Fasd Booklet Final Web
22
-
Upload
ebredberg -
Category
Health & Medicine
-
view
2.106 -
download
3
description
Thanks to FNESC and Madeline Price for this resource. Liz
Transcript of Fasd Booklet Final Web


This booklet was written to provide useful information about Fetal Alcohol Spectrum Disorder (FASD), and to
focus on an approach and an attitude when working with individuals affected by FASD.
If you have further questions about
FASD or would like more information,
please contact:
First Nations Special Education at:
1.877.422.3672
This handbook was updated by Madeline Price Desktop Design by Brent Scout
© 2006 FNESC

Inside:
Introduction……………………………………….. 2
What is FASD?…………………………………... 3
FASD Identification……………………………… 4
Understanding People with FASD…………….. 5
Basic Needs of Persons with FASD…………… 8
The Ideal Classroom…………………………….. 9
Individual Education Plan (IEP)………………… 10
Paradigm Shifts and FASD……………………... 11
TABLE OF CONTENTS Talking About Special Education Volume
FASD in the Classroom…………………………. 12
Teaching Students with FASD/FAE…………… 13
Design Concrete Measures of Time…………... 14
The T Chart………………………………………. 15
Supporting Behavioural Changes…………….. 16
Trying Differently………………………...…….... 17
Appendices ……………………………………... 19
A - An Example of an IEP
B - Resources
“Trying Differently Rather Than Harder”
Understanding the role of the brain in FASD and the shift in recognizing the difference between non-competence and non compliance sets the stage for Trying Differently Rather than Harder”
Adapted from the book: Trying Differently Rather Than Harder
(Diane Malbin M.S.W. 2nd Edition) Fetal Alcohol Syndrome and
Alcohol-Related Neurodevelopmental Disorders. 2002

What is Fetal Alcohol Spectrum Disorder?
Fetal Alcohol Spectrum Disorder (FASD) is an umbrella term that refers to a range of birth defects caused by drinking during pregnancy. Fetal Alcohol Syndrome (FAS) is a medical diagnosis and has 4 key features: • prenatal exposure to alcohol • growth deficiency • certain facial characteristics • brain damage *Although the term Fetal Alcohol Effects (FAE) is being phased out, it still appears in the literature usually referred to as Alcohol Related Neurodevelopmental Disorders (ARND). Partial FAS (pFAS) - confirmed maternal alcohol exposure - has some but not all of the physical signs of FAS (learning and behaviour difficulties). Alcohol-Related Birth Defects (ARBD) - confirmed maternal alcohol exposure - displays some physical anomalies resulting from prenatal alcohol exposure, for example heart, skeletal, vision, hearing, and fine and gross motor problems. Alcohol Related Neurodevelopmental Disorders (ARND) — confirmed alcohol exposure — refers to the variable range of central nervous system dysfunctions that are associated with alcohol consumption during pregnancy. ARND is demonstrated by learning difficulties, poor impulse control, poor social skills, and problems with memory, attention and judgment.
Talking About Special Education Volume II - FASD , 2006
Introduction This is an updated handbook from the series of informational handbooks prepared by the First Nations Education Steering Committee (FNESC) and the First Nations Schools Association (FNSA). This handbook follows from the general discussion of special needs included in Talking About Special Education Volume I, which includes issues such as parental involvement, special needs identification, individual education plans, and advocacy. Several sources of information were used in the development of this publication. FNESC and the FNSA would like to gratefully acknowledge the following work as most of this information in this booklet comes from these sources: Trying Differently Rather Than Harder 2nd Edition Diane Malbin, M.S.W. — Director of FASCETS (Fetal Alcohol Syndrome Consultation, Education and Training Services www.FASCETS.org Submissions from Deb Evenson — Project FACTS http://fasalaska.com/links-html Aboriginal Nurses Association of Canada (ANAC). 1997. It Takes a Community. A Resource Manual for Community-Based Prevention of Fetal Alcohol Syndrome.
Contact the ANAC at: 192 Bank Street, Ottawa, ON K2P 1W8, phone (613) 236 - 3373, e-mail [email protected]
Proceedings of the 2005 FASD National Conference
Page 2
Talking About Special Education Volume II - FASD , 2006
Page 3

