Favourite Immune Cell Assignment: Mast Cell
17
Favourite Immune Cell Assignment BIOL 4931 – Immunology Samantha Bray December 1 st , 2015 Q1-1: What is your favourite cell of the immune system? The mast cell is my favourite cell of the innate immune system. Q1-2: In what organ(s) do you find these cells? Mast cells can be found in most tissues because they circulate in the blood stream and distribute through the body. They are found in abundance in areas susceptible to pathogens from the external environment such as the skin, gastrointestinal tract and lungs. 1 Q1-3: Find a micrograph of your cell and label its cell structures. Figure 1. Mast cell electron micrograph. 2 Q2-1: How does your favourite cell interact with the human microbiome? If the bacteria in the human microbiome become pathogenic mast cells act to kill them. To kill pathogenic microbes mast cells use produce reactive oxygen species and/or antimicrobial peptides. Another common method used by mast cells to kill pathogenic microbes is engulfing the microbe through phagocytosis. 1 Q2-2: Has your favourite cell been implicated in dysbiosis? Yes, mast cells are involved when bacteria enter a state of dysbiosis. When normally benign microbes proliferate to levels that become pathogenic mast cells traffic to the area infected via the circulatory system and releases granules and cytokines that act to kill the pathogenic microbes. 1
-
Upload
samantha-bray -
Category
Science
-
view
79 -
download
0
Transcript of Favourite Immune Cell Assignment: Mast Cell

Favourite Immune Cell Assignment
BIOL 4931 – Immunology
Samantha Bray
December 1st, 2015
Q1-1: What is your favourite cell of the immune system?
The mast cell is my favourite cell of the innate immune system.
Q1-2: In what organ(s) do you find these cells?
Mast cells can be found in most tissues because they circulate in the blood stream and
distribute through the body. They are found in abundance in areas susceptible to pathogens from
the external environment such as the skin, gastrointestinal tract and lungs.1
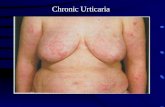
Q1-3: Find a micrograph of your cell and label its cell structures.
Figure 1. Mast cell electron micrograph.2
Q2-1: How does your favourite cell interact with the human microbiome?
If the bacteria in the human microbiome become pathogenic mast cells act to kill them.
To kill pathogenic microbes mast cells use produce reactive oxygen species and/or antimicrobial
peptides. Another common method used by mast cells to kill pathogenic microbes is engulfing
the microbe through phagocytosis.1
Q2-2: Has your favourite cell been implicated in dysbiosis?
Yes, mast cells are involved when bacteria enter a state of dysbiosis. When normally
benign microbes proliferate to levels that become pathogenic mast cells traffic to the area
infected via the circulatory system and releases granules and cytokines that act to kill the
pathogenic microbes.1

Q2-3: Can your immune cell respond to antigens?
Mast cells have high affinity IgE receptors on their surface that when stimulated by
antigens bound to IgE causes the cell to degranulate emptying histamine, heparin, other enzymes,
and cytokines that attract other immune cells (leukocytes, macrophages) to the site of infection in
order to combat/kill pathogen in the site of infection.1
Q3-1: From what HSC lineage is your favourite cell derived?
Mast cells are from the myeloid lineage of hematopoietic stem cells.3
Q3-2: In what location does the ultimate differentiation of your favourite cell occur?
Mast cells are made in the bone marrow and leave as undifferentiated cells. They travel
through the blood to a tissue where they will differentiate and then reside as mature mast cells.3
Q3-3: Using http://web.expasy.org/cellosaurus/ (or similar resource), find a human cell line
representative of your favourite cell type.
Figure 2. Human mast cell 1 cell line.4
Q4-1: What innate immune sensors are expressed in your favourite cell?
Mast cells express high amounts of high-affinity IgE receptors on their surface. This
receptor binds IgE class antibodies that trigger the cell to degranulate and contributes to allergic
reaction.5 They express TLRs 1-9 that detects intracellular or extracellular pathogens usually of
bacterial or viral origin.6
Q4-2: Does your cell express MHC molecules?
Yes, mast cells express MHC class I and class II molecules on their cell surface that
present antigenic peptide.6
Q4-3: Does your cell interact with the BcR or TcR complex?

Yes, studies have shown that mast cells are able to present antigenic peptide to TcR
complex on T cells. They are able to induce clonal expansion of T cells and migration of T cells
to the lymph nodes to induce an immune response.6
Q5-1: Does your favourite cell interact with DCs?
Mast cells indirectly interact with dendritic cells by releasing cytokines that regulate
dendritic cell migration, maturation and activation. Mast cells release TNF that causes the up
regulation of MHC class II, CD80, CD86 and CD40 on the cell surface facilitating functional
maturation. They also release IL-1, IL-16, IL-18 and CCL5, which promote the migration of
dendritic cells.6 In more recent examples, DC and mast cells have shown direct cell to cell
interactions that last for minutes. Broadly speaking, mast cells and DCs form synapses using the
integrin protein. The synapse then facilitates passage of internalized mast cell antigen to DCs that
then present the antigen on their surface leading to the activation of T cells.7
Q5-2: Is co-stimulation involved in the activation of your favourite cell?
Mast cells express the FcεRI-IgE and the c=Kit (CD117) receptors. When FcεRI and KIT
receptors are co stimulated by antigen the mast cells are triggered to release their granules,
produce more cytokines and promotes cytokine mRNA synthesis. Mast cells can also be co-
stimulated by TLRs, NLRs, CLRs. For example, TLR-2 and TLR-4 signaling combines with
FcεRI receptor signaling to enhance the release of granules and mediators.8 Additionally, C3a
and C5a through the C3aR and C5aR (CD88) can activate mast cells. Mast cells can also be
activated by nerve growth factors such as TRKA, and by IgG through the FcγRI. The co
stimulation of all these receptors determines the extent and pattern of the immune response
produced by mast cell.9
Q5-3: Is your cell’s function influenced by CD4+ T cells.
Yes, CD4+ T cells influence mast cells degranulation. Specifically, CD4+ CD25+ T
regulatory cells influence mast cell degranulation. These T regulatory cells have OX40 receptors
that bind to mast cells OX40 ligand. Through these interactions T regulatory cells cause increased
levels of cAMP and decreased calcium influx inhibiting mast cell degranulation. When
researchers antagonized cAMP allowing the levels to decrease, calcium levels returned to normal
allowing the mast cell to degranulate.10
Q6-1: Does your favourite cell form MTOCs?
Yes, mast cells do form MTOCs. Mast cells use MTOCs for granule secretion. Upon
stimulation of mast cell IgE receptors intracellular calcium levels rise. Syt, a lysosomal sensor,
detects calcium rise and initiates granule mobilization towards the MTOC. From the MTOC, the
granule attaches to kinesin, a motor protein, and moves along the microtubule towards the cells
plasma membrane. It then detaches and fuses with the membrane releasing the granule that
contains histamine, heparin, and serotonin.11
Q6-2: What are the major signalling cascades initiated when your cell is activated?
The major signalling cascade initiates when the mast cell FcεRI (IgE receptor) becomes
activated. Upon IgE binding to FcεRI tyrosine kinases FYN LYN and SYK phosphorylate
NTAL. Through downstream signaling events NTAL activates PI3K that activates both PLCγ

