area, occlusal function, systemic disorders,
or the socioeconomic status or unwillingness of the patient to experience invasive implant
surgery or the preparation of natural teeth for retainers.
• The fiber reinforced composite resin FPD (FRC FPD) can be considered a viable
alternative in such situations or in those in which conservative preparation is needed.
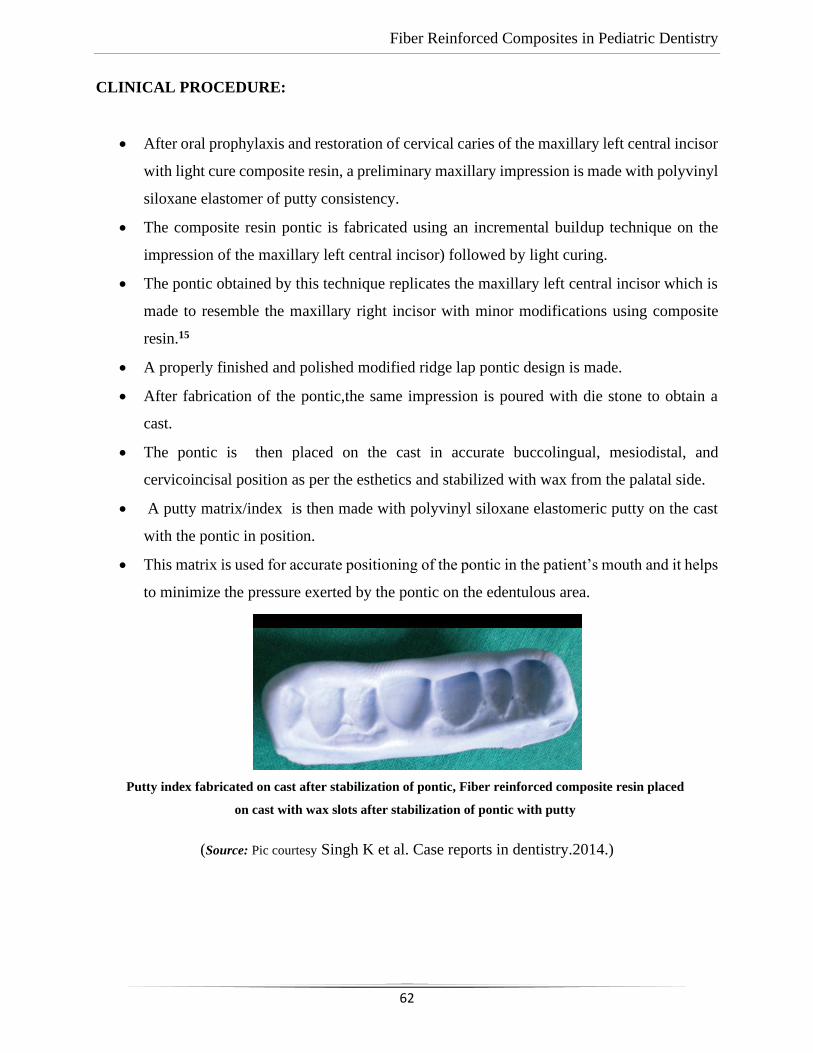
Fiber Reinforced Composites in Pediatric Dentistry
62
CLINICAL PROCEDURE:
• After oral prophylaxis and restoration of cervical caries of the maxillary left central incisor
with light cure composite resin, a preliminary maxillary impression is made with polyvinyl
siloxane elastomer of putty consistency.
• The composite resin pontic is fabricated using an incremental buildup technique on the
impression of the maxillary left central incisor) followed by light curing.
• The pontic obtained by this technique replicates the maxillary left central incisor which is
made to resemble the maxillary right incisor with minor modifications using composite
resin.15
• A properly finished and polished modified ridge lap pontic design is made.
• After fabrication of the pontic,the same impression is poured with die stone to obtain a
cast.
• The pontic is then placed on the cast in accurate buccolingual, mesiodistal, and
cervicoincisal position as per the esthetics and stabilized with wax from the palatal side.
• A putty matrix/index is then made with polyvinyl siloxane elastomeric putty on the cast
with the pontic in position.
• This matrix is used for accurate positioning of the pontic in the patient’s mouth and it helps
to minimize the pressure exerted by the pontic on the edentulous area.
(Source: Pic courtesy Singh K et al. Case reports in dentistry.2014.)
Putty index fabricated on cast after stabilization of pontic, Fiber reinforced composite resin placed
on cast with wax slots after stabilization of pontic with putty

Fiber Reinforced Composites in Pediatric Dentistry
63
• Palatal grooves, approximately 3mm wide and 1.5mm deep, involving at least three-
quarters of the mesiodistal width of the abutments, were prepared with round and inverted
cone diamond rotary burs, in the patient’s mouth.15
(Source: Pic courtesy Singh K et al. Case reports in dentistry.2014.)
• A similar size groove involving the whole of mesiodistal width of the pontic was prepared
on the pontic.
• The grooves prepared on abutments and pontic should be at the same level.The distance
between the grooves was measured and a piece of the fiber ribbon (Perfect Splint, Hager
Werken, Germany) is cut with the same dimensions as the space between two grooves.
• The bonding agent is applied on the cut piece of fiber ribbon and kept aside.
• The fiber impregnated with bonding agent should be kept out of the dental light until used.
• One should avoid touching the fiber ribbon after it is wetted with bonding agent via the
fingers, because any contact can contaminate its reactive surface layer.
• The prepared slots and mesioproximal surfaces of both the abutments were then etched
with 37% phosphoric acid for 15 seconds.
• After thoroughly rinsing and drying, a bonding agent was applied with amicrobrush
applicator on both the prepared abutment areas and on the groove on the pontic.
• Excess bonding agent was removed with the brush tip and by gently blowing with air. The
bonding agent was light cured for 15 seconds.15
• The pontic was then placed in the patient’s mouth and held in accurate position with the
putty index.
Slots prepared at palatal surface of abutments
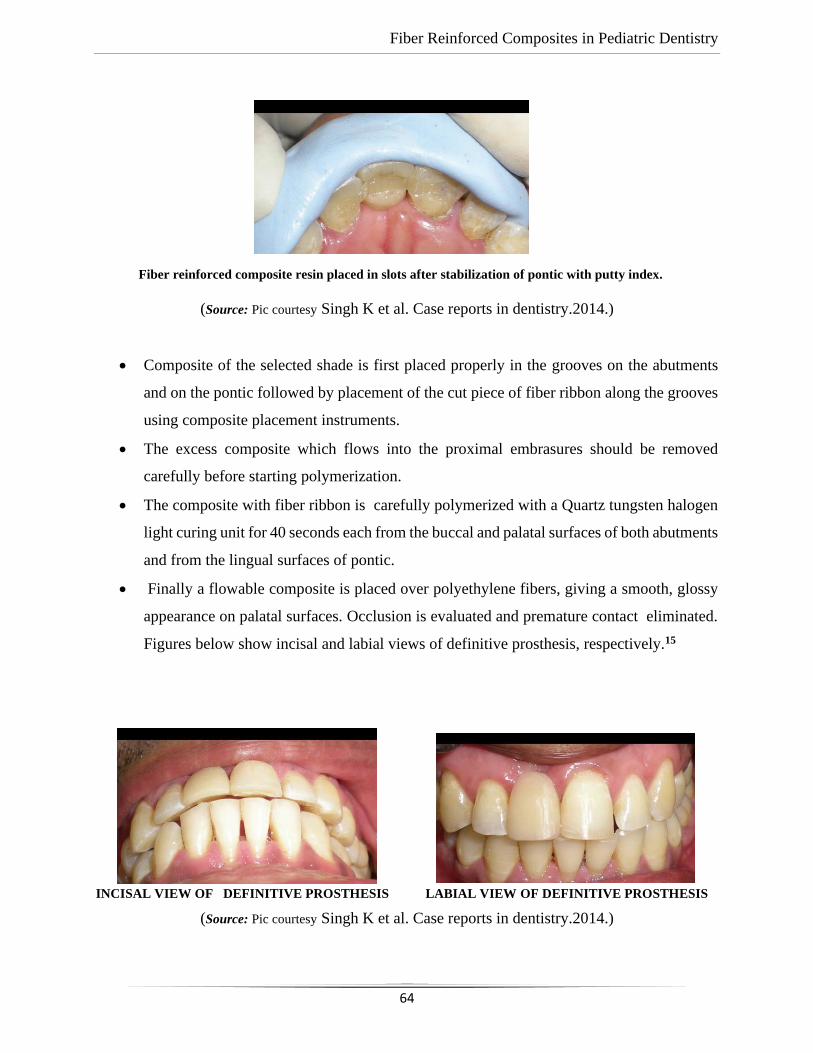
Fiber Reinforced Composites in Pediatric Dentistry
64
(Source: Pic courtesy Singh K et al. Case reports in dentistry.2014.)
