Off-pump versus on-pump coronary artery bypass grafting for ischemic heart disease

A PROSPECTIVE RANDOMIZED TRIAL TO DETERMINE THE EFFECTS OF STEROID ON THE
fc INCIDENCE OF POSTOPERATIVE ATRIAL FIBRILLATION AFTER CORONARY ARTERY
BYPASS GRAFTING SURGERY (CABG)
B Y KRIENGCHAIPRASONGSUKARN, MD
M.D., Mahidol University, Thailand, 1992
A THESIS SUBMITTED IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE
OF MASTER OF SCIENCE IN
THE FACULTY OF GRADUATE STUDIES DEPARTMENT OF SURGERY
We acceptftfiis thesis a$ conforming to the required standard
UNIVERSITY OF BRITISH COLUMBIA VANCOUVER, BRITISH COLUMBIA
DECEMBER 2001
© Kriengchai Prasongsukarn, 2001
I
ABSTRACT
Background
Atrial fibrillation remains one of the most common postoperative
complications of coronary artery bypass grafting (CABG). Because of the
additional hospital costs associated with this arrhythmia, owing to increased use of
antiarrhythmic medications, diagnostic studies, and prolonged hospitalization, this
subject continues to draw the interest of cardiac surgeons and cardiologists. Despite
many clinical studies, there is still no consensus regarding the best prevention
strategy for this arrhythmia. There are several mechanisms that explain why atrial
fibrillation occurs after C A B G , still the pathophysiological mechanism remains
unclear, and therefore mutifactorial causes are likely. One of the mechanisms that
we believe is inflammation around the sac of the heart and surgical trauma,
including the generalized inflammation response induced by the heart-lung
machine. As we know, steroid can decrease the body's response to trauma and
inflammation and may reduce the chance of atrial fibrillation occurring. For this
reason we design the study to assess the short-term effect of steroid on the
incidence of postoperative atrial fibrillation after C A B G .
Methods This study was done during the time from August 2000 to February
2001 .Eighty-eight consecutive consenting patients were prospectively entered into
a randomized, double blind, placebo-controlled trial to determine the efficacy of
steroid on the incidence of atrial fibrillation after elective coronary artery bypass
grafting. No patient had documented or suspected arrhythmias preoperatively. Two
patients were excluded from the study due to Off-PumpCABG, forty-three patients
11

received 1 gm of methyprednisolone before surgery and 4 mg of dexamethasone
every 6 hours for one day after surgery, and forty-three patients received only
placebo.
Results Postoperative atrial fibrillation occurred in 9 of the 43 patients in the steroid
group (21 percent) and 22 of the 43 patients in the placebo group (51 percent)
(p=0.003). Minor postoperative complications occurred in 15 steroid patients (34
percent) and in 6 patients receiving placebo (14 percent). Major complications
occurred in 4 patients who received steroid (9 percent) and in 2 who received
placebo (5 percent) (p=0.052) Patients with atrial fibrillation were hospitalized for
significantly longer days than were patients with normal sinus rhythm (median
8Vs.6 days, p=0.002); however, the length of hospital stay in Steroid group was 6
days compare with 7 days in Placebo group (p=0.337).
Conclusions
The use of prophylactic Short-Term Steroid Administration in patients
undergoing coronary bypass grafting surgery reduced the incidence of
postoperative atrial fibrillation by approximately 50 percent. Patients without
postoperative atrial fibrillation had a shorter length of hospital stay. Overall,
there was no significant difference between Steroid Group and Placebo Group
with regard to the length of hospital stay. In this study, we found that Steroid
had higher complications which may contribute to prolonged hospitalization.
• * «
111
Table of contents
Abstract \L
Table of Contents l v . List of Tables ^ List of Figures Vlll Acknowledgements X
Chapter 1. INTRODUCTION Overview 1
Epidemiology 1
Pathophysiology 6
Potential Preoperative Markers for the Risk of developing.Atrial
Fibrillation after CABG 19
Sequelae 29 Prophylaxis 34
Chapter 2. OBJECTIVE OF THE THESIS 39
Possible mechanism of inflammatory response of cardiopulmonary
bypass 40
Steroid and inflammatory response process 42
Research plan 44
Study hypothesis 44
Primary outcome 45
Secondary outcome 45
Benefit 45
Study design 46

Material and Methods
Sample size
Patient Selection
Steroid administration
Operative technique
Hemodynamic Measurement and Monitor
Statistics
Breaking the code-Interim analysis
Estimated duration of study
Data base form
Result
Postoperative atrial fibrillation
Complication
Length of Hospital stay
Risk Factors of Postoperative AF
Discussion
References

List of Tables
Table 1. Risk Factors by Univariate Logistic Regression Analysis. 23
Table 2. Independent Risk Factors for the Development of Postoperative
Atrial Arrhythmias. 24
Table 3. Patient Characteristics. 58
Table 4. Number of Atrial Fibrillation patients of two groups. 59
Table 5. Number of Episode of Atrial Fibrillation of two groups. 59
Table 6. Number of sex of Patients of two groups. 61
Table 7. Number of Congestive Heart Failure Patients of two groups. 61
Table 8. Number of Myocardial Infarction Patients of two groups. 62
Table 9. Number of Chronic Obstructive Lung Disease Patients of two
groups. 62
Table 10. Number of Asthma Patients of two groups. 63
Table 11. Number of Smoking Patients of two groups. 63
Table 12. Number of Chronic Renal Failure Patients of two groups. 64
Table 13. Number of Hypertension Patients of two groups. 64
Table 14. Number of A-Pacing Patients of two groups. 65
Table 15. Number of AV-Pacing Patients of two groups. 65
Table 16. Number of Bypass Grafts in Patients of two groups. 66
Table 17. Left Ventricular Ejection Fraction of Patients in Each Group
in Detail. 66
Table 18. Patients Characteristics in Age, Cross clamp time, and Bypass
time. 67
Table 19. Complications in Each Group in Detail. 69

Table 20. Number of Complication Patients in Detail. 70
Table 21. Number of White Blood Cell Count at 12-hour postoperative
period of two groups. 71
Table 22. Number of White Blood Cell count at 24-hour postoperative
period of two groups. 72
Table 23. Length of Hospital stay compare between normal sinus rhythm
and atrial fibrillation patient. 73
Table 24. Length of hospital stay compare between steroid group and
placebo group. 75
Table 25. Risk factors by multivariate logistic regression analysis 77
Table 26. Univariate analysis in myocardial infarction between NSR and
AF patient. 78
Table 27. Univariate analysis in congestive heart failure between NSR and
AF patient. 78
Table 28. Univariate analysis in A-pacing between NSR and AF patient. 79
Table 29. Univariate analysis in AV-pacing between NSR and AF patient. 79
Table 30. Univariate analysis in chronic obstructive lung disease between
NSR and AF patient. 80
Table 31. Univariate analysis in age, cross-clamp time, and bypass-time
between NSR and AF patient. 80
vii

List of Figures
Figure 1. Time of occurrence of atrial fibrillation after coronary artery
bypass grafting. 4
Figure 2. Atria showing a composite map of the distribution of effective
refractory periods (ERPs) in 14 dogs before cardiopulmonary
bypass. 10
Figure 3. (A) Distribution of the preoperative ERPs in a dog. 12
Figure 3. (B) Distribution of the postoperative ERPs in the same dog. 12
Figure 4. Simultaneous measurement of the temperatures of the atrial septum
and the ventricular septum during the first 10 minutes of cardioplegic
arrest in a C A B G patient. 14
Figure 5. Univariate logistic regression analysis in age and incidence of
postoperative atrial arrhythmia. 21
Figure 6. Univariate logistic regression analysis in aortic cross-clamp time
and incidence of postoperative atrial arrhythmia. 22
Figure 7. (A) ICU and nursing ward hospitalization compare between NSR
and atrial arrhythmia patients. 31
Figure 7. (B) Number of ventricular arrhythmia patients, permanent pacemaker
implantation, and postoperative stroke compare between NSR and
atrial arrhythmia patients. 32
Figure 8. Relationship between duration of hospitalization and development of
postoperative atrial fibrillation. 33
Figure 9. Incidence of postoperative atrial fibrillation compare between steroid
- and placebo group. 60
Vill

Figure 10. Percentages of major and minor complication in steroid and
placebo group.
Figure 11. Mean score length of hospital stay compare between NSR and AF
patient.
Figure 12. Mean score length of hospital stay compare between steroid and
placebo group.

ACKNOWLEDGEMENTS
I dedicate this thesis to my mother and father, Porntip and Prasong
Prasongsukarn, who have always encouraged me to strive, and to Taddao and
Amie Prasongsukarn, who understand and had the patience to see this journey
through with me. I 'm much obliged to Anandamahidol Foundation who
sponsors me to pursue my study in Cardiac Surgery in Canada.
I am grateful to Samuel V. Lichtenstein MD.PhD.FRCSC, James G. Abel
MD.MSc.FRCSC who educated me in the science and art of the profession and
taught me the operations, including giving their constant guidance and
support. In particular, special thanks to my Supervisory committee James A.
Russell MD.FRCPC, Keith R.Walley MD.FRCPC, Stanley K K . Tung
MD.FRCPC, who have provided much encouragement, support and
constructive criticism as my experiments and my thesis took shape.
I would like to thank the ICU research nurse (Carol), Kanya R N for
helping me collect the data. Finally, I would like to thank Min, Lilian for her
expertise in the statistical analysis, and to Donny for his help in the computer
program.
X
CHAPTER 1 Introduction
Overview
Few problems are more common or recalcitrant than atrial fibrillation
after cardiac surgery. This postoperative complication is the major reason for
hospital stays that exceed 4 days after coronary artery bypass surgery. Partly
because of its frequency, and therefore its familiarity, postoperative atrial
fibrillation is commonly considered to be more nuisance than a potentially
serious complication. Nowadays the increased mean age of patients
undergoing open-heart surgery is expected to result in an increase incidence
of postoperative atrial fibrillation and greater costs for the management of
these patients.
Epidemiology
Supraventricular arrhythmias are common after all major surgical
procedures, including thoracic and abdominal surgical procedures. The
incidence of atrial fibrillation and atrial flutter was reported by Favaloro et al.
to be 12 % in the first 100 patients undergoing C A B G at the Cleveland clinic
from 1967 to 1968(1). The incidence of supraventricular arrhythmias was
reported to be 4% by Goldman in a large registry of patients undergoing
major noncardiac surgery (2). A multicenter study of patients undergoing
1

abdominal aortic aneurysm repair reported an incidence of supraventricular
arrhythmias of 3.2%, and in a prospective study of 295 patients undergoing
thoracotomy for lung cancer, the incidence of supraventricular arrhythmias
was almost 13% (3,4). Data published during the past decade show an
incidence of atrial fibrillation after C A B G that varies considerably between
studies, ranging from 5% to 40% (5). A recent preliminary report from the
Cleveland Clinic cited an incidence of postoperative atrial fibrillation of 19%
in 42 patients undergoing minimally invasive cardiac surgery, which was
similar to the incidence of atrial fibrillation for patients undergoing C A B G
using standard techniques (6). Two recent prospective multicenter studies of
C A B G from the 1990s reported an incidence of postoperative atrial
fibrillation between 27% and 33% (7,8). The incidence of atrial fibrillation is
higher in patients undergoing valve replacement with or without C A B G ,
occurring in 30% to 70% of patients.
The incidence of postoperative atrial fibrillation has varied markedly
between trials owing mostly to the intensity and duration of postoperative
monitoring. A meta-analysis by Andrews et al (9) reported a 27% incidence
of postoperative atrial fibrillation in the control group. However, atrial
fibrillation was documented in 41% of patients using continuous
electrocardiographic (Holter) monitoring compared with only 20% in patients
using other forms of electrocardiographic monitoring. Mathew et al(10) also
reported an incidence of 27% in a multicenter trial involving 2,265 patients
undergoing elective coronary artery bypass graft surgery. Creswell et al
reviewed 6 years of data and reported an incidence of 32% in 2,833 patients
2
undergoing coronary artery bypass surgery (11). Of note, this incidence was
60% in patients undergoing coronary plus aortic valve surgery and 64% in
patients having combined coronary and mitral valve surgery.
We looked at the incidence of atrial fibrillation postoperative C A B G in
our province. The data from B.C. Cardiac registry from 1993 to 1998 showed
the incidence of atrial fibrillation after Coronary artery bypass surgery at
St.Paul's hospital was 43.5%.
Atrial fibrillation may occur at any time after C A B G , but generally
occurs 2-4 days after open-heart surgery (7,8). The episodes generally tend to
be transient, short-lived, frequent, and recurrent. Atrial fibrillation occurs less
commonly immediately (less than 24 hours) or late (greater than 5 days) after
bypass surgery with a time course approximating a bell-shaped curve and the
peak occurring 2-4 days after surgery (Fig 1). Episodes may recur or persist
for weeks before finally resolving spontaneously. Up to 10% to 15% of
patients with post-CABG atrial fibrillation are discharged from the hospital
with atrial fibrillation. It is rare for chronic atrial fibrillation to develop after
C A B G .
3

30
0 1 2 3 4 5 6 6+ Post Op Day
Figure 1
Time of occurrence of atrial fibrillation after coronary artery bypass grafting.
(From Aranki SF, Shaw DP, Adams DH, et al: Predictors of atrial fibrillation
after coronary artery bypass surgery. Current trends and impact on hospital
resources. Circulation 94:390-397.1996)
Patients undergoing cardiac surgery may be categorized into 3 groups,
depending on their vulnerability to the development of postoperative atrial
fibrillation (12). The percentages quoted below are all approximate but are
based on those reported in the literature.
Groupl. Five percent of patients undergoing any type of surgery will develop
postoperative atrial fibrillation. These are patients who undergo peripheral
4

vascular surgery, abdominal surgery, orthopedic surgery, and so forth, and
develop postoperative atrial fibrillation. Clearly, these patients enter surgery
with an underlying propensity to develop postoperative atrial fibrillation
regardless of the type of surgery performed.
Group 2. Thirty-five percent of patients develop atrial fibrillation after
cardiac surgery if untreated, but atrial fibrillation can be controlled in all but
5% of patients by a variety of prophylactic measures. This irreducible level of
5% postoperative atrial fibrillation represents the patients in Group I. The
remaining patients, with a rate of around 30%, represent those patients in
Group 2 whose postoperative atrial fibrillation can be prevented by
appropriate prophylactic measures.
Group3. The remaining 65% of patients will not develop atrial fibrillation
after cardiac surgery no matter the complexity of the surgical procedure.
Clearly, these patients do not have the underlying vulnerability, whatever that
may be, that makes Group 1 patients invariably have postoperative atrial
fibrillation and that makes Group 2 patients have it unless prophylaxed
against it.
Because Group 1 patients invariably develop postoperative atrial
fibrillation and Group 3 patients never develop it, the only patients in whom
prophylactic measures are of any potential importance are those in Group 2,
ie, in only 30% of patients undergoing cardiac surgery. Furthermore, the best
result that such an intervention can attain is a rate of approximately 5%, ie,
the irreducible level of postoperative atrial fibrillation caused by the
intractability of the Group 1 patients.
5

