Fertility preservation and pregnancy in cancer patients ... · Fertility preservation and pregnancy...
60
Fertility preservation and pregnancy in cancer patients Fedro A Peccatori, MD PhD European Institute of Oncology European School of Oncology Milan, ITA 5th ESO-ESMO Latin American Masterclass in Clinical Oncology
Transcript of Fertility preservation and pregnancy in cancer patients ... · Fertility preservation and pregnancy...

Fertility preservation and pregnancy in cancer
patients
Fedro A Peccatori, MD PhD
European Institute of Oncology
European School of Oncology
Milan, ITA
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Personal financial interests: I received honoraria in the last 5 years on
occasional basis from Roche, Astra Zeneca, Clovis, Takeda, Ipsen, PrIME
Non-financial interests: I am member of ASCO, ESMO, AIOM and ESGO
Other: I act as Scientific Director of the European School of Oncology
NO CONFLICTS OF INTERESTS FOR THIS PRESENTATION
Declaration of interests
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Fertility issues and fertility preservation in cancer patients
Cancer during pregnancy
Plan of the talk
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Fertility concerns of cancer patients
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

657 patients, median age 32.9 years
57% seriously concerned about sterility
29% did not comply to their treatment because of fertility issues
Fertility concerns of breast cancer patients
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Fertility preservation, doctors’ perspective
32% of patients did not recall discussing fertility issues with their doctors
37% of doctors never read fertility preservation guidelines
49% of doctors were confused about safety of pregnancy after cancer
Ruddy KJ, et al. J Clin Oncol. 2014;32(11):1151-1156. Lambertini M, et al. Submitted to The Breast, 2018 Biglia N, et al. Gynecol Endocrinol. 2015;31(6):458-464.
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Stensheim et al; Int J Cancer 2011
Analysis adjusted foreducation level, previous pregnancyage
0.0 0.5 1.0 1.5
Breast cancer
Epithelial ovarian cancer
Cervical cancer
Acute leukemia
Germ cell tumors
Brain tumors
All cancers
Hodgkin's lymphoma
Non-Hodgkin's lymphoma
Melanoma
Thyroid cancer
Pregnancy rate after cancer: not all alike
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Main determinants of infertility after oncological treatment
Age
Treatment
Disease
Fertility preservation access
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Age
Broekmans FJ et al; Endocrine Reviews, 2009
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Stearns et al; Nature Rev Cancer, 2006
Treatment
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Disease
23.201 women with cancer <40 y
Fewer pregnancies than expected:
SIR 0.62 (95%CI 0.60-0.63)
Cervical and breast cancer:
SIR 0.31 and 0.36, respectively
Anderson RA et al; Human Reprod, 2018
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology
Fertility preservation access