Understanding People With FASD Infants Infants may experience a range of characteristics. Severely affected infants may require hospitalization from disorders affecting major organs. Infants with FASD are also prone to infections, and they generally develop more slowly than other infants. They may have difficulty sleeping, sucking and swallowing, keeping food down, gaining weight, and may be irritable and unpredictable. Be patient, and keep their level of stimulation low. (Adapted from Aboriginal Nurses Association, 1997) Young Children From toddler through preschool, children with FASD may be slow to develop, and if they are severely affected they may continue to have health problems due to organ damage. Delays in their speech and vocabulary may be noticeable in preschool years, and referral to therapy and special needs preschools may be considered. Children with FASD may be clumsy and accident prone due to late development of their motor skills, and their learning through experience, seeing and hearing may also be delayed. They may rely more on touch to explore their surroundings.
Page 5
Talking About Special Education Volume II - FASD , 2006
(This larger group is now believed to be at greater risk for failure since they are often not seen as having a disability). People with ARND may have significant brain differences, yet their behaviours may be the only symptoms of their disability. ARND is often referred to as an “invisible handicapping condition” (Streissguth 1996). FASD Identification The diagnosis of Fetal Alcohol Syndrome requires the presence of measurable physical characteristics in addition to symptoms of brain damage and is generally made by a multidisciplinary team. It is the only alcohol-related diagnosis that may be make in the absence of a confirmed maternal alcohol history. The majority of people prenatally exposed to alcohol have no external physical characteristics, since the facial features of FAS result from specific timing of prenatal alcohol exposure — during days 18-21 of gestation. However, even though a person with FASD has no physical features, their brain dysfunction may be as severe as for full Fetal Alcohol Syndrome. Identification for this larger group with FASD is crucial since they are at greater risk for failure due to the greater invisibility of their disability (Clarren et al; 1998; Riley, 2003, Streissguth et al. 1996).
Page 4
Talking About Special Education Volume II - FASD , 2006

Adolescents and Young Adults with FASD Youth with FASD and their caregivers are dealing with normal teenage issues plus the concerns of FASD. Youth with FASD can be easily misled, and may need social skills interventions, a supervised environment and appropriate school programming. Affected youth may have problems making friends because of unacceptable or immature behaviour, and they may have difficulty in communicating and understanding instructions. Abstract thinking is slow to develop, and their literacy and numeracy skills may be below their age and grade level. Attention deficit and hyperactivity will affect learning and relationships with peers. Their excess energy should be directed. Some affected youth become skilled in individual sports like swimming or running, and sports can help to build self-esteem and social skills. The youth, however, may have difficulty with rules, daily living skills, managing money and time; therefore, life skills must be reinforced from an early age.
Talking About Special Education Volume II - FASD , 2006
Page 7
Understanding People With FASD Young Children (continued) Over-stimulation or changes in daily routine can lead to tantrums and destructive behaviour, and interacting with other children may be a problem. An assessment may be needed to determine what special services are needed to ensure a successful transition to school. School Age Children with FASD There are physical, learning and behavioural difficulties common to most children with FASD. Their speech and language development may be delayed. They may have problems mentally “registering” information, and once information is learned it may take more time to be “retrieved.” Their ability to understand consequences may be impaired, and learning disabilities are common. The child may have a short attention span, under-developed motor skills and reasoning, and learning disabilities resulting in inappropriate behaviour.
Page 6
Talking About Special Education Volume II - FASD , 2006

The Ideal Classroom • Structured with flexibility • Visual supports • Little clutter The Ideal Teacher Interaction • Warm and accepting • Consistent in behavioural expectations • Frequent positive feedback based on realistic expec-
tations • Regular communications between parent and school • An Individual Education Plan outlining strengths with
realistic and achievable goals in place. Teaching Methods in the Ideal Classroom • Emphasis on collaborative problem solving • Emphasis on explicit teaching (make it as concrete
as possible) • Programs adaptations (example: more time allowed
for completion of in-class • Assignments - less written work, visual supports, use
of a computer)
Talking About Special Education Volume II - FASD , 2006
Page 9
Basic Needs of Persons Living with FASD (Adapted from Aboriginal Nurses Association, 1997) The person affected with FASD needs nurturing, understanding and support. A stable home, responsive school system, supporting friends and caring community are also important aspects of nurturing the child. The person with FASD needs to feel that he or she is a part of the community. Self-esteem and acceptance are critically important. Parents of children with FASD need connections with the community, other parents, and services that provide family centred and culturally sensitive support. Parents may need help dealing with addictions, poverty, low self-esteem, and limited work and parenting skills. Caregivers should be respectful and non-judgmental toward families living with FAS/E and acknowledge that the parents are performing a demanding job. The community social safety net should meet the basic needs of family members and provide early assistance to the child’s family. Families should have access to appropriate assessments and diagnoses and be empowered to contribute to all discussions about their children.
Page 8
Talking About Special Education Volume II - FASD , 2006

From seeing the child as To understanding the child as
Won’t Can’t
Bad, annoying Lazy, unmotivated Lying Fussy Acting young, babied Trying to get attention Inappropriate Doesn’t try Mean Doesn’t care Refuses to sit still Resisting Trying to annoy me Showing off
Frustrated, challenged Trying hard, tired of failing Story telling to compensate for memory, filling in the blanks Oversensitive Being younger Needing contact, support Displaying behaviours of a younger child Exhausted or can’t get started Defensive, hurt Can’t show feeling Over stimulated Doesn’t get it Can’t remember
From Personal Feelings of:
To Feelings of:
Hopelessness Fear Chaos, confusion Power struggles Isolation
Hope Understanding Organization, comprehension Working with Networking, collaboration
Professional shifts from: To:
Stopping behaviours Behaviour Modification Changing people
Preventing Problems Modeling, using cues Changing environments
Paradigm Shifts and FASD Taken from Building Strengths, Creating Hope — Alberta Learning. For a complete manual for instruction online at: http://www.education.gov.ab.ca/K_12/specialneeds/fasd.asp
Talking About Special Education Volume II - FASD , 2006
Page 11
Individual Education Plan (IEP) The Individual Education Plan is the cornerstone to the educational program of many students with FASD. Students with FASD can be successful when realistic and effective approaches are used. There is much hope for this population!
When realistic and achievable goals are designed based on previous and appropriate assessment, the stage is set for student growth and success. The successful IEP is collaborative in nature, and involves all team members (teacher, teacher assistants, family members, the student, and others working with the student in their educational program). The IEP is designed to set the student up for success. It focuses on the student strengths, and incorporates support in the areas of student need. * If you would like to have FNESC Special Education Support demonstrate and facilitate an IEP at your school, please call or email Kelly Kitchen at 1.877.422.3672 or [email protected] If you have questions related to the IEP please email or cal l Madeline Price at 1.877.422.3672, [email protected] or call our Toll Free resource Line at 1.877.547.1919 or email Lisa Ellis at [email protected]
***** See Appendix for Example of IEP *****
Page 10
Talking About Special Education Volume II - FASD , 2006

