
& FELLOW Clinical Reasoning: A young adult presents with...
5
Clinical Reasoning: A young adult presents with focal weakness and hemorrhagic brain lesions Tuhin Virmani, MD, PhD Ashima Agarwal, MD Eric C. Klawiter, MD SECTION 1 A 25-year-old man who emigrated from Mexico 5 years ago presented with headache, altered mental status, and left hemiparesis. Initial history obtained from collateral sources indicated the patient had complained of a headache of increasing severity for the past 2 months. Two weeks prior to presentation, he experienced malaise, decreased appetite, nausea and vomiting, visual changes, and gait difficulties re- sulting in 2 falls. The day of presentation, he devel- oped acute onset left upper and lower extremity weakness prompting emergency evaluation. On ar- rival he was lethargic, disoriented, and did not follow commands. Following intubation in the emergency department, he was transferred to the neurologic in- tensive care unit (ICU). He was febrile and tachycardic on arrival to the ICU. Upon cessation of sedation, the patient was ill-appearing but awake and able to cooperate with the neurologic examination. He was oriented to hos- pital name and year and was able to follow one-step commands. His pupils were equal, round, and reac- tive to light and accommodation. Bedside fundu- scopic examination showed normal discs and vessels. His extraocular movements were full except for the inability to adduct his right eye. He blinked to threat bilaterally but had left-sided visual neglect with a right gaze preference. He had left lower facial weak- ness. On motor examination, he had left flaccid pa- ralysis as well as mild decreased strength in his right upper and lower extremities (4/5) that might have been attributable to incomplete cooperation. Sensa- tion was intact to light touch on the right but only to noxious painful nail bed stimulation on the left. Re- flexes were brisk on the right and diminished on the left. He had a left Babinski sign. Head CT revealed 2 foci of hemorrhage in the right frontal and parietal lobes with associated vaso- genic edema (figure 1). Questions for consideration: 1. What is the differential diagnosis? 2. What would be the next step in your management of this patient? GO TO SECTION 2 From the Departments of Neurology (T.V., E.C.K.) and Pathology (A.A.), Washington University, St. Louis, MO. Study funding: Supported by the NIH (UL1RR024992 to E.C.K.). E.C.K. was supported by an American Academy of Neurology Foundation Clinical Research Training Fellowship. Disclosure: Author disclosures are provided at the end of the article. Address correspondence and reprint requests to Dr. Tuhin Virmani, Neurology, Box 8111, 660 S. Euclid Ave., St. Louis, MO 63110 [email protected] Figure 1 CT findings Two foci of hemorrhage are seen in the right frontal and parietal lobes with surrounding vasogenic edema. RESIDENT & FELLOW SECTION Section Editor Mitchell S.V. Elkind, MD, MS e106 Copyright © 2011 by AAN Enterprises, Inc.
Transcript of & FELLOW Clinical Reasoning: A young adult presents with...
Clinical Reasoning:A young adult presents with focal weaknessand hemorrhagic brain lesions
Tuhin Virmani, MD,PhD
Ashima Agarwal, MDEric C. Klawiter, MD
SECTION 1A 25-year-old man who emigrated from Mexico 5years ago presented with headache, altered mentalstatus, and left hemiparesis. Initial history obtainedfrom collateral sources indicated the patient hadcomplained of a headache of increasing severity forthe past 2 months. Two weeks prior to presentation,he experienced malaise, decreased appetite, nauseaand vomiting, visual changes, and gait difficulties re-sulting in 2 falls. The day of presentation, he devel-oped acute onset left upper and lower extremityweakness prompting emergency evaluation. On ar-rival he was lethargic, disoriented, and did not followcommands. Following intubation in the emergencydepartment, he was transferred to the neurologic in-tensive care unit (ICU).
He was febrile and tachycardic on arrival to theICU. Upon cessation of sedation, the patient wasill-appearing but awake and able to cooperate withthe neurologic examination. He was oriented to hos-pital name and year and was able to follow one-stepcommands. His pupils were equal, round, and reac-tive to light and accommodation. Bedside fundu-scopic examination showed normal discs and vessels.His extraocular movements were full except for theinability to adduct his right eye. He blinked to threatbilaterally but had left-sided visual neglect with aright gaze preference. He had left lower facial weak-ness. On motor examination, he had left flaccid pa-ralysis as well as mild decreased strength in his rightupper and lower extremities (4�/5) that might have
been attributable to incomplete cooperation. Sensa-tion was intact to light touch on the right but only tonoxious painful nail bed stimulation on the left. Re-flexes were brisk on the right and diminished on theleft. He had a left Babinski sign.
