Feline Colonic Disorders

of 14
-
Upload
tanersoysuren -
Category
Documents
-
view
233 -
download
0
Transcript of Feline Colonic Disorders
-
8/14/2019 Feline Colonic Disorders
1/14
Vol. 21, No. 8 August 1999 20TH ANNIVERSARY
Refereed Peer Review
FOCAL POINT
KEY FACTS
5Feline colonic disease presentseither as large bowel diarrhea or
constipation; the key to proper
management is to identify the
inciting cause if possible and
choose the appropriate dietaryand/or pharmacologic
intervention program.
Diet and Drugs:The Keys to ManagingFeline Colonic DiseaseTexas A&M University
Debra L. Zoran, DVM, PhD
ABSTRACT: Feline colonic diseases are less common than diseases of the small bowel but are
nevertheless diagnostic and therapeutic challenges. One aspect of developing a rational ap-
proach to diagnosing and treating colonic disease is to understand the colons unique physio-
logic and functional differences. Large bowel diarrhea can be acute (present for less than 3
weeks) or chronic. Acute diarrhea is often associated with dietary disturbances (e.g., dietary
indiscretion, food intolerance) or infectious/inflammatory diseases, including parasitic or pro-
tozoal infestations. Empiric therapy with antibiotics or anthelmintics or dietary changes often
correct the problem. However, many chronic colonic diseases (e.g., inflammatory bowel dis-
ease, neoplasia) require lifelong pharmacologic and/or dietary intervention.
Gastrointestinal (GI) tract diseases are common causes of anorexia, vomit-ing, diarrhea, and weight loss in cats. Diseases affecting the colon are lesscommon than those affecting the remainder of the GI tract and general-
ly cause fewer signs. Because of the less demanding presentation, however,chronic disorders of the large bowel often pose diagnostic and therapeutic chal-lenges for practitioners. Disturbances of large intestinal function are typicallycategorized into two groups: disorders causing diarrhea and those resulting inconstipation. These categories can be further defined as acute disorders, whichare often responsive to dietary and/or empiric treatment approaches, and chron-
ic and/or recurrent disorders, which require an aggressive, systematic diagnosticand therapeutic approach. This article reviews common causes of feline largebowel diarrhea and constipation and discusses the approach to diagnosing andmanaging colonic disease, with special emphasis on the appropriate use of di-etary therapy.
UNDERSTANDING COLON PHYSIOLOGYThe physiology and function of the feline colon are unique compared with
the remainder of the GI tract.1Although the colons storage function and role inwater and electrolyte balance are well known, its importance in other aspects ofnormal physiology are not. Much has been learned about certain aspects of nor-mal and abnormal feline colonic function, such as the importance of different
CE
s Dietary fibers are divided into
soluble and insoluble groups,
which have complex and entirely
different effects in the colonic
lumen and on colonocytes.
s Dietary intolerance is a form of
diet-induced diarrheal disease
caused by nonimmunologic
reactions to a food or food
substance, whereas true dietary
allergy is an immunologic reaction
to a specific component of food.
s Inflammatory bowel disease,
which is a diagnosis of exclusion,
requires histopathology for
diagnosis.
s Constipation is a common,
reversible problem in cats that
has many causes; however,
untreated or chronic constipation
will lead to irreversible colon
damage resulting in obstipation
or megacolon.
-
8/14/2019 Feline Colonic Disorders
2/14
cell populations in inflammatory boweldisease (IBD), normal colonic motility,and role of cisapride in the managementof megacolon. However, information isstill lacking in other areas, such as the ef-
fects of different diets, especially dietaryfiber; the role of the intestinal microbialpopulation in the development of IBDand colitis and its effect on dietary com-ponents; the connection between IBD andlymphosarcoma; and the effect of dietarysensitivity in IBD. Diseases of the colonhave often been considered as extensionsof diseases affecting the small intestine,and thus many are treated with smallbowel disease in mind. However, man-agement of colonic disease is most effec-
tive if treatment is implemented with nor-mal colon physiology in mind.One of the unique functions of the
colon is the further digestion of unab-sorbed carbohydrates, proteins, and dietaryfiber by the luminal bacterial flora. Thedegradation of this undigested material inthe colonic lumen results in the formationof short-chain fatty acids (SCFAs; e.g., acetate, propi-onate, and butyrate) as well as carbon dioxide, water,methane, and hydrogen gas.2 Luminal SCFAs acidifythe luminal microenvironment, which may keep poten-
tially toxic or mutagenic compounds in an un-ionizedform3; are precursors for lipid synthetic (cholesterol, fat-ty acids) and gluconeogenic pathways in the liver4; andhelp maintain normal colonic fluid and electrolyte bal-ance.5 SCFAs also help maintain a healthy bacterial pop-ulation, which reduces the intrusion of pathogenic oropportunistic bacteria.
In rats, pigs, and humans, butyrate is rapidly ab-sorbed by colonic epithelial cells and is used preferen-tially for metabolic energy over glucose, glutamine, andthe other SCFAs.6,7 Studies of colonocyte fuel utiliza-tion in cats have not been conducted. Because colono-
cytes have a short life span (approximately 4 to 7 days),a readily available source of metabolic energy is neededto sustain their ability to proliferate. The presence ofbutyrate in the lumen serves this purpose, much likeglutamine does for small intestinal cells. In humans androdent models, a lack of butyrate has been associated
with the development of colitis and starved colonsyndrome.8
The most important dietary source of butyrate isfiber. Dietary fiber is a catch-all term for a heteroge-neous group of complex carbohydrates that are notreadily broken down by the digestive enzymes of the
normal mammalian intestine but are fermented (de-graded) by enzymes produced by colonic (and small in-testinal) bacteria. Soluble (highly fermentable) fibers,such as oat bran, pectin, beet pulp, or vegetable gums,
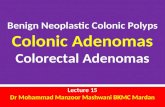
are readily digested by colonic bacteria and produce thelargest quantities of SCFAs (Figure 1).9 However, be-cause soluble fibers are so completely degraded, they re-tain less ability to increase fecal bulk or dilute luminaltoxins.10 Insoluble (poorly fermentable) fibers, such ascellulose, methylcellulose, coarse wheat bran, or thehulls of oats/peas, are degraded by colonic bacteria moreslowly and thus retain a greater dilution potential andfecal bulking capacity.9 Fibers that increase fecal bulk areimportant for several reasons: They improve or normal-ize colonic motility by distending colonic lumen, diluteluminal toxins (e.g., secondary bile acids, ammonia, in-
gested toxins), and increase the rate of passage of ingest-ed material to reduce the exposure of colonic epithelialcells to luminal toxins.11
CAUSES OF LARGE BOWEL DIARRHEAThe characteristics of large bowel diarrhea include
hematochezia, increased mucus in and on the feces, in-creased frequency and urgency of defecation, increasedtenesmus associated with defecation, and generally soft-formed to loose stools. Vomiting, dehydration, and
weight loss are not commonly associated with colonicdisease but may occur in cats with chronic constipa-
Small Animal/Exotics 20TH ANNIVERSARY Compendium August 1999
I N F L A M M A T O R Y B O W E L D I S E A S E s S H O R T - C H A I N F A T T Y A C I D S s F I B E R
Figure 1The effects of soluble (highly fermentable) and insoluble (less ferment-able) dietary fibers on the gastrointestinal tract. (LI= large intestine; SCFAs=short-chain fatty acids; SI= small intestine)
Soluble Fibers Insoluble Fibers
Decreased gastric emptying
Slowed SI transit
Slowed LI transitIncreased SCFAs
Reduced luminal pHIncreased mucosal growth
Decreased pathogen growthReduced dilution potential
Reduced fecal weight
Increased gastricemptying
Increased SItransit
Increased LI transitDecreased SCFAs compared
with soluble fiberIncreased dilution of
luminal contentsIncreased absorption of
luminal toxinsIncreased fecal weight
Stomach
Colon
Smallintestine
-
8/14/2019 Feline Colonic Disorders
3/14
tion, colonic neoplasia, or severe colonic IBD. Condi-tions causing large bowel diarrhea in cats generally fitinto one of four categories: (1) infectious diseases, in-cluding bacterial, viral, and fungal (and, for the purpos-es of this article, parasitic and protozoal) diseases; (2)dietary allergy, intolerance, or indiscretion; (3) IBD; or(4) neoplasia (Table I). These diseases or disorders canbe further categorized as acute or chronic.