Pathophysiology
Multiple mechanisms have been proposed to be responsible for the
pathogenesis of atrial fibrillation in the postoperative setting (13). These
mechanisms include acute atrial distension or inflammation from the trauma
of surgery; alteration in autonomic tone from surgery and the stress of the
postoperative period; ischemic injury to atria as a result of surgery and/or
inadequate protection during bypass; electrolyte and volume shifts during
bypass resulting in changes in repolarization; inflammation resulting from
pericarditis; and a variety of other electrophysiologic changes that may occur
as a result of the bypass procedure, the cardioplegia, or the surgery itself that
all may result in a lower atrial fibrillation threshold.
The pathophysiology of atrial fibrillation in the nonsurgical setting has
been intensively studied. One of the more widely held theories is the multiple
wavelet hypothesis advanced by Moe(14). This theory proposes that atrial
fibrillation is the result of multiple wavelets caused by reentry that move
through the atria constantly colliding or extinguishing themselves, and
reforming or combining with new wavelets. Mapping studies in animals and
humans have demonstrated these multiple wavelets, whose course is dictated
by atrial conduction, refractoriness, and excitability (15). The wavelets are
believed to be primarily functionally determined, and a predisposition to atrial
6

reentry is caused by a combination of several factors including heterogeneity
of conduction in the atria, large atrial size, alterations in electrical coupling in
the atrial myocardium, and fixed anatomical obstacles.
The mechanism of postoperative atrial fibrillation is less well defined.
Multiple mechanisms likely play a role. Several electrophysiologic changes
that may predispose to atrial fibrillation have been documented to occur in the
postoperative setting. For example, Chung and colleagues have performed a
series of studies before and after bypass showing suppressed sinus node
function after C A B G (16,17). These investigators have also demonstrated a
variety of changes in atrial refractoriness and conduction latency in patients
undergoing C A B G that may predispose them to have atrial fibrillation
develop (17,18). Sato et al. found prolongation of atrial conduction times
during the first 2 hours after bypass in the canine heart (19). Several groups
have used prolonged P wave duration measured directly from the surface
E C G or with signal averaging techniques as an index of intraatrial conduction
delay and shown that it correlated with an increased incidence of
postoperative atrial fibrillation (20,21). A practical limitation to relying on
these observations for screening patients preoperatively is the lack of
standardization of P-wave measurements and the absence of commercially
available P-wave signal averaging equipment.
There is one recent theory from Cox et al that explained the cause of
postoperative atrial fibrillation (12). In an effort to elucidate the cause of
postoperative atrial fibrillation, they performed a series of experiments in the
7

1980s(22-30) and 1990s(19) in which several assumptions were made. The
first assumption was that the underlying vulnerability to the development
of postoperative atrial fibrillation was a preexisting electrophysiological
abnormality. The second assumption was that the degree of derangement of
this electrophysiological abnormality was most severe in Group 1 patients,
less severe in Group 2 patients, and nonexistent in Group 3 patients. They
hypothesized that in Group 1 patients, the electrophysiological abnormality
was so severe that atrial fibrillation would occur after any type of surgery
including noncardiac surgery. They further hypothesized that the less severe
electrophysiological abnormality in Group 2 patients had to be activated by
some trigger associated with cardiac surgery per se before it would lead to
atrial fibrillation. This, they believed, would also explain why Group 2
patients develop postoperative atrial fibrillation if they are not prophylaxed
but do not develop it if appropriate prophylactic measures are taken. Finally,
this uniform theory of postoperative atrial fibrillation included the absence of
postoperative atrial fibrillation in Group 3 patients because they did not have
the underlying electrophysiological abnormality.
The experiments mentioned identified an underlying
electrophysiological abnormality that was consistent with their theory. That
abnormality related to the manner in which the atrial myocardium recovered
in different areas after the completion of electrical activation. The period of
time between electrical activation of the atrium and complete repolarization
of the atrium is called the refractory period. However, the atrial refractory
period is not a singular entity but rather it varies from one part of the atrium
8

to another. By performing a complex series of stimulation tests, the local
refractory periods for sites all over the atrium can be determined. There is
normally an orderly progression from the relatively short refractory periods of
the left atrium to the relatively long refractory periods of the right atrium.
This orderly progression can be plotted to determine the so-called dispersion
of refractoriness in the atria.
9

(Fig2)
110 120 130 140 150 160
Figure 2.Atria showing a composite map of the distribution of effective
refractory periods (ERPs) in 14 dogs before cardiopulmonary bypass. The
10

lower panel shows the posterior view of the atria. The upper panel represents
the anterior surface of the atria shown as if a sagittal section had been taken
through both atria and the anterior portion of the atria was flipped up to show
their surfaces. The area of shortest ERPs was in the posteroinferior left atrium
below the pulmonary veins. The area of longest ERPs was in the inferior
aspect of the posterior right atrium. ANT, anterior; POST, posterior; L A A ,
left atrial appendage; R A A , right atrial appendage; M , mitral valve; T,
tricuspid valve; SVC, superior vena cava; IVC, inferior vena cava; PV,
pulmonary veins, from Sato et al. The effect of augmented atrial hypothermia
on atrial refractory period, conduction, and atrial flutter/fibrillation in the
canine heart. JThorac Cardiovasc Surg 104: 297- 306, 1992.
Under normal circumstances, there are no areas in the atrium where short
and long refractory periods lie in close apposition. However, i f the dispersion
of refractoriness is nonuniform, it results in areas where atrial myocardiums
with a short refractory period lie adjacent to an area of atrium with a long
refractory period (Fig 3A). This would appear to be the major underlying
electrophysiological abnormality that causes the atria to be vulnerable to the
development of postoperative atrial fibrillation (Fig
11

3B).
Figure 3. (A) Distribution of the preoperative ERPs in a dog. There is
some similarity between this ERP distribution map and the composite shown
in Figure 2. However, the area immediately beneath the inferior pulmonary
veins shows several regions where relatively long refractory periods lie in
close proximity to regions of relatively short refractory periods. Despite these
findings, no arrhythmias could be induced by programmed electrical
stimulation in this dog preoperatively. (B) Distribution of the postoperative
ERPs in the same dog. Note the greater nonuniformity (heterogeneity) of
distribution of the ERPs after cardiopulmonary bypass in this animal. The
asterisks mark the sites where a single prematurely paced beat induced atrial
fibrillation in this animal postoperatively. The lower panel shows the
posterior view; the upper panel represents the anterior surface.
1 2

ANT, anterior; POST, posterior; L A A , left atrial appendage; R A A , right atrial
appendage; M , mitral valve; T, tricuspid valve; SVC, superior vena cava;
IVC, inferior vena cava; PV, pulmonary veins. (From Sato et al: The effect of
augmented atrial hypothermia on atrial refractory period, conduction ,and
atrial flutter/fibrillation in the canine heart; J Thorac cardiovasc Surg
104:297-306,1992)
Because of several clinical observations, they were strongly suspicious
that the trigger mechanism necessary to activate the underlying
electrophysiological mechanism was ischemia of the atrial myocardium
during the period of cardioplegic arrest. Although major efforts are expended
intraoperatively to maintain the temperature of the ventricular myocardium at
acceptable levels of hypothermia during the period of cardioplegic arrest,
little or no attention is usually paid to the level of hypothermia in the atrial
myocardium. Because the atrial myocardium is also susceptible to ischemic
injury, they decided to evaluate its degree of protection with cardioplegia,
suspecting that it would be dismal. Indeed, they found that after an infusion
of cardioplegia, the level of hypothermia attained in the atrial septum is
invariably less than that in the ventricular septum and that within 2 to 3
minutes after cessation of cardioplegia infusion, the temperature of the atrial
septum returns to the temperature of the systemic perfusion (Fig 4). Knowing
that such inadequate hypothermia in the ventricles would likely cause
ventricular failure (and perhaps ventricular fibrillation) postoperatively, it is
13

reasonable to assume that the incidence of atrial fibrillation would be
increased by such blatantly, inadequate protection of the myocardium during
the period of cardioplegic arrest. Once this observation was made, they felt
that the likely trigger for bringing out the underlying vulnerability to atrial
fibrillation in Group 2 patients was atrial myocardial ischemia (23).
14
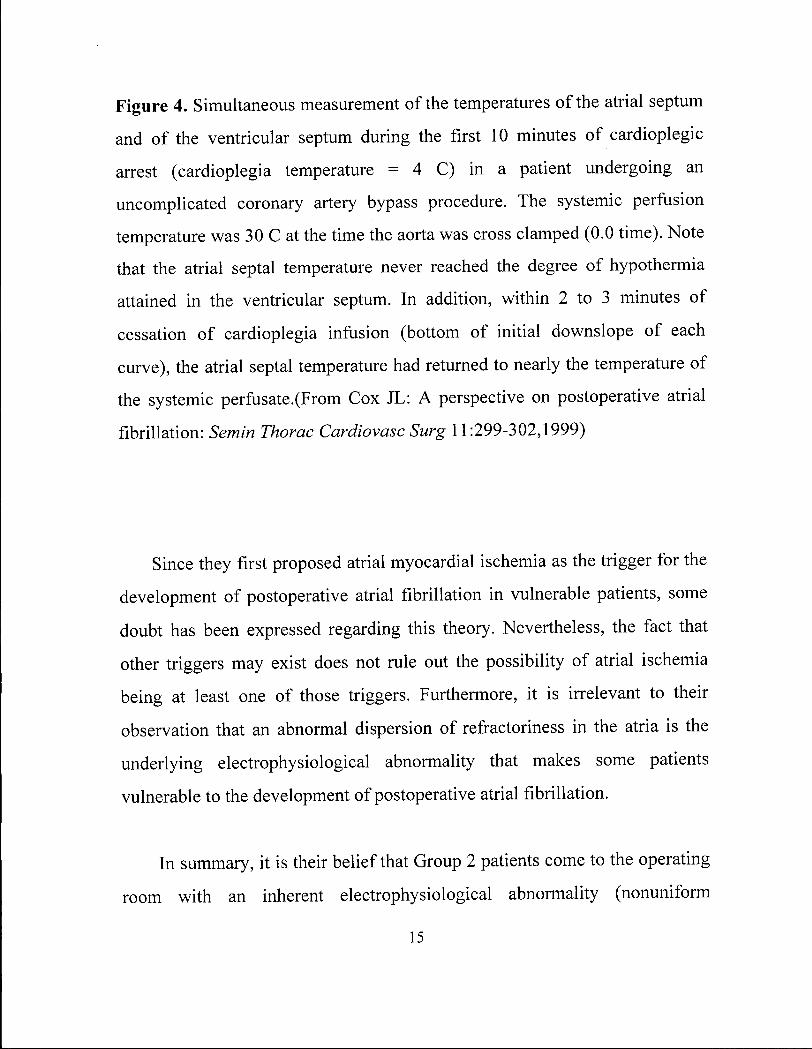
Figure 4. Simultaneous measurement of the temperatures of the atrial septum
and of the ventricular septum during the first 10 minutes of cardioplegic
arrest (cardioplegia temperature = 4 C) in a patient undergoing an
uncomplicated coronary artery bypass procedure. The systemic perfusion
temperature was 30 C at the time the aorta was cross clamped (0.0 time). Note
that the atrial septal temperature never reached the degree of hypothermia
attained in the ventricular septum. In addition, within 2 to 3 minutes of
cessation of cardioplegia infusion (bottom of initial downslope of each
curve), the atrial septal temperature had returned to nearly the temperature of
the systemic perfusate.(From Cox JL: A perspective on postoperative atrial
fibrillation: Semin Thorac Cardiovasc Surg 11:299-302,1999)
Since they first proposed atrial myocardial ischemia as the trigger for the
development of postoperative atrial fibrillation in vulnerable patients, some
doubt has been expressed regarding this theory. Nevertheless, the fact that
other triggers may exist does not rule out the possibility of atrial ischemia
being at least one of those triggers. Furthermore, it is irrelevant to their
observation that an abnormal dispersion of refractoriness in the atria is the
underlying electrophysiological abnormality that makes some patients
vulnerable to the development of postoperative atrial fibrillation.
In summary, it is their belief that Group 2 patients come to the operating
room with an inherent electrophysiological abnormality (nonuniform
15

dispersion of refractoriness) that makes them vulnerable to the development
of postoperative atrial fibrillation. Because the abnormality is of intermediate
severity, some trigger mechanism (perhaps atrial ischemia) is necessary to
activate that vulnerability, resulting in postoperative atrial fibrillation. In the
absence of such a trigger, or i f the trigger is suppressed or overcome
prophylactically, postoperative atrial fibrillation will not develop in these
patients. Because Group 1 patients will always develop atrial fibrillation and
Group 3 patients will never develop it, the Group 2 patients are the only ones
with which we should concern ourselves as cardiac surgeons.
Despite what would appear to be a reasonably clear picture of the
underlying electrophysiological abnormality that makes some patients more
vulnerable than others to the development of postoperative atrial fibrillation,
many limitations in their knowledge remain. For example, essentially all of
the electrophysiological observations described earlier were made in animal
experiments and, therefore, may have limited applicability in humans. The
reason that refractory period distribution maps such as those shown in Figures
2 and 3 have not been performed in humans is that the process is an extremely
laborious one requiring several minutes of programmed electrical stimulation
and recording at each electrode site on the atria. In the case of the animal data
shown in Figures 2 and 3, there were approximately 250 electrodes on the
atrial surfaces and the entire process took several hours. This is obviously not
feasible in humans. Therefore, even if the theory is correct, there is no way of
identifying those patients before surgery who are vulnerable to the
development of postoperative atrial fibrillation.
16

Again, assuming that their theory regarding the vulnerability of atrial
fibrillation is true, other questions remain regarding why the abnormal
dispersion of refractoriness is present in some patients and not in others. For
example, is it congenital or acquired? The increasing incidence of
postoperative atrial fibrillation with increasing patient age suggests that the
problem is acquired. Is it owing to a defective gene, a chemical imbalance in
the atrial myocardium, an abnormality in the autonomic input to the heart, an
anatomic substrate such as fibrosis, hypertrophy, or stretch of the atrium, or a
maldistribution of atrial receptor sites? Until this question is answered com
pletely, the problem of postoperative atrial fibrillation is likely to persist. In
the meantime, we can only attempt to prevent postoperative atrial fibrillation
in the 30% of patients who are vulnerable to developing it and in whom it is
preventable. Decreasing the incidence of postoperative atrial fibrillation after
cardiac surgery to 5% is a worthy and attainable goal.
Another mechanism that explained the cause of atrial fibrillation in
patients undergoing C A B G is a significant increase in epinephrine and
norepinephrine levels measuring for up to 3 days in the postoperative period
(31,32). This hyperadrenergic state may contribute to increased automaticity
and increased frequency of premature atrial contractions, serving as a
"trigger" for episodes of atrial fibrillation. Postoperative withdrawal of beta-
adrenergic blockers has also been postulated as a predisposing cause.
However, investigators have not been able to demonstrate any direct
17

correlation between the elevation of catecholamines and the development of
atrial fibrillation in patients.
The time course of the development of atrial fibrillation parallels the
development of postoperative pericarditis, which through acute inflammation
may alter atrial coupling and lead to transient structural or electrophysiologic
changes that predispose patients to atrial fibrillation. It has been difficult to
study the relationship between pericarditis and atrial fibrillation because the
diagnosis of atrial pericarditis is dependent on relatively nonspecific clinical
and E C G findings. The ability of pericarditis to induce atrial flutter and atrial
fibrillation is clear from animal models. The sterile pericarditis model in dogs
is a well-established animal model of atrial flutter that, as the name suggests,
relies on pericardial inflammation from pericardiectomy and pericardial
irritation to induce atrial flutter (33). The high incidence of pericardial
effusions (up to 85% in some studies), as well as the time course of
pericarditis in animal models and humans, suggests that further investigation
into the role of pericardial inflammation contributing to postoperative atrial
fibrillation is necessary (34,35).
18