and S1P which both act to mobilize calcium. NTAL also causes activation of MAPK pathway.
The MAPK pathway, P13K, as well as the mobilization of calcium signaling all integrate and
cause the mast cell to degranulate.12
Q7-1: What cytokines are produced by your favourite cell of the immune system?
Mast cells produce many cytokines IL-6, IL-8, TNF, IFNγ, VEGF, MCP-1, etc. They
produce TNF in response to TLR-4 activation by bacterial LPS. LPS can also trigger release of
IL-5, IL-10, and IL-13. Mast cells can also produce IFN in response to double stranded viral
RNA activating TLR-3.13
Q7-2: What cytokines receptors are expressed by your favourite cell of the immune system?
Mast cells may express cytokine receptors IL-3R, IL-4R, IL-5R, IL-9R, IL-10R, IFN-γR.
These cytokine receptors modulate mast cells immune response. For example, IL-4 up regulates
the expression of FcεRI on mast cell surface. IL-5 causes the proliferation of mast cells (in the
presence of SCF), and IFN-γ down regulates the population of mast cells.14
Q7-3: What chemokines attract or repulse your favourite cell of the immune system?
Mast cells are attracted to chemokines that are chemoattractants. They move towards
chemokines CCL2, CCL5 and when exposed to antigen display enhanced migration towards
chemokines CXCL4 and CCL3.15
Q7-4: What chemokine receptors are expressed by your favourite cell of the immune
system?
Mast cells express of different tissue origin are able to express up to 9 different
chemokine receptors, CXCR1, CXCR2, CXCR3, CXCR4, CX3CR1, CCR1, CCR3, CCR4 and
CCR5. Mast cells have unique arrangement of CCR3, CXCR1 and CXCR2 on intracellular
cytoplasmic membranes. When mast cells become activated, CCR3 expression is upregulated on
the cell surface.16
Q8-1: Does your favourite cell of the immune system ever reside in the bone marrow?
Mast cells are made in the bone marrow and leave as undifferentiated cells. They travel
through the blood to a tissue where they will differentiate and then reside as mature mast cells.3
They do not however typically do not reside in the bone marrow as mature mast cells. When
mature mast cells do accumulate in the bone marrow it is abnormal and is usually associated with
a disease called bone marrow mastocytosis that is associated with symptoms like pruritus,
nausea, vomiting, diarrhea, and vascular instability.17
Q8-2: Does your favourite cell of the immune system ever reside in the thymus?
Yes, mast cells are normal residents of the thymus and are usually found in the connective
tissue septa. Mast cells are rare in the cortex of the thymus and also some found in the medulla
and the lobules. In people that have myasthenia gravis intralobular mast cell density of 6.5
increased to an intralobular mast cell density of 21.5 and is associated with an increase in thymic
microvessels due to mast cell secretion of angiogenic growth factors.18

Q8-3: Does your favourite cell undergo a positive or negative selection process?
Due to exhaustive literature research to date generally mast cells do not undergo a
positive or negative selection process. Generally speaking they likely would not undergo a
selection process because they do not bind antigen with TcR receptors or BcR receptors. If they
did have these receptors they might undergo a selection process to ensure their receptors do not
bind self-antigen, or bind MHC-antigen complexes too strong.19
Q9-1: Does your favourite cell of the immune system traffic to lymph nodes?
Yes mast cells do migrate to the lymph nodes. In research done by Wang et al. mice were
exposed to DNFB to induce a hypersensitivity reaction. At 24 hours 77% of mast cells de-
granulated. During DNFB sensitization the density of mast cells in the skin by approximately
50%, and mast cell density in the draining lymph nodes. To see if these mast cells were migrating
to the lymph nodes the researchers then fluorescently labelled mast cells then injected them into
the skin of the mice. Next the researchers subjected these mice to DNFB sensitization and found
that the fluorescently labelled mast cells migrated from the injection point to the draining lymph
node, then eventually migrating to the spleen. They believed that mast cells migrate from the site
of antigen encounter (DNFB) to the lymph nodes where they recruit T lymphocytes.20
Q9-2: Does your favourite cell interact with MALT?
Mast cells are part of the make up of MALT. During chronic inflammation the (mucosal)
gut associated lymphoid tissue undergoes mast cell hyperplasia. The accumulation of
extraordinary numbers of mast cells in the lamina propria and epithelium of the intestinal GALT
play a critical role in protective immunity against microbes and pathogens.21
Q10-1: Find an intravital microscopy video of your favourite cell of the immune system.
Describe the model system and what your cell is doing in that tissue.
Unfortunately I was unable to find a video the only one that I could find required paid
access. In a documented study without with the model system requires intravital microscopy of a
hamster cheek pouch for studies of microvascular dynamics of mast cell degranulation (histamine
release) when mast cells are activated. They introduced antigen to the hamster’s cheek to cause
an inflammatory reaction. In the model the mast cell degranulates and causes an influx of
leukocytes.22
Q11-1: Find an example of a pathogen immune evasion strategy against a PRR signalling
cascade. Describe in a short paragraph the significance of this host-pathogen interaction.
Host cell RNA fragments are not detected by RLRs because they are usually capped.
Some RNA viruses mimic these host cell structures as an immune evasion mechanism. They can
acquire their capped structures using host cell mRNA processing, can steal cap structure from
host mRNA fragments (e.g. influenza A virus), or they can encode their own capping enzymes
(e.g. poxviridae). With the viral genome capped and unrecognizable by the RLRs, RIG-I and
MDA5 cannot activate their downstream signalling molecules that activate IRF3, IRF7 and
NFκB. Thus, avoiding activation of Type 1 Interferon antiviral pathway.23