Acute large bowel diarrheal episodes are often appro-priately managed by dietary changes and/or empiric
pharmacotherapy. Pharmacotherapy for acute largebowel diarrhea may include antibiotics, anthelmintics,or motility-modifying agents (e.g., loperamide; TableII); however, the use of empiric therapy should be de-termined after carefully evaluating the cats signalment,history, and physical examination for other diseases thatrequire additional assessment. In cats with chronic (du-ration of more than 3 to 4 weeks) or recurrent largebowel diarrhea, a definitive diagnosis must be obtainedfor effective treatment to be instituted (Figure 2). Manycats with chronic colitis will require both dietary andpharmacologic therapy to control the disease. However,
appropriate use of dietary therapy may reduce the needfor drug therapy and also may increase the duration ofclinical remission.
Acute Large Bowel DiarrheaDietary AspectsIndiscretion. Cats are more fastidious eaters than are
dogs; nevertheless, dietary indiscretion is an importantcause of acute feline diarrhea, especially in young catsor kittens. Dietary indiscretion in cats is often caused
by a change in diet (e.g., new diet, introduction of hu-man food, or prey consumption) but may result fromconsumption of foreign substances (e.g., hair, string,rubber bands, plants). Longhaired cats may have inter-mittent bouts of large bowel diarrhea associated withthe passage of a hair mass, which may alter colonicmotility or cause irritant colitis. The addition of dietaryfiber (a strategy used by a new commercial hairballdiet) or lubrication (e.g., hairball remedies) to soften afecal mass are the most common therapeutic methodsof combating this problem. Diets that contain in-creased insoluble fiber are often successfully used to
Compendium August 1999 20TH ANNIVERSARY Small Animal/Exotics
C A U S E S s D I E T C H A N G E s F O R E I G N S U B S T A N C E S
TABLE I
Causes of Large Bowel Diarrhea in Cats
Inflammatory or Infectious
BacterialSalmonellaspecies,Clostridium perfringens,Clostridium difficile,Campylobacterspecies,Yersinia enterocolitica,Escherichia coli,Mycobacterium
ViralFeLV (neoplasia), FIV,FIP (rare), panleukopenia(kittens)
Dietary Allergy,Intolerance, or Indiscretion
AllergyProtein, glycoproteins
IntoleranceAdditives, preservatives,flavors, colors, histamine,protein, carbohydrates
IndiscretionOvereating, change of diet,new food, garbage intake,prey, foreign body
Neoplastic
Malignant tumorsAdenocarcinoma,lymphosarcoma,mast-cell tumor,fibrosarcoma,undifferentiated sarcoma
Benign tumorsPlasmacytoma, leiomyoma,adenomatous polyps
Inflammatory Bowel Disease
LymphoplasmacyticIdiopathic; most common
EosinophilicMay be associated withdietary allergy
NeutrophilicMay be present secondary toan infectious agent
GranulomatousRare in cats
aMore common in the small intestine.FeLV= feline leukemia virus; FIP= feline infectious peritonitis; FIV= feline immunodeficiency virus.
Parasitic/protozoal/fungal/miscellaneousCryptosporidiosisa, coccidiaa,giardiasisa, toxoplasmosisa,pentatrichomonas,histoplasmosis, pythiosis,Balantidium coli, Entamoeba,phycomycosis
-
8/14/2019 Feline Colonic Disorders
4/14
manage acute colitis due to dietary indiscretion; the in-creased fecal bulk and fecal water content normalizecolonic motor activity and protect colonocytes from lu-minal toxins or irritants11 (Tables III and IV).
Fructooligosaccharides. Fructooligosaccharides(FOS) are complex carbohydrates with a glucose at-tached to two or more fructose units. FOS are digestedby the microbes of the colon (rather than in the smallintestine by mammalian enzymes) to produce SCFAsmuch like soluble dietary fiber.12 There is increasing ev-idence in humans that adding FOS to the diet increasesthe number of bifidobacteria, the normal beneficial flo-ra, in the large intestine.13 FOS have also been helpfulin treating secretory diarrhea in humans and pigs, pre-sumably by increasing the number of beneficial bacteria
while slowing the growth of pathogenic bacterial
species.14 In dogs and cats, FOS are readily fermentedin the colon to produce SCFAs.15
In a recent study examining the effects of FOS onsmall intestinal bacterial overgrowth in dogs, FOS sup-
plementation did not reduce or alter the growth ofpathogenic species.16 However, the normal small intes-tine of dogs does not have a large population of bacte-ria that utilizes FOS. Alternatively, there is strong evi-dence that cats have a significant population of normalbacteria in the small intestine.17A preliminary study ofthe effects of FOS on small intestinal bacterial popula-tions in cats found no effect on bacterial numbers orspecies in the duodenum.17 Conversely, FOS supple-mentation did alter the fecal microflora of healthy catsby increasing the numbers oflactobacilli and Bacteroidesspecies while significantly decreasing the numbers of
Small Animal/Exotics 20TH ANNIVERSARY Compendium August 1999
B I F I D O B A C T E R I A s S E C R E T O R Y D I A R R H E A s B A C T E R I A L O V E R G R O W T H
TABLE II
Drugs for Treating Feline Large Bowel Diseasesa
Dose Frequency Drug (mg/kg) Route (hourly interval b) Indications
AntibioticsAmpicillin 1122 PO, IM, IV 8 Anaerobic and gram-positive bacterial
infectionsCephalosporins 1133 PO, IM, IV 612 Anaerobic and aerobic bacterial infectionsClindamycin 511 PO, IM 12 Toxoplasmosis, anaerobic infectionsDoxycycline 2.55 PO 12 Aerobic, anaerobic, and intracellular
bacterial infectionsEnrofloxacin 12 PO, SC 12 Gram-positive and -negative infectionsFurazolidone 4 PO 12 Resistant giardiasisMetronidazole 1025 PO 1224 Colitis, IBD, giardiasisTylosin 510 PO 12 Bacterial infectionsTetracycline 1020 PO 8 Aerobic, anaerobic, and intracellular
bacterial infectionsTrimethoprim sulfa 30 PO 1224 Gram-positive and -negative bacterial
infection, toxoplasmosis
AnthelminticsFenbendazole 2550 PO 24 for 36 days Ascarids, flukes, GiardiaPyrantel pamoate 510 PO 24 Acarids
AntiinflammatoriesAzathioprine 0.20.3 PO 2448 IBDChlorambucil 0.250.33 PO 3 days IBDPrednisolone 14 PO, IM 1224 IBDSulfasalazine 1020 PO 824 IBD
MiscellaneousCisapride 0.30.5 PO 812 Colonic motility disorders, megacolonCyproheptadine 12 PO 1224 Stimulate appetite
Diphenhydramine 2.2 PO 1224 Decrease histamineDiphenoxylate HCl 0.0630.6 PO 8 AntidiarrhealLoperamide 0.04 PO 1224 Antidiarrheal
aDosages are recommendations only and must be tailored to the needs of the patient.bUnless otherwise specified.IBD= inflammatory bowel disease; IM= intramuscularly; IV= intravenously; PO= orally; SC= subcutaneously.
