Female Infertility - Department of Radiology
21
Note: This copy is for your personal, non-commercial use only. To order presentation-ready copies for distribution to your colleagues, use the RadioGraphics Reprints form at the end of this article. 1353 EDUCATION EXHIBIT Jill A. Steinkeler, MD • Courtney A. Woodfield, MD • Elizabeth Lazarus, MD Mary M. Hillstrom, MD Imaging plays a key role in the diagnostic evaluation of women for infertility. The pelvic causes of female infertility are varied and range from tubal and peritubal abnormalities to uterine, cervical, and ovar- ian disorders. In most cases, the imaging work-up begins with hystero- salpingography to evaluate fallopian tube patency. Uterine filling defects and contour abnormalities may be discovered at hysterosal- pingography but typically require further characterization with hys- terographic or pelvic ultrasonography (US) or pelvic magnetic reso- nance (MR) imaging. Hysterographic US helps differentiate among uterine synechiae, endometrial polyps, and submucosal leiomyomas. Pelvic US and MR imaging help further differentiate among uterine leiomyomas, adenomyosis, and the various müllerian duct anomalies, with MR imaging being the most sensitive modality for detecting en- dometriosis. The presence of cervical disease may be inferred initially on the basis of difficulty or failure of cervical cannulation at hystero- salpingography. Ovarian abnormalities are usually detected at US. The appropriate selection of imaging modalities and accurate characteriza- tion of the various pelvic causes of infertility are essential because the imaging findings help direct subsequent patient care. © RSNA, 2009 • radiographics.rsna.org Female Infertility: A Systematic Approach to Radiologic Imaging and Diagnosis 1 LEARNING OBJECTIVES FOR TEST 4 After reading this article and taking the test, the reader will be able to: Recognize com- ■ mon tubal, uterine, cervical, and ovarian causes of infertility. Describe the im- ■ portance of hystero- salpingography for evaluating infertility in women. Identify appropri- ■ ate uses of pelvic MR imaging for evaluating infertility in women. Abbreviation: DES = diethylstilbestrol RadioGraphics 2009; 29:1353–1370 • Published online 10.1148/rg.295095047 • Content Codes: 1 From the Department of Diagnostic Imaging, Warren Alpert Medical School of Brown University and Rhode Island Hospital, 593 Eddy St, Provi- dence, RI 02903. Recipient of a Certificate of Merit award for an education exhibit at the 2008 RSNA Annual Meeting. Received March 5, 2009; revision requested March 23 and received May 2; accepted May 8. All authors have no financial relationships to disclose. Address correspondence to J.A.S. (e-mail: [email protected]). © RSNA, 2009 CME FEATURE See accompanying test at http:// www.rsna.org /education /rg_cme.html See last page TEACHING POINTS
Transcript of Female Infertility - Department of Radiology
Note: This copy is for your personal, non-commercial use only. To order presentation-ready copies for distribution to your colleagues, use the RadioGraphics Reprints form at the end of this article.
1353EDUCATION EXHIBIT
Jill A. Steinkeler, MD • Courtney A. Woodfield, MD • Elizabeth Lazarus, MD Mary M. Hillstrom, MD
Imaging plays a key role in the diagnostic evaluation of women for infertility. The pelvic causes of female infertility are varied and range from tubal and peritubal abnormalities to uterine, cervical, and ovar-ian disorders. In most cases, the imaging work-up begins with hystero-salpingography to evaluate fallopian tube patency. Uterine filling defects and contour abnormalities may be discovered at hysterosal-pingography but typically require further characterization with hys-terographic or pelvic ultrasonography (US) or pelvic magnetic reso-nance (MR) imaging. Hysterographic US helps differentiate among uterine synechiae, endometrial polyps, and submucosal leiomyomas. Pelvic US and MR imaging help further differentiate among uterine leiomyomas, adenomyosis, and the various müllerian duct anomalies, with MR imaging being the most sensitive modality for detecting en-dometriosis. The presence of cervical disease may be inferred initially on the basis of difficulty or failure of cervical cannulation at hystero-salpingography. Ovarian abnormalities are usually detected at US. The appropriate selection of imaging modalities and accurate characteriza-tion of the various pelvic causes of infertility are essential because the imaging findings help direct subsequent patient care.©RSNA, 2009 • radiographics.rsna.org
Female Infertility: A Systematic Approach to Radiologic Imaging and Diagnosis1
LEARNING OBJECTIVES FOR TEST 4After reading this article and taking the test, the reader
will be able to:
Recognize com- ■
mon tubal, uterine, cervical, and ovarian causes of infertility.
Describe the im- ■
portance of hystero-salpingography for evaluating infertility in women.
Identify appropri- ■
ate uses of pelvic MR imaging for evaluating infertility in women.
Abbreviation: DES = diethylstilbestrol
RadioGraphics 2009; 29:1353–1370 • Published online 10.1148/rg.295095047 • Content Codes: 1From the Department of Diagnostic Imaging, Warren Alpert Medical School of Brown University and Rhode Island Hospital, 593 Eddy St, Provi-dence, RI 02903. Recipient of a Certificate of Merit award for an education exhibit at the 2008 RSNA Annual Meeting. Received March 5, 2009; revision requested March 23 and received May 2; accepted May 8. All authors have no financial relationships to disclose. Address correspondence to J.A.S. (e-mail: [email protected]).
©RSNA, 2009
CME FEATURESee accompanying
test at http://www.rsna.org
/education/rg_cme.html
See last page
TEACHING POINTS
1354 September-October 2009 radiographics.rsna.org
IntroductionAn estimated 7.4 million women, or 12% of the female population of reproductive age in the United States, were reported to be infertile in the 2002 National Survey of Family Growth (1). The demand for general infertility services showed rapid growth between 1996 and 2004, with a reported 92% increase in the number of assisted reproduction procedures (2). In association with that increase, there has been an increased demand for female infertility imaging services, including hysterosalpingography, hysterographic and pelvic ultrasonography (US), and pelvic magnetic resonance (MR) imaging. The potential causes of female infertility are numerous and may involve the fallopian tubes, peritoneum, endo-metrium, uterus, cervix, and ovaries. Therefore, imaging plays a crucial role in diagnostic work-up and treatment planning for female infertility.
An imaging evaluation for female infertility typically takes place after a clinical assessment. Because tubal occlusion is the most common cause of female infertility, the imaging evaluation begins with hysterosalpingography to determine whether the fallopian tubes are patent. Hys-terosalpingography readily depicts the course, size, and contour as well as patency of the tubes. Peritubal abnormalities due to pelvic adhesions or endometriosis also may be detected; and en-dometrial and uterine abnormalities such as syn-echiae, polyps, leiomyomas, and müllerian duct anomalies may be depicted as filling defects and contour abnormalities, respectively. The findings at hysterosalpingography help the referring clini-cian and radiologist determine the next appropri-ate step in diagnosis and management.
Intrauterine filling defects seen at hysterosalpin-gography are best evaluated with hysterographic US, which can help confirm the presence and characteristics of uterine synechiae, endometrial polyps, and submucosal leiomyomas. Uterine contour abnormalities detected at hysterosalpin-gography may be due to adenomyosis, leiomyomas, or müllerian duct anomalies. While pelvic US may be helpful for further evaluation of uterine contour abnormalities, MR imaging is especially useful
for differentiating between adenomyosis uteri and uterine leiomyomas, which have a similar appear-ance at US. MR imaging provides optimal and ac-curate characterization of müllerian duct anoma-lies, crucial information for predicting pregnancy outcomes and choosing appropriate methods of intervention. Cervical causes of female infertil-ity that can be evaluated with imaging include cervical stenosis, the presence of which may be indicated by an inability to cannulate the external cervical os or by narrowing of the endocervical canal seen at hysterosalpingography. When the cervical appearance at hysterosalpingography is normal, ovarian causes such as premature ovarian failure, gonadal dysgenesis, and polycystic ovary syndrome should be considered. The observation of characteristic features of polycystic ovary syn-drome at US, in combination with clinical symp-toms, may be indicative of the diagnosis.
The article describes the tubal, peritoneal, endometrial, uterine, cervical, and ovarian causes of infertility and illustrates their imag-ing appearances. A systematic multimodality imaging approach is advocated in which initial hysterosalpingography is followed by hystero-graphic US, pelvic US, pelvic MR imaging, or a combination thereof, with the selection of modalities depending on the findings at hysterosalpingography.
Fallopian Tube AbnormalitiesFallopian tube abnormalities are the most com-mon cause of female infertility, accounting for 30%–40% of cases (3). Hysterosalpingography provides optimal depiction of the fallopian tubes, allowing detection of tubal patency, tubal oc-clusion, tubal irregularity, and peritubal disease (4). If there is evidence of occlusion due to en-dometriosis, hysterosalpingography should be followed by MR imaging. A process diagram for diagnostic imaging of fallopian tube abnormali-ties is shown in Figure 1.
Tubal OcclusionThe fallopian tubes have three segments that are visible at hysterosalpingography: the interstitial portion, which traverses the myometrium; the isthmic portion, which courses within the broad
TeachingPoint
RG ■ Volume 29 • Number 5 Steinkeler et al 1355
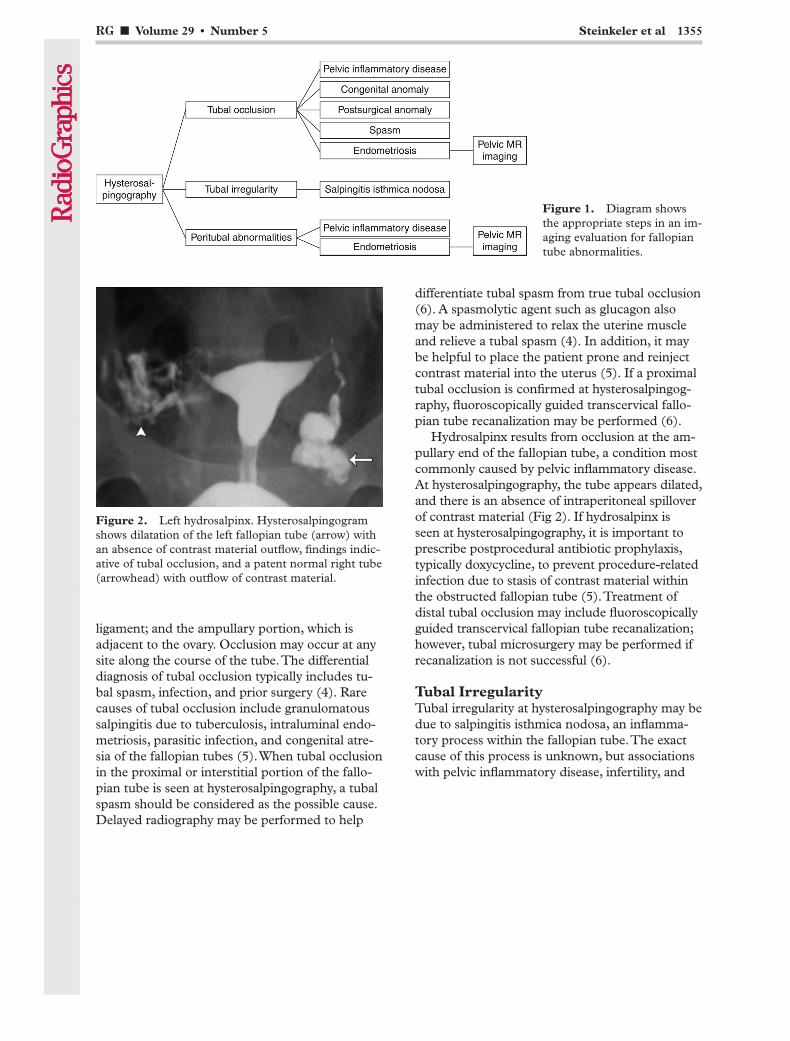
Figure 2. Left hydrosalpinx. Hysterosalpingogram shows dilatation of the left fallopian tube (arrow) with an absence of contrast material outflow, findings indic-ative of tubal occlusion, and a patent normal right tube (arrowhead) with outflow of contrast material.
