Farmacologische behandeling van neuropathische pijn bij ... Huynen... · Bosilkovska M. Analgesics...
13
Farmacologische behandeling van neuropathische pijn bij orgaanlijden Philippe Huynen Promotor: Pr. Dr. B. Morlion 22-04-2016
Transcript of Farmacologische behandeling van neuropathische pijn bij ... Huynen... · Bosilkovska M. Analgesics...

Farmacologische behandeling van
neuropathische pijn bij orgaanlijden
Philippe Huynen
Promotor: Pr. Dr. B. Morlion 22-04-2016

Neuropathische pijn: definitie
• IASP: “Pijn die ontstaat als een direct gevolg van een letsel of een ziekte die het somatosensorisch systeem aantast”
• Etiologie:
– Radiculopathie
– Diabetische polyneuropathie
– Uremische neuropathie
– Postoperatieve neuralgie
– Postherpetische neuralgie
– Oncologische pathologie
– Trigeminusneuralgie
– CVA
• Prevalentie: ± 7 à 8 %
International Association for the Study of Pain; 2011

Farmacotherapie: (atypische) analgetica
Finnerup NB et al. Pharmacotherapy for neuropathic pain in adults: a systematic review and
meta-analysis. Lancet Neurol 2015; 14(2): 162-73.

Chronische Nierinsufficiëntie: Definitie
• Definitie: afwijking in nierfunctie of –structuur, minstens 3 maanden
aanwezig, met een weerslag op de gezondheid (KDIGO; 2012)
• Etiologie: diabetes mellitus, arteriële hypertensie, immuuncomplexen,
inflammatie, systeemziekten, genetische aanlegstoornissen…
• CKD ↔ Neuropathische pijn: Rol in ontstaan van pijn:
– toxische effecten op CZS en PZS
– accumulatie van advanced glycation end-products
– uremische symmetrische axonale degeneratieve polyneuropathie
• Prevalentie: CKD
– 11-13% (NHANES; 2007, NIDDK; 2012)
Chronische Nierinsufficiëntie: Aanbevelingen
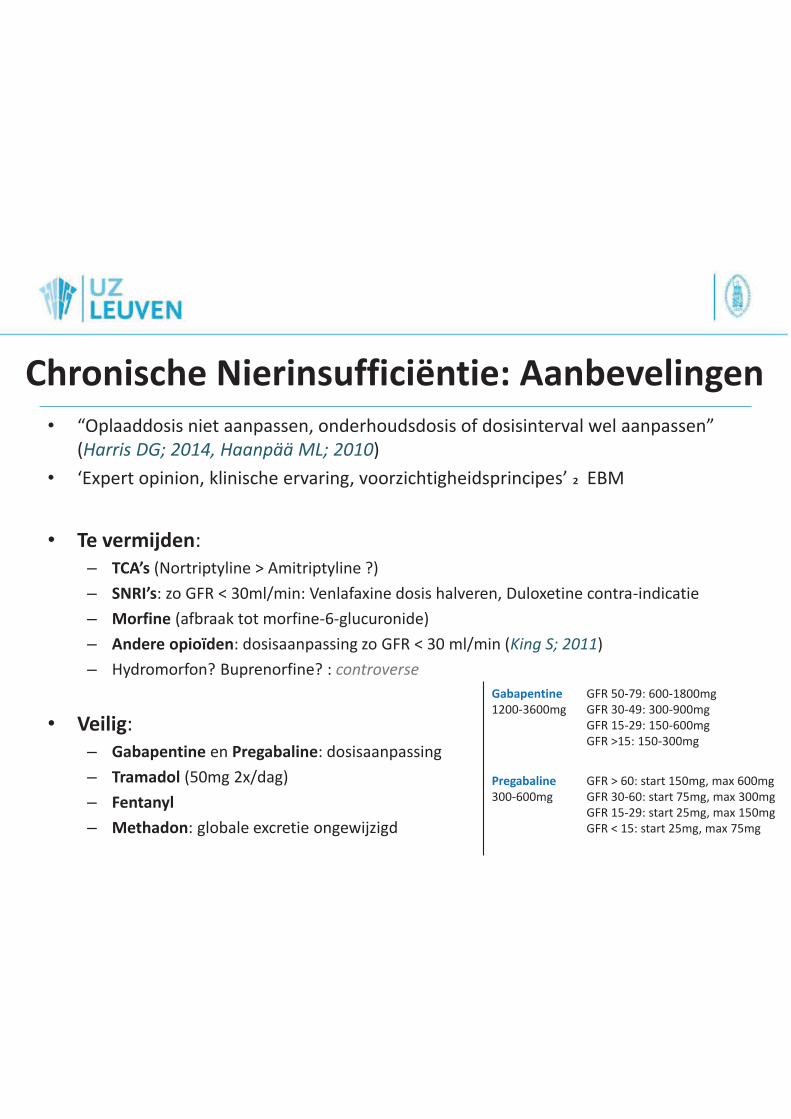
• “Oplaaddosis niet aanpassen, onderhoudsdosis of dosisinterval wel aanpassen”
(Harris DG; 2014, Haanpää ML; 2010)
• ‘Expert opinion, klinische ervaring, voorzichtigheidsprincipes’ > EBM
• Te vermijden:
– TCA’s (Nortriptyline > Amitriptyline ?)
– SNRI’s: zo GFR < 30ml/min: Venlafaxine dosis halveren, Duloxetine contra-indicatie
– Morfine (afbraak tot morfine-6-glucuronide)
– Andere opioïden: dosisaanpassing zo GFR < 30 ml/min (King S; 2011)
– Hydromorfon? Buprenorfine? : controverse
• Veilig:
– Gabapentine en Pregabaline: dosisaanpassing
– Tramadol (50mg 2x/dag)
– Fentanyl
– Methadon: globale excretie ongewijzigd
Gabapentine
1200-3600mg
GFR 50-79: 600-1800mg
GFR 30-49: 300-900mg
GFR 15-29: 150-600mg
GFR >15: 150-300mg
Pregabaline
300-600mg
GFR > 60: start 150mg, max 600mg
GFR 30-60: start 75mg, max 300mg
GFR 15-29: start 25mg, max 150mg
GFR < 15: start 25mg, max 75mg