-
8/14/2019 Feline Colonic Disorders
5/14
clostridia and Escherichia coli.18 Although dietary FOS
supplementation may alter the fecal flora of healthycats, whether it effectively alters the microflora of catswith colonic disease is unknown. Nevertheless, severalcommercial diets have added FOS to their diet formu-lations (Table III).Intolerance. Dietary intolerance is a diet-induced di-
arrheal condition initiated by a nonimmunologic re-sponse to a substance that may or may not be food. 19
One example of food intolerance is lactose intolerance,in which diarrhea results from intestinal lactase deficien-cy. However, food intolerance can be caused by foodcomponents, such as coloring, flavoring, preservatives,
or vasoactive substances (e.g., histamine, spermine).19
Finally, nonimmunologic adverse responses to protein,carbohydrate, or lipid sources in a diet also occur (e.g.,gluten intolerance), but these are not well documentedin cats.19 There is no definitive diagnostic test for dietaryintolerance other than elimination of the offending sub-stance by food trial. Cats with dietary intolerance willrespond to any diet that does not contain the offendingsubstance, and diets that are highly digestible and hy-poallergenic will often be effective (Table III).Allergy/Hypersensitivity. In contrast, dietary allergy or
hypersensitivity is an adverse reaction to a food or foodadditive that has a proven immunologic basis.19 Almost
Compendium August 1999 20TH ANNIVERSARY Small Animal/Exotics
L A C T O S E I N T O L E R A N C E s F O O D C O M P O N E N T S s F O O D T R I A L
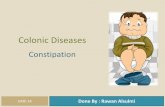
Figure 2Algorithm of a suggested diagnostic pathway for evaluating cats with acute or chronic large bowel diarrhea. ( FeLV= fe-line leukemia virus; FIV= feline immunodeficiency virus; FPL= feline panleukopenia, TLI= trypsinlike immunoreactivity)
Diagnosing Large Bowel Diarrhea
Fecal flotation
Large bowel diarrhea
Acute (1 mo)
Minimum databaseFecal examinations (as per acute)
Viral testing (FeLV, FIV, FPL)Toxoplasma titers, TLI assay
Positive
Treat
Negative
Imaging studies(radiology, ultrasonography)
Endoscopy (biopsy)
NegativePositive
Repeat diagnosticsConsider elimination diet
Treat
-
8/14/2019 Feline Colonic Disorders
6/14
-
8/14/2019 Feline Colonic Disorders
7/14
all food allergens in cats are proteins or glycoproteinsfrom beef, fish, eggs, chicken, pork, rabbit, or dairy prod-ucts, but sensitivity to lamb has also been reported.20,21
The clinical signs associated with an allergic reaction tofood can be cutaneous (e.g., facial pruritus, miliary der-
matitis, endocrine alopecia, eosinophilic granuloma, gen-eralized pruritus) or gastrointestinal (e.g., acute or chronicvomiting or diarrhea). Although cutaneous signs report-edly occur in up to 30% of cats with food hypersensitivi-ty, prevalence of GI signs is unknown.20
Diagnosing dietary allergy is difficult, primarily be-cause a 6- to 12-week food-elimination trial is required.Measurement of allergen-specific IgE via skin testing orserum-based immunoassays (e.g., radioallergosorbenttest [RAST], ELISA, monoclonal antibodybasedELISA) and gastroscopic food-sensitivity testing havebeen proposed as alternative diagnostic approaches to
elimination diets; however, these tests have been incon-sistent and unreliable (false-positive and -negative re-sults are common) and are thus not recommend-ed.20,22,23 Both intradermal skin testing and ELISA orRAST tests have a high incidence of false-positive val-ues (40% to 60%), which may be caused by food anti-gen alteration during processing, digestion, or me-tabolism.23 Gastroscopic food testing is a good test forruling out food sensitivity (i.e., it has a very high nega-tive predictive value), but false-positive reactions arerelatively common.23 In addition, skin and gastroscopictests will not positively identify animals that have a de-
layed hypersensitivity response (not mediated by IgE)as having an allergic response.23
The best diets for identifying and treating food aller-gies are homemade elimination diets that contain novelprotein sources that have highly digestible, modified
proteins smaller than 18,000 D.
24
Several recent reviewshave addressed this subject and provided recipes andcommercial dietary information concerning hypoaller-genic diets.23A food-elimination trial is initiated by en-suring that all food sources other than the prescribeddiet are removed from the diet, including flavor-coatedantibiotic or preventative preparations and nonhypoal-lergenic treats. It is important that owners realize thatcats can also acquire a sensitivity to the protein in thetherapeutic diet, and thus a recurrence of signs may oc-cur.