Figure 1. Diagram shows the appropriate steps in an im-aging evaluation for fallopian tube abnormalities.
ligament; and the ampullary portion, which is adjacent to the ovary. Occlusion may occur at any site along the course of the tube. The differential diagnosis of tubal occlusion typically includes tu-bal spasm, infection, and prior surgery (4). Rare causes of tubal occlusion include granulomatous salpingitis due to tuberculosis, intraluminal endo-metriosis, parasitic infection, and congenital atre-sia of the fallopian tubes (5). When tubal occlusion in the proximal or interstitial portion of the fallo-pian tube is seen at hysterosalpingography, a tubal spasm should be considered as the possible cause. Delayed radiography may be performed to help
differentiate tubal spasm from true tubal occlusion (6). A spasmolytic agent such as glucagon also may be administered to relax the uterine muscle and relieve a tubal spasm (4). In addition, it may be helpful to place the patient prone and reinject contrast material into the uterus (5). If a proximal tubal occlusion is confirmed at hysterosalpingog-raphy, fluoroscopically guided transcervical fallo-pian tube recanalization may be performed (6).
Hydrosalpinx results from occlusion at the am-pullary end of the fallopian tube, a condition most commonly caused by pelvic inflammatory disease. At hysterosalpingography, the tube appears dilated, and there is an absence of intraperitoneal spillover of contrast material (Fig 2). If hydrosalpinx is seen at hysterosalpingography, it is important to prescribe postprocedural antibiotic prophylaxis, typically doxycycline, to prevent procedure-related infection due to stasis of contrast material within the obstructed fallopian tube (5). Treatment of distal tubal occlusion may include fluoroscopically guided transcervical fallopian tube recanalization; however, tubal microsurgery may be performed if recanalization is not successful (6).
Tubal IrregularityTubal irregularity at hysterosalpingography may be due to salpingitis isthmica nodosa, an inflamma-tory process within the fallopian tube. The exact cause of this process is unknown, but associations with pelvic inflammatory disease, infertility, and
1356 September-October 2009 radiographics.rsna.org
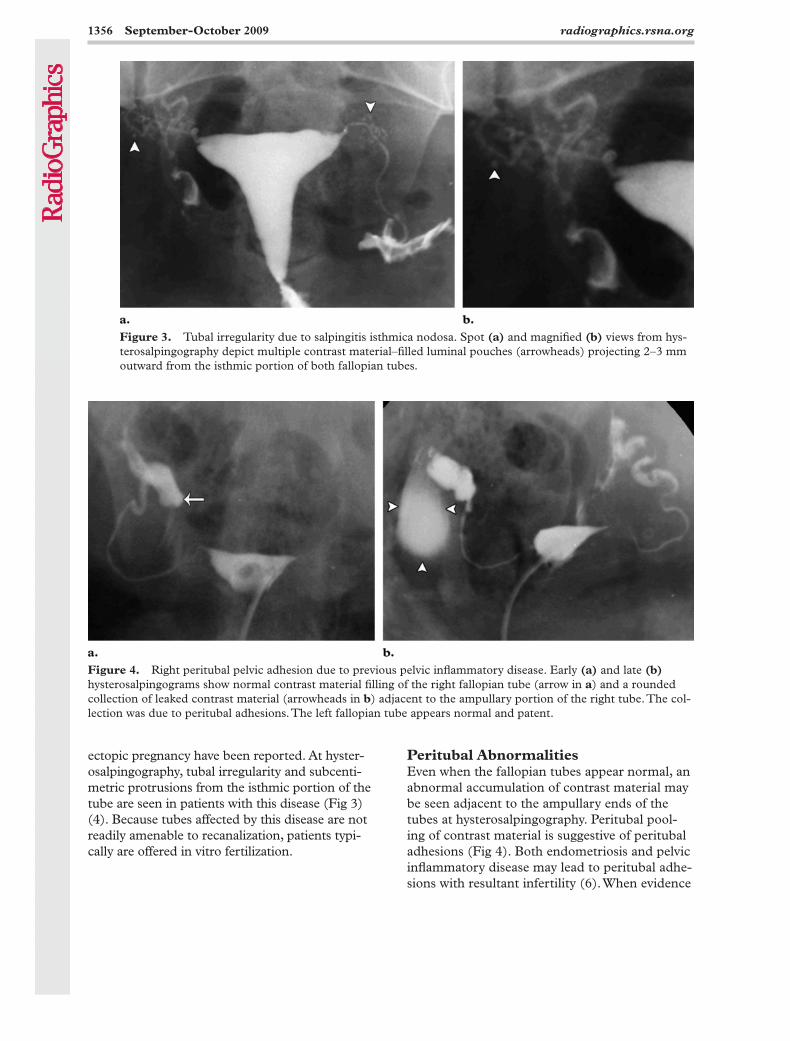
Figure 4. Right peritubal pelvic adhesion due to previous pelvic inflammatory disease. Early (a) and late (b) hysterosalpingograms show normal contrast material filling of the right fallopian tube (arrow in a) and a rounded collection of leaked contrast material (arrowheads in b) adjacent to the ampullary portion of the right tube. The col-lection was due to peritubal adhesions. The left fallopian tube appears normal and patent.
Peritubal AbnormalitiesEven when the fallopian tubes appear normal, an abnormal accumulation of contrast material may be seen adjacent to the ampullary ends of the tubes at hysterosalpingography. Peritubal pool-ing of contrast material is suggestive of peritubal adhesions (Fig 4). Both endometriosis and pelvic inflammatory disease may lead to peritubal adhe-sions with resultant infertility (6). When evidence
ectopic pregnancy have been reported. At hyster-osalpingography, tubal irregularity and subcenti-metric protrusions from the isthmic portion of the tube are seen in patients with this disease (Fig 3) (4). Because tubes affected by this disease are not readily amenable to recanalization, patients typi-cally are offered in vitro fertilization.
Figure 3. Tubal irregularity due to salpingitis isthmica nodosa. Spot (a) and magnified (b) views from hys-terosalpingography depict multiple contrast material–filled luminal pouches (arrowheads) projecting 2–3 mm outward from the isthmic portion of both fallopian tubes.

RG ■ Volume 29 • Number 5 Steinkeler et al 1357
Figure 6. Endometriosis. Unenhanced axial T1-weighted fat-suppressed MR image shows dilatation of the right fallopian tube (arrow) with internal high signal intensity due to blood products, findings indica-tive of hematosalpinx. Smaller high-signal-intensity foci along the posterior uterine serosa (arrowhead) are indicative of endometrial implants.
Figure 5. Endometrioma. Sagittal transvaginal US image obtained in a woman with a history of endo-metriosis shows an ovarian mass with multiple fine internal echoes (arrows) and several hyperechoic mural foci (arrowheads).
women have endometriosis, a condition defined by the presence of endometrial glands and stroma outside the uterus (7). This condition almost exclusively affects women during their reproduc-tive years. It may be asymptomatic or may cause multiple symptoms, including pelvic pain and infertility (8,9). Imaging tests for endometriosis include pelvic US and MR imaging. Endometrio-sis may take the form of either small implants or cysts that change in size and appearance dur-ing the menstrual cycle and that may initiate an inflammatory response leading to fibrosis and adhesions. Endometriotic cysts, referred to as endometriomas, result from repeated hemorrhage within an implant.
The US features of endometriosis are vari-able; US has low sensitivity for the detection of focal implants, but it may depict endometriomas (8,10). Endometriomas have a variable appear-ance, with the most specific US signs being an adnexal mass with faint internal echoes and highly echogenic mural foci (Fig 5) (9). They generally occur within the ovary, often bilaterally. The sensitivity and specificity of MR imaging for the identification of endometriosis are higher (71% and 82%, respectively) than those of US (11). MR imaging features of endometriosis in-clude cystic masses with thickened walls and loss of the interface between the lesion and adjacent organs. The masses have internal high signal intensity on T1-weighted images and low signal intensity on T2-weighted images. Other high-signal-intensity features seen on T1-weighted im-ages may include hydrosalpinx (the luminal con-tents of which may include blood products) and endometrial implants (Fig 6) (3,9,12). However, the sensitivity (13%) of MR imaging for the de-tection of endometrial implants is low (13). For this reason, MR imaging alone cannot take the place of laparoscopy for the definitive diagnosis of endometriosis (11,13).
Intrauterine Filling DefectsIntrauterine filling defects seen at hysterosalpin-gography may be caused by air bubbles in the contrast material injection, intrauterine adhe-sions, submucosal leiomyomas, endometrial polyps, or blood clots. Bilateral oblique views may help identify mobile, nondependent, round filling defects caused by air bubbles and to avoid mistaking these findings for intrauterine disease.
of peritubal adhesions is seen at hysterosalpin- gography, pelvic MR imaging is particularly help-ful for further noninvasive evaluation.
EndometriosisAn estimated 30%–50% of women with en-dometriosis are infertile, and 20% of infertile
1358 September-October 2009 radiographics.rsna.org
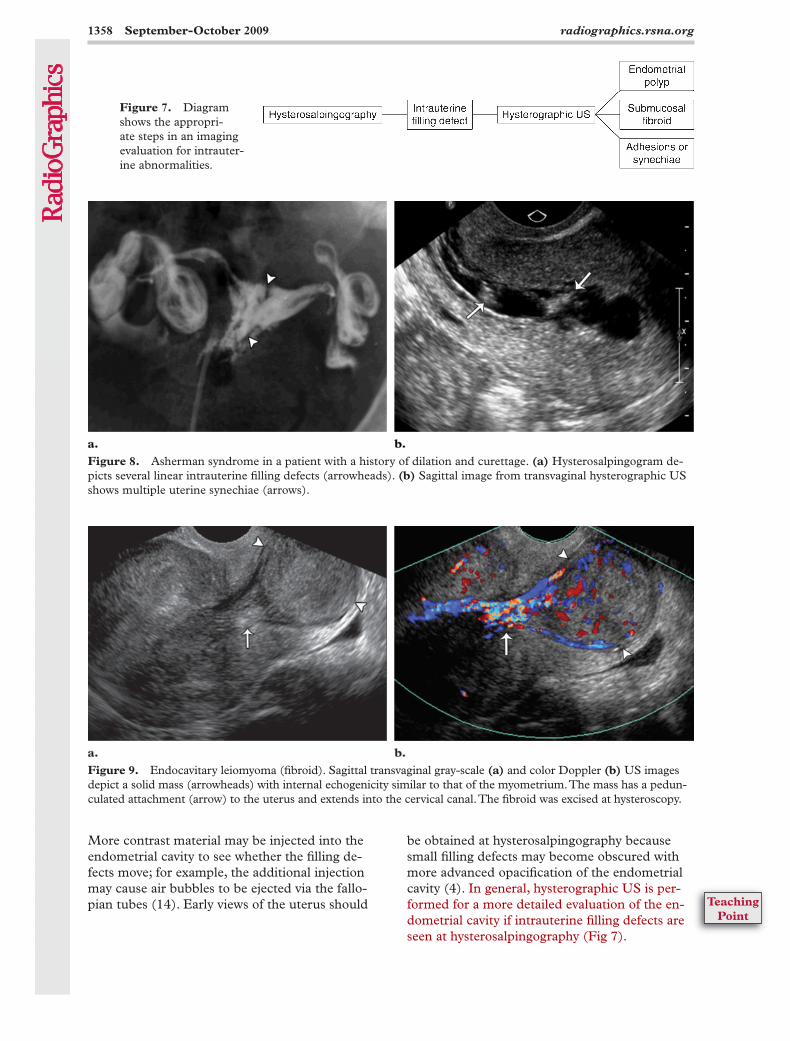
Figure 9. Endocavitary leiomyoma (fibroid). Sagittal transvaginal gray-scale (a) and color Doppler (b) US images depict a solid mass (arrowheads) with internal echogenicity similar to that of the myometrium. The mass has a pedun-culated attachment (arrow) to the uterus and extends into the cervical canal. The fibroid was excised at hysteroscopy.
Figure 8. Asherman syndrome in a patient with a history of dilation and curettage. (a) Hysterosalpingogram de-picts several linear intrauterine filling defects (arrowheads). (b) Sagittal image from transvaginal hysterographic US shows multiple uterine synechiae (arrows).
Figure 7. Diagram shows the appropri-ate steps in an imaging evaluation for intrauter-ine abnormalities.