When teaching students with FAS/FAE...
Remove charts, maps, etc. after use Break down work into small pieces In group activities, pair a FAS/E child with a high
tolerance child Have the same teacher, Teacher aide, assistant all
year Teach memory strategies Control interruptions of the classroom Do not allow any talking-out with out hands up Use homework books with parents, making the
teacher and parents responsible for the books Clean out the child’s desk with them at least once
weekly Use a wide spaced paper Use pink highlighters, not yellow Find a way to provide at least some lunch hour and
recess supervision Keep any time out very short Supervise the child when going from one place to
another Use open book tests with the areas being tested
highlighted Limit homework to a reasonable amount Allow the student more time to respond to questions Try to have all people who interact with the child use
the same language to mean the same thing Give thought to developing a peer monitoring
program After elementary school, emphasize life skills and
vocational training Don’t personalize behaviour Use concrete measures of time (see next page) Teach explicitly, never assume the student will get it
(see T chart—Page 26) Listen to parents! They often know what works best
Page 13
Talking About Special Education Volume II - FASD , 2006
FASD in the Classroom (Adapted from FAS/E Support Network 604.576.9911 or email [email protected] When teaching students with FAS/FAE, try the following:
Provide order!!! Keep a routine oriented classroom Provide a highly structured environment Build in transition periods Make areas of the room clearly defined by
activity (wall decorations should reflect only what goes on in that area) Put as little as possible on the walls Keep colour to a minimum Put desks in rows—groupings do not work Put the child directly across from speaker for
eye contact Use uncluttered worksheets Give immediate feedback on assignments Keep a posted schedule for the day’s activities Ask visitors to the classroom to arrive on time Flick the classroom lights to get attention Test one on one for knowledge, not attention Use redirects—”this is your”…”this is where it
goes” Plan ahead for special events and keep them
infrequent Break up concentration activities with physical
activities Store books, materials, etc. by type, not size Label shelves and cupboards with words and
pictures/symbols
Page 12
Talking About Special Education Volume II - FASD , 2006

The T Chart T Chart’s can make rules more concrete and visual. This is an example of a T Chart for a high school student who could read but could not remember how to leave the breakfast area in the resource room clean.
Rule: Breakfast area is clean after breakfast ☺
Page 15
Talking About Special Education Volume II - FASD , 2006
Looks like:
Sounds like:
• Dishes in cupboard • Knives, forks and
spoons in tray • Cereal put away in cup-
board • Bread bag has clip on it • Bread is put in the cup-
board • Milk is in the fridge • Counters are wiped
and shiny • Floor does not have
anything on it
• Teachers and Teacher’s Assistants will be smiling and saying: “GOOD JOB KOBI, I REALLY LIKE THE WAY YOU CLEANED UP EVERYTHING ON THE COUNTER, ON THE TABLE AND ON THE FLOOR!” * insert photo of student working
*Good Job!
* insert a digital photo of the real-life situation
HOW TO DESIGN A CONCRETE MEASURE OF TIME Many students have great difficulty working on an assignment to completion — sometimes this is because they cannot grasp the measure of time and don’t know when they will be finished. Time is often a difficult and abstract concept to grasp. A concrete measure of time can help. For younger kids paper chains work well — each part of the chain can represent 1 minute — the task could be 5 or 10 minutes and at each minute one link is taken off — this can be attached to the board at the front of the room or on the student’s desk. Teacher Assistants can help with this support. For more sophisticated students — the teacher may give them 30 minutes on task work. The teacher could count down the time by 5’’s and write it on the board. There are many creative ways to use concrete measures of time. Egg timers work and can be placed on a student’s desk, or a big one on the teachers desk. Timers with bells can work as well. Sometimes students need to know that they can have a break after they have successfully completed a certain amount of time on task — so you can pair time on task with 5 minutes of time that the student can have personally — whatever works to make the student successful and able to complete time on task!
Page 14
Talking About Special Education Volume II - FASD , 2006