Q11-2: Find an example of a pathogen immune evasion strategy against a pathogen
restriction factor. Describe in a short paragraph the significance of this host-pathogen
interaction.
HIV-1 encodes viral infectivity protein (Vif) protein. HIV Vif-Cul5 E3 ubiquitin ligase
complex forms and induces the polyubiquitination of APOBEC3G. The ubiquitin tags the
APOBEC3G for proteosomal degradation. By inducing the degradation of APOBEC3G HIV-1
avoids their antiviral mechanisms such as inhibiting reverse transcription. They do this by
inducing mutations into newly synthesized negative strand DNA’s. This can prevent the
transcription of the plus strand viral genome and can even target the viral DNA for degradation.
APOBEC3G also inhibits reverse transcription by inhibiting reverse transcription DNA
elongation, as well as reverse transcription strand switching capabilities. Since HIVs Vif protein
thus allows HIV virions to be packaged without host cell APOBEC3G aboard and allowing the
virus to go forth and infect other cells successfully.24
Q12-1: Describe the type I IFN-driven anti-viral state within your favourite cell.
Interferon α and β has been shown to inhibit histamine release by mast cells in a dose
dependent manner.25 Human nasal mucosal mast cells secrete TNF-α that activates neighbouring
mast cell histamine release. IFN-α is able to inhibit mast cells release of TNF-α and thus inhibits
histamine release.26 Furthermore another study suggests that mast cells respond to IFN-α with a
decrease in TNF-α production but an increase in IL-10 and TGF-β production. Additionally the
study showed IFN-α down regulated the expression of the OX40 ligand on the mast cell surface
that is necessary for mast cell-T cell interactions therefore lowering levels of proliferating CD4+
T cells. Overall, it appears as if Type I IFNs suppress mast cell anti-viral defenses.27
Q12-2: How does your favourite cell contribute towards inflammatory processes?
Mast cells release an abundance of molecules that contribute towards inflammation. Mast
cells release protease, generating histamine-releasing peptides that contribute to inflammation.
They release tryptase that causes tissue damage, activation of PAR, inflammation and pain. They
also release corticotrophin-releasing hormone (CRH) peptides that contribute to inflammation
and vasodilation. Mast cells also releases an abundance of pro-inflammatory cytokines (IL-
1,2,3,4,5,6,9,10,13,16), INFs and TNFs (TNFα) that that cause inflammation, leukocyte
migration, proliferation and activation. Mast cells are so good at causing inflammation that they
sometimes cause inflammatory associated diseases such as asthma, atopic dermatitis,
fibromyalgia and many others. Mast cells also degranulate releasing histamine and heparin that
contributes to inflammation by promoting vasodilation, angiogenesis and mitogenesis.28
Q12-3: How is your favourite cell implicated in the resolution of inflammation and tissue
repair?
Mast cells are able to release somatostatin and chondroitin sulphate that both act as anti-
inflammatories. Mast cells also produce many cytokines/chemokines that acts as chemo
attractants for innate and adaptive immune cells that resolves the pathogen invading the tissue,
and promotes tissue repair. They release CCL1 that recruits T cells that can recognize antigen,
and then return to the lymph node to activate B cells that make antibodies against the pathogen in
order to clear it from the tissues. Mast cells also release CCL12 that attracts fibrocytes,
monocytes, eosinophils and lymphocytes, CCL20 that attracts dendritic cells, and TNF-α that
recruits neutrophils. All of these cells are able to combat the pathogen, resolving/clearing the site

of infection. Mast cells release CXCL8 that activates endothelial tissues to start angiogenesis (the
development of blood vessels) repairing vasculature in damaged tissues. Mast cells can also
release TGF-β (facilitates tissue repair by inhibits epithelial cell proliferation and increases rate
of angiogenesis) and IFN-α (increases, cytotoxicity, macrophage development and maturation,
dendritic cell activation, maturation, upregulated IFN-γ secretion).28
Q13-1: Describe how your favourite cell interacts with NK cells.
Bone marrow derived mast cells can become activated by bacterial lipopolysaccharide
(LPS). Activated mast cells induce natural killer (NK) cells to secrete IFN-γ. LPS activated mast
cells induce an NK cell IFN-γ response that is 20 fold greater than NK cell IFN-γ response
without LPS activated mast cells. It is postulated that mast cells induce the NK IFN response via
mast cells OX40 ligand binding to NK cells OX40 receptor. Researchers confirmed their findings
by blocking the OX40 ligand on mast cells, thus causing decreased IFN-γ secretion by NK
cells.29
Q13-2: What are the cytotoxic modalities in common between NK cells, NKT cells and
CD8+ T cells? Make a table with 6 comparative characteristics.
Table 1. Comparison of cytotoxic modalities between NK cells, NKT cells and CD8+ T cells.30
Comparative
Characteristics
NK cells 30 NKT cells 30 CD8+ T cells 30
Response Time Responds immediately to
antigen stimulation.
Responds immediately
to antigen stimulation.
Responds within ~7
days to antigen
stimulation (time it
takes precursors to
form functional CTLs).
Main
secretions
Perforins and granzymes,
IFN-γ,IL-6, TNF-α, Type
I and Type II IFNs and
FasL.
IFN-γ, IL-4, GMCSF,
IL-2, TNF.
Perforins and
granzymes, IFN-γ,
TNF, FasL.
Activation
Receptors
Recognizes loss of MHC
molecules on antigen
presenting cells. Can
bind directly to viral and
tumour antigens. (MHC
presence inhibits NK
activation). Activating
and inhibitory receptors
combine signals that
activate and inactivate
NK cells.
T-cell receptor that
does not recognize
MHC-antigen
complexes rather it
recognizes glycolipids
presented by the CD1d
molecule
T-cell receptor binding
to class I MHC-antigen
complex on antigen
presenting cell leads to
activation of CD8+ T
cells
Killing
Mechanism
Release of cytotoxic
granules and FasL-Fas
interactions triggering
apoptosis.
Mainly through FasL
interactions that trigger
apoptosis; indirect
activation of NK cells.
Release of cytotoxic
granules and FasL-Fas
interactions triggering
apoptosis.
Functions of
cytokines
IFN-γ promotes
macrophage
IFN-γ promotes
macrophage
IFN-γ promotes
macrophage