More contrast material may be injected into the endometrial cavity to see whether the filling de-fects move; for example, the additional injection may cause air bubbles to be ejected via the fallo-pian tubes (14). Early views of the uterus should
be obtained at hysterosalpingography because small filling defects may become obscured with more advanced opacification of the endometrial cavity (4). In general, hysterographic US is per-formed for a more detailed evaluation of the en-dometrial cavity if intrauterine filling defects are seen at hysterosalpingography (Fig 7).
TeachingPoint
RG ■ Volume 29 • Number 5 Steinkeler et al 1359
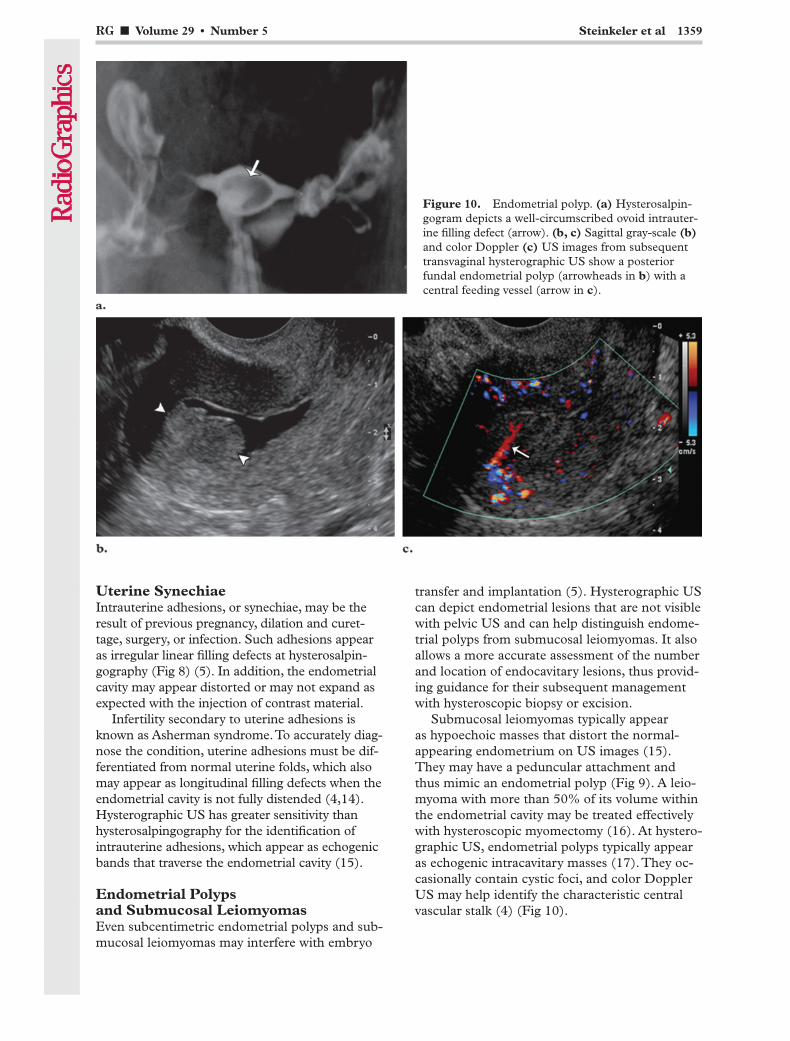
Uterine SynechiaeIntrauterine adhesions, or synechiae, may be the result of previous pregnancy, dilation and curet-tage, surgery, or infection. Such adhesions appear as irregular linear filling defects at hysterosalpin-gography (Fig 8) (5). In addition, the endometrial cavity may appear distorted or may not expand as expected with the injection of contrast material.
Infertility secondary to uterine adhesions is known as Asherman syndrome. To accurately diag-nose the condition, uterine adhesions must be dif-ferentiated from normal uterine folds, which also may appear as longitudinal filling defects when the endometrial cavity is not fully distended (4,14). Hysterographic US has greater sensitivity than hysterosalpingography for the identification of intrauterine adhesions, which appear as echogenic bands that traverse the endometrial cavity (15).
Endometrial Polyps and Submucosal LeiomyomasEven subcentimetric endometrial polyps and sub-mucosal leiomyomas may interfere with embryo
transfer and implantation (5). Hysterographic US can depict endometrial lesions that are not visible with pelvic US and can help distinguish endome-trial polyps from submucosal leiomyomas. It also allows a more accurate assessment of the number and location of endocavitary lesions, thus provid-ing guidance for their subsequent management with hysteroscopic biopsy or excision.
Submucosal leiomyomas typically appear as hypoechoic masses that distort the normal-appearing endometrium on US images (15). They may have a peduncular attachment and thus mimic an endometrial polyp (Fig 9). A leio-myoma with more than 50% of its volume within the endometrial cavity may be treated effectively with hysteroscopic myomectomy (16). At hystero-graphic US, endometrial polyps typically appear as echogenic intracavitary masses (17). They oc-casionally contain cystic foci, and color Doppler US may help identify the characteristic central vascular stalk (4) (Fig 10).
Figure 10. Endometrial polyp. (a) Hysterosalpin-gogram depicts a well-circumscribed ovoid intrauter-ine filling defect (arrow). (b, c) Sagittal gray-scale (b) and color Doppler (c) US images from subsequent transvaginal hysterographic US show a posterior fundal endometrial polyp (arrowheads in b) with a central feeding vessel (arrow in c).
1360 September-October 2009 radiographics.rsna.org
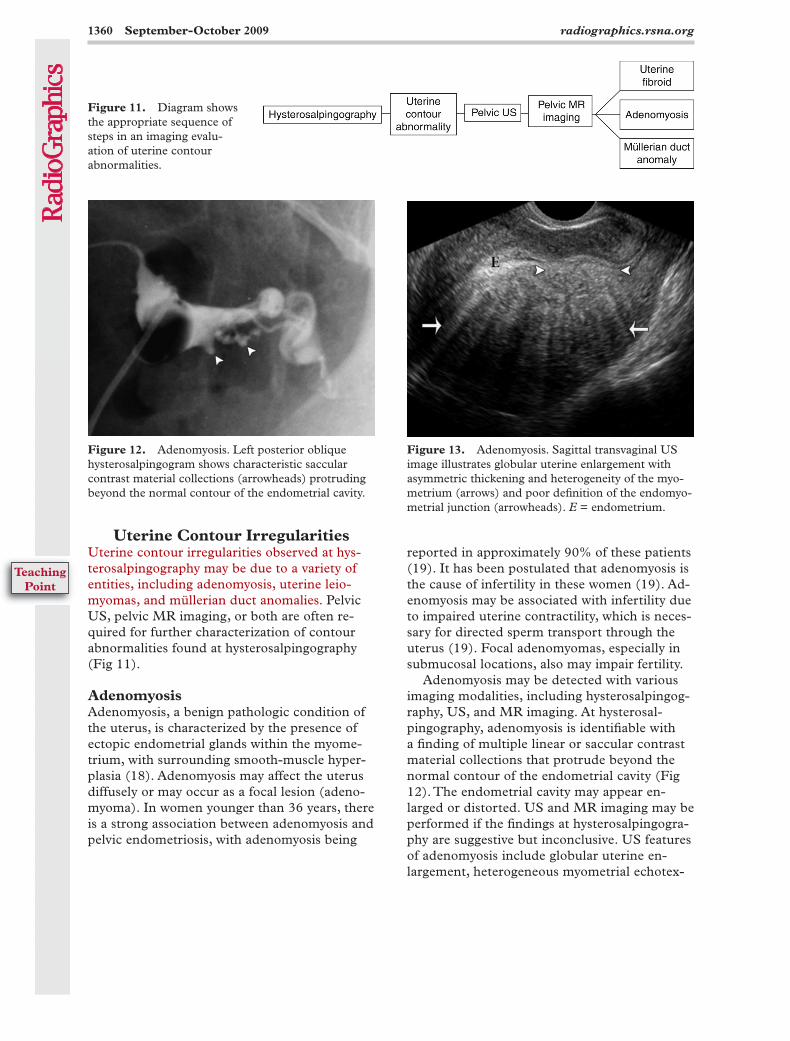
Figure 13. Adenomyosis. Sagittal transvaginal US image illustrates globular uterine enlargement with asymmetric thickening and heterogeneity of the myo-metrium (arrows) and poor definition of the endomyo-metrial junction (arrowheads). E = endometrium.
Figure 12. Adenomyosis. Left posterior oblique hysterosalpingogram shows characteristic saccular contrast material collections (arrowheads) protruding beyond the normal contour of the endometrial cavity.
reported in approximately 90% of these patients (19). It has been postulated that adenomyosis is the cause of infertility in these women (19). Ad-enomyosis may be associated with infertility due to impaired uterine contractility, which is neces-sary for directed sperm transport through the uterus (19). Focal adenomyomas, especially in submucosal locations, also may impair fertility.
Adenomyosis may be detected with various imaging modalities, including hysterosalpingog-raphy, US, and MR imaging. At hysterosal-pingography, adenomyosis is identifiable with a finding of multiple linear or saccular contrast material collections that protrude beyond the normal contour of the endometrial cavity (Fig 12). The endometrial cavity may appear en-larged or distorted. US and MR imaging may be performed if the findings at hysterosalpingogra-phy are suggestive but inconclusive. US features of adenomyosis include globular uterine en-largement, heterogeneous myometrial echotex-
Uterine Contour IrregularitiesUterine contour irregularities observed at hys-terosalpingography may be due to a variety of entities, including adenomyosis, uterine leio-myomas, and müllerian duct anomalies. Pelvic US, pelvic MR imaging, or both are often re-quired for further characterization of contour abnormalities found at hysterosalpingography (Fig 11).
AdenomyosisAdenomyosis, a benign pathologic condition of the uterus, is characterized by the presence of ectopic endometrial glands within the myome-trium, with surrounding smooth-muscle hyper-plasia (18). Adenomyosis may affect the uterus diffusely or may occur as a focal lesion (adeno-myoma). In women younger than 36 years, there is a strong association between adenomyosis and pelvic endometriosis, with adenomyosis being
Figure 11. Diagram shows the appropriate sequence of steps in an imaging evalu-ation of uterine contour abnormalities.
TeachingPoint
RG ■ Volume 29 • Number 5 Steinkeler et al 1361
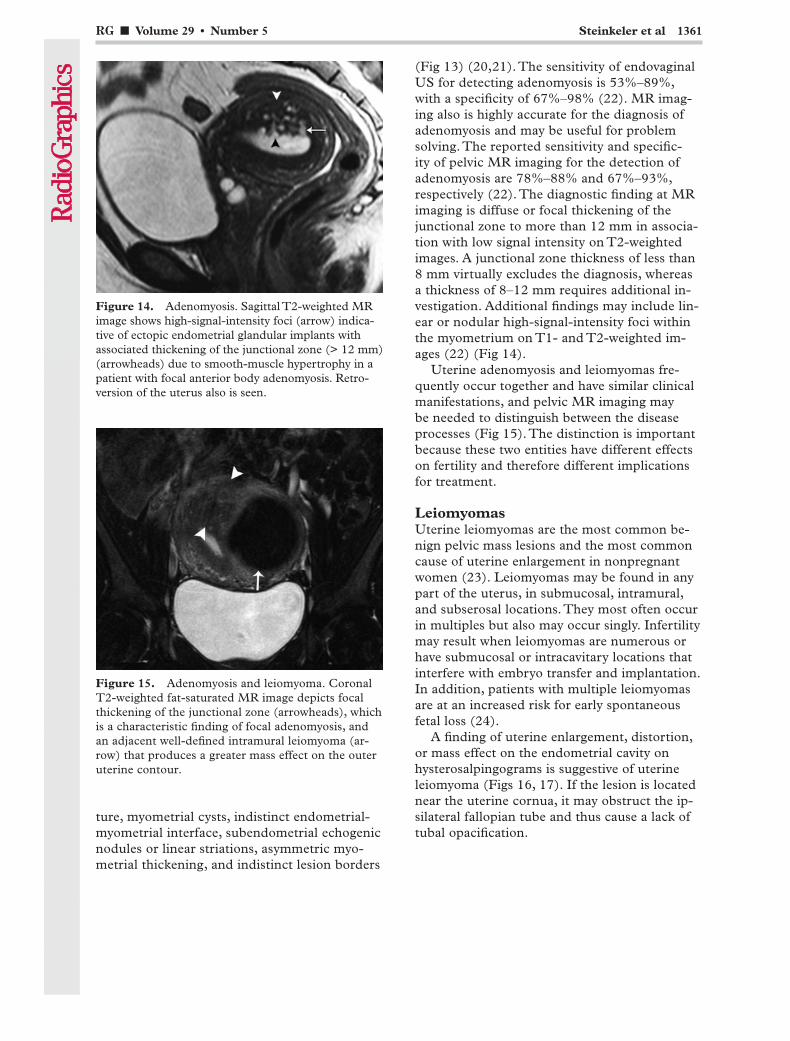
Figure 15. Adenomyosis and leiomyoma. Coronal T2-weighted fat-saturated MR image depicts focal thickening of the junctional zone (arrowheads), which is a characteristic finding of focal adenomyosis, and an adjacent well-defined intramural leiomyoma (ar-row) that produces a greater mass effect on the outer uterine contour.