Only 5% of young cancer patients had access to fertility
preservation techniques
Main reasons:
• Oncologists not aware of fertility preservation techniques
• Too little time
• Reimbursement issues
• Concerns about safety of ovarian stimulation
Letourneau JM et al; Cancer 2012
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Breast cancer and impact on fertility
- Most frequent above 35 years
- High impact of adjuvant treatments
- Low awareness/access to fertility preservation
- High fear of pregnancy
- Endocrine-responsive disease
- Hormonal treatment
- Effects of pregnancy on breast cancer recurrence/mortality?-
0.0 0.5 1.0 1.5
Breast cancer
Epithelial ovarian cancer
Cervical cancer
Acute leukemia
Germ cell tumors
Brain tumors
All cancers
Hodgkin's lymphoma
Non-Hodgkin's lymphoma
Melanoma
Thyroid cancer
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Safety of pregnancy after breast cancer: meta-analysis
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

14 studies7 case control studies4 population based studies3 hospital based studies
1244 cases e 18145 controlsFollow-up 5-30 years
Sensitivity analysis and subgroup analysis
Safety: meta-analysis
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Safety: meta-analysis
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Safety: multicentre study according to ER status
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology
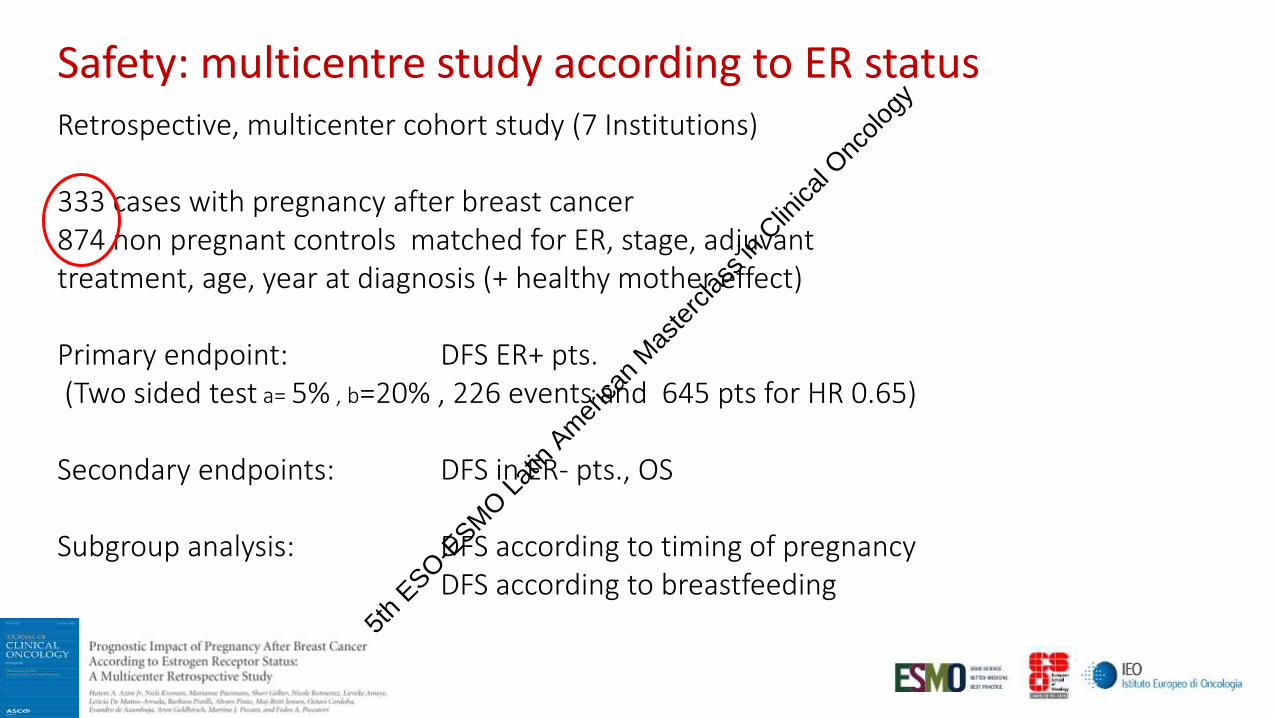
Retrospective, multicenter cohort study (7 Institutions)
333 cases with pregnancy after breast cancer874 non pregnant controls matched for ER, stage, adjuvant treatment, age, year at diagnosis (+ healthy mother effect)
Primary endpoint: DFS ER+ pts.(Two sided test a= 5% , b=20% , 226 events and 645 pts for HR 0.65)
Secondary endpoints: DFS in ER- pts., OS
Subgroup analysis: DFS according to timing of pregnancyDFS according to breastfeeding
Safety: multicentre study according to ER status
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

DFS in ER+ patientsMedian F-UP: 7.2 years
Safety: long term follow-up according to ER status
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

OS in ER+ patientsMedian F-UP: 7.2 years
Safety: long term follow-up according to ER status
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Inform, plan, act
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Guidelines
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Prompt use of fertility preservation techniques
Controlled ovarian stimulation and oocyte freezing
Ovarian tissue harvesting
LHRHa during chemotherapy
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Controlled ovarian stimulation and oocyte freezing
First choice up to 40y
Results according to age
No doubts about safety also for endocrine responsive
tumors (+Letrozole)
Random start and double stimulation
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Kim J, et al. J Clin Endocrinol Metab. 2016;101(4):1364-1371. Rodriguez-Wallberg KA, et al. Breast Cancer Res Treat. 2018;167(3):761-769.