released. phagocytosis and
increases in class II
MHC expression, class
switching to IgG type
antibodies. IL-6 regulates
B and T cell functions
and induces
inflammation. TNF-α
mediates inflammation,
differentiation of many
cell types, cytotoxicity.
phagocytosis and
increases in class II
MHC expression, class
switching to IgG type
antibodies. IL-4
promotes Th2 cell
types, B cell growth
and differentiation and
class switching to IgE
antibodies. IL-2
activates NK cells and
promotes proliferation
and differentiation of T
and B cells.
phagocytosis and
increases in class II
MHC expression, class
switching to IgG type
antibodies. TNF
promotes inflammation,
growth and
differentiation of many
cell types.
Memory
Capacity
Yes. Express a receptor
that binds viral peptides
and transfer memory of
this antigen to naïve
animals.
No. Not capable of
forming memory NKT
cells.
Yes. Form memory
CD8+ cytotoxic T cells.
Q14-1: Describe how your favourite cell interacts with co-stimulatory molecules on DCs.
Overall, to date mast cells are not known to directly interact with co-stimulatory
molecules on dendritic cells. Mast cells are however able to bind to other receptors on dendritic
cells that leads to the up regulation of certain co-stimulatory molecules on the dendritic cell
surface. During the sensitization phase of contact hypersensitivity response bone marrow derived
mast cell use ICAM-1 adhesion interact with LFA-1 on bone marrow derived dendritic cells. This
interaction causes the up regulation of CD40, CD80, CD86, and CCR7 that in turn promote
dendritic cell maturation and migration.31
Q14-2: Compare the antigen presentation capacity between DCs, monocytes and B cells.
Make a table with 6 comparative characteristics.
Table 2. Comparison of antigen presentation capacity between dendritic cells, monocytes
(macrophages) and B cells.32
Comparative
Characteristics
Dendritic Cells 32 Monocytes 32 B Cells 32
Mechanism of
Antigen Uptake
Endocytosis and
Phagocytosis
Phagocytosis only B cell receptor-
mediated endocytosis.
Activation PRR recognition of
PAMPS, DAMPS,
cytokines.
PRR recognition of
PAMPS, DAMPS,
and cytokines. T cell
secretion of IFN- γ
B cell receptor
binding to antigen.
MHC expression Expresses both MHC
I and MHC II
Expresses both MHC
I and MHC II
Expresses both MHC
I and MHC II
Costimulatory
Molecules
CD80/86 CD80/86 CD80/86
Location of Non-
Activated Cells
Blood, Circulatory
System, Peripheral
Blood, Circulatory
System, Peripheral
Circulation, Lymph
nodes and Spleen,

Tissue Tissue Follicles
Location of Cell
When Activated
Migrates to T cell
Zone of
Subcapsular cortex of
lymph nodes,
marginal zone of
spleen and peripheral
tissues.
B cell zone- T cell
zone interface,
germinal centers, and
marginal zones of
Secondary Lymphoid
Organs (lymph nodes,
spleen).
Q15-1: Describe the complement of MHC I molecules on your favourite cell.
Mast cells major function is not antigen presentation therefore it does not have a vast
array of either MHC I or MHC II molecules. However, mast cells abnormally express HLA-G
class I MHC molecules in areas of liver fibrosis caused by hepatitis C virus.33
Q15-2: What is an MHC I tetramer? Explain how this technology could be used to
evaluate the frequency of cells responding to a specific antigen presented in MHC I
molecules.
Historically scientists have tried to directly measure CD8+ T cell responses using
antigenic peptides and MHC I. Unfortunately they had problems, as there was low affinity
between MHC/antigen complex and the CD8+ T cell receptors. This results in the
underestimation of CTLs that respond to certain antigens. A MHC I tetramer is a probe of
multiple copies of merged MHC/antigen complexes. This solves the problem of affinity as
affinity for CTLs higher and thus detects a response rate that is up to 500 times greater than past
methods.34
Q16-1: Does your favourite cell expression or interact with MHC II molecules?
‘Resting’ mast cells normally do not express MHC class II molecules. However, in tissues
that are infected or when mast cells are exposed to (TNF), IFN-γ or bacterial LPS mast cells have
been shown to have up regulated amounts of MHC class II expression on their surface.6
Q16-2: Give an example of an infection or disease in which MHC II alleles of the affected
individuals may affect the clinical outcome.
HLA MHC II alleles affect the clinical outcome of patients that are diseased with
ulcerative colitis. HLA DRB1*0103 was thought to be associated with severe cases of ulcerative
colitis. Researchers tested the hypothesis using DRB1 and DRQ1 genotyping of patients with
ulcerative colitis. They found that HLA DRB1*0103 was in 14.1% of patients they tested
compared to 3.2% of controls (individuals not infected with colitis). HLA DRB1*0103 was also
more pronounced in patients with extensive disease, it was in 25.8% of patients with mouth
ulcers, 27.2% of patients with arthritis and 35.7% of patients with uveitis. Thus DRB1*0103 is
associated with severe ulcerative colitis which usually ends with the patient requiring surgery.
Clinically, the DRB1*0103 HLA allele can then be used to predict the severity of ulcerative
colitis disease in patients as well as the likelihood that the patient will require surgery.35
Q17-1: Does your favourite cell expression or interact with TcR molecules?