Figure 14. Adenomyosis. Sagittal T2-weighted MR image shows high-signal-intensity foci (arrow) indica-tive of ectopic endometrial glandular implants with associated thickening of the junctional zone (> 12 mm) (arrowheads) due to smooth-muscle hypertrophy in a patient with focal anterior body adenomyosis. Retro-version of the uterus also is seen.
ture, myometrial cysts, indistinct endometrial-myometrial interface, subendometrial echogenic nodules or linear striations, asymmetric myo-metrial thickening, and indistinct lesion borders
(Fig 13) (20,21). The sensitivity of endovaginal US for detecting adenomyosis is 53%–89%, with a specificity of 67%–98% (22). MR imag-ing also is highly accurate for the diagnosis of adenomyosis and may be useful for problem solving. The reported sensitivity and specific-ity of pelvic MR imaging for the detection of adenomyosis are 78%–88% and 67%–93%, respectively (22). The diagnostic finding at MR imaging is diffuse or focal thickening of the junctional zone to more than 12 mm in associa-tion with low signal intensity on T2-weighted images. A junctional zone thickness of less than 8 mm virtually excludes the diagnosis, whereas a thickness of 8–12 mm requires additional in-vestigation. Additional findings may include lin-ear or nodular high-signal-intensity foci within the myometrium on T1- and T2-weighted im-ages (22) (Fig 14).
Uterine adenomyosis and leiomyomas fre-quently occur together and have similar clinical manifestations, and pelvic MR imaging may be needed to distinguish between the disease processes (Fig 15). The distinction is important because these two entities have different effects on fertility and therefore different implications for treatment.
LeiomyomasUterine leiomyomas are the most common be-nign pelvic mass lesions and the most common cause of uterine enlargement in nonpregnant women (23). Leiomyomas may be found in any part of the uterus, in submucosal, intramural, and subserosal locations. They most often occur in multiples but also may occur singly. Infertility may result when leiomyomas are numerous or have submucosal or intracavitary locations that interfere with embryo transfer and implantation. In addition, patients with multiple leiomyomas are at an increased risk for early spontaneous fetal loss (24).
A finding of uterine enlargement, distortion, or mass effect on the endometrial cavity on hysterosalpingograms is suggestive of uterine leiomyoma (Figs 16, 17). If the lesion is located near the uterine cornua, it may obstruct the ip-silateral fallopian tube and thus cause a lack of tubal opacification.
1362 September-October 2009 radiographics.rsna.org
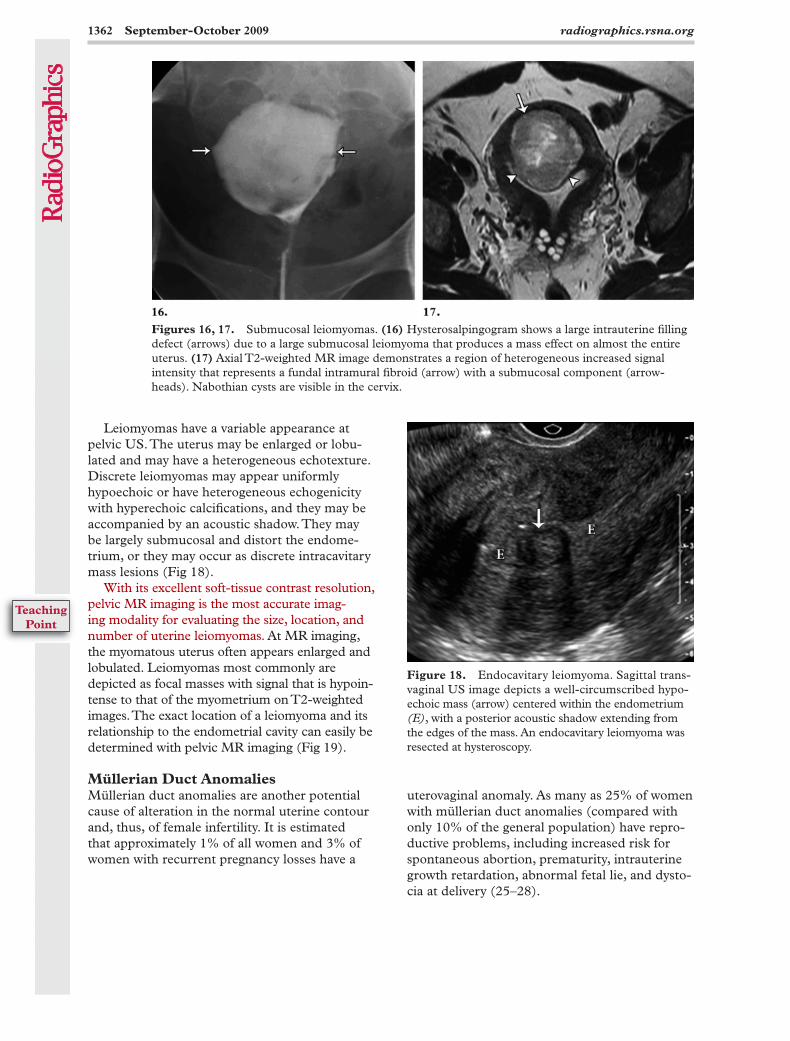
Figure 18. Endocavitary leiomyoma. Sagittal trans- vaginal US image depicts a well-circumscribed hypo-echoic mass (arrow) centered within the endometrium (E), with a posterior acoustic shadow extending from the edges of the mass. An endocavitary leiomyoma was resected at hysteroscopy.
Leiomyomas have a variable appearance at pelvic US. The uterus may be enlarged or lobu-lated and may have a heterogeneous echotexture. Discrete leiomyomas may appear uniformly hypoechoic or have heterogeneous echogenicity with hyperechoic calcifications, and they may be accompanied by an acoustic shadow. They may be largely submucosal and distort the endome-trium, or they may occur as discrete intracavitary mass lesions (Fig 18).
With its excellent soft-tissue contrast resolution, pelvic MR imaging is the most accurate imag-ing modality for evaluating the size, location, and number of uterine leiomyomas. At MR imaging, the myomatous uterus often appears enlarged and lobulated. Leiomyomas most commonly are depicted as focal masses with signal that is hypoin-tense to that of the myometrium on T2-weighted images. The exact location of a leiomyoma and its relationship to the endometrial cavity can easily be determined with pelvic MR imaging (Fig 19).
Müllerian Duct AnomaliesMüllerian duct anomalies are another potential cause of alteration in the normal uterine contour and, thus, of female infertility. It is estimated that approximately 1% of all women and 3% of women with recurrent pregnancy losses have a
uterovaginal anomaly. As many as 25% of women with müllerian duct anomalies (compared with only 10% of the general population) have repro-ductive problems, including increased risk for spontaneous abortion, prematurity, intrauterine growth retardation, abnormal fetal lie, and dysto-cia at delivery (25–28).
Figures 16, 17. Submucosal leiomyomas. (16) Hysterosalpingogram shows a large intrauterine filling defect (arrows) due to a large submucosal leiomyoma that produces a mass effect on almost the entire uterus. (17) Axial T2-weighted MR image demonstrates a region of heterogeneous increased signal intensity that represents a fundal intramural fibroid (arrow) with a submucosal component (arrow-heads). Nabothian cysts are visible in the cervix.
TeachingPoint
RG ■ Volume 29 • Number 5 Steinkeler et al 1363
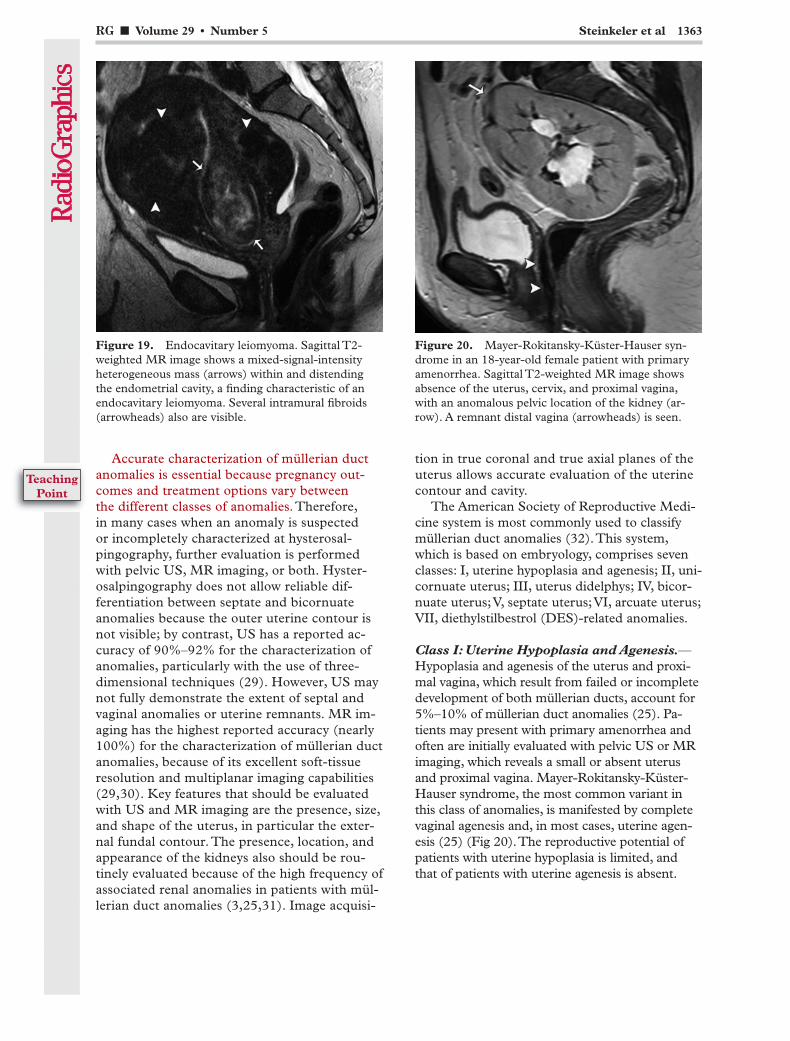
Figure 20. Mayer-Rokitansky-Küster-Hauser syn-drome in an 18-year-old female patient with primary amenorrhea. Sagittal T2-weighted MR image shows absence of the uterus, cervix, and proximal vagina, with an anomalous pelvic location of the kidney (ar-row). A remnant distal vagina (arrowheads) is seen.
Figure 19. Endocavitary leiomyoma. Sagittal T2-weighted MR image shows a mixed-signal-intensity heterogeneous mass (arrows) within and distending the endometrial cavity, a finding characteristic of an endocavitary leiomyoma. Several intramural fibroids (arrowheads) also are visible.