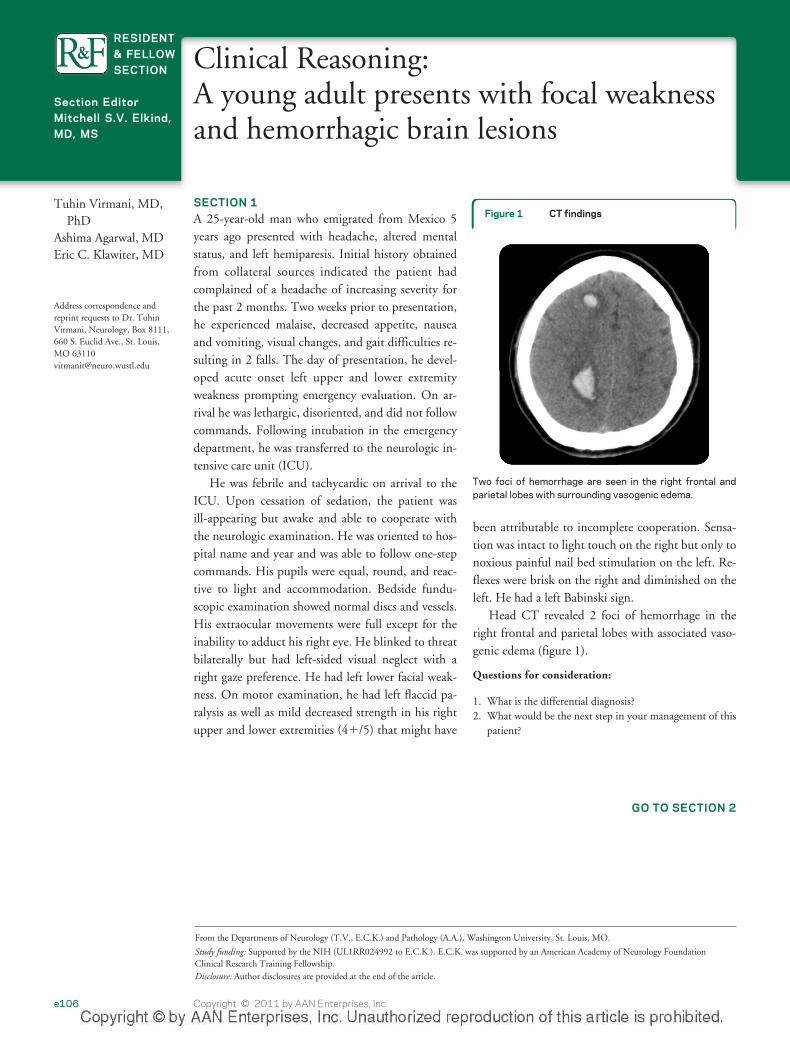
Head CT revealed 2 foci of hemorrhage in theright frontal and parietal lobes with associated vaso-genic edema (figure 1).
Questions for consideration:
1. What is the differential diagnosis?2. What would be the next step in your management of this
patient?
GO TO SECTION 2
From the Departments of Neurology (T.V., E.C.K.) and Pathology (A.A.), Washington University, St. Louis, MO.
Study funding: Supported by the NIH (UL1RR024992 to E.C.K.). E.C.K. was supported by an American Academy of Neurology FoundationClinical Research Training Fellowship.Disclosure: Author disclosures are provided at the end of the article.
Address correspondence andreprint requests to Dr. TuhinVirmani, Neurology, Box 8111,660 S. Euclid Ave., St. Louis,MO [email protected]
Figure 1 CT findings
Two foci of hemorrhage are seen in the right frontal andparietal lobes with surrounding vasogenic edema.
RESIDENT& FELLOWSECTION
Section EditorMitchell S.V. Elkind,MD, MS
e106 Copyright © 2011 by AAN Enterprises, Inc.
