
Fever, PUO and SIRS
25
Fever, PUO & SIRS •History, examination, differential diagnoses, investigations and management. •Common terms and definitions. •Antibiotics???? KHAIRUL AZHAR ABU BAKAR 3MB3 2011
-
Upload
meducationdotnet -
Category
Documents
-
view
202 -
download
0
Transcript of Fever, PUO and SIRS
Fever, PUO & SIRS
•History, examination, differential diagnoses, investigations and management.
•Common terms and definitions.
•Antibiotics????
KHAIRUL AZHAR ABU BAKAR 3MB3 2011
CASE SCENARIO
Flapping penguins. “Pick me! Pick me!” =)
CASE 1
A 15 year old girl presented to ED through GP referral c/o two days history of new onset fever, headache, photophobia, rash and sore throat with no previous background hx, medications, or known allergies.
She denied any previous seizure, epilepsy, loss of consciousness, agitation, chest pain, palpitations, shortness of breath, cough, abdominal pain, or GI bleeding.
CASE 2
A 51 years old lady was transferred from LGH to MAU in UCHG c/o of one week history of jaundice and two months episodes of general malaise, fever, night sweats, unintentional weight loss and vague abdominal pain.
No previous gallstones or jaundice, denied any illicit drug use, tattooing, alcohol excess, recent travel or contact with jaundiced people.
8 Questions for you???
Did these two ladies have fever?
Did they both have SIRS?
Did they both have PUO?
What is the most likely aetiology?
What questions should you ask these patients?
What findings would you expect on examinations?
What are the appropriate investigations and why?
How would you manage these patients? As outpatients or inpatients?
What antibiotics would you prescribe?

DIFFERENTIAL
DIAGNOSES
WOAAAHHHH....... Don’t panic. Try to be systematic =)
Fever
A rise/?decrease in body temp (T>37.3°C or <36.6°C) in response to endogenous cytokines.
Causes:
i. Infections – bacterial, viral, parasitic, fungal, rickettsial.
ii. Malignancy – lymphoma, leukaemia, liver mets, HCC, RCC, pancreatic ca.
iii. Inflammatory – SLE, RF, RA, IBD, sarcoidosis, pancreatitis, gout.
iv. Vascular- PE, GCA, WG, PAN.
v. Endocrinology – adrenal insufficiency, DM I, hyperthyroidism.
vi. Miscellaneous – drugs, factitious.
Pyrexia of unknown origin
First definition by Petersdorf & Beeson (1961): fever of >38.3°C (101°F) on several occasions persisting w/o Dx for ≥3/52 despite ≥1/12 investigations in hospital.
Types:
i. Classic ( as above or >2 visits or >3/7 inpt)
ii. Nosocomial (none O/A, posthosp >24 hrs)
iii. Immune deficient (>3/7, -ve C+S >48 hrs).
iv. HIV related
Causes:
all the above.
Hyperthermia
An elevation in body temp >41.6°C due to loss of homeostatic mechanisms and inability to ↑ heat loss in resp to env heat.
Causes:
i. Heat stroke – CNS dysf(x), Xs physical exertion in warm env
ii. NMS – idiosyncratic reaction to antipsychotic Mx e.g butyrophenones, phenothiazines, thoxanthenes.
iii. Malignant hyperthermia – a rare genetic abn in muscle membrane that predispose pts to severe rhabdomyloysis and temp dysregulation. i.e anaesthetics, hot ambient temp.
HISTORY
Tulips... Summertime!
History-taking
Quality – how high is your fever?
Time course/ types
i. Continued – thyphoid, thypus, drug, malignant hyperthermia
ii. Intermittent – pyogenic, lymphomas, miliary TB
iii. Remittent
iv. Relapsing – malaria (tertian – P. vivax, P. ovale; quartan – P. malariae), lymphoma (Pel-Ebstein fever of HL), pyogenic.
Associated symptoms: ALARM – headache, dizziness, LOC, confusion, seizure, rash, recent unint wieght loss, night sweats, CP, SOB, hemoptysis, hematuria, jaundice.
Modifying factors
Risk factors – dental work, Mx, surgery, IV catheter, antibiotics, sick contacts, recent hosp, recent travel, living condition, arthritis, FMHx of vasculitis or inflamm disease.
EXAMINATION
As soft as a jellyfish =)
Examination
GEN – pt’s general conditions, skin, vitals.