Accurate characterization of müllerian duct anomalies is essential because pregnancy out-comes and treatment options vary between the different classes of anomalies. Therefore, in many cases when an anomaly is suspected or incompletely characterized at hysterosal-pingography, further evaluation is performed with pelvic US, MR imaging, or both. Hyster-osalpingography does not allow reliable dif-ferentiation between septate and bicornuate anomalies because the outer uterine contour is not visible; by contrast, US has a reported ac-curacy of 90%–92% for the characterization of anomalies, particularly with the use of three-dimensional techniques (29). However, US may not fully demonstrate the extent of septal and vaginal anomalies or uterine remnants. MR im-aging has the highest reported accuracy (nearly 100%) for the characterization of müllerian duct anomalies, because of its excellent soft-tissue resolution and multiplanar imaging capabilities (29,30). Key features that should be evaluated with US and MR imaging are the presence, size, and shape of the uterus, in particular the exter-nal fundal contour. The presence, location, and appearance of the kidneys also should be rou-tinely evaluated because of the high frequency of associated renal anomalies in patients with mül-lerian duct anomalies (3,25,31). Image acquisi-
tion in true coronal and true axial planes of the uterus allows accurate evaluation of the uterine contour and cavity.
The American Society of Reproductive Medi-cine system is most commonly used to classify müllerian duct anomalies (32). This system, which is based on embryology, comprises seven classes: I, uterine hypoplasia and agenesis; II, uni-cornuate uterus; III, uterus didelphys; IV, bicor-nuate uterus; V, septate uterus; VI, arcuate uterus; VII, diethylstilbestrol (DES)-related anomalies.
Class I: Uterine Hypoplasia and Agenesis.—Hypoplasia and agenesis of the uterus and proxi-mal vagina, which result from failed or incomplete development of both müllerian ducts, account for 5%–10% of müllerian duct anomalies (25). Pa-tients may present with primary amenorrhea and often are initially evaluated with pelvic US or MR imaging, which reveals a small or absent uterus and proximal vagina. Mayer-Rokitansky-Küster-Hauser syndrome, the most common variant in this class of anomalies, is manifested by complete vaginal agenesis and, in most cases, uterine agen-esis (25) (Fig 20). The reproductive potential of patients with uterine hypoplasia is limited, and that of patients with uterine agenesis is absent.
TeachingPoint
1364 September-October 2009 radiographics.rsna.org
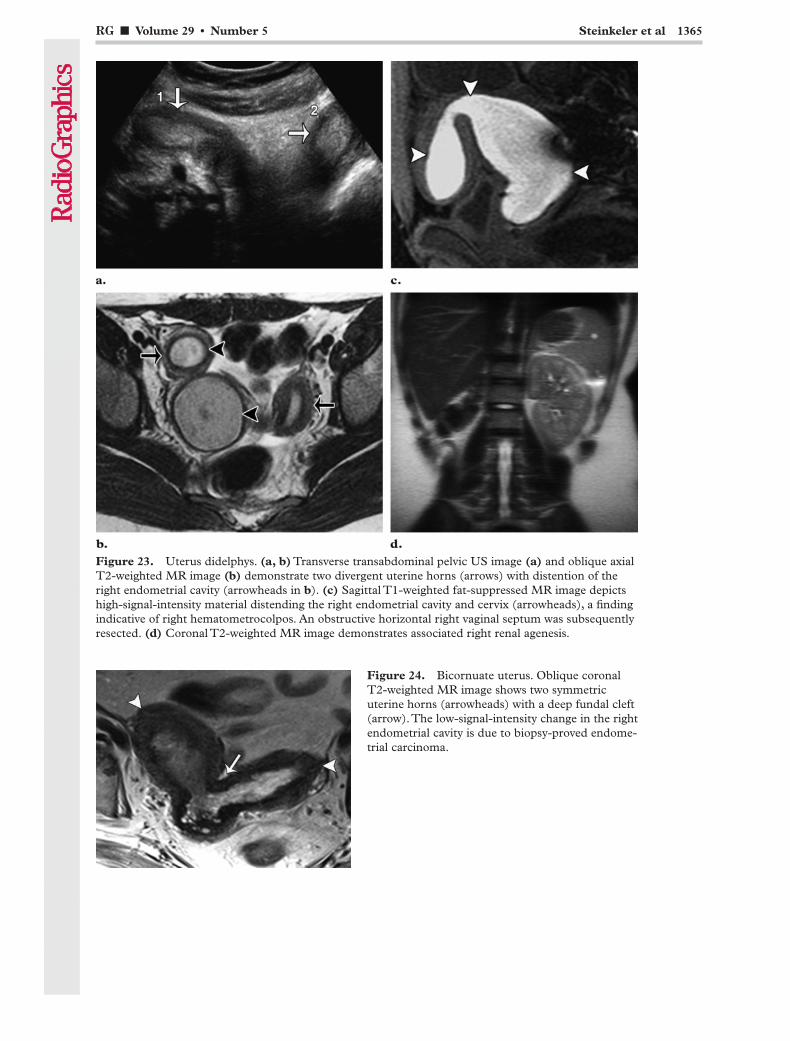
75% of cases, a longitudinal vaginal septum is pre-sent, with or without a unilateral horizontal vaginal septum and resultant unilateral hematometrocol-pos (34) (Fig 23). Metroplasty may be performed in patients who have experienced recurrent spon-taneous abortions or preterm deliveries, but the benefit of such surgery remains unclear (35).
Class IV: Bicornuate Uterus.—Incomplete fu-sion of the müllerian ducts results in a bicornuate uterus, a condition that accounts for approxi-mately 10% of uterine anomalies (25). In patients with this condition, hysterosalpingography shows two symmetric but divergent uterine horns. US and MR imaging may help confirm the presence of a bicornuate uterus by depicting a deep (> 1 cm) fundal cleft in the outer uterine contour and an intercornual distance of more than 4 cm (Fig 24) (29). In some patients, US and MR imaging show two separate cervical canals; in such a case,
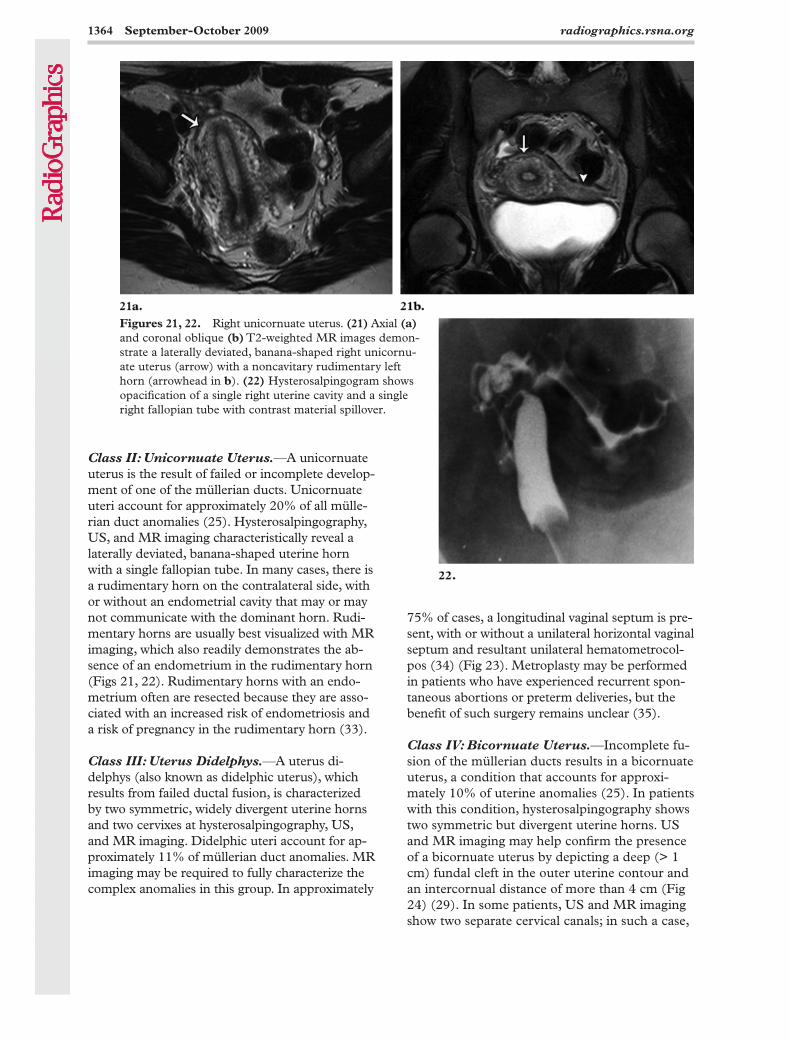
Figures 21, 22. Right unicornuate uterus. (21) Axial (a) and coronal oblique (b) T2-weighted MR images demon-strate a laterally deviated, banana-shaped right unicornu-ate uterus (arrow) with a noncavitary rudimentary left horn (arrowhead in b). (22) Hysterosalpingogram shows opacification of a single right uterine cavity and a single right fallopian tube with contrast material spillover.
Class II: Unicornuate Uterus.—A unicornuate uterus is the result of failed or incomplete develop-ment of one of the müllerian ducts. Unicornuate uteri account for approximately 20% of all mülle-rian duct anomalies (25). Hysterosalpingography, US, and MR imaging characteristically reveal a laterally deviated, banana-shaped uterine horn with a single fallopian tube. In many cases, there is a rudimentary horn on the contralateral side, with or without an endometrial cavity that may or may not communicate with the dominant horn. Rudi-mentary horns are usually best visualized with MR imaging, which also readily demonstrates the ab-sence of an endometrium in the rudimentary horn (Figs 21, 22). Rudimentary horns with an endo-metrium often are resected because they are asso-ciated with an increased risk of endometriosis and a risk of pregnancy in the rudimentary horn (33).
Class III: Uterus Didelphys.—A uterus di-delphys (also known as didelphic uterus), which results from failed ductal fusion, is characterized by two symmetric, widely divergent uterine horns and two cervixes at hysterosalpingography, US, and MR imaging. Didelphic uteri account for ap-proximately 11% of müllerian duct anomalies. MR imaging may be required to fully characterize the complex anomalies in this group. In approximately
RG ■ Volume 29 • Number 5 Steinkeler et al 1365
Figure 23. Uterus didelphys. (a, b) Transverse transabdominal pelvic US image (a) and oblique axial T2-weighted MR image (b) demonstrate two divergent uterine horns (arrows) with distention of the right endometrial cavity (arrowheads in b). (c) Sagittal T1-weighted fat-suppressed MR image depicts high-signal-intensity material distending the right endometrial cavity and cervix (arrowheads), a finding indicative of right hematometrocolpos. An obstructive horizontal right vaginal septum was subsequently resected. (d) Coronal T2-weighted MR image demonstrates associated right renal agenesis.
Figure 24. Bicornuate uterus. Oblique coronal T2-weighted MR image shows two symmetric uterine horns (arrowheads) with a deep fundal cleft (arrow). The low-signal-intensity change in the right endometrial cavity is due to biopsy-proved endome-trial carcinoma.
1366 September-October 2009 radiographics.rsna.org
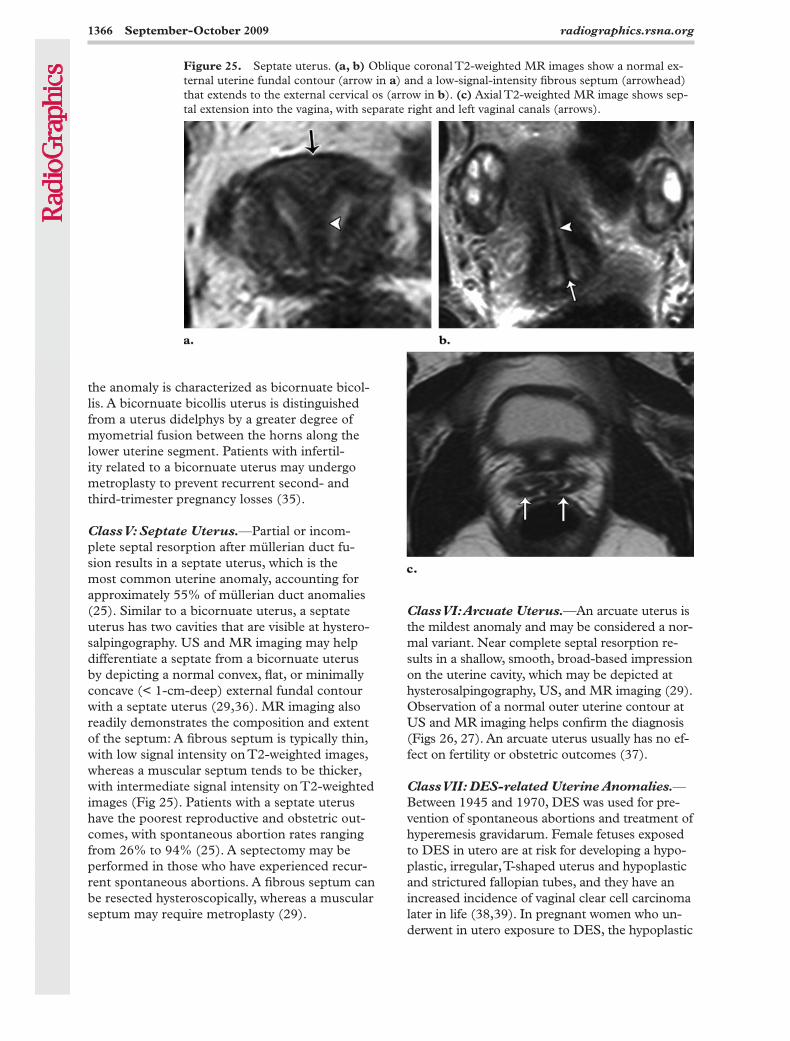
Class VI: Arcuate Uterus.—An arcuate uterus is the mildest anomaly and may be considered a nor-mal variant. Near complete septal resorption re-sults in a shallow, smooth, broad-based impression on the uterine cavity, which may be depicted at hysterosalpingography, US, and MR imaging (29). Observation of a normal outer uterine contour at US and MR imaging helps confirm the diagnosis (Figs 26, 27). An arcuate uterus usually has no ef-fect on fertility or obstetric outcomes (37).