SECTION 2The differential diagnosis for this presentation withmultiple neurologic symptoms rapidly cumulativeover time should initially be kept broad to avoidmissing a treatable disease. Both the neurologic ex-amination and initial imaging implicate a multifocallocalization. Given the prolonged headache, malaise,and fever at presentation, one must first consider in-fectious processes such as viral and bacterial meningi-tis or encephalitis including tuberculous meningitis,cysticercosis, and aspergillosis. Infective endocarditisleading to multiple septic emboli could also account
for the clinical picture and the potential involvementof both anterior and posterior circulation territories.Other causes of multifocal stroke with hemorrhagicconversion include CNS vasculitis and moyamoyadisease. Central demyelinating conditions such asacute hemorrhagic leukoencephalitis are possiblegiven the patient’s age and presentation. Finally, neo-plasms (primary CNS tumors, metastatic disease, orprimary CNS lymphoma) could potentially causemultiple hemorrhagic lesions that become symptom-atic with dissemination in time.
Additional history revealed no prior illness. Hehad not visited Mexico since arrival to the UnitedStates. A brother presented with sudden onset ofweakness at age 17 with a fluctuating course that re-sulted in death. His father died of renal failure.
Initial studies showed normal serum chemistriesexcept for low sodium (127 mmol/L). White bloodcell (WBC) count was elevated at 18,000/mm3 with90% neutrophils. Additional testing included nega-tive antinuclear antibodies, antineutrophil cytoplas-mic antibodies, and extractable nuclear antigenscreens with a mildly elevated erythrocyte sedimenta-tion rate at 16 mm/hour (0–12). HIV testing wasnegative. Lumbar puncture was remarkable formildly elevated protein (53 mg/dL), normal glucose,1 WBC/mm3, 2 red blood cells (RBC)/mm3, nega-tive bacterial culture, and negative varicella zoster virus,herpes simplex virus, Epstein-Barr virus, cytomegalovi-rus, and enterovirus PCRs.
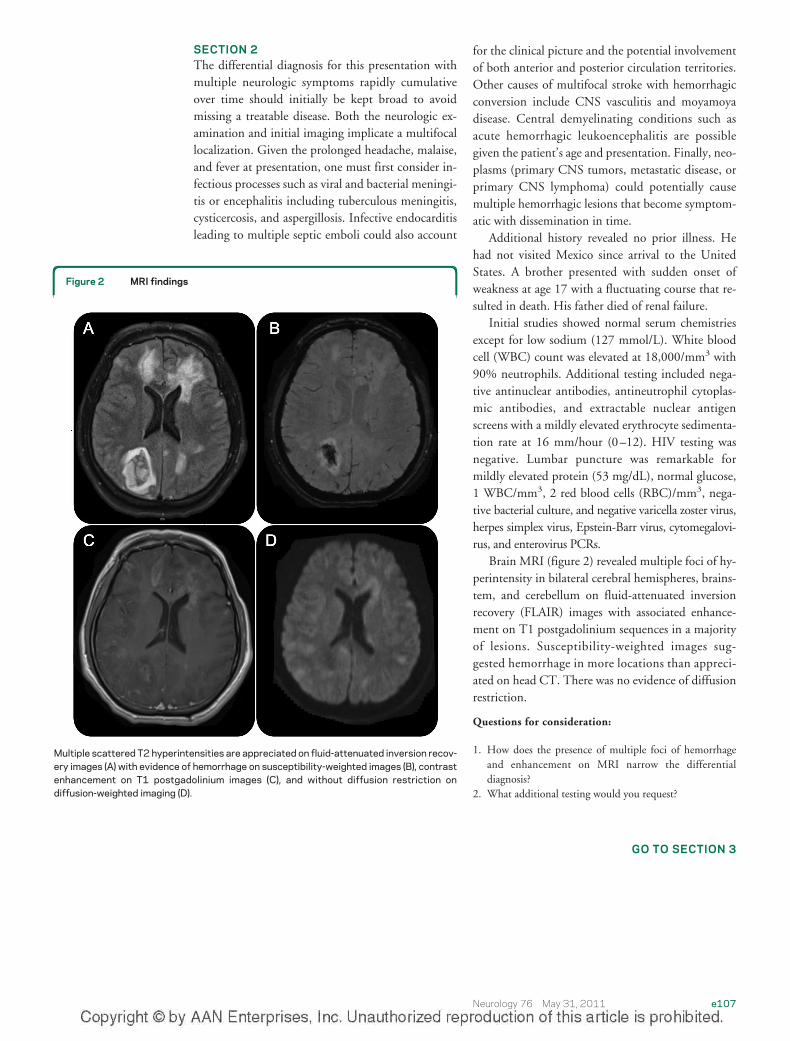
Brain MRI (figure 2) revealed multiple foci of hy-perintensity in bilateral cerebral hemispheres, brains-tem, and cerebellum on fluid-attenuated inversionrecovery (FLAIR) images with associated enhance-ment on T1 postgadolinium sequences in a majorityof lesions. Susceptibility-weighted images sug-gested hemorrhage in more locations than appreci-ated on head CT. There was no evidence of diffusionrestriction.