Yes, studies have shown that mast cells are able to present antigenic peptide to TcR
complex on T cells. They are able to induce clonal expansion of T cells and migration of T cells
to the lymph nodes to induce an immune response.6
Q17-2: Give an example of an infection or disease in which γδ T cells play a larger role in
altering the clinical outcome than αβ T cells.
Chikungunya virus is an alpha virus that causes polyarthralgia (swelling/joint pain) in
human infections. γδ T cells play a larger role in altering the clinical outcome of this disease
compared to αβ T cells. During CHIKV infection γδ T cells are increased in number and offer a
protective role against the virus. When γδ T cell genes are knocked out in mice, leaving only to
αβ T cells as a defense, there is more intensified inflammation in the mouse foot and ankle joints.
Therefore T cells were shown to protect the host by reducing the amount of viral induced
inflammation, tissue and joint damage.36
Q18-1: What type of proteome is active in your favourite immune cell?
Mast cell have a proteome that is involved in activation of mast cell degranulation to
induce a proinflammatory response to encountered antigens. The mast cell genome carries genes
for many proteins involved in the signalling pathways such as SYK, LYN, MAPK, and others.12
Q18-2: Give an example of an infection or disease in which the expression levels of CD5+ on
T cells correlated with the immune outcome.
In tumours that can be cancerous or viral caused CD5 expression levels control the
activation of some T cells and thus their susceptibility to cell death. Researchers were able to
show that T cell death was inversely proportional to the expression of CD5+ on T cells. When
CD5+ was neutralized with an antibody there was an increase in tumour mediated T lymphocyte
cell death. Thus as CD5 increases T cell lysis decreases and CD8+ survival is promoted and thus
defense against the tumour is promoted.37
Q19-1: What signals are active in your favourite immune cell?
The main signal that is active in activated mast cells are the signalling pathways that are
induced by stimulation of the high–affinity IgE (FcεRI) receptor. It signals through LYN and
SYK tyrosine kinases that phosphorylate LAT adapter molecule. This leads to down stream
signaling activating MAPK and ERK that activate transcription factors (NFAT, NFκB, API) that
promotes to cytokine production. LAT also activates PLCγ that activates protein kinase C (PKC)
through down stream signaling molecules (DAG). PKC promotes the increase of free cytosolic
calcium, which is an essential signal for mast cell degranulation. cKit stimulation causes
recruitment and activation of SRC kinases, PLCγ and P13K, and JAK-STAT molecules. JAK-
STAT pathway and MAPK pathway promotes mast cell growth, differentiation, survival,
chemotaxis and cytokine production.12
Q19-2: Give an example of how effector T cells affect the function or survival of your
favourite immune cell.
Th1 and Th2 are effector T cells that secrete cytokines that have chemotactic activity for
mast cells. Th2 cells can secrete interleukin-4 (IL-4) and IL-8 that are mast cell chemo
attractants. Th1 cell secrete TNF-α that is also a mast cell chemoattractants. Thus, Th1 mediated

inflammation (TNF-α release) and Th2 mediated inflammation (IL-4 and IL-8 release) recruits
mast cells to the site of inflammation. This migration completely changes the mast cells function,
at the site of inflammation the mast cell is likely to encounter antigen, thus causing the mast cell
to degranulate contributing to further inflammation.38
Q19-3: Give an example of how memory T cells affect the function or survival of your
favourite immune cell.
Due to exhaustive literature search, one may conclude that there is limited studies about
how memory T cells affect the function or survival of mast cells. However, there is data about
how mast cells affect the function of CD4+ memory T cells. Mast cells are able to form an
immunologic synapse with memory CD4+ T cells. Mast cells secrete IL-22 and TNF-α that
promote the differentiation of memory CD4+ T cells into the Th22 T cell phenotype.39
Q20-1: Does your favourite cell secrete or binding antibodies?
Generally mast cells do not secrete antibodies however they do bind antibodies. IgE
molecules have a tail region that has a high affinity for Fc receptors (FcεRI) on the surface of
mast cells. IgE antibodies then bind the Fc receptor on the mast cell. This bound complex mast
cell surface receptors for antigen detection. When antigen does bind to the IgE antibodies that are
bound to the mast cell surface this promotes mast cell degranulation and cytokine secretion.40
Q20-2: Can your favourite cell modulate isotype switching in B cells? Why or why not?
Mast cells secrete IL-6, IL-5, TGF, and other cytokines and express the CD40 ligand that
can interact with B cell CD40 receptor. When B cells were co cultured with mast cells they were
able to interact and B cells showed and increased expression of IgA. The increase expression of
IgA suggests that B cells were modulated by mast cells to isotype switch to IgA.41
Q21-1: Does your favourite cell participate in B cell somatic hypermutation or class-switch
recombination? If so, how?
Due to exhaustive literature search it can be concluded that no, mast cells do not directly
participate in B cell somatic hypermutation. However, generally speaking they may play an
indirect role. Mast cells have been shown to have upregulated expression of MHC class II in the
presence of LPS, TNF, or IFN-γ.6 These mast cells can present antigen on MHC class II
molecules to naïve T cells that become activated and move to T cell zones in the lymph nodes.
Here B cells make contact with antigen specific T cells that can last for many hours activating the
B cells down regulating CCR7 and maintaining CXCR5 levels that promote B cell chemotaxis to
the follicular region where the B cells form germinal centers. Here the B cells undergo somatic
hypermutation that provides antibody diversification. 42
Q21-2: Does your favourite cell interact with B-1 cells?
Mast cells usually do not interact directly with B-1 cells. Although studies have shown
that mast cells indirectly play a role in B-1 B cell proliferation. IL-33 promotes B-1 cell
proliferation but depends on IL-5 that is largely mast cell dependent. When mast cells were
deficient, IL-33 activation of B-1 cells was also reduced.43