Class VII: DES-related Uterine Anomalies.—Between 1945 and 1970, DES was used for pre-vention of spontaneous abortions and treatment of hyperemesis gravidarum. Female fetuses exposed to DES in utero are at risk for developing a hypo-plastic, irregular, T-shaped uterus and hypoplastic and strictured fallopian tubes, and they have an increased incidence of vaginal clear cell carcinoma later in life (38,39). In pregnant women who un-derwent in utero exposure to DES, the hypoplastic
Figure 25. Septate uterus. (a, b) Oblique coronal T2-weighted MR images show a normal ex-ternal uterine fundal contour (arrow in a) and a low-signal-intensity fibrous septum (arrowhead) that extends to the external cervical os (arrow in b). (c) Axial T2-weighted MR image shows sep-tal extension into the vagina, with separate right and left vaginal canals (arrows).
the anomaly is characterized as bicornuate bicol-lis. A bicornuate bicollis uterus is distinguished from a uterus didelphys by a greater degree of myometrial fusion between the horns along the lower uterine segment. Patients with infertil-ity related to a bicornuate uterus may undergo metroplasty to prevent recurrent second- and third-trimester pregnancy losses (35).
Class V: Septate Uterus.—Partial or incom-plete septal resorption after müllerian duct fu-sion results in a septate uterus, which is the most common uterine anomaly, accounting for approximately 55% of müllerian duct anomalies (25). Similar to a bicornuate uterus, a septate uterus has two cavities that are visible at hystero-salpingography. US and MR imaging may help differentiate a septate from a bicornuate uterus by depicting a normal convex, flat, or minimally concave (< 1-cm-deep) external fundal contour with a septate uterus (29,36). MR imaging also readily demonstrates the composition and extent of the septum: A fibrous septum is typically thin, with low signal intensity on T2-weighted images, whereas a muscular septum tends to be thicker, with intermediate signal intensity on T2-weighted images (Fig 25). Patients with a septate uterus have the poorest reproductive and obstetric out-comes, with spontaneous abortion rates ranging from 26% to 94% (25). A septectomy may be performed in those who have experienced recur-rent spontaneous abortions. A fibrous septum can be resected hysteroscopically, whereas a muscular septum may require metroplasty (29).
RG ■ Volume 29 • Number 5 Steinkeler et al 1367
Figure 28. DES-related uterine anomaly. Hysterosal-pingogram demonstrates a hypoplastic T-shaped uterus. The patient had been exposed to DES while in utero.
Figures 26, 27. Arcuate uterus. Three-dimensional coronal US image (26) and coronal oblique T2-weighted MR image (27), obtained in different patients, show a smooth, broad-based, shallow endometrial impression (arrow) with a normal external contour of the uterine fundus (arrowhead).
uterus incurs a higher risk of spontaneous abor-tion, preterm delivery, and ectopic pregnancy. The classic features of DES-related uterine anomalies, unlike other classes of müllerian duct anomalies, are best depicted by hysterosalpingography (Fig 28). Hysteroscopic dilation of the uterine cavity may improve reproductive outcomes (40).
Cervical Abnormalities
Cervical Factor InfertilityThe phrase cervical factor infertility connotes an inadequate quality or volume of cervical mucus, a condition that accounts for approximately 10% of cases of female infertility. Patients in
whom the presence of this condition is sus-pected may be assessed with a postcoital test that does not involve imaging.
Cervical StenosisThe term cervical stenosis is clinically defined as cervical narrowing that prevents the insertion of a 2.5-mm-wide dilator (41). This condition may be congenital or secondary to infection or trauma. Risk factors include previous cone biopsy, cryo-therapy, laser treatment, and biopsy for cervical dysplasia (42,43). The more severe the stenosis, the more likely it is to be symptomatic (43). Con-sequences of cervical stenosis include obstruction of menstrual flow with resulting amenorrhea, dys-menorrhea, and potential infertility due to inability of sperm to enter the upper genital tract (41). Cer-vical stenosis also may be a serious impediment to assisted fertility techniques including embryo transfer and intrauterine insemination (42).
At hysterosalpingography, cervical stenosis may appear as narrowing of the endocervical canal (normal diameter, 0.5–3.0 cm), or it may manifest as complete obliteration of the cervical os, preventing insertion of the hysterosalpingo-graphic catheter (44). Observations of narrowing of the endocervical canal on hysterosalpingo-grams should be correlated with clinical findings, because the diameter of the normal endocervical canal and internal os may vary (45). Masses such as cervical polyps, fibroids, and neoplasms also may cause narrowing of the cervical lumen (45).
1368 September-October 2009 radiographics.rsna.org
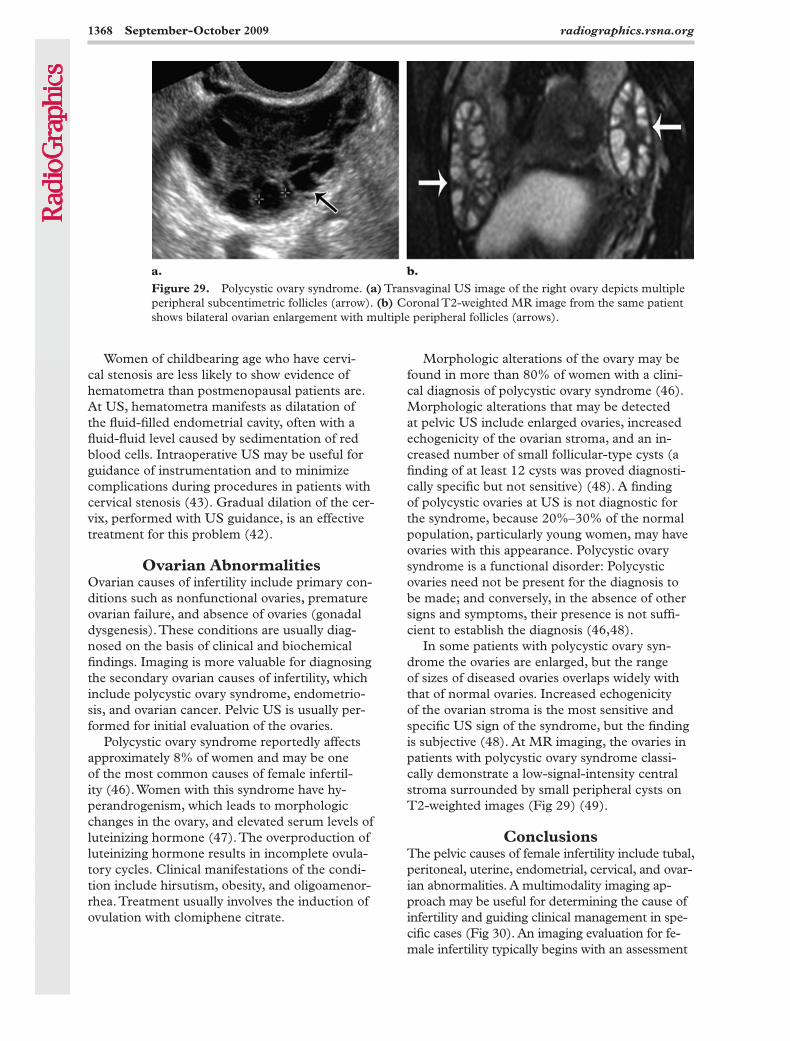
Morphologic alterations of the ovary may be found in more than 80% of women with a clini-cal diagnosis of polycystic ovary syndrome (46). Morphologic alterations that may be detected at pelvic US include enlarged ovaries, increased echogenicity of the ovarian stroma, and an in-creased number of small follicular-type cysts (a finding of at least 12 cysts was proved diagnosti-cally specific but not sensitive) (48). A finding of polycystic ovaries at US is not diagnostic for the syndrome, because 20%–30% of the normal population, particularly young women, may have ovaries with this appearance. Polycystic ovary syndrome is a functional disorder: Polycystic ovaries need not be present for the diagnosis to be made; and conversely, in the absence of other signs and symptoms, their presence is not suffi-cient to establish the diagnosis (46,48).
In some patients with polycystic ovary syn-drome the ovaries are enlarged, but the range of sizes of diseased ovaries overlaps widely with that of normal ovaries. Increased echogenicity of the ovarian stroma is the most sensitive and specific US sign of the syndrome, but the finding is subjective (48). At MR imaging, the ovaries in patients with polycystic ovary syndrome classi-cally demonstrate a low-signal-intensity central stroma surrounded by small peripheral cysts on T2-weighted images (Fig 29) (49).
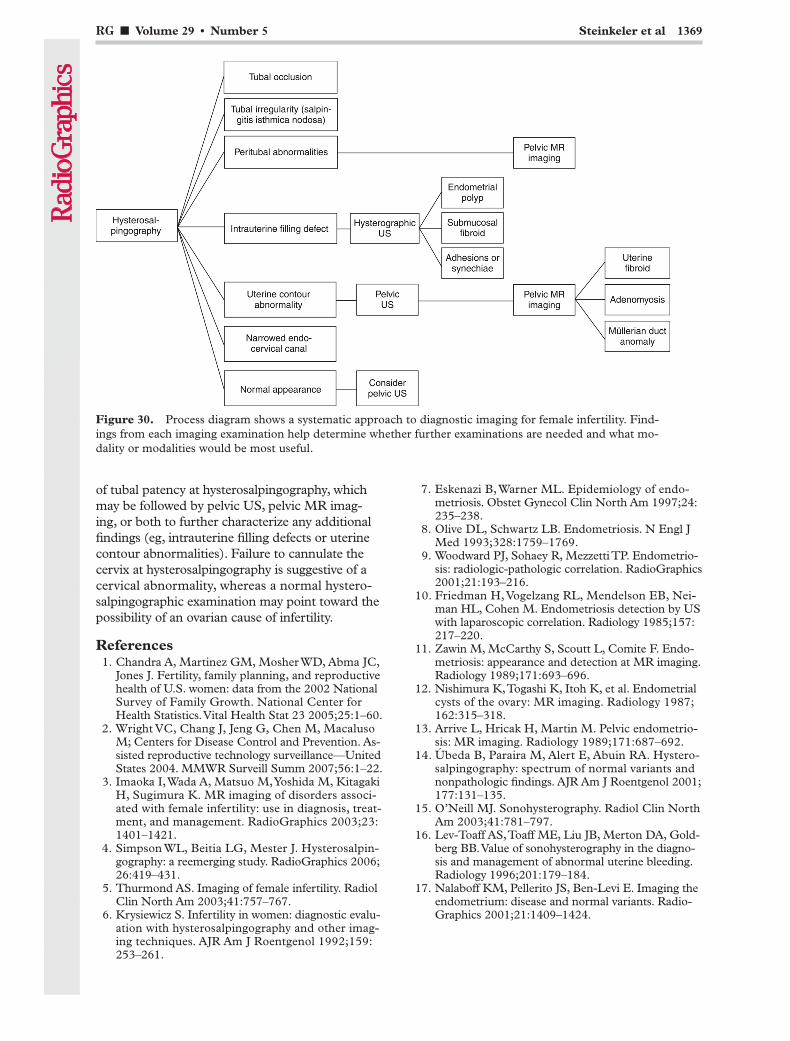
ConclusionsThe pelvic causes of female infertility include tubal, peritoneal, uterine, endometrial, cervical, and ovar-ian abnormalities. A multimodality imaging ap-proach may be useful for determining the cause of infertility and guiding clinical management in spe-cific cases (Fig 30). An imaging evaluation for fe-male infertility typically begins with an assessment
Women of childbearing age who have cervi-cal stenosis are less likely to show evidence of hematometra than postmenopausal patients are. At US, hematometra manifests as dilatation of the fluid-filled endometrial cavity, often with a fluid-fluid level caused by sedimentation of red blood cells. Intraoperative US may be useful for guidance of instrumentation and to minimize complications during procedures in patients with cervical stenosis (43). Gradual dilation of the cer-vix, performed with US guidance, is an effective treatment for this problem (42).