FP = 120Control = 217
FP = 145Control = 351
SINGLE CENTER STUDY (US)
MULTICENTRICREGISTRY-BASED COHORT STUDY (SWE)
Controlled ovarian stimulation in breast cancer
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology
Ovarian tissue harvesting
Only choice in prepubertal girls
No need of ovarian stimulation
Results according to age
Restoration of endocrine function
2 surgical operations
Tumor cell contamination ?5t
h ESO-E
SMO L
atin
Amer
ican
Mas
terc
lass i
n Clin
ical O
ncolo
gy
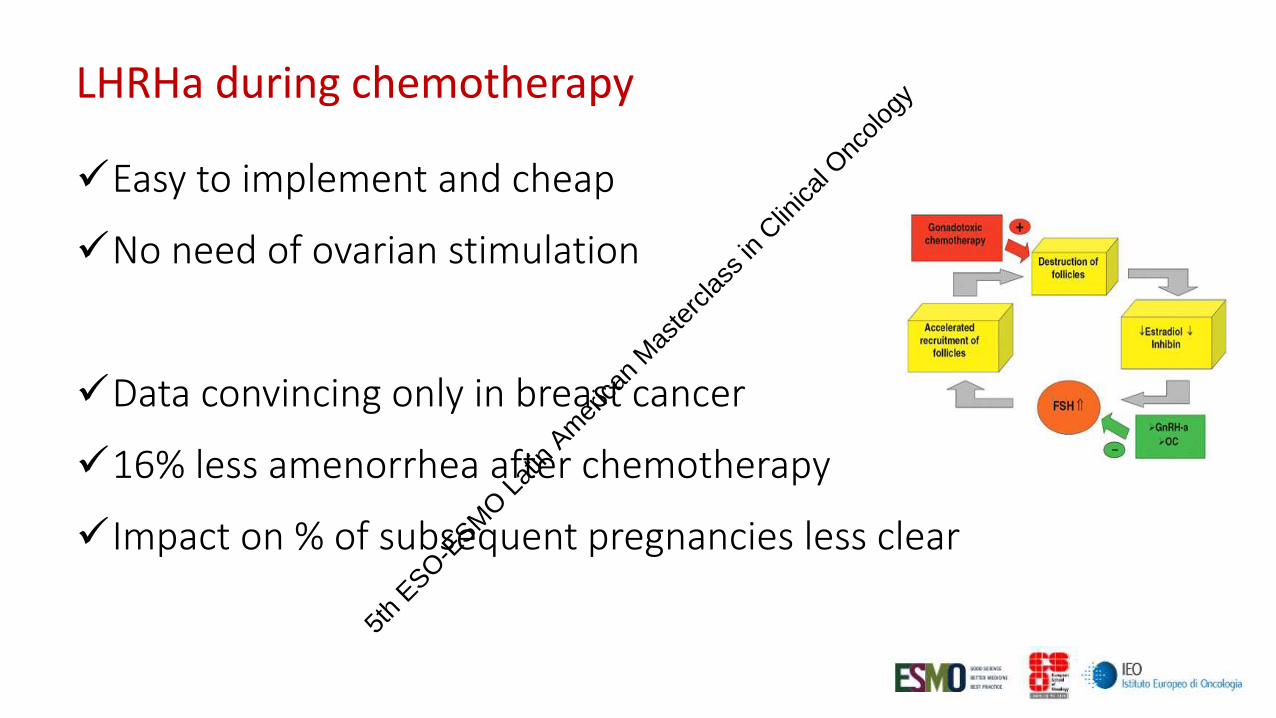
LHRHa during chemotherapy
Easy to implement and cheap
No need of ovarian stimulation
Data convincing only in breast cancer
16% less amenorrhea after chemotherapy
Impact on % of subsequent pregnancies less clear
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

LHRHa during chemotherapy for breast cancer
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Premature-Ovarian Insufficiency Rate
0%
10%
20%
30%
40%
50%
14.1%
GnRHa Group
n = 363 Control Group
n = 359
30.9%
OR* 0.38 (95% CI 0.26–0.57) P<.001 Meta-analysis approach
*Odds ratio (OR) adjusted for age, estrogen receptor status, type and duration of chemotherapy administered
Overall (I≤=0%,p=0.73) 51/363 111/359
GBG-37 ZORO
OPTION
Study
UCSF-led trial
POEMS/SWOG S0230
PROMISE-GIM6
6/28
GnRHa
21/95
Events/pts
3/26
5/66
16/148
13/29
Control
41/107
Events/pts
2/21
15/69
40/133
0.37 (0.25, 0.57)
0.54 (0.14, 2.07)
0.41 (0.20, 0.81)
OR (95% CI)
1.17 (0.14, 9.55)
0.33 (0.10, 1.14)
0.29 (0.15, 0.57)
0.37 (0.25, 0.57)
0.54 (0.14, 2.07)
0.41 (0.20, 0.81)
OR (95% CI)
1.17 (0.14, 9.55)
0.33 (0.10, 1.14)
0.29 (0.15, 0.57)
1.0982 1 10.2
GnRHa better Control better
Lambertini M, et al. Cancer Res. 2018;78(4 Suppl)
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

GnRHa Group: 37/359 (10.3%)
vs
Control Group: 20/367 (5.5%)
IRR* 1.83 (95% CI 1.06-3.15)
P = .030
Meta-analysis approach
GnRHa
Group
n = 37
Number (%)
Control
Group
n = 20
Number (%)
Age distribution, years
≤40
≥41
37 (100)