• Composite of the selected shade is first placed properly in the grooves on the abutments
and on the pontic followed by placement of the cut piece of fiber ribbon along the grooves
using composite placement instruments.
• The excess composite which flows into the proximal embrasures should be removed
carefully before starting polymerization.
• The composite with fiber ribbon is carefully polymerized with a Quartz tungsten halogen
light curing unit for 40 seconds each from the buccal and palatal surfaces of both abutments
and from the lingual surfaces of pontic.
• Finally a flowable composite is placed over polyethylene fibers, giving a smooth, glossy
appearance on palatal surfaces. Occlusion is evaluated and premature contact eliminated.
Figures below show incisal and labial views of definitive prosthesis, respectively.15
INCISAL VIEW OF DEFINITIVE PROSTHESIS LABIAL VIEW OF DEFINITIVE PROSTHESIS
(Source: Pic courtesy Singh K et al. Case reports in dentistry.2014.)
Fiber reinforced composite resin placed in slots after stabilization of pontic with putty index.
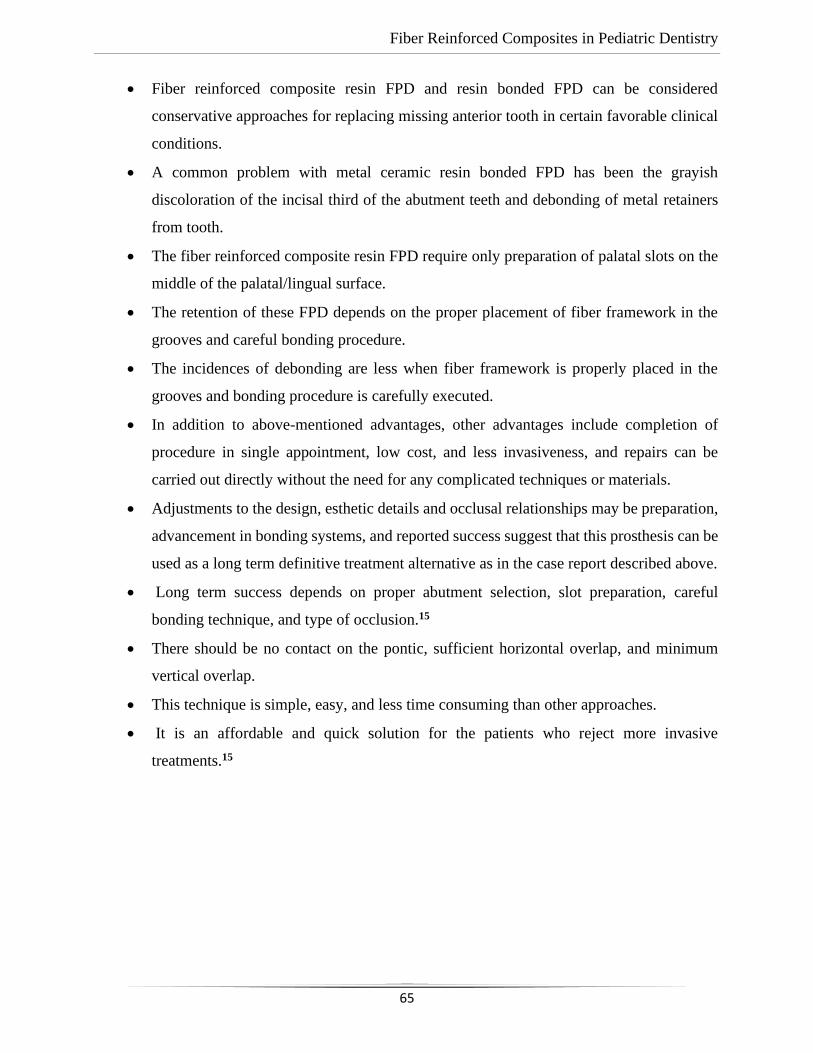
Fiber Reinforced Composites in Pediatric Dentistry
65
• Fiber reinforced composite resin FPD and resin bonded FPD can be considered
conservative approaches for replacing missing anterior tooth in certain favorable clinical
conditions.
• A common problem with metal ceramic resin bonded FPD has been the grayish
discoloration of the incisal third of the abutment teeth and debonding of metal retainers
from tooth.
• The fiber reinforced composite resin FPD require only preparation of palatal slots on the
middle of the palatal/lingual surface.
• The retention of these FPD depends on the proper placement of fiber framework in the
grooves and careful bonding procedure.
• The incidences of debonding are less when fiber framework is properly placed in the
grooves and bonding procedure is carefully executed.
• In addition to above-mentioned advantages, other advantages include completion of
procedure in single appointment, low cost, and less invasiveness, and repairs can be
carried out directly without the need for any complicated techniques or materials.
• Adjustments to the design, esthetic details and occlusal relationships may be preparation,
advancement in bonding systems, and reported success suggest that this prosthesis can be
used as a long term definitive treatment alternative as in the case report described above.
• Long term success depends on proper abutment selection, slot preparation, careful
bonding technique, and type of occlusion.15
• There should be no contact on the pontic, sufficient horizontal overlap, and minimum
vertical overlap.
• This technique is simple, easy, and less time consuming than other approaches.
• It is an affordable and quick solution for the patients who reject more invasive
treatments.15
Fiber Reinforced Composites in Pediatric Dentistry
66
USE OF FRC IN DENTAL TRAUMA:
➢ FRCs can be used for splinting in case of trauma to primary or permanent teeth.
➢ Clinical steps in splinting are as follows:
• The labial surfaces of the teeth to be etched, rinsed and dried, and Single Bond applied.
• To insure semi-rigidity, the interproximal region is not etched or bonded.
• After applying a flowable composite to the enamel surfaces, the Ribbond is pressed through
thecomposite against the teeth and cured.
• The Ribbond is then coated with additional flowablecomposite and cured again for 20 s.17
(Source: Pic courtesy Tuloglu N, Bayeak S and Tunc E. European journal of dentistry2009;3.)
• Two weeks later, the Ribbond splint at the interproximals is cut with a diamond bur. Then,
the splint is removed from the abutment by sliding a scalpel blade between the Ribbond
and the teeth on the most distal end.
• The remaining adhesive is then removed with a tungsten carbide bur (KometH284;
Brasseler Co., Lemgo, Germany) in a lowspeedhandpiece under coolant water and surfaces
are polished with disks.17
(A). Frontal view after stabilization with a Ribbond-composite splint.
(B). Frontal view after healing.