Q22-1: Does your favourite cell participate in antibody- dependent effector immune
responses? If so, how?
Yes. Mast cells participate in an antibody-dependent degranulatory synapse. Mast cells
express IgE and IgG antibodies on the surface that act as receptors for certain antigens. When
mast cells bind antigen on their antibodies they are triggered to begin their effector response.
Their effector immune response involves degranulation and release of inflammatory molecules
such as histamine, chymases, tryptases, and many cytokines that draw other cells to the site of
antigen encounter.
In study done they found that mast cell FcR stimulation by (IgE/IgG) antibody cell bound
antigen results in a degranulatory synapse formation that allows direct delivery of secretory
granules to the mast cells target cell.44
Q22-2: Does your favourite cell participate in cytotoxic killing of target cells? If so, how?
Mast cells indirectly participate in cytotoxic killing of target cells. Mast cells are able to
internalize some bacteria (enterobacteria) through phagocytosis. They process the pathogen and
then present the antigen on MHC class I molecules to T cell receptors on CD8+ cytotoxic T cells.
Mast cells also produce IL-4. Mast cell antigen presentation and IL-4 secretion leads to the
activation, proliferation and differentiation of CTLs. IL-4 can also enhance the cytotoxic killing
of antigen of CTLs. Therefore, mast cells can indirectly participate in the cytotoxic killing of
some bacteria.45
Q23-1: Does your favourite cell participate in atopic disease?
Asthma, allergic rhinitis, and atopic dermatitis are all atopic diseases of childhood that are
all mediated by IgE.46 Mast cells participate in atopic disease as they play a large role in asthma.
When asthmatics inhale allergens, mast cells equipped with a particular IgE antibody binds to the
allergen.47 These mast cells are found in the airway smooth muscle bundles and when activated
release histamine, prostaglandin D2, cysteinyl leukotrienes that cause airway smooth muscle
spasms. Mast cells also release serine protease tryptases that can cause bronchoconstriction,
airway remodeling, and airway hyper-responsiveness through a variety of mechanisms.48
Q23-2: Does your favourite cell interact with epithelial cells? If so, how?
Yes during asthma mast cells migrate to the airway epithelial cells. Here mast cells
infiltrate bronchial epithelium where they sit at the place of entry for any inhaled antigenic
allergens. If they encounter antigen they may play a part in antigen presentation and T cell
proliferation and differentiation responses. They may also adhere directly to the epithelium and
secrete tryptases that promote epithelial production of IL-8 release that promotes neutrophil
infiltration and inflammatory responses.49
Q24-1: Does your favourite cell interact with T regulatory cells? If so, how?
Mast cell interacts with T regulatory cells through and OX40 receptor-ligand interaction.
This interaction shows that T regulatory cells can inhibit FcεRI-dependent mast cell
degranulation.50 Activated mast cells have been shown to be able to counteract T regulatory cell
inhibition of degranulation through engagement of OX40 receptor and ligand and the production
of IL-6 and Th1 and Th2 cytokines that promote T regulatory cell differentiation into Th17 T cell
phenotype.51

Q24-2: Does your favourite cell participate in autoimmune disease?
Yes. Mast cells participate in autoimmune rheumatoid arthritis. Mice that were deficient
in mast cells were found to have much less joint inflammation. Mast cells secrete many
proinflammatory cytokines (TNF, IL-1β, IL-17, and tryptases). Tryptase works with heparin to
promote neutrophil infiltration and activates synovial fibroblasts that degrade cartilage and bone
through interaction with PAR2 receptor. Mast cells self amplify in rheumatoid arthritis by
secreting TNF-α that causes fibroblasts to produce SCF that increases mast cell recruitment to the
synovial fluid in the joint.50 When mast cells degranulate they release heparin, proteases, TNF,
IL-1, 2, 3, 4, 6, VEGF and many other cytokines into the synovial fluid histamine further increase
inflammation, neutrophil and leukocyte infiltration, fibroblast activation and additional
outcomes.52
Q25-1: Is your favourite cell impacted by a primary immunodeficiency? If so, how?
Yes, mast cells are impacted by PLAID is PLCγ2 associated antibody deficiency and
immune dysregulation a primary immunodeficiency disease. It is caused by a mutation in
phospholipase C-γ2 gene. It effects people from birth and causes abnormal allergic responses to
cold temperatures. Mast cells are impacted by abnormal activation by cold temperatures that
leads to their degranulation.53
Q25-2: Is your favourite cell impacted by a secondary immunodeficiency? If so, how?
Yes. Patients that have AIDS, an acquired secondary immunodeficiency showed
decreased mast cell reactivity to antigen. Researchers believe that AIDS is associated with
decrease in local mast cell density and releasibility. It is hypothesized that the decrease in mast
cell density is related to HIV-related hematopoietic dysfunction that causes decreased
proliferation of mast cells. Another hypothesis is that HIV may directly inhibit mast cell
degranulation through binding in ways similar to the ways in which HIV gp120 depresses β-
adrenergic responsiveness of astrocytes and microglia.54
Q26-1: With a partner from BIOL4931, pick a human infection or disease that involves
both your cell types. Explain how together your favourite cells cooperate to ensure an
effective immune response. You must present information comparing and contrasting how
your cells are involved in innate immune signalling, antigen presentation and effector
responses. 300 word minimum.
Atopic dermatitis, also called eczema, causes itchy skin that is red, warm, and tender and
it usually runs in the family. Researchers are still trying to figure out what exactly causes atopic
dermatitis.55 Many inflammatory diseases such as atopic dermatitis involve mast cells in cross-
talk with T cells.56 Studies have shown that mast cell and T cell interaction can promote the
activation of mast cell transcriptional activity.55 When mast cells bind to activate T cells in atopic
dermatitis mast cell effector response is promoted which is defined as mast cell degranulation,
proinflammatory cytokine production, and TNF-α production.56 T cells play a large role part in
effector response in atopic dermatitis. In atopic dermatitis there are several effector T cell
subtypes such as Th9, Th17, Th22 cells (that are differentiated CD4+ T cells) that express high
levels of IL-9, IL-17, IL-22.56 T regulatory cells as well as mast cells are also present and secrete
IL-10 that is an immunomodulatory cytokine that functions to inhibit skin inflammatory
processes in atopic dermatitis.57,58 Th9 cell are pro-inflammatory because they recruit mast cells
to the site of atopic dermatitis through the production of IL-9. Mast cells that secrete IL-13 and
IL-4 promote Th2 T cell effector responses.58Activated effector mast cells in atopic dermatitis

secrete many cytokines such as, TNF-α, TGF-β, VEGF, IFN-α/β/γ, IL- (1-6,8-16, 18 and 25). In
atopic dermatitis mast cells can function as antigen presenters, where they use class II MHC
molecules to present antigen to CD4+ T cells. T cells do not present antigen. T-cells and mast
cells may also interact through OX40-OX40L interactions triggering T cell proliferation in atopic
dermatitis.59 Overall, mast cells promote the pathogenic inflammatory response of atopic
dermatitis while CD4+ T helper cell subtypes regulate the function of mast cells to ensure they
are not overly pathogenic to the host.
Bibliography
1. Urb, M., & Sheppard, D. C. (2012). The Role of Mast Cells in the Defence against
Pathogens. PLoS Pathogens, 8(4), e1002619.
2. “Mast Cell Electron Micrograph.” Histology @ Yale. n.d. Web. 29 Nov 2015.
3. Owen, J. A., Punt, J., & Stranford, S. A. (2013). Kuby immunology. New York: WH Freeman.
p 33.
4. “Cellosaurus- HMC-1 (CVCL_0003).” SIB ExPASy Bioinformatics Research Portal. n.d.
Web. 30 Nov 2015.
5. Beghdadi, W., Madjene, L. C., Benhamou, M., Charles, N., Gautier, G., Launay, P., & Blank,
U. (2011). Mast cells as cellular sensors in inflammation and immunity. Frontiers in
immunology, 2.

