
Farmacogenetica: huidige toepassing van genetische .... Guchelaar... · and PD pathway of sunitinib...
84
Farmacogenetica: huidige toepassing van genetische screening in de dagelijkse praktijk Prof. Dr. Apr. Henk-Jan Guchelaar Klinische Farmacie & Toxicologie 7 de Leuvens symposium Klinische Farmacie 6 oktober 2012
Transcript of Farmacogenetica: huidige toepassing van genetische .... Guchelaar... · and PD pathway of sunitinib...

Farmacogenetica: huidige toepassing van genetische screening in
de dagelijkse praktijk
Prof. Dr. Apr. Henk-Jan GuchelaarKlinische Farmacie & Toxicologie
7de Leuvens symposium Klinische Farmacie 6 oktober 2012
2
Leiden University Medical Center
Leiden University Medical Center
3
4
Translational Drug Research
Leiden University Medical Center Leiden Amsterdam Centerfor Drug Research

Klinische Farmacie & Toxicologie LUMC
5

Nieuwbouw GMP-faciliteit
6
7
Klinische Farmacie & Toxicologie LUMC
Pharmacogenetics
8
Two patients at your outpatient clinic
• Two patients A and B
• The same symptoms
• The same doctor
• The same diagnostic procedures
• The same diagnosis X
• The same treatment• Drug Rx at a dose x mg/day
• After 3 weeks• Patient A: symptoms resolved
• Patient B: still symptoms, side effects
• How is this possible?9

10
Pharmacogenetics: drug response is a heritable trait
Huang, Clin Pharmacol Ther 2008;84(3):287

11
Heritability of common conditions
• Freckles 90%• Short sight 90%• Autism 80+%• Acne 80%• Height 80%• Osteoporosis 75%• Diabetes 70%• Obesitas 70%• Blood clotting 70%• Backpain 65%• IQ 65%• Asthma, allergic 60%
• Arthritis 60%• Cataract 60%• Motion sickness 60%• Migraine 50%• Varicose vein 50%• Menopause 50%• Blood pressure 50%• Parkinson’s disease 0-10%• Irritable bowel syndr 10%• Left handedness <10%
• Drug response ??
Tim Spector, CBG meeting, Apr 2007

12
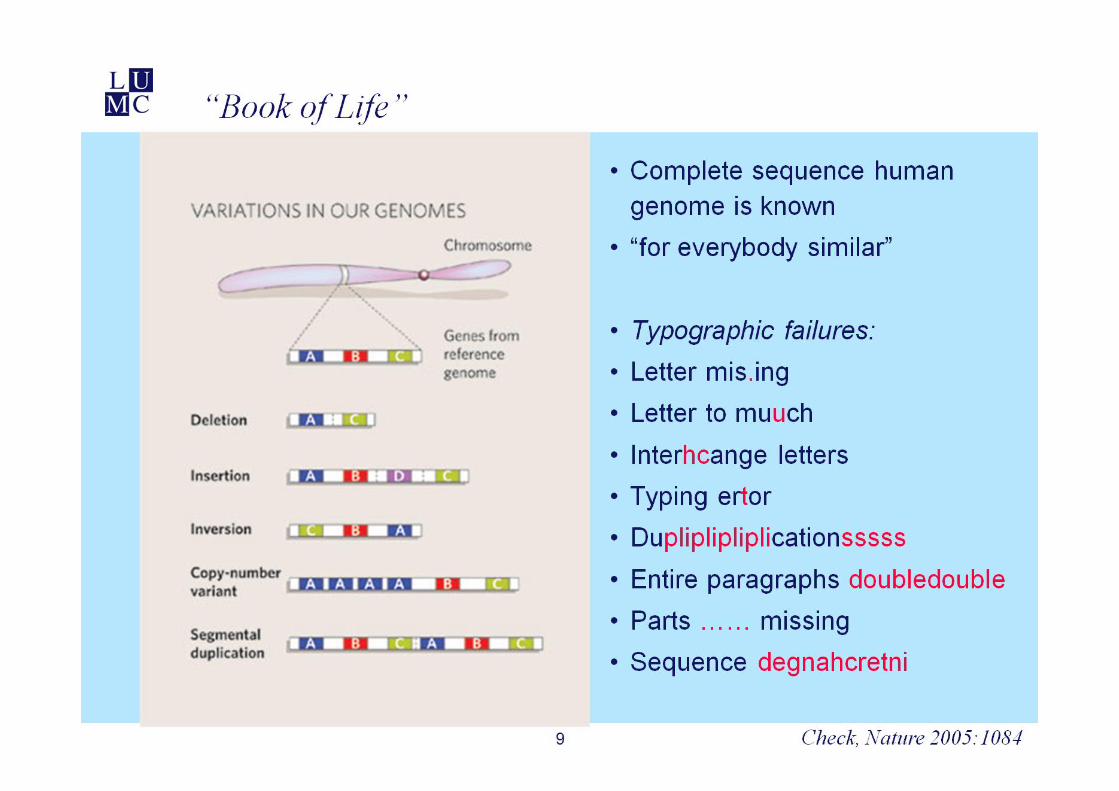
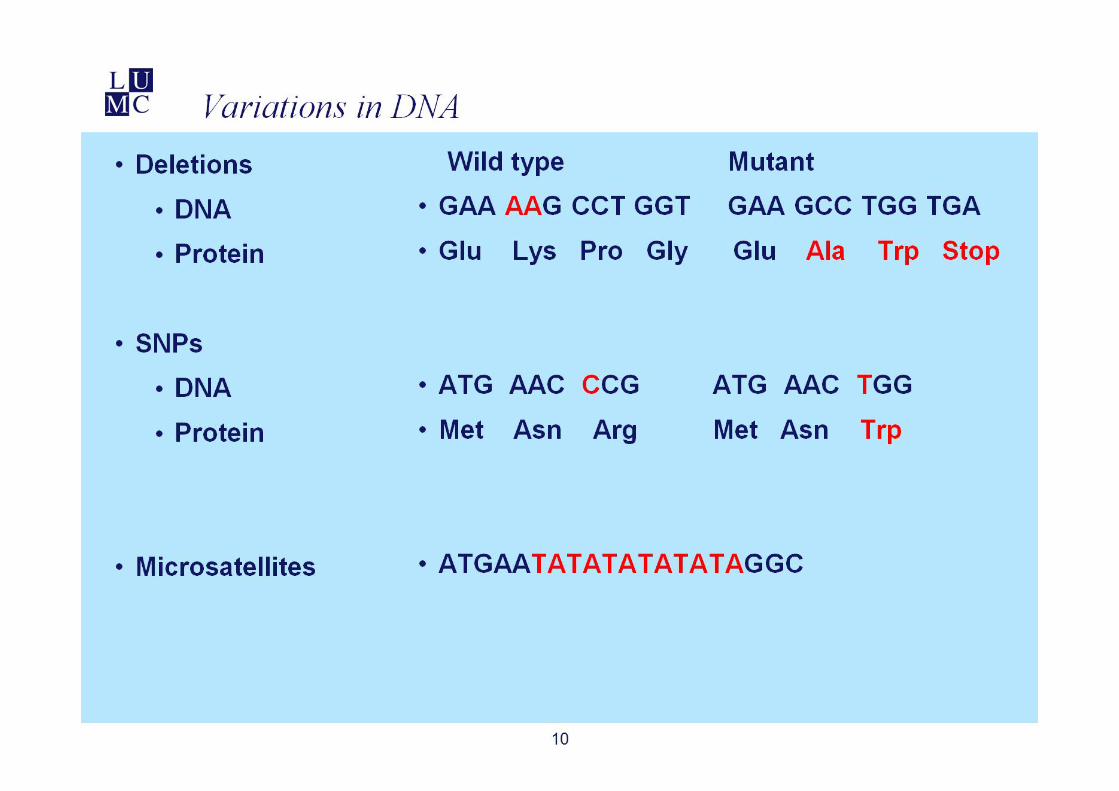
Variability in DNA
99.9% 99.9%
70%
3,200 * 106 base paires1: 300-1000 basepaires are different3-10 * 106 basepaires are different
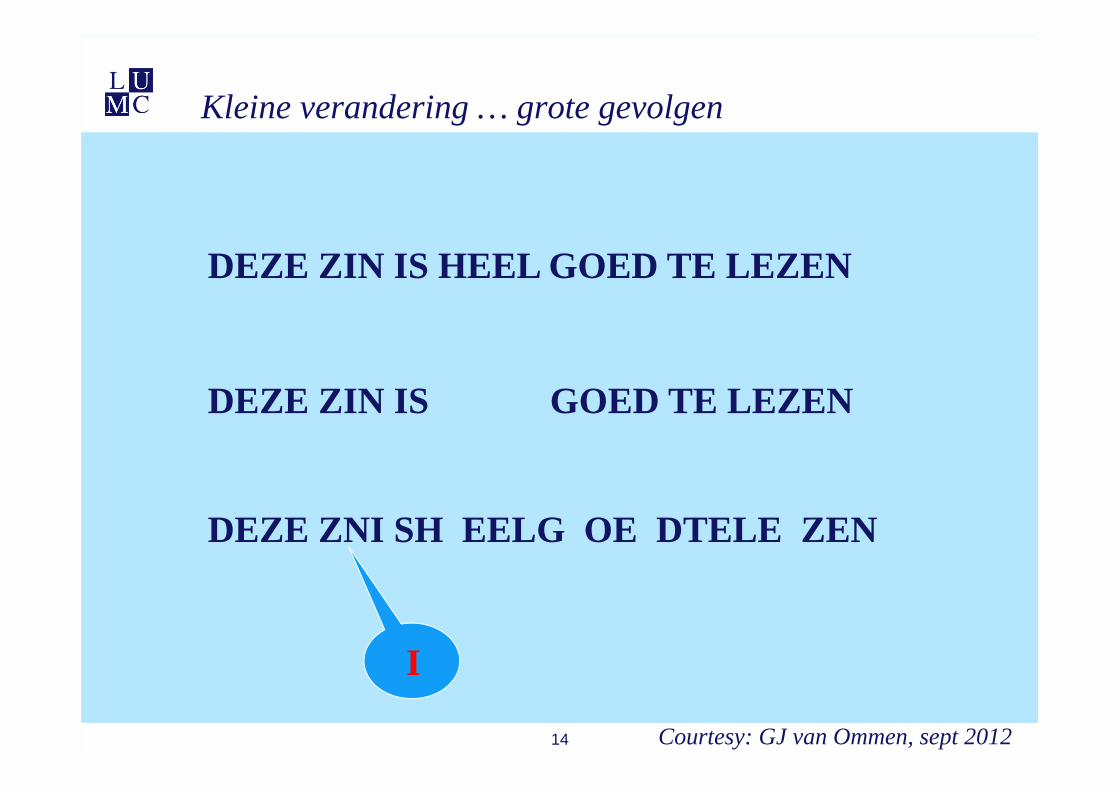
Kleine verandering … grote gevolgen
14 Courtesy: GJ van Ommen, sept 2012
DEZE ZIN IS HEEL GOED TE LEZEN
DEZE ZIN IS GOED TE LEZEN
DEZE ZNI SH EELG OE DTELE ZEN
I