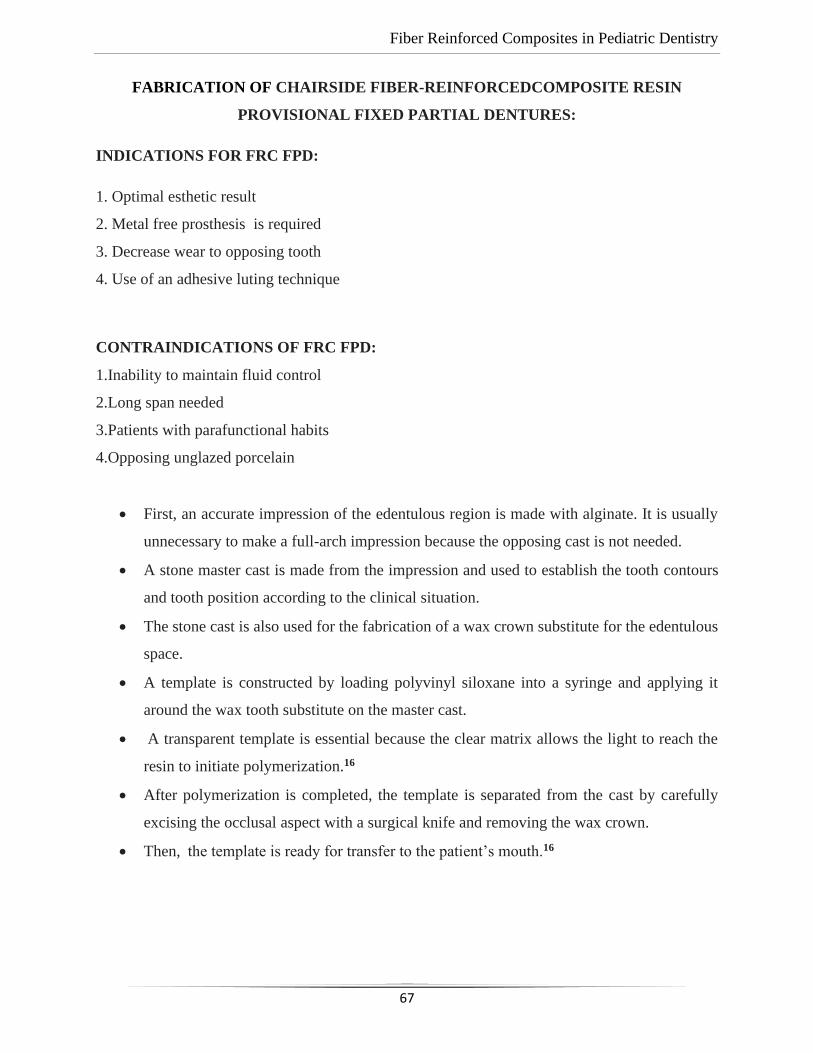
Fiber Reinforced Composites in Pediatric Dentistry
67
FABRICATION OF CHAIRSIDE FIBER-REINFORCEDCOMPOSITE RESIN
PROVISIONAL FIXED PARTIAL DENTURES:
INDICATIONS FOR FRC FPD:
1. Optimal esthetic result
2. Metal free prosthesis is required
3. Decrease wear to opposing tooth
4. Use of an adhesive luting technique
CONTRAINDICATIONS OF FRC FPD:
1.Inability to maintain fluid control
2.Long span needed
3.Patients with parafunctional habits
4.Opposing unglazed porcelain
• First, an accurate impression of the edentulous region is made with alginate. It is usually
unnecessary to make a full-arch impression because the opposing cast is not needed.
• A stone master cast is made from the impression and used to establish the tooth contours
and tooth position according to the clinical situation.
• The stone cast is also used for the fabrication of a wax crown substitute for the edentulous
space.
• A template is constructed by loading polyvinyl siloxane into a syringe and applying it
around the wax tooth substitute on the master cast.
• A transparent template is essential because the clear matrix allows the light to reach the
resin to initiate polymerization.16
• After polymerization is completed, the template is separated from the cast by carefully
excising the occlusal aspect with a surgical knife and removing the wax crown.
• Then, the template is ready for transfer to the patient’s mouth.16
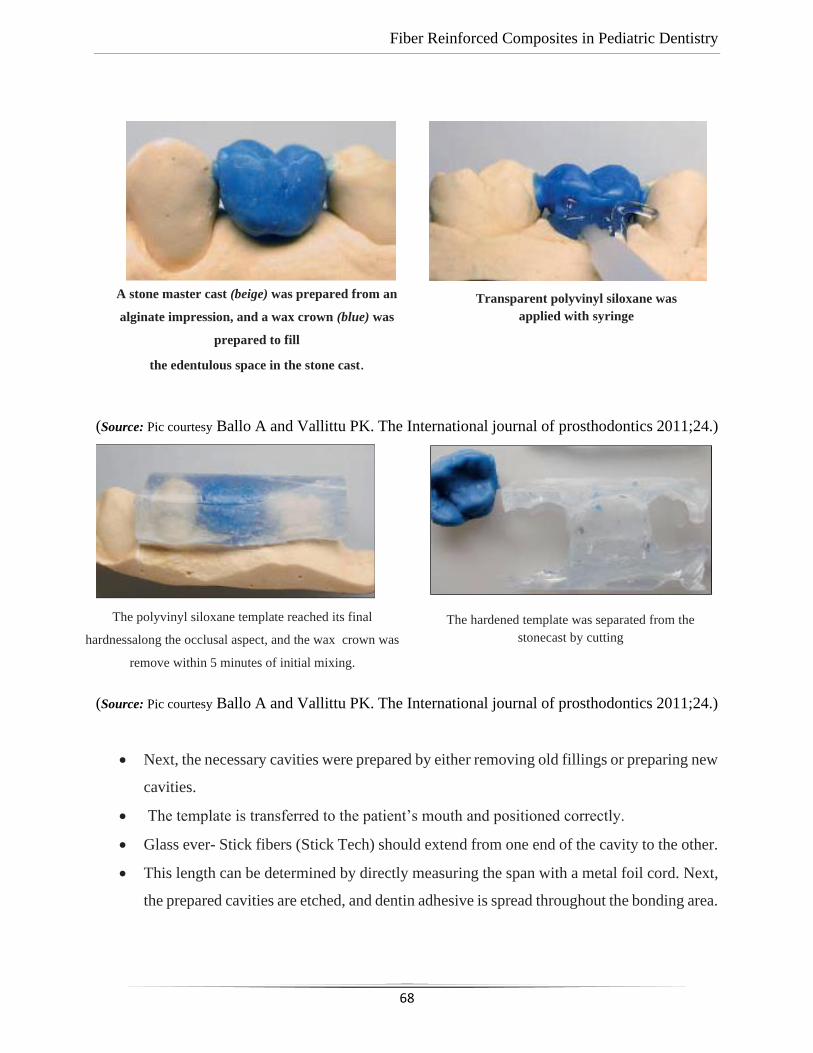
Fiber Reinforced Composites in Pediatric Dentistry
68
(Source: Pic courtesy Ballo A and Vallittu PK. The International journal of prosthodontics 2011;24.)
(Source: Pic courtesy Ballo A and Vallittu PK. The International journal of prosthodontics 2011;24.)
• Next, the necessary cavities were prepared by either removing old fillings or preparing new
cavities.
• The template is transferred to the patient’s mouth and positioned correctly.
• Glass ever- Stick fibers (Stick Tech) should extend from one end of the cavity to the other.
• This length can be determined by directly measuring the span with a metal foil cord. Next,
the prepared cavities are etched, and dentin adhesive is spread throughout the bonding area.
A stone master cast (beige) was prepared from an
alginate impression, and a wax crown (blue) was
prepared to fill
the edentulous space in the stone cast.
Transparent polyvinyl siloxane was
applied with syringe
The polyvinyl siloxane template reached its final
hardnessalong the occlusal aspect, and the wax crown was
remove within 5 minutes of initial mixing.