Potential Preoperative Markers for the Risk of developing
Atrial Fibrillation after CABG
There were several studies shown the risk factors associated with
postoperative atrial fibrillation. One study from Creswell et al, reviewed their
experience at the Barnes Hospital from January 1,1996 through December
31,1999(36). During that period, a total of 4,507 adult patients underwent
cardiac surgeries that required the use of cardiopulmonary bypass. A
univariate logistic regression analysis was performed to identify risk factors
that were associated with the development of postoperative atrial arrhythmias
(table 1). Independent risk factors for the development of postoperative atrial
arrhythmias were analyzed in table 2. These risk factors were reduced to a
relatively small set: increasing patient age, preoperative use of digoxin,
history of rheumatic heart disease, history of chronic obstructive pulmonary
disease, and increasing aortic cross-clamp time. In addition, some studies
show a history of congestive heart failure and a history of preoperative atrial
fibrillation increase the risk of developing postoperative atrial fibrillation
(41,43,44).
Increasing patient age has consistently been the most commonly
identified risk factor for the development of postoperative atrial arrhythmias
and their experience confirms the finding of other investigators (37-42). To
show the effect of increasing patient age on the development of postoperative
atrial arrhythmias, they used the univariate regression coefficient and
19
intercept to create a graph that might be useful for predicting the risk for an
individual patient (figure 5). This curve is sigmoidal, with a low incidence of
postoperative atrial arrhythmias for patients younger than 40 years of age and
a steep increase in the incidence in patients between 45 and 85 years of age.
(Only 3.7% in patients younger than 40 years compared with 28 % of patients
70 years) A similar graph was constructed to show the effect of increasing
aortic cross-clamp time of the incidence of these arrhythmias (Figure 6). This
curve is nearly linear, with a small increase in incidence for increasing aortic
cross-clamp times. Although this effect is statistically significant, the effect is
small and the increase in the incidence of these arrhythmias caused by
increasing patient age is obviously much greater.
20

100 - i
Figure 5. The slope and intercepts from a univariate logistic regression model
were used to construct a graph of the predicted incidence of postoperative
atrial arrhythmias according to patient age. (From Creswell L L : Hazards of
postoperative atrial arrhythmias. The Annals of Thoracic Surgery 1993,
vol.56, 539-549,1993).
21

100 —i
Figure 6. The slope and intercepts from univariate logistic regression model
were used to construct a graph of the predicted incidence of postoperative
atrial arrhythmias according to the period of aortic cross clamping. (From
Creswell L L : Hazards of postoperative atrial fibrillation: The Annals of
Thoracic Surgery 1993, vol. 56, 539-549,1993).
22
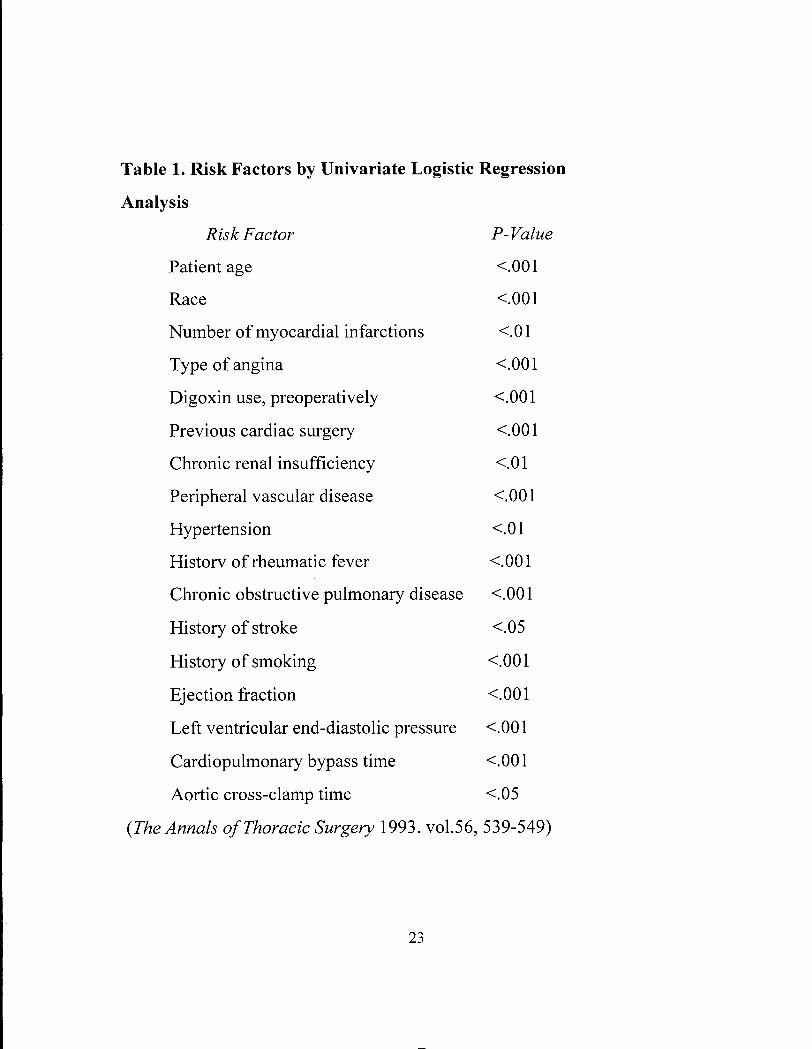
Table 1. Risk Factors by Univariate Logistic Regression
Analysis
R isk Factor P- Value
Patient age <.001
Race <.00l
Number of myocardial infarctions <.01
Type of angina <.001
Digoxin use, preoperatively <.001
Previous cardiac surgery <.001
Chronic renal insufficiency <.01
Peripheral vascular disease <.001
Hypertension <.0l
Historv of rheumatic fever <.001
Chronic obstructive pulmonary disease <.001
History of stroke <.05
History of smoking <.001
Ejection fraction <.001
Left ventricular end-diastolic pressure <.001
Cardiopulmonary bypass time <.001
Aortic cross-clamp time <.05
{The Annals of Thoracic Surgery 1993. vol.56, 539-549)
23

Table 2. Independent Risk Factors for the Development of Postoperative
Atrial Arrhythmias
• Increasing patient age
• Preoperative use of digoxin
• History of rheumatic heart disease
• Chronic obstructive pulmonary disease
• Increasing aortic cross-clamp (ischemic) time
From Creswell LL:Postoperative atrial arrhythmias: Risk factors and
associated adverse outcomes: Semin Thorac Cardiovasc Surg 11:303-
307,1999
Insight into the role of atrial preservation or atrial ischemia may be
gained by searching for a relationship between the various aspects of surgical
technique and their relationship to the incidence of atrial fibrillation (45). One
hypothesis proposes that atrial ischemia secondary to inadequate protection of
atrial myocardium, or prolonged aortic cross clamp time may predispose
patients to the development of postoperative atrial fibrillation. Several studies
have shown an increased incidence of atrial fibrillation with increased cross-
clamp or total pump time, but other studies have found no relationship (8,45).
Other factors that may influence the incidence of atrial fibrillation are the
type and volume of cardioplegia used to afford myocardial protection and the
method of cannulation. Several small studies have examined the incidence of
24
atrial fibrillation with cold cardioplegia, crystalloid cardioplegia, blood
cardioplegia, intermittent aortic cross-clamping time, and diltiazem
containing cardioplegia(46-48). No consistent or only small differences in the
incidence of atrial fibrillation with different types of cardioplegia were
discovered in these studies.
Considerable work is ongoing to further study the electrophysiologic
effects of different methods of providing cardioplegia to the heart. The
method of cardiac cannulation for delivery of cardioplegia will also affect
atrial preservation. No clear-cut advantage has been demonstrated for single
vs. bicaval cannulation on the incidence of atrial fibrillation (8,49).
Other surgical variables that have been associated with a higher
incidence of atrial fibrillation include bypass grafting to the right coronary
artery, concomitant right coronary artery endarterectomy, use of the internal
mammary artery graft, pulmonary vein venting, and postoperative atrial
pacing (7,8,44). In a preliminary report from a large multicenter study,
frequent preoperative premature atrial contractions (PACs) were a risk factor
for post-CABG atrial fibrillation (50). The major limitation to most of these
studies is the small sample size or failure to determine whether the surgical
variable is independent of poor left ventricular function and age. These issues
will only be clarified by analyzing the results of large, prospective
multicenter registries comparing different surgical techniques in patients at
high risk for having postoperative atrial fibrillation develop.
25

The role of preoperative digoxin in changing the incidence of atrial
fibrillation has been reviewed in several large series. In one large recent
report of 2,833 patients undergoing C A B G , the incidence of postoperative
atrial fibrillation was 32% in patients not taking digoxin preoperatively and
44% in patients taking preoperative digoxin (P< 0.001)(39). In another study,
preoperative use of digoxin was a univariate but not a multivariate predictor
of the development of atrial fibrillation. The major limitation of these
analyses is that the reason for preoperative digoxin use is often unclear. It is
possible that most of these patients were taking digoxin because of a history
of previous atrial fibrillation, which is also a risk factor for postoperative
atrial fibrillation.
Because histopathological examination of cardiac myocardium can
identify degrees of cellular injury less severe than frank necrosis, A d et al felt
that postoperative atrial fibrillation might be predictable on the basis of
preoperative histological abnormalities in the atrial myocardium. In the
ventricular myocardium, changes such as muscle fiber atrophy, myolysis
(sarcomere loss), fiber disarray, cellular and/or interstitial edema, and
perinuclear intracellular vacuolation can be identified when the ventricle is
exposed to toxic and/or ischemic insults(51-56). Unfortunately, much less is
known about morphological correlates of mild damage in the atrial
myocardium. Therefore they designed the study to identify the
histopathophysiological changes in atrial cardiomyocytes that might predict
the development of atrial fibrillation during the postoperative period. Atrial
26

tissue from 60 patients was sampled before and after cardiopulmonary bypass.
Fifteen patients(25%) developed postoperative atrial fibrillation.
Histologically, there were 3 findings in the atrial myocardium that were more
common in patients who developed postoperative atrial fibrillation:(l)
vacuolation size (p=.017), (2) vacuolation frequency (p=.0136), and (3)
lipofuscin content (p=.013)(57). In this study, they hypothesized that
susceptibility to the development of postoperative atrial fibrillation might
derive from preexisting metabolic deficits in the atrium and, therefore,
examined the atrial myocardium for such changes. Their working hypothesis
was that it might be possible to detect histopathological markers in the atrial
tissue that would serve as predictors for postoperative atrial tachyarrhythmias.
By identifying such markers i f present, a more selective approach to
prophylaxis would then be possible. They chose vacuolation of atrial
myocardium and lipofuscin accumulation in atrial myocardium as the
potential markers for increased vulnerability to the development of
postoperative atria fibrillation.
Lipopigment storage is considered to be a part of the ubiquitous process
of aging(52) and affects especially postmitotic cells such as neurons and
cardiac myocytes(53) This pigment represents the end product of lysosomal
degradation, and is causally associated with the long-term oxygen free radical
attacks upon cellular lipids(54). However, in the present study, they did not
observe any association between the subjective estimation of the lipofuscin
accumulation and the chronological age of the patient.
27

Vacuolation of cardiac cells has been described in multiple conditions
of mild, reversible damage to cardiac cells, both in man and experimental
animals, including exposure to toxic stimuli, (55) or hypoxia and
ischemia(56,5 8-60). On the other hand, the occasional finding of vacuoles in
cardiac cells with no known disease led other investigators to consider this
vacuolation as an insignificant aging phenomenon(59). Despite its being a
potential marker of damage, vacuolation has not been previously correlated
with a clinical postoperative outcome and has been studied in man only in
ventricular cells and not in atrial cells.
Although the findings in this study strongly suggest that vacuolation is a
predictor of vulnerability to the development of postoperative atrial
fibrillation, further investigation in larger numbers of patients is required to
confirm this association. If confirmed in a larger series of patients, these
findings may have several potential outcomes. Better predictability of the risk
for developing atrial fibrillation may lead to better monitoring of vulnerable
patients, and possibly to better treatment. Preventive antiarrhythmic drugs,
that are not recommended for the treatment of all patients after cardiac
surgery, may be indicated for those patients at higher risk for developing
atrial fibrillation.
The impression that the staining intensity of lipofuscin, the aging
pigment, might also be associated with the risk of developing atrial
fibrillation also merits attention. It should be noted that, at the narrow range
of ages of patients in their study, no correlation was found between lipofuscin
28
levels and chronological age. It is possible that lipofuscin reflects aging
processes in the cells better than the actual chronological age of the patient.
On the other hand, it is possible that vacuolation accentuates the visibility of
lipofuscin, so that the correlation between atrial fibrillation and this pigment
reflects another facet of the correlation between vacuolation and atrial
fibrillation.
The mechanism of the initiation of postoperative atrial fibrillation is still
unknown, but this study indicates that the metabolic status of the atrium,
reflected in its morphology, is a major determinant in the pathogenesis of this
frequent complication of cardiac surgery.
Sequelae
Long-term sequelae of postoperative atrial fibrillation are unusual;
however, major complications may occur in a small percentage of patients.
The most serious complications are thromboembolic events, especially
stroke. Creswell et al(40) showed that postoperative atrial fibrillation was
associated with an increased incidence of postoperative strokes compared
with patients without atrial fibrillation (3.3% vs 1.4%, P<.0005). This
association was independent of age. In addition, atrial fibrillation can result
in hypotension or congestive heart failure, an increased incidence of
ventricular arrhythmias(tachycardia or fibrillation), and an increased need for
the placement of a permanent pacemaker. However, the most common
complication of postoperative atrial fibrillation is an increased length and
29

cost of hospitalization (Figure7). In a single patient, atrial fibrillation is not
the most expensive complication of cardiovascular surgery, but its high
incidence results in a cumulative cost that exceeds all other complications.
Aranki et al(8) found that the length of hospitalization in creased by 4.9 days
as a direct result of atrial fibrillation (Figure 8). This translated into an
additional $10,055 in hospital charges per patient. Therefore, any inter
vention that would reduce the incidence of postoperative atrial fibrillation
would result in a tremendous economic benefit.
30

ICU Nursing Ward
• Without Atrial Arrhythmias ^ With Atrial Arrhythmias
Figure 7. (A) Patients with postoperative atrial arrhythmias experienced a
longer intensive care unit (ICU) and nursing ward hospitalization. (From
Creswell L L : Hazards of postoperative atrial fibrillation. The Ann Thorac
Surg 56:539-549,1993)
31

• Without Atrial Arrhythmias ^ With Atrial Arrhythmias
p<0.0005
V-Tach/V-Fib Pacemaker Stroke
Figure 7. (B) Patients with postoperative atrial arrhythmias increased
frequency of ventricular tachycardia (V-Tach) or ventricular fibrillation (V-
Fib), permanent pacemacker implantation, and stroke. (From Creswell L L :
Hazards of postoperative atrial arrhythmias: The Annals of Thoracic Surgery
1993, vol. 56,539-549).
32

50
5 6 7 8 9 10 >10 Length of Stay (days)
Figure 8. Relationship between duration of hospitalization and development
of postoperative atrial fibrillation (AFIB). (From Aranki SF, Shaw DP,
Adams DH, et al: Predictors of atrial fibrillation after coronary artery surgery.
Current trends and impact on hospital resources. Circulation 94:390-397,
1996)
33