Questions for consideration:
1. How does the presence of multiple foci of hemorrhageand enhancement on MRI narrow the differentialdiagnosis?
2. What additional testing would you request?
GO TO SECTION 3
Figure 2 MRI findings
Multiple scattered T2 hyperintensities are appreciated on fluid-attenuated inversion recov-ery images (A) with evidence of hemorrhage on susceptibility-weighted images (B), contrastenhancement on T1 postgadolinium images (C), and without diffusion restriction ondiffusion-weighted imaging (D).
Neurology 76 May 31, 2011 e107
SECTION 3The MRI findings help narrow the differential diag-nosis by excluding acute ischemic stroke. Infectious,demyelinating, inflammatory, and neoplastic pro-cesses should continue to be considered. The low se-rum sodium was likely secondary to the syndrome ofinappropriate anti-diuretic hormone secretion fromthe multiple CNS lesions.
Subsequent CSF testing demonstrated normal im-munoglobulin G index and synthesis rate and no oligo-clonal bands. Extensive infectious evaluation includingCSF acid fast bacteria (AFB) stain and culture, CSFtoxoplasma PCR, blood and urine histoplasma antigen,CSF and blood Cryptococcus antigen, Aspergillus galacto-mannan antigen, CSF and nasal Mycoplasma pneu-moniae PCR, CSF ova and parasites screen, and CSFAcanthamoeba culture were all negative. The patientwas still without a definitive diagnosis.
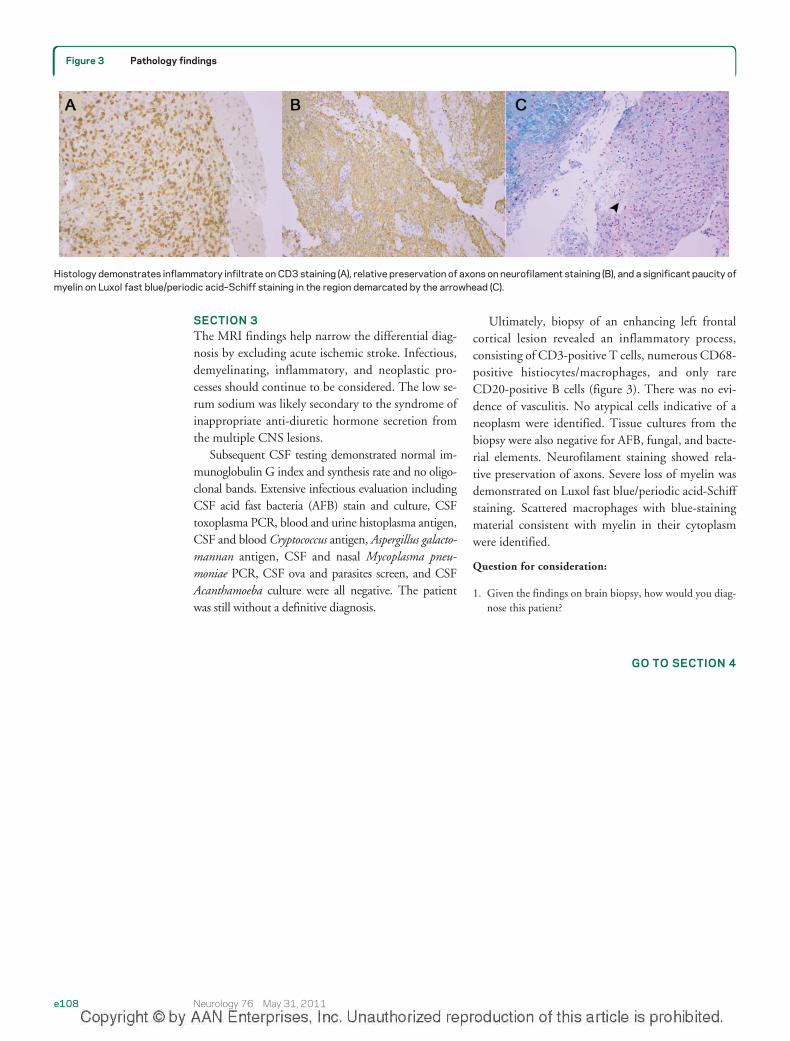
Ultimately, biopsy of an enhancing left frontalcortical lesion revealed an inflammatory process,consisting of CD3-positive T cells, numerous CD68-positive histiocytes/macrophages, and only rareCD20-positive B cells (figure 3). There was no evi-dence of vasculitis. No atypical cells indicative of aneoplasm were identified. Tissue cultures from thebiopsy were also negative for AFB, fungal, and bacte-rial elements. Neurofilament staining showed rela-tive preservation of axons. Severe loss of myelin wasdemonstrated on Luxol fast blue/periodic acid-Schiffstaining. Scattered macrophages with blue-stainingmaterial consistent with myelin in their cytoplasmwere identified.
Question for consideration:
1. Given the findings on brain biopsy, how would you diag-nose this patient?
GO TO SECTION 4
Figure 3 Pathology findings
Histology demonstrates inflammatory infiltrate on CD3 staining (A), relative preservation of axons on neurofilament staining (B), and a significant paucity ofmyelin on Luxol fast blue/periodic acid–Schiff staining in the region demarcated by the arrowhead (C).
e108 Neurology 76 May 31, 2011

SECTION 4This patient initially had a headache followed byrapid progression of neurologic symptoms resultingin decreased level of consciousness and left hemipare-sis. MRI showed multiple T2 hyperintensities, somewith hemorrhagic involvement. Brain biopsy showedpatchy demyelination with axon preservation. Pres-ence of CD3-positive T cells and CD68 histiocytes/macrophages with rare B cells indicated a reactiveprocess, less likely to be neoplastic. These findingsare consistent with a diagnosis of acute hemorrhagicleukoencephalitis (AHLE).
Interestingly, the cause of death of the patient’sbrother is unknown, but he presented in a similarfashion. One could speculate that it is possible the 2siblings had the same disorder.
AHLE is a rare disorder on the spectrum of acutepostinfectious leukoencephalopathies includingacute disseminated encephalomyelitis and Bickerstaffbrainstem encephalitis.1 AHLE typically presentswith an abrupt onset of neurologic symptoms includ-ing encephalopathy, focal neurologic deficits, sei-zures, and coma up to 20 days after a nonspecificviral illness, similar to this case report.2 CSF typicallyshows a lymphocytic pleocytosis, elevated RBCcount, and elevated protein. MRI may demonstratewhite matter T2 hyperintensities with associatededema and often hemorrhage.3,4 Contrast enhance-ment is not typically present but was appreciated inthis patient. Pathology shows fibrinoid vascular ne-crosis, widespread perivascular polymorphonuclearinfiltrates, “ring and ball” hemorrhages, and loss ofmyelin with preservation of axons.5 The etiology ofAHLE remains unclear, with a prevailing theory thatinfectious agents trigger the formation of T-cellclones, resulting in an inflammatory cascade target-ing myelin basic protein. The perivascular infiltratehas been suggested to represent an acute vasculitiswith occlusion of vessels eventually leading to vesselwall necrosis and subsequent hemorrhage.3,6,7 Treat-ment currently includes surgical decompression forincreased intracranial pressure with craniectomy orventriculostomy if necessary. Immunosuppressiveagents such as IV steroids, IV immunoglobulins, andcyclophosphamide have also been employed withvarying success, although morbidity and mortalityremain high.8,9
This patient was treated with IV methylpred-nisolone (5 g) over 5 days. His symptoms improved
with in-patient physical, occupational, and speechtherapy over his 3-week hospitalization. At the timeof discharge to a specialized rehabilitation hospital,he still had a significant left hemiparesis. After a1-month stay in the rehabilitation hospital, he con-tinued to recover, improving to only a mild lefthemiparesis. Although prognosis is variable inAHLE, further improvement in strength could beexpected in this case.
This case emphasizes that demyelinating condi-tions should be included in the differential diagnosisof a young adult presenting with multifocal com-plaints with a decreased level of consciousness andevidence of hemorrhage on neuroimaging.
DISCLOSUREDr. Virmani and Dr. Agarwal report no disclosures. Dr. Klawiter has
served on a scientific advisory board and as a consultant for Teva Pharma-
ceutical Industries Ltd.; has served on speakers’ bureaus for and received
speaker honoraria from Teva Pharmaceutical Industries Ltd. and Bayer
Schering Pharma; and has received research support from the NIH and an
American Academy of Neurology Foundation Clinical Research Training
Fellowship.
REFERENCES1. Sonneville R, Klein IF, Wolff M. Update on investigation
and management of postinfectious encephalitis. CurrOpin Neurol 2010;23:300–304.
2. Sonneville R, Klein I, de Broucker T, Wolff M. Post-infectious encephalitis in adults: diagnosis and manage-ment. J Infect 2009;58:321–328.
3. Mader I, Wolff M, Niemann G, Kuker W. Acute haemor-rhagic encephalomyelitis (AHEM): MRI findings. Neuro-pediatrics 2004;35:143–146.
4. Kuperan S, Ostrow P, Landi MK, Bakshi R. Acute hemor-rhagic leukoencephalitis vs ADEM: FLAIR MRI and neu-ropathology findings. Neurology 2003;60:721–722.
5. Lann MA, Lovell MA, Kleinschmidt-DeMasters BK.Acute hemorrhagic leukoencephalitis: a critical entity forforensic pathologists to recognize. Am J Forensic MedPathol 2010;31:7–11.
6. Dale RC, de Sousa C, Chong WK, Cox TC, Harding B,Neville BG. Acute disseminated encephalomyelitis, multi-phasic disseminated encephalomyelitis and multiple scle-rosis in children. Brain 2000;123:2407–2422.
7. Stone MJ, Hawkins CP. A medical overview of encephali-tis. Neuropsychol Rehabil 2007;17:429–449.
8. Payne ET, Rutka JT, Ho TK, Halliday WC, Banwell BL.Treatment leading to dramatic recovery in acute hemor-rhagic leukoencephalitis. J Child Neurol 2007;22:109–113.
9. Markus R, Brew BJ, Turner J, Pell M. Successful outcomewith aggressive treatment of acute haemorrhagic leukoen-cephalitis. J Neurol Neurosurg Psychiatry 1997;63:551.
Neurology 76 May 31, 2011 e109
DOI 10.1212/WNL.0b013e31821d748a2011;76;e106-e109 Neurology
Tuhin Virmani, Ashima Agarwal and Eric C. Klawiterlesions
Clinical Reasoning: A young adult presents with focal weakness and hemorrhagic brain
This information is current as of May 30, 2011
ServicesUpdated Information &
http://n.neurology.org/content/76/22/e106.fullincluding high resolution figures, can be found at:
References http://n.neurology.org/content/76/22/e106.full#ref-list-1
This article cites 9 articles, 2 of which you can access for free at:
Subspecialty Collections
http://n.neurology.org/cgi/collection/postinfectious_Post-infectious
http://n.neurology.org/cgi/collection/mriMRI
http://n.neurology.org/cgi/collection/encephalitisEncephalitis
http://n.neurology.org/cgi/collection/autoimmune_diseasesAutoimmune diseases
http://n.neurology.org/cgi/collection/all_demyelinating_disease_cnsAll Demyelinating disease (CNS)following collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.neurology.org/about/about_the_journal#permissionsits entirety can be found online at:Information about reproducing this article in parts (figures,tables) or in
Reprints
http://n.neurology.org/subscribers/advertiseInformation about ordering reprints can be found online:
rights reserved. Print ISSN: 0028-3878. Online ISSN: 1526-632X.1951, it is now a weekly with 48 issues per year. Copyright Copyright © 2011 by AAN Enterprises, Inc.. All
® is the official journal of the American Academy of Neurology. Published continuously sinceNeurology




![Medulloblastoma: [Print] - eMedicine Neurology · emedicine.medscape.com eMedicine Specialties > Neurology > Pediatric Neurology Medulloblastoma George I Jallo, MD, Associate Professor](https://static.fdocuments.net/doc/165x107/5d472c3c88c993527c8b60e5/medulloblastoma-print-emedicine-neurology-emedicinemedscapecom-emedicine.jpg)