Chronische Nierinsufficiëntie: Dialyse
• 12,6% van dialyse patiënten lijdt aan NeP
• Milde pijn: dafalgan, NSAIDs, tramadol (50% dialyseerbaar)
• Vd en proteïnebinding:
– Gabapentine: 35% dialyseerbaar
– Pregabaline: 50-60% dialyseerbaar
– Carbamazepine: niet dialyseerbaar
– TCA’s: beperkt dialyseerbaar: TDM
– Duloxetine: contra-indicatie
– Venlafaxine: dosis halveren
• Opioïden: – Te vermijden: codeïne, morfine: M6G
– Tegenstrijdige gegevens: Oxycodon, Hydromorfon
– Aanbevolen: BUPRENORFINE, Fentanyl, Hydromorfon, Methadon
King S; 2011

Chronische Leverinsufficiëntie: Definitie
• “Lever-functie”? Child-Pugh score, MELD?
– Kliniek > labo
– Frequente her-evaluatie
• “Lever-falen”?
• Hepatische klaring
– ClH = ERH x QH
– First pass mechanisme
– Hypo-albuminemie
• Metabolisme:
– Fase 1: oxidatie, reductie, hydroxylatie (CYP 450)
– Fase 2: NAT2, UGT
– Inductie en inhibitie, genetische variaties
• Leverziekten en pijn: Frequent!
– ethylische NeP, comorbiede DM, B1-deficiëntie
Branch RA; drugs in liver disease 1998

CLI: Dosisaanpassing (1)
• Anti-depressiva:
– TCA’s:
• CYP2D6, afhankelijk van QH, sterk proteïne gebonden
• Nortriptyline > Amitriptyline
– SNRI’s:
• Venlafaxine (hoge first pass, CYP2D6): cave t½ ↑↑
• Duloxetine: Contra-indicatie!
• Anti-epileptica:
– Gabapentine & Pregabaline: Geen dosisaanpassing
– Carbamazepine: controverse: risico op hepatotoxiciteit en DRESS