Although homemade diets are good for diagnostic
purposes, they may fail for long-term management offood hypersensitivities because many clients are unwill-ing or unable to prepare consistent, balanced diets fortheir cats. A recent study showed that a large percentage(80%) of homemade diets were nutritionally inadequatefor the maintenance of adult cats.19An imbalanced dietmay not be too detrimental during the course of a di-etary trial but over several months will create protein de-ficiency, deficiency of specific amino acids or essentialfatty acids (e.g., taurine, arachidonic acid), or vitaminand mineral imbalances.19 Several commercial hypoal-lergenic or limited-antigen diets have been developed
Compendium August 1999 20TH ANNIVERSARY Small Animal/Exotics
S K I N T E S T I N G s G A S T R O S C O P I C F O O D T E S T I N G s H O M E M A D E D I E T S
TABLE IV
Soluble and Insoluble Sources of Dietary Fiber24,a,b
Soluble Insoluble Combination
Vegetable gums Cellulose Metamucil (Procter & Gamble, Cincinnati, OH)
Carrageenans Wheat bran/germ Oat/rice bran (including oatmeal)
Mucilages Hemicelluloses Pea fiber (whole or soup)
Pectins Lignins Beans (whole, pinto, kidney)
Oligosaccharides Methylcellulose (Citrucel; Potatoes (with skin)(e.g., lactulose or FOS) SmithKline Beecham,
Pittsburgh, PA)
Potatoes (no skin) Pumpkin (canned)
Fibercon (Lederle, Philadelphia, PA)
aSoluble (highly fermentable) and insoluble (less fermentable) fiber sources do not contain exclusively one fiber type but rather amajority of one type and minimal amounts of the other.bThis table provides a representative listing of products and is not exhaustive.FOS= fructooligosaccharides.
-
8/14/2019 Feline Colonic Disorders
8/14
for treating dietary allergy(Table III). These diets areformulated with unique pro-tein and carbohydratesources; some have other ad-
ditives (e.g., added omega-3[n-3] fatty acids), however,and thus a lack of responseto one commercial reduced-antigen diet does not neces-sarily rule out dietary allergy.Keys to successful manage-ment of cats with food hy-persensitivity include persis-tence and flexibility becausemultiple food trials may berequired to find the best diet
for the patient.
Infectious CausesInfectious diseases, including parasitic or protozoal
infections, are a frequent cause of acute large bowel di-arrhea in cats (Table I). Evaluation of a cat with acutecolitis should begin with obtaining a good history, es-pecially a complete dietary history. All cats with largeintestinal diarrhea should have multiple fecal flotations(three to five over several days), using salt and sugarflotation media and zinc sulfate centrifugation tech-niques. Microscopic examination of feces using saline-
mounted direct smears and stained specimens (fecal cy-tology using Diff-Quik or Wright stains) are alsoexcellent diagnostic tests. Fecal cytology is used to iden-tify clostridial spores, Histoplasmaorganisms, Giardia, orother protozoal agents as well as to characterize the typeand degree of inflammation. Special sedimentationtechniques (e.g., Baerman) should be considered afterother avenues of evaluating the fecal specimen havebeen explored. It is rarely necessary to culture feces incats with acute colonic disease; however, in some cats
with chronic colitis, a fecal culture may be indicated.The key to obtaining diagnostic fecal cultures is col-
lecting and transporting samples in media appropriatefor each organism. For example, microaerophilic trans-port and culture conditions are required to cultureCampylobacter from fecal samples, and thus specialtransport tubes and media (Campy BAP) are necessary.Culturing obligate anaerobes from feces requires spe-cialized transport tubes and sample handling and is avery difficult, time-consuming laboratory process;therefore, culture of fecal anaerobes may not be rou-tinely available at some commercial microbiology labo-ratories. It is essential to find a laboratory that is capa-ble of handling such requests and then obtain the
specific media and transporttubes needed.
Clostridiumspecies are nor-mal inhabitants of the felinesmall intestine and colon.
Under the normal, acidicconditions of the colonic lu-men (with the presence ofnormal anaerobic flora),these potential pathogens donot cause problems. Howev-er, after a change in diet,stressful event or illness, orantibiotic therapy that altersthe normal bacterial flora,clostridia wi ll overgrow,sporulate, and produce en-
terotoxin. The enterotoxinis believed to be responsiblefor the development of diarrhea in affected animals.25
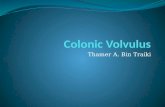
Clostridial enterocolitis is well recognized in dogs butis a less common cause of diarrhea in cats. In addition,there is little information regarding cats on the compar-ative usefulness of identification of spores versus detec-tion of enterotoxin by commercial assays. In dogs, diag-nosis of clostridial colitis has previously been based onthe identification of safety-pinshaped spores on stainedfecal smears (Figure 3). However, the presence of sporesdoes not necessarily indicate the presence of enterotox-
in; thus assays for detection of enterotoxin have beenused to guide treatment.The reverse passive latex antigen (RPLA) kit was re-
cently compared with fecal spore counts for diagnosisof clostridial enterocolitis in dogs. A poor correlationamong fecal spore counts, clinical signs, and theRPLA assay was found.25 The other commercial kit,an ELISA, has not been evaluated in dogs or cats, soits effectiveness is unknown. Thus, until assays for de-tection of enterotoxin in feces are validated, diagnosisof clostridial enterocolitis in cats should be based onfinding large numbers of spores on a stained fecal
smear as well as on the response to treatment. Treat-ment with antibiotics with an anaerobic spectrum(e.g., ampicillin/amoxicillin, metronidazole, clin-damycin, tylosin) for 5 to 7 days is effective in mostcases. In addition to antibiotic therapy, adding solublefiber or FOS to the diet may enhance the recovery ofthe normal bacterial flora and acidify the colonic lu-men, which may inhibit further clostridial sporulation(Table III).
Other specific infectious causes of enterocolitis incats include E. coli; Clostridium difficile; and Salmonella,Campylobacter, Giardia, and Entamoebaspecies. (Table
Small Animal/Exotics 20TH ANNIVERSARY Compendium August 1999
F E C A L F L O T A T I O N S s C L O S T R I D I A L E N T E R O C O L I T I S s R P L A A S S A Y
Figure 3Photomicrograph of a fecal smear stained withDiff-Quik showing clostridial spores (safety-pin structures)surrounded by epithelial cells and bacteria. The examination
was performed with the 100 objective under oil immersion.
-
8/14/2019 Feline Colonic Disorders
9/14
I). These infectious agents rarely cause clinical diseasein cats (most cases are asymptomatic), with the excep-tion of giardiasis26; however, Giardia species usuallycause small bowel diarrhea instead of colitis. Cats thatdevelop enterocolitis caused by these agents are often
purebred, cattery-raised, young, or immunocompro-mised (feline leukemia virus [FeLV] or feline immuno-deficiency viruspositive).27 Cats may shed these organ-isms for many weeks following clinical or subclinicalinfections.26 This is especially important because mostof these agents are zoonotic, making client communica-tion and awareness essential.
Chronic Large Bowel DiarrheaAs in any chronic disease process, it is very important
in chronic large bowel diarrhea to obtain a definitivediagnosis for the best chance at treatment success. The
first, and possibly most important, step is to obtain acomplete history, including onset, frequency of signs,character of fecal mass, presence or absence of blood ormucus, presence of vomiting or weight loss, and any ef-fective treatments as well as a complete dietary history.