GCS, NEURO inc eyes
ENT
CVS
RESP
GIT/GUT
???GYNAE
HAEM (if appropriate)
ENDO (if appropriate)
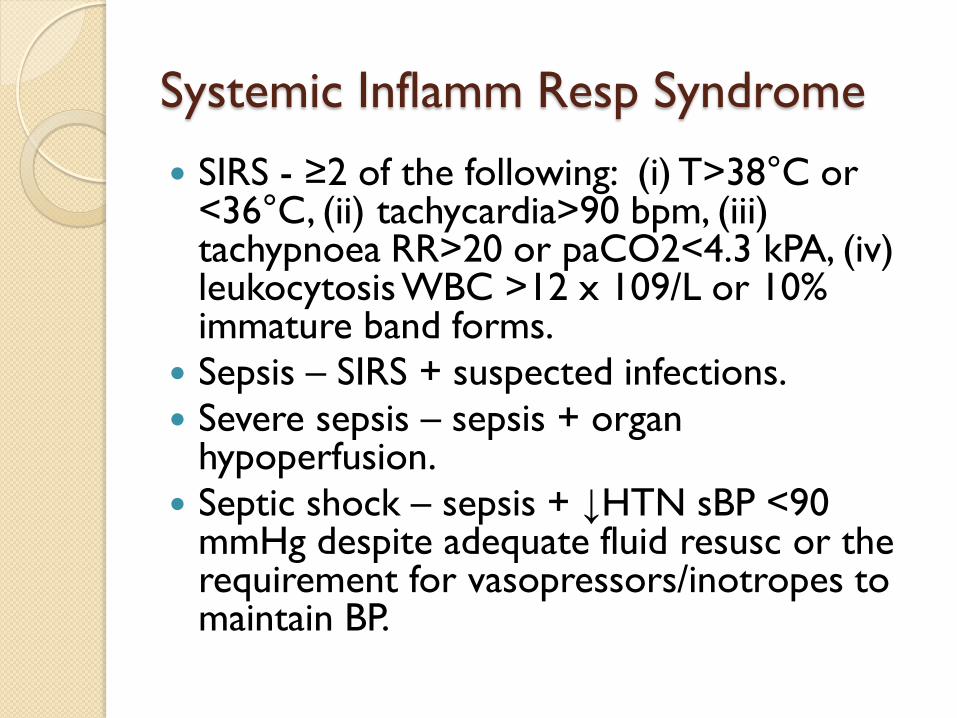
Systemic Inflamm Resp Syndrome
SIRS - ≥2 of the following: (i) T>38°C or <36°C, (ii) tachycardia>90 bpm, (iii) tachypnoea RR>20 or paCO2<4.3 kPA, (iv) leukocytosisWBC >12 x 109/L or 10% immature band forms.
Sepsis – SIRS + suspected infections.
Severe sepsis – sepsis + organ hypoperfusion.
Septic shock – sepsis + ↓HTN sBP <90 mmHg despite adequate fluid resusc or the requirement for vasopressors/inotropes to maintain BP.
INVESTIGATIONS
Chrysanthemum tea. Mmm.... Nice.

Investigations
ECG
Haematological – ABG, FBC, U&E, Coag
profile.
Biochemistry – LP, MSU, blood and urine
C+S, CRP, D-dimer LFTs, TFTs, serum
Ca2+, mantoux or skin prick test.
Radiological – erect CXR, ?PFA.
Further inv – ?ECHO, ?abdominal USS,
?liver biopsy.