The hardened template was separated from the
stonecast by cutting
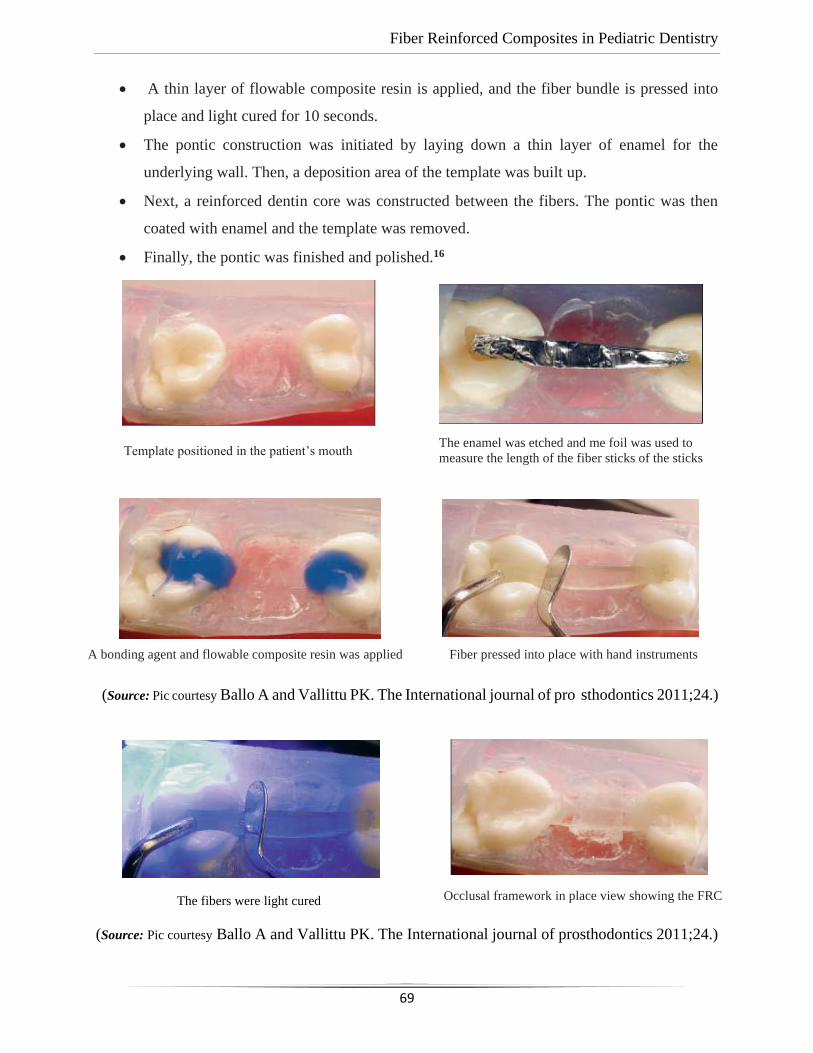
Fiber Reinforced Composites in Pediatric Dentistry
69
• A thin layer of flowable composite resin is applied, and the fiber bundle is pressed into
place and light cured for 10 seconds.
• The pontic construction was initiated by laying down a thin layer of enamel for the
underlying wall. Then, a deposition area of the template was built up.
• Next, a reinforced dentin core was constructed between the fibers. The pontic was then
coated with enamel and the template was removed.
• Finally, the pontic was finished and polished.16
(Source: Pic courtesy Ballo A and Vallittu PK. The International journal of pro sthodontics 2011;24.)
(Source: Pic courtesy Ballo A and Vallittu PK. The International journal of prosthodontics 2011;24.)
Template positioned in the patient’s mouth The enamel was etched and me foil was used to
measure the length of the fiber sticks of the sticks
A bonding agent and flowable composite resin was applied
Fiber pressed into place with hand instruments
The fibers were light cured Occlusal framework in place view showing the FRC
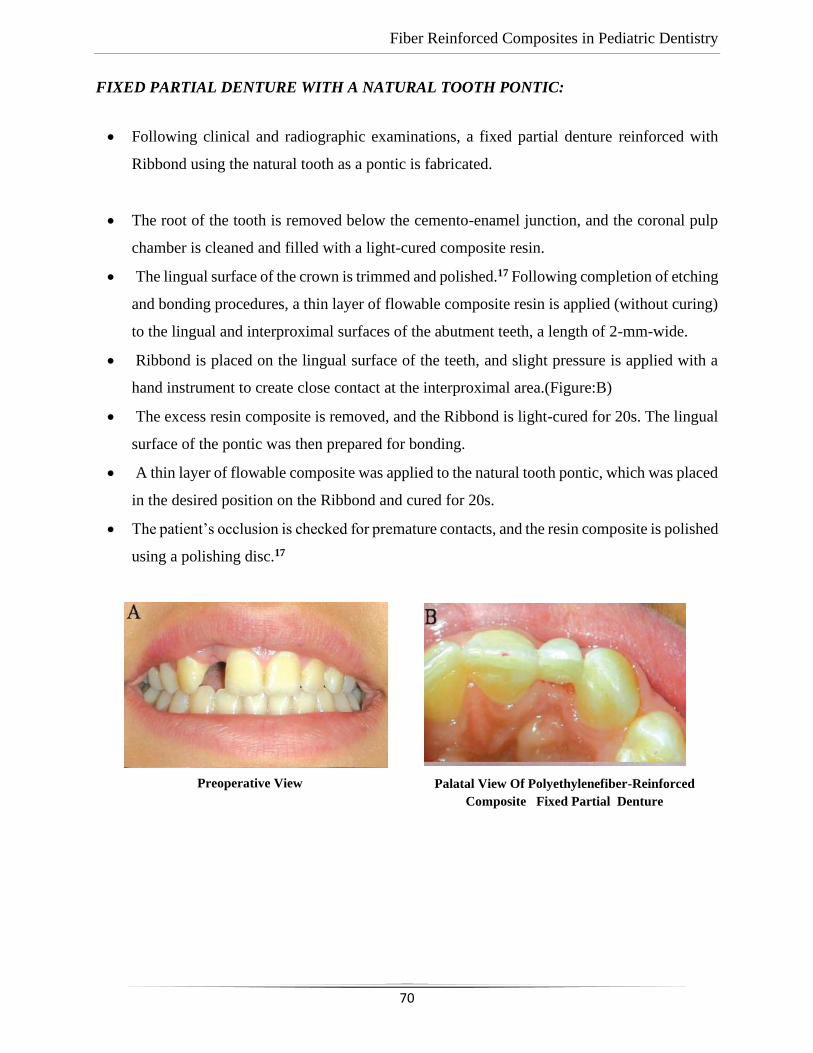
Fiber Reinforced Composites in Pediatric Dentistry
70
FIXED PARTIAL DENTURE WITH A NATURAL TOOTH PONTIC:
• Following clinical and radiographic examinations, a fixed partial denture reinforced with
Ribbond using the natural tooth as a pontic is fabricated.
• The root of the tooth is removed below the cemento-enamel junction, and the coronal pulp
chamber is cleaned and filled with a light-cured composite resin.
• The lingual surface of the crown is trimmed and polished.17 Following completion of etching
and bonding procedures, a thin layer of flowable composite resin is applied (without curing)
to the lingual and interproximal surfaces of the abutment teeth, a length of 2-mm-wide.
• Ribbond is placed on the lingual surface of the teeth, and slight pressure is applied with a
hand instrument to create close contact at the interproximal area.(Figure:B)
• The excess resin composite is removed, and the Ribbond is light-cured for 20s. The lingual
surface of the pontic was then prepared for bonding.
• A thin layer of flowable composite was applied to the natural tooth pontic, which was placed
in the desired position on the Ribbond and cured for 20s.