16
‘Most drugs don’t work’
Effective (%)…..• Alzheimer 30• Depression (SSRI) 62• Asthma 60• Diabetes mellitus 57• Incontinence 40• Migraine (acute) 52• Migraine (profyl.) 50• Cradiac dysrhythmia 60• Tumors 25• Schizophrenia 60• Reumatoid arthritis 50• Reumat. art. (Cox-2) 80• Hepatitis C 47
Spear, Trends Mol Med 2001;7(5):201
Clinical Drug Toxicity
• Harvard Medical Practice Study – Lucian Leape• Nature of adverse events in hospitalized patients
• 30,195 randomly selected patients records
• 1,113 (= 3.7%) disabling injury caused by medical treatment• 19% adverse drug events (ADEs)
• Hospital Admissions Related to Medication• Incidence of hospital admissions related to drug related problems
• 21 hospitals in The Netherlands
• 5.6% of acute admissions were drug related: 50% preventable
17
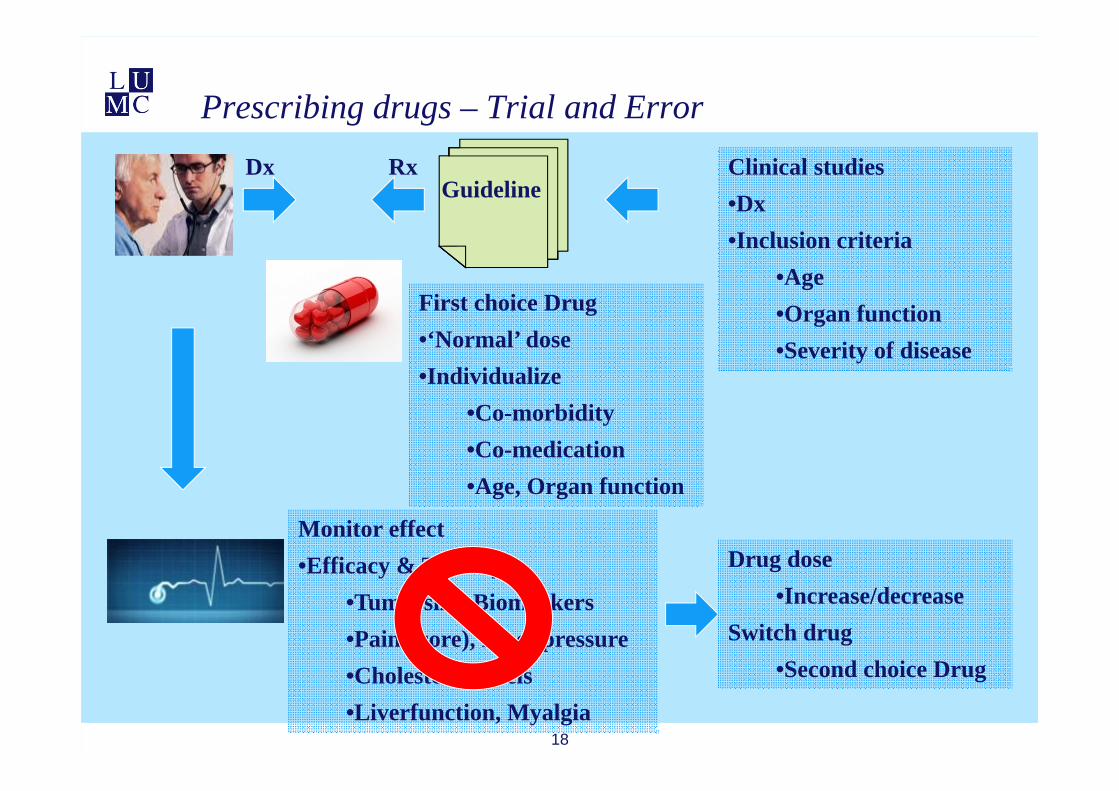
Prescribing drugs – Trial and Error
18
DxGuideline
Rx Clinical studies•Dx•Inclusion criteria
•Age•Organ function•Severity of disease
First choice Drug•‘Normal’ dose•Individualize
•Co-morbidity•Co-medication•Age, Organ function
Monitor effect•Efficacy & Toxicity
•Tumorsize, Biomarkers•Pain(score), Bloodpressure•Cholesterol levels•Liverfunction, Myalgia
Drug dose•Increase/decrease
Switch drug•Second choice Drug
1919
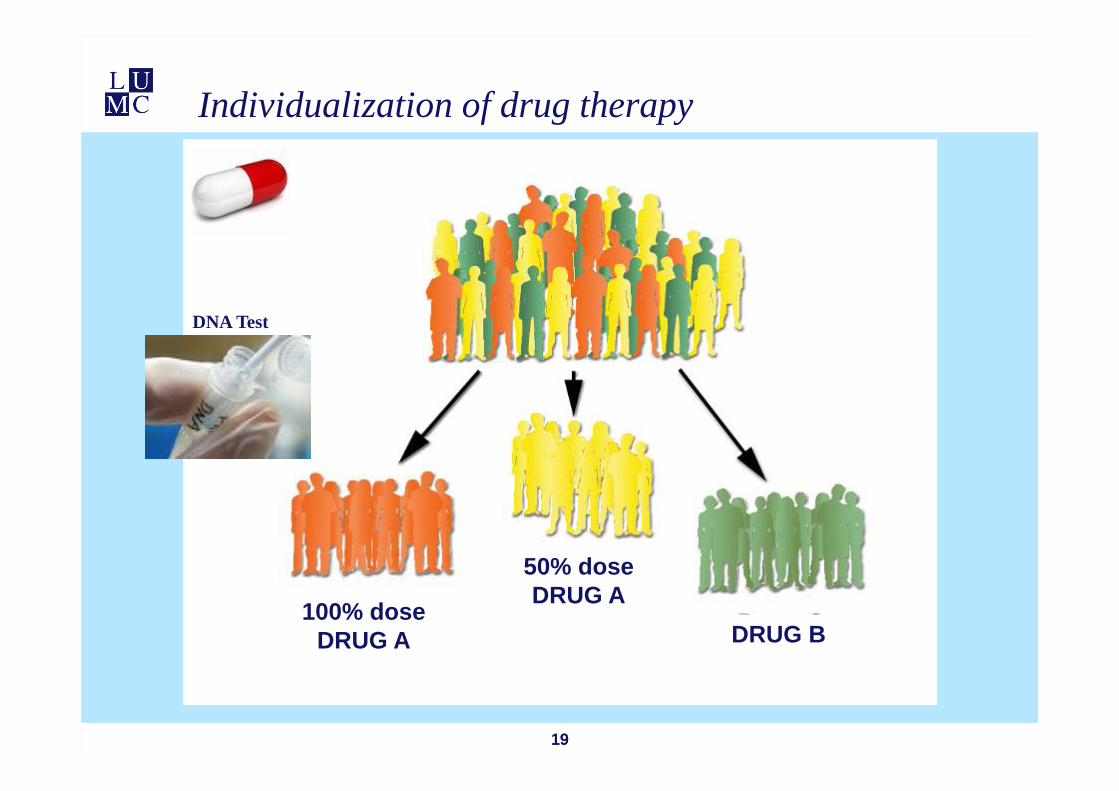
Individualization of drug therapy
100% dose DRUG A
50% dose DRUG A
DRUG B
DNA Test
• High Blood Pressure
• Antihypertensive drug: 2-4 wks BP cardiovascular risk
• Consequences of delay of efficacious treatment
• 3 months
• 10 yr (= 120 mo) treatment may result in an absolute risk reduction of 2,5% of 10 years risk death
• absolute risk: 7,50% 7.56%
20
Monitoring drug effects – ‘Trial and Error’ prescribing
• Metastatic colorectal cancer
• 3-6 courses chemotherapy: 9-18 weeks CT-scan response
• Consequences of delay of efficacious treatment
• 2-4 months
• mCRC: OS= 24 months
21
Monitoring drug effects – ‘Trial and Error’ prescribing