PROPHYLAXIS
A variety of agents have shown to be effective in preventing the
occurrence of atrial fibrillation in this setting. The most solid evidence for
atrial fibrillation prophylaxis exists for the effectiveness of beta-blockers. In
1988, Lauer reported from a survey of chiefs of cardiothoracic surgery that
44% were using beta-blockers for atrial fibrillation prophylaxis in the
postoperative setting (5). Hesitancy to use beta-blockers probably represents
the increasing prevalence of elderly patients with poor left ventricular
function and other relative contraindications to beta-blocker use among those
who are now currently undergoing C A B G .
A variety of beta-blockers including propanolol, timolol, metoprolol,
nadolol, and acebutolol have been found effective when administered
postoperatively to prevent or decrease the number of episodes of atrial
fibrillation (61-63). Two meta-analyses of beta-blockers have confirmed the
beneficial effects of their prophylactic administration. Andrews et al. selected
24 of 69 studies that had adequate control groups or proper randomization
procedures and reported a decrease in the incidence of post-CABG atrial
fibrillation from 34% to 8.7% (P < 0.0001) in 1,549 patients receiving
prophylactic beta-blockers (64). Their analysis suggested beta-blocker
34

therapy was of most benefit in patients at greatest risk of hemodynamic
compromise from atrial fibrillation (e.g., those patients with left ventricular
dysfunction). Kowey's meta-analysis of 7 trials included 2,482 patients and
showed a reduction in the incidence of supraventricular arrhythmias from
20% to 9.8% in patients taking beta-blockers (P < 0.001)(65). Various
definitions of atrial fibrillation are used in different studies, with some
varying from 30 seconds to several minutes in length. The effect of the time
of initiation and dose of beta-blocker on the incidence of atrial fibrillation
does not seem to be important. A final concern they have is the relevance of
applying the results of studies done mostly during 1970-1980 to the current
practice of cardiac surgery. The patients now being operated on are older,
sicker, and have more severe underlying cardiac disease. Additional trials are
needed to determine the safety and efficacy of beta-blocker prophylaxis in
this patient population.
Digoxin does not appear to have a consistent effect on the prevention of
postoperative atrial fibrillation (66,67). Meta-analyses of the prophylaxis
trials using digoxin showed no significant benefit of digoxin use in the
prevention of atrial fibrillation. There are no placebo-controlled, double-blind
trials of digoxin as a prophylactic agent for atrial fibrillation. A combination
of digoxin and beta-blockers caused a greater reduction in the incidence of
atrial fibrillation, suggesting a possible synergism between the two agents.
Studies with oral verapamil and a meta-analysis of oral verapamil have
failed to show any effect of this agent on preventing atrial fibrillation
35

(64,68,69). Oral verapamil was, however, shown to cause a lower ventricular
rate, but higher rates of hypotension and pulmonary edema were also seen. In
a small-randomized study of IV diltiazem vs. IV nitroglycerin, there was a
lower incidence of atrial fibrillation in the patients who received IV diltiazem
(70).
Studies of the efficacy of magnesium in preventing post-CABG atrial
fibrillation have shown variable results. Two placebo-controlled trials of IV
magnesium beginning immediately in the postoperative setting failed to show
any benefit (71,72). Others have found a benefit of IV magnesium when
levels were increased to 2.0 mEq/L or more, but in general this difference is
small. The mechanisms by which magnesium may have an effect on the
incidence of atrial fibrillation are unknown.
Amiodarone has also been shown to be beneficial in the prevention of
postoperative atrial fibrillation. Daoud et al (73) administered oral
amiodarone for at least 7 days before elective cardiac surgery. As a result,
the incidence of postoperative atrial fibrillation decreased from 53% to 25%
(P = .003). This was associated with a decreased length and cost of
hospitalization. In addition, complication rates were similar in the 2 groups.
Because many cardiac surgical patients cannot delay their surgery for 1 week
to receive oral amiodarone, the Amiodarone Reduction in Coronary Heart
(ARCH) Trial was performed (74). In this study, patients received
intravenous amiodarone immediately after surgery. Once again, this resulted
36

in a reduction in the incidence of postoperative atrial fibrillation (47% vs.
35%), without significant morbidity or mortality.
Antiarrhythmic agents such as procainamide, quinidine, and
propafenone have also failed to significantly impact on the incidence of
postoperative atrial fibrillation. (75-77)
Nonpharmacological interventions have also been attempted because
the use of beta-blockers and amiodarone may be limited by bradycardia, heart
block, hypotension, and bronchospasm. As a result, atrial pacing has been
studied to prevent postoperative atrial fibrillation (78-80). Gerstenfeld et al
showed that continuous right atrial or biatrial pacing was safe and well
tolerated. Recently, some data have suggested an additional protective effect
of biatrial pacing compared with pacing the right atrium alone (81). It is
common clinical practice to perform overdrive atrial pacing in the
postoperative period to suppress atrial ectopy and provide optimal
hemodynamics. A recent preliminary report from a randomized, controlled
clinical trial of atrial overdrive pacing (AAI pacing mode) at rates greater
than or equal to 10 beats/min faster than the intrinsic heart rate (i.e.,
approximately 90-110 beats/min) did not prevent postoperative atrial
fibrillation (82). Future studies must address whether biatrial pacing has any
benefit in the prevention of atrial fibrillation.
However, one study showed that atrial pacing only prevented
postoperative atrial fibrillation in patients who were also treated with a
37

beta-blocker. They studied the effects of atrial pacing in 123 patients
undergoing coronary artery bypass graft surgery, who were also treated with
propranolol (80). In this study, epicardial pacing reduced the incidence of
postoperative atrial fibrillation from 31% to 13% (P = .04). In addition, the
length of hospitalization was also reduced.
Strategies to prevent postoperative at atrial fibrillation are most
beneficial in high-risk patients. Therefore, these strategies are most
important in patients with advanced age, a prior history of atrial fibrillation,
or undergoing valvular surgery. Both beta-blockers and amiodarone have
been shown to be beneficial, but neither has been proven superior to the
other. Depite many clinical studies, there is still no consensus regarding the
best prevention strategy for postoperative atrial fibrillation. Consequently,
cardiac surgeons are challenged to devise strategies to prevent its
occurrence.
3 8

CHAPTER 2
OBJECTIVE OF THE THESIS
Everyone in the cardiac surgery team (Residents, Fellows, Nurses,
Cardiac surgeons) has to deal with Postoperative Atrial Fibrillation. We
found that this problem is the most common complication of postoperative
coronary artery bypass grafting surgery in our hospital. Although often a
benign complication, it can result in significant morbidity and prolong
hospitalization with attendant increased expenditure of health care resources.
The pathophysiological mechanisms responsible for atrial fibrillation after a
cardiac procedure remain unclear, although several clinical studies published
during the past decade have identified certain preoperative risk factors
associated with postoperative atrial fibrillation, there is still no consensus
regarding the best prevention strategy for this arrhythmia. We recently
reviewed the literatures and discussed this problem in a group. Because of the
multifactorial etiology of postoperative atrial fibriallation (for example,
increased catecholamines, pericardial inflammation/effusion, rapid shifts in
fluid and electrolyte status, atrial ishemia, autonomic dysfunction, local
surgical trauma, abnormal electrophysiological substrate (aging,
hypertension), and well known inflammatory response to cardiopulmonary
bypass (83,84)) steroid might have a beneficial effect in decreasing the
incidence of postoperative atrial fibrillation after coronary artery bypass
grafting (CABG).
Consequently, we designed the study to identify the incidence of
postoperative atrial fibrillation between two groups (Steroid and Placebo)
39

Possible mechanism of inflammatory response of cardiopulmonary bypass
Despite the normal convalescence of the vast majority of patients
undergoing open cardiac operations, the experienced surgeon will
occasionally see the patient who has an adverse reaction to the CPB
experience (the "postperfusion syndrome"), with evidence of prolonged
pulmonary insufficiency, excessive accumulation of extravascular water, and
to a variable degree, renal and other organ dysfunction, hyperthermia,
vasoconstriction, and coagulopathy. These sequelae of CPB may occur in the
face of an apparently effective and complete cardiac operation with good
hemodynamic performance. Such occurrences are more frequent if the
surgeon operates on infants and neonates or the very elderly.
Dating from the early experience with open-heart surgery, surgeons have
noted the tendency for extravascular fluid accumulation in patients after CPB.
Cleland and colleagues at the Mayo Clinic (85) published their observations
in 1966 and related the increase in extravascular fluid to the duration of CPB.
It was not until 1987, however, that Smith and colleagues (86) provided the
first direct evidence for increased microvascular permeability after CPB using
ultrafiltration techniques in a canine model. Using the microvascular colloid
osmotic sieving ratio determined by minimal lymph-plasma protein ratios,
these investigators demonstrated an increase in permeability to proteins after
2 hours of normothermic CPB in the dog.
40

It has been hypothesized that the damaging effects of CPB are related to
the exposure of blood to abnormal surfaces and conditions, which then
initiates a systemic inflammatory response involving both formed and
unformed blood elements that normally act locally at sites of injury (87). A
critical aspect of this "whole body inflammatory response" involves the
humoral amplification system, which includes the coagulation cascade, the
kallikrein system, the fibrinolytic system and the complement cascade. The
damaging effects of CPB likely result in large part from the activation and
interaction of these cascades.
The organ most commonly associated with CPB induced dysfunction is
the lung. During the initial phase of CPB, complement is activated primarily
through the alternative pathway (88), resulting in release of the
anaphylatoxins C3a and C5a. Increased pulmonary and other subsystem
morbidity has been associated with higher complement C3a levels during
CPB (89). Chenoweth and Hugh (90) demonstrated specific binding sites on
neutrophils for the anaphylatoxin C5a. After cleavage of C5 in the
complement cascade another active component, pore-forming C5b-9
complex, is known to stimulate arachidonic metabolism and further promote
granulocyte activation (91). Salama and colleagues (91) have demonstrated
pore-forming C5b-9 complexes on neutrophils as well as on erythrocytes
during CPB. The end result is leukocyte activation and subsequent deposition
in the lungs and other organs. Transpulmonary leukocyte sequestration occurs
during partial bypass (88), and previous studies in patients on hemodialysis
41
demonstrated transient neutropenia with temporary pulmonary dysfunction
associated with complement activation at the beginning of hemodialysis
(92,93). In a sheep model, Flick and colleagues (94) showed that leukocytes
are required for the increased pulmonary water seen after microembolization.
These effects of CPB may in part result from oxygen free radical release (95)
during pulmonary reperfusion and lysosomal enzyme release from activated
neutrophils (96,97). It thus appears that leukocyte (and possibly platelet)
activation and sequestration are closely linked to the changes in
extrapulmonary water and to occasional pulmonary dysfunction observed
after CPB.
Over the past several years, the literature has been replete with studies
demonstrating high circulating levels of metabolic by-products of the various
cascades as well as other inflammatory by-products during CPB.
Unfortunately, the vast majority of these studies simply identify the presence
of various inflammatory by-products or mediators without showing some
relevance to patient morbidity after CPB. Because most patients tolerate the
experience of CPB extremely well, there must be a sophisticated natural
process that allows neutralization, inhibition, or interruption of these
pathways and the prevention of important organ damage in most patients.
Steroid and inflammatory response process
With the discovery of cytokines as inflammatory mediators and the
ability to measure many of these molecules, many studies have demonstrated
42

the ability of glucocorticoids to blunt the cardiopulmonary bypass-related in
creases in circulating levels of many of these inflammatory mediators,
including IL-6, IL-8, TNF-alpha, C D l l b , leukotrieneB4, and tissue
plasminogen activator (98-106).
Teoh and associates (98) have shown that the peripheral vasodilatation
seen after normothermic cardiopulmonary bypass from effects of cytokines
can be improved by steroid administration.
Jansen et al demonstrated a leukocyte inflammatory response on
reperfusion of the heart and lungs, shown by an increase of TNF, LTB4, and
t-PA activity, which correlates with the clinical hemodynamic condition after
Cardiopulmonary bypass. They also showed that dexamethasone treatment
significantly inhibits the formation of these inflammatory mediators and thus
prevents the hemodynamic instability after cardiopulmonary bypass, which
improves the postoperative course (99).
Another study from Engelman et al showed a dramatic decrease in the
level of cytokine response related to steroid administration and recommended
prophylactic steroid use during routine open-heart operations (100).
Although many studies showed beneficial effects of corticosteroid on
open-heart operations, Mayumi et al concluded that T-cell functions are
synergistically suppressed by cardiopulmonary bypass and high-dose
methylpredinolone in heart operation (107).
43

Research plan
With unknown mechanism of postoperative atrial fibrillation,
multifactorial etiology (including pericardial inflammation/effusion from
surgery, pericarditis, local surgical trauma and cannulation, postsurgical
effects on previously damaged myocardial tissue, systemic inflammatory
response induced by cardiopulmonary bypass, poor atrial preservation during
aortic crossclamping, atrial distention, autonomic disruption from surgery,
enhanced sympathetic activity, postoperative hemodynamic changes,
metabolic derangements and fluid shifts, abnormal electrophysiological
substrate (aging, hypertension), and the beneficial effects of steroid from the
literature review, we decided to design a prospective randomized trial to
determine the effects of short-term steroid administration on the incidence of
postoperative atrial fibrillation after coronary artery bypass grafting surgery
(CABG).
Study hypothesis
The purpose of this study is to investigate whether steroid (combined
preoperative and postoperative in acute short term) can reduce the incidence
of postoperative atrial fibrillation after C A B G , including the length of
hospital stay and the adverse effects of steroid. The null and alternative
hypotheses of this study are:
44

HO: Steroid (acute short term) administration pre and postoperative C A B G
surgery has no effect on incidence of postoperative atrial fibrillation after
C A B G .
Ha: Steroid administration pre and postoperative C A B G surgery can
change the incidence of postoperative atrial fibrillation after C A B G .
Primary outcome
In this study we plan to follow up the incidence of postoperative atrial
fibrillation after C A B G compared between steroid group and placebo group.
Secondary outcome
In addition to the primary outcome, we plan to study the length of
hospital stay between the two groups and compare the length of hospital stay
between normal sinus rhythm patients and atrial fibrillation patients. Since
there was one study showed that steroid administration and cardiopulmonary
bypass could synergistically suppress T-cell function, we also plan to study
the adverse effects (in term of complications) of steroid.
Benefit
Despite many clinical studies, there is still no consensus regarding the
best prevention strategy for postoperative atrial fibrillation after C A B G . If we
find in this study that short term steroid administration can reduce the
4 5

incidence of postoperative atrial fibrillation after C A B G , shorten the length of
hospital stay with no adverse effects, prophylaxis with short term steroid in
patients undergoing coronary artery bypass grating surgery would be an ideal
approach.
Study design
This study is designed as a randomized, double blind placebo controlled
clinical trial. Patients are randomized into one of the two study groups,
placebo group and steroid treatment group, in blocks of 8.
Material and Methods
The Ethics committee for Human Experimentation of St.Paul's hospital,
Vancouver, B.C. approved this study in May 2000. (Study no# p 99-0254)
Sample size
We reviewed the data from B.C. cardiac registration and found that the
incidence of postoperative atrial fibrillation after C A B G in St.Paul's Hospital
from 1993 to 1999 is 43.5%.
To detect a 50 % reduction in the steroid treatment group with power of
80 % and two-sided type I error of 0.05.
The require sample size for this study is 162 patients. (Placebo group
81, Steroid group 81)
46

Before we started running the study, we decided to do 50 % interim
analysis and planned to stop the study if the result showed a significant
decrease in the incidence of postoperative atrial fibrillation after C A B G . As a
result, from August 1,2000 to February 28,2001, 88 patients were enrolled for
this study, two patients were excluded from the study because the surgeon did
Off-Pump coronary artery bypass grafting surgery, when we did the interim
analysis we found the incidence of postoperative atrial fibrillation in the
steroid group was significantly less than placebo group.
PATIENT SELECTION
Inclusion criteria
• The patient is undergoing elective first-time coronary artery bypass
grafting and was on beta-blockage.
• The patient has signed a study-specific consent form agreeing to the
randomization, data collection, and follow-up requirements.
Exclusion criteria
• The patient has history of heart block,
• The patient has a permanent pacemaker.
• The patient has any documented or suspected supraventricular or
ventricular arrhythmias, including isolated atrial or ventricular
premature depolarization noted on preoperative surface
electrocardiography.
47