6. Galli, S. J., Nakae, S., & Tsai, M. (2005). Mast cells in the development of adaptive immune
responses. Nature immunology, 6(2), 135-142.
7. Carroll-Portillo, A., Cannon, J. L., Riet, J., Holmes, A., Kawakami, Y., Kawakami, T., &
Lidke, D. S. (2015). Mast cells and dendritic cells form synapses that facilitate antigen
transfer for T cell activation. The Journal of cell biology, 210(5), 851-864.
8. Bachelet, Ido, and Francesca Levi-Schaffer. "Mast Cells as Effector Cells: A Co-Stimulating
Question." Trends in immunology 28.8 (2007): 360-5. ProQuest. 1 Nov. 2015 .
9. Stone, Kelly D., Calman Prussin, and Dean D. Metcalfe. "IgE, mast cells, basophils, and
eosinophils." Journal of Allergy and Clinical Immunology 125.2 (2010): 73-80.
10. Gri, G., Piconese, S., Frossi, B., Manfroi, V., Merluzzi, S., Tripodo, C., Viola, A., Odom, S.,
Rivera, J., Colombo, M.P., & Pucillo, C. E. (2008). CD4+CD25+ regulatory T cells suppress
mast cell degranulation and allergic responses through OX40-OX40L interaction.
Immunity, 29(5), 771–781.
11. Blott, E. J., & Griffiths, G. M. (2002). Secretory lysosomes. Nature Reviews Molecular Cell
Biology, 3(2), 122-131.
12. Gilfillan, A. M., & Tkaczyk, C. (2006). Integrated signalling pathways for mast-cell
activation. Nature Reviews Immunology, 6(3), 218-230.
13. Theoharides, Theoharis C. et al. “Mast Cells and Inflammation.” Biochimica et Biophysica
Acta 1822.1 (2012): 21–33. PMC. Web. 2 Nov. 2015.
14. Stone, Kelly D., Calman Prussin, and Dean D. Metcalfe. "IgE, mast cells, basophils, and
eosinophils." Journal of Allergy and Clinical Immunology 125.2 (2010): S73-S80.
15. Halova I, Draberova L and Draber P (2012) Mast cell chemotaxis – chemoattractants and
signaling pathways. Fronteirs in Immunology, 3:119.
16. Juremalm, M., & Nilsson, G. (2005). Chemokine receptor expression by mast cells. 130-144.
17. Da Silva, E. Z. M., Jamur, M. C., & Oliver, C. (2014). Mast Cell Function A New Vision of
an Old Cell. Journal of Histochemistry & Cytochemistry, 62(10), 698-738.
18. Raica, M., Cîmpean, A. M., Encică, S., Scridon, T., & Bârsan, M. (2007). Increased mast cell
density and microvessel density in the thymus of patients with myasthenia gravis. Romanian
Journal of Morphology and Embryology, 48(1), 11-6.
19. Owen, J. A., Punt, J., & Stranford, S. A. (2013). Kuby immunology. New York: WH Freeman.
p 305.
20. Wang, H. W., Tedla, N., Lloyd, A. R., Wakefield, D., & McNeil, P. H. (1998). Mast cell
activation and migration to lymph nodes during induction of an immune response in
mice. Journal of Clinical Investigation, 102(8), 1617.
21. Pretlow, T. G., & Pretlow, T. P. (Eds.). (2014). Cell separation: methods and selected
applications. Academic Press. 155.
22. Raud, J. (1988). Intravital microscopic studies on acute mast cell-dependent
inflammation. Acta physiologica Scandinavica. Supplementum, 578, 1-58.
23. Bowie, A. G., & Unterholzner, L. (2008). Viral evasion and subversion of pattern-recognition
receptor signalling. Nature Reviews Immunology, 8(12), 911-922.
24. Niewiadomska, A. M., & Yu, X. F. (2009). Host restriction of HIV-1 by APOBEC3 and viral
evasion through Vif. In HIV Interactions with Host Cell Proteins. Springer Berlin Heidelberg.
p 1-25.
25. Swieter, M., Ghali, W. A., Rimmer, C., & Befus, D. (1989). Interferon-alpha/beta inhibits
IgE-dependent histamine release from rat mast cells. Immunology, 66(4), 606–610.
26. Riccardi-Arbi, R., Bacci, S., Romagnoli, P., & Rucei, L. (2004). ч Interferon-alpha affects the
tumour necrosis factor-alpha content of mast cells in human nasal mucosa. A pilot study in
allergic patients. Italian Journal of Anatomy and Embryology, 109(2):115-22.
27. Fujita, T., Kambe, N., Uchiyama, T., & Hori, T. (2006). Type I interferons attenuate T cell
activating functions of human mast cells by decreasing TNF-α production and OX40 ligand