Biomarkers needed for predicting drug response
• Drug effect presents after months-years
• Important clinical consequences of treatment delay
• Diseases with a poor prognosis
• Severe side effects
22
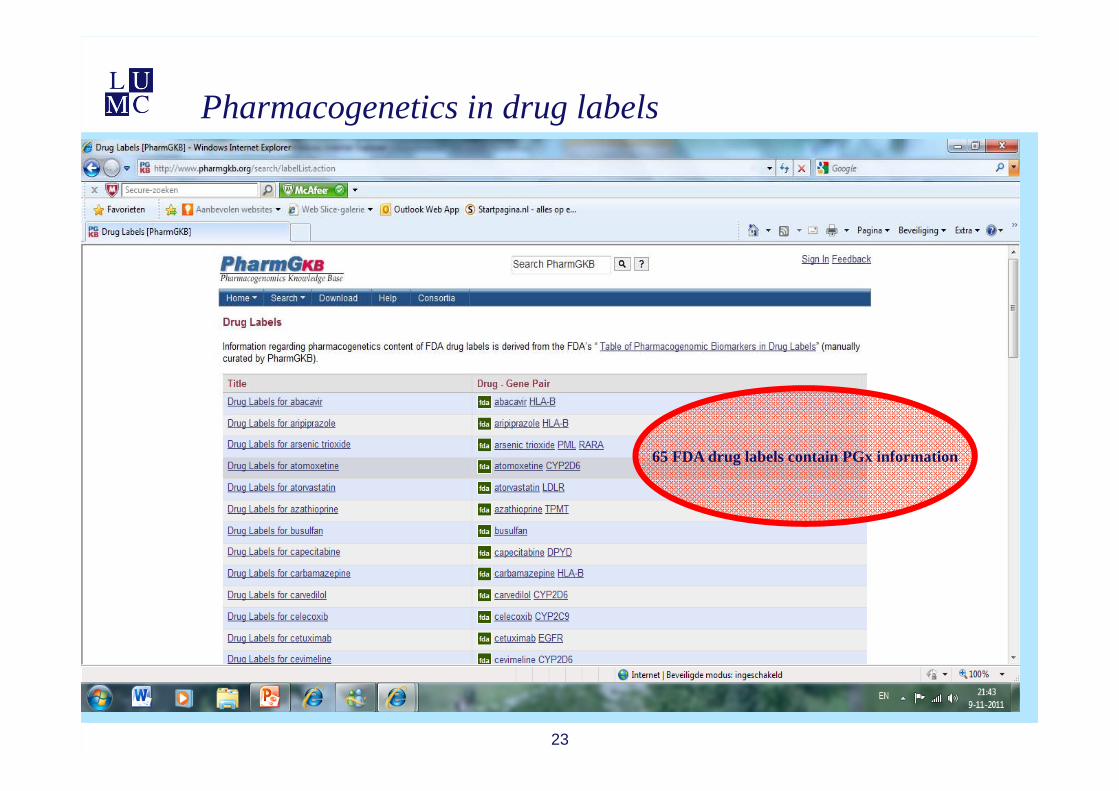
Pharmacogenetics in drug labels
23
65 FDA drug labels contain PGx information
6-Mercaptopurine - TPMT
24
25
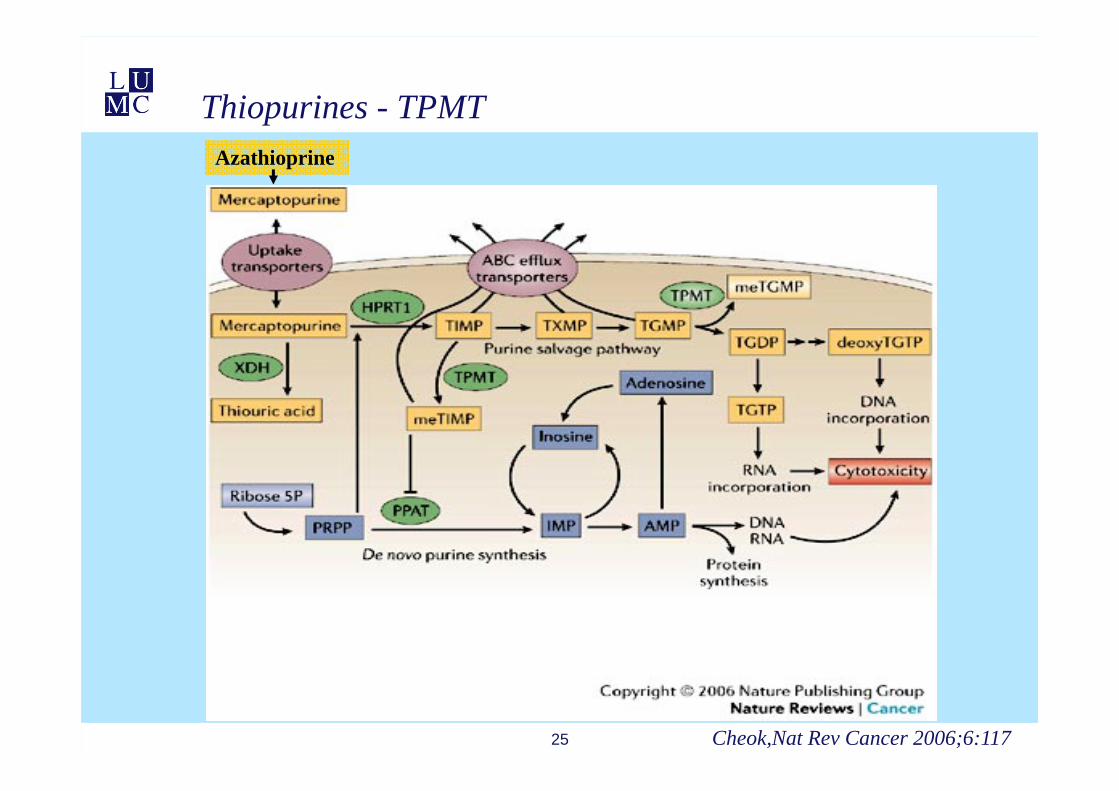
Thiopurines - TPMT
Cheok,Nat Rev Cancer 2006;6:117
Azathioprine
26
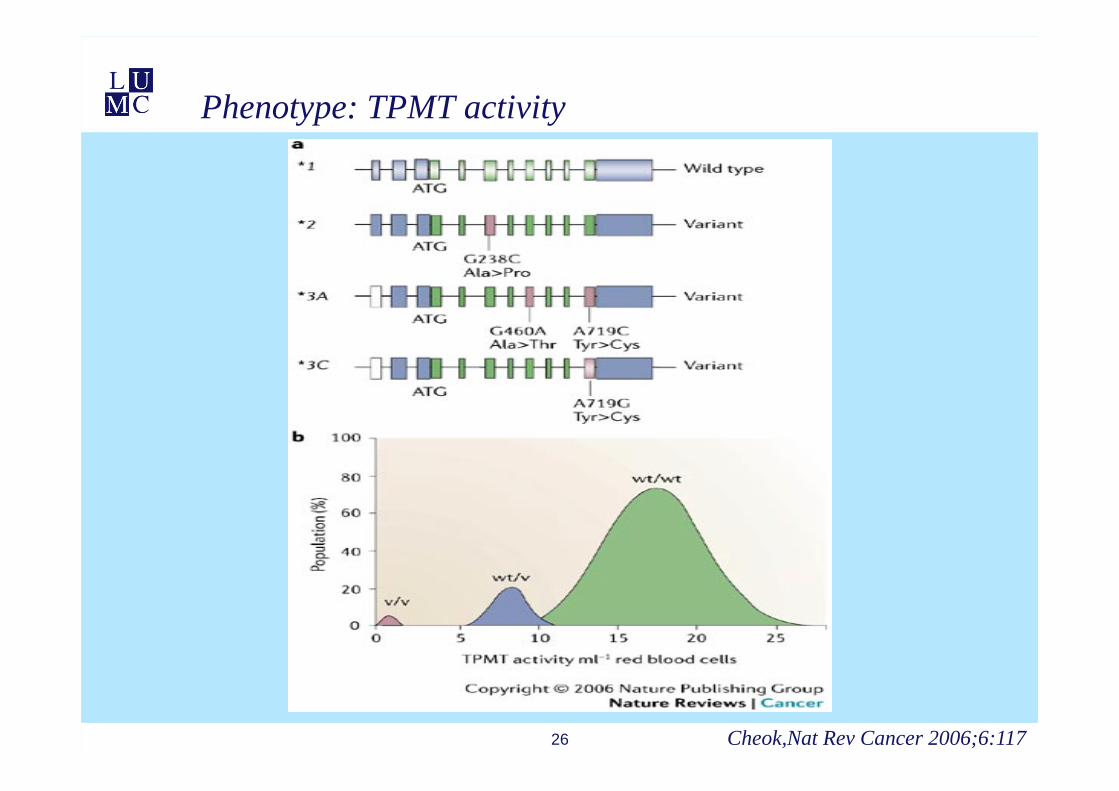
Phenotype: TPMT activity
Cheok,Nat Rev Cancer 2006;6:117
27
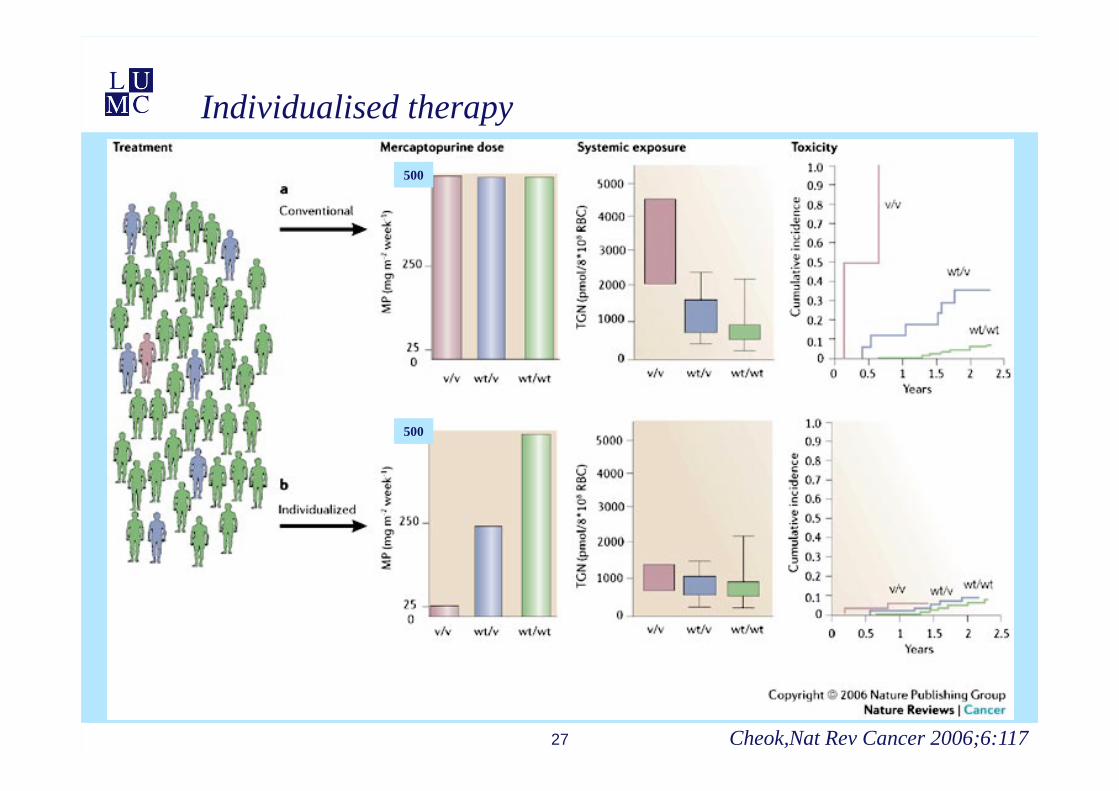
Individualised therapy
Cheok,Nat Rev Cancer 2006;6:117
500
500
28
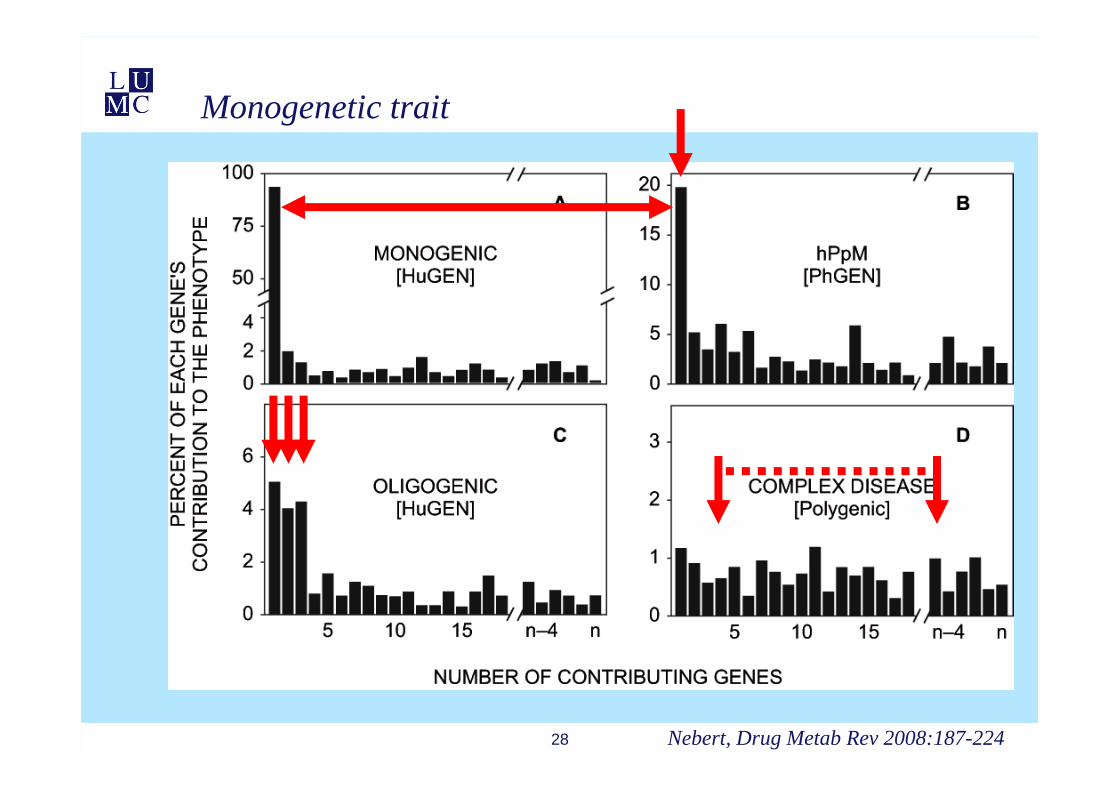
Monogenetic trait
Nebert, Drug Metab Rev 2008:187-224
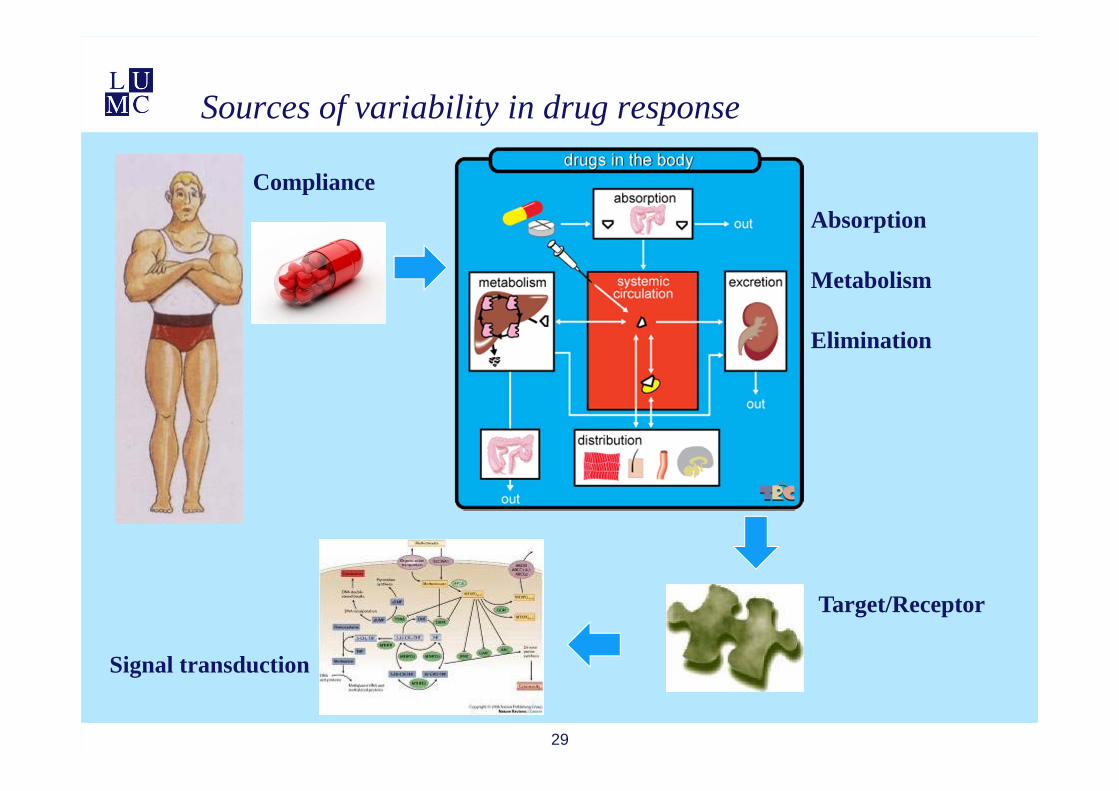
Sources of variability in drug response
29
ComplianceAbsorption
Metabolism
Elimination
Target/Receptor
Signal transduction
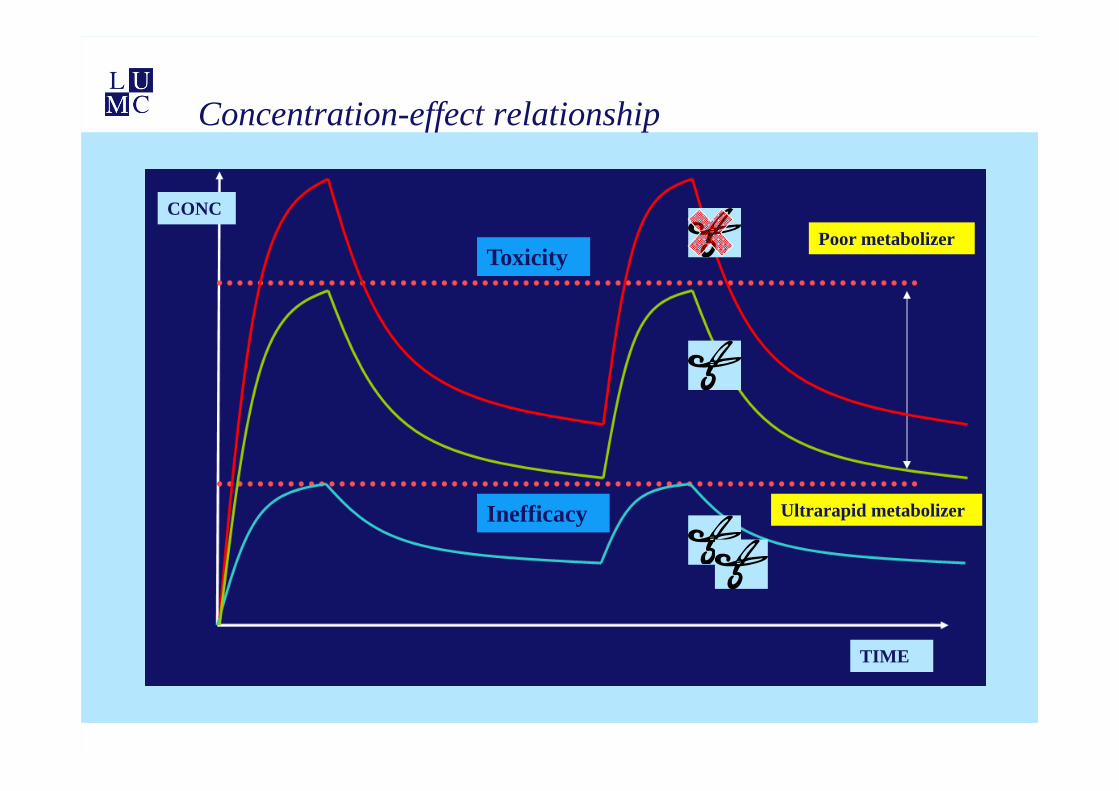
Concentration-effect relationship
Toxicity
Inefficacy
CONC
TIME
Poor metabolizer
Ultrarapid metabolizer
31
Explaining PK variability: Busulfan
• DNA Alkylating agent • Part of conditioning schemes prior to hematopoietic stem cell
transplantations (HSCT) • In combination (LUMC): fludarabine, cyclofosfamide, alemtuzumab
• Dosing (LUMC): 0.8 mg/kg iv 4x daily during 2 or 4 days non-myeloablative or myeloablatieve setting
• Busulfan exposure is related to clinical outcome• Toxicity: aGVHD,VOD
• Efficacy: Rejection, non-engraftment
• Busulfan has a high variability in pharmacokinetics• GST – glutathione conjugation
32
DMET-Plus array: Busulfan
• To find genetic biomarkers to understand the intraindividual variability in busulfan clearance
• 62 adult patients undergoing HSCT • busulfan in conditioning regimen
• Busulfan clearance• Therapeutic drug monitoring
• Individual busulfan clearance (Bayesian estimation)
• Genotyping: DMET array• 1,936 variants in 225 genes
• Genes involved in drug absorption, distribution, metabolism, excretion and transporters
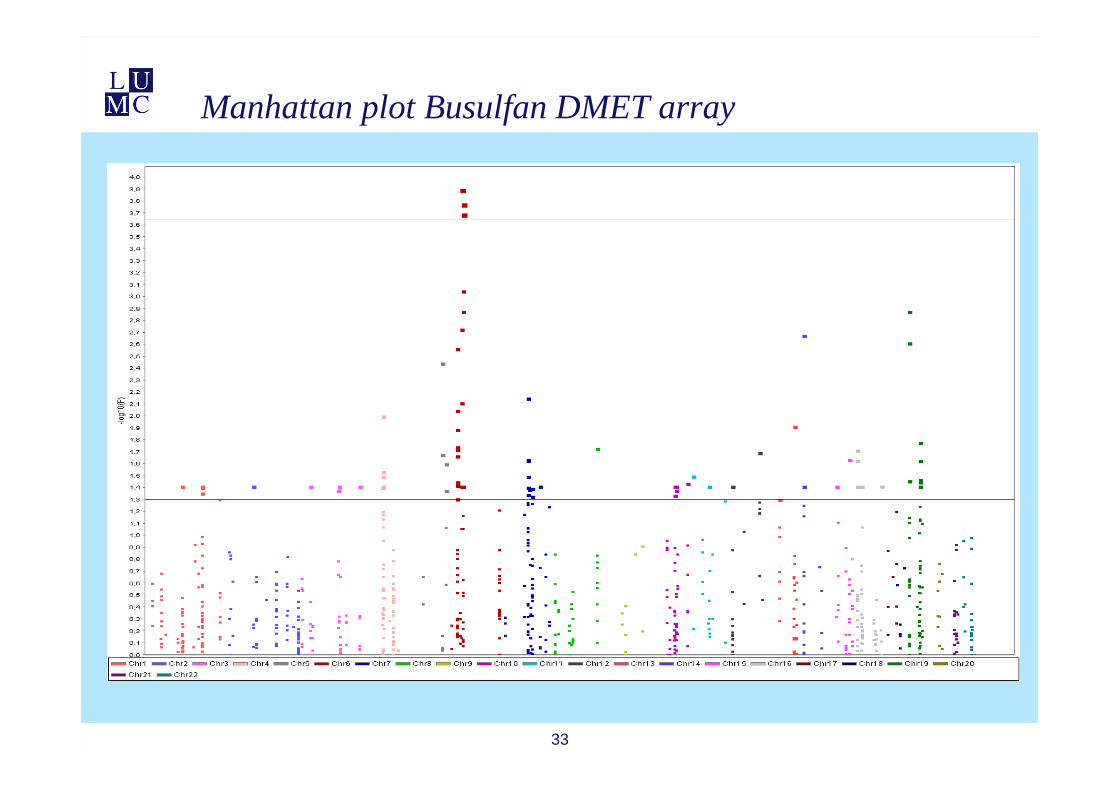
Manhattan plot Busulfan DMET array
33
34
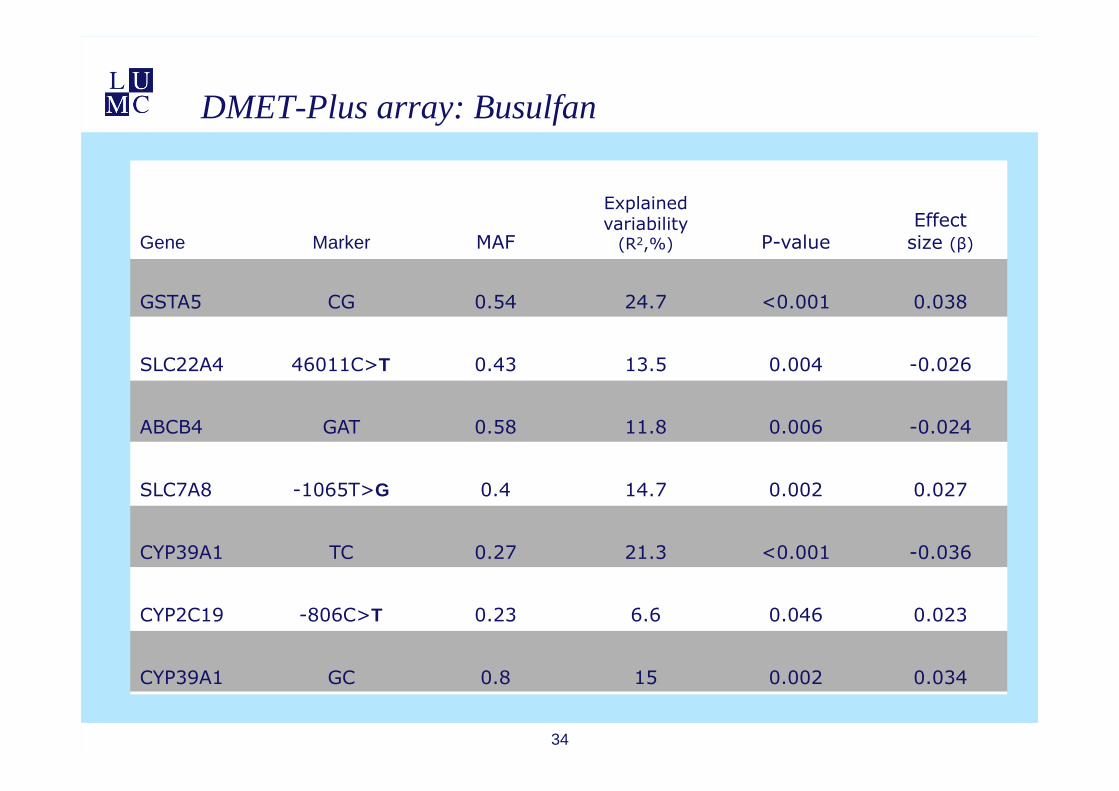
DMET-Plus array: Busulfan
Gene Marker MAF
Explainedvariability
(R2,%) P-valueEffect
size (β)
GSTA5 CG 0.54 24.7 <0.001 0.038
SLC22A4 46011C>T 0.43 13.5 0.004 -0.026
ABCB4 GAT 0.58 11.8 0.006 -0.024
SLC7A8 -1065T>G 0.4 14.7 0.002 0.027
CYP39A1 TC 0.27 21.3 <0.001 -0.036
CYP2C19 -806C>T 0.23 6.6 0.046 0.023
CYP39A1 GC 0.8 15 0.002 0.034