Trying Differently Rather Than Harder — Supporting Behavioural Changes by Recognizing Cognitive Differences
By Diane Malbin — FACETS Inc. www.FASCETS.ORG
(Taken from the 2005 Alcohol Spectrum Disorder National Conference — Equality of Access: Rights and the Right Thing To Do) Parents and teachers tend to try harder, using good techniques, to change behaviours. Good techniques that work with other children may simply not work for people with FASD. Paradoxically, their behaviours change as a function of changes in the environment. In other words we can set these individuals up for success if we adapt the environment to ensure better outcomes. 1. Accept that the person has an invisible physical disability.
Establish relationship.
2. Clarify your needs, feelings, resources and supports.
3. As with other more obvious physical handicapping conditions, evaluate environments for their “goodness of fit” and adapt /modify environments as appropriate to maximize potentials. Recognize which elements of environments may be posing undue challenges, chronic frustrations...or be inappropriate. Adjust accordingly.
4. Ask the “what if” questions and continue to explore
5. Identify strengths, interests, and work through these.
6. Create climates characterized by structure rather than control.
7. Control tends to be top-down, other-initiated, set up power struggles.
Page 17
Talking About Special Education Volume II - FASD , 2006
Supporting Behavioral Changes By Recognizing Cognitive Differences A Neurobehavioural Approach
Recent studies have shown the importance of linking brain damage with behaviour and communication to improve outcomes for students with FASD. Brain damage causes behavioural and communication symptoms. Our Attitudes and Approach in working with students with FASD will make a difference. What Interventions are a poor fit?
Interventions based on changing behaviour symptoms have not worked. Traditional methods of teaching behaviour have often been unsuccessful. Techniques based on “learning theory” which include behaviour modification techniques to eliminate or change behaviour often make things worse. These approaches do not include a conscious recognition of brain dysfunction.
Page 16
Talking About Special Education Volume II - FASD , 2006

8. Structure is safe, respectful, invites participation,
establishes a “with” “not at” relationship and values the person’s input for developing solutions.
9. Our challenge in part is to recognize the articulate learning abilities we take for granted, i.e. Inferential learning, generalizing information, linking words with action, and to then clarify whether a discrepancy exists between apparent ability and actual ability.
10. Observe patterns; consciously rethink events. Recall that there may be a delayed reaction from the time of stressor and acting out behaviour. A behaviour at home that apparently occurs in response to a request to do a chore may actually relate to a frustration that occurred at school, or with friends. Think broader context, bigger picture.
11. Depersonalize. Reframe perceptions, shifting from thinking “willful” to considering “organic” component, or possible gaps in ability. Shift from thinking “won’t” to understanding “can’t.”
12. Work to 90% success. Break down tasks into small steps and check for completion and comprehension prior to adding more tasks. These may gradually be expanded with pattern development and maturity.
13. Recognize that individual needs may be at direct odds to environmental constraints. Difficult decisions may be necessary.
14. Consider: There’s always logic to the behaviour. It’s our challenge to understand the context and recognize the potential role of “brain damage.”
15. Specifically include the person with FASD in the strategizing or problem solving process. Choose words such as “show me” or “How” rather than “why” to invite input.
16. Keep it concrete, specific, and simple.
17. Always consider the neurological potential. “Think younger”, and remember “Fair is not same.”
Page 18
Talking About Special Education Volume II - FASD , 2006
Page 19
Chart
By Diane Malbin FASCETS — WWW.FASCETS.ORG
Page 19
Talking About Special Education Volume II - FASD , 2006
Standard
Interventions
Secondary Behaviours
Environmental Accommodations to Prevent Challenging
Behaviours Talk fast Therapy Punish
Anxiety Frustration Shut down
Slow down Give time
Adjust workload Take away privileges
Shame Ridicule
Anxiety Frustration Tantrums
Give time, Slow down Reduce work load Accept slow pace
Punish
Fear Frustration
Anger
Accept need to re-teach a concept in
different settings Teach age-based
skills, Punish “inappropriate”
behaviours
Lonely
Isolated Depression
Think younger, Establish develop-
mentally appropriate expectations
Punish Ground Shame
Anxiety, fear, No confidence,
Erode self-esteem
Recognize and allow for variability
Prevent anxiety Punish, More work
Medicate No Recess
Agitation, overactive, avoidance, anger, anxiety, tantrums
Evaluate the environment
Adjust accordingly Provide breaks
Punish More work
Anger Tantrums
Adjust workload Provide breaks &
snacks
Punish
Avoidance Defiance
Prevent problems Build on strengths Use visual cues
More hours on homework, No recess
Therapy
Burnout Shut down
Give up
Provide Kinesthetic Experiential Relational
options for learning Interrupt
Assert control Require transitions
Resistance Anger
Big Tantrums
Adjust workload to achieve closure
Provide time

Talking About Special Education Volume II - FASD , 2006
APPENDICES 1: Example of an IEP
ELEMENTARY SCHOOL
Phone:
Fax:
Individual Education Plan YEAR 2005-2006
Student: Kobi Anderson
DATE OF IEP MEETING: June 11, 2005 BIRTH DATE: September 4th, 1994 AGE: 11 GENDER M MAIL ADDRESS: Box 2220 Sechelt BC VON 3AO GRADE: 8 PHONE: 604-885-9039 PARENT/GUARDIAN: Victor and Gloria Anderson
School: Pine Elementary IEP Year 2005-2006 Student: Kobi Anderson
Talking About Special Education Volume II - FASD , 2006
Appendix A Example of an IEP
Talking About Special Education Volume II - FASD , 2006
A1