• The patient requires additional procedures, such as valvular surgery or
left ventricular aneurysmectomy.
• The patient refused to participate in this study.
• The patient need radial artery to be grafted.
• The patient who was steroid dependent.
• The patient who was allergic to steroid.
• The patient who was not on beta-blockage.
Steroid administration
Patients are randomly assigned to receive in a double blind fashion
either
• Placebo group receives maintenance fluids (5% dextrose water with 20
mEq of potassium chloride per liter) or
• Steroid group receives the steroid dosage 1 gm of intravenous
methylprednisolone sodiumsuccinate (Solu-Medrol; Upjohn,
Kalamazoo, MI) before Cardiopulmonary bypass and 4 mg of
intravenous dexamethasone (Decadron; Merck Sharp & Dohme, West
Point, PA) every 6 hours for a total of four doses in the first 24 hours
after operation.
• A l l vials of the steroid and placebo medications were prepared and
randomized by the pharmacists.
48

Operative technique
A standardized anesthesia and surgical protocol was applied in all
cases. A l l operations were performed using normothermic (37°c)
cardiopulmonary bypass with antegrade warm blood cardioplegia.
Cardiopulmonary bypass was performed using aortic and right atrial
cannulation, a membrane oxygenator, and nonpulsatile flow.
Standard surgical techniques were used to create the distal coronary
anastomoses first, and then proximal anastomoses were followed.
After weaning off cardiopulmonary bypass system, inotropic support
was initiated when needed to maintain cardiac contractility or i f the
cardiac index was less than 2L.min-l.m-2, or i f the mean arterial pressure
was less than 70 mmHg. Electrical pacing was instituted (atrial or
atrioventricular) when needed to maintain a heart rate greater than 70
beats/min. Patients were continuously monitored in the cardiothoracic
intensive care unit. Patients were weaned off mechanical ventilation based
on hemodynamic stability, blood gas analysis, and level of alertness.
Discharge from the cardiothoracic intensive care unit was generally
accomplished after extubation and the discontinuation of all vasoactive
infusions.
Patients receiving beta blockage, digitalis, calcium channel
blockage had these medications continued until the day of operation.
Standard postoperative medication will be performed. Patients received
the usual postoperative cardiac care, including the use of beta blockade to
prevent atrial arrhythmias as a standard protocol.
49

Hemodynamic Measurement and Monitor
Patients will be continuously monitored in the cardiothoracic intensive
care unit with arterial, central venous, and pulmonary artery pressure
monitoring with thermodilution cardiac output determination.
Cardiac rhythm will be continuously monitored in the intensive care
unit with bedside monitors (MARQUETTE Hard-wire SOLAR 7000) and,
after intensive care unit discharge date with Telemetry on the floor 5A/5B
(HEWLETT P A C K A R D model M2360A serial no.3329A02191). Twelve
lead electrocardiograms will be obtained immediately postoperatively and on
the first morning after the operation. Supraventricular and ventricular
arrhythmias and respective treatment interventions will be documented by the
patient's nurse and supported by the inclusion of rhythm strips in the patient
chart. The investigator reviewed all patients' rhythm strips on a daily basis
until the patients were discharged from the hospital.
For the purpose of defining end points in this study, postoperative atrial
fibrillation was defined by the group as:
Atrial fibrillation was defined when irregularly irregular
supraventricular rhythm was present in the absence of P waves, that required
treatment, which was typically sustained for more than 15 minutes.
50

Episodes of atrial fibrillation that recurred or continued into the
following 24-hour period as an additional episode. Arrhythmia data were
collected and recorded for the first 7 postoperative days.
Using these definitions, cardiac arrhythmias will be treated under the
direction of the attending surgeon. Standardized protocols for the treatment of
supraventricular and ventricular arrhythmias were adhered to during the
course of the study. Blood gas abnormalities will be corrected. Potassium,
Magnesium, and Calcium will be administered as needed to maintain serum
concentrations greater than 4 mmol/L, 1.5 mEq/L, and 8.5 mg/dL,
respectively.
Therapeutic approaches for treatment postoperative atrial fibrillation on
the floor included:
a. Drugs to control ventricular rate (digoxin or beta adrenergic
blockers intravenous consider by left ventricular ejection
function, heart failure, and lung disease).
b. Drugs to convert to normal sinus rhythm (sotolol, propafenone,
amiodarone, or any beta-blocker consider as patient status, sex,
and conditions).
c. Electrical cardioconversion will be attempted when atrial
fibrillation results in hemodynamic instability or when clinically
indicated in the setting of failure of pharmacologic conversion.
Patients will be routinely anticoagulated with heparin, warfarin, or both
when atrial fibrillation persisted for longer than 36 hours.
Patients were followed up as routine protocol on the ward until they
were discharged from the hospital. The length of hospital stay was calculated
51

from the day of surgery until the day of discharge. A l l complications were
recorded in the data form. We divided complications into major and minor
complication. Major complications were defined as the situations or problems
that patients needed to have an operation: for example, severe sternal
infection that needed debridement or rewiring. Minor complications were
defined as the situations or problems that patients needed only medication for
treatment: for example, superficial wound infection that needed only
antibiotic for treatment.
Major complications included severe strenum infection needing
rewiring, acute pancreatitis, and perforated GU. Minor complications were
defined as situations or problems that patients need only medication
treatment. These included GI upset (gastrointestinal upset patients that need
IV Fluid treatment for at least 4 days postoperative), high blood sugar (that
need endocrinologist to control blood sugar postoperative), mental confusion
(that need antipsychotic medication for at least 4 days postoperative),
elevated creatinine postoperative, UTI (Urinary tract infection that need IV
Antibiotic Treatment), sternum wound infection, IV line infection and Leg
wound infection needed IV antibiotic treatment, gastritis that need
Gastroenterologist consultation.
52

Statistics
At the time of study termination, the treatment code was broken.
Medical history, demographic data, and the clinical course were analyzed for
each patient.
Comparison of continuous variable across the two treatment groups was
accomplished using a two-sample t test or Wilcoxon rank-sum test where
appropriate.
Comparison of categorical variables across the two groups was analyzed
by using chi-square test or Fisher's exact test (where applicable). A logistic
regression analysis was carried out to compare the two groups with possible
confounders adjusted.
P values of less than 0.05 are considered to be statistically significant.
Statistical analysis was performed using SAS software (Cary,NC).
Breaking the code-Interim analysis
After 50 % of enrollment, we planned to do an Interim analysis. The
benefit is that the trial might be stopped earlier if we can find a significant
reduction of the incidence of postoperative atrial fibrillation after C A B G in
steroid treatment group or significant detrimental effect of steroid is
identified.
Based on O'BRIEN-FLEMING approach, the p-value for the interim
analysis is 0.005 and the p-value for the final analysis for the total patient is
0.048.
5 3

Estimated duration of study
After the ethics committee accepted this study, we enrolled 88 patients
as described in the inclusion criteria, followed up the patient and strips review
on a daily basis and collected the data. The study was run from August 1,2000
to February 28,2001. After that the files were reviewed. The codes were
broken by the pharmacists. The data were separated into two groups by the
nurse and analyzed by the statisticians. The result showed significantly
decreasing in postoperative atrial fibrillation in Steroid treatment group, and
then we decide to stop and analyze all the data.
54

Data base form
Supervisor:Dr.Samuel V.Lichtenstein,
Investigator:Dr.Kriengchai Prasongsukarn No
Patient name code
Sex : m _ f _ DOA DOS DOC
Hx of M I : Y _ N _ Hx of C H F : Y _ N _
Hx of COPD: Y _ N _ Hx of s m o k i n g : Y _ N _
Hx of Asthma: Y _ N _ Hx of HTN: Y _ N _
H x o f C R F : Y _ N _
Pre -op Med:
beta-blocker
Ca blocker
digitalis
Ejection fraction % Temp of cardioplegia cel.
Xclamp time min. No. of bypass
bypass time min.
Pacing :A-pace Avpace Vpace Start time Stop time
Pacing:A-pace Avpace Vpace Start time Stop time
Pacing :A-pace Avpace Vpace Start time Stop time
Pacing:A-pace Avpace Vpace Start time Stop time
Pacing :A-pace Avpace Vpace Start time Stop time
5 5

Arrhythmias:
Date Start time Stop Time Rhythm Rx
Date Start time Stop Time Rhythm Rx
Date Start time Stop Time Rhythm Rx
Date Start time Stop Time Rhythm Rx
Date Start time Stop Time Rhythm Rx
Date Start time Stop Time Rhythm Rx
Date Start time Stop Time Rhythm Rx
Date Start time Stop Time Rhythm Rx
Medication for control arrhythmia when D/C
Complication Date Rx
Complication Date Rx
Complication Date Rx
Complication Date Rx
White blood cell count 12 hour 24 hour
56

Result
This randomized, prospective clinical trial was carried out in 88
patients, and two patients were excluded from the study due to Off-pump
Coronary artery bypass grafting surgery, 43 patients with steroid and 43
patients with placebo. Selected patient demographics are presented in table 9.
Statistically significant differences were found for age and ejection fraction
(LVEF). Other variables including sex, History of MI, asthma, COPD,
Congestive heart failure, hypertension, smoking, chronic renal failure,
preoperative medications, ischemic time, number of bypass grafts, pacing
type were not different between two groups (table 3,5-18). There was no
death in the study period.
Postoperative Atrial fibrillation
The percentages of incidence of postoperative atrial fibrillation
patients between two groups are shown in Figure 9. The incidence of
postoperative atrial fibrillation was 20.93 % (9 of 43 patients) in the short-
term steroid group, as compared with 51.16 % (22 of 43 patients) in the
placebo group (P=0.0035) (Table 4).
The number of episode of atrial fibrillation was compared between two
groups (Table 5). It is appeared that Placebo group had a higher number of
episodes of postoperative atrial fibrillation than Steroid group (P=0.0164).
57
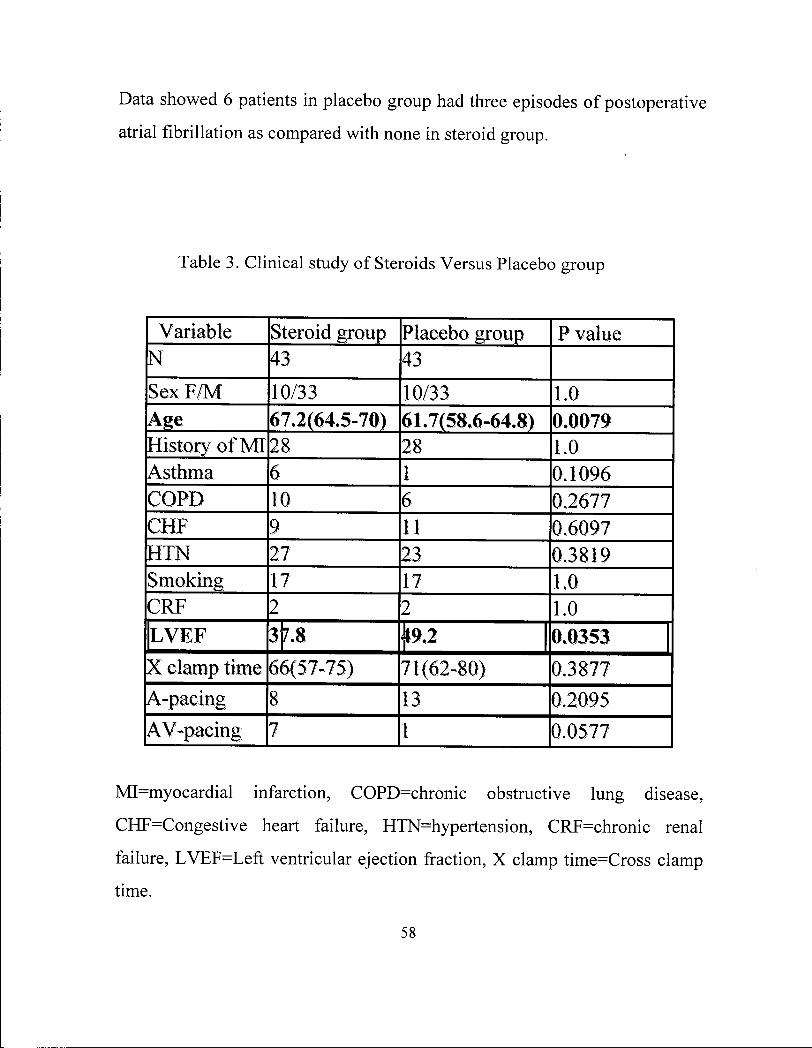
Data showed 6 patients in placebo group had three episodes of postoperative
atrial fibrillation as compared with none in steroid group.
Table 3 . Clinical study of Steroids Versus Placebo group
Variable Steroid group Placebo group P value N 43 43 Sex F /M 10/33 10/33 1.0 Age 67.2(64.5-70) 61.7(58.6-64.8) 0.0079 History of MI 28 28 1.0 Asthma 6 1 0.1096 COPD 10 6 0.2677 CHF 9 11 0.6097 HTN 27 23 0.3819 Smoking 17 17 1.0 CRF 2 2 1.0 LVEF 3]7.8 0.0353 X clamp time 66(57-75) 71(62-80) 0.3877 A-pacing 8 13 0.2095 AV-pacing 7 1 0.0577
MI=myocardial infarction, COPD=chronic obstructive lung disease,
CHF=Congestive heart failure, HTN=hypertension, CRF=chronic renal
failure, LVEF=Left ventricular ejection fraction, X clamp time=Cross clamp
time.
58
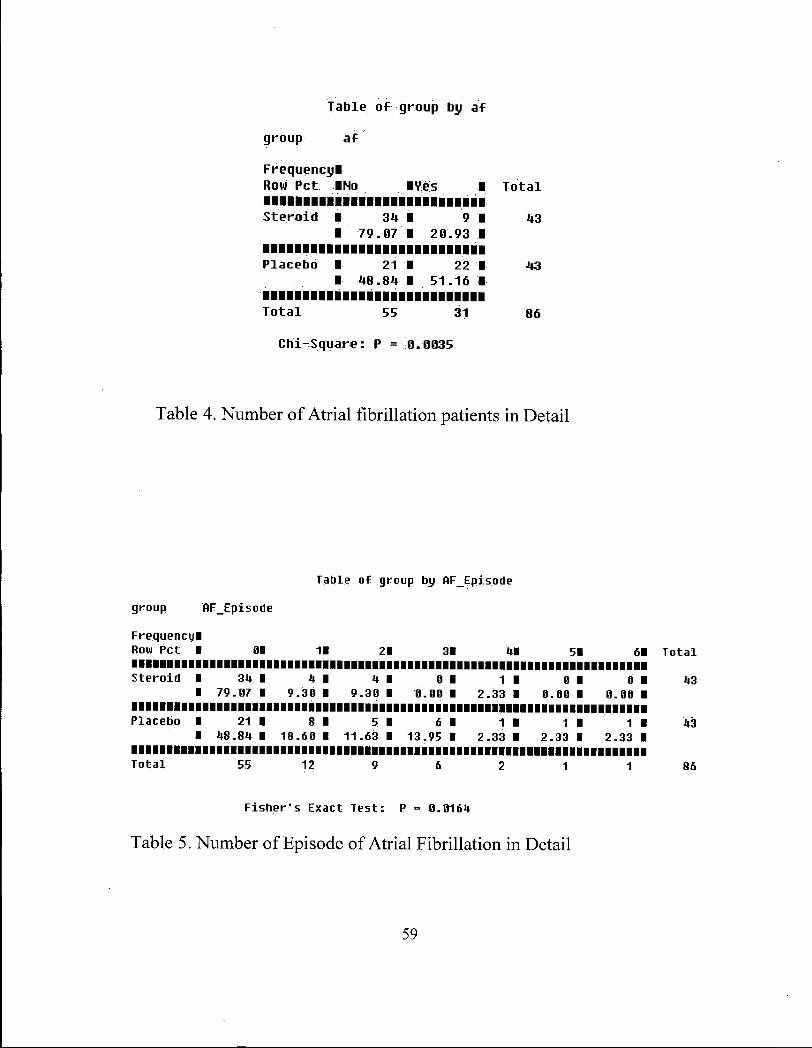
T a b l e o f group by a f
group a f
F r e q u e n c y ! Row Pet INo IVes I T o t a l
S t e r o i d I 34 I 9 I 43 1 79 .07 I 20 .93 1
P l a c e b o I 21 I 22 I 43 I 48 • 84 1 51 .16 I
T o t a l 55 31 86
C h i - S q u a r e : P = 0.0035
Table 4. Number of Atrial fibrillation patients in Detail
Table of group by HFEpisode
group AF_Episode
Frequency! Row Pet I 01 11 21 31 41 51 61
S t e r o i d I 34 I 4 I 4 I 0 I 1 I 0 I 0 I I 79 . 0 7 I 9 . 3 0 I 9 . 3 0 I 0 . 0 0 I 2 . 3 3 I 0 . 0 0 I 0 . 0 0 I
Placebo • 21 I 8 I 5 I 6 1 1 I 1 I 1 1 I 48 . 8 4 I 18 . 6 0 I 11 .63 I 1 3 . 9 5 1 2 . 3 3 I 2 . 3 3 I 2 . 3 3 I
T o t a l 55 12 9 6 2 1 1
Fisher's Exact Test: P = 0 .0164
Table 5. Number of Episode of Atrial Fibrillation in Detail
59