• The patient’s occlusion is checked for premature contacts, and the resin composite is polished
using a polishing disc.17
Palatal View Of Polyethylenefiber-Reinforced
Composite Fixed Partial Denture
Preoperative View
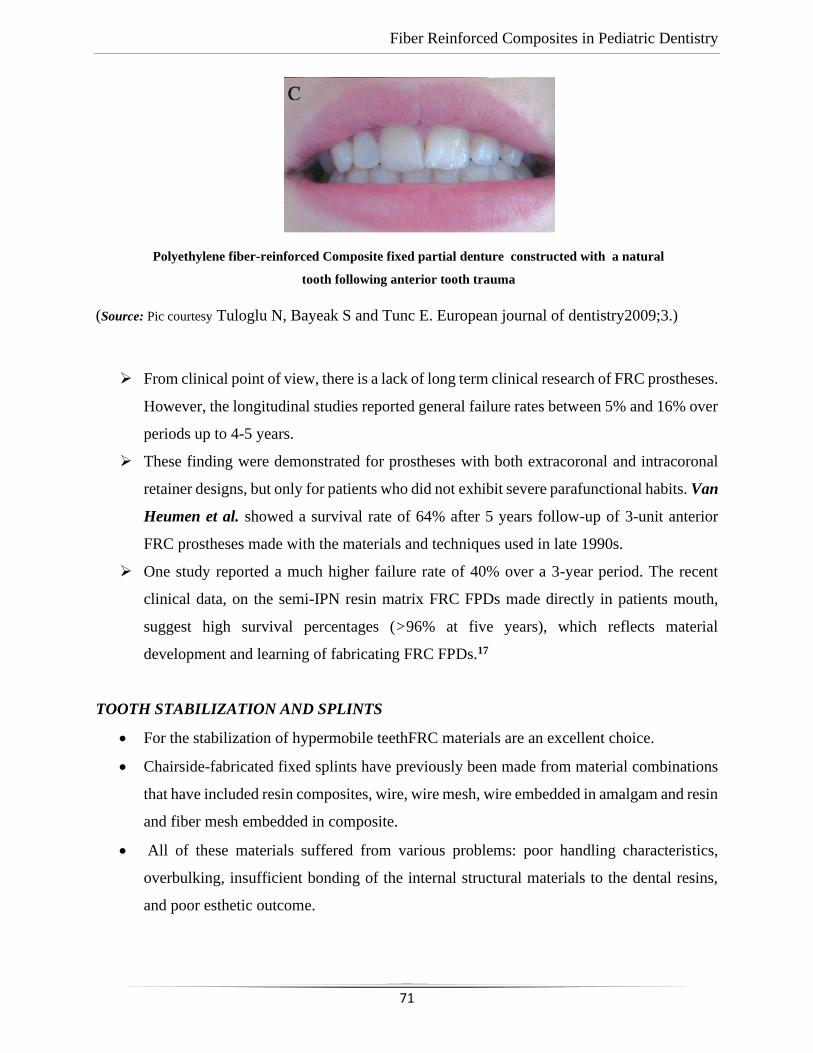
Fiber Reinforced Composites in Pediatric Dentistry
71
(Source: Pic courtesy Tuloglu N, Bayeak S and Tunc E. European journal of dentistry2009;3.)
➢ From clinical point of view, there is a lack of long term clinical research of FRC prostheses.
However, the longitudinal studies reported general failure rates between 5% and 16% over
periods up to 4-5 years.
➢ These finding were demonstrated for prostheses with both extracoronal and intracoronal
retainer designs, but only for patients who did not exhibit severe parafunctional habits. Van
Heumen et al. showed a survival rate of 64% after 5 years follow-up of 3-unit anterior
FRC prostheses made with the materials and techniques used in late 1990s.
➢ One study reported a much higher failure rate of 40% over a 3-year period. The recent
clinical data, on the semi-IPN resin matrix FRC FPDs made directly in patients mouth,
suggest high survival percentages (>96% at five years), which reflects material
development and learning of fabricating FRC FPDs.17
TOOTH STABILIZATION AND SPLINTS
• For the stabilization of hypermobile teethFRC materials are an excellent choice.
• Chairside-fabricated fixed splints have previously been made from material combinations
that have included resin composites, wire, wire mesh, wire embedded in amalgam and resin
and fiber mesh embedded in composite.
• All of these materials suffered from various problems: poor handling characteristics,
overbulking, insufficient bonding of the internal structural materials to the dental resins,
and poor esthetic outcome.
Polyethylene fiber-reinforced Composite fixed partial denture constructed with a natural
tooth following anterior tooth trauma
Fiber Reinforced Composites in Pediatric Dentistry
72
• FRC stabilization can be either intracoronal or extracoronal, depending on the clinical
situation.
• The intracoronal technique requires a prepared horizontal channel that will accommodate
the width and thickness of the FRC reinforcement material.
• The dimensions of this channel usually range from 2.0 to 3.0mm wide and from 1.0 to
2.0mm deep. This channel is prepared in the middle to incisal third of the teeth.
• Mandibular splints are usually placed on the lingual surfaces, while a maxillary splint can
be placed on either the lingual or facial surface, depending on the occlusal relationships
between the teeth.
• The facial approach has the advantage of maintaining the occlusal stops on sound tooth
structure, preventing the restorative (particulate) composite from interfering with function.
• Intracoronal splints for posterior teeth require channels that are usually placed on the
occlusal surface; the channel can be prepared into an existing restoration and then inserted
into particulate composite, which is placed within the channel preparation.2
• FRC materials are available with different fiber architectures.
• Fiber architecture has a significant impact on both mechanical properties and handling
characteristics.
• Woven fiber is less technique-sensitive and easier to manipulate because it has less memory
than unidirectional fiber and is thebest choice for rotated or malpositioned teeth.
Unidirectional fiber has greater flexure strength and rigidity and is the better choice for
high stress situations.
• Currently, two categories of fiber reinforcement material can be used for intraoral use:
pre-impregnated and non–pre-impregnated.
Resin Pre-impregnated FRC Splinting Technique
• Pre-impregnated material (Splint-It, Jeneric/Pentron) has two fiber designs: a 2-mm woven
fiber and a 3-mm unidirectional fiber.2
Fiber Reinforced Composites in Pediatric Dentistry
73
Materials required for the intraoral(chairside) fabrication of a periodontal splint are as
follows:
• Diagnostic cast
• Rubber dam
• Wedges, Stimudents, high-viscosity polyvinyl siloxane impression material
• High-speed handpiece and burs
• Phosphoric acid gel etchant
• Fourth-generation (multiple bottle) or fifth generation (single bottle) enamel-dentin
bonding agent
• Intraoral FRC material (Splint-It, Jeneric/Pentron)
• Visible light–curing flowable particulate composite resin
• Visible light–curing unit2
EXTRACORONAL SPLINTING TECHNIQUE USING PRE-IMPREGNATED FRC
MATERIAL
NON-PRE-IMPREGNATED FRC SPLINTING TECHNIQUE
• Non—pre-impregnated materials include plasma-treated, woven, polyethylene ribbons
(Ribbond Reinforcement Ribbon, Ribbond; Connect, Kerr) and flexible white continuous
filament glass ceramic fiber that has been etched and silanated (GlasSpan, GlasSpan)
Plasma treatment of the polyethylene ribbon permits a chemical union to take place
between the resin and the polyethylene fibers.
• Etching and silanation of the glass allow for both a mechanical and a chemical union of the
fibers.
• The Ribbond Reinforcement Ribbon is available in a 1.0-mm width for orthodontic
stabilization and 2.0-, 3.0-, and 4.0-mm widths for tooth stabilization and tooth
replacement.
• Connect is available in 2.0- and 3.0-mm widths. GlasSpan is available in 1.0-, 1.5 and 2.0-
mm-wide braided ropes and a 2.0-mm-wide woven tape.
• The materials used for this chairside procedure are the same as for the pre-impregnated
FRC splinting technique with the exception of the type of FRC material that is used.