Genetic variants encoding drug receptor
35
receptor-agonist
Sunitinib toxicity – Pharmacogenetic biomarkers
36

37
• 219 patients treated with sunitinib from five Dutch medical centers
• mRCC (159), GIST (50), other (10)
• Toxicity was evaluated in first treatment cycle (6 weeks) by NCI–CTC-AE version 3.0
• Aim was to identify genetic markers in the PK and PD pathway of sunitinib that predispose for toxicity
• 31 single nucleotide polymorphisms in 12 candidate genes – PK and PD sunitinib
Van Erp, J Clin Oncol 2009:27(26):4406-12
Sunitinib toxicity – Pharmacogenetic biomarkers

38
RET
1580T/C
-1171C/G
-735G/A
-573G/T
738T/C 2251G/A -604T/C
-92G/A
54T/C
1191C/T
1718T/A
1501A/G
Pharmacodynamics
Van Erp, J Clin Oncol 2009:27(26):4406-12
1501A/G
39
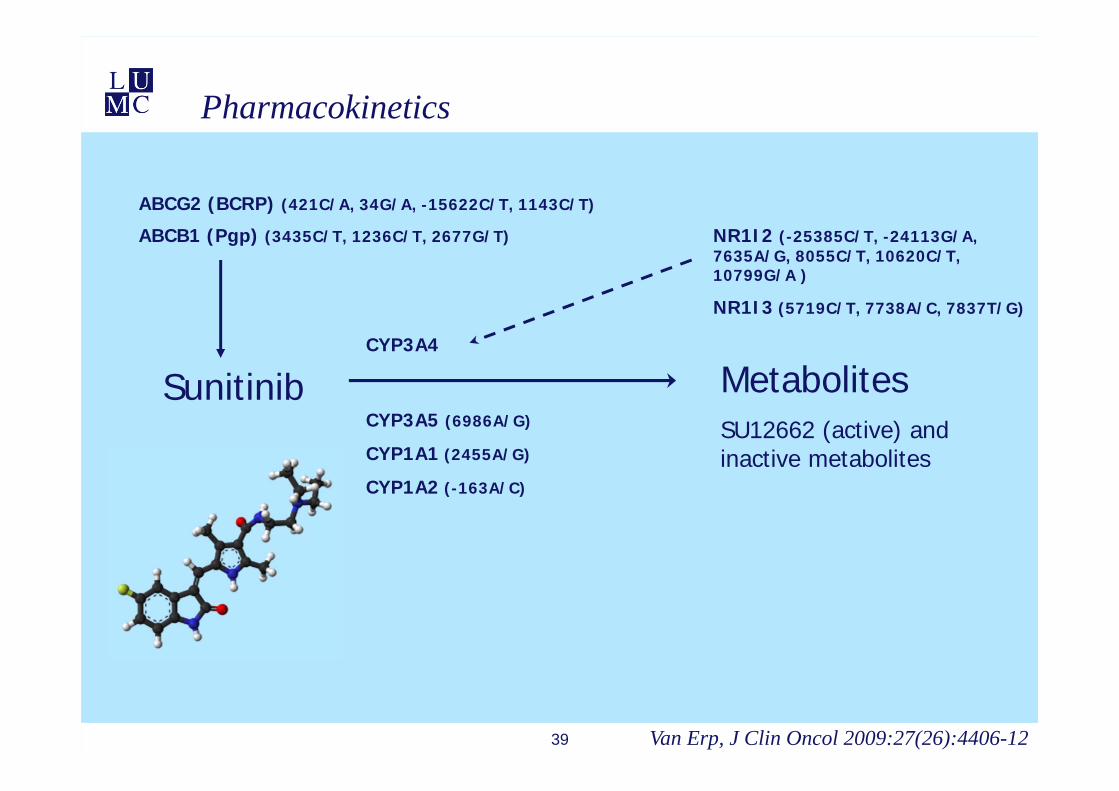
Sunitinib MetabolitesSU12662 (active) and inactive metabolites
ABCB1 (Pgp) (3435C/T, 1236C/T, 2677G/T)
ABCG2 (BCRP) (421C/A, 34G/A, -15622C/T, 1143C/T)
CYP3A4 (
CYP3A5 (6986A/G)
CYP1A1 (2455A/G)
CYP1A2 (-163A/C)
NR1I2 (-25385C/T, -24113G/A, 7635A/G, 8055C/T, 10620C/T, 10799G/A )
NR1I3 (5719C/T, 7738A/C, 7837T/G)
Pharmacokinetics
Van Erp, J Clin Oncol 2009:27(26):4406-12
40
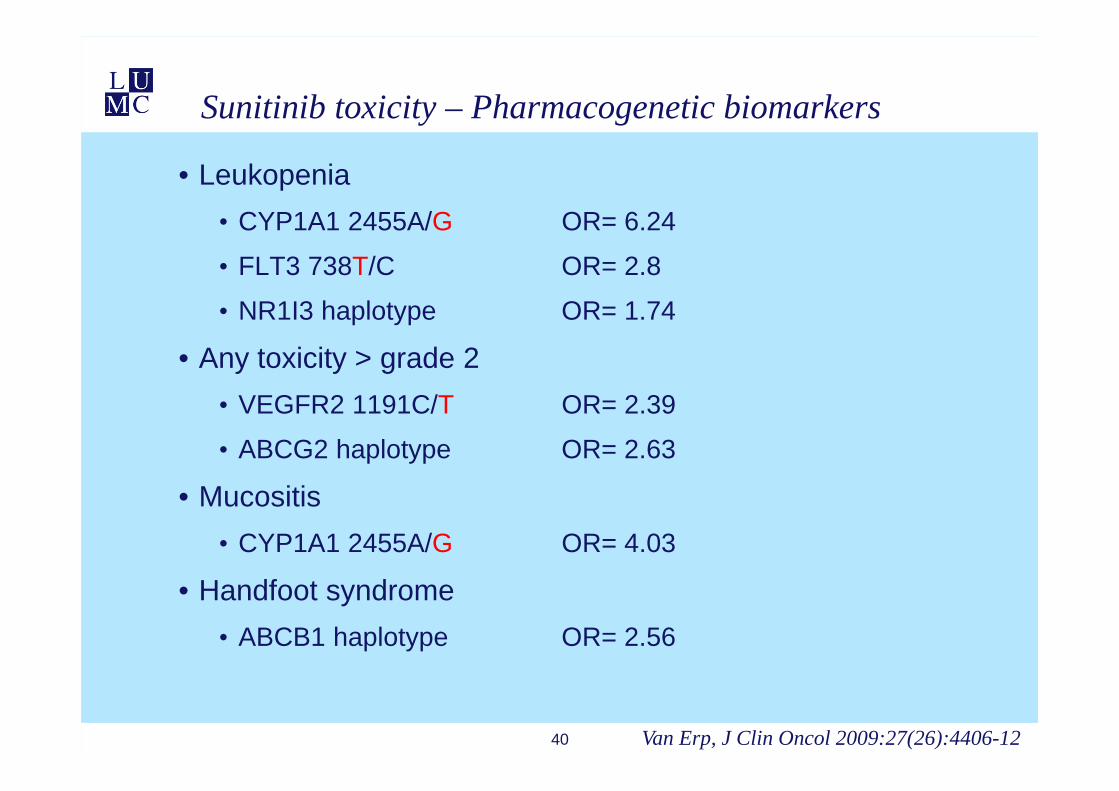
• Leukopenia• CYP1A1 2455A/G OR= 6.24
• FLT3 738T/C OR= 2.8
• NR1I3 haplotype OR= 1.74
• Any toxicity > grade 2• VEGFR2 1191C/T OR= 2.39
• ABCG2 haplotype OR= 2.63
• Mucositis• CYP1A1 2455A/G OR= 4.03
• Handfoot syndrome• ABCB1 haplotype OR= 2.56
Van Erp, J Clin Oncol 2009:27(26):4406-12
Sunitinib toxicity – Pharmacogenetic biomarkers
Sunitinib efficacy - Pharmacogenetic biomarkers
• Identify predictive biomarkers for sunitinib efficacy in mRCC
• 136 mRCC ‘clear cell’• PFS/OS
• 31 ‘single nucleotide polymorphisms’ in 12 candidate genes – PK en PD sunitinib
• Clinical characteristics41 Van der Veldt, Clin Cancer Res 2011;17(3):620-9

42
PFS OS
Favorable profile: (n=95) at least an A-allele in CYP3A5, a TCG copy in the ABCB1 haplotype or a missing CAT copy in the NR1I3 haplotype
Median PFS: 13.1 mo vs 7.5 mo (p= 0.001)
Median OS: 19.9 mo vs 12.3 mo (p= 0.009)
Sunitinib efficacy - Pharmacogenetic biomarkers
Van der Veldt, Clin Cancer Res 2011;17(3):620-9