A dietary history should include any changes in diet; allcomponents of the diet, including table foods; howlong the current diet has been fed; and how much isfed. The diagnostic approach to chronic diarrheashould follow the algorithm for evaluating a cat withacute diarrhea (e.g., multiple fecal examinations andempiric or dietary therapy as indicated). However, in
many cats, a minimum database (including thyroxine ifindicated), survey or contrast radiographs, and ultra-sonography may be necessary. Ultimately, other diag-nostics, such as fecal culture, intestinal permeability as-says (e.g., hydrogen breath tests, fecal -1 protease),specialized tests of motility (e.g., scintigraphy), or en-doscopy (to obtain biopsies, aspirates, or cytology ofthe GI tract), may be indicated (Figure 2).
Inflammatory Bowel DiseaseThe diagnosis and medical management of feline
IBD has changed very little in the past several years.
This is primarily because the disease continues to be adiagnosis of exclusion for which the pathogenesis re-mains largely unknown, despite considerable researchinto the immunologic mechanisms and histologic pat-terns of IBD. Therefore, IBD remains an idiopathicdisease for which a definitive cause is unknown.28,29 Themost common histologic classification of colonic IBDin cats is lymphoplasmacytic colitis.2831 However,eosinophilic, neutrophilic, and granulomatous infil-trates occur with variable frequency. Any of these in-flammatory conditions may occur as a primary colonicdisease but may also be associated with disease of the
small bowel or stomach. Thus, it is reasonable to per-form gastric and duodenal biopsies on cats that appearto have only large bowel diarrhea. In addition, the en-doscopic appearance of the region should be noted be-cause mucosal friability, erythema, and ulceration may
occur with IBD.
30
Despite mucosal appearance, it is ex-tremely important to obtain multiple (e.g., six to eight)high-quality (presence of submucosa, not just mucosaltissue) biopsies from each location (including normal-appearing mucosa).
The treatment of feline IBD continues to be pred-nisolone and metronidazole in combination or sepa-rately3032 (Table II). The reasons for the effectiveness ofmetronidazole in feline IBD may be multifactorial andinclude its anaerobic antibacterial spectrum, effective-ness against Giardia, and proposed immunomodulatingeffects on the gut. Antibacterial therapy (e.g., tylosin,
metronidazole, amoxicillin, tetracycline) may be indi-cated in cats with a neutrophilic inflammatory compo-nent, whereas cats with eosinophilic enterocolitis willoften require aggressive therapy with prednisolone orother immunosuppressive agents.33 Azathioprine, cy-closporine, chlorambucil, and sulfasalazine/olsalazineare used to reduce the dose of prednisolone required forlong-term maintenance or in those cats that are intoler-ant of, or poorly responsive to, prednisolone therapy.33
Although it is unusual to need 5-aminosalicylatecontaining drugs (e.g., sulfasalazine, olsalazine/me-salamine) to manage feline colonic IBD, sulfasalazine
has been recommended for cats with IBD unresponsiveto other therapies.30,33 Olsalazine and the other mesal-amine-containing, antileukotriene drugs used in humanand canine colitis have not been evaluated in cats. Therisk of salicylate toxicity must be considered but ap-pears to be minimized if a low dose is used.33 Omega-3fatty acids have also been included in diets used fortreating feline IBD because of their antiinflammatoryproperties.34 Omega-3 fatty acids reduce inflammationby altering the fatty acid profile of lipid membranes sothat cyclooxygenase and lipoxygenase action on the fat-ty acid releases the 3-series prostaglandins and
leukotrienes, which are antiinflammatory comparedwith the normal 2-series prostaglandins.34 However,there have been no controlled studies of the effective-ness of these agents for treating feline IBD. As newertherapeutic approaches are being developed for use inhuman IBD (e.g., biologic therapy [tumor necrosis fac-tor-]) and specific nitric oxide synthase or cyclooxyge-nase-2 inhibitors are identified, the therapeutic optionsfor cats with IBD will expand.
In addition to the pharmacologic management of fe-line IBD, there is keen interest in the role of diet.There are a few cats for which dietary therapy alone
Small Animal/Exotics 20TH ANNIVERSARY Compendium August 1999
L Y M P H O P L A S M A C Y T I C C O L I T I S s P R E D N I S O L O N E s M E T R O N I D A Z O L E
-
8/14/2019 Feline Colonic Disorders
10/14
will be sufficient to control IBD. These cats usuallyhave either fiber-responsive colitis or dietary intoler-ance/sensitivity as the cause of the diarrhea. However,the goal of dietary therapy in those cats that do nothave diet-responsive colitis is to reduce disease severity,
frequency of relapses, and drugs needed to control thedisease. One of the reasons dietary intervention is advo-cated in treating IBD is the hypothesis that dietary al-lergy may have an important role in the disease. Onekey is that multiple hypoallergenic diets may have to betried before an effective diet is discovered. This is a tri-al-and-error process that, until better methods for iden-tifying food hypersensitivity are developed, is the onlyaccurate means of diagnosing this disease.
In human colonic IBD, increasing the amount of bu-tyrate available to the colonic epithelium reduces theincidence and severity of disease recurrences.35Whether
this effect is important in feline colonic IBD is un-known. Because there have been few studies in cats onthe effects of soluble or insoluble dietary fiber on nor-mal colonic function, it is difficult to make specific rec-ommendations concerning dietary fiber for cats withIBD. In addition, because of the presence of a signifi-cant population of bacteria in the small intestine ofcats, fiber may be metabolized quite differently by thisspecies.17 However, adding modest amounts of solubleand/or insoluble fiber to the diet to increase fecal bulkand motility while providing a source of butyrate as acolonic fuel source seems reasonable as part of the man-
agement of feline IBD. There are several high-fiber di-ets available commercially, but each has different typesand amounts of fiber (Table III). There have been nostudies performed to determine the beneficial or ad-verse effects of these different fiber sources in cats withIBD. Finally, some cats with colonic IBD may respondbest to a diet that is highly digestible, which will leaveless residue for the diseased colon or the abnormal mi-croflora to act upon. Until a better understanding of fe-line IBD is achieved, the role of diet in the develop-ment or treatment of feline colonic disease will remainuncertain.
NeoplasiaNeoplasia of the intestinal tract in cats, representing
less than 1% of all tumors, is uncommon comparedwith tumors in other sites.36,37 Tumors of the colon arerare, but adenocarcinoma, lymphoma, and mast-cell tu-mors are the most frequently reported feline colonic tu-mors; leiomyosarcoma, plasmacytoma, and fibrosarco-ma are also reported, but infrequently.36,37 The mostcommon nonhematopoietic neoplasm of the colon incats is adenocarcinoma.36,38 Unlike most other diseasesof the large bowel, weight loss is often the most com-
mon presenting complaint for cats with colonic neopla-sia; anorexia and hematochezia are also common pre-senting complaints. Most colonic neoplasia is not dis-covered until the tumor has metastasized. Nevertheless,examination of cats with a palpable or suspected ab-
dominal tumor should include routine hematologicand biochemical assays, radiographs (abdominal, con-trast, thoracic metastasis check), and ultrasonography
with fine-needle aspiration of lymph nodes or the massas indicated.