0 (0.0)
20 (100)
0 (0.0)
Estrogen receptor status
Positive
Negative
6 (16.2)
31 (83.8)
2 (10.0)
18 (90.0)
IRR, Incidence rate ratio
Overall (I≤=0%,p=0.85) 37/359 20/367
POEMS/SWOG S0230
PROMISE-GIM6
Study
OPTION
22/105
8/148
GnRHa
Events/pts
7/106
12/113
3/133
Control
Events/pts
5/121
1.82 (1.05, 3.14)
1.77 (0.87, 3.57)
2.52 (0.67, 9.50)
IRR (95% CI)
1.54 (0.49, 4.85)
1.82 (1.05, 3.14)
1.77 (0.87, 3.57)
2.52 (0.67, 9.50)
IRR (95% CI)
1.54 (0.49, 4.85)
1.105 1 9.5
Control better GnRHa better
Post treatment pregnancy rate
Lambertini M, et al. Cancer Res. 2018;78(4 Suppl)
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology
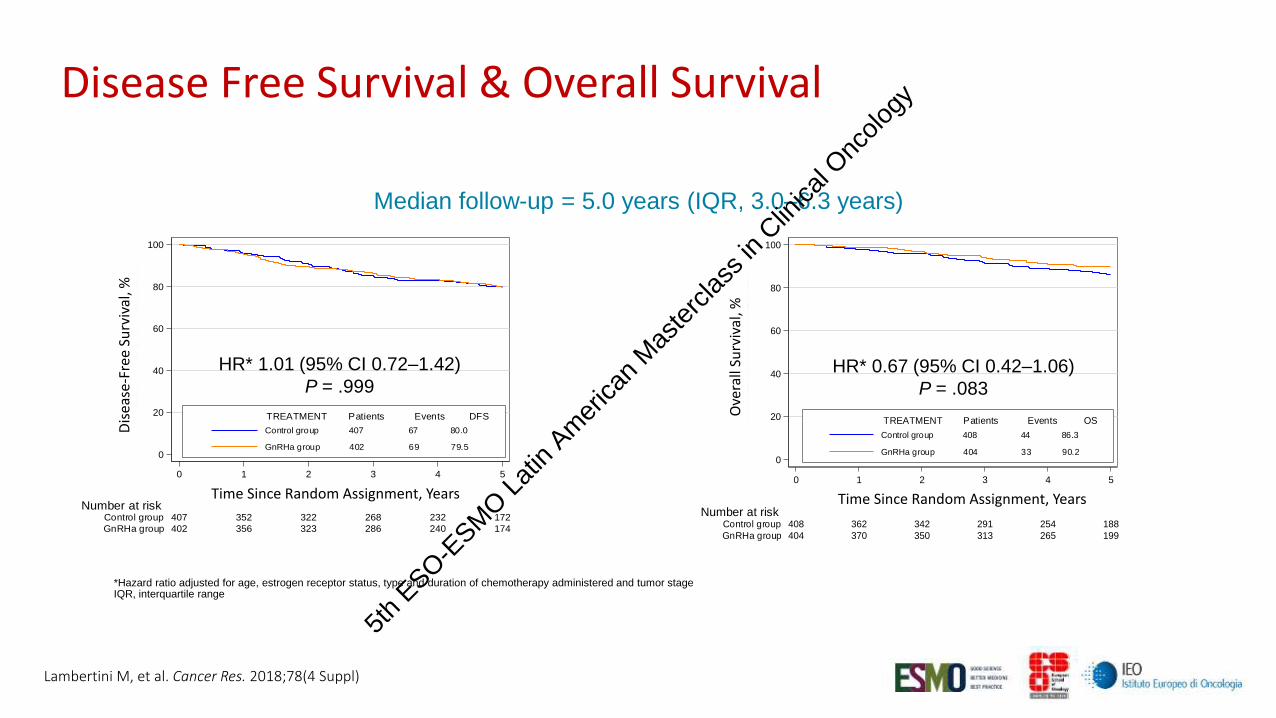
Median follow-up = 5.0 years (IQR, 3.0–6.3 years)
*Hazard ratio adjusted for age, estrogen receptor status, type and duration of chemotherapy administered and tumor stageIQR, interquartile range
0
20
40
60
80
100
Dis
ea
se F
ree
Su
rviv
al (%
)
402 356 323 286 240 174GnRHa group
407 352 322 268 232 172Control groupNumber at risk
0 1 2 3 4 5
Time Since Random Assignment (years)
Control group 407 67 80.0
GnRHa group 402 69 79.5
TREATMENT Patients Events DFS
All Patients
HR* 1.01 (95% CI 0.72–1.42)
P = .999
0
20
40
60
80
100
Overa
ll S
urv
iva
l (%
)
404 370 350 313 265 199GnRHa group
408 362 342 291 254 188Control groupNumber at risk
0 1 2 3 4 5
Time Since Random Assignment (years)
Control group 408 44 86.3
GnRHa group 404 33 90.2
TREATMENT Patients Events OS
All Patients
HR* 0.67 (95% CI 0.42–1.06)
P = .083
Dis
ease
-Fre
e S
urv
ival
, %
Ove
rall
Surv
ival
, %
Time Since Random Assignment, Years Time Since Random Assignment, Years
Disease Free Survival & Overall Survival
Lambertini M, et al. Cancer Res. 2018;78(4 Suppl)
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Fertility issues and fertility preservation in cancer patients
Cancer during pregnancy
Plan of the talk
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Epidemiology
de Haan J et al, Lancet Oncol 2018