Example of IEP (continued):
STUDENT PROFILE
Talking About Special Education Volume II - FASD , 2006
INFORMAL ASSESSMENT:
(Classroom Based/Teacher Assessment)
Date Assessment Name
Comments/Recommendations
June 2005
Reading/Writing
Informal Teacher Assessment/ Observation Unit tests at Grade 6 level
Comprehension needs to be sup-ported by activities prior, during and after reading. Is working in a reme-dial literacy class in the afternoons
June 2005 Math
Working at a Grade 3/4 level
Informal teacher Assessment - Mastery unit tests
Enrolled in a Math Mastery Skills Program
2005 PE
Woodwork Computer
Projects Excels in these classes (has 2 block of PE) One block is Physio — working on weights
************************* Requires rigid routine/TA Support, and
accommodations in all areas
************************
A2 A3
Example of Individual Education Plan:
Student Profile
Talking About Special Education Volume II - FASD , 2006
Date Assessment Name Comments/Recommendations
2003
Weschler Intelligence Scale for Children 111
(WISC)
Verbal SS-76 Performance SS-98
Recommendations: - Small group language instruction - Comprehension Strategies Counsellor at school recommended 2X weekly. Explicit teaching of strate-gies for sensory overload
- Visual calm down strategies - Social story folder - Quiet place to ‘hang out’ for sensory overload
2003
Bender Visual Motor Integration — * area of strength for Kobi
- Include in timetable —extra computer/and wood work electives
ASSESSMENT INFORMATION: Formal Assessment: (Standard Scores)
2003 Weschler Individual Achievement Test Reading SS 90 Math SS 70 Writing SS 96
- Include extra scaffolding strategies for ‘inferential’ comprehension - Stress/Add a ‘Life Skills’ to Math Program - Money - Banking - Accounting program
2003 Peabody Picture Vocabulary Test (Receptive Language) SS 79
*See SLP handout Pre-teach vocabulary. Use as many visuals as possible Support “words with double meanings” * Use Rewards Program
2003 Referral to Asante Centre for complete assessment

A4 A5
AREAS OF NEED
ACADEMIC Math Skills: money, time, accounting Reading for comprehension Practical Writing Skills
BEHAVIOURAL Protocol for managing behaviour outbursts Strict routine to support success
SOCIAL/EMOTIONAL Self Esteem Confidence
LANGUAGE COMMUNICATION Build skills in receptive and expressive language
PHYSICAL Bilateral Hearing Loss (FM Systems in place)
LIFE SKILLS Work towards Communications 11 and 12 Math Essentials/Accounting Career Prep. And Job Support/ Work Experience
LONG TERM GOALS/DREAMS/DESIRES
To graduate Grade 12 and get a job. To play on the Men’s Soccer Team after Grade 12
WHAT DO WE WANT KOBI TO ACCOMPLISH THIS YEAR?
• To complete and master all literacy units • To complete Grade 4 Saxon Math Program • To follow his outlined visual schedules • To try to remember using polite words • To use his color coded binders/bins in the resource room • To put his breakfast food/dishes away in the resource room • To continue to take weights class and PE Class • To find his TA/Teacher when he feels he is “losing it” • To use the Resource Room as a calm place to rest • To try to stay in his classes until they are finished • If he feels tired, to go ask to go to the resource Room • Morning routine: 7:30 in Resource Room, makes own
breakfast, cleans up afterwards.
Talking About Special Education Volume II - FASD , 2006 Talking About Special Education Volume II - FASD , 2006
CURRENT SKILL LEVELS: R = Regular Program A = Adapted Program M = Modified
A Reading
M Math
A Writing
A Social Studies
A Science
R Physical Education
R Art/Woodwork
R Music
A Spelling
A Listening
A Expressive Language
Strengths: Athletic (enjoys PE); likes to be helpful; enjoys music, art and woodwork; creative; likes to make things; can be independent with a visual schedule; enjoys structure and routine; loves computers
Descriptors: Hard working; good sense of humour; can be volatile/anger triggers; likes to be independent but has trouble remembering; likes to have a concrete visual schedule; prints neatly; can be easily stimulated i.e. sensory system overloads, requires a consistent calming quiet place
Learns Best When: Has visual schedules for timetable and routines; All program adaptations are in place; when feels respected; in a quiet environment; 1 on 1 for new concepts; has a Learning Assistance Block; When language is spoken slowly, clearly, concretely and with few words (“get to the point)” with personal feelings left out
Medical History: Bilateral hearing loss; exposure to alcohol prenatally, chronic congestion; Overactive Sensory System (not on medication at this time)
School History: K—7 Pine Elementary