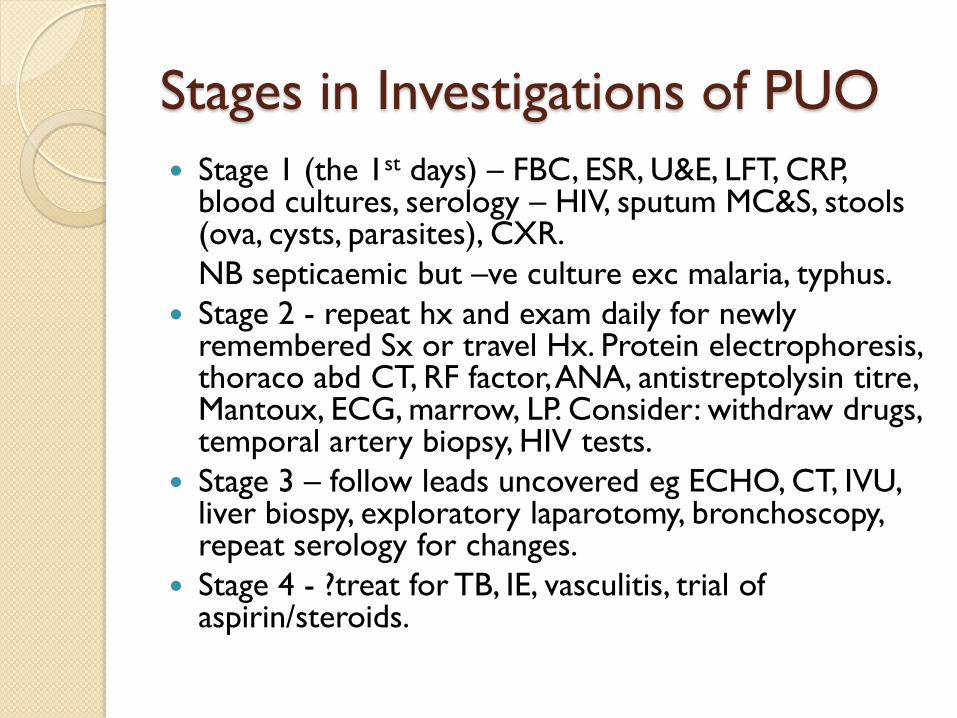
Stages in Investigations of PUO
Stage 1 (the 1st days) – FBC, ESR, U&E, LFT, CRP, blood cultures, serology – HIV, sputum MC&S, stools (ova, cysts, parasites), CXR.
NB septicaemic but –ve culture exc malaria, typhus.
Stage 2 - repeat hx and exam daily for newly remembered Sx or travel Hx. Protein electrophoresis, thoraco abd CT, RF factor, ANA, antistreptolysin titre, Mantoux, ECG, marrow, LP. Consider: withdraw drugs, temporal artery biopsy, HIV tests.
Stage 3 – follow leads uncovered eg ECHO, CT, IVU, liver biospy, exploratory laparotomy, bronchoscopy, repeat serology for changes.
Stage 4 - ?treat for TB, IE, vasculitis, trial of aspirin/steroids.
MANAGEMENT
Tongue twisting: Try “She sells seashells by the seashore” until you bite your own tongue. =P
Management
IV/IM benzylpenicillin if suspected meningitis
ABC
O2 support, 2 large IV bores, IVF, IV antibiotics, oral paracetamol.
If meningitis – manage according to
(i) septicaemic or (ii) meningitic.
If encephalitis – manage before cause known
1. start aciclovir within 30 min of pt arrival.
2. specific Rx for CMV and toxoplasmosis.
3. supportive – ↑ICP, IV dexamethasone.
Continue Ix and Rx for PUO.

Not really a good diagram: see OHCM for chapter on meningitis.
Our patients =)
PATIENT 1
On examination: pharyngitis, strawberry tongue, blanching itchy rash seems to disappear.
GCS = 15/15, no nuchalrigidity, negative Kernig’sor Brudzinski’s
DDx? Scarlet fever
Management – discharge, isolate,10 days full course of amoxicillin PO, follow up in 3 days.
PATIENT 2
On examination –palpable gallbladder, jaundice. ?painless
DDx? Pancreatic ca, lymphoma, cholangiocarcinoma, TB hepatitis.
Management – liver biopsy, refer to hepatologist.
ANTIBIOTICS
Did I miss anything? Am I lost? Is this a desert? What a pain? HUHHH?!!
Antibiotics Choices: Look up!
1. Intra abdominal infections
2. Cellulitis/wound infections
3. CAP
4. Acute pharyngitis
5. Cystitis
6. Pyelonephritis
7. Bacterial meningitis
8. Septicaemia (sources unclear).
References
Oxford Handbook of Clinical Medicine 8E
Oxford Handbook of Infectious Diseases
Lange’s The Patient History Evidence-
Based Approach
Talley et. al. Clinical Examination A
Systematic Guide to Physical Diagnosis 6E
UCHG Guidelines of Antibiotics
prescriptions 2011.
Thank you =)


