Figure 9. Incidence of Postoperative Atrial Fibrillation compared
between Short-Term Steroid Treatment Group and Placebo Group
60

Table of group by Sexa
group Sexa
Frequency! Row Pet IF IM I Total
Steroid I 10 I 33 '1 43 1 23 .26 I 76 .74 I
Placebo I 10 I 33 • 43 1 23 .26 I 76 .74 I
Total 20 66 86
Chi-Square: P = 1.0000
Table 6. Number of sex of Patients in Detail
Table of group by chf
group chf
Frequencyl Row Pet IHo IVes I Total
Steroid 1 34 1 9 1 43 1 79 .07 1 20 .93 1
Placebo 1 32 1 11 1 43 1 74 .42 1 25 .58 I
Total 66 20 86
Chi-Square: P = 0.6097
Table 7. Number of Congestive Heart Failure Patients in Detail
61

Table of group by ni
group mi
Frequency! Row Pet •No • Yes • Total
Steroid 1 15 • 28 • 43 1 34 .88 • 65 -12 1
Placebo I 15 • 28 • 43 I 34 .88 • 65 .12 •
Total 30 56 86
Chi-Square: P = 1 0000
Table 8. Number of Myocardial Infarction Patients in Detail
Table of group by COPD
group COPD
Frequencyl Row Pet INo IVes I Total
Steroid 1 33 1 10 1 43 I 76 .74 1 23 .26 1
Placebo I 37 1 6 1 43 1 86 .05 1 13 .95 I
Total 70 16 86
Chi-Square: p = 0.2677
Table 9. Number of Chronic Obstructive Lung Disease Patients in
Detail
62

Table of group by Asthma
group Asthma
Frequency! Row Pet INo IVes I Tota l
S tero id I 37 I 6 I 43 I 86 .05 1 13 .95 1
Placebo • 42 • 1 • 43 • 97 .67 I 2 .33 I
Tota l 79 7 86
F i s h e r ' s Exact Tes t : P = 0.1096
Table 10. Number of Asthma Patients in Detail
Table of group by smoking
group smoking
Frequency! Row Pet INo IVes I To ta l
S te ro id 1 26 1 17 1 43 1 60 .47 1 39 .53 1
Placebo 1 26 1 17 1 43 I 60 .47 I 39 .53 I
To ta l 52 34 86
Chi -Square: P = 1.0000
Table 11. Number of Smoking Patients in Detail
63

Table of group by erf
group erf
Frequency! Row Pet INo IVes I Total
Steroid I 41 1 2 1 43 I 95. 35 1 4 .65 I
Placebo 1 41 1 2 1 43 • ?!>•- 35 1 4 -65 I
Total 82 4 86
Fisher's Exact Test: P = 1.0000
Table 12. Number of Chronic Renal Failure Patients in Detail
Table of group by HT
group HT
Frequency! Row Pet !No !Ves I Total
Steroid 1 16 1 27 1 43 1 37 •2.1 1 62 .79 1
Placebo 1 20 1 23 1 43 1 46 .51 1 53 .49 1
Total 36 50 86
Chi-Square : P = 0.3819
Table 13. Number of Hypertension Patients in Detail
64

T a b l e o f group by a p a c e
group a p a c e
F r e q u e n c y l Row Pet INo IVes I T o t a l
S t e r o i d I 35 1 8 1 43 1 81 .40 1 18 .60 1
P l a c e b o 1 30 1 13 1 43 1 69 .77 1 30 .23 1
T o t a l 65 21 86
C h i - S q u a r e : P = 0.2095
Table 14. Number of A-Pacing Patients in Detail
T a b l e o f group by aupace
group aupace
F r e q u e n c y l Row Pet INo IVes I T o t a l
S t e r o i d 1 36 1 7 1 43 1. 83 .72 1 16 .28 1
P l a c e b o 1 42 1 1 1 43 1 97 .67 1 2 .33 1
T o t a l 78 8 86
F i s h e r " s E x a c t T e s t : p = 0.-0577
Table 15. Number of AV-Pacing patients in Detail
65

Table of group by No_BP
group No_BP
Frequency! Row Pet I 11 21 31 41 51 61 71 Total
S t e r o i d 1 1 I 7 I 13 1 15 I 4 I 2 I 1 I 43 I 2. 33 I 16 .28 I 30.23 1 34 .88 I 9 .30 I 4 .65 I 2 .33 •
Placebo I e • 9 I 10 I 13 • 10 I 1 I 0 I 43 I 0. 00 I 20 .93 • 23.26 1 30 .23 I 23 .26 I 2 .33 I 0 .00 I
Total 1 16 23 28 14 3 1 86
Fisher's Exact Test: P = 0.4803
Table 16. Number of Bypass Grafts in Patients in Detail
Wilcoxon Scores (Rank Suns) for Uariable EF Classif ied by Uariable group
Sum of Expected Std Deu Mean group N Scores Under HO Under HO Score
Steroid 43 1625.0 1870.50 114.535648 37.790698 Placebo 43 2116.0 1870.50 114.535648 49.209302
Wilcoxon Two-Sample Test: P = 0.0353
Table 17.Left Ventricular Ejection Fraction of Patients in Each Group hr
Detail. This table demonstrates that Patients in Steroid Group had lower Left
Ventricular Ejection Fraction than Patients in Placebo Group (P=0.0353)
66

The TTEST Procedure
S t a t i s t i c s
Var iable group N Lower CL
Mean Mean Upper
Mean CL Lower Std Dew
CL Std Dev
Upper Std Deu
CL Std Err Minimum Maximum
age age
Steroid Placebo
43 43
64.491 58.645
67.263 61.7
70.035 64.754
7.4258 8.1841
9 9.
.006 9256
11.447 12.616
1 .3734 1 .5136
44 39
019 389
88.487 79.477
X_clamp_tine X^clanp_tirie
Steroid Placebo
1)3 43
57.029 62.902
66.186 71.628
75.343 80.354
24.534 23.379
29 28
.755
.354 37.819 36.038
4.5376 4.324
28 29
195 136
Bypass_time Bypass_time
Steroid Placebo
13 43
83.806 86.246
92.512 94.837
101.22 103.43
23.323 23.017
28 27
.286
.915 35.952
35 .48 4.3136
4.257 48 45
213 158
T-Tests
Uariable t Ualue Pr > |t |
age 2.72 0.0079 X_clamp_time -0.87 0.3877 Bypass_tine -0.38 0.7021
Table 18. Patients Characteristics in Age, Cross clamp time, and Bypass time.
From this table, Patients in steroid group were older than patients in placebo
group, the mean age was 67.2 in steroid group compared with 61.7 in placebo
group, and the difference was statistically significant (P =0.0079). Other two
variables (cross clamp time and bypass time) did not show any significant
differences between the two groups.
6 7

Complication
Data showed Steroid Group had higher complications than Placebo
Group (15 Minor complications and 4 Major complications in Steroid Group,
as compared with 6 Minor complications and 2 Major complications in
Placebo group), but there was no statistically significant difference in the
incidence of postoperative complication between two groups
(P=0.0525)(Table 19,20,Figure 10).
There was a significant difference in the number of White blood cell
count at 12,24-hour postoperative period (Table 21,22). It was appeared that
Steroid patients had higher white blood cell count at 12, 24-hours (51.2,51.2
respectively) than Placebo Group (28.5,21,7 respectively)(P<. 0001).
Length of Hospital stay
Normal sinus patients had a shorter length of hospital stay than Atrial
fibrillation patients (median 6 days compared with 8 days, p=0.002)(Table23,
Figure! 1). However, there was no statistically significant difference between
the lengths of Hospital stay between two groups (median 6 days in Steroid
Group as compared with 7 days in Placebo Group, p=0.3371)(Table
24,Figurel2).
68
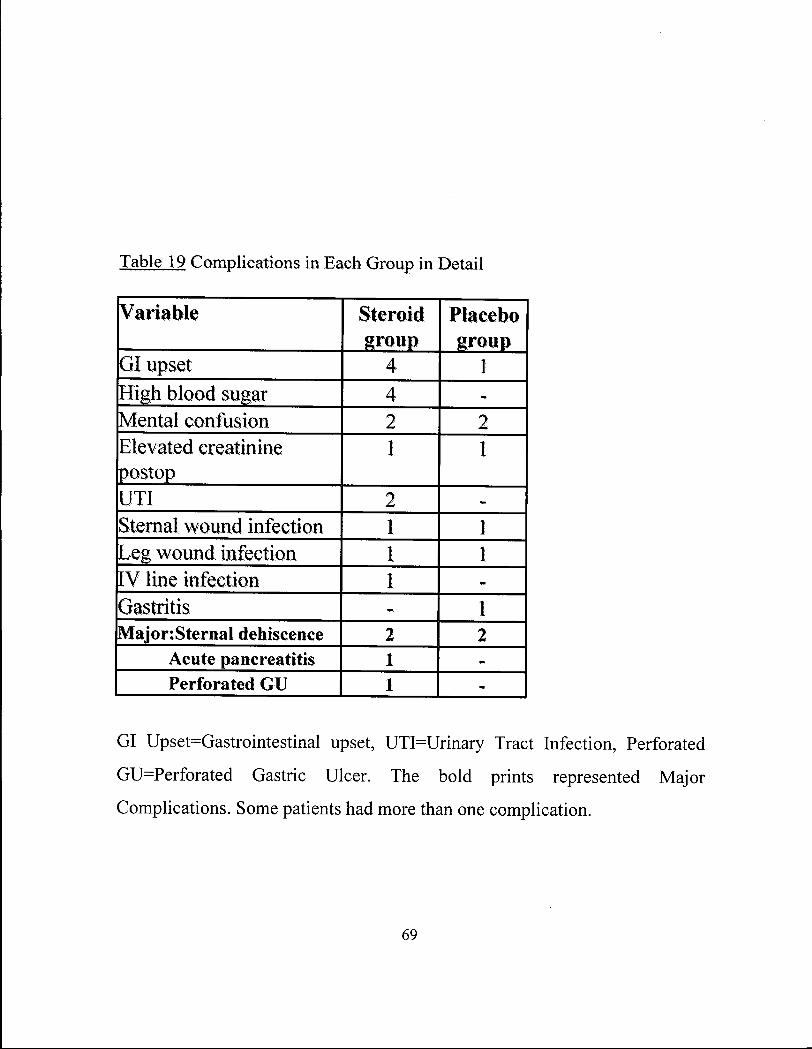
Table 19 Complications in Each Group in Detail
Variable Steroid Placebo group group
GI upset 4 1 High blood sugar 4 -Mental confusion 2 2 Elevated creatinine 1 1 postop UTI 2 -Sternal wound infection 1 1 Leg wound infection 1 1 IV line infection 1 Gastritis - 1 MajonSternal dehiscence 2 2
Acute pancreatitis 1 -Perforated GU 1
GI Upset=Gastrointestinal upset, UTI=Urinary Tract Infection, Perforated
GU=Perforated Gastric Ulcer. The bold prints represented Major
Complications. Some patients had more than one complication.
69

T a b l e o f group by comp
group comp
F r e q u e n c y ! Row Pet INo Comp Imajor I m i n o r I T o t a l
S t e r o i d 1 24 1 4 1 15 1 43 1 55 .81 1 9 .30 1 34 .88 1
P l a c e b o I 35 1 2 1 6 1 43 1 81 .40 1 4 .65 1 13 .95 1
T o t a l 59 6 21 86
F i s h e r ' s E x a c t T e s t : P = 0.0525
Table 20. Number of Complication patients in Detail.
34.88%
• Minor Complication M Major Complication
Steroid Placebo
Figure 10. Percentages of Major and Minor Complications in
Each Group.
70

Wilcoxon Scores (Rank Suns) For Uariable wbc12diFF ClassiFied by Uariable group
Sun oF Expected Std Deu Mean group N Scores Under H0 Under H0 Score
Steroid 40 2048.50 1600.0 101.975425 51.21250 Placebo 39 1111.50 1560.0 101.975425 28.50000
Wilcoxon Two-̂ Sanple Test: P <-.0001
Group N Mean Median Min. Max.
Steroid 40 6.80750 6.5 0.4 21.5
Placebo 39 2.96667 2.7 -1.4 9.1
Table 21. Number of White Blood Cell Count at 12-hour postoperative Period
in Detail.
71

Wilcoxon Scores (Rank Suns) for Uariable wbc24diff Classi f ied by Uariable group
Sun of Expected Std Deu Mean group N Scores Under HO Under HO Score
Steroid 36 1846.0 1314.0 88.786895 51.277778 Placebo 36 782.0 1314.O 88.786895 21.722222
Wilcoxon Two-Sanple Test: P <.0001
Group N Mean Median Min. Max.
Steroid 36 9.57222 8.45 3.2 21.7
Placebo 36 3.40000 2.50 0.2 11.1
Table 22. Number of White Blood Cell count at 24-hour postoperative period
in Detail.
72

W i l c o x o n S c o r e s (Rank Suns) f o r U a r i a b l e l o s _ s u r g e r y C l a s s i f i e d by U a r i a b l e a f
Sun o f E x p e c t e d S t d Deu Mean a f N S c o r e s Under H Q Under H O S c o r e
NO 55 2 054 .0 2392 .50 109.318924 37 .345455 Ves 31 1687 .0 1348 .50 109.318924 54 .419355
W i l c o x o n T w o - S a n p l e T e s t : P = 0 .0020
Analysis variable length of hospital stay (by AF rhythm)
AF N Mean Median Min. Max.
No 55 7.52727 6 3 32
Yes 31 9.03226 8 5 24
Table 23. The Length of Hospital Stay compare between Normal Sinus
Rhythm Patient and Atrial Fibrillation Patients.
73