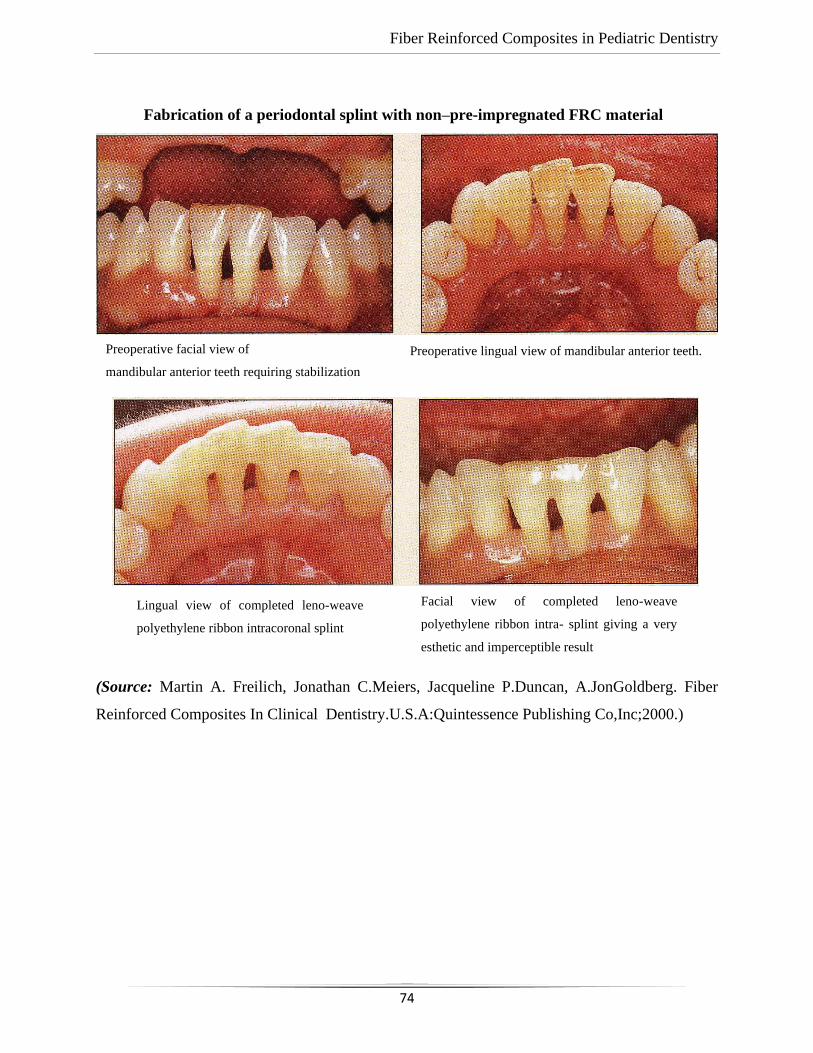
Fiber Reinforced Composites in Pediatric Dentistry
74
Fabrication of a periodontal splint with non–pre-impregnated FRC material
(Source: Martin A. Freilich, Jonathan C.Meiers, Jacqueline P.Duncan, A.JonGoldberg. Fiber
Reinforced Composites In Clinical Dentistry.U.S.A:Quintessence Publishing Co,Inc;2000.)
Preoperative facial view of
mandibular anterior teeth requiring stabilization
Preoperative lingual view of mandibular anterior teeth.
Lingual view of completed leno-weave
polyethylene ribbon intracoronal splint
Facial view of completed leno-weave
polyethylene ribbon intra- splint giving a very
esthetic and imperceptible result
Fiber Reinforced Composites in Pediatric Dentistry
75
CHAIRSIDE CONSERVATIVE TOOTH REPLACEMENT:
• Chairside tooth replacement is an excellent application for FRC technology. Previous
attempts at chairside tooth replacement involved the use of pontics derived from extracted
teeth, acrylic resin denture teeth with or without lingual wire reinforcement and resin
composite.
• These were attached to abutment teeth with acid-etched bonded particulate composite,
acid-etched particulate composite, and either wire designs or plasma-treated, polyethylene
fiber ribbon.
• The abutment teeth used for these approaches were usually not prepared; most often, tooth
replacement was only for the anterior region and the procedure was considered a short-
term solution.2
• The chairside FRC prosthesis offers a fast, minimally invasive approach for tooth
replacement that combines all of the benefits of the FRC material for an esthetic,
functional, and potentially durable result.
• A denture tooth or a natural tooth (in the case of an extraction of a periodontally involved
incisor) can be used as the pontic.
Selection criteria for this tooth replacement approach include:
A patient who desires an immediate, minimally invasive approach
• A patient who requires an extraction in an esthetic area and desires an immediate replacement
• Abutment teeth with a questionable long term prognosis
• Anterior disarticulation during mandibular protrusive movements
• A nonbruxing patient
• Cost considerations
Materials required for the chairside FRCprosthesis procedure are as follows:
• Diagnostic casts
• Denture or natural tooth
• Intraoral putty occlusal-incisal pontic index
• Phosphoric acid gel etchant

Fiber Reinforced Composites in Pediatric Dentistry
76
• Fourth-generation (multiple bottle) or fifthgeneration (single bottle) enamel-dentin bonding
system
• Visible light—curing flowable particulate composite
• Unidirectional pre-impregnated FRC
• Finishing and polishing burs and points
Chairside Fixed Partial Denture:
Initial Visit
• During the initial visit, a shade is selected for the denture tooth, and an alginate impression
of the arch in which the FPD will be placed is taken to create a diagnostic cast.2
• This diagnostic cast is used for selecting and modifying the denture tooth pontic.
Denture Tooth Modification
• A denture tooth of appropriate shade that best fits the shape of the edentulous space and
that matches the anatomic shape of the adjacent teeth is selected. It is modified so as to
lightly contact the proximal surfaces of the abutment teeth and to conform to the ridge of
the edentulous space.
• The denture tooth is then tacked to the cast in an optimal position and a line is inscribed on
its occlusal/lingual surface to indicate where the slots are to be placed in the abutment teeth
at the time of insertion.
• The adjusted denture tooth is modified as follows (1) Proximal Class III preparations are
placed on the mesial and distal facial surfaces.
• These will be used to tack the denture tooth interproximally to the abutment teeth when
first positioned in the mouth. (2) An occlusal/lingual groove, at least 2 mm wide and 2 mm
deep, is prepared, with the base undercut following the occlusal/lingual line drawn earlier.
This groove will receive the FRC.
Fiber Reinforced Composites in Pediatric Dentistry
77
Alternative Technique Using Extracted Tooth
• If the natural tooth is unsalvagable and must be extracted, it can be used as the pontic.
• The length of the tooth is determined by measuring from the extraction site to the incisal
edge of the adjacent teeth; the root is then cut from the tooth crown at this determined
length.
• The root canal opening at the apical end is restored by preparing the root canal with a 330
bur to a depth of 1.5 mm. The preparation is restored with particulate composite using an
adhesive technique.The technique for placing the natural tooth crown is similar to that for
a denture tooth.2
Fabrication of an Intraoral, Occlusal-Incisal Pontic Index
• The denture tooth is positioned on the diagnostic cast and a positioning index is fabricated
to aid in the accurate alignment of the denture tooth pontic in the mouth.
• Fabricated from vinyl siloxane putty, the positioning index encompasses the occlusal-
incisal portion of the pontic and the adjacent abutment teeth and fills the occlusal/lingual
groove for the FRC.
• The gingival extension should not block facial access to the Class III proximal retentive
forms of the pontic.2
Chairside Insertion Technique
• The abutment teeth are anesthetized; the denture tooth is tried in to verify fit, shade, and
contour; and a rubber dam is placed.
• Grooves are prepared in the abutment teeth to align with the groove in the denture tooth
these are to be at least 2 mm wide and2 mm deep so as to duplicate the groove in the pontic.
• The occlusal/lingual groove in the denture tooth pontic is sandblasted with 50 pm
aluminum oxide.
• The occlusal/lingual grooves and the interproximal areas of the abutment teeth adjacent to
the edentulous space are etched and treated with a dentin bonding agent.
• The denture tooth is placed in the putty index and positioned in the mouth.2
• A flowable composite is placed and light cured into the Class III interproximal
preparations and onto the proximal surfaces of the abutment teeth.