Talking About Special Education Volume II - FASD , 2006
Adaptations & Modifications Adaptations/Accommodations needed for student to meet regular grade outcomes:
Accessibility: access to all areas of school fire exits & routes furniture & storage health & professional care parking lot, roads & walk-
ways play areas & equipment showers, washrooms &
fountains transportation to and from
school other:
Assignments & Homework alternate assignments or
format length and/or number
(decrease) partner or group
assignments time allowed (increase) other:
Behaviour Management consequences — clear/
consistent expectations/rules —clear/
consistent home-school program outside agency support reinforcement (class/group/
individual) school counselling program student contract/goal
setting teach/assignments at skill
level teach & reinforce social
skills other:
Teaching Strategies: advance organizers/key
visuals alternate content/skills
demo/model processes/product feedback immediate/frequent practice guided/independent multisensory (oral/experiential/
written) memory (reduce/teach
strategies) pace quick/slow short sessions/lessons teach key concepts/vocabulary other:
Organizational & Study Strategies
b.b. or chart reminders class schedule/timetable clock/timer/watch desk/locker/tote tray (personal) furniture arrangement routines for use of materials student planner/home-school
book teach organizational/study skills other:
Equipment & Specialized Materials
augmentative commun device Braille machine/materials calculator (large keys/regular/
voice) camera (Polaroid/digital/
regular/video) computer/word processor computer printer/peripherals fine/gross motor equipment hearing aids/fm system headphones/listening centre Language Master & cards magnifier/lenses overhead projector reference books Spell Checker/Grammar
Checker
A7
GOAL CHART
Need (6 areas )
Goal: Student
Strategy and Team Responsibility
Measurement of Progress
Academic Literacy
Kobi will: - Complete level 20 by next reporting time Oct. 28 - Use LA time to complete assign-ments if needed - Hand in all assignments into the RED “IN” BOX Work with TA to be on time
CT’s will: - Follow Kobi’s protocol for all classes - Use a concrete measure of time to help Kobi focus on assignments - Chart his progress so can visually see his work completed - Support all program adaptations, literacy strategies
CT will: Graph Kobi’s pro-gress unit by unit - Liaise with RR Teacher, to help Kobi bring assign-ments to RR for completion support - RR teacher will check in with Literacy Teacher and support when needed
Behaviour
Kobi will: - Use his “calm down” visual sup-port when he feels upset/angry - Go directly to the Resource Room (RR) if he is not managing his be-haviour well - Remember to use polite words/use journal
CT’s will: - Direct Kobi to use his calm-down routines. - Allow him to leave the room if he chooses, must go directly to RR with TA - Use of concrete measure of time - Use the same language, “remember your polite words” - Follow protocol, use of T charts
Anecdotal notes Positive phone calls home Record of behav-iour/solution work-sheets
Math
Kobi will: - Complete up to level 14 by Oct. 28 - Attend all Math Classes
CT’s (and TA’s) will: - Graph progress, Praise all efforts, liaise with RR Teachers, RR Teachers will Liaise with CT’s for work completion and focus on task - Use concrete measures of time - Ensure all outlined program adaptations are in place: calcula-tor, recipe cards, calculation process, 1 on 1 support to check understanding
CT will: - Graph Kobi’s progress unit by unit - Liaise with RR Teacher to help Kobi bring assign-ments to RR for completion support - RR Teacher will check in with Literacy Teacher and support when needed - Home commun. once weekly to advise of progress
Behaviour
Late for Class
Kobi will: work with his TA to get to class on time
TA will meet Kobi at the first bell and walk with him to class in time for second bell
Visual attendance graph
Talking About Special Education Volume II - FASD , 2006
A6

SUPPORT TEAM
Role Participant Name
Contact Information
Mother/Father
Teacher
Principal
Teacher Assistant (TA)
Teacher/Hearing Imp.
Classroom Teacher (CT)
Classroom Teacher
Classroom Teacher
Classroom Teacher
Resource Room Teacher (RR)
Special Ed. Teacher
Talking About Special Education Volume II - FASD , 2006
A9
KEY:
A = ADAPTED (Regular Grade Learning Outcomes w/ Accomm./Adapt.) E/G = ENRICHED/GIFTED (i.e., Extended Learning Outcomes or Advanced Level) R = REGULAR (Grade Level Learning Outcomes: Content & Skills) M = MODIFIED ('Substantially Different" from Regular)
Equipment & Specialized Materials
standing frame/walker switches/adapted handles,
etc tape recorder wheelchair other: _______________
Reading, Writing & Note taking:
alternate formats note tak-ing: carbon copy/outline/photocopy/taped notes
alternate formats reading: Braille/enlarged print/rebus/tapes/videos
alternate formats writing: computer /p r in t ing /word process
alternate materials/texts: easier reading level/parallel unit
note taker, reader and/or scribe (parent/peer/staff/volunteer)
other: _______________
Following Directions: Provide only one or two
directions at a time Restate directions in clear
simple language Stand close to the student
and gain eye contact before giving directions
Provide visual support for directions (on students desk or on board
Increasing Written Input: Allow for a scribe or record
responses on tape Establish the process for
revision (first draft, sharing, revising, 2nd draft, sharing 3rd draft, polishing;, final, publishing
Have student write ideas on post it notes and then rear-range them to make an outline
Teach keyboarding skills Use an outline and 2 column
notes for paragraph and essay writing
Use graphic organizers Use the dot procedure (work to
the dot and get feedback) other: _________________
Testing & Evaluation
alternate setting/time alternate test/format time (increase/short sessions) open book/take home exams oral (reader/scribe/tape) programmed learning rewriting permitted Recognize and give credit for
class participation Review the grading process
before the test provide examples of criteria for
each letter grade Allow student to retake test Teach Relaxation strategies Provide sample items at the
beginning of the test Provide visual graphic cues as
the test directions change Repeat directions to the stu-
dent once you have given them to the class
Use take home tests for practice
other: __________________
Talking About Special Education Volume II - FASD , 2006
A8