43
How much variance is explained by pharmacogenetics?
Tamoxifen – CYP2D6

44
ON
H
C H 3
CH 3
O H
ON
H
C H 3
CH 3
ON
C H 3
C H 3
CH 3
ON
C H 3
CH 3
C H 3
O H
TAMOXIFEN 4-OH-TAM
NDM-TAM ENDOXIFEN
CYP2D6
CYP2B6CYP2C9CYP2C19CYP3A
CYP2D6
CYP3A4/5CYP1A2CYP2C9CYP2C19CYP2D6
Tamoxifen metabolism
CYP3A4/5
SULT1A1UGT
SULT1A1UGT
Dezentje, Clin Cancer Res 2009;15(1):15-21
Allel Enzymactiviteit
Genetische variant Allel frequentie (%)
Caucasisch (Europa) Japan Tanzania
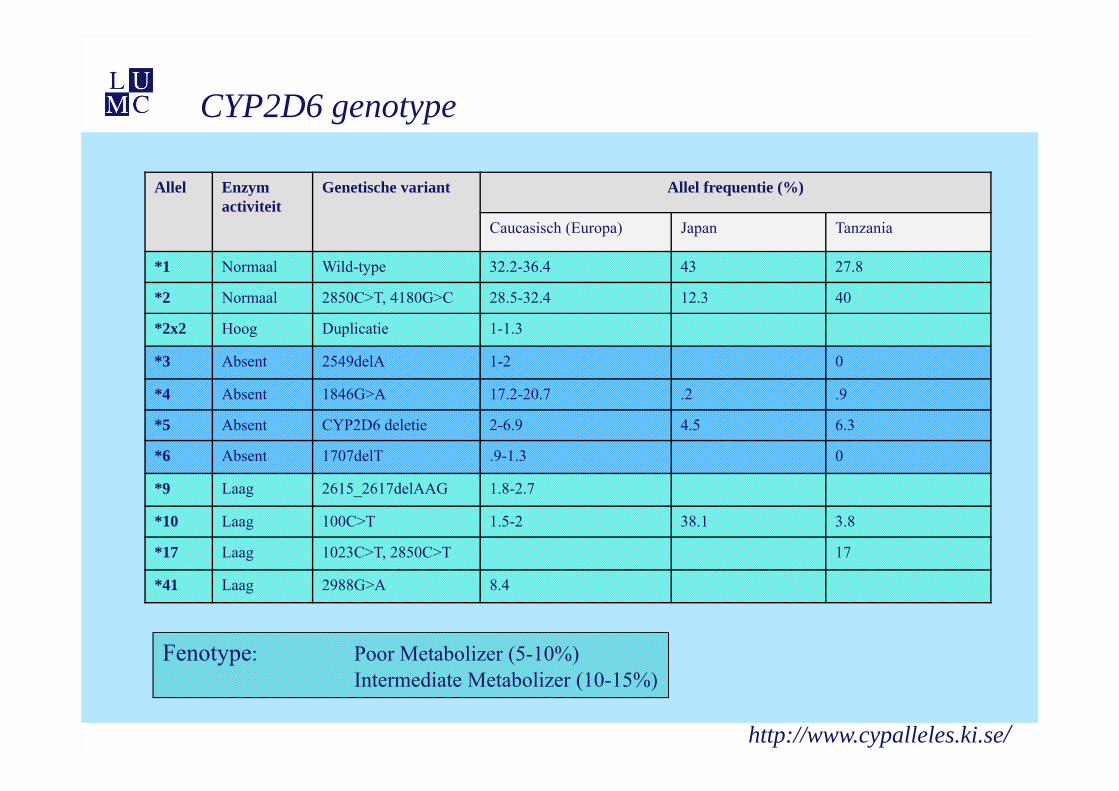
*1 Normaal Wild-type 32.2-36.4 43 27.8
*2 Normaal 2850C>T, 4180G>C 28.5-32.4 12.3 40
*2x2 Hoog Duplicatie 1-1.3
*3 Absent 2549delA 1-2 0
*4 Absent 1846G>A 17.2-20.7 .2 .9
*5 Absent CYP2D6 deletie 2-6.9 4.5 6.3
*6 Absent 1707delT .9-1.3 0
*9 Laag 2615_2617delAAG 1.8-2.7
*10 Laag 100C>T 1.5-2 38.1 3.8
*17 Laag 1023C>T, 2850C>T 17
*41 Laag 2988G>A 8.4
CYP2D6 genotype
Fenotype: Poor Metabolizer (5-10%)Intermediate Metabolizer (10-15%)
http://www.cypalleles.ki.se/

Goetz, 2005

48
Genotype to phenotype translation
Roche, AmpliChip CYP450 Test, manual
E

Presentation SABCS ‘09
CYP2D6 genotype association studies
Positive studiesN HR p
Goetz ’05 190 1.86 .08Schroth ’07 197 1.89 .02Newman ’08 68 3.6 .09Ramon ’09 91 >1 .02Bijl ’09 85 2.1 .03Kiyotani ’08/’10 282 9.5 <.001Xu ’08 152 4.7 .04Lim ’07 21 .02Bonanni ’06/’10 182 .04Schroth ’09 1325 1.29 .02
Negative studiesN HR p
Wegman ’05 76 <1 NSWegman ’07 677 <1 .055Nowell ’05 162 .67 .19Okishiro ’09 173 .6 .39Toyamo ’09 154 NSDieudonnée ’09Dezentje’10 747 1 NS
Goetz 2,880 NS
Dezentje, ASCO 2010
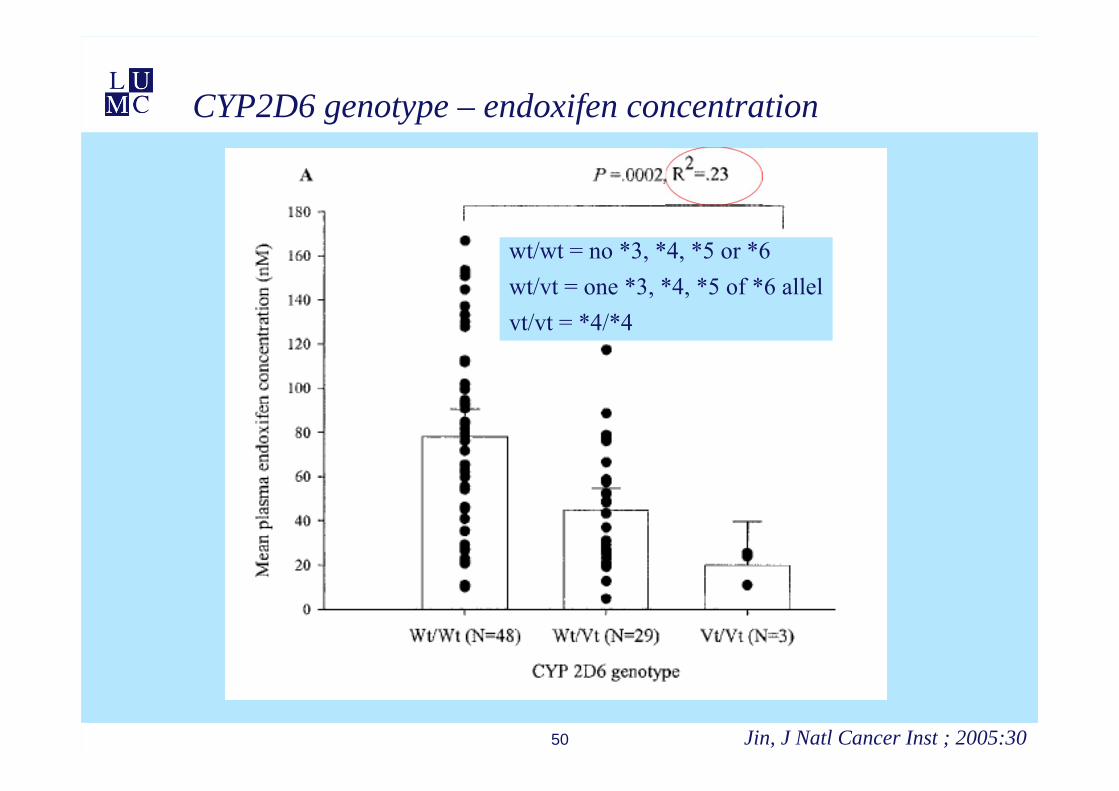
50
CYP2D6 genotype – endoxifen concentration
Jin, J Natl Cancer Inst ; 2005:30
wt/wt = no *3, *4, *5 or *6wt/vt = one *3, *4, *5 of *6 allelvt/vt = *4/*4
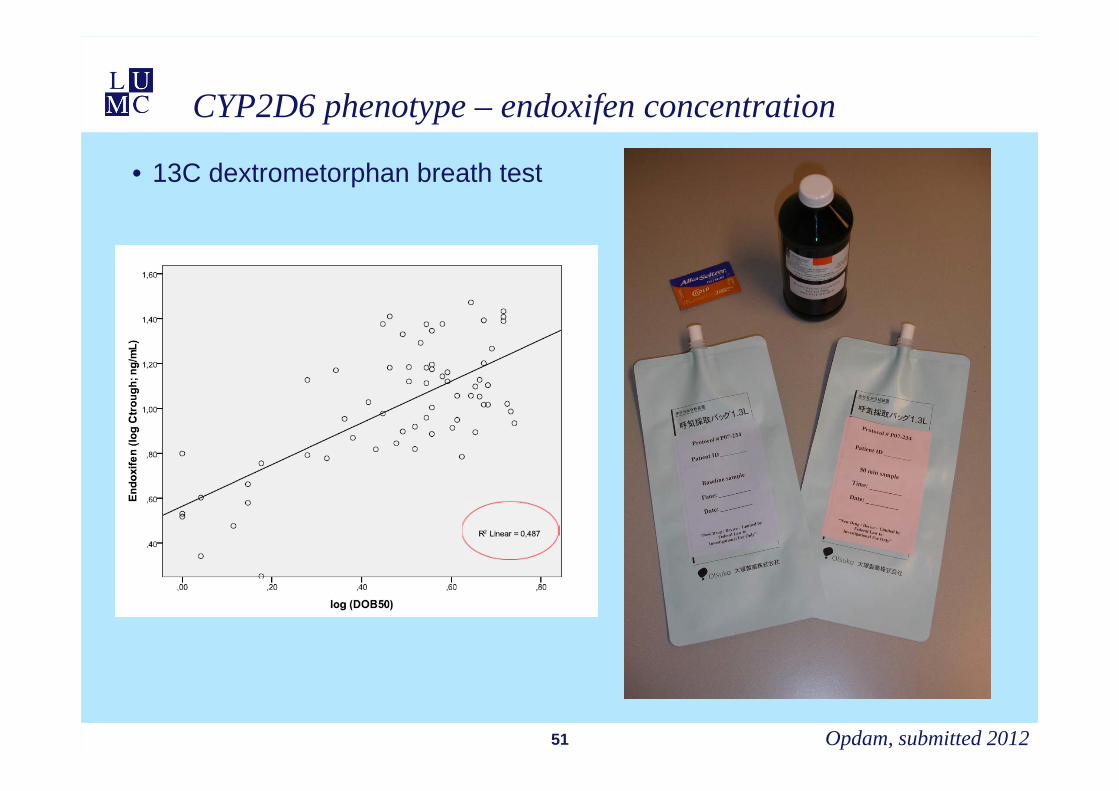
• 13C dextrometorphan breath test
51
CYP2D6 phenotype – endoxifen concentration
Opdam, submitted 2012
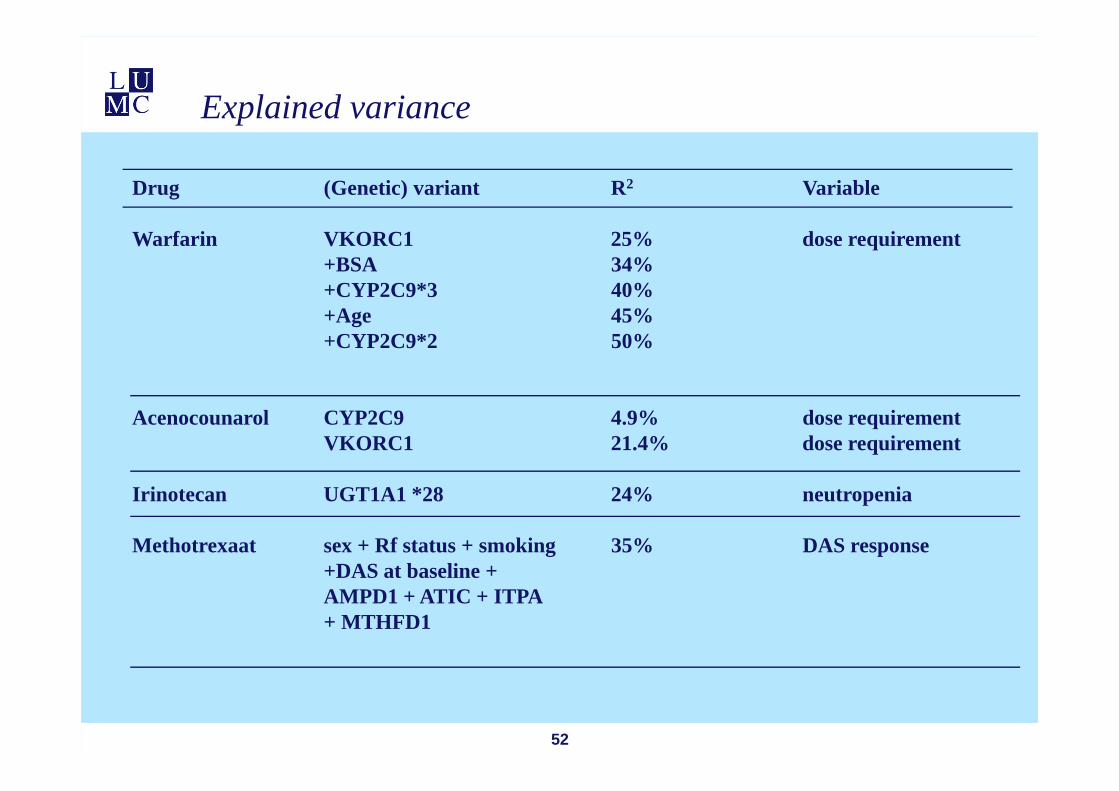
Explained variance
52
Drug (Genetic) variant R2 Variable
Warfarin VKORC1 25% dose requirement+BSA 34%+CYP2C9*3 40%+Age 45%+CYP2C9*2 50%
Acenocounarol CYP2C9 4.9% dose requirementVKORC1 21.4% dose requirement
Irinotecan UGT1A1 *28 24% neutropenia
Methotrexaat sex + Rf status + smoking 35% DAS response +DAS at baseline + AMPD1 + ATIC + ITPA + MTHFD1
Implementation PGx: How much evidence is needed?
• Randomized Clinical Trial• Endpoints: safety and efficacy
• Cost-effectiveness
• Observational evidence• Well powered, well designed
• Including replication studies
• Compare with dose adjustments
• Decreased renal function
• Drug interactions
53 Van Wielen, Pharmacogen 2011;12(9):1231
5454
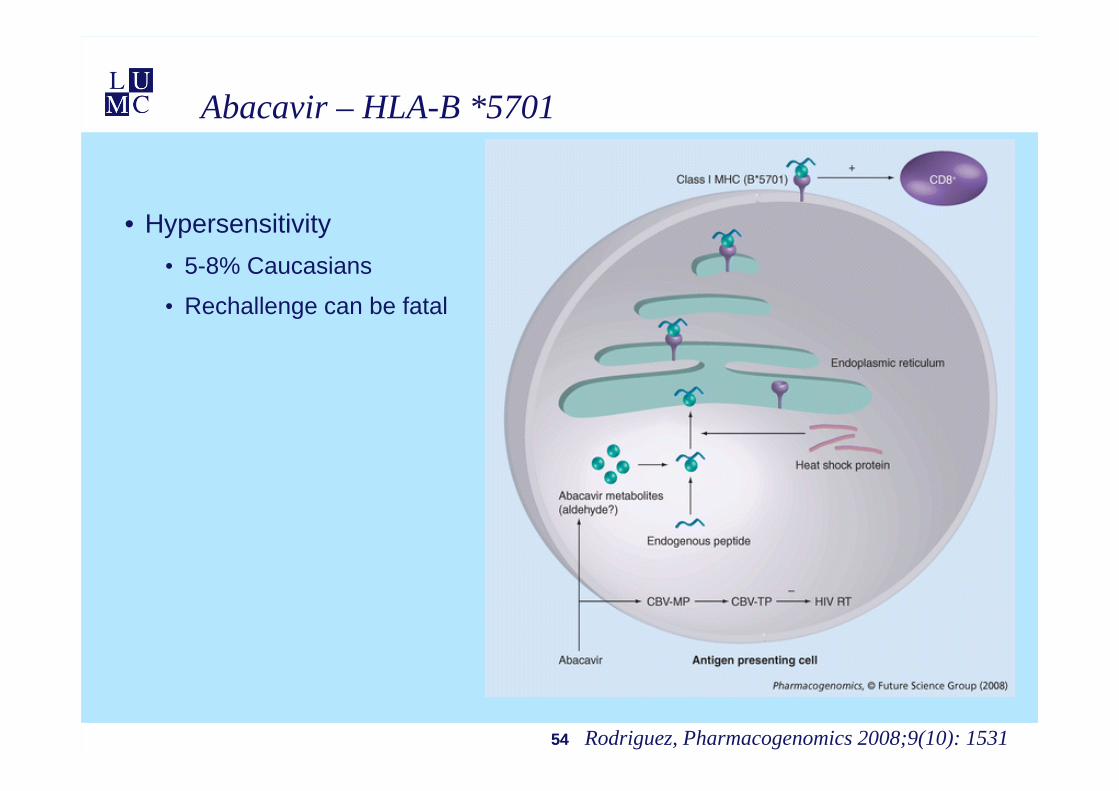
Abacavir – HLA-B *5701
• Hypersensitivity• 5-8% Caucasians
• Rechallenge can be fatal
Rodriguez, Pharmacogenomics 2008;9(10): 1531
5555
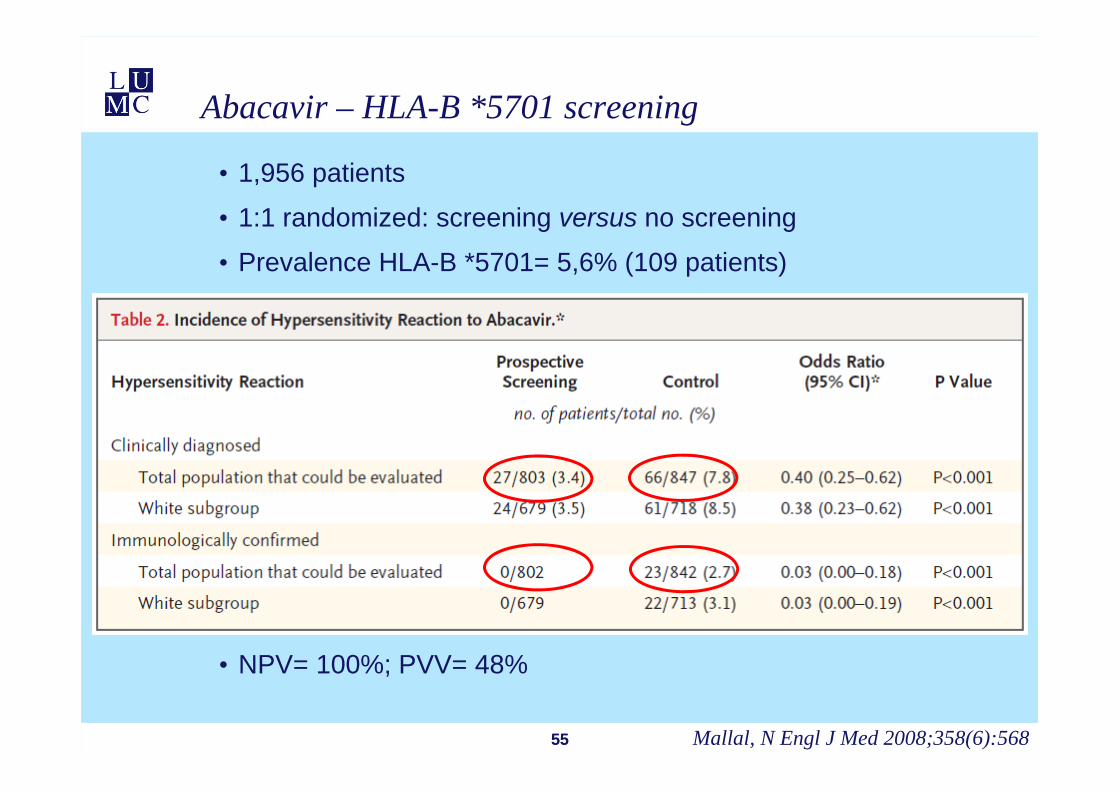
Abacavir – HLA-B *5701 screening
• 1,956 patients
• 1:1 randomized: screening versus no screening
• Prevalence HLA-B *5701= 5,6% (109 patients)
• NPV= 100%; PVV= 48%
Mallal, N Engl J Med 2008;358(6):568
Simvastatine – SLCO1B1
• Statins• Myopathy
• 1:10.000 patients per year
• Dose dependent
• Drug interactions
• cyclosporin, amiodarone
56 SEARCH, N Engl J Med 2008;359(8):789