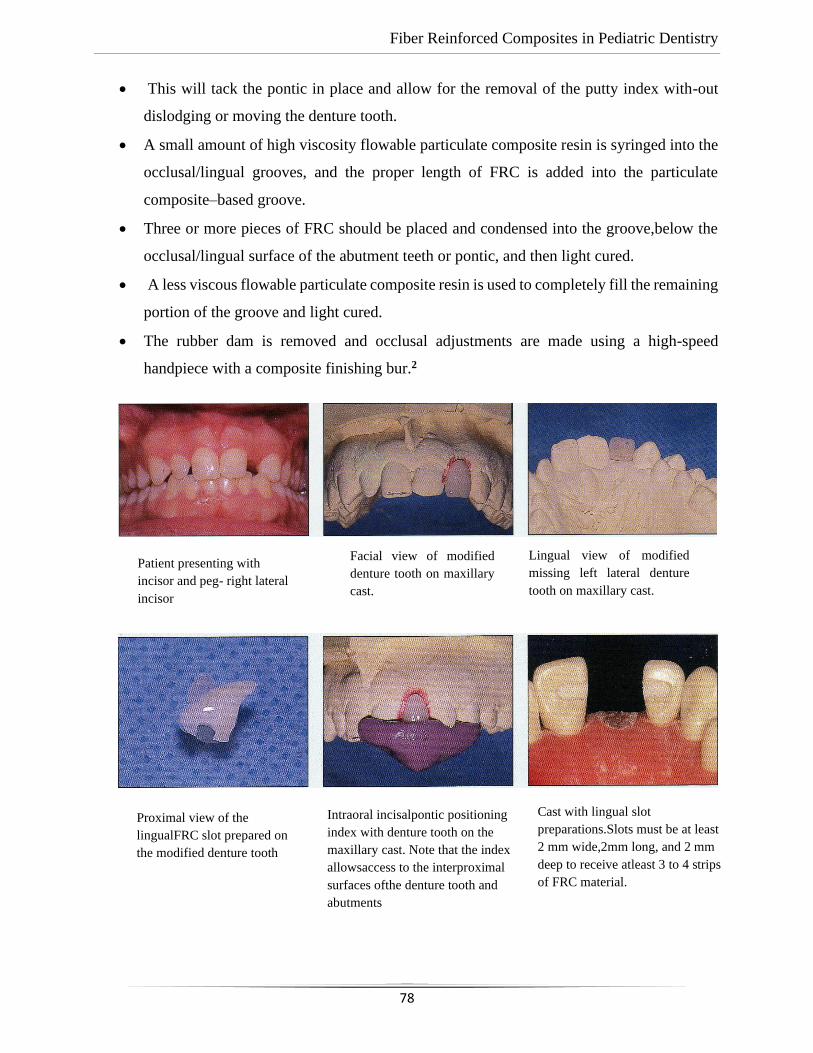
Fiber Reinforced Composites in Pediatric Dentistry
78
• This will tack the pontic in place and allow for the removal of the putty index with-out
dislodging or moving the denture tooth.
• A small amount of high viscosity flowable particulate composite resin is syringed into the
occlusal/lingual grooves, and the proper length of FRC is added into the particulate
composite–based groove.
• Three or more pieces of FRC should be placed and condensed into the groove,below the
occlusal/lingual surface of the abutment teeth or pontic, and then light cured.
• A less viscous flowable particulate composite resin is used to completely fill the remaining
portion of the groove and light cured.
• The rubber dam is removed and occlusal adjustments are made using a high-speed
handpiece with a composite finishing bur.2
Patient presenting with
incisor and peg- right lateral
incisor
Facial view of modified
denture tooth on maxillary
cast.
Lingual view of modified
missing left lateral denture
tooth on maxillary cast.
Proximal view of the
lingualFRC slot prepared on
the modified denture tooth
Intraoral incisalpontic positioning
index with denture tooth on the
maxillary cast. Note that the index
allowsaccess to the interproximal
surfaces ofthe denture tooth and
abutments
Cast with lingual slot
preparations.Slots must be at least
2 mm wide,2mm long, and 2 mm
deep to receive atleast 3 to 4 strips
of FRC material.
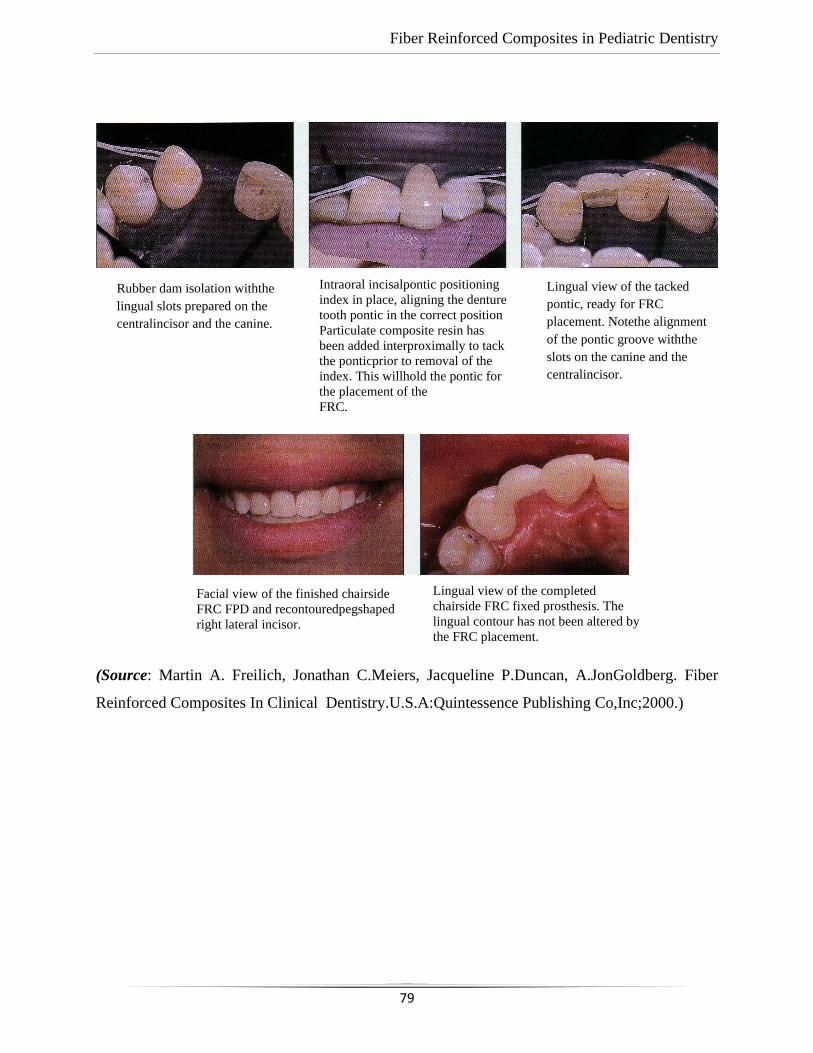
Fiber Reinforced Composites in Pediatric Dentistry
79
(Source: Martin A. Freilich, Jonathan C.Meiers, Jacqueline P.Duncan, A.JonGoldberg. Fiber
Reinforced Composites In Clinical Dentistry.U.S.A:Quintessence Publishing Co,Inc;2000.)
Rubber dam isolation withthe
lingual slots prepared on the
centralincisor and the canine.
Intraoral incisalpontic positioning
index in place, aligning the denture
tooth pontic in the correct position
Particulate composite resin has
been added interproximally to tack
the ponticprior to removal of the
index. This willhold the pontic for
the placement of the
FRC.
Lingual view of the tacked
pontic, ready for FRC
placement. Notethe alignment
of the pontic groove withthe
slots on the canine and the
centralincisor.
Facial view of the finished chairside
FRC FPD and recontouredpegshaped
right lateral incisor.
Lingual view of the completed
chairside FRC fixed prosthesis. The
lingual contour has not been altered by
the FRC placement.
Fiber Reinforced Composites in Pediatric Dentistry
80
SURGICAL APPLICATIONS FOR FIBER REINFORCED COMPOSITES:
• FRC in combination of bioactive modifiers like bioactive glass eliminates several
shortcomings of bulk material made implants of metals, ceramics and polymers. FRC
materials are durable and tough and have proven their suitability to surgical applications
of implantology.
• Particles of bioactive glass (BG) have been added to the surface or inner space of FRC
implants to improve osteoconductivity and osteoinductivity of the FRC material.
• The need for skull reconstructions is increasing mainly due to an increase in decompressive
craniectomies, a life-saving maneuver to relieve intracranial pressure resulting from
swelling of the brain due to e.g. trauma or cerebrovascular accidents. Radiation therapy
can also be given in the presence of FRC implant.
• The most commonly used fibers in medical FRC are made of glass of specific composition
but carbon/graphite fibers have also been tested as spinal fusion cages.8
• Surgically used glass fibers are referred as S glass and they are basically free of leaching
ions in physiologically moist environment like in living tissues with presence of
extracellular liquid.
• Use of carbon/ graphite fibers has been limited due to risk of release of micro and
nanometer scale carbon wear debris to tissues.
• Glass fibers of diameter micrometers are used in implants as continuous fibers which have
been woven to textile form before impregnating and coupling with resin, and this method
inhibits the release of wear debris.
• In the presently used designs of FRC implants, both woven textile form of fibers and
unidirectional continuous fibers are used in the implant construction.
• The role of continuous unidirectional fibers is to connect the outer and inner surface
laminates together for providing high strength to the implant.