SAMPLE PROTOCOL
ATTENTION ALL TEACHERS: Date: _________ Student: Kobi Anderson — Grade 8
Structure: Create a structured environment-includes choices and clear routines. Supervise: Carefully supervise so the behaviour does not escalate into a situation that becomes unworkable. Simplicity Use clear simple language - stated briefly—leave personal feelings out of the conversation-leave out any verbal justifications, explanations. Steps: Break down tasks into small steps, and teach each step through repetition, and social, verbal or appropriate Reward Context: Teach skills into the context in which the skills are to be used- be careful not to assume that the student will generalize from one concept to another, or understand in which contexts the behaviour is appropriate and when it is not.
Kobi may not be able to translate information into action- understand cause and effect. Kobi may not be able to take information learned from one situation and apply it to another.
To repeat instructions can sometimes help but does not ensure compliance or understanding.
Often problems are not behavioural, emotional, or environmental - they are neurological - damage to the brain.
Situations need to be set up for a “win-win” as much as possible- confrontational or punitive actions will not support the student well or provide for an ongoing positive relationship.
Sometimes Kobi’s behaviour may seem to be willful behaviour, however this may not be the case and in most circumstances is the result of a disability and therefore we need to set up situations that will ensure that structures and routines are in place and external supports are in place to ensure success and safety.
Chronological Age 10-11 Developmental Age 6 in the areas of social skills, emotional maturity and concept development.
Auditory memory is weak. Please support Kobi with as many visual supports in the classroom as possible. Homework written on the board, and in his planner. TA may need to ensure this is done at the end of each class.
Please send Kobi to the Resource Room if he is having problems adjusting to changes in the classroom setting, or settling down.
*** Kobi has a visual support for calming down-please prompt him to use this before he decides to leave the room.
***PLEASE LET KOBI OUT OF CLASS 2 MIN. BEFORE THE BELL. THIS WILL EN-SURE A SAFE AND INCIDENT FREE TRAVEL TO THE RESOURCE ROOM TO CHANGE BINDERS AND BOOKS FOR NEXT CLASS. PLEASE CALL MADELINE POHLMANN “FIRST” CASE MANAGER/RESOURCE ROOM IF A SITUATION ARISES WHERE THE PRINCIPAL OR FAMILY ARE ASKED TO BE INVOLVED.
Talking About Special Education Volume II - FASD , 2006
A 11
Baseline Measure
Review #1 Review #2 End of Year Measure
Reading Level
16
Math Level 12
# of times
missed Math Class
BASELINE MEASURE DOCUMENTATION
# of times
missed Literacy Class
Talking About Special Education Volume II - FASD , 2006
INDIVIDUAL EDUCATION PLAN REVIEW DATE: __________
ACCOMPLISHMENTS
GOAL REVIEW
TRANSITION PLAN
Transition to Grade 8 , Plan begins _______
A10

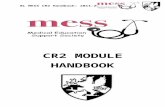
FASD Neurocognitive Characteristics,
Expectations, Secondary Behaviours and Examples of Accommodations
B1
Talking About Special Education Volume II - FASD , 2006
Primary Behavioural
Characteristics FASD
“Fit” within Environments:
Values Expectations
Interpretation of Behaviours
when Expectations Are not met
Slow auditory pace,
goes blank
Think fast, Pay attention Stay on task
Ignoring me, Resistant
Personalize
Slow cognitive pace Doesn’t answer
Think fast, timed tests Finish work within
allotted time/schedule
Controlling, Avoidant Not trying, holding
others up on purpose Difficulty generalizing get the piece, not the
picture
Follow the rules, learn inferentially
“gets it by watching”
Willful on purpose, intentional. He knew
what the rule was Dysmaturity:
Developmentally younger than their
age: 7.5 more like a 3 year old & 15 more like a 10 year old
Act your age
Be responsible Be appropriate
Poor Social Skills Acting like a baby
Inappropriate Overprotective
parents
Memory problems “on days/off days”
Learn the first time and remember from
day to day
He/she doesn’t care — lazy, needs to try
harder Sensory issues Over stimulated Overwhelmed,
distractible
Pay attention
Sit still Ignore distractions
Not trying Undisciplined
Off task, ADD
Easily fatigued
Keep up
Try harder
Not trying, Lazy Work Avoidant Unmotivated
Impulsive inability to predict
outcomes acts fast—thinks slow
Think ahead Plan
Set goals Rein in impulses
Willful Disobedient
Inappropriate Doesn’t care
Concrete thinker Learns by doing
Abstract, sit still pay attention, listen/learn
Lazy, unmotivated and/or poor parenting
Rigid, perseverance, difficulty stopping/changing activities
Stop when told! Don’t resist
Controlling, wants all the power, bossy,
Oppositional
Appendix B Resources
Talking About Special Education Volume II - FASD , 2006