The incidence of intestinal adenocarcinoma metasta-sizing to regional lymph nodes, mesentery, omentum,and other abdominal organs is nearly 50%.3739Adeno-carcinomas and mast-cell tumors tend to create ob-structive lesions, whereas lymphomas are often infiltra-tive throughout large regions of the GI tract. 36,37
Diagnosis can be obtained via endoscopic biopsy in
many cats; however, an exploratory laparotomy is also areasonable approach because intestinal resection is thetreatment of choice for both adenocarcinomas andmast-cell tumors.36,39 Despite the fact that adenocarci-nomas metastasize early, cats can have long survivaltimes (e.g., average of 6 to 15 months, sometimes aslong as 4 years) after intestinal resection of the tu-mor.37,39 Cats with intestinal mast-cell tumors rarely livelonger than 4 to 6 months because of the aggressive na-ture of this neoplasm and lack of effective chemothera-py.37 Palliative therapy for intestinal mast-cell tumorsincludes histamine blockers and corticosteroids to re-
duce release of vasoactive amines; however, the effec-tiveness of these treatments is unknown.37
Lymphoma is the most common hematopoietic tu-mor of the GI tract in cats and can be part of multicen-tric disease or alimentary lymphosarcoma.37 Most cats
with alimentary lymphoma are FeLV-antigen negative,37
whereas most with multicentric lymphoma are FeLV-antigen positive. The presence or absence of FeLV anti-genemia may influence the long-term prognosis (i.e.,FeLV-positive cats often have shorter survival times as aresult of FeLV-associated disease rather than reduced re-sponsiveness to chemotherapy).37,40 Lymphosarcoma and
IBD can be quite difficult to distinguish by histo-pathology alone, especially in the early stages of the dis-ease; in cats with lymphoplasmacytic IBD that is unre-sponsive to conventional therapy, or when suspicion oflymphoma is high, immunocytochemistry for cell sur-face markers can be used to differentiate the two (lym-phomas are usually monoclonal [i.e., their origin is asingle cell clone that has identical cell surface markers]).These assays are not universally available and are quiteexpensive but may be invaluable for differentiatinglymphoma and IBD. Staging and treatment protocolsfor lymphoma are available in the literature.37
Compendium August 1999 20TH ANNIVERSARY Small Animal/Exotics
B U T Y R A T E s A D E N O C A R C I N O M A s L Y M P H O M A
-
8/14/2019 Feline Colonic Disorders
11/14
Constipation, Obstipation, and MegacolonConstipation is a common problem in cats. The con-dition can be induced by changes in diet or environ-ment (e.g., soiled litter, hospitalization, new cat), inges-tion of foreign objects (e.g., hair, string, plants, bones,feathers), intra- and extraluminal obstructions (e.g., tu-mors, intussusception, pelvic fractures, anal stricture,hair mats around anus), ileus (e.g., postoperative, in-flammatory, metabolic), neurologic diseases (e.g.,dysautonomia, paraplegia, Manx cats with sacral spinalcord deformity), drug therapy (e.g., anticholinergics,opioids, antacids, sucralfate), dehydration, or miscella-
neous causes (e.g., hypokalemia, hyperparathyroidism,physical disability).41 Obstipationis intractable constipa-tion, and its presence implies loss of colonic function.Feline megacolon can be acquired (chronic constipa-tion or obstipation) or can result from idiopathic dila-tion of the colon caused by a loss of neuromuscularfunction.41
The key to effective management of feline constipa-tion is identification and correction of the cause. Un-complicated cases of constipation are resolved by restor-ing hydration status or assisting the removal of the fecalmass via administration of warm-water enemas and/or
Small Animal/Exotics 20TH ANNIVERSARY Compendium August 1999
O B S T I P A T I O N s M E G A C O L O N s M A N A G E M E N T
TABLE V
Laxatives for Treating Constipation in Catsa
FrequencyLaxative Dose Route (hourly interval) Trade Name
Bulk-formingPsyllium 12 tsp PO 1224 Metamucil (Procter & Gamble,
Cincinnati, OH)Methylcellulose 14 tsp PO 824 Citrucel(SmithKline Beecham,
Pittsburgh, PA)
EmollientsDioctyl sodium sulfosuccinate 2550 mg PO, per rectum 1224 Colace (Mead Johnson,
Evansville, IN)Dioctyl calcium sulfosuccinate 50100 mg PO, per rectum 24 Surfak (Hoechst Marion
Roussel, Kansas City, MO)
Lubricants
Petrolatum jelly 12 ml PO 24 Vaseline(Chesebrough-PondsUSA Co., Greenwich, CT)
Petrolatum jellybased 12 ml PO 1224 Laxatone(EVSCOPharmaceuticals, Buena, NJ),Laxaine(Pfizer Animal Health,New York, NY)
OsmoticsLactulose 1ml/cat PO, per rectum 812 ChronularCephulac(both from
(Hoechst Marion Roussel)Polyethylene glycol 2540 ml/kg PO 4 Colyte, GoLYTELY (bothand electrolytes (for bowel preparation) from Carter Products,
Cranbury, NJ)
SalineMagnesium hydroxide 510 ml (dogs) PO 1224 Milk of Magnesia(UDL Labs,
26 ml (cats) Rockford, IL)
StimulantBisacodyl 5 mg PO 24 Dulcolax(Novartis, East
Hanover, NJ)
aThis table provides a representative listing of products and is not exhaustive.PO= orally.
-
8/14/2019 Feline Colonic Disorders
12/14
stool softeners (e.g., dioctyl sulfosuccinate). Alterna-tively, uncomplicated constipation may be corrected by
increasing fecal bulk eithervia diet or pharmacologicmeans (e.g., laxatives; Table
V). Cats with recurrentconstipation due to an ob-structive lesion that causesconstipation that is not sur-gically correctable may re-quire lifelong dietary and/orlaxative therapy to controltheir disease.