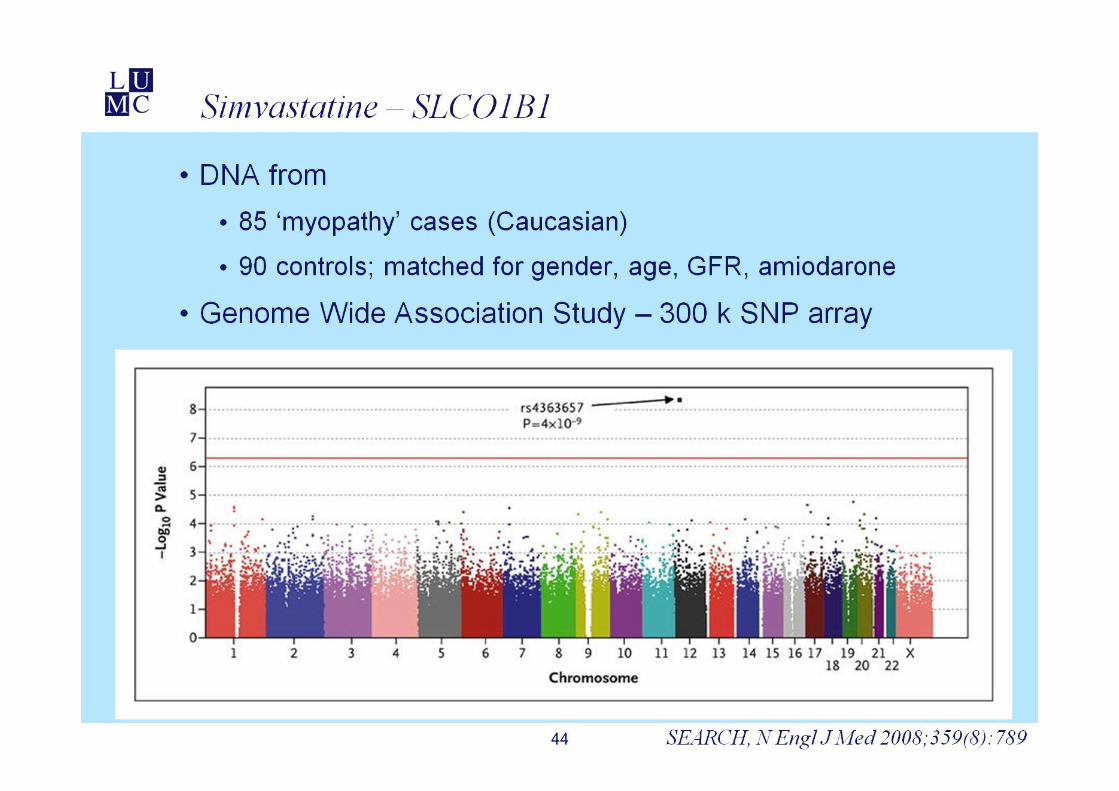

• Rs4363657 (SLCO1B1)• C-allel OR: 4.3
• CC OR: 17.4
• 60% myopathy-cases explained
• SLCO1B1 encodes OATP1B1• Uptake of statins liver
Simvastatine – SLCO1B1
59 SEARCH, N Engl J Med 2008;359(8):789