- 1/100 cancers in reproductive age are diagnosed during pregnancy- 1/1000 pregnancies are complicated with cancer
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Epidemiology (by age at diagnosis)
Berry et al, JCO 1999
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Epidemiology (by year of diagnosis)
Stensheim et al 2009, JCO 27: 45ff
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Increasing age at pregnancy (temporal trend)
Stensheim et al 2009, JCO 27: 45ff
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Diagnosis
Diagnosis of gestational cancer is frequently delayed
- misinterpretation of symptoms
breast nodule
changing mole
vaginal discharge
- physician and patient denial
2 young 4 cancer
- diagnostic difficulties
physical exam and radiology5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

* Without gadolinium
Safe Not safe
Breast Ultrasound
Mammogram
MRI with gadolinium
Chest X-rays, Low dose CT scan
(first trimester)
DW-MRI*
X-rays, CT scan
(beyond first
trimester)
Abdomen Ultrasound /DW-MRI* CT scan
Bone DW-MRI* Bone scan
Brain DW-MRI*
Whole body DW-MRI* PET scan
Staging
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Diffusion-weighted MRI
• Exploits random motion of free water molecules within tissues
• In highly cellular tissues (cancer) water molecules movement is restricted and this can be detected in T2 sequences
• No need of contrast media/gadolinium
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology
In most series, cancers diagnosed during pregnancy have the same biologic characteristics compared to non gestational cancers, but
- the jury is still out for endocrine responsive tumors
- changes in blood flow can account for rapid tumor growth (breast, cervix)
- No detrimental effect of the so called “pregnancy immunosuppression”
Biology and prognosis
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Even if prognosis can be severe due to diagnostic delay and biology, it is not influenced by gestation for most tumor types.