• A F Patient • NSR Patient
Figure 11.Mean score Length of Hospital Stay compare between Normal
Sinus Patient and Atrial Fibrillation Patient.
7 4

Wilcoxon Scores (Rank Sums) for Uariable lossurgery Classif ied by Uariable group
Sum of Expected Std Deu Mean group N Scores Under HO Under HO Score
Steroid 43 1803.50 1870.50 113.841763 41.941860 Placebo 43 1937.50 1870.50 113.841763 45.058140
Wilcoxon Two-Sample Test: P = 0.5607
Analysis Variable length of hospital stay (by Group)
Group N Mean Median Min. Max.
Steroid 43 8.32558 6 3 32
Placebo 43 7.81395 7 4 23
Table 24. The Length of Hospital Stay Compare between Steroid Group and
Placebo Group.
75

36 Steroid Placebo
Figure 12. Mean score Length of Hospital Stay Compare between Steroid
Group and Placebo Group.
76

Risk factors of Postoperative Atrial Fibrillation
A univariate logistic regression analysis was performed to identify risk
factors that were associated with the development of postoperative atrial
fibrillation (Table25). Statistically significant differences were found for
Steroid Group and Age. (P=0.0006,0.0047 respectively). Other variables
showed no statistically significant differences (Table 26-31)
Risk Factor P-Value
Group 0.0006
Age 0.0047
History of MI 0.6745
History of asthma 0.6200
History ofCOPD 0.7296
History ofCITF 0.6441
Hypertension 0.2875
History of smoking 0.9106
L V EF 0.3227
Cross clamp Time 0.8323
By pass Time 0.5231
A-Pacing 0.7600
Table 25. Risk Factors by Multivariate Logistic Regression Analysis.
77

T a b l e o f a f by n i
a f n i
F r e q u e n c y l Row Pet •No • Ves • T o t a l
No I 21 1 34 • 55 I 38 .18 I 61 .82
Ves I 9 I 22 • 31 I 29 .03 • 70 .97 • .
T o t a l 30 56 86
C h i - S q u a r e : P = 0.3927
Table 26. Univariate analysis in Myocardial infarction between
NSR and AF Patients.
T a b l e o f a f by Chf
c h f
F r e q u e n c y ! Row Pet •No • V e s • T o t a l
No • 43 • 12 • 55 1 78 .18 • 21 .82 I
Ves • 23 • 8 1 31 • 74 -19 • 25 -81 •
T o t a l 66 20 86
C h i - S q u a r e : P = 0.6742
Table 27. Univariate analysis in Congestive Heart Failure between
NSR and AF patients.
78

Table of af by a p a c e
af a p a c e
Frequency! Row Pet INo IVes I Tota l
No 1 44 1' 11 1 55 I 80.00 1 20.00 1.
Ves 1 21 I 10 I 31 I 67.74 I 32.26 I
Tota l 65 21 86
Chi -Square: P = 0. 2039
Table 28. Univariate analysis in A-Pacing between NSR and AF
patients.
Table of af by aupace
af aupace
Frequency! Row Pet INo IVes I Tota l
No 1 50 1 5 1 55 I 90.91 1 9.09 I
Ves 1 28 I 3 1 31 1 90.32 1 9.68 I
Tota l 78 8 86
f i s h e r ' s Exact Tes t : P = 1. 0000
Table 29. Univariate analysis in AV-Pacing between NSR and AF
patients.
79

Table of af by COPD
af COPD
Frequencyl Row Pet •No • Ves I Total
No 1 44 1 11 I 55 I 80 .00 1 20 .00 I
Ves I 26 I 5 I 31 1 83 .87 I 16 .13 1
Total 70 16 86
Chi-Square: P = 0 .6578
Table 30. Univariate analysis in Chronic Obstructive Lung Disease
between NSR and AF patients.
The TTEST Procedure
S t a t i s t i c s
Lower CL Upper CL Lower CL Upper CL Uar iab le af N Mean Mean Mean Std Deu Std Deu Std Deu Std Er r Minimum Maximum
age No 55 60 098 62.771 65.443 8.3216 9.8847 12. 176 1.3329 39.389 82.957 age Ves 31 64 .177 67.516 70.856 7.2759 9.105 12 .17 1.6353 48.397 88.487
X_clamp_time Ho 55 56 .603 64.545 72.488 24.734 29.38 36. 191 3.9616 28 195 X c l a m p t i m e Ves 31 66 .696 76.645 86.595 21.676 27.125 36. 257 4.8718 29 136
Bypass_time No 55 81 .574 89.473 97.371 24.598 29.218 35. 992 3.9398 46 213 Bypass_time Ves 31 92 .231 101.13 110.03 19.386 24.259 32. 427 4.3571 45 158
T-Tests
Uariable t Ualue Pr > |t |
age -2.20 0.0307 Xclamptime -1.88 0.0630 Bypasstime -1.88 0.0630
Table 31. Univariate analysis in age, cross-clamp time, and bypass-time
between NSR and AF patients. From this table, statistically significant
difference was found in Age (P=0.0307)
80

Discussion
The use of prophylactic Short-Term Steroid Administration in patients
undergoing coronaray bypass grafting surgery reduced the incidence of
postoperative atrial fibrillation by approximately 50 percent. Due to
statistically significant difference in two patient characteristics, advancing
age and low ejection fraction in steroid group (p=0.007,0.035 respectively)
which are the risk factors of postoperative atrial fibrillation , the efficacy of
steroid may be stronger than we expect.
In our study, patients without postoperative atrial fibrillation had a
shorter length of hospital stay. Overall, there was no significant difference
between Steroid Group and Placebo Group with regard to the length of
hospital stay. Data showed that Steroid had higher complications which may
contribute to prolong hospitalization.
Although there was no statistically significant difference in
complication between Steroid Group and Placebo Group (P=0.0525), there
was a trend toward complications in Steroid Group as P-value was close to
0.05. In our study we found 4 patients had high glucose intolerance that need
to consult the endocrinologist to control blood sugar. Mayumi et al showed
that glucose intolerance was worsened by the steroid during cardiopulmonary
bypass (107). This might be the disadvantage of the Steroid Use.
Infection is another complication that we might concern during Steroid
Administration. In our study, we found infection in both group and no
statistically significant difference. White blood cell count was increased
significantly in Steroid Group (p<.0001) at 12,24-hour postoperative period.
81

However, we followed up white blood cell count 5 day postoperative and
found that the number of white blood cell count returned back to preoperative
level. This can be explained by demargination process of white blood cell
which could be effect from the steroid.
Many studies mentioned about the advantage of Steroid Use in Open-
heart surgery. Jansen et al showed that Steroid can inhibit TNF and LTB4
release, which is the primary mediators involved in reperfusion phenomenon
and sepsis. In his study, steroid improved postoperative course after
Cardiopulmonary bypass (99).Teoh et al found steroid decrease cytokines
release and decrease vasodilation effect (98). Engelman et al found the same
result and recommended prophylactic steroid use in open heart surgery (100).
We used the same dose that recommended by Engelman. This steroid doses
can maintain therapeutic steroid effects for 4 days, which covers the peak
incidence of postoperative atrial fibrillation. Engelman et al did not find any
adverse effects of steroid use, possibly due to small sample sizes (10 steroid
19 placebo) in his study. In our study, we had an opportunity to study
cytokine in some of our patient due to limited research funding. Walley KR.
and Macintyre L. analysed the cytokine level in 22 of Steroid group and 86 of
Placebo group. The results showed IL6 at 4,24-hour postoperative period in
steroid group were statistically significant different (p=0.041,p=0.014
respectively). This showed the same result as other studies.
The median of length of hospital stay of A F patient was 8 days compare
with 6 days in NSR patient (p=0.002). However, the median length of
hospital stay of steroid group was 6 days and in Placebo group was 7 days
(p=0.337). This might be explained by increased length of hospital stay in
82

steroid group. We found that two Major complication patients in steroid
group had 30 and 32 days length of hospital stay, and this was significant
difference between complication and non-complication patient (p=0.0004).
In our study, only advancing age has consistently been associated with
an increased risk of postoperative atrial fibrillation (p=0.030). Creswell L L
found Chronic obstructive lung disease and cross clamp time are the risk
factors for the development of postoperative atrial fibrillation, this might be
from our small sample sizes (86 compared with 4507 patients).
In conclusion, with the high efficacy of steroid in decreasing the
posoperative atrial fibrillation and slightly increasing in complications, we
might try to adjust the steroid dose; for example give half dose of
Methylprednisolone (500mg as we usually give in heart transplant patient).
Or we can use prophylactic steroid for the patients who are high-risk of
development of postoperative atrial fibrillation, such as old-age patients, long
cross clamp time operation, low Ejection fraction patient, COPD patients,
preoperative use of digoxin, valvular patients. Or we can select to use
prophylactic steroid with patients who are not diabetes. Subsequently, we can
design other studies about prophylactic steroid administration in
postoperative atrial fibrillation ; for instance, high Vs low dose steroid use,
Steroid in high risk AF patient, Steroid combined with beta-blocker , Steroid
combined with amiodarone, Steroid with biatrial pacing. Hopefully one day
we can find the best prevention for postoperative atrial fibrillation.
83
References
1. Favaloro RG, Effler DB, Groves L K , et al: Direct myocardial
revascularization with saphenous vein autograft. Dis Chest 56:279-283,
1969.
2. Goldman L: Supraventricular tachyarrhythmias in hospitalized adults
after surgery. Chest 73:450-454, 1978.
3. Johnston K W . Multicenter prospective study of nonruptured abdominal
aortic aneurysm. J Vase Surg 9:437-447, 1989.
4. Nielsen JB, Sorensen HR, Alstrup P: Atrial fibrillation following
thoracotomy for non-cardiac diseases, in particular cancer of the lung.
Acta MedScand 193:425-429, 1973.
5. Lauer MS, Eagle K A , Buckley MJ, et al: Atrial fibrillation following
coronary artery bypass surgery. Prog Cardiovasc Dis 16:367-378,
1989.
6. Asher CR, Chung M K , Grimm RA, et al: Is the incidence of
postoperative atrial fibrillation following cardiac valve surgery reduced
by minimally invasive surgery (abstract). Circulation 94:651, 1996.
7. Aranki SF, Shaw DP, Adams DH, et al: Predictors of atrial fibrillation
after coronary artery surgery: Current trends and impact on hospital
resources. Circulation 94:390-397, 1996.
84

8. Matthew JP, Parks R, Savino JS, et al: Atrial fibrillation following
coronary artery bypass graft surgery: Predictors, outcomes, and
resource utilization. JAMA 276:300-306, 1996.
9. Andrew TC, Reimold SC, Berlin JA, et al: Prevention of
supraventricular arrhythmias after coronary artery bypass surgery.
Circulation 84:236-244,1991 (suppl'3)
10. Cox JL: A perspective of postoperative atrial fibrillation in cardiac
opearation. Ann Thorac Surg 56:405-409, 1993
11. Creswell L L , Schuessler RB, Rosenbloom M , et al: Hazards of
postoperative atrial fibrillation. Ann Thorac Surg 56:539-549,1993
12. Cox JL: A perspective on postoperative atrial fibrillation. Semin
Thorac cardiaovasc Surg 11:299-302,1999
13. Fuller JA, Adams GG, Buxton B: Atrial fibrillation after coronary
artery bypass grafting: Is it a disorder of the elderly? J Thorac
Cardiovasc Surg 97:821-825, 1989.
14. Moe GK: On the multiple wavelet hypothesis of atrial fibrillation. Arch
Int Pharmacodyn Ther 140:183-188, 1962.
15. Konings K , Kirchof CJJ, Smeets JRLM, et al: High density mapping of
electrically induced atrial fibrillation in humans. Circulation 89:1665-
1680, 1994.
16. Pool DP, Lee HL, Nadzam G, et al: Cardiac surgery results in changes
of atrial refractoriness that may explain vulnerability to postoperative
atrial fibrillation (abstract). J Am Coll Cordiol 27:64 65, 1995.
85

17. Chung M K , Pool DP, Leo HL, et al: Atrial conduction latency predicts
occurrence of postoperative atrial fibrillation in patients undergoing
bypass surgery (abstract). J Am Coll Cordiol 27:65A, 1995.
18. Augostini RS, Pool DP, Leo HL, et al: Sinus node function after
cardiopulmonary bypass predicts the development of postoperative
atrial fibrillation (abstract). Circulation 92:141, 1995.
19.Sato S, Yamauchi S, Schuessler RB, et al: The effect of augmented
atrial hypothermia on atrial refractory period, conduction, and atrial
flutter/fibrillation in the canine heart. J Thorac Cardiovasc Surg
104:297-306, 1992.
20. Buxton A E , Josephson M E : The role of P wave duration as a predictor
of postoperative atrial arrhythmias. Chest 80:68-73, 1981.
21. Hutchinson L A , Ehlert FA, Menchavez Tan E, et al: Towards a better
understanding of the development of atrial fibrillation after cardiac
surgery: Risk factor analysis in a large prospective study (abstract). J
Am Coll Cardiol 27:318A, 1995.
22. Cox Jl, Sabiston DC Jr: Electrophysiologic consequences of
cardioplegic preservation, Ischemia and Reperfusion, in Engelman R M :
A textbook of clinical cardioplegia. New york, Futura publishing,
1982,406-417.
23.Smith PK, Buhrman WC, Levett JM, et al: Supraventricular conduction
abnormalities following cardiac operations: A complication of
inadequate atrial preservation. J Thorac Cardiovasc Surg 85:105,1983
86

24.Smith PK, Buhrman WC, Ferguson TB Jr, et al: Conduction block after
cardioplegia arrest: Prevention by augmented atrial hypothermia.
Circulation 68:1141-1148, 1983
25. Ferguson TB Jr, Smith PK, Buhrman WC, et al: Monitoring of the
electrical status of the ventricle during cardioplegic arrest.
Circulation6S:ll27-ll33, 1983
26. Ferguson TB Jr, Smith PK, Buhrman WC, et al: Studies on the
physiology of the conduction system during hyperkalemia,
hypothermic cardioplegic arrest. Surg Forum 39:302,1983
27.Smith PK, Buhrman WC, Ferguson TB Jr et al: Relationship of atrial
hypothermia and cardioplegic solution potassium concentration to
postoperative conduction defects. Surg Forum 34:304,1983
28. Ferguson TB Jr, Damiano RJ, Smith PK, et al: The electrophysiological
effects of calcium channel blockade during standard hyperkalemic
hypothermic cardioplegic arrest. Ann Thorac Swrg 41:622-629,1986
29. Ferguson TB Jr, Smith PK, Lofland PK, et al: The effects of
cardioplegic potassium concentration and myocardial temperature on
electrical activity in the heart during elective cardioplegic arrest. J
Thorac Cardiovasc Surg 92:755-765,1986
30. Ferguson TB Jr, Smith Ls, Smith PK, et al: Electrical activity in the
heart during hyperkalemic hypothermic cardioplegic arrest: Site of
origin and relationship to specialized conduction tissue. Ann Thorac
Surg 43:373-379,1987
87

