
Fatigue in Child Chronic Health Conditions: A Systematic ... fatigue assessment instruments used in...
19
Fatigue in Child Chronic Health Conditions: A Systematic Review of Assessment Instruments Alison Crichton, DPsych a,b,c , Sarah Knight, PhD a,b,d , Ed Oakley, PhD b,d,e , Franz E. Babl, MD b,d,e , Vicki Anderson, PhD b,c,e abstract BACKGROUND AND OBJECTIVE: Fatigue is common in chronic health conditions in childhood, associated with decreased quality of life and functioning, yet there are limited data to compare assessment instruments across conditions and childhood development. Our objective was to describe fatigue assessment instruments used in children with chronic health conditions and critically appraise the evidence for the measurement properties of identified instruments. METHODS: Data sources included Medline, Cumulative Index to Nursing and Allied Health Literature, and PsycINFO (using the EBSCOhost platform). Study selection included quantitative assessment of fatigue in children with health conditions. Data extraction was as follows: (1) study design, participant and fatigue instruments, (2) measurement properties of fatigue instruments, (3) methodological quality of included studies, and (4) synthesis of the quality of evidence across studies for the measurement properties of fatigue instruments. RESULTS: Twenty fatigue assessment instruments were identified (12 child reports, 7 parent reports, 1 staff report), used in 89 studies. Fatigue was assessed in over 14 health conditions, most commonly in children with cancer and chronic fatigue syndrome. Evidence for the measurement properties of instruments varied, and overall quality was low. Two fatigue instruments demonstrated strong measurement properties for use in children with diverse health conditions and children with cancer. CONCLUSIONS: The review is limited to children younger than 18 years and results are specific to health conditions described, limiting generalizability of findings to other populations. Evidence for the measurement properties of fatigue instruments varied according to the population in which instruments were used and informant. Further evidence is required for assessment of fatigue in younger children, and children with particular health conditions. a Victorian Pediatric Rehabilitation Service, Monash Children’ s, Melbourne, Australia; b Murdoch Childrens Research Institute, Melbourne, Australia; c School of Psychological Sciences and d Department of Pediatrics, University of Melbourne, Melbourne, Australia; and e Royal Children’ s Hospital, Melbourne, Australia Dr Crichton conceptualized and designed the study, carried out the literature searches, completed the initial analysis, drafted the initial manuscript, and revised the manuscript; Dr Knight assisted with the data collection instrument, screened articles for inclusion, reviewed analysis, and reviewed the manuscript; Dr Anderson supervised data collection and critically reviewed the manuscript; Drs Oakley and Babl cosupervised data collection and reviewed the manuscript; and all authors approved the final manuscript as submitted. www.pediatrics.org/cgi/doi/10.1542/peds.2014-2440 DOI: 10.1542/peds.2014-2440 Accepted for publication Dec 30, 2014 Address correspondence to Alison Crichton, DPsych, Senior Clinical Neuropsychologist, Critical Care and Neurosciences Theme, Murdoch Childrens Research Institute, Royal Children’ s Hospital, Flemington Rd, Parkville, 3052, Australia. E-mail: [email protected] PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2015 by the American Academy of Pediatrics PEDIATRICS Volume 135, number 4, April 2015 REVIEW ARTICLE by guest on April 14, 2017 Downloaded from
Transcript of Fatigue in Child Chronic Health Conditions: A Systematic ... fatigue assessment instruments used in...

Fatigue in Child Chronic HealthConditions: A Systematic Review ofAssessment InstrumentsAlison Crichton, DPsycha,b,c, Sarah Knight, PhDa,b,d, Ed Oakley, PhDb,d,e, Franz E. Babl, MDb,d,e, Vicki Anderson, PhDb,c,e
abstractBACKGROUND AND OBJECTIVE: Fatigue is common in chronic health conditions in childhood, associatedwith decreased quality of life and functioning, yet there are limited data to compareassessment instruments across conditions and childhood development. Our objective was todescribe fatigue assessment instruments used in children with chronic health conditions andcritically appraise the evidence for the measurement properties of identified instruments.
METHODS: Data sources included Medline, Cumulative Index to Nursing and Allied HealthLiterature, and PsycINFO (using the EBSCOhost platform). Study selection includedquantitative assessment of fatigue in children with health conditions. Data extraction was asfollows: (1) study design, participant and fatigue instruments, (2) measurement properties offatigue instruments, (3) methodological quality of included studies, and (4) synthesis of thequality of evidence across studies for the measurement properties of fatigue instruments.
RESULTS: Twenty fatigue assessment instruments were identified (12 child reports, 7 parentreports, 1 staff report), used in 89 studies. Fatigue was assessed in over 14 health conditions,most commonly in children with cancer and chronic fatigue syndrome. Evidence for themeasurement properties of instruments varied, and overall quality was low. Two fatigueinstruments demonstrated strong measurement properties for use in children with diversehealth conditions and children with cancer.
CONCLUSIONS: The review is limited to children younger than 18 years and results are specific tohealth conditions described, limiting generalizability of findings to other populations. Evidencefor the measurement properties of fatigue instruments varied according to the population inwhich instruments were used and informant. Further evidence is required for assessment offatigue in younger children, and children with particular health conditions.
aVictorian Pediatric Rehabilitation Service, Monash Children’s, Melbourne, Australia; bMurdoch Childrens Research Institute, Melbourne, Australia; cSchool of Psychological Sciences anddDepartment of Pediatrics, University of Melbourne, Melbourne, Australia; and eRoyal Children’s Hospital, Melbourne, Australia
Dr Crichton conceptualized and designed the study, carried out the literature searches, completed the initial analysis, drafted the initial manuscript, and revised themanuscript; Dr Knight assisted with the data collection instrument, screened articles for inclusion, reviewed analysis, and reviewed the manuscript; Dr Andersonsupervised data collection and critically reviewed the manuscript; Drs Oakley and Babl cosupervised data collection and reviewed the manuscript; and all authorsapproved the final manuscript as submitted.
www.pediatrics.org/cgi/doi/10.1542/peds.2014-2440
DOI: 10.1542/peds.2014-2440
Accepted for publication Dec 30, 2014
Address correspondence to Alison Crichton, DPsych, Senior Clinical Neuropsychologist, Critical Care and Neurosciences Theme, Murdoch Childrens Research Institute,Royal Children’s Hospital, Flemington Rd, Parkville, 3052, Australia. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2015 by the American Academy of Pediatrics
PEDIATRICS Volume 135, number 4, April 2015 REVIEW ARTICLEby guest on April 14, 2017Downloaded from

Fatigue refers to a subjectivelyoverwhelming sense of tiredness, lackof energy, and feeling of exhaustion.1
It is a common, independent, andnonspecific symptom identified innumerous chronic health conditionsin childhood. Consequently, it hasbeen described as 1 of the mostuniversal experiences for childrenwith chronic health conditions,2
although reported rates of fatigue varywithin and between conditions.3–7
Excessive fatigue leads to reducedquality of life,8 depression,9 andreduced school participation.10–13
Fatigue is also identified in healthychildren with normal daily functioning.Given these characteristics, it isimportant to identify accurate andreliable child-friendly measures todetect excessive fatigue.
EPIDEMIOLOGY
Excess fatigue is a common presentingproblem in clinical practice, occurringin children with cancer,14,15
neurologic conditions,16 chronicfatigue syndrome,17 posturaltachycardia syndrome,18 multiplesclerosis,6 epilepsy,19 traumatic braininjury,20 juvenile idiopathic arthritis,21
diabetes,22,23 inflammatory boweldisease,24 fibromyalgia,25,26 andobesity.27 Importantly, fatigue in theseconditions is distinguishable fromother related symptoms includingsleepiness, depression, and apathy,28
and is not ameliorated by sleep.1
Precise prevalence estimates areconstrained by issues related toassessment, terminology, andmeasurement, which are heightenedin childhood.
MEASUREMENT
Fatigue has been defined as anoverwhelming and sustained sense ofexhaustion that decreases one’scapacity for physical and mentalwork.29 Quantification of fatigueremains impeded by lack ofconsensus framework, terminology,and the subjective andmultidimensional nature of
symptoms. Three alternativeframeworks for describing subjectivefatigue are as follows: “centralfatigue” (resulting from central asopposed to peripheral nervoussystem damage and incorporatingmental and physical symptoms)30; asa “feeling state”;28 and asa combination of primary (diseasespecific) and secondary factors (suchas pain, sleep disturbance, or moodchanges).31 The subjectivity andbreadth of symptoms makequantification challenging, andresultantly assessment instrumentsfocus on the duration or severity ofsymptoms (physical, mental,affective) and other dimensions of thefatigue experience, including impacton daily functioning and exacerbatingfactors (eg, sleep habits).31–36 In thisreview, based on earlier work,37 thetheoretical construct of fatigue will becategorized as “impact of fatigue ondaily life,” “fatigue severity,” or“factors influencing fatigue.”
It is important for instruments thatassess children’s fatigue to be childspecific. It is a unique experience withits own symptomatology,presentation, and naturalhistory.38–41 Fatigue is inherentlysubjective,28 and its assessment inchildhood is challenging because theaccuracy and relevance of parent-proxy reports is questionable.42
Further, fatigue in the generalchildhood population varies throughdevelopment; it is greater in infancy,early childhood, and late adolescencethan during midchildhood, and ismore common in girls.43–45 Accurateassessment requires recognition ofthe developmental stages andreference to age and gender norms.
Although fatigue is a commonsymptom in a range of chronic healthconditions, and notable challengeswith its measurement exist, there hasbeen limited evaluation of assessmentinstruments in use with children.
TABLE 1 Data Extraction Items
Data Category Description Data Extracted
1 Study description Study aims, design, study duration, and any bias. Participantnumbers, setting, diagnostic criteria, age, gender, country,comorbidity, and diagnostic criteria used.
2 Instrument description For each study: name of instrument(s), language version,theoretical constructs, number of items, description ofdomains assessed, theoretical construct,a age, respondents,response format, and extent of active patient involvement ininstrument development.b
3 Psychometric propertiesof fatigue measures
Criteria ratingc for instrument-level measurement properties(as reported in study): (1) internal consistency, (2)reliability, (3) measurement error, (4) content validity, (5)construct validity, (6) structural validity, (7) hypothesistesting, (8) cross-cultural validity, and (9) responsiveness.
4 Study quality Ratingd of study methodological quality for each of thefollowing measurement properties reported: (1) internalconsistency, (2) reliability, (3) measurement error, (4)content validity, (5) construct validity, (6) structural validity,(7) hypothesis testing, (8) cross-cultural validity, (9)responsiveness (add * if measurement properties were notchecked, and the authors cite published measurementproperties in another article).
5 Acceptability andfeasibility
Acceptability (respondent burden, time for completion) andfeasibility (time for scoring, ease of scoringe).
6 Risk of bias Study and outcome level data: outcome data completeness,drop-out rate description, any selective outcome reporting.
a Theoretical construct of fatigue rated as impact of fatigue on daily life, fatigue severity, or factors influencing fatigue.37b INVOLVE definitions of extent of patient involvement in instrument development (“consultation,” “collaboration,” or “user-led”).136c Criteria for good measurement properties on the basis of criteria proposed by Terwee et al.55d The quality of each included study was evaluated by using the COSMIN checklist54 and rating system.57e Ease of scoring criteria were “easy,” “moderate,” or “difficult” according to Elbers et al.37
e1016 CRICHTON et alby guest on April 14, 2017Downloaded from
Exceptions are reviews of measuresin children with cancer46,47 andchronic fatigue syndrome.48 It isimportant to identify the instrumentsavailable and to evaluate theirmeasurement properties. Theobjectives of this review of fatigue inchildren and adolescents with chronichealth conditions were to (1)describe participant and studycharacteristics of included studies,(2) describe and systematicallyreview available instruments used toassess fatigue, detailing thoseavailable for child (self) and parent(proxy) report, (3) interpretinstruments by usinga multidimensional framework offatigue, (4) review identifiedinstruments within a developmentalframework, and (5) summarize andsynthesize the psychometricproperties of the these instrumentsand the quality of the evidence.
METHODS
Information Sources
The search strategy was designed toretrieve literature relating tomeasures of subjective fatigue inchildren with chronic healthconditions. The systematic reviewwas conducted according to thePreferred Reporting Items forSystematic Reviews and Meta-Analyses (PRISMA).49 The EBSCOhostplatform was used to search theelectronic databases Medline,Cumulative Index to Nursing andAllied Health Literature, andPsycINFO from 1990 to August 24,2013 (updated June 12, 2014).Nonconventional documents (gray
literature) and publications,50 andsecondary references were alsochecked.
Search
The searches were limited to English-language publications. Subjectheadings and key words used werethe following: (1) fatigue, weary,weariness, exhaustion, exhausted,lacklustre or astheni*, letharg*, tired;or (2) (lack* or loss or lost) and(energy or vigor or vigor); (3) feelingand (drained or sleepy or sluggish orweak*); (4) central nervous systemdiseases, neoplasms, multiplesclerosis, congenital heart defects,anemia, chronic pain, chronic disease,cerebral palsy, cardiovasculardiseases, diabetes mellitus (type 1);chronic fatigue syndrome; and (5)questionnaires or psychological tests.
Eligibility Criteria
Population
Children and/or adolescents (#18years of age) with a health condition.
Assessment Tool
Any questionnaire designed tomeasure fatigue by using more than1 item. Fatigue subscales included inquality-of-life or other measureswere eligible for inclusion, providedthat fatigue scores could beextracted separately (ie, totalsubscale scores provided). Fatigueassessment must be subjective,quantified, and based on child reportor parent/other report, to be eligiblefor inclusion.
Outcome
Any clinical outcome.
Study Design
Interventional and observationalstudies published in peer-reviewedjournals were eligible for inclusion.
Exclusion Criteria
Review articles, opinion pieces, andsingle case studies were excluded asfollows: studies that only reportedqualitative information as a measureof fatigue (ie, professional opinion orinterview data); fatigue measuresthat used a single item, either standalone (single item visual analog scales[VASs]) or as part of anotherquestionnaire (ie, quality of life/depression/symptom checklists); andobjective measures of performancedecrement (ie, attention vigilance,muscle fatigue).
Study Selection
Titles and abstracts of all articleswere assessed for inclusion by 2independent reviewers (Drs Crichtonand Knight) and agreement checked.
Data Collection Process
A standardized data extraction formwas developed and informed bystandard processes for systematicreviews,51,52 earlier reviews in thefield,37,46–48 and incorporatingrecommendations for patient-reported outcome measureevaluation and standards forappraisal of methodologicalquality.53–55 The form wasindependently piloted in 2 randomlyselected studies by Drs Crichton andKnight. Data were extracted by DrCrichton, independently checked byDr Knight, and disagreements wereresolved by consensus withconsultation of a third reviewer(Dr Anderson; Table 1).
The data extraction and assessmentincluded information from 6 domains(Table 1). The measurementproperties evaluated in datacategories 3 and 4 in Table 1incorporate a consensus-basedtaxonomy of measurement propertiesconsidered important in patient-reported outcome measures, defined
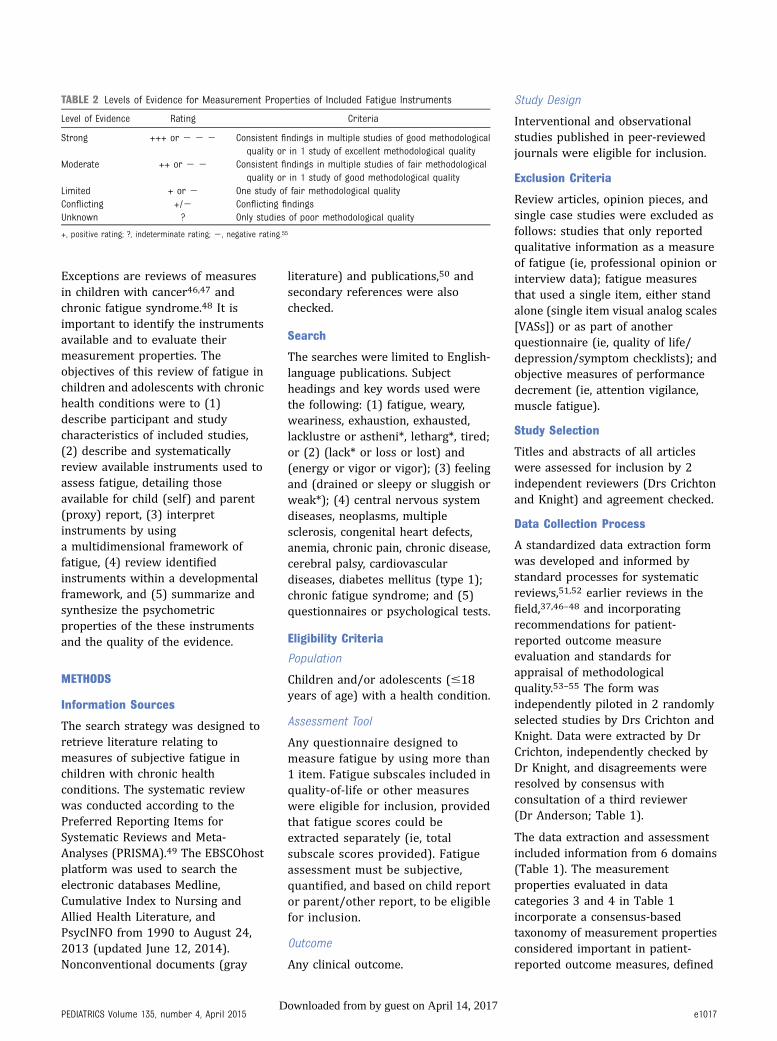
TABLE 2 Levels of Evidence for Measurement Properties of Included Fatigue Instruments
Level of Evidence Rating Criteria
Strong +++ or 2 2 2 Consistent findings in multiple studies of good methodologicalquality or in 1 study of excellent methodological quality
Moderate ++ or 2 2 Consistent findings in multiple studies of fair methodologicalquality or in 1 study of good methodological quality
Limited + or 2 One study of fair methodological qualityConflicting +/2 Conflicting findingsUnknown ? Only studies of poor methodological quality
+, positive rating; ?, indeterminate rating; 2, negative rating.55
PEDIATRICS Volume 135, number 4, April 2015 e1017by guest on April 14, 2017Downloaded from

by Mokkink et al56 (Table 2, p. 743).Relevant properties include thefollowing: (1) internal consistency,(2) reliability, (3) measurement error,(4) content validity, (5) constructvalidity, (6) structural validity, (7)hypothesis testing, (8) cross-culturalvalidity, and (9) responsiveness.Criterion validity is not relevant forfatigue assessment, so it wasexcluded. The 9 listed measurement
properties provided the domains fordata extraction for 2 key data sets atan individual study level: (1) ratingthe measurement property of theinstrument; (2) rating the quality ofthe study (data categories 3 and 4,Table 1; floor/ceiling effects andinterpretability not rated). Accordingto predefined criteria, eachmeasurement property was rated as“positive,” “indeterminate,” “negative,”
or “no information available.”55 Ifmeasurement properties were notchecked, but the authors citedpublished measurement properties inanother article, this was recorded andthe above ratings were maintained.
The methodological quality ofincluded studies were evaluated byusing the consensus-based standardsfor the selection of healthmeasurement instruments (COSMIN)checklist and 4-point rating scale.57
The COSMIN checklist contains 114data points (12 boxes, 9 assessingmeasurement properties), relating todesign requirements and preferredstatistical methods and consensus onstatistical values consideredadequate. Of these, 91 data points(8 boxes) were relevant to the currentreview: internal consistency (11),reliability (14), measurement error(11), content validity (5), structuralvalidity (7), hypothesis testing (10),cross-cultural validity (15), andresponsiveness (18). Each item wasscored on a 4-point rating scale (ie,“poor,” “fair,” “good,” or “excellent,”and “not applicable” if omitted). Foreach measurement property, the finalrating was determined by the lowestrating of any of the items within thebox. If more than 1 instrument wasincluded in a study (eg, parent andchild versions), the samemeasurement property was assessedfor each instrument.
Data Synthesis
Study level data were synthesized toprovide summary information foreach fatigue instrument. Informationacross studies was summarized todescribe identified instruments andthe populations to whom instrumentswere administered. Second, asguidelines for pooling ofmeasurement properties are stillunder development, best evidencesynthesis was performed integrating:(1) the rating for the instrument’smeasurement property acrossstudies55 and (2) the COSMIN ratingfor the methodological quality of thestudies.57 For each fatigue
FIGURE 1PRISMA flow diagram of study identification and selection. a The sum of the included instruments ishigher than n = 89 because some studies evaluate more than 1 measure.
e1018 CRICHTON et alby guest on April 14, 2017Downloaded from

instrument, the consistency acrossstudies was reviewed for eachmeasurement property. The level ofevidence for the measurementproperties of instruments acrossstudies was rated by using predefinedcriteria of positive, indeterminate, ornegative, accompanied by levels ofevidence, as proposed by theCochrane Back Review Group(Table 1),52 detailed in Table 2.
RESULTS
Figure 1 illustrates the flow of articleselection. A total of 89 studiesmeasuring fatigue by using 20instruments were included in dataextraction and synthesis.4,6,7,11,12,17,20,23–25,27,33,36,38,58–132 One studywas not included in data synthesis formeasurement properties becauseinsufficient information was availablefor data extraction.97
Patient and Study Characteristics
Most reviewed studies were cross-sectional (55; 62%), with a mediansample size of 69 subjects(6–3890). Instruments were used toassess fatigue in children witha number of health conditions(grouped into 14 diagnosticcategories). The most frequentlystudied patient groups werehematology/oncology diagnoses(37; 42%) and chronic fatiguesyndrome (17; 19%; Fig 2).
Identified Instruments
Twenty fatigue instruments wereidentified (Fig 3). The PediatricQuality of Life Inventory (PedsQL)Multidimensional Fatigue Scale (MFS)parent and child report was the mostcommonly used, cited in 26 (29%)and 20 (22%) studies,respectively.20,23–25,27,36,64,65,70,72,74,84,86,93,94,98,100,103,111,115,
116,118,125,126,129,131 The fatiguescales (Fatigue Scale-Child [FS-C];Fatigue Scale-Adolescent [FS-A], andthe Fatigue Scale-Parent [FS-P]) werethe second most commoninstruments to be cited in 18 (20%),16 (18%), and 12 (13%) studies,
respectively.38,61,67,68,75,76,78–83,85,95,107–109,113,128,132
Most (69; 77%) studies assessedfatigue by using 1 or more of 12identified child report instruments,whereas 48 (54%) of includedstudies assessed fatigue by using 1 ormore of 7 identified parent reportinstruments. Five studies (6%)included staff (“other”) report, using1 instrument. Insufficient informationwas available for 1 parent reportquestionnaire.97 Descriptive
information on the child andparent (and other) reportinstruments to assess fatigue arefound in Tables 3 and 4,respectively. See Table 5 forrespondent types within studies.
Respondent type varied across thediagnostic groups of participants; instudies of children with chronicfatigue syndrome, child reportinstruments were exclusively used,whereas studies of children withhematology/oncology diagnoses were
FIGURE 2Child health conditions of patient group in included studies, n (%).
FIGURE 3Fatigue instruments used across identified studies, n (%).
PEDIATRICS Volume 135, number 4, April 2015 e1019by guest on April 14, 2017Downloaded from
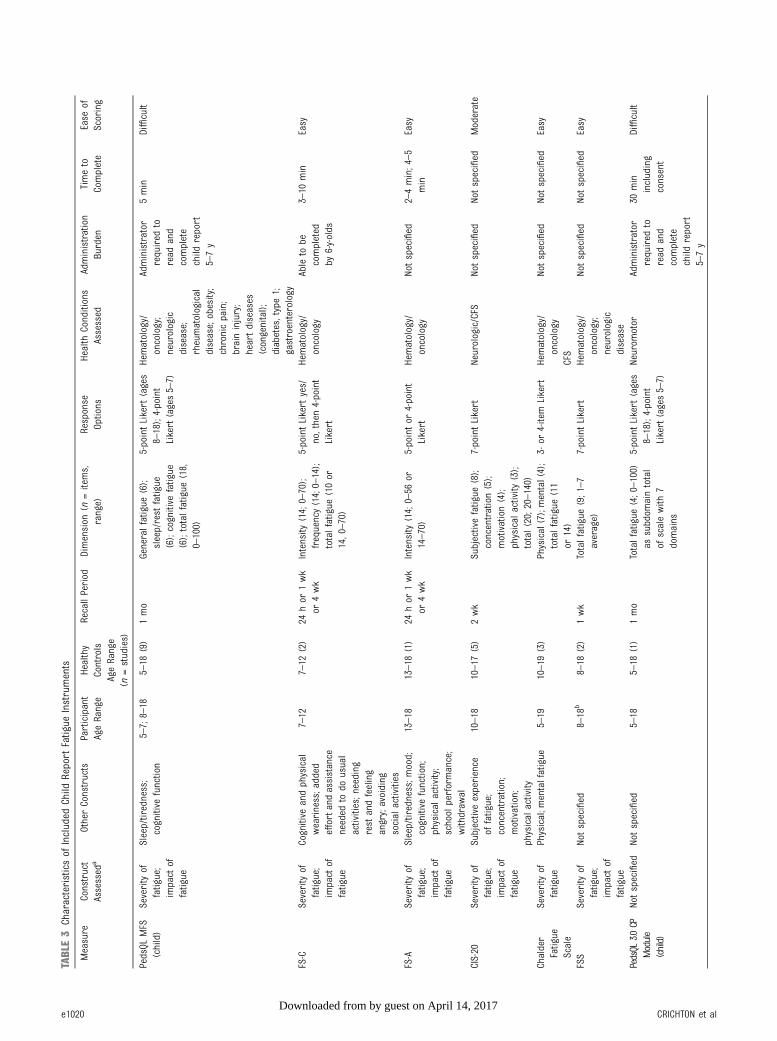
TABLE3
Characteristicsof
Included
Child
Report
Fatigue
Instruments
Measure
Construct
Assessed
aOtherConstructs
Participant
AgeRange
Healthy
Controls
AgeRange
(n=studies)
RecallPeriod
Dimension
(n=items,
range)
Response
Options
Health
Conditions
Assessed
Administration
Burden
Timeto
Complete
Ease
ofScoring
PedsQL
MFS
(child)
Severityof
fatigue;
impact
offatigue
Sleep/tiredness;
cognitive
function
5–7;8–18
5–18
(9)
1mo
Generalfatigue
(6);
sleep/rest
fatigue
(6);cognitive
fatigue
(6);totalfatigue
(18,
0–100)
5-pointLikert
(ages
8–18);4-point
Likert(ages5–7)
Hematology/
oncology;
neurologic
disease;
rheumatological
disease;obesity;
chronicpain;
braininjury;
heartdiseases
(congenital);
diabetes,type1;
gastroenterology
Administrator
required
toread
and
complete
child
report
5–7y
5min
Difficult
FS-C
Severityof
fatigue;
impact
offatigue
Cognitive
andphysical
weariness;added
effortandassistance
needed
todo
usual
activities;needing
rest
andfeeling
angry;avoiding
social
activities
7–12
7–12
(2)
24hor
1wk
or4wk
Intensity
(14;0–70);
frequency(14;0–14);
totalfatigue
(10or
14,0–70)
5-pointLikert
yes/
no,then4-point
Likert
Hematology/
oncology
Ableto
becompleted
by6-y-olds
3–10
min
Easy
FS-A
Severityof
fatigue;
impact
offatigue
Sleep/tiredness;m
ood;
cognitive
function;
physical
activity;
school
performance;
withdraw
al
13–18
13–18
(1)
24hor
1wk
or4wk
Intensity
(14;0–56
or14–70)
5-pointor
4-point
Likert
Hematology/
oncology
Notspecified
2–4min;4–5
min
Easy
CIS-20
Severityof
fatigue;
impact
offatigue
Subjectiveexperience
offatigue;
concentration;
motivation;
physical
activity
10–18
10–17
(5)
2wk
Subjectivefatigue
(8);
concentration(5);
motivation(4);
physical
activity
(3);
total(20;20–140)
7-pointLikert
Neurologic/CFS
Notspecified
Notspecified
Moderate
Chalder
Fatigue
Scale
Severityof
fatigue
Physical;m
entalfatigue
5–19
10–19
(3)
Physical(7);mental(4);
totalfatigue
(11
or14)
3-or
4-item
Likert
Hematology/
oncology
CFS
Notspecified
Notspecified
Easy
FSS
Severityof
fatigue;
impact
offatigue
Notspecified
8–18
b8–18
(2)
1wk
Totalfatigue
(9;1–7
average)
7-pointLikert
Hematology/
oncology;
neurologic
disease
Notspecified
Notspecified
Easy
PedsQL
3.0CP
Module
(child)
Notspecified
Notspecified
5–18
5–18
(1)
1mo
Totalfatigue
(4;0–100)
assubdom
aintotal
ofscalewith
7domains
5-pointLikert
(ages
8–18);4-point
Likert(ages5–7)
Neurom
otor
Administrator
required
toread
and
complete
child
report
5–7y
30min
including
consent
Difficult
e1020 CRICHTON et alby guest on April 14, 2017Downloaded from
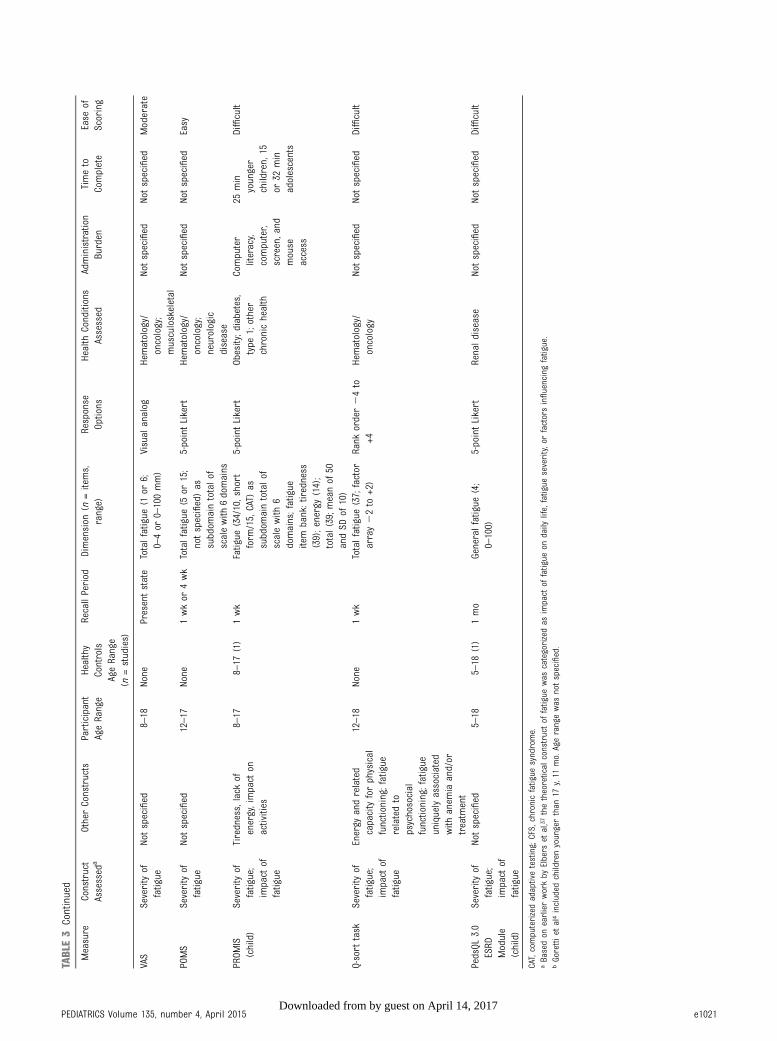
TABLE3
Continued
Measure
Construct
Assessed
aOtherConstructs
Participant
AgeRange
Healthy
Controls
AgeRange
(n=studies)
RecallPeriod
Dimension
(n=items,
range)
Response
Options
Health
Conditions
Assessed
Administration
Burden
Timeto
Complete
Ease
ofScoring
VAS
Severityof
fatigue
Notspecified
8–18
None
Presentstate
Totalfatigue
(1or
6;0–4or
0–100mm)
Visual
analog
Hematology/
oncology;
musculoskeletal
Notspecified
Notspecified
Moderate
POMS
Severityof
fatigue
Notspecified
12–17
None
1wkor
4wk
Totalfatigue
(5or
15;
notspecified)as
subdom
aintotalof
scalewith
6domains
5-pointLikert
Hematology/
oncology;
neurologic
disease
Notspecified
Notspecified
Easy
PROM
IS(child)
Severityof
fatigue;
impact
offatigue
Tiredness,lack
ofenergy,impact
onactivities
8–17
8–17
(1)
1wk
Fatigue
(34/10,short
form
/15,CAT)
assubdom
aintotalof
scalewith
6domains;fatigue
item
bank:tiredness
(39);energy(14);
total(39;m
eanof
50andSD
of10)
5-pointLikert
Obesity;diabetes,
type
1;other
chronichealth
Computer
literacy,
computer,
screen,and
mouse
access
25min
younger
children,15
or32
min
adolescents
Difficult
Q-sort
task
Severityof
fatigue;
impact
offatigue
Energy
andrelated
capacityforphysical
functioning;fatigue
relatedto
psychosocial
functioning;fatigue
uniquelyassociated
with
anem
iaand/or
treatm
ent
12–18
None
1wk
Totalfatigue
(37;factor
array22to
+2)
Rank
order24to
+4Hematology/
oncology
Notspecified
Notspecified
Difficult
PedsQL
3.0
ESRD
Module
(child)
Severityof
fatigue;
impact
offatigue
Notspecified
5–18
5–18
(1)
1mo
Generalfatigue
(4;
0–100)
5-pointLikert
Renaldisease
Notspecified
Notspecified
Difficult
CAT,computerizedadaptivetesting;CFS,chronicfatigue
syndrome.
aBasedon
earlierworkby
Elbers
etal,37
thetheoretical
constructof
fatigue
was
categorizedas
impact
offatigue
ondaily
life,fatigue
severity,orfactorsinfluencingfatigue.
bGorettiet
al4included
childrenyoungerthan
17y,11
mo.Agerangewas
notspecified.
PEDIATRICS Volume 135, number 4, April 2015 e1021by guest on April 14, 2017Downloaded from

TABLE4
Characteristicsof
Included
Parent
andOtherReport
Fatigue
Instruments
Measure
Construct
Assessed
aOtherConstructs
Participant
AgeRange
Healthy
Controls
AgeRange
(n=studies)
Recall
Period
Dimension
(n=Items,
Range)
Response
Options
Health
Conditions
Assessed
Administration
Burden
Timeto
Complete
Ease
ofScoring
PedsQL
MFS
(parent)
Severityof
fatigue;
impact
offatigue
Sleepand
tiredness;
cognitive
function
2–18
2–18
(11)
1mo
Generalfatigue
(6);sleep/
restfatigue
(6);cognitive
fatigue
(6)(total
=18;
0–100)
5-pointLikert
Hematology/oncology;
neurologicdisease;
rheumatologicaldisease;
obesity;chronicpain;
braininjury;heart
diseases
(congenital);
diabetes,type1;
gastroenterology
Notspecified
5min
Difficult
FS-P
Severityof
fatigue;
impact
offatigue
Cognitive
and
physical
weariness;effort
andassistance
needed
todo
usualactivities;
needingrestand
feelingangry;
avoiding
social
activities
7–18
7–18
(2)
24hor
1wk
Intensity
(14,17,or18
items;14–17
or18–90);
total(18;17–85
or0–68)
5-pointLikert
Hematology/oncology
Notspecified
Notspecified
Easy
PedsQL
3.0CP
Module
(parent)
Notspecified
Notspecified
2–18
2–18
(1)
1mo
Totalfatigue
(4;0–100)
assubdom
aintotalofscale
with
7domains
5-pointLikert
Neurom
otor
Notspecified
30min
including
consent
Dif ficult
PROM
IS(parent)
Severityof
fatigue;
impact
offatigue
Tiredness;lack
ofenergy;impact
onactivities
5–18
1wk
Lack
ofenergy
(11);
tiredness
(23);total
fatigue
(34)
(meanof
50,
SDof
10)
5-pointLikert
or4-point
Likert
(physical
health)
Otherchronichealth
Computer
literacy;
computer
screen;
mouse
access
12–22
min
(PROMIS
I);30–40
min
(PROMIS
II)all
domains
Difficult
EOSQ
Severityof
fatigue
Lack
ofenergy
1–12
4wk
Totalfatigue
(2;n
otspecified)subdom
ainof
scalewith
13domains
5-pointLikert
Musculoskeletal
Notspecified
Notspecified
Difficult
FACIT-F
(modified
parent)
Severityof
fatigue;
impact
offatigue
Notspecified
2–18
1wk
Totalfatigue
(13;0–52)as
subdom
aintotalofscale
with
5domains
5-pointLikert
Hematology/oncology
Notspecified
Notspecified
Easy
PedsQL
ESRD
(parent)
Severityof
fatigue;
impact
offatigue
Notspecified
2–18
1mo
Generalfatigue
(4;0–100)
5-pointLikert
Renaldisease
Notspecified
Notspecified
Difficult
FS-S
Severityof
fatigue;
impact
offatigue
Notspecified
7–18
7–18
(1)
24hor
1wk
Fatigue
intensity
(9,10or
18;9–36)
4-pointLikert
Hematology/oncology
Notspecified
Notspecified
Easy
aBasedon
earlierworkby
Elbers
etal,37
thetheoretical
constructof
fatigue
was
categorizedas
impact
offatigue
ondaily
life,fatigue
severity,orfactorsinfluencingfatigue.
e1022 CRICHTON et alby guest on April 14, 2017Downloaded from

unique in using staff-ratedinstruments (Fig 3).
Dimensions of Fatigue Assessed
Most instruments assessed impact offatigue on daily life and fatigueseverity (14; 70%). Few (4; 20%)assessed fatigue severity symptomsonly, and no instruments assessedimpact of fatigue on daily life inisolation. Although item contentrelated to these dimensions, scoringrarely reflected the dimensionality ofthe constructs assessed, and items formost instruments (14; 70%) weresummed into a total fatigue score.A minority (6; 30%) consisted ofscores for multiple fatigue dimensions:5 child-report measures summeditems into 2 to 4 dimensions, and1 parent report measure summed itemsinto fatigue dimensions (3). There wasinsufficient information on itemcontent for 2 instruments (10%).
Developmental Framework
Overall, participant age was skewedtoward children 12 years and older(Fig 4). Healthy control participantswere included in 23 of 81 studies forwhich age range could be extracted(29%). Self-report of fatigue ischallenging in younger children, andonly 4 (33%) child report instrumentswere identified in use between 5 and7 years of age. Greater administrationburden was commonly noted becauseitems need to be read aloud tochildren or administrators need to beavailable to note children’s verbalresponses. In contrast, 4 (57%) parentreport instruments were identified toassess fatigue symptoms in children asyoung as 2 years of age.
Synthesis of Results
Psychometric Properties
A synthesis summary of theinvestigated methodological
properties of measures andmethodological quality of theincluded studies is provided inTable 6. Full details of the resultantCOSMIN ratings for each study (permeasurement property andquestionnaire) are provided inSupplemental Tables 7–26. Thequality of evidence available acrossquestionnaires varied bymeasurement properties as shown,and no single instrumentdemonstrated positive findings acrossall properties. Content validity wasrated for all instruments and revealedthe most promising evidence.Although assessed in severalinstruments, poor results were foundfor internal consistency. This wasprimarily because studies did not testfor unidimensionality (factoranalysis), or because despitecompleting factor analysis andevidence of more than 1 factor, itemswere summarized into a single score.Cultural validity was not considered,and COSMIN items were used to ratethe quality of the translation acrossall studies with cultural validity data.Few studies revealed informationabout measurement error, reliability,or responsiveness. There was limitedevidence of the floor and ceilingeffects across studies, with ,5% ofincluded studies providinginformation.
There was robust evidence for themeasurement properties of thePedsQL MFS and the FS-C/FS-P. ThePedsQL MFS (child and parentversions) was the only includedinstrument to have strong evidence ofreliability, and the only instrument tohave strong evidence acrossa number of dimensions ofassessment. There were positiveratings for reliability, content validity,and hypothesis testing for the PedsQLMFS. Despite the overall rating forreliability, internal consistencycoefficient (ICC) values varied acrossdifferent populations assessed fromlow to high (eg, 0.27–0.93 for totalfatigue).23,125 Additionally, variabilitywith age has been noted.64 There was
limited evidence for the structuralvalidity of the child version fittinga bifactor model (3 subscales: generalfatigue, sleep-rest fatigue, andcognitive fatigue and a total fatiguescore),122 lending new support toprevious research finding good toexcellent internal consistencystatistics (Cronbach a values between0.70 and 0.95). Strong evidence forhypothesis testing validity for thePedsQL MFS was evident, althoughinternal consistency andmeasurement error of the PedsQLMFS require further research. Thedata for these measurementproperties were gathered in childrenwith numerous health conditions,noted in Tables 3 and 4.
The FS-C, FS-A, and FS-P (standardand 24-hour formats) demonstratedrobust measurement properties,notably content validity. There wasmoderate evidence for the structuralvalidity of the child and parent forms,but limited evidence for thestructural validity of the adolescentform. Internal consistency andreliability data were mixed; althoughinternal consistency statistics weregood (0.70 or greater),79–81,107,113
these statistics were calculated basedon the total fatigue scores, despitefindings of a 3-factor model for theFS-C and a 4-factor model for the FS-A.79,80 One study revealed adequatereliability statistics for the FS-A,presenting pooled data from a seriesof studies, and variable agreementbetween parent and child were foundacross included studies (ICC values0.13–0.65).79 The Fatigue Scale-Staff(FS-S) demonstrated moderateevidence for internal consistency andcontent validity and limited evidencefor structural validity.38,68,75,79 Theassessed evidence for FS-C, FS-A, andFS-P was gathered exclusively instudies of children with hematology/oncology diagnoses, limitinggeneralizability of findings to otherhealth conditions.
The Patient-Reported OutcomesMeasurement Information System
TABLE 5 Respondent Types Within Studies
Respondent No. (%) of Studies
Child only 36 (40)Child and parent 33 (37)Parent only 15 (17)
PEDIATRICS Volume 135, number 4, April 2015 e1023by guest on April 14, 2017Downloaded from

(PROMIS)77,88,89,114,123 is a newlydeveloped outcome measure (fatiguesubscale). Among identified studies,those that used PROMIS were theonly ones to employ item responsetheory for statistical analysis. Morepublished information was availablefor the child version, with positiveratings evident for content validityand hypothesis testing. However,there were also some positive
findings for the content and validityof the PROMIS parent report. Overall,properties were given largelyindeterminate ratings because themeasurement properties have not yetbeen evaluated. Evidence wasgathered in study populations ofchildren with mixed healthconditions.
There was limited evidence forhypothesis testing validity of the
Checklist Individual Strength-20 (CIS-20)7,17,101,102,117,119–121 in childrenwith neurologic disorders and chronicfatigue syndrome. Overall findings forthe scale were equivocal.
Some disease-specific instrumentsdemonstrated positive ratings forcontent validity in these specificpopulations (eg, the PedsQL 3.0Cerebral Palsy Module [PedsQL 3.0CP Module]11,12 and the Early Onset
FIGURE 4Age range representation for clinical and healthy participants in included studies (proportion of studies, %). Mean age data for participants set out for81 studies; no mean age participant data reported for 8 studies. Mean age data for controls set out for 26 studies; no mean age control data reported for63 studies.
TABLE 6 Levels of Evidence for the Overall Quality of the Measurement Property per Instrument
Instrument Namea InternalConsistency
Reliability MeasurementError
ContentValidity
StructuralValidity
HypothesisTesting
Cross CulturalValidity
Responsiveness
PedsQL MFS (parent) ? +++ ? +++ ? +++ + ?PedsQL MFS (child) ? +++ ? +++ + +++ + ?FS-C or FS-C 24 h 2 ? ? +++ ++ + + ?FS-A or FS-A 24 h ? 2 ? +++ + + ? ?FS-P or FS-P 24 h ? ? ? +++ ++ + + ?FS-S ++ ? ? ++ + ? ? ?Chalder Fatigue Scale ? ? ? ? ? 2 ? ?CIS-20 ? ? ? ? ? + ? ?PROMIS (child) ? + ? +++ ? ++ ? ?PROMIS (parent) ? ? ? ++ ? ? ? ?FSS ? ? ? ? ? 2 ? ?PedsQL 3.0 CP Module (parent) ? 2 ? ++ ? +/2 ? ?PedsQL 3.0 CP Module (child) ? ? ? + ? + ? ?VAS ? ? ? ? ? ? ? ?POMS ? ? ? ? ? ? ? ?FACIT-F (modified parent) + ? ? + ? ? ? ?Q-sort ? ? ? + ? ? ? ?PedsQL ESRD (parent) ? ? ? + ? ? ? ?PedsQL ERSD (child) ? ? ? + ? ? ? ?EOSQ (parent) ? ? ? ++ ? ? ? ?a Strong +++ or222, Consistent findings in multiple studies of good methodological quality or in 1 study of excellent methodological quality; Moderate ++ or22, Consistent findingsin multiple studies of fair methodological quality or in 1 study of good methodological quality; Limited + or 2, 1 study of fair methodological quality; Conflicting +/2, Conflicting findings;Unknown ?, Only studies of poor methodological quality.
e1024 CRICHTON et alby guest on April 14, 2017Downloaded from

Scoliosis Questionnaire [EOSQ]),62,127
although lacked other evidence forthe quality of their measurementproperties. However, the majority ofincluded instruments demonstratedlow ratings overall. There was limitedevidence for the content validity ofthe Pediatric Functional Assessmentof Chronic Illness Therapy-Fatigue(FACIT-F)33,69,92 and the Q-sort92
instruments for use in hematology/oncology populations, despite nopublished evidence for other assessedmeasurement properties. There wasno positive evidence formeasurement properties of theChalder FatigueScale,58,59,63,90,91,96,106 or the FatigueSeverity Scale (FSS),4,6,73,87 used inchildren with chronic fatiguesyndrome. Often these studies did notreport on measurement properties.There was also no published evidencefor the measurement properties ofthe Profile of Mood States (POMS;hematology/oncology andneurology),104,109 the PedsQL EndStage Renal Disease Module (PedsQLERSD) parent or child (renaldisease),62,71,105,127 nor the includedVASs (hematology/oncology andmusculoskeletal illnesses).66,112
Risk of Bias
Risk of bias was identified acrossstudies for several instruments, dueto reanalysis of participant dataacross studies, including PedsQLMFS,23–25,36,72,93,125 the FatigueScales (child, parent, andadolescent),81,82 and the CIS-20.119,120 Repeated analysis of groupdata possibly skews findings andlimits the generalizability of findingsto other populations. Further,although declared, a primaryresearcher holds the copyright for thePedsQL including PedsQL MFS,23,25,27
PedsQL 3.0 CP Module,11,12 andthe PedsQL ESRD Module.71
DISCUSSION
This study is the first tosystematically review and criticallyappraise fatigue instruments across
the range of childhood chronic healthconditions and ages. Twentyinstruments (12 child reports, 7parent reports, and 1 staff report)were described with reference topatient characteristics (age anddiagnosis), dimensionality of fatigueassessed, and child development. Thisreview provides a thorough andunique review of childhood fatigueinstruments across conditions, usingstandardized published measures toassess the measurement properties ofthese instruments and to assess thequality of the evidence for theseproperties.
In applying COSMIN criteria andassessing the quality of the study,evidence for the measurementproperties of the 20 instruments canbe compared. This review did notidentify any child or parent reportinstrument that met all of the criteria.This appraisal highlights key issues inthe assessment of fatigue inchildhood health conditions. It iswidely acknowledged that asa subjective symptom, fatigue shouldbe assessed by using self report,although developmentalconsiderations necessarily restrict thefeasibility of this in younger children.However, it is important to recognizethe noted lack of robust evidence forreliability. Where ICC values wererecorded, they were often low,indicating lack of agreement betweenchild and parent report onassessment instruments, meaningchild and parent report instrumentscannot be directly compared. It isrecommended that parent and childperspectives be carefully consideredwhen interpreting findings relating tofatigue symptoms in children.
Over 14 health conditions wereidentified as experiencing symptomsof fatigue; however, evidence forinstruments varied across theseconditions. Findings from this reviewsuggest that evidence is limited toinstruments that assess fatigue inchildren with hematology/oncology,and other health conditions.
Specifically, there was support forthe measurement properties of thePedsQL MFS, and limited evidencefor the PROMIS instrument inchildren with a range of chronichealth conditions, and for the FS-C,FS-P, and the FS-A in children withcancer. Evidence for instrumentproperties in children with chronicfatigue syndrome was lacking,despite the high proportion ofstudies with this population. Further,although literature suggests the lowthreshold of fatigue symptomsdistinguishes this clinicalcondition,133 no reviewedinstruments assessed this. Practicingclinicians should be aware thatfatigue can arise from many causesand conditions, and awareness of theunderlying disorder and relevantclinical features is critical toselecting the appropriate validassessment tool.
Whether fatigue should beconceptualized as unidimensional ormultidimensional has been a matterof considerable debate, and evidentlymeasurement of fatigue is a complexissue. Descriptive findings suggestthat this issue is poorly managedby currently available fatigueinstruments. Notably, studies failedto confirm the number of fatiguedimensions (by factor analysis orother methods), or assessment offatigue was conducted by usinginstruments in which the number ofscales did not correspond to thenumber of dimensions identified infactor analysis. For example, of thequestionnaires with the most robustpsychometric properties and studyquality, scores are summed to 3dimensions for the PedsQL MFS, anda total score for the fatigue scales(FS-C, FS-A, and FS-P). However, thereis evidence from factor analysis thatboth instruments are explained by3 to 4 factors.79,80,122 Studies beyondthe scope of this review furthersuggest multiple factors in fatigueassessment instruments, with recentevidence confirming a 3-factorstructure of the PedsQL MFS,134 and
PEDIATRICS Volume 135, number 4, April 2015 e1025by guest on April 14, 2017Downloaded from

a 2-factor structure of the PROMISscale.2 The field of research is yet todevelop a coherent way of relatingthis emerging evidence regardingfatigue dimensionality withquantification of symptoms. Inclinical practice, it is important torecognize the complexity of fatigue,and to move beyond simplisticassessment of the symptom toconsider a multidimensionalapproach to assessment. Cliniciansshould be aware of the differentinformation provided by the range ofassessment instruments.
This review considered child-specificissues relating to fatigue assessment.However, the findings for reviewedfatigue instruments cannot begeneralized across age rangesbecause participants were mainlyolder than 12 years of age, and gapsin the quality of evidence wereidentified at key developmentalstages. It is important to identify theages in which studies have beenperformed because measurementproperties may vary in different ageranges. Few instruments arevalidated for use in younger children,with robust evidence provided onlyby the PedsQL MFS (age range, 2–18years), and limited evidenceprovided by the PedsQL 3.0 CPModule and the EOSQ. There was
limited reference to healthy controlparticipants in included studies. It iscrucial to the determination ofexcessive fatigue that normaldevelopmental differences are takeninto account because fatigue isa symptom that occurs in healthypopulations, and revealsdevelopmental variation.85,128,135
Further studies are required toexamine fatigue expression acrossage groups, including notablyyounger children, and makereference to normal development, tounderstand how age affects theexperience of fatigue.
LIMITATIONS
Limitations of this review includea focus on children 18 years oryounger with different healthconditions. Evidence ofmeasurement properties in use inother populations was notconsidered. For example, despiteseveral of these measures beingdescribed in older or healthychildhood populations, the inclusionof these findings was beyond thescope of this review. Care should betaken when considering thegeneralizability of the findings toother patient groups. Further, thereview was restricted to subjectivemeasures of fatigue and did not
include studies that have attemptedto measure fatigue objectively.
CONCLUSIONS
There are a large number ofinstruments available to measurefatigue across a range of childhoodhealth conditions, yet there is limitedevidence for their utility. There wasbest evidence for the use of thePedsQL MFS (parent and child report)in a range of pediatric chronic healthconditions across childhood, and theFS-C, FS-A, and FS-P in children withcancer of school age. Use of otherinstruments should be limited toresearch into the validity of theinstrument, not patient outcomes.Further data are required to supportthe measurement properties ofinstruments used to assess fatigue inchildren with chronic fatiguesyndrome, to identify appropriatetools to assess fatigue in childrenyounger than school age, and toclarify the nature of agreementbetween child and proxy reportacross developmental stages.
ACKNOWLEDGMENT
We thank Poh Chua, DeputyLibrarian, RCH, Melbourne, for herhelp in use of the EBSCOhost platformand search terms.
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: Supported in part by a Moving Ahead Seed grant, a National Health and Medical Research Council Postgraduate Scholarship (Dr Crichton, awarded 2014),
Canberra, Australia, a Neurosciences Victoria Brain and Mind Scholarship, Melbourne, Australia (Dr Crichton, awarded 2012), and the Victorian Government
Operations Infrastructure Scheme.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
REFERENCES
1. Levine J, Greenwald BD. Fatigue inParkinson disease, stroke, andtraumatic brain injury. Phys MedRehabil Clin N Am. 2009;20(2):347–361
2. Lai J-S, Stucky BD, Thissen D, et al.Development and psychometricproperties of the PROMIS(®) pediatricfatigue item banks. Qual Life Res. 2013;22(9):2417–2427
3. Bottomley S, Teegarden C, Hockenberry-Eaton M. Fatigue in children with cancer:clinical considerations for nursing.J Pediatr Oncol Nurs. 1996;13(3):178
4. Goretti B, Ghezzi A, Portaccio E, et al;Study Group of the Italian NeurologicalSociety. Psychosocial issue in childrenand adolescents with multiplesclerosis. Neurol Sci. 2010;31(4):467–470
5. Goretti B, Portaccio E, Ghezzi A, et al;Multiple Sclerosis Study Group of theItalian Neurological Society. Fatigue andits relationships with cognitivefunctioning and depression inpaediatric multiple sclerosis. MultScler. 2012;18(3):329–334
6. Amato MP, Goretti B, Ghezzi A, et al;Multiple Sclerosis Study Group of theItalian Neurological Society. Cognitive
e1026 CRICHTON et alby guest on April 14, 2017Downloaded from

and psychosocial features of childhoodand juvenile MS. Neurology. 2008;70(20):1891–1897
7. Ketelslegers IA, Catsman-Berrevoets CE,Boon M, et al. Fatigue and depression inchildren with multiple sclerosis andmonophasic variants. Eur J PaediatrNeurol. 2010;14(4):320–325
8. Eddy L, Cruz M. The relationshipbetween fatigue and quality of life inchildren with chronic health problems:a systematic review. J Spec PediatrNurs. 2007;12(2):105–114
9. Schönberger M, Herrberg M, PonsfordJ. Fatigue as a cause, nota consequence of depression anddaytime sleepiness: a cross-laggedanalysis. J Head Trauma Rehabil. 2014;29(5):427–431
10. Carter BD, Edwards JF, KronenbergerWG, Michalczyk L, Marshall GS. Casecontrol study of chronic fatigue inpediatric patients. Pediatrics. 1995;95(2):179–186
11. Varni JW, Burwinkle TM, Berrin SJ, et al.The PedsQL in pediatric cerebral palsy:reliability, validity, and sensitivity of theGeneric Core Scales and Cerebral PalsyModule. Dev Med Child Neurol. 2006;48(6):442–449
12. Berrin SJ, Malcarne VL, Varni JW, et al.Pain, fatigue, and school functioning inchildren with cerebral palsy: a path-analytic model. J Pediatr Psychol. 2007;32(3):330–337
13. Crawley EM, Emond AM, Sterne JAC.Unidentified Chronic Fatigue Syndrome/myalgic encephalomyelitis (CFS/ME) isa major cause of school absence:surveillance outcomes from school-based clinics. BMJ Open. 2011;1(2):e000252
14. Wolfe J, Grier HE, Klar N, et al.Symptoms and suffering at the end oflife in children with cancer. N Engl JMed. 2000;342(5):326–333
15. Jalmsell L, Kreicbergs U, Onelöv E,Steineck G, Henter JI. Symptomsaffecting children with malignanciesduring the last month of life:a nationwide follow-up. Pediatrics.2006;117(4):1314–1320
16. Nutini M, Karczewski M, Capoor J.Fatigue in children with neurologicimpairments. Phys Med Rehabil Clin NAm. 2009;20(2):339–346
17. Nijhof SL, Maijer K, Bleijenberg G,Uiterwaal CSPM, Kimpen JLL, van dePutte EM. Adolescent chronic fatiguesyndrome: prevalence, incidence, andmorbidity. Pediatrics. 2011;127(5).Available at: www.pediatrics.org/cgi/content/full/127/5/e1169
18. Jarjour IT. Postural tachycardiasyndrome in children and adolescents.Semin Pediatr Neurol. 2013;20(1):18–26
19. Elliott IM, Lach L, Smith ML. I just wantto be normal: a qualitative studyexploring how children and adolescentsview the impact of intractable epilepsyon their quality of life. Epilepsy Behav.2005;7(4):664–678
20. Limond J, Dorris L, McMillan TM. Qualityof life in children with acquired braininjury: parent perspectives 1-5 yearsafter injury. Brain Inj. 2009;23(7):617–622
21. Butbul Aviel Y, Stremler R, Benseler SM,et al. Sleep and fatigue and therelationship to pain, disease activityand quality of life in juvenile idiopathicarthritis and juvenile dermatomyositis.Rheumatology (Oxford). 2011;50(11):2051–2060
22. Lévy-Marchal C, Papoz L, de Beaufort C,et al. Clinical and laboratory features oftype 1 diabetic children at the time ofdiagnosis. Diabet Med. 1992;9(3):279–284
23. Varni JW, Limbers CA, Bryant WP,Wilson DP. The PedsQLMultidimensional Fatigue Scale in type1 diabetes: feasibility, reliability, andvalidity. Pediatr Diabetes. 2009;10(5):321–328
24. Marcus SB, Strople JA, Neighbors K,et al. Fatigue and health-related qualityof life in pediatric inflammatory boweldisease. Clin Gastroenterol Hepatol.2009;7(5):554–561
25. Varni JW, Burwinkle TM, Limbers CA,Szer IS. The PedsQL as a patient-reported outcome in children andadolescents with fibromyalgia: ananalysis of OMERACT domains. HealthQual Life Outcomes. 2007;5:9
26. Buskila D. Pediatric fibromyalgia.Rheum Dis Clin North Am. 2009;35(2):253–261
27. Varni JW, Limbers CA, Bryant WP, WilsonDP. The PedsQL multidimensionalfatigue scale in pediatric obesity:
feasibility, reliability and validity. Int JPediatr Obes. 2010;5(1):34–42
28. Kluger BM, Krupp LB, Enoka RM. Fatigueand fatigability in neurologic illnesses:proposal for a unified taxonomy.Neurology. 2013;80(4):409–416
29. North American Nursing DiagnosisAssociation. Nursing Diagnoses:Definition and Classification,1997–1998. Philadelphia, PA: McGraw-Hill; 1996
30. Chaudhuri A, Behan PO. Fatigue andbasal ganglia. J Neurol Sci. 2000;179(1–2):34–42
31. DeLuca J. Fatigue: its definition, itsstudy and its future. In: DeLuca J, ed.Fatigue as a Window to the Brain.Cambridge, MA: MIT Press; 2005:319–325
32. Christodoulou C. The assessment andmeasurement of fatigue. In: DeLuca J,ed. Fatigue as a Window to the Brain.Cambridge, MA: MIT Press; 2005:19–35
33. Lai J-S, Cella D, Kupst MJ, et al.Measuring fatigue for children withcancer: development and validation ofthe pediatric Functional Assessment ofChronic Illness Therapy-Fatigue(pedsFACIT-F). J Pediatr Hematol Oncol.2007;29(7):471–479
34. Cella D, Lai J-S, Stone A. Self-reportedfatigue: one dimension or more?Lessons from the FunctionalAssessment of Chronic Illness Therapy—Fatigue (FACIT-F) questionnaire.Support Care Cancer. 2011;19(9):1441–1450
35. Chalder T, Berelowitz G, Pawlikowska T,et al. Development of a fatigue scale.J Psychosom Res. 1993;37(2):147–153
36. Varni JW, Burwinkle TM, Katz ER,Meeske K, Dickinson P. The PedsQL inpediatric cancer: reliability and validityof the Pediatric Quality of Life InventoryGeneric Core Scales, MultidimensionalFatigue Scale, and Cancer Module.Cancer. 2002;94(7):2090–2106
37. Elbers RG, Rietberg MB, van Wegen EEH,et al. Self-report fatigue questionnairesin multiple sclerosis, Parkinson’sdisease and stroke: a systematic reviewof measurement properties. Qual LifeRes. 2012;21(6):925–944
38. Hockenberry MJ, Hinds PS, Barrera P,et al. Three instruments to assessfatigue in children with cancer: the
PEDIATRICS Volume 135, number 4, April 2015 e1027by guest on April 14, 2017Downloaded from

child, parent and staff perspectives.J Pain Symptom Manage. 2003;25(4):319–328
39. Hockenberry-Eaton M, Hinds P, O’NeillJB, et al. Developing a conceptualmodel for fatigue in children... includingcommentary by Eiser C and Enskar K.Eur J Oncol Nurs. 1999;3(1):5–13
40. Hockenberry-Eaton M, Hinds PS, AlcoserP, et al. Fatigue in children andadolescents with cancer. J PediatrOncol Nurs. 1998;15(3):172–182
41. Hockenberry-Eaton M, Hinds PS. Fatiguein children and adolescents withcancer: evolution of a program of study.Semin Oncol Nurs. 2000;16(4):261–272,discussion 272–278
42. Eiser C, Morse R. Can parents rate theirchild’s health-related quality of life?Results of a systematic review. Qual LifeRes. 2001;10(4):347–357
43. Hiscock H, Canterford L, Ukoumunne OC,Wake M. Adverse associations of sleepproblems in Australian preschoolers:national population study. Pediatrics.2007;119(1):86–93
44. Haines LC, Saidi G, Cooke RWI.Prevalence of severe fatigue in primarycare. Arch Dis Child. 2005;90(4):367–368
45. ter Wolbeek M, van Doornen LJP,Kavelaars A, Heijnen CJ. Severe fatiguein adolescents: a commonphenomenon? Pediatrics. 2006;117(6).Available at: www.pediatrics.org/cgi/content/full/117/6/e1078
46. Tomlinson D, Hinds PS, Ethier M-C, NessKK, Zupanec S, Sung L. Psychometricproperties of instruments used tomeasure fatigue in children andadolescents with cancer: a systematicreview. J Pain Symptom Manage. 2013;45(1):83–91
47. Minton O, Stone P. A systematic reviewof the scales used for the measurementof cancer-related fatigue (CRF). AnnOncol. 2009;20(1):17–25
48. Haywood KL, Staniszewska S, ChapmanS. Quality and acceptability of patient-reported outcome measures used inchronic fatigue syndrome/myalgicencephalomyelitis (CFS/ME):a systematic review. Qual Life Res. 2012;21(1):35–52
49. Moher D, Liberati A, Tetzlaff J, AltmanDG; PRISMA Group. Preferred reportingitems for systematic reviews and meta-
analyses: the PRISMA statement. J ClinEpidemiol. 2009;62(10):1006–1012
50. Alberani V, De Castro Pietrangeli P,Mazza AM. The use of grey literature inhealth sciences: a preliminary survey.Bull Med Libr Assoc. 1990;78(4):358–363
51. Higgins JPT, Green S. CochraneHandbook for Systematic Reviews ofInterventions. The CochraneCollaboration; 2011
52. van Tulder M, Furlan A, Bombardier C,Bouter L; Editorial Board of theCochrane Collaboration Back ReviewGroup. Updated method guidelines forsystematic reviews in the Cochranecollaboration back review group. Spine.2003;28(12):1290–1299
53. Aaronson N, Alonso J, Burnam A, et al.Assessing health status and quality-of-life instruments: attributes and reviewcriteria. Qual Life Res. 2002;11(3):193–205
54. Mokkink LB, Terwee CB, Patrick DL, et al.The COSMIN checklist for assessing themethodological quality of studies onmeasurement properties of healthstatus measurement instruments: aninternational Delphi study. Qual LifeRes. 2010;19(4):539–549
55. Terwee CB, Bot SDM, de Boer MR, et al.Quality criteria were proposed formeasurement properties of healthstatus questionnaires. J Clin Epidemiol.2007;60(1):34–42
56. Mokkink LB, Terwee CB, Patrick DL,et al. The COSMIN study reachedinternational consensus ontaxonomy, terminology, anddefinitions of measurementproperties for health-related patient-reported outcomes. J Clin Epidemiol.2010;63(7):737–745
57. Terwee CB, Mokkink LB, Knol DL, OsteloRWJG, Bouter LM, de Vet HCW. Ratingthe methodological quality insystematic reviews of studies onmeasurement properties: a scoringsystem for the COSMIN checklist. QualLife Res. 2012;21(4):651–657
58. Bould H, Collin SM, Lewis G, Rimes K,Crawley E. Depression in paediatricchronic fatigue syndrome. Arch DisChild. 2013;98(6):425–428
59. Chalder T, Tong J, Deary V. Familycognitive behaviour therapy for chronic
fatigue syndrome: an uncontrolledstudy. Arch Dis Child. 2002;86(2):95–97
60. Chiang Y-C, Hinds PS, Yeh C-H, Yang C-P,Srivastava DK. Reliability and validity ofthe Chinese version of the FatigueScale-Adolescent. Cancer Nurs. 2008;31(3):E1–E8
61. Chiang YC, Hinds PS, Yeh CH, Yang CP.Development and psychometric testingof a Chinese version of the FatigueScale-Children in Taiwan. J Clin Nurs.2008;17(9):1201–1210
62. Corona J, Matsumoto H, Roye DP, VitaleMG. Measuring quality of life in childrenwith early onset scoliosis: developmentand initial validation of the early onsetscoliosis questionnaire. J PediatrOrthop. 2011;31(2):180–185
63. Crawley E, Hunt L, Stallard P. Anxiety inchildren with CFS/ME. Eur Child AdolescPsychiatry. 2009;18(11):683–689
64. Dampier C, Lieff S, LeBeau P, et al;Comprehensive Sickle Cell Centers(CSCC) Clinical Trial Consortium (CTC).Health-related quality of life in childrenwith sickle cell disease: a report fromthe Comprehensive Sickle Cell CentersClinical Trial Consortium. Pediatr BloodCancer. 2010;55(3):485–494
65. Dieruf K, Burtner PA, Provost B, PhillipsJ, Bernitsky-Beddingfield A, Sullivan KJ.A pilot study of quality of life inchildren with cerebral palsy afterintensive body weight-supportedtreadmill training. Pediatr Phys Ther.2009;21(1):45–52
66. Gedaly-Duff V, Lee KA, Nail L, NicholsonHS, Johnson KP. Pain, sleepdisturbance, and fatigue in childrenwith leukemia and their parents:a pilot study. Oncol Nurs Forum. 2006;33(3):641–646
67. Ekti Genc R, Conk Z. Impact of effectivenursing interventions to the fatiguesyndrome in children who receivechemotherapy. Cancer Nurs. 2008;31(4):312–317
68. Gerçeker GÖ, Yilmaz HB. Reliability andvalidity of Turkish versions of the child,parent and staff cancer fatigue scales.Asian Pac J Cancer Prev. 2012;13(7):3135–3141
69. Gibson F, Garnett M, Richardson A,Edwards J, Sepion B. Heavy to carry:a survey of parents’ and healthcareprofessionals’ perceptions of
e1028 CRICHTON et alby guest on April 14, 2017Downloaded from

cancer-related fatigue in children andyoung people. Cancer Nurs. 2005;28(1):27–35
70. Gold JI, Mahrer NE, Yee J, Palermo TM.Pain, fatigue, and health-related qualityof life in children and adolescents withchronic pain. Clin J Pain. 2009;25(5):407–412
71. Goldstein SL, Graham N, Warady BA,et al. Measuring health-related qualityof life in children with ESRD:performance of the generic and ESRD-specific instrument of the PediatricQuality of Life Inventory (PedsQL). Am JKidney Dis. 2008;51(2):285–297
72. Gordijn MS, van Litsenburg RR, GemkeRJ, et al. Sleep, fatigue, depression, andquality of life in survivors of childhoodacute lymphoblastic leukemia. PediatrBlood Cancer. 2013;60(3):479–485
73. Gordon B, Lubitz L. Promising outcomesof an adolescent chronic fatiguesyndrome inpatient programme.J Paediatr Child Health. 2009;45(5):286–290
74. Harder LL, Holland AA, Frohman E,Graves D, Greenberg BM. Cognitivefunctioning in pediatric transversemyelitis. Mult Scler. 2013;19(7):947–952
75. Hinds PS, Hockenberry M, Rai SN, et al.Clinical field testing of an enhanced-activity intervention in hospitalizedchildren with cancer. J Pain SymptomManage. 2007;33(6):686–697
76. Hinds PS, Hockenberry MJ, Gattuso JS,et al. Dexamethasone alters sleep andfatigue in pediatric patients with acutelymphoblastic leukemia. Cancer. 2007;110(10):2321–2330
77. Hinds PS, Nuss SL, Ruccione KS, et al.PROMIS pediatric measures in pediatriconcology: valid and clinically feasibleindicators of patient-reportedoutcomes. Pediatr Blood Cancer. 2013;60(3):402–408
78. Hinds PS, Hockenberry M, Rai SN, et al.Nocturnal awakenings, sleepenvironment interruptions, and fatiguein hospitalized children with cancer.Oncol Nurs Forum. 2007;34(2):393–402
79. Hinds PS, Hockenberry M, Tong X, et al.Validity and reliability of a newinstrument to measure cancer-relatedfatigue in adolescents. J Pain SymptomManage. 2007;34(6):607–618
80. Hinds PS, Yang J, Gattuso JS, et al.Psychometric and clinical assessmentof the 10-item reduced version of theFatigue Scale-Child instrument. J PainSymptom Manage. 2010;39(3):572–578
81. Hockenberry MJ, Hooke MC, GregurichM, McCarthy K, Sambuco G, Krull K.Symptom clusters in children andadolescents receiving cisplatin,doxorubicin, or ifosfamide. Oncol NursForum. 2010;37(1):E16–E27
82. Hockenberry MJ, Hooke MC, GregurichM, McCarthy K. Carnitine plasma levelsand fatigue in children/adolescentsreceiving cisplatin, ifosfamide, ordoxorubicin. J Pediatr Hematol Oncol.2009;31(9):664–669
83. Hockenberry MJ, Hooke MC, McCarthyK, Gregurich MA. Sickness behaviorclustering in children with cancer.J Pediatr Oncol Nurs. 2011;28(5):263–272
84. Holland AA, Graves D, Greenberg BM,Harder LL. Fatigue, emotionalfunctioning, and executive dysfunctionin pediatric multiple sclerosis. ChildNeuropsychol. 2014;20(1):71–85
85. Hooke MC, Garwick AW, Gross CR.Fatigue and physical performance inchildren and adolescents receivingchemotherapy. Oncol Nurs Forum. 2011;38(6):649–657
86. Huang IC, Anderson M, Gandhi P, et al.The relationships between fatigue,quality of life, and family impactamong children with special healthcare needs. J Pediatr Psychol. 2013;38(7):722–731
87. Huang Y, Katz BZ, Mears C, KielhofnerGW, Taylor R. Postinfectious fatigue inadolescents and physical activity. ArchPediatr Adolesc Med. 2010;164(9):803–809
88. Irwin DE, Gross HE, Stucky BD, et al.Development of six PROMIS pediatricsproxy-report item banks. Health QualLife Outcomes. 2012;10:22
89. Irwin DE, Stucky BD, Thissen D, et al.Sampling plan and patientcharacteristics of the PROMISpediatrics large-scale survey. Qual LifeRes. 2010;19(4):585–594
90. Jóhannsdóttir IM, Hjermstad MJ, MoumT, et al. Increased prevalence of chronicfatigue among survivors of childhoodcancers: a population-based study.
Pediatr Blood Cancer. 2012;58(3):415–420
91. Kawatani J, Mizuno K, Shiraishi S, et al.Cognitive dysfunction and mentalfatigue in childhood chronic fatiguesyndrome—a 6-month follow-up study.Brain Dev. 2011;33(10):832–841
92. Lai J-S, Kupst MJ, Cella D, Brown SR,Peterman A, Goldman S. UsingQ-methodology to understand perceivedfatigue reported by adolescents withcancer. Psychooncology. 2007;16(5):437–447
93. Looman WS, Thurmes AK, O’Conner-VonSK. Quality of life among children withvelocardiofacial syndrome. Cleft PalateCraniofac J. 2010;47(3):273–283
94. MacAllister WS, Christodoulou C, TroxellR, et al. Fatigue and quality of life inpediatric multiple sclerosis. Mult Scler.2009;15(12):1502–1508
95. Mandrell BN, Yang J, Hooke MC, et al.Psychometric and clinical assessmentof the 13-item reduced version of thefatigue scale-adolescent instrument.J Pediatr Oncol Nurs. 2011;28(5):287–294
96. May M, Emond A, Crawley E. Phenotypesof chronic fatigue syndrome in childrenand young people. Arch Dis Child. 2010;95(4):245–249
97. McCarthy AM, Lindgren S, MengelingMA, Tsalikian E, Engvall JC. Effects ofdiabetes on learning in children.Pediatrics. 2002;109(1). Available at:www.pediatrics.org/cgi/content/full/109/1/e9
98. Meeske K, Katz ER, Palmer SN,Burwinkle T, Varni JW. Parent proxy-reported health-related quality of lifeand fatigue in pediatric patientsdiagnosed with brain tumors and acutelymphoblastic leukemia. Cancer. 2004;101(9):2116–2125
99. Menard JC, Hinds PS, Jacobs SS, et al.Feasibility and acceptability of thepatient-reported outcomes measurementinformation system measures in childrenand adolescents in active cancertreatment and survivorship. CancerNurs. 2014;37(1):66–74
100. Mört S, Lähteenmäki PM, Matomäki J,Salmi TT, Salanterä S. Fatigue in youngsurvivors of extracranial childhoodcancer: a Finnish nationwide survey.Oncol Nurs Forum. 2011;38(6):E445–E454
PEDIATRICS Volume 135, number 4, April 2015 e1029by guest on April 14, 2017Downloaded from

101. Nijhof SL, Bleijenberg G, UiterwaalCSPM, Kimpen JLL, van de Putte EM.Effectiveness of internet-basedcognitive behavioural treatment foradolescents with chronic fatiguesyndrome (FITNET): a randomisedcontrolled trial. Lancet. 2012;379(9824):1412–1418
102. Nijhof SL, Priesterbach LP, UiterwaalCSPM, Bleijenberg G, Kimpen JLL, vande Putte EM. Internet-based therapy foradolescents with chronic fatiguesyndrome: long-term follow-up.Pediatrics. 2013;131(6). Available at:www.pediatrics.org/cgi/content/full/131/6/e1788
103. Palmer SN, Meeske KA, Katz ER,Burwinkle TM, Varni JW. The PedsQLBrain Tumor Module: initial reliabilityand validity. Pediatr Blood Cancer. 2007;49(3):287–293
104. Pandina GJ, Ness S, Polverejan E, et al.Cognitive effects of topiramate inmigraine patients aged 12 through 17years. Pediatr Neurol. 2010;42(3):187–195
105. Park K-S, Hwang YJ, Cho MH, et al.Quality of life in children with end-stagerenal disease based on a PedsQL ESRDmodule. Pediatr Nephrol. 2012;27(12):2293–2300
106. Patel MX, Smith DG, Chalder T, WesselyS. Chronic fatigue syndrome inchildren: a cross sectional survey. ArchDis Child. 2003;88(10):894–898
107. Perdikaris P, Merkouris A, Patiraki E,Tsoumakas K, Vasilatou-Kosmidis E,Matziou V. Evaluating cancer relatedfatigue during treatment according tochildren’s, adolescents’ and parents’perspectives in a sample of Greekyoung patients. Eur J Oncol Nurs. 2009;13(5):399–408
108. Perdikaris P, Merkouris A, Patiraki E,Papadatou D, Vasilatou-Kosmidis H,Matziou V. Changes in children’s fatigueduring the course of treatment forpaediatric cancer. Int Nurs Rev. 2008;55(4):412–419
109. Post-White J, Fitzgerald M, Savik K,Hooke MC, Hannahan AB, Sencer SF.Massage therapy for children withcancer. J Pediatr Oncol Nurs. 2009;26(1):16–28
110. Richards J, Turk J, White S. Childrenand adolescents with Chronic FatigueSyndrome in non-specialist settings:
beliefs, functional impairment andpsychiatric disturbance. Eur ChildAdolesc Psychiatry. 2005;14(6):310–318
111. Ringold S, Ward TM, Wallace CA. Diseaseactivity and fatigue in juvenileidiopathic arthritis. Arthritis Care Res(Hoboken). 2013;65(3):391–397
112. Sällfors C, Hallberg LR, Fasth A. Genderand age differences in pain, coping andhealth status among children withchronic arthritis. Clin Exp Rheumatol.2003;21(6):785–793
113. Sanford SD, Okuma JO, Pan J, et al.Gender differences in sleep, fatigue,and daytime activity in a pediatriconcology sample receivingdexamethasone. J Pediatr Psychol.2008;33(3):298–306
114. Selewski DT, Collier DN, MacHardy J,et al. Promising insights into the healthrelated quality of life for children withsevere obesity. Health Qual LifeOutcomes. 2013;11:29
115. Sumpter R, Brunklaus A, McWilliam R,Dorris L. Health-related quality-of-lifeand behavioural outcome in survivorsof childhood meningitis. Brain Inj. 2011;25(13–14):1288–1295
116. Sumpter R, Dorris L, Brannan G,Carachi R. Quality of life andbehavioural adjustment in childhoodhydrocephalus. Scott Med J. 2012;57(1):18–25
117. Takken T, Henneken T, van de Putte E,Helders P, Engelbert R. Exercise testingin children and adolescents withchronic fatigue syndrome. Int J SportsMed. 2007;28(7):580–584
118. Tomlinson D, Hinds PS, Bartels U,Hendershot E, Sung L. Parent reports ofquality of life for pediatric patients withcancer with no realistic chance of cure.J Clin Oncol. 2011;29(6):639–645
119. van de Putte EM, Böcker KB, Buitelaar J,et al. Deficits of interference control inadolescents with chronic fatiguesyndrome. Arch Pediatr Adolesc Med.2008;162(12):1196–1197
120. van de Putte EM, Engelbert RHH, Kuis W,Kimpen JLL, Uiterwaal CSPM.Alexithymia in adolescents with chronicfatigue syndrome. J Psychosom Res.2007;63(4):377–380
121. van Geelen SM, Fuchs CE, Sinnema G,et al. Self-investigation in adolescent
chronic fatigue syndrome: narrativechanges and health improvement.Patient Educ Couns. 2011;83(2):227–233
122. Varni JW, Beaujean AA, Limbers CA.Factorial invariance of pediatric patientself-reported fatigue across age andgender: a multigroup confirmatoryfactor analysis approach utilizing thePedsQL� Multidimensional FatigueScale. Qual Life Res. 2013;22(9):2581–2594
123. Varni JW, Magnus B, Stucky BD, et al.Psychometric properties of the PROMIS® pediatric scales: precision, stability,and comparison of different scoringand administration options. Qual LifeRes. 2014;23(4):1233–1243
124. Varni JW, Thissen D, Stucky BD, et al.PROMIS® Parent Proxy Report Scales forchildren ages 5-7 years: an itemresponse theory analysis of differentialitem functioning across age groups.Qual Life Res. 2014;23(1):349–361
125. Varni JW, Burwinkle TM, Szer IS. ThePedsQL Multidimensional Fatigue Scalein pediatric rheumatology: reliabilityand validity. J Rheumatol. 2004;31(12):2494–2500
126. Verberne LM, Maurice-Stam H,Grootenhuis MA, Van Santen HM,Schouten-Van Meeteren AYN. Sleepdisorders in children after treatmentfor a CNS tumour. J Sleep Res. 2012;21(4):461–469
127. Vitale MG, Corona J, Matsumoto H, et al.Development and initial validation ofa disease specific outcome measure forearly onset scoliosis. Stud HealthTechnol Inform. 2010;158:172–176
128. Whitsett SF, Gudmundsdottir M, DaviesB, McCarthy P, Friedman D.Chemotherapy-related fatigue inchildhood cancer: correlates,consequences, and coping strategies.J Pediatr Oncol Nurs. 2008;25(2):86–96
129. Yeh CH, Man Wai JP, Lin U-S, Chiang Y-C.A pilot study to examine the feasibilityand effects of a home-based aerobicprogram on reducing fatigue inchildren with acute lymphoblasticleukemia. Cancer Nurs. 2011;34(1):3–12
130. Yeh CH, Wang CH, Chiang YC, Lin L, ChienLC. Assessment of symptoms reportedby 10- to 18-year-old cancer patients in
e1030 CRICHTON et alby guest on April 14, 2017Downloaded from

Taiwan. J Pain Symptom Manage. 2009;38(5):738–746
131. Zafar A-B, Ness J, Dowdy S, Avis K,Bashir K. Examining sleep, fatigue, anddaytime sleepiness in pediatric multiplesclerosis patients. Mult Scler. 2012;18(4):481–488
132. Zupanec S, Jones H, Stremler R. Sleephabits and fatigue of children receivingmaintenance chemotherapy for ALL and
their parents. J Pediatr Oncol Nurs.2010;27(4):217–228
133. Carruthers BM, van de Sande MI, DeMeirleir KL, et al. Myalgicencephalomyelitis: InternationalConsensus Criteria. J Intern Med. 2011;270(4):327–338
134. Panepinto JA, Torres S, Bendo CB, et al.PedsQL� Multidimensional FatigueScale in sickle cell disease: feasibility,
reliability, and validity. Pediatr BloodCancer. 2014;61(1):171–177
135. Davies E, Clarke C. Early symptoms ofbrain tumours. J Neurol NeurosurgPsychiatry. 2004;75(8):1205–1206
136. Buckland S, Hayes H, Ostrer C, et alHow to Get Actively Involved in NHS,Public Health, and Social CareResearch. Eastleigh, UK: INVOLVE;2007
PEDIATRICS Volume 135, number 4, April 2015 e1031by guest on April 14, 2017Downloaded from

DOI: 10.1542/peds.2014-2440; originally published online March 23, 2015; 2015;135;e1015Pediatrics
Alison Crichton, Sarah Knight, Ed Oakley, Franz E. Babl and Vicki AndersonInstruments
Fatigue in Child Chronic Health Conditions: A Systematic Review of Assessment
ServicesUpdated Information &
/content/135/4/e1015.full.htmlincluding high resolution figures, can be found at:
Supplementary Material
html/content/suppl/2015/03/17/peds.2014-2440.DCSupplemental.Supplementary material can be found at:
References
/content/135/4/e1015.full.html#ref-list-1free at:This article cites 130 articles, 21 of which can be accessed
Subspecialty Collections
/cgi/collection/evidence-based_medicine_subEvidence-Based Medicinethe following collection(s):This article, along with others on similar topics, appears in
Permissions & Licensing
/site/misc/Permissions.xhtmltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints /site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2015 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by guest on April 14, 2017Downloaded from

DOI: 10.1542/peds.2014-2440; originally published online March 23, 2015; 2015;135;e1015Pediatrics
Alison Crichton, Sarah Knight, Ed Oakley, Franz E. Babl and Vicki AndersonInstruments
Fatigue in Child Chronic Health Conditions: A Systematic Review of Assessment
/content/135/4/e1015.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2015 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by guest on April 14, 2017Downloaded from


