Pregnancy termination does not ameliorate prognosis, unless effective treatment is excessively postponed (consider also gestational age, tumor stage and growth rate).
Biology and prognosis
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Higher risk of abortion in 1st and early 2nd
trimester (RR=1.5)
Blood pressure monitoring !
No increased risk of abortion for
non-abdominal surgery
Duncan PG et al. Anesthesiology 1986 64 790ffGentilini O et al. EJSO 2005 31 232 ffRing A et al. JCO 2005 23 4192
Surgery during pregnancy
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Peccatori F et al; Ann Oncol 2013
Usually contraindicated
- Increased risk of fetal malformation, mental retardation with radiation exposure > 100-200 mGy
- This dose is not reached if RT to sites away from uterus (e.g. brain, head/neck) with adequate shielding
- Yet, uncertainty regarding risk of cancer / sterility in offspring exists even with low doses
Radiation during pregnancy
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Cardonick E et al; Lancet Oncol 2004
Chemotherapy during pregnancy
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Malformation rate 20%
First trimester
Chemotherapy during pregnancy
Cardonick E et al; Lancet Oncol 2004
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

The role of placenta
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Number Drug detected in fetus (n) % drug detected in fetus
Doxorubicin 15 6 7.5 ± 3.2
Epirubicin 11 8 4.0 ± 1.6
Paclitaxel 11 7 1.4 ± 0.8
Docetaxel 9 0 0
Cyclophosphamide 4 3 25.1 ± 6.3
Carboplatin 7 7 57.5 ± 14.2
DOXORUBICIN EPIRUBICIN
van Calsteren et al; Gynecol Oncol 2011
Maternal/fetal transfer of chemotherapy (monkeys)
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Ring, 2005 Hahn, 2006 Peccatori, 2009 Loibl, 2012
Study type Retrospective Prospective Prospective Prospective
Multicentric Monocentric Monocentric Registry
N. 28 57 20 197
Regimen A(E)C=16CMF=12
FAC (100%) Weekly E (100%) A-based=178A(E)C (n=55) Taxane=14CMF=15
Median gestational W at chemo
W20 (15 – 33) W23 (11 – 34) W19 (16 – 30) W24 (NR)
Median gestational W at delivery
W37 (30 – 40) W37 (29 – 42) W35 (28 – 40) W37 (32 – 42)
Congenital malformations 0 3/57 (5%) 1/20 (5%) 8/179 (4.5%)
Ring A et al; JCO 2005, Hahn et al; Cancer 2006; Peccatori F et al; BCRT 2009, Loibl S et al; Lancet Oncol 2012
Anthracyclines during pregnancy
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Number
- Breast cancer
- Other
55
39
16
- Paclitaxel
- Docetaxel
- Both
33
19
3
Neonatal outcome
- Mean Gestational age at delivery
- Foetal weight
- Early preterm delivery
- Foetal complications
- Foetal malformations
W 36
2400 g
1 (2%)
Anaemia (n=1), neutropenia (n=1)
Pyloric stenosis (n=1)
Mir O et al; Ann Oncol 2010, Cardonick E et al; Ann Oncol 2012
Taxanes during pregnancy
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Number
- Cisplatin
- Carboplatin
48
47
1
Regimen - Single agent (61.7%)
- Combination with bleomycin, or taxanes (38.3%)
Neonatal outcome
- Mean Gestational age at delivery
- Foetal weight
- Foetal complications
- Foetal malformations
W 33
2200 g
++ creatinin (n=1), intraventricular hge (n=1), hypoglycemia (n=1), hypotension (n=1)
None
Zagouri F et al; Obstet Gynecol 2013
Cisplatin and carboplatin during pregnancy
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Anthracycline (N=328), Taxanes (N=84), Platinum (N=74)
Around 10-20% of patients experienced pregnancy complications.
Need for specialized obstetrical care!