Ovarian AbnormalitiesOvarian causes of infertility include primary con-ditions such as nonfunctional ovaries, premature ovarian failure, and absence of ovaries (gonadal dysgenesis). These conditions are usually diag-nosed on the basis of clinical and biochemical findings. Imaging is more valuable for diagnosing the secondary ovarian causes of infertility, which include polycystic ovary syndrome, endometrio-sis, and ovarian cancer. Pelvic US is usually per-formed for initial evaluation of the ovaries.
Polycystic ovary syndrome reportedly affects approximately 8% of women and may be one of the most common causes of female infertil-ity (46). Women with this syndrome have hy-perandrogenism, which leads to morphologic changes in the ovary, and elevated serum levels of luteinizing hormone (47). The overproduction of luteinizing hormone results in incomplete ovula-tory cycles. Clinical manifestations of the condi-tion include hirsutism, obesity, and oligoamenor-rhea. Treatment usually involves the induction of ovulation with clomiphene citrate.
Figure 29. Polycystic ovary syndrome. (a) Transvaginal US image of the right ovary depicts multiple peripheral subcentimetric follicles (arrow). (b) Coronal T2-weighted MR image from the same patient shows bilateral ovarian enlargement with multiple peripheral follicles (arrows).
RG ■ Volume 29 • Number 5 Steinkeler et al 1369
7. Eskenazi B, Warner ML. Epidemiology of endo-metriosis. Obstet Gynecol Clin North Am 1997;24: 235–238.
8. Olive DL, Schwartz LB. Endometriosis. N Engl J Med 1993;328:1759–1769.
9. Woodward PJ, Sohaey R, Mezzetti TP. Endometrio-sis: radiologic-pathologic correlation. RadioGraphics 2001;21:193–216.
10. Friedman H, Vogelzang RL, Mendelson EB, Nei-man HL, Cohen M. Endometriosis detection by US with laparoscopic correlation. Radiology 1985;157: 217–220.
11. Zawin M, McCarthy S, Scoutt L, Comite F. Endo-metriosis: appearance and detection at MR imaging. Radiology 1989;171:693–696.
12. Nishimura K, Togashi K, Itoh K, et al. Endometrial cysts of the ovary: MR imaging. Radiology 1987; 162:315–318.
13. Arrive L, Hricak H, Martin M. Pelvic endometrio-sis: MR imaging. Radiology 1989;171:687–692.
14. Úbeda B, Paraira M, Alert E, Abuin RA. Hystero-salpingography: spectrum of normal variants and nonpathologic findings. AJR Am J Roentgenol 2001; 177:131–135.
15. O’Neill MJ. Sonohysterography. Radiol Clin North Am 2003;41:781–797.
16. Lev-Toaff AS, Toaff ME, Liu JB, Merton DA, Gold-berg BB. Value of sonohysterography in the diagno-sis and management of abnormal uterine bleeding. Radiology 1996;201:179–184.
17. Nalaboff KM, Pellerito JS, Ben-Levi E. Imaging the endometrium: disease and normal variants. Radio-Graphics 2001;21:1409–1424.
of tubal patency at hysterosalpingography, which may be followed by pelvic US, pelvic MR imag-ing, or both to further characterize any additional findings (eg, intrauterine filling defects or uterine contour abnormalities). Failure to cannulate the cervix at hysterosalpingography is suggestive of a cervical abnormality, whereas a normal hystero-salpingographic examination may point toward the possibility of an ovarian cause of infertility.
References 1. Chandra A, Martinez GM, Mosher WD, Abma JC,
Jones J. Fertility, family planning, and reproductive health of U.S. women: data from the 2002 National Survey of Family Growth. National Center for Health Statistics. Vital Health Stat 23 2005;25:1–60.
2. Wright VC, Chang J, Jeng G, Chen M, Macaluso M; Centers for Disease Control and Prevention. As-sisted reproductive technology surveillance—United States 2004. MMWR Surveill Summ 2007;56:1–22.
3. Imaoka I, Wada A, Matsuo M, Yoshida M, Kitagaki H, Sugimura K. MR imaging of disorders associ-ated with female infertility: use in diagnosis, treat-ment, and management. RadioGraphics 2003;23: 1401–1421.
4. Simpson WL, Beitia LG, Mester J. Hysterosalpin-gography: a reemerging study. RadioGraphics 2006; 26:419–431.
5. Thurmond AS. Imaging of female infertility. Radiol Clin North Am 2003;41:757–767.
6. Krysiewicz S. Infertility in women: diagnostic evalu-ation with hysterosalpingography and other imag-ing techniques. AJR Am J Roentgenol 1992;159: 253–261.
Figure 30. Process diagram shows a systematic approach to diagnostic imaging for female infertility. Find-ings from each imaging examination help determine whether further examinations are needed and what mo-dality or modalities would be most useful.
1370 September-October 2009 radiographics.rsna.org
33. Brody JM, Koelliker SL, Frishman GN. Unicornu-ate uterus: imaging appearance, associated anoma-lies, and clinical implications. AJR Am J Roentgenol 1998;171:1341–1347.
34. Sarto GE, Simpson JL. Abnormalities of the Mül-lerian and Wolffian duct systems. Birth Defects Orig Artic Ser 1978;14:37–54.
35. Patton PE, Novy MJ. Reproductive potential of the anomalous uterus. Semin Reprod Endocrinol 1988; 6:217–233.
36. Homer HA, Li TC, Cooker ID. The septate uterus: a review of management and reproductive outcome. Fertil Steril 2000;73:1–14.
37. Tulandi T, Arronet GH, McInnes RA. Arcuate and bicornuate uterine anomalies and infertility. Fertil Steril 1980;34:362–364.
38. Herbst AL, Senekjian EK, Frey KW. Abortion and pregnancy loss among diethylstilbestrol-exposed women. Semin Endocrinol 1989;7:124–129.
39. Kaufman RH, Adam E, Binder GL, Gerthoffer E. Upper genital tract changes and pregnancy outcome in offspring exposed in utero to diethylstilbestrol. Am J Obstet Gynecol 1980;137:299–308.
40. Nagel TC, Malo JN. Hysteroscopic metroplasty in the diethylstilbestrol exposed uterus and similar non fusion anomalies: effect on subsequent obstetric per-formance. Fertil Steril 1993;59:502–506.
41. Baldauf JJ, Dreyfus M, Wertz JP, Cuénin C, Ritter J, Philippe E. Consequences and treatment of cervical stenoses after laser conization or loop electrosurcial excision [in French]. J Gynecol Obstet Biol Reprod (Paris) 1997;26:64–70.
42. Valle RF, Sankpal R, Marlow JL, Cohen L. Cervi-cal stenosis: a challenging clinical entity. J Gynecol Surg 2002;18:129–143.
43. Christianson MS, Barker MA, Lindheim SR. Over-coming the challenging cervix: techniques to access the uterine cavity. J Low Genit Tract Dis 2008;12: 24–31.
44. Suh-Burgmann EJ, Whall-Strojwas D, Chang Y, Hundley D, Goodman AK. Risk factors for cervi-cal stenosis after loop electrocautery excision pro-cedure. Obstet Gynecol 2000;96:657–660.
45. Ott DJ, Chen MYM. General diagnostic principles. In: Ott DJ, Fayez JA, Zagoria RJ, eds. Hysterosalpin-gography: a text and atlas. 2nd ed. Baltimore, Md: Williams & Wilkins, 1998.
46. Azziz R, Carmina E, Dewailly D, et al. The An-drogen Excess and PCOS Society criteria for the polycystic ovary syndrome: the complete task force report. Fertil Steril 2009;91:456–488.
47. Legro RS, Barnhart HX, Schlaff WD, et al. Clo-miphene, metformin, or both for infertility in the polycystic ovary syndrome. N Engl J Med 2007;356: 551–566.
48. Pache TD, Wladimiroff JW, Hop WC, Fauser BC. How to discriminate between normal and polycystic ovaries: transvaginal US study. Radiology 1992;183: 421–423.
49. Kimura I, Togashi K, Kawakami S, et al. Polycystic ovaries: implications of diagnosis with MR imag-ing. Radiology 1996;201:549–552.
18. Matalliotakis IM, Katsikis IK, Panidis DK. Adeno-myosis: what is the impact on fertility? Curr Opin Obstet Gynecol 2005;17:261–264.
19. Kunz G, Beil D, Huppert P, Noe M, Kissler S, Leyendecker G. Adenomyosis in endometriosis—prevalence and impact on fertility. Evidence from magnetic resonance imaging. Hum Reprod 2005;20: 2309–2316.
20. Reinhold C, Tafazoli F, Mehio A, et al. Uterine adenomyosis: endovaginal US and MR imaging fea-tures with histopathologic correlation. RadioGraph-ics 1999;19(spec no):S147–S160.
21. Atri M, Reinhold C, Mehio AR, Chapman WB, Bret PM. Adenomyosis: US features with histologic cor-relation in an in vitro study. Radiology 2000;215: 783–790.
22. Tamai K, Togashi K, Ito T, Morisawa N, Fujiwara T, Koyama T. MR imaging findings of adenomyo-sis: correlation with histopathologic features and diagnostic pitfalls. RadioGraphics 2005;25:21–40.
23. Salem S, Wilson SR. Gynecologic ultrasound. In: Rumack CM, Wilson SR, Charboneau JW, eds. Di-agnostic ultrasound. 3rd ed. St. Louis, Mo: Elsevier Mosby, 2005.
24. Benson CB, Chow JS, Chang-Lee W, Hill JA, Dou-bilet PM. Outcome of pregnancies in women with uterine leiomyomas identified by sonography in the first trimester. J Clin Ultrasound 2001;29:261–264.
25. Troiano RN, McCarthy SM. Müllerian duct anom-alies: imaging and clinical issues. Radiology 2004; 233:19–34.
26. Golan A, Langer R, Bukovsky I, Caspi E. Congeni-tal anomalies of the müllerian system. Fertil Steril 1989;51:747–755.
27. Harger JH, Archer DF, Marchese SG, Muracca-Clemens M, Garver KL. Etiology of recurrent preg-nancy losses and outcome of subsequent pregnan-cies. Obstet Gynecol 1983;62:574–581.
28. Buttram VC, Gibbons WE. Müllerian anomalies: a proposed classification (an analysis of 144 cases). Fertil Steril 1979;32:40–46.
29. Pellerito JS, McCarthy SM, Doyle MB, Glickman MG, DeCherney AH. Diagnosis of uterine anoma-lies: relative accuracy of MR imaging, endovaginal sonography, and hysterosalpingography. Radiology 1992;183:795–800.
30. Mueller GC, Hussain HK, Smith YR, et al. Mül-lerian duct anomalies: comparison of MRI diag-nosis and clinical diagnosis. AJR Am J Roentgenol 2007;189:1294–1302.