Actionable predictive biomarkers
• Endpoint current PGx studies:
• OR= 1.90
• (Un)favorable genetic profile
• Increased risk
• Association with ..
• Relationship ..
• …
• Dosing algorithm
• Decision tree
• Scoring system
• Clinical guidelines
60
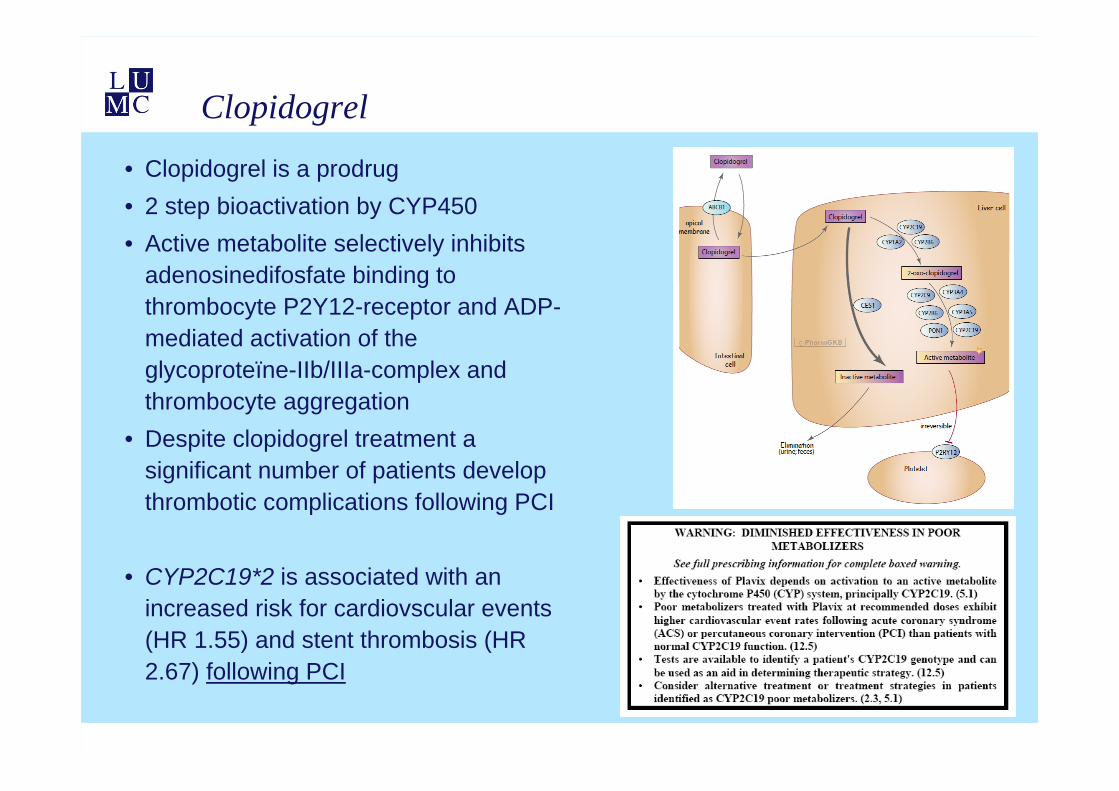
Clopidogrel
• Clopidogrel is a prodrug• 2 step bioactivation by CYP450• Active metabolite selectively inhibits
adenosinedifosfate binding to thrombocyte P2Y12-receptor and ADP-mediated activation of the glycoproteïne-IIb/IIIa-complex and thrombocyte aggregation
• Despite clopidogrel treatment a significant number of patients develop thrombotic complications following PCI
• CYP2C19*2 is associated with an increased risk for cardiovscular events (HR 1.55) and stent thrombosis (HR 2.67) following PCI
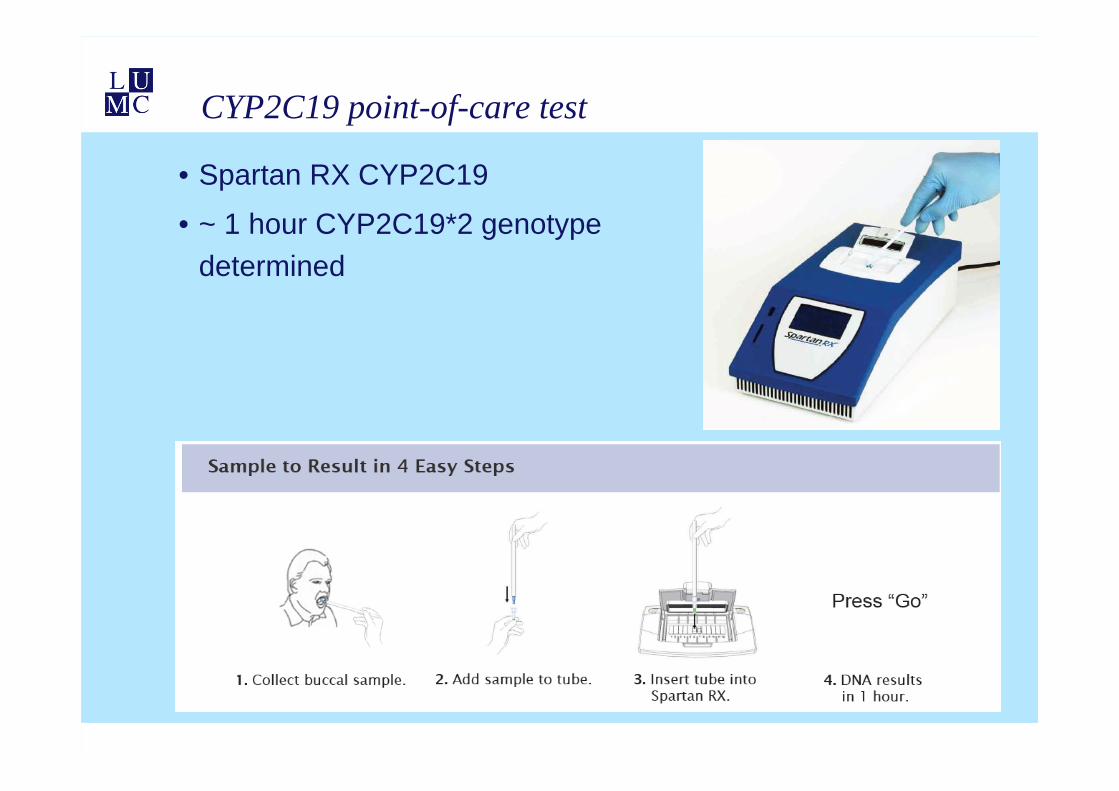
CYP2C19 point-of-care test
• Spartan RX CYP2C19
• ~ 1 hour CYP2C19*2 genotype determined
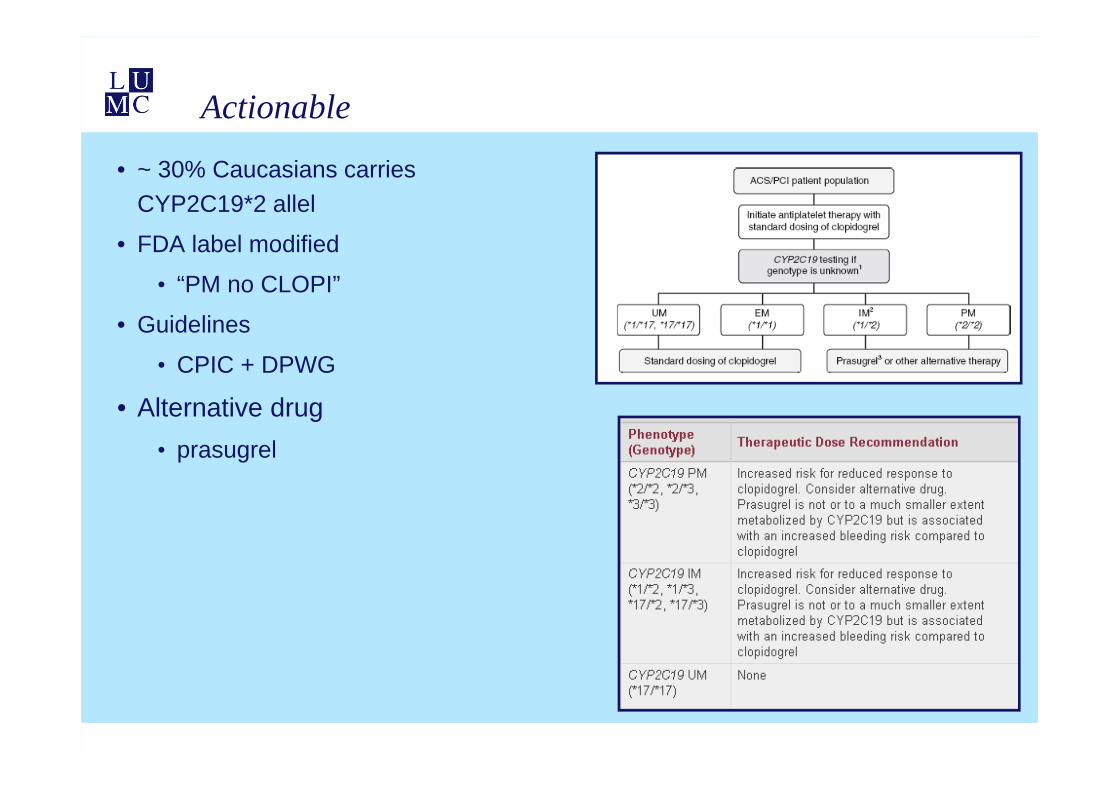
Actionable
• ~ 30% Caucasians carries CYP2C19*2 allel
• FDA label modified
• “PM no CLOPI”
• Guidelines
• CPIC + DPWG
• Alternative drug• prasugrel
DPWG
64
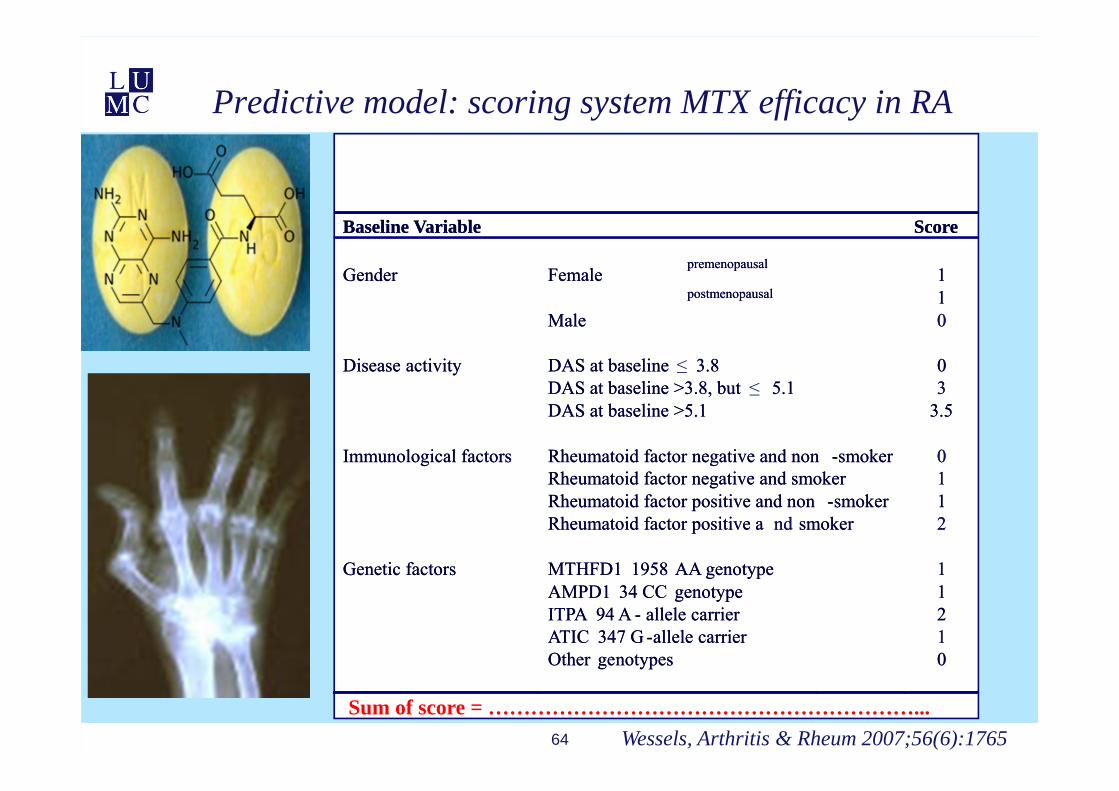
Predictive model: scoring system MTX efficacy in RA
Baseline Variable Score
premenopausal1Gender Female
postmenopausal 1Male 0
Disease activity DAS at baseline 3.8 0DAS at baseline >3.8, but 5.1 3DAS at baseline >5.1 3.5
Immunological factors Rheumatoid factor negative and non -smoker 0Rheumatoid factor negative and smoker 1Rheumatoid factor positive and non -smoker 1Rheumatoid factor positive a nd smoker 2
Genetic factors MTHFD1 1958 AA genotype 1AMPD1 34 CC genotype 1ITPA 94 A - allele carrier 2ATIC 347 G -allele carrier 1Other genotypes 0
Baseline Variable Score
premenopausal1Gender Female
postmenopausal 1Male 0
Disease activity DAS at baseline 3.8 0DAS at baseline >3.8, but 5.1 3DAS at baseline >5.1 3.5
Immunological factors Rheumatoid factor negative and non -smoker 0Rheumatoid factor negative and smoker 1Rheumatoid factor positive and non -smoker 1Rheumatoid factor positive a nd smoker 2
Genetic factors MTHFD1 1958 AA genotype 1AMPD1 34 CC genotype 1ITPA 94 A - allele carrier 2ATIC 347 G -allele carrier 1Other genotypes 0
≤≤
Wessels, Arthritis & Rheum 2007;56(6):1765Sum of score = ……………………………………………………...

65
Good clinical response
Good clinical response (proportion at t= 6 months)
Wessels, Arthritis & Rheum 2007;56(6):1765

Is pharmacogenetic testing feasible?
$1,0 $10,0
$100,0 $1000,0
$10000,0 $100000,0
$1000000,0 $10000000,0
$100000000,0 $1000000000,0
Wetterstrand KA. www.genome.gov/sequencingcosts