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology
Child’s behavior, general health, hearing and growth was reported as in a general population
Most of the children have an age-adequate neurological development (intelligence, attention, memory) and cardiac function
Prematurity was frequently encountered, and was associated with impairment in cognitive development
Long term effects of gestational chemotherapy on children (n=70)
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

0
5
10
15
20
25
30
Nu
mb
er
<34 weeks 34-37 weeks >37 weeksn=23
0
5
10
15
20
25
30
Nu
mb
er
0
5
10
15
20
25
30
Nu
mb
er
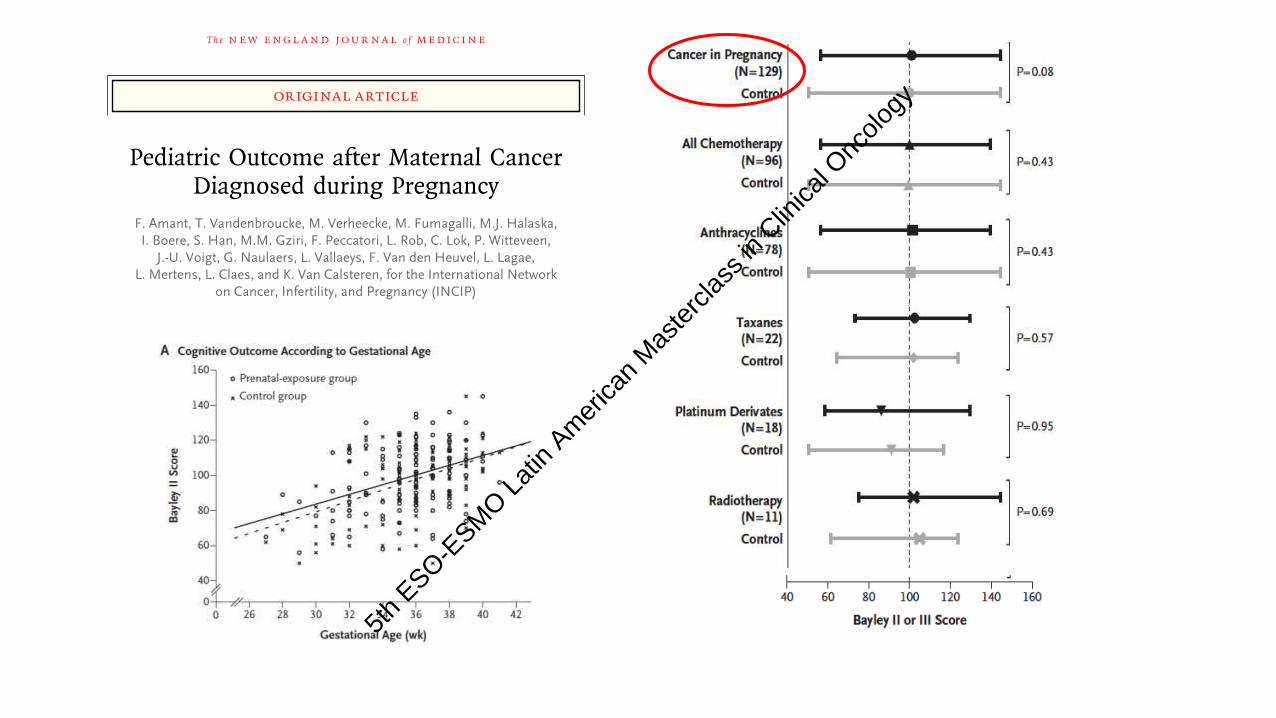
IQ score increases with 2.5 (95% CI:1.2-3.9) for each week increase in pregnancy duration (p= 0.0003).
Long term effects of gestational chemotherapy on children (n=70)
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Peccatori F et al, Nature Rev Clin Oncol 2015
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Conclusions
Effective fertility preservation and care of pregnant cancer
patients need:
Organization
Knowledge
Involvement of all actors (oncologists, ob/gyn, psychologists, family)
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Conclusions
Effective fertility preservation and care of pregnant cancer
patients need:
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology

Thank you!
Fedro Alessandro Peccatori, MD PhD European Institute of Oncology IRCCS, European School of OncologyMilan, Italy
[email protected]@eso.net
+393498357703
5th
ESO-ESM
O Lat
in Am
erica
n M
aste
rclas
s in
Clinica
l Onc
ology