Adding insoluble fiber tothe diet, which increases fe-cal bulk, can be very help-ful in managing constipation
if cats are well hydrated. In-creased fecal bulk creates alarger, softer stool that iseasier to pass and stimulatesan increase in segmentationand propulsion contractionsthat move the stool distal-ly.11 However, in cats thatare dehydrated or do notdrink adequate quantities of
water, large quantities of in-soluble fiber present in
some diets may contributeto constipation because thefecal mass becomes dehy-drated. Fibers that increasefecal bulk are pea fiber, oatfiber, coarse wheat bran,cellulose, methylcellulose,or pumpkin fiber.42 In cats
with colitis, increasing theamount of soluble fiber (toincrease SCFAs and de-crease fecal bulk) is pro-
posed to be beneficial.34
Commercial diets con-taining increased fiber aregenerally better for long-term fiber therapy than arediets to which fiber hasbeen added because theyare balanced and morepalatable (Table III). How-ever, commercial diets dif-fer in types and amounts ofdietary fiber, so diet selec-
tion is important. For example, Hills Prescription Dietr/d contains primarily insoluble fiber (cellulose orpeanut hulls), which is an excellent bulk-forming laxa-tive. Alternatively, an example of a diet formulationthat contains both soluble and insoluble fiber is IVDs
Feline Hifactor Formula
. Table IV illustrates a fewsources of soluble and insoluble fibers that are availablecommercially (health food stores, pharmacies, grocerystores) for managing fiber-responsive diseases by addingfiber to the cats regular diet.42
Laxatives are used to prevent or alleviate constipa-tion. The best general-purpose laxatives are bulk-form-ing (e.g., psyllium, methylcellulose), osmotic (e.g., lac-tulose), or emollient (e.g., docusate sodium/calcium)(Table V).32,33 However, osmotic and emollient laxativescan be irritating to the colonic mucosa and should notbe used before endoscopic procedures or in cats with
colitis or severe constipation that will likely have con-current colonic irritation.32 Magnesium-containingcathartic laxatives and phosphate-containing enemasshould not be used in cats because they may cause fatalhyperphosphatemia or hypermagnesemia. Stimulantlaxatives (e.g., bisacodyl) can be quite useful in cats
with chronic constipation, obstipation, or early-stagemegacolon. Bisacodyl stimulates inducible nitric oxidesynthetase,43 which increases colonic contractions butmay cause fatigue of the myenteric plexus if used con-tinuously over a long period (days to weeks). Prokineticagents (e.g., cisapride) can be used to increase colonic
smooth muscle contractions
44
and may be quite usefulfor treating cats with postoperative ileus; constipationdue to such chronic, irreparable conditions as neopla-sia; or idiopathic megacolon.41 Metoclopramide is aneffective prokinetic agent for the upper GI tract but isineffective in the colon. The cholinergic drugs (e.g.,bethanechol) are difficult to administer to cats and havenumerous side effects and thus should be avoided.
Feline idiopathic megacolon is an uncommon syn-drome for which pathogenesis is slowly beginning to beunderstood. Recent studies suggest that colonic smoothmuscle function is impaired in cats with this disease
and that the use of cisapride is effective in improvingcolonic function in cats with some remaining colonicmotor function.44 In its early stages (i.e., dilated colonfor typically less than 6 months), this disease is usuallymanaged with combination therapy that includes oneor all of the following: increased dietary fiber (bulk),osmotic laxatives (lactulose), stimulant laxatives(bisacodyl), and cisapride (up to 10 mg/kg every 12hours) along with occasional warm-water enemas asneeded. The oral colonic lavage solutions (e.g., poly-ethylene glycols) have not been shown to be effective incats with this condition and require administration of
Small Animal/Exotics 20TH ANNIVERSARY Compendium August 1999
F E C A L B U L K s C O M M E R C I A L D I E T S s L A X A T I V E S
There have been many advances
in our understanding and
treatment of feline colonic
diseases. Specific examples
include the recognition of
clostridial enterocolitis and
giardiasis as important causes of
infectious diarrhea in cats,increased understanding of and
interest in the importance of
diet in the management and
prevention of gastrointestinal
(GI) disease, and the role of
cisapride in the management of
feline idiopathic megacolon. We
are also gradually beginning to
understand the important
differences in the feline GI tract
(e.g., cats have a sizable entericflora that may be important in
specific digestive processes or
development of inflammatory
bowel disease [IBD]). Although
there have been many advances
in our knowledge of the feline
large intestine, there is still
much we need to learn about its
function as well as the
development of diets that
prevent or reduce the incidence
of diet-associated colonic disease,
improved methods of diagnosing
and managing idiopathic
megacolon, and the
pathophysiology of colonic IBD.
A LookBack
COMP
ENDIUMS
20thANNIVERSARY
19 7
9 - 19 9 9
-
8/14/2019 Feline Colonic Disorders
13/14
large volumes, which is not practical for cats on a regu-lar basis. If a cats colon is impacted with hard, dry fe-ces, administering warm-water enemas or mechanicallyremoving fecal material is necessary before initiatingcisapride therapy. When megacolon has been present
for more than 6 months or pharmacologic and dietarytherapy is no longer effective, the best approach is sur-gical palliation via a subtotal colectomy with or with-out pelvic osteotomy.45,46 Following colectomy, cats willhave soft to liquid stools for several months but willeventually produce soft to semi-formed feces withproper management, including a low-residue diet;small, frequent feedings; and time to adapt.
REFERENCES1. Kararli TT: Comparison of the gastrointestinal anatomy,
physiology and biochemistry of humans and commonly usedlaboratory animals. Biophar Drug Disp16:351380, 1995.
2. Bergman EN: Production and utilization of metabolites bythe alimentary tract as measured in portal and hepatic blood,in McDonald IM, Warner ACI (eds): Digestion andMetabolism in the Ruminant. Australia, University of NewEngland, 1975, pp 292305.
3. Bugaut M, Bentejac M: Biological effects of short chain fattyacids in nonruminant mammals.Ann Rev Nutr13:217241,1993.
4. Remesy C, Demigne D, Morand C: Metabolism and utiliza-tion of short chain fatty acids produced by colonic fermenta-tion, in Schweizer TF, Edwards CA (eds): Dietary Fiber: AComponent of Food. London, UK, Springer-Verlag, 1992, pp137150.
5. Newmark HL, Lupton JR: Determinants and consequencesof colonic luminal pH: Implications for colon cancer. NutrCanc14:161173, 1990.
6. Roediger WEW: Utilization of nutrients by isolated epithe-lial cells of the rat colon. Gastroenterology83:424429, 1982.
7. Drackley JK, Beaulieu AD, Sunvold GD: Energetic sub-strates for intestinal cells, in Reinhart GA, Carey DP (eds):Recent Advances in Canine and Feline Nutrition, vol II.
Wilmingham, DE, Orange Frazier Press, 1998, pp 463473.8. Roediger WEW: The starved colonDiminished absorp-
tion and colitis. Dis Col Rec33:858862, 1990.9. Sunvold GD, Fahey GC Jr, Merchen NR, et al: Dietary
fiber for cats: In vitro fermentation of selected fiber sourcesby cat fecal inoculum and in vivoutilization of diets contain-ing selected fiber sources and their blends. J Anim Sci73:23292339, 1995.
10. Fleming SE: Influence of dietary fiber on the production,absorption or excretion of short chain fatty acids in humans,in Spiller GA (ed): Dietary Fiber in Human Nutrition. BocaRaton, FL, CRC Press, 1993, pp 387412.