31. Kyosola A U , Mattila K, Harjula T, et al: Life threatening complications
of cardiac operations and occurrence of myocardial catecholamine
bombs. J Thorac Cardiovasc Surg 95:334-339, 1988.
32. Engelman R M , Haag,B, Lemeshow S, et al: Mechanism of plasma
catecholamine increases during coronary artery bypass and valve
procedures. J Thorac Cardiovasc Surg 86:608-615, 1983.
33. Page P, Plumb VJ , Okumura K, et al: A new model of atrial flutter. J
Am Coll Cardiol 8:872-879, 1986.
34. Angelini GD, Penny WJ, El Ghamary F, et al: The incidence and
significance of early pericardial effusion after open heart surgery. Eur J
Car diothorac Surg 1:165-168, 1987.
35. Weitzman L B , Tinker WP, Kronzon 1, et al: The incidence and natural
history of pericardial effusion after cardiac surgery: An
echocardiographic study. Circulation 69:506-511, 1984.
36. Creswell L L : Postoperative atrial arrhythmias: Risk Factors and
Associated adverse outcomes. Semin Thorac Caardiovasc Surg 11:303-
307,1999
37.0mmen SR, Odell JA, Stanton MS: Atrial arrhythmias after
cardiothoracic surgery. N Engl J Med 336:1429-1434,1997
38. Hashimoto K, Ilstrup D M , Schaff HV:Influence of clinical and
hemodynamic variables on risk of supraventricular tachycardia after
coronary artery bypass. J Thorac Cardiovasc Surg 101:56-65,1991
39. Leitch JW, Thomson D, Baird DK, et al: The importance of age as a
predictor of atrial fibrillation and flutter after coronary artery bypass
grafting. J Thorac Cardiovasc Surg 100:338-342, 1990.
88

40. Creswell L L , Schuessler RB, Rosenbloom M , et al: Hazards of
postoperative atrial arrhythmias. Ann Thorac Surg 56:539-549, 1993.
41. Frost L , Molgaard H, Christiansen EH, et al: Atrial fibrillation and
flutter after coronary artery bypass surgery: Epidemiology, risk factors
and preventive trials. Int J Cardiol 36:253-261, 1992.
42. Kannel WB, Abbott RD, Savage DD, et al: Epidemiologic features of
chronic atrial fibrillation: The Framingham Study, N Engl J Med
206:1018 1022, 1982.
43. Crosby L H , Pifalo WB, Woll KR, et al: Risk factors for atrial
fibrillation after coronary artery bypass grafting. Am J Cardiol 66:1520
1522, 1990.
44.0merod O M , McGregor CA, Stone DL, et al: Arrhythmias after
coronary bypass surgery. Br Heart J 51:618-621, 1984.
45. Dixon FE, Genton E, Vacek JL, et al: Factors predisposing to
supraventricular tachyarrhythmias after coronary artery bypass grafting.
Am J Cardiol 58:476-478, 1986.
46. Butler J, Chong JL, Rocker G M , et al: Atrial fibrillation after coronary
artery bypass grafting: A comparison of cardioplegia versus
intermittent aortic cross clamping. Eur J Cardiothorac Surg 7:23-25,
1983.
47. Pattison C, Dimitri WR, Williams BT: Dysrhythmias following
coronary artery surgery: A comparison between cold cardioplegic and
intermittent ischaemic arrest (32 C) with the effect of right coronary
artery endarterectomy. J Cardiovasc Surg 29:601-605, 1988.
89

48. Muller JC, Khan N , Weisel RD, et al: Atrial activity during
cardioplegia and postoperative arrhythmias. J Thorac Cardiovasc Surg
94:558-565, 1987.
49. Cheung EH, Arcidi JM, Jackson ER, et al: Intracavitary right heart
cooling during coronary bypass surgery, a prospective randomized
trial. Circulation 78:1735-1795, 1988.
50. Bigger JT Jr, Bloomfield D M , Rottman JN, et al: Frequent pre
operative atrial premature complexes predicts atrial fibrillation after
C A B G surgery (abstract). Circulation 94:191, 1996.
51 .Falk RH: Etiology and complications of atrial fibrillation: Insight from
pathology studies. Am J Cardiol 82:10N-17N, 1998.
52. Wolman M : Lipid pigments (chromolipids): Their origin, nature, and
significance. Pathobiol Annu 10:253-267, 1980.
53. Cotran RS, Kumar V, Collins T: Cell injury and cell death, in Robbins
Pathologic Basis of Disease (ed 6). Philadelphia, Saunders, 1999,pp 1-
29.
54. Brunk UT, Jones CB, Sohal RS: A novel hypothesis of
lipofuscinogenesis and cellular aging based on interactions between
oxidative stress and autophagocytosis. Mutat Res 275:395-403, 1992.
55.Islam M N , Kuroki H, Hongcheng B, Ogura Y , Kawaguchi N , Onishi S,
Wakasugi C: Cardiac lesions and their reversibility after long term
administration of methamphetamine. Forensic Sci Int 75:29-43, 1995.
56.Maes A, Flameng W, Nuyts J, Borgers M , Shivalkar B, Ausma J,
Bormans G, et al: Histological alterations in chronically hypoperfused
90

myocardium. Correlation with PET findings. Circulation 90:735-745,
1994.
57. A d N , Snir E, Vinde B A , et al: Potential preoperative markers for the
risk of developing atrial fibrillation after cardiac surgery. Semin Thorac
Cardiovasc Surg 11:308-313,1999.
58. Pirolo JS, Hutchins G M , Moore GW: Myocyte vacuolization in infarct
border zones is reversible. Am J Pathol 121:444-450, 1985.
59.Salerno TA, Wasan SM, Charrette EJ: Prospective analysis of heart
biopsies in coronary artery surgery. Ann Thorac Surg 28:436-439,
1979.
60. Mambo NC, Silver MD, McLaughlin PR, Huckell VF, McEwan P M ,
Britt B A , Morch JE: Malignant hyperthermia susceptibility. A light and
electron microscopic study of endomyocardial biopsy specimens from
nine patients. Hum Pathol 11:381-388, 1980.
61. Matangi MF, Neutze JM, Grahm KJ , et al: Arrhythmia prophylaxis
after aorta coronary bypass: The effect of minidose propranolol. J
Thorac Cardiovasc Surg 89:439 443, 1985.
62. Martinussen HJ, Lolk A, Szczepanski C, et al: Supraventricular
tachyarrhythmias after coronary bypass surgery: A double blind
randomized trial of prophylactic low dose propranolol. Thorac
Cardiovasc Surg 36:206 207, 1988.
63. Khuri. SF, Okike ON, Josa M , et al: Efficacy of nadolol in preventing
supraventricular tachycardia after coronary artery bypass grafting. Am J
Cardiol 60:5ID 58D, 1987.
91

64. Andrews TC, Reimold SC, Berlin JA, et al: Prevention of
supraventricular arrhythmias after coronary artery bypass surgery: A
metaanalysis of randomized control trials. Circulation 84:2365
2445,1991.
65. Kowey PR, Taylor JE, Rials SJ, et al: Meta analysis of the effectiveness
of prophylactic drug therapy in preventing supraventricular arrhythmia
early after coronary artery bypass grafting. Am J Cardiol 69:863865,
1992.
66. Johnson LW, Dickstein RA, Fruehan CT, et al: Prophylactic
digitalization for coronary artery bypass surgery. Circulation 53:819
822, 1976.
67. Tyras DH, Stothert JC, Kaiser GC, et al: Supraventricular
tachyarrhythmias after myocardial revascualrization: A randomized
trial of prophylactic digitalization. J Thorac Cardiovasc Surg 77:310
313, 1979.
68. Davison R, Hartz R, Kaplan K, et al: Prophylaxis of supraventricular
tachyarrhythmia after coronary bypass surgery with oral verapamil: A
randomized double blind trial. Ann Thorac Surg 39:336 339, 1985.
69.Smith EJ, Shore DF Monro JL, et al: Oral verapamil fails to prevent
supraventricular tachycardia following coronary artery surgery. Int J
Cardiol 9:37 44, 1985.
70.Seitelberger R, Hannes W, Gleichauf M , et al: Effects of diltiazem on
perioperative ischemia, arrhythmias, and myocardial function in
patients undergoing elective coronary bypass grafting. J Thorac
Cardiovasc Surg 107:811 821, 1994.
92

71. Fanning WJ, Thomas CS, Roach A, et al: Prophylaxis of atrial
fibrillation with magnesium sulfate after coronary artery bypass
grafting. Ann Thorac Surg 52:529 533, 1991.
72. Parikka H, Toivonen L , Pellinen T et al: The influence of intravenous
magnesium sulphate on the occurrence of atrial fibrillation after
coronary artery bypass operation. Eur Heart J 14:251 258, 1993.
73. Daoud EG, Strickberger SA, Man K C , et al: Preoperative amiodarone
as prophylaxis against atrial fibrillation after heart surgery. TV Engl J
Med?,?,!: 1785-1791, 1997.
74. Guarnieri T, Nolan S, Gottlieb SO, et al: Intravenous amiodarone for
the prevention of atrial fibrillation after open heart surgery: the
amiodarone reduction in coronary heart (ARCH) trial. J Am Coll
Cardiol 34:343-347, 1999.
75. Gold MR, O'Gara PT, Buckley MJ, et al: Efficacy and safety of
procainamide in preventing arrhythmias after coronary artery bypass
surgery. Am J Cardiol 78:975 979, 1996.
76. McCarty RJ, Jahnke EJ, Walker WJ: Ineffectiveness of quinidine in
preventing atrial fibrillation following mitral valvotomy . Circulation
34:792-794, 1996.
77. Merrick AF , Odom NJ, Keenan DJ, et al: Comparison of propafenone
to atenolol for the prophylaxis of postcardiotomy supraventricular
tachyarrhythmias: A prospective trial. Eur J Cardiothorac Surg 9:146-
149, 1995.
78.Solomon AJ , Verdino RJ, Katz NM:Dual site atrial pacing in
cardiovascular surgical patients. Circulation 94:1-677, 1996(abstr).
93

79. Gerstenfeld EP, Hil l MRS, French SN, et al: Evaluation of right atrial
and biatrial temporary pacing for the prevention of atrial fibrillation
after coronary artery bypass surgery. J Am Coll Cardiol 33:1981-1988,
1999.
80. Greenberg M D , Katz N M , Tempesta BJ, et al: Atrial pacing following
cardiovascular surgery reduces the incidence of postoperative atrial
fibrillation. Circulation 98:1-509, 1998(abstr)
81.Saksena S, Prakash A, Hil l M , et al: Prevention of recurrent atrial
fibrillation with chronic dual-site right atrial pacing. J AM Coll Cardiol
28:687-694, 1996.
82. Chung M K , Augostini RS, Asher CR, et al: A randomized controlled
study of atrial overdrive pacing for the prevention of atrial fibrillation
after coronary bypass surgery (abstract). Circulation 69:188, 1996.
83. Butler J, Rocker G M , Westaby S: Inflammatory response to
cardiopulmonary bypass. The Ann Thorac Surg 55:552-9,1993
84. Kirklin JK: Prospects for understanding and eliminating the deleterious
effects of cardiopulmonary bypass. The Ann Thorac Surg 51:529-
31,1991
85. Cleland J, Pluth JR, Tauxe WN, Kirklin JW. Blood volume and body
fluid compartment changes soon after closed and open intracardiac
surgery. J Thorac Cardiovasc Surg 1966;52:698-705.
86.Smith EEJ, Naftel DC, Blackstone EH, Kirklin JW. Microvascular
permeability after cardiopulmonary bypass. J Thorac Cardiovasc Surg
1987;94:225-33.
94

87. Kirklin JK. The postperfusion syndrome: inflammation and the
damaging effects of cardiopulmonary bypass. In: John Tinker, ed.
Cardiopulmonary bypass current concepts and controversies.
Monograph. Philadelphia: W.B. Saunders,1989:131-46.
88. Chenoweth DE, Cooper SW, Hugley TE, et al. Complement activation
during cardiopulmanory bypass: evidence for generation of C3a and
C5a anaphylatoxins. N Engl J Med 1981;304:497-503.
89. Kirklin JK, westaby S, Blackson EH, Kirklin JW, Chenoweth DE,
Pacifico A D . Complement and the damaging effects of
cardiopulmonary bypass. J Thorac Cardiovasc Surg 1983;86:845-57.
90. Chenoweth DE, Hugh TE. Demonstration of specific C5a receptor on
intact human polymorphonuclear leukocytes Proc Natl Acad Sci USA
1978;75:3943-7.
91.Salama A, Hugo F, Heinrich D, et al. Deposition of terminal C5b-9
complement complexes on erythrocytes and leukocytes during
cardiopulmonary bypass. N Engl J Med 1988;318:408-13/
92. Craddock PR, Fehr J, Brigham K L , et al. Complement and leukocyte-
mediated pulmonary dysfunction in hemodialysis. N Engl J Med
1977;296:769-7'4.
93. Craddock PR, Fehr J, Dalmasso AP, et al. Pulmonary vascular
leukostasis resulting from complement activation by dialyzer
cellophane membranes. J Clin Invest 1977;59:879-88.
94. Flick MR, Perel A , Staub NC. Leukocytes are required for increased
lung microvascular permeability after microembolization in sheep. Circ
Res 1981;48:344.

95. Gu Y J , Wang YS, Chiang B Y , Gao X D , Ye C X , Wildevuur CRH.
Membrane oxygenator prevents lung reperfusion injury in canine
cardiopulmonary bypass. Ann Thorac Surg 1991;51:573-8.
96. Rinaldo JE, Rodgers R. Adult respiratory distress syndrome:changing
concepts of lung injury and repair. TV Engl JMed 1982;396:900-9.
97. Hammerschmidt DE, Stroncek DF, Bowers TK, et al. Complement
activation and neutropenia during cardiopulmonary bypass. J Thorac
Cardiovasc Surg 1981;81:370-7.
98. Teoh KHT, Bradley CA, Gauldie J; Steroid Inhibition of Cytokine-
Mediated Vasodilation After Warm Heart
Surgery.Circulation. 1995;92(Suppl II):II-347-II-353.)
99. Jansen NJG, Oeveren WV, Broek L V D , Inhibition by dexamethasone
of the reperfusion phenomena in cardiopulmonary bypass.J Thorac
Cardiovasc Surg 102:515-25,1991.
100. Engelman R M , Rousou JA, Flack JE; Influence of Steroids on
Complement and Cytokine Generation After Cardiopulmonary Bypass.
Ann Thorac Surg 60:801-4, 1995.
101. Lodge AJ , Chai PJ, Daggett CW; Methylprednisolone reduces the
inflammatory response to cardiopulmonary bypass in neonatal piglets../
Thorac Cardiovasc SurgMl:515-22, 1999.
102. HH1 GE, Alonso A , Spurzem JR, Stammers A H , Robbins RA.
Aprotinin and methylprednisolone equally blunt cardiopulmonary
bypass-induced inflammation in humans. J Thorac Cardiovasc
110:1658-62, 1995.
96

103. Hi l l GE, Alonso A, Thiele G M , Robbins RA. Glucocorticoids blunt
neutrophil C D l l b surface glycoprotein upregulation during
cardiopulmonary bypass in humans. Anesth Analg 79:23-7, 1994.
104. Jansen NJ, van Oeveren W, van Vliet M , Stoutenbeek CP, Eysman L,
Wildevuur CR. The role of different types of corticosteroids on the
inflammatory mediators in cardiopulmonary bypass. Eur J
Cardiothorac Surg 5:211-7, 1991.
105. Jorens PG, De Jongh R, De Backer W, Van Damme J, Van Overveld
F, Bossaert L, et al. Interleukin-8 production in patients undergoing
cardiopulmonary bypass: the influence of pretreatment with
methylprednisolone. Am Rev Respir Dis 148:890-5, 1993.
106. Kawamura T, Inada K, Okada H, Okada K, Wakusawa R.
Methylprednisolone inhibits increase of interleukin 8 and 6 during
open heart surgery. Can J Anaesth 42:399-403, 1995.
107. Mayumi H, Zhang QW, Nakashima A. Synergistic
immunosuppression caused by high-dose methylprednisolone and
cardiopulmonary bypass. Ann Thorac surg 63;129-37,1997.
97