Genotyping technology
67
Taqman
Pyrosequenching
High Resolution Melting
68
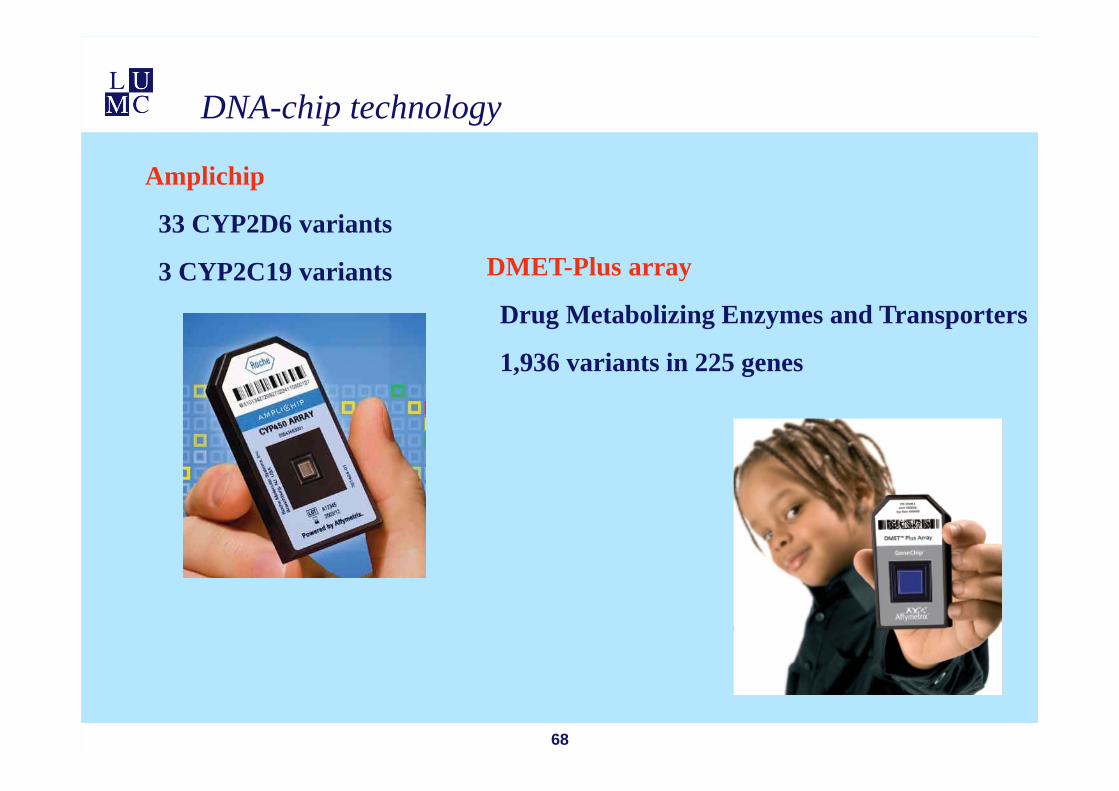
DNA-chip technology
Amplichip
33 CYP2D6 variants
3 CYP2C19 variants DMET-Plus array
Drug Metabolizing Enzymes and Transporters
1,936 variants in 225 genes
69
Affymetrix fluidic station 450Dx en Scanner 3000Dx
Pharmacogenetic service: genotyping and consult
70
http://www.lumc.nl/con/3092/
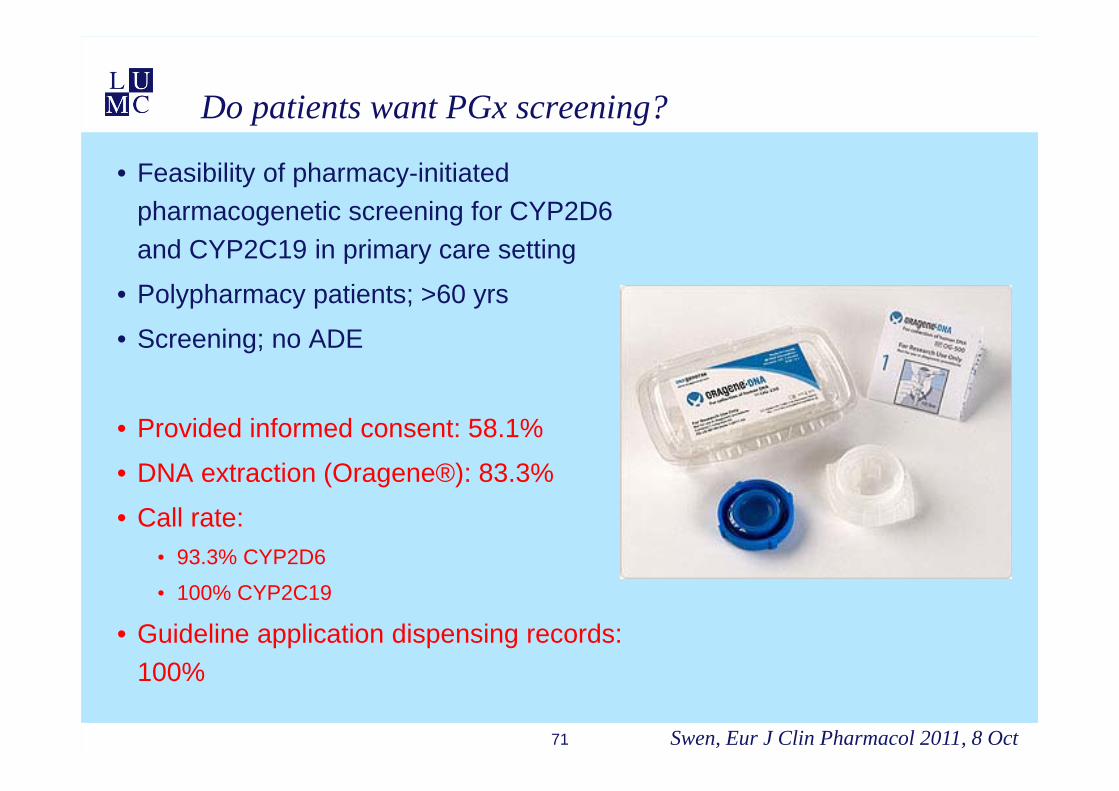
Do patients want PGx screening?
• Feasibility of pharmacy-initiated pharmacogenetic screening for CYP2D6 and CYP2C19 in primary care setting
• Polypharmacy patients; >60 yrs
• Screening; no ADE
• Provided informed consent: 58.1%
• DNA extraction (Oragene®): 83.3%
• Call rate:• 93.3% CYP2D6
• 100% CYP2C19
• Guideline application dispensing records: 100%
71 Swen, Eur J Clin Pharmacol 2011, 8 Oct
Adoptation of PGx by US Physicians: National survey
• To benchmark physicians’ level of knowledge and extent of use of PGx testing
• 397,832 questionnaires
• 10,303 respondents
• 97.6% agreed that genetic variations may influence drug response
• 10.3% felt adequately informed about PGx
• 29% had received any PGxeducation
• 12.9% had ordered a PGx test (6 mo)
pharmacological expertise
Stanek, Clin Pharmacol Ther 2012;91(3):450
Difficulties in interpretation
• One gene – one drug• TPMT – mercaptopurine• UGT1A1 – irinotecan• HLA *5701 - abacavir
• One gene – many drugs• CYP2D6, CYP2C19• polypharmacy
• More genes – one drug• Tricyclic antidepressants
• More genes – many drugs
• Pharmacological knowledge clinical pharmacist
• Drug metabolism, interactions
73
75
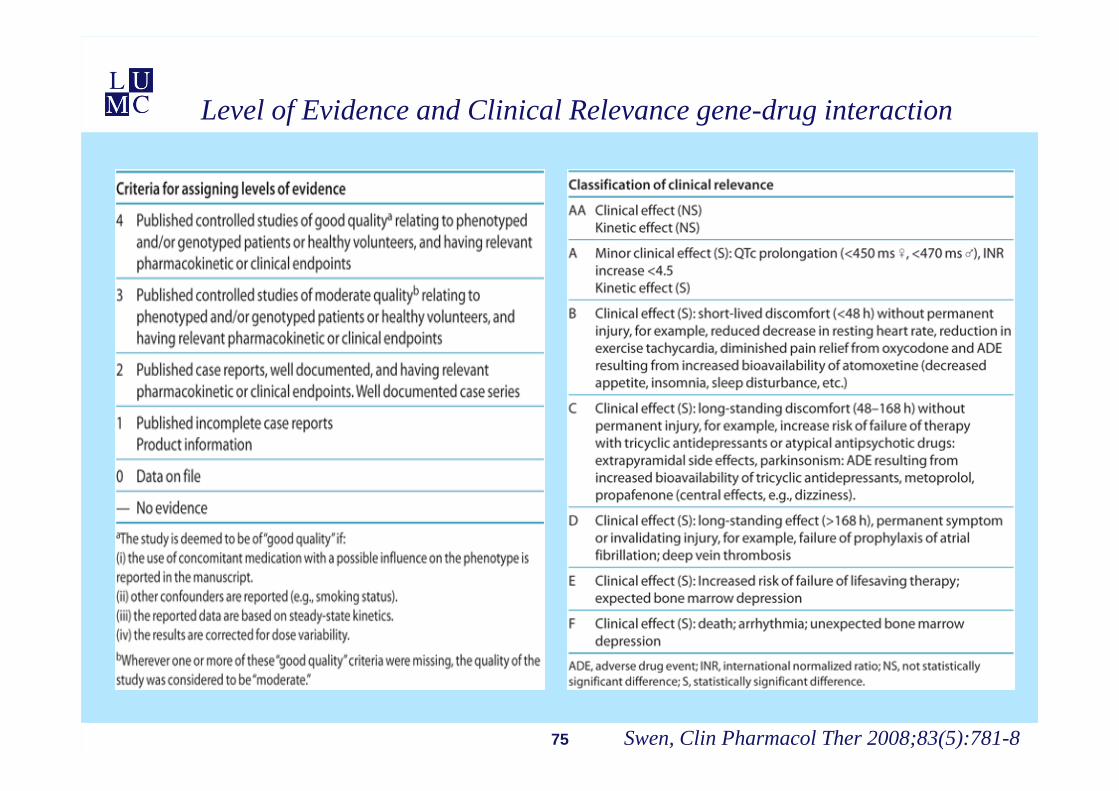
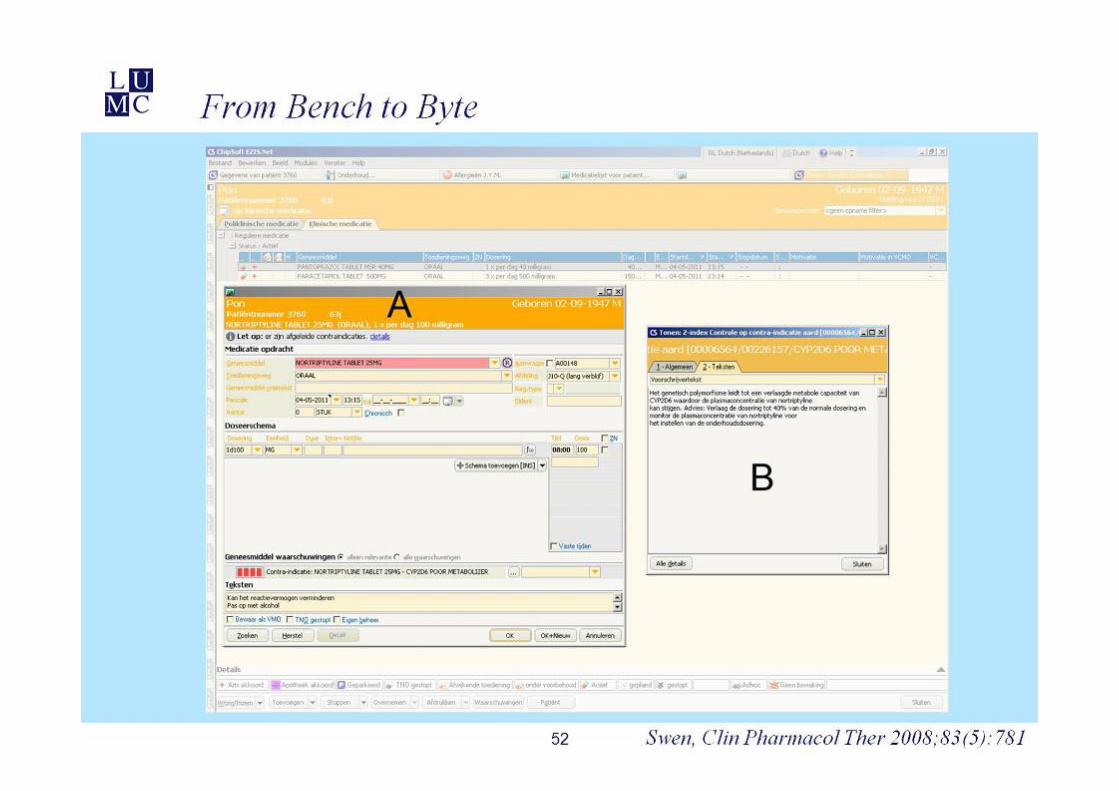
Level of Evidence and Clinical Relevance gene-drug interaction
Swen, Clin Pharmacol Ther 2008;83(5):781-8

Swen et al, Clin Pharmacol Ther. 2011 ;89(5):662

www.pharmgkb.org
78
Dosing guidelines
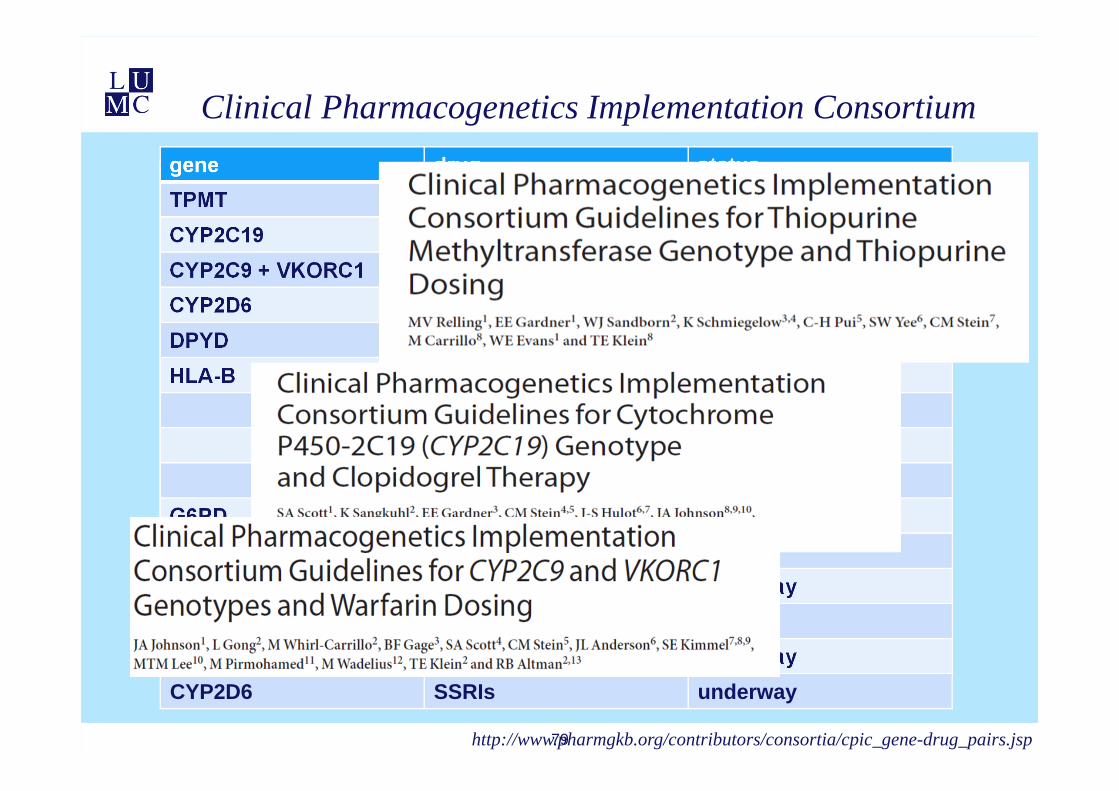
gene drug statusTPMT thiopurines publishedCYP2C19 clopidogrel publishedCYP2C9 + VKORC1 warfarin publishedCYP2D6 codeine publishedDPYD 5FU/capecitabine underwayHLA-B abacavir published
carbamazepine underwayphenytoin plannedallopurinol underway
G6PD rasburicase underwayUGT1A1 irinotecan plannedIL28B pegintron underwaySLCO1B1 simvastatin in pressCYP2D6 + CYP2C19 Tricyclic antidepress. underwayCYP2D6 SSRIs underway
79
Clinical Pharmacogenetics Implementation Consortium
http://www.pharmgkb.org/contributors/consortia/cpic_gene-drug_pairs.jsp
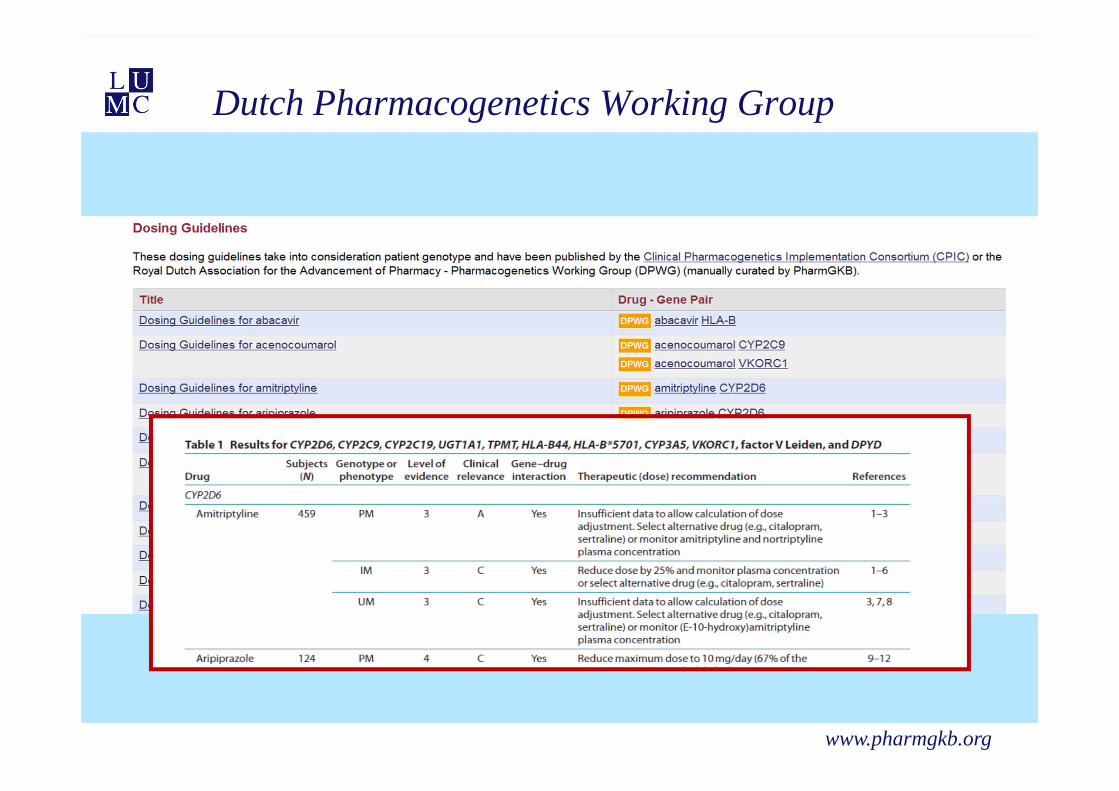