• Special features of the FRC cranial implant construction are mesh-like surface laminates
and presence of free space between the outer and inner laminates, which is loaded with
particles of bioactive glass.
Fiber Reinforced Composites in Pediatric Dentistry
81
• Long-term durability of the cranioplasty implant is important because according to the
present best knowledge, the cranial defects need years of time to be closed by new forming
bone even the presence of osteoinductive implant materials.
• This is the reason why any of the biodegradable polymers or composites cannot be used
for repairs of large bone defects in the cranium.8
• Biodegradable polymer based materials degrade and loose the mechanical strength too fast
in relation to the bone regeneration.
• With regard to degradable metal alloys of magnesium, there are problems in tissue healing
due to release of hydrogen gas during degradation process.
• Thermoset copolymer and the silanized glass fibers form a durable composite for
fabrication of patient specific and standard shaped implants.
• Biocompatibility of FRC implants is the biocompatibility of its components.
• Presence of BG on the implant surface or inside the implant enhance cell maturation of
differentiated bone forming cells. In many of the FRC implant studies, there have been BG
(S53P4) particles in the FRC implant.
• BGs are synthetic dissolving biocompatible osteoconductive- osteoinductive bone
substitutes. Some compositions (S53P4) of BGs have clinically been used because of
antibacterial and angiogenesis-promoting properties.
• Antimicrobial efficiency has been shown for more than 20 microbe species, including
Staphylococcus aureus and Staphylococcus epidermis, which are the most common
pathogens in periprosthetic infections.
• Clinical studies with cranial FRC-BG implants have been for improving osteogenesis,
angiogenesis and antimicrobial properties and long term protection of brain tissues.
• In the biological environment ions of calcium and phosphorus are released from the BG
and they biomineralize on the material surface, like the surface of glass FRC-BG implant.8
• For cells, at the early stage of osteogenesis, released ions from the BG and slightly
increased pH due to ion exchange reactions are inducing differentiation of mesenchymal
stem cells to cell lines for bone formation.
• This, in conjunction with biomineralization promotes bone growth. A series of reactions
starting at the glass surface followed by a series of biological reactions are occurring with
regard to osseointegration, i.e. bonding between the BG of the implant and bone tissue.
Fiber Reinforced Composites in Pediatric Dentistry
82
• The different reaction steps taking place at the glass surface depend not only on the glass
composition but also on the surface topography, surface area of glass, and interstistial fluid
flow in the microenvironment around the glass surfaces.
• In the subsequent steps, calcium and phosphate from the solution, and migrating from the
bulk glass, form first amorphous hydroxyapatite and then crystallize at carbonate
substituted hydroxyapatite layer (HA) at the glass surface.
• This HA layer is compatible with the biological apatite and provides an interfacial bonding
between the material and tissue.
• The present design of FRC-BG cranial implant was approved for clinical use as patient-
specific implant and standard shaped implant in Europe in 2014.
FUTURE ASPECTS FOR THE RESEARCH OF FRCS:
➢ Use of FRCs in dentistry and medicine has now taken the first steps and the use is
increasing rapidly.
➢ New applications are tested due to versatile properties of FRC in terms of biomechanics,
possibility to add biologically active compounds to the medical device structure and into
the polymer matrix.8
➢ The limitations of biodegradable implants and stem cell based tissue engineering
approaches in cranial bone repair can be overcome by using glass FRC-BG implants. New
applications for FRC will be found from orthopaedic and trauma surgery and spine surgery
and in more specific dental fields including dental implantology.
NEW FEATURES AND FUTURE APPLICATIONS
➢ Future research on FRCs needs to focus on many aspects such as optimization of the design
of the frameworks in FRC devices, incorporation of bioactive minerals into the reinforced
resin composites, and the change to fiber binding matrix from resin base to inorganic type.
➢ Another improvement is related to nanotechnology, with the production of functional
structures in the range of 0.1-100 nm by various physical or chemical methods. Dental
nanocomposites provided a cosmetically acceptable result with excellent mechanical
properties.
Fiber Reinforced Composites in Pediatric Dentistry
83
➢ The addition of nanofillers particles to resin-based dental materials is the main point
involved with this new trend. The utilization of continuous and discontinuous nanofillers
has been proposed in conjunction with FRCs.
➢ FRC utilization has been proposed also in combination with Computer-Aided-
Design/Computer-Aided-Machining (CAD/CAM) technologies.
➢ The interaction between the two technologies seems to be promising based on limited
information.
➢ One other field where FRCs are starting to be utilized is implantology. Implant
applications could benefit from certain biomechanical properties of FRCs, and the
possibility of incorporating additional bioactive components into the implant structure
may open new research fields.7
➢ FRCs have been suggested for tissue engineering for orthopaedic scaffolds. As
biocompatibility results are promising, FRC biomaterials developed may constitute an
optimized alternative to the other materials used for the reconstruction of craniofacial bone
defects.
➢ The research options with FRC materials are open and future reports about the topic are
expected to widen FRC utilization in both dental and medical fields.7
Fiber Reinforced Composites in Pediatric Dentistry
84
BIBLIOGRAPHY
1. Kandilaya V and Raj J.Recent advances and modifications of dental restorative materials-A
review. International Journal Of Recent Advances In Multidisciplinary Research
2016;03:1609-1616.
2. Martin A. Freilich, Jonathan C.Meiers, Jacqueline P.Duncan, A.JonGoldberg. Fiber
Reinforced Composites In Clinical Dentistry.U.S.A:Quintessence Publishing Co,Inc;2000.
3. Butterworth C, Ellakwa A and Shortall A. Fiber reinforced composites in restorative
dentistry.Dental Update 2003;30:300-306.
4. Tayab T, Shetty A and Kayalvizhi G. The clinical applications of fiber reinforced composites
in all specialities of dentistry an overview. International Journal of composite materials
2015;5:18-24.
5. Kumar A, Tekriwal S, Rajkumar B,Gupta V and Rastogi R.A review on fiber reinforced
composite resins. Annals of prosthodontics and restorative dentistry2016;2:11-16.
6. Zhang M and Matinlinna J. E-Glass fiber reinforced composites in dental
applications.Silicon2012;4:73-78.
7. Scribnate A, Vallittu PK, Ozcan M,Lippo V, Lassila,Gandini P and SfondriniM.Travel beyond
clinical uses of fiber reinforced composites(FRCs) in dentistry: A review of past employments,
present applications and future perspectives.Biomed research international2018.
8. Vallittu PK. An overview of development and status of fiber reinforced composites as
dental and medical biomaterials. Acta Biomaterialia Scandinavica2018;4:44-45.
9. Vallittu PK. Flexural properties of acrylic polymers reinforced with unidirectional and woven
glass fibres. J Prosthet Dent 1999;81:318-326.
10. Acharya S and Tandon S. Fiber-reinforced composite: Post and core material in pediatric
patient: An alternative to usual.SRM Journal of Research in Dental Sciences2015;6.
11. Delperi S. Direct Fiber-reinforced Composite Restoration in an Endodontically-treated
Molar:A Three-year Case Report. Operative dentistry2008;33:209-214.
Fiber Reinforced Composites in Pediatric Dentistry
85
12. Tayab T and Srinivasan I.Space maintainer using fiber-reinforced composite and natural tooth-
a non –invasive technique.Dental Traumatology2011;27:159-162.
13. Yeluri R and Munshi AK.Fiber reinforced composite loop space maintainer:An alternative to
the conventional band and loop. Contemp Clin Dent 2012;3:S1:26-8.
14. Kirzioglu Z, Zahit Z and Ceylan C.Clinical success of FRC space maintainer.The journal of
contemporary dental practice2017;18:188-193.
15. Singh K et al. A conservative treatment approach to replacing a missing anterior tooth.Case
reports in dentistry2014.
16. Ballo A and Vallittu PK. Alternative fabrication method for chairside fiber-reinforced
composite resin provisional fixed partial dentures.The International journal of
prosthodontics2011;24.
17. Tuloglu N, Bayeak S and Tunc E. Different clinical applications of bondable reinforcement of
Ribbond in pediatric dentistry. European journal of dentistry2009;3.