Tramadol:
- SNRI >> µ-agonist
Fentanyl:
- CYP3A4, echter QH > Clint
Hydromorfon:
- Fase-2-metabolisme (UGT)
Methadon:
- CYP3A4, klaring ongewijzigd
Buprenorfine: ?
CLI: Dosisaanpassing (2)
• Opioïden:
– Cave overgevoeligheid, risico op hepatische encefalopathie
– Metabolisatie = Fase-1-metabolisme. Uitz: Morfine, Hydromorfon
– Associeer laxativa!
• Voorkeur:
Bosilkovska M; 2012, Enggaard TP; 2006

Short Bowel Syndrome: definitie
• Definitie American Gastroenterology Association: residuele lengte < 200cm
• Etiologie:
– Volwassenen: darmresectie ikv trauma, mesenteriële ischemie
– Kinderen: volvulus, necrotiserende enterocolitis
• Intestinaal falen: wat bepaalt ernst?
• Vroegtijdige complicaties:
– Diarree, steattorree
– Ion-deficienties (K, Zn, Mg) & Vitaminosen (A, D, E, K, B12)
• Laattijdige complicaties:
– Cholelithiasis, nefrolithiasis & osteoporose
– Transiënte D-lactaat-accumulatie
• Intestinale adaptatiecapaciteit: 6-12 maanden
Jeejeebhoy; 2002

SBS: Farmacotherapeutische uitdaging
• Kennis van de farmacokinetiek
• Zo mogelijk per oraal!
• Buiten kaders denken: buccaal, sublinguaal, transdermaal, rectaal
– Amitriptyline: case report (buccaal)
– Nortriptyline: case report (per os)
– Gabapentine
– Carbamazepine, tramadol: rectaal
– Methadon: per os!
– Oxycodon (Proladone®)
• Te vermijden: enteric coated formulering, tabletvorm, pletten van
vertraagde vrijzetting voor buccaal… è www.pletmedicatie.be

Besluit
• Neuropathische pijn + comorbiditeiten– stijgende prevalentie
– farmacologische vraagstukken
• Farmacotherapie blijft hoeksteen– Atypische analgetica
– Ruimte voor opioïden
• CKD: – Atypische analgetica: dosisreductie
– Opioïden: Buprenorfine, fentanyl, hydromorfon, methadon
• CLI: – Atypische analgetica: gabapentine, pregabaline
– Opioïden: Fentanyl, hydromorfon, (buprenorfine?)
• SBS:– Weinig literatuur, plaats van absorptie vaak niet gekend
– Think outside the box!

Referenties
Amato AA, Barohn RJ. Chapter 384. Peripheral Neuropathy. Harrison’s Principles of Internal Medicine. 18th ed. 2011.
Treede RD. Redefinition of neuropathic pain and a grading system for clinical use. Neurology 2008;70:1630-5
Finnerup NB. Pharmacotherapy for neuropathic pain in adults. Lancet Neurol 2015; 14(2): 162-73.
Nicholson B. Comorbidities in chronic neuropathic pain. Pain Med. 2004;5 Suppl 1:S9-S27
Santoro D. Pain in end-stage renal disease: a frequent and neglected clinical problem. Clin Nephrol 2013;79 Suppl1:S2-11
Wittmann I. Neuropathy in chronic kidney disease. Diabetes Stoffwechsel Herz 2015 24:4 (251-255)
Lynch ME. A review of the use of methadone for the treatment of chronic noncancer pain. Pain Res Manage 2005;10:133-144
Haanpää ML. Treatment considerations for patients with neuropathic pain and other medical comorbidities. Mayo Clin Proc. 2010;85:S15-25
Jeejeebhoy KN. Short Bowel Syndrome: a nutritional and medical approach. CMAJ 2002; 166(10):1297-302
Severijnen R. Enteral drug absorption in patients with short small bowel: a review. Clin Pharmacokinet 2004; 43(14):951-62
Bosilkovska M. Analgesics in patients with hepatic impairment: pharmacology and clinical implications. Drugs 2012; 72(12):1645-69.
Anderson GD. Pharmacokinetic of antiepileptic drugs in patients with hepatic or renal impairment. Clin Pharmacokinet 2014;53(1):29-49
Perlman R. Intradialytic clearance of opioids: methadone versus hydromorphone. Pain. 2013;154(12):2794-80