expression while increasing IL-10 production. Journal of clinical immunology, 26(6), 512-
518.
28. Theoharides, T. C., & Kalogeromitros, D. (2006). The critical role of mast cells in allergy and
inflammation. Annals of the New York Academy of Sciences, 1088(1), 78-99.
29. Vosskuhl, K., Greten, T. F., Manns, M. P., Korangy, F., & Wedemeyer, J. (2010).
Lipopolysaccharide-Mediated Mast Cell Activation Induces IFN-γ Secretion by NK
Cells. The Journal of Immunology, 185(1), 119-125.
30. Owen, J. A., Punt, J., & Stranford, S. A. (2013). Kuby immunology. New York: WH Freeman.
p 428-447.
31. Blank, U., & Benhamou, M. (2013). Deciphering new molecular mechanisms of mast cell
activation. Frontiers in immunology, 4, 55-56.
32. Owen, J. A., Punt, J., & Stranford, S. A. (2013). Kuby immunology. New York: WH Freeman.
p 366.
33. Amiot, L., Vu, N., Rauch, M., L’Helgoualc’h, A., Chalmel, F., Gascan, H., Turlin, B.,
Guyader, D., & Samson, M. (2014). Expression of HLA-G by mast cells is associated with
hepatitis C virus-induced liver fibrosis. Journal of hepatology, 60(2), 245-252.
34. “MHC Tetramer Technology – Note 7.2.” Thermo Fisher Scientific. n.d. Web. 28 Nov 2015.
35. Roussomoustakaki, M., Satsangi, J., Welsh, K., Louis, E., Fanning, G., Targan, S., & Jewell,
D. P. (1997). Genetic markers may predict disease behavior in patients with ulcerative colitis.
Gastroenterology, 112(6), 1845-1853.
36. Long, K. M., Ferris, M. T., Whitmore, A. C., Montgomery, S. A., Thurlow, L. R., McGee, C.
E., ... & Heise, M. T. (2015). Gamma-delta T cells play a protective role in chikungunya
virus-induced disease. Journal of virology, JVI-02159.
37. Friedlein, G., El Hage, F., Vergnon, I., Richon, C., Saulnier, P., Lécluse, Y., Caignard, A., &
Mami-Chouaib, F. (2007). Human CD5 protects circulating tumor antigen-specific CTL from
tumor-mediated activation-induced cell death. The Journal of Immunology, 178(11), 6821-
6827.
38. Olsson, N., Taub, D. D., & Nilsson, G. (2004). Regulation of Mast Cell Migration by TH1
and TH2 Cytokines: Identification of Tumour Necrosis Factor‐ α and Interleukin‐ 4 as Mast
Cell Chemotaxins. Scandinavian journal of immunology, 59(3), 267-272.
39. Gaudenzio, N., Laurent, C., Valitutti, S., & Espinosa, E. (2013). Human mast cells drive
memory CD4+T cells toward an inflammatory IL-22+phenotype. Journal of Allergy and
Clinical Immunology, 131(5), 1400-1407
40. Alberts, B., Johnson, A., Lewis, J., Raff, M., Roberts, K., & Walter, P. (2002). B Cells and
Antibodies.
41. Merluzzi, S., Frossi, B., Gri, G., Parusso, S., Tripodo, C., & Pucillo, C. (2010). Mast cells
enhance proliferation of B lymphocytes and drive their differentiation toward IgA-secreting
plasma cells. Blood Journal, 115(14), 2810-2817.
42. Owen, J. A., Punt, J., & Stranford, S. A. (2013). Kuby immunology. New York: WH Freeman.
p 388-398.
43. Komai-Koma, M., Gilchrist, D. S., McKenzie, A. N., Goodyear, C. S., Xu, D., & Liew, F. Y.
(2011). IL-33 activates B1 cells and exacerbates contact sensitivity.The Journal of
Immunology, 186(4), 2584-2591.
44. Joulia, R., Gaudenzio, N., Rodrigues, M., Lopez, J., Blanchard, N., Valitutti, S., & Espinosa,
E. (2015). Mast cells form antibody-dependent degranulatory synapse for dedicated secretion
and defence. Nature communications, 6(6174).
45. Mekori, Y. A., & Metcalfe, D. D. (1999). Mast cell–T cell interactions. Journal of Allergy
and Clinical Immunology, 104(3), 517-523.
46. Stone, K. D. (2002). Atopic diseases of childhood. Current opinion in pediatrics, 14(5), 634-
646.

47. “Allergies.” Asthma and Allergy Foundations of America. Sept 2015. Web. 30 Nov 2015.
48. Brightling, C. E., Bradding, P., Symon, F. A., Holgate, S. T., Wardlaw, A. J., & Pavord, I. D.
(2002). Mast-cell infiltration of airway smooth muscle in asthma. New England Journal of
Medicine, 346(22), 1699-1705.
49. Bradding, P. (2008). Asthma: Eosinophil Disease, Mast Cell Disease, or Both? Allergy,
Asthma, and Clinical Immunology : Official Journal of the Canadian Society of Allergy and
Clinical Immunology, 4(2), 84–90.
50. Xu, Y., & Chen, G. (2015). Mast Cell and Autoimmune Diseases. Mediators of
inflammation, 2015.
51. Piconese, S., Gri, G., Tripodo, C., Musio, S., Gorzanelli, A., Frossi, B., Pedotti, R., Pucillo,
C. E., & Colombo, M. P. (2009). Mast cells counteract regulatory T-cell suppression through
interleukin-6 and OX40/OX40L axis toward Th17-cell differentiation. Blood
Journal, 114(13), 2639-2648.
52. Nigrovic, P. A., & Lee, D. M. (2005). Mast cells in inflammatory arthritis. Arthritis Research
& Therapy, 7(1), 1–11.
53. “PLCG2-associated Antibody Deficiency and Immune Dysregulation (PLAID).” National
Institute of Allergy and Infectious Disease. 11 Jun 2015. Web. 29 Nov 2015.
54. Simonart, T., Parent, D., Heenen, M., Farber, C. M., & Van Vooren, J. P. (1996). Decreased
skin reactivity to codeine in patients with the acquired immunodeficiency syndrome. Clinical
immunology and immunopathology, 81(1), 12-15.
55. “Atopic Dermatitis: Who Gets and Causes.” American Academy of Dermatology. n.d. Web.
30 Nov 2015.
56. Theoharides, T. C., Alysandratos, K. D., Angelidou, A., Delivanis, D. A., Sismanopoulos, N.,
Zhang, B., ... & Kalogeromitros, D. (2012). Mast cells and inflammation. Biochimica et
Biophysica Acta (BBA)-Molecular Basis of Disease, 1822(1), 21-33.
57. Auriemma, M., Vianale, G., Amerio, P., & Reale, M. (2013). Cytokines and T cells in atopic
dermatitis. European cytokine network, 24(1), 37-44.
58. Kawakami, T., Ando, T., Kimura, M., Wilson, B. S., & Kawakami, Y. (2009). Mast cells in
atopic dermatitis. Current opinion in immunology, 21(6), 666-678.
59. Gri, G., Frossi, B., D’Inca, F., Danelli, L., Betto, E., Mion, F., Sibilano, F., & Pucillo, C.
(2012). Mast cell: an emerging partner in immune interaction. Frontiers in immunology, 3.