31. Speroff L, Glass RH, Kase NG. Development of the müllerian system. In: Mitchell C, ed. Clinical gyne-cologic endocrinology and infertility. 6th ed. Balti-more, Md: Lippincott, Williams & Wilkins, 1998.
32. The American Fertility Society classifications of ad-nexal adhesions, distal tubal occlusion, tubal occlu-sion secondary to tubal ligation, tubal pregnancies, müllerian anomalies and intrauterine adhesions. Fertil Steril 1988;49:944–955.
This article meets the criteria for 1.0 credit hour in category 1 of the AMA Physician’s Recognition Award. To obtaincredit, see accompanying test at http://www.rsna.org/education/rg_cme.html.
RG Volume 29 Number 5 September-October 2009 Steinkeler et al
Female Infertility: A Systematic Approach to Radiologic Imaging
and Diagnosis
Jill A. Steinkeler, MD, et al
Page 1354
Hysterosalpingography provides optimal depiction of the fallopian tubes, allowing detection of tubal
patency, tubal occlusion, tubal irregularity, and peritubal disease.
Page 1358
In general, hysterographic US is performed for a more detailed evaluation of the endometrial cavity if
intrauterine filling defects are seen at hysterosalpingography.
Page 1360
Uterine contour irregularities observed at hysterosalpingography may be due to a variety of entities,
including adenomyosis, uterine leiomyomas, and müllerian duct anomalies.
Page 1362
With its excellent soft-tissue contrast resolution, pelvic MR imaging is the most accurate imaging
modality for evaluating the size, location, and number of uterine leiomyomas.
Page 1363 Accurate characterization of müllerian duct anomalies is essential because pregnancy outcomes and treatment options vary between the different classes of anomalies.
RadioGraphics 2009; 29:1353–1370 • Published online 10.1148/rg.295095047 • Content Codes:
RadioGraphics 2009 This is your reprint order form or pro forma invoice
(Please keep a copy of this document for your records.)
Author Name _______________________________________________________________________________________________ Title of Article _______________________________________________________________________________________________ Issue of Journal_______________________________ Reprint # _____________ Publication Date ________________ Number of Pages_______________________________ KB # _____________ Symbol Radio Graphics Color in Article? Yes / No (Please Circle) Please include the journal name and reprint number or manuscript number on your purchase order or other correspondence. Order and Shipping Information Reprint Costs (Please see page 2 of 2 for reprint costs/fees.) ________ Number of reprints ordered $_________ ________ Number of color reprints ordered $_________ ________ Number of covers ordered $_________ Subtotal $_________
Taxes $_________ (Add appropriate sales tax for Virginia, Maryland, Pennsylvania, and the District of Columbia or Canadian GST to the reprints if your order is to be shipped to these locations.)
First address included, add $32 for each additional shipping address $_________
TOTAL $_________
Shipping Address (cannot ship to a P.O. Box) Please Print Clearly Name ___________________________________________ Institution _________________________________________ Street ___________________________________________ City ____________________ State _____ Zip ___________ Country ___________________________________________ Quantity___________________ Fax ___________________ Phone: Day _________________ Evening _______________ E-mail Address _____________________________________ Additional Shipping Address* (cannot ship to a P.O. Box)
Name ___________________________________________ Institution _________________________________________ Street ___________________________________________ City ________________ State ______ Zip ___________
Country _________________________________________ Quantity __________________ Fax __________________ Phone: Day ________________ Evening ______________ E-mail Address ____________________________________ * Add $32 for each additional shipping address
Payment and Credit Card Details Enclosed: Personal Check ___________ Credit Card Payment Details _________ Checks must be paid in U.S. dollars and drawn on a U.S. Bank. Credit Card: __ VISA __ Am. Exp. __ MasterCard Card Number __________________________________ Expiration Date_________________________________ Signature: _____________________________________ Please send your order form and prepayment made payable to: Cadmus Reprints P.O. Box 751903 Charlotte, NC 28275-1903 Note: Do not send express packages to this location, PO Box.
FEIN #:541274108
Invoice or Credit Card Information Invoice Address Please Print Clearly Please complete Invoice address as it appears on credit card statement Name ____________________________________________ Institution ________________________________________ Department _______________________________________ Street ____________________________________________ City ________________________ State _____ Zip _______ Country ___________________________________________ Phone _____________________ Fax _________________ E-mail Address _____________________________________ Cadmus will process credit cards and Cadmus Journal
Services will appear on the credit card statement. If you don’t mail your order form, you may fax it to 410-820-9765 with
your credit card information. Signature __________________________________________ Date _______________________________________ Signature is required. By signing this form, the author agrees to accept the responsibility for the payment of reprints and/or all charges described in this document.
Reprint order forms and purchase orders or prepayments must be received 72 hours after receipt of form either by mail or by fax at 410-820-9765. It is the policy of Cadmus Reprints to issue one invoice per order.
Please print clearly.
Page 1 of 2 RB-1/01/09
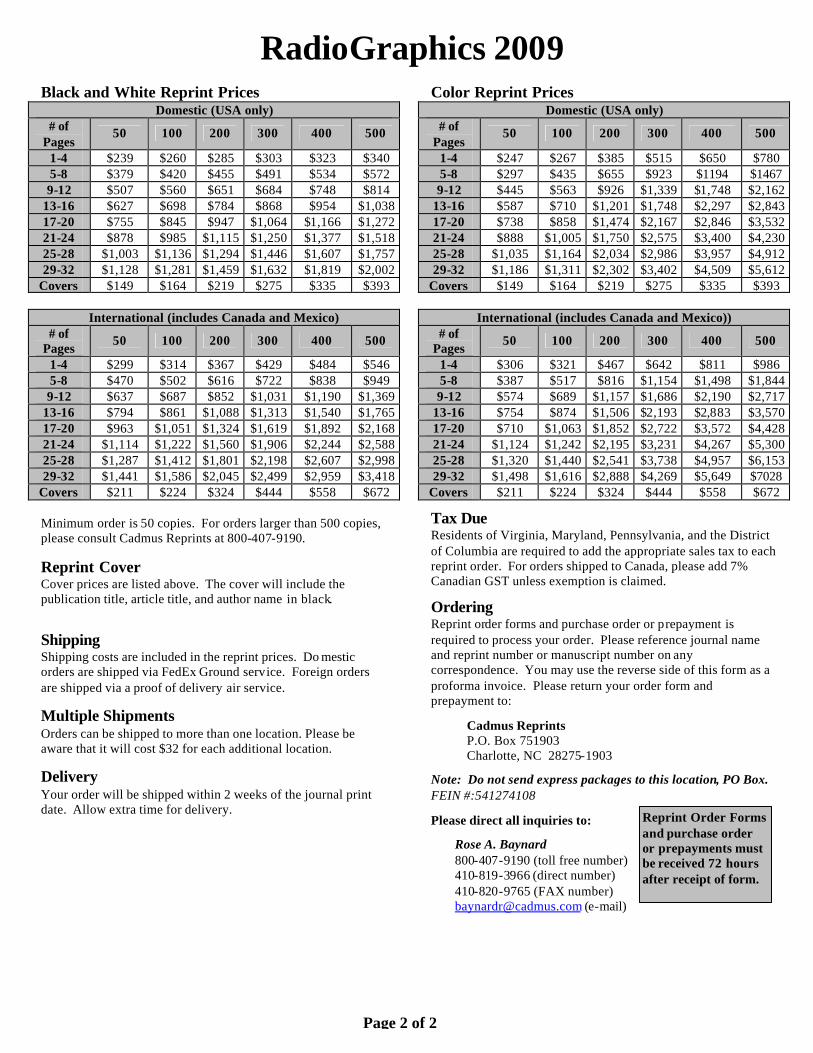
RadioGraphics 2009 Black and White Reprint Prices
Domestic (USA only) # of
Pages 50 100 200 300 400 500
1-4 $239 $260 $285 $303 $323 $340 5-8 $379 $420 $455 $491 $534 $572 9-12 $507 $560 $651 $684 $748 $814
13-16 $627 $698 $784 $868 $954 $1,038 17-20 $755 $845 $947 $1,064 $1,166 $1,272 21-24 $878 $985 $1,115 $1,250 $1,377 $1,518 25-28 $1,003 $1,136 $1,294 $1,446 $1,607 $1,757 29-32 $1,128 $1,281 $1,459 $1,632 $1,819 $2,002
Covers $149 $164 $219 $275 $335 $393
International (includes Canada and Mexico) # of
Pages 50 100 200 300 400 500
1-4 $299 $314 $367 $429 $484 $546 5-8 $470 $502 $616 $722 $838 $949 9-12 $637 $687 $852 $1,031 $1,190 $1,369
13-16 $794 $861 $1,088 $1,313 $1,540 $1,765 17-20 $963 $1,051 $1,324 $1,619 $1,892 $2,168 21-24 $1,114 $1,222 $1,560 $1,906 $2,244 $2,588 25-28 $1,287 $1,412 $1,801 $2,198 $2,607 $2,998 29-32 $1,441 $1,586 $2,045 $2,499 $2,959 $3,418
Covers $211 $224 $324 $444 $558 $672 Minimum order is 50 copies. For orders larger than 500 copies, please consult Cadmus Reprints at 800-407-9190. Reprint Cover Cover prices are listed above. The cover will include the publication title, article title, and author name in black. Shipping Shipping costs are included in the reprint prices. Do mestic orders are shipped via FedEx Ground service. Foreign orders are shipped via a proof of delivery air service. Multiple Shipments Orders can be shipped to more than one location. Please be aware that it will cost $32 for each additional location. Delivery Your order will be shipped within 2 weeks of the journal print date. Allow extra time for delivery.
Color Reprint Prices
Domestic (USA only) # of
Pages 50 100 200 300 400 500
1-4 $247 $267 $385 $515 $650 $780 5-8 $297 $435 $655 $923 $1194 $1467 9-12 $445 $563 $926 $1,339 $1,748 $2,162
13-16 $587 $710 $1,201 $1,748 $2,297 $2,843 17-20 $738 $858 $1,474 $2,167 $2,846 $3,532 21-24 $888 $1,005 $1,750 $2,575 $3,400 $4,230 25-28 $1,035 $1,164 $2,034 $2,986 $3,957 $4,912 29-32 $1,186 $1,311 $2,302 $3,402 $4,509 $5,612
Covers $149 $164 $219 $275 $335 $393
International (includes Canada and Mexico)) # of
Pages 50 100 200 300 400 500
1-4 $306 $321 $467 $642 $811 $986 5-8 $387 $517 $816 $1,154 $1,498 $1,844 9-12 $574 $689 $1,157 $1,686 $2,190 $2,717
13-16 $754 $874 $1,506 $2,193 $2,883 $3,570 17-20 $710 $1,063 $1,852 $2,722 $3,572 $4,428 21-24 $1,124 $1,242 $2,195 $3,231 $4,267 $5,300 25-28 $1,320 $1,440 $2,541 $3,738 $4,957 $6,153 29-32 $1,498 $1,616 $2,888 $4,269 $5,649 $7028
Covers $211 $224 $324 $444 $558 $672 Tax Due Residents of Virginia, Maryland, Pennsylvania, and the District of Columbia are required to add the appropriate sales tax to each reprint order. For orders shipped to Canada, please add 7% Canadian GST unless exemption is claimed. Ordering Reprint order forms and purchase order or prepayment is required to process your order. Please reference journal name and reprint number or manuscript number on any correspondence. You may use the reverse side of this form as a proforma invoice. Please return your order form and prepayment to: Cadmus Reprints P.O. Box 751903 Charlotte, NC 28275-1903 Note: Do not send express packages to this location, PO Box. FEIN #:541274108 Please direct all inquiries to:
Rose A. Baynard 800-407-9190 (toll free number) 410-819-3966 (direct number) 410-820-9765 (FAX number)
[email protected] (e-mail)
Reprint Order Forms and purchase order or prepayments must be received 72 hours after receipt of form.
Page 2 of 2

![Role of L-carnitine in female infertility › ...Role_of_L-carnitine_in_female_infertility.pdf · female infertility [11, 18, 36] (Table 1). Several studies found that both LC and](https://static.fdocuments.net/doc/165x107/5f0d0d177e708231d4386f9b/role-of-l-carnitine-in-female-a-roleofl-carnitineinfemaleinfertilitypdf.jpg)