Sources of Information on FASD in BC To order Diane Malbin’s book: Trying Differently Rather Than Harder contact FASCETS, Inc at www.FASCETS.org Website: http//fasal.aska.com/links-html Teaching Students with FASD A complete manual for instruction online from Alberta Learning:http://www.education.gov.ag.ca/k_12/specialneeds/fasd.asp. FAS Bookshelf — Books and Videos on FASD 604-942-2024 For Diagnosis and Assessment: Sunnyhill Hospital for Children 604-453-8314 http://www.sunnyhill.ca http://www.bcchf.ca/index/html Asante Centre for Fetal Alcohol Spectrum Disorder 1-866-FAS-7101 (1-866-327-7101) Email: [email protected] Web: www.asantecentre.org Canadian Guidelines for the diagnosis of FASD http://www.cmha.ca/cai/content/full/172/5supply/F1 (Adapted from Materials from the Provincial FAS/E Prevention Coordinator)
B2
Talking About Special Education Volume II - FASD , 2006
Alcohol and Drug Information and Referral Service #202 - 3102 Main Street, Vancouver, B.C., V5T 3G7 Toll-free: 1 - 800 - 663 - 1441 phone: (604) 660 - 9382 fax: (604) 660 - 9415 Information and referral to treatment services and agencies for those who are seeking assistance with alcohol and other drug misuse. B.C. FAS Resource Society Sunny Hill Health Centre for Children 3644 Slocan Street, Vancouver, B.C., V5M 3E8 (604) 465 - 8204 Project Office: #302 - 11965 Fraser Street, Maple Ridge, B.C. V2X 8H7 phone: (604) 465 - 5211 Information about support and services to families, professionals and the broader community around prevention, intervention and treatment issues related to alcohol and other drug related developmental disabilities. BC Aboriginal Network on Disabilities Society 1179 Kosapsum Crescent Victoria, B.C. V8X 7K7 Toll free: 1 - 888 - 815 - 5511 or: (250) 381 - 7303 Resources are available to First Nations parents, groups and educators, including videos, manuals, displays and brochures dealing with FAS and the effects of alcohol on pregnancy.
B3
Talking About Special Education Volume II - FASD , 2006

Prevention Source BC 2750 Commercial Drive, Vancouver, B.C. V5N 5P4 Toll free: 1 - 888 - 663 - 1880 phone: (604) 874 - 8452 Information service to residents of BC seeking information about prevention, organizations, programs, materials and research in the area of substance abuse. FAS/E Provincial Prevention Coordinator: (604) 875 - 2039 Women’s Health Centre Room 501, 4500 Oak Street, Vancouver, B.C. V6H 3N1 phone: (604) 875 - 3599 Information on how to access information, resources, expertise and services related to FAS/E. Helps with networking among relevant agencies, and setting up community based initiatives. Society of Special Needs Adoptive Parents (SNAP) FAS/E Support Network (604) 589 - 8438 e-mail: [email protected] 151 - 10090 152nd Ave., Suite 187, Surrey, B.C. V3R 8X8 phone: (604) 589 - 1854 fax: (604) 687 - 3364 #1150 - 409 Granville Street, Vancouver, B.C. V6C 1T2 Toll-free: 1 - 800 - 663 - 7627 phone: (604) 687 - 3114 Information on support, consultation and advocacy services for individuals, families, professionals and the broader community around prevention, intervention and treatment issues. Assists special needs adoptive families through mutual support, information sharing
B4
Talking About Special Education Volume II - FASD , 2006
and advocacy through support groups, one-on-one resource parents, and a lending library. FAS/E Information Service YWCA Crabtree Corner FAS/NAS Prevention Project (604) 689 - 5463 101 East Cordova Street, Vancouver, B.C. V6A 1K7 phone: (604) 689 - 2808 fax: (613) 235 - 8101 Canadian Centre on Substance Abuse #300 - 75 Albert Street, Ottawa, Ontario, K1P 5E7 Toll-free: 1 - 800 - 559 - 4514 or phone: (613) 235 - 4048 A national service that includes a list server for discussion with other individuals interested in FAS/E. E-mail message to [email protected] and type “join fastlink” in the message. Offers educational workshops, a resource lending library, a peer support group for moms with children with FAS/NAS and information and crisis counselling. Posters and pamphlets are available, as well as guides to prevention, caring for children and a guide to resources. FAS Early Intervention Consultant Aurora Centre 4500 Oak Street, 5th floor, Vancouver, B.C. V6H 3N1 phone: (604) 875 - 2017 Works with health/social providers on early intervention approaches with women at risk. Develops policy regarding treatment and disseminates information on early intervention.
B5
Talking About Special Education Volume II - FASD , 2006

Copyright ©
The First Nations Education Steering Committee and
The First Nations Schools Association 2006
For additional copies, please write to:
Suite #113-100 Park Royal South West Vancouver, BC
V7T 1A2
Email: [email protected]
Or download a copy at: www.fnsa.ca