11. Maskell IE, Bauer JE: Role of dietary fiber in gastrointestinalfunction. Proc 17th Waltham/OSU Symp:6372, 1994.
12. Roberfroid MB: Health benefits of non-digestible oligosac-charides.Adv Exp Med Biol427:211219, 1997.
13. Tashiro Y, Satchithanadam S, Calvert RJ: Gastrointestinaleffects of fructooligosaccharides, in Kritchevsky D, BonfieldC (eds): Dietary Fiber in Health and Disease. New York,Plenum Press, 1997, pp 221234.
14. Oli MW, Petschow BW, Buddington RK: Evaluation offructooligosaccharide supplementation for oral electrolytesolutions for treatment of diarrhea. Recovery of intestinalbacteria. Dig Dis Sci43:138147, 1998.
15. Sunvold GD, Fahey GC Jr, Merchen NR, et al: In vitrofer-mentation of selected fibrous substrates by dog and cat fecal
inoculum: Influence of diet composition on substrate organ-ic matter disappearance and short chain fatty acid produc-tion.J Anim Sci73:11101122, 1995.
16. Willard MD, Simpson RB, Delles EK, et al: Effects of di-etary supplementation of fructooligosaccharides on small in-testinal bacterial overgrowth in dogs. Am J Vet Res55:654659, 1994.
17. Sparkes AH, Papasouliotis K, Sunvold G, et al: Bacterial flo-ra in the duodenum of healthy cats, and effect of dietarysupplementation with fructo-oligosaccharides.Am J Vet Res59:431435, 1998.
18. Sparkes AH, Papasouliotis K, Sunvold G, et al: Effect of di-etary supplementation with fructo-oligosaccharides on fecalflora of healthy cats.Am J Vet Res59:436440, 1998.
19. Guilford WG: Adverse reaction to foods: A gastrointestinalperspective. Compend Contin Educ Pract Vet16(8):957968,1994.
20. Roudebush P: Adverse reactions to foods: A clinical nutri-tionists perspective. Proc AAVD/ACVD:6975, 1998.
21. Reedy LM: Food hypersensitivity to lamb in a cat.JAVMA204:10391040, 1994.
22. Mueller RS, Tsohalis J: Evaluation of serum allergen specificIgE for the diagnosis of food adverse reactions in the dog.Proc AAVD/ACVD14:9394, 1998.
23. Brown CM, Armstrong PJ, Globus H: Nutritional manage-ment of food allergy in dogs and cats. Compend Contin EducPract Vet17(5):637659, 1995.
24. Jeffers JG, Shanley KJ, Meyer EK: Diagnostic testing of dogs
for food hypersensitivity.JAVMA198:245250, 1991.25. Marks SL, Melli A, Kass PH, et al: Evaluation of methods to
diagnose Clostridium perfringensassociated diarrhea in dogs.JAVMA214:357360, 1999.
26. Leib MS, Matz ME: Diseases of the large intestine, in Et-tinger S, Felman E (eds): Textbook of Veterinary InternalMedicine, ed 4. Philadelphia, WB Saunders Co, 1995, pp12321260.
27. Fox JG, Greene CE: Enteric bacterial infections, in GreeneCE (ed): Infectious Diseases of the Dog and Cat, ed 2.Philadelphia, WB Saunders Co, 1998, pp 226243.
28. Scherk M: IBD: A misleading misnomer (inflammatory di-gestive tract syndrome). Proc ACVIM16:537539, 1998.
29. Lecoindre P, Chevallier M: Contribution to the study of fe-
line inflammatory bowel disease51 cases (19911994).Reveie de Medecine Veterinarire148:893902, 1997.
30. Jergens AE: Feline idiopathic inflammatory bowel disease.Compend Contin Educ Pract Vet14(4):509520, 1992.
31. Dennis JS, Kruger KM, Mullaney TP: Lymphocytic-plasma-cytic colitis in cats: 14 cases (19851990). JAVMA 202:313317, 1993.
32. Willard MD: Gastrointestinal drugs. Vet Clin North Am28:377394, 1998.
33. Dimski DS: Therapy of inflammatory bowel disease, inBongura JD (ed): Kirks Current Veterinary Therapy XII.Philadelphia, WB Saunders Co, 1995, pp 723728.
34. Hickman MA: Interventional nutrition for gastrointestinal
Compendium August 1999 20TH ANNIVERSARY Small Animal/Exotics
-
8/14/2019 Feline Colonic Disorders
14/14
Small Animal/Exotics 20TH ANNIVERSARY Compendium August 1999
Nutrition. Boca Raton, FL, CRC Press, 1993, pp 567593.43. Gaginella TS, Macolo N, Izzo M, et al: Nitric oxide as a me-
diator of bisacodyl and phenolphthalein laxative action: In-duction of nitric oxide synthase. J Pharmacol Exp Ther270:12391244, 1994.
44. Washabau RJ, Sammarco J: Effects of cisapride on felinecolonic smooth muscle function. Am J Vet Res57:541546,1996.
45. Sweet DC, Hardie EM, Stone EA: Preservation versus exci-sion of the ileocolic junction during colectomy for mega-colon: A study of 22 cats. J Small Anim Prac35:358363,1994.
46. Schrader SC: Pelvic osteotomy as a treatment for obstipationin cats with acquired stenosis of the pelvic canal: 6 cases(19781989).JAVMA200:208213, 1992.
About the AuthorDr. Zoran is affiliated with the Department of Small Animal
Medicine and Surgery, College of Veterinary Medicine,
Texas A&M University, College Station, Texas, and is aDiplomate of the American College of Veterinary Internal
Medicine.
disease. Clin Tech Small Anim Pract13:211216, 1998.35. Rombeau JL: Therapeutic effects of short chain fatty acids in
human conditions of inflammation. Proc ACVIM:542546,1994.
36. Straw RC: Tumors of the intestinal tract, in Withrow SJ,MacEwen EG (eds): Small Animal Clinical Oncology, ed 2.Philadelphia, WB Saunders Co, 1996, pp 252261.
37. Ogilvie GK, Moore AS: Gastrointestinal tumors, in OgilvieGK, Moore AS (eds): Managing the Veterinary Cancer Pa-tient, Trenton, Veterinary Learning Systems, 1995, pp355359.
38. Cribb AE: Feline gastrointestinal adenocarcinoma: A reviewand retrospective study. Can Vet J29:709712, 1988.
39. Slawienski MJ, Mauldin CE, Mauldin GN, et al: Malignantcolonic neoplasia in cats46 cases (19901996). JAVMA211:878881, 1997.
40. Mooney S, Hayes A, MacEwen E: Treatment and prognosticfactors in lymphoma in cats: 103 cases (19771981).JAVMA194:696699, 1989.
41. Washabau RJ, Hasler AH: Constipation, obstipation, andmegacolon, in August JR (ed): Consultations in Feline Inter-
nal Medicine. Philadelphia, WB Saunders Co, 1996, pp104112.
42. Schakel SF, Sievert YA, Buzzard IM: Dietary fiber values forcommon foods, in Spiller GA (ed): Dietary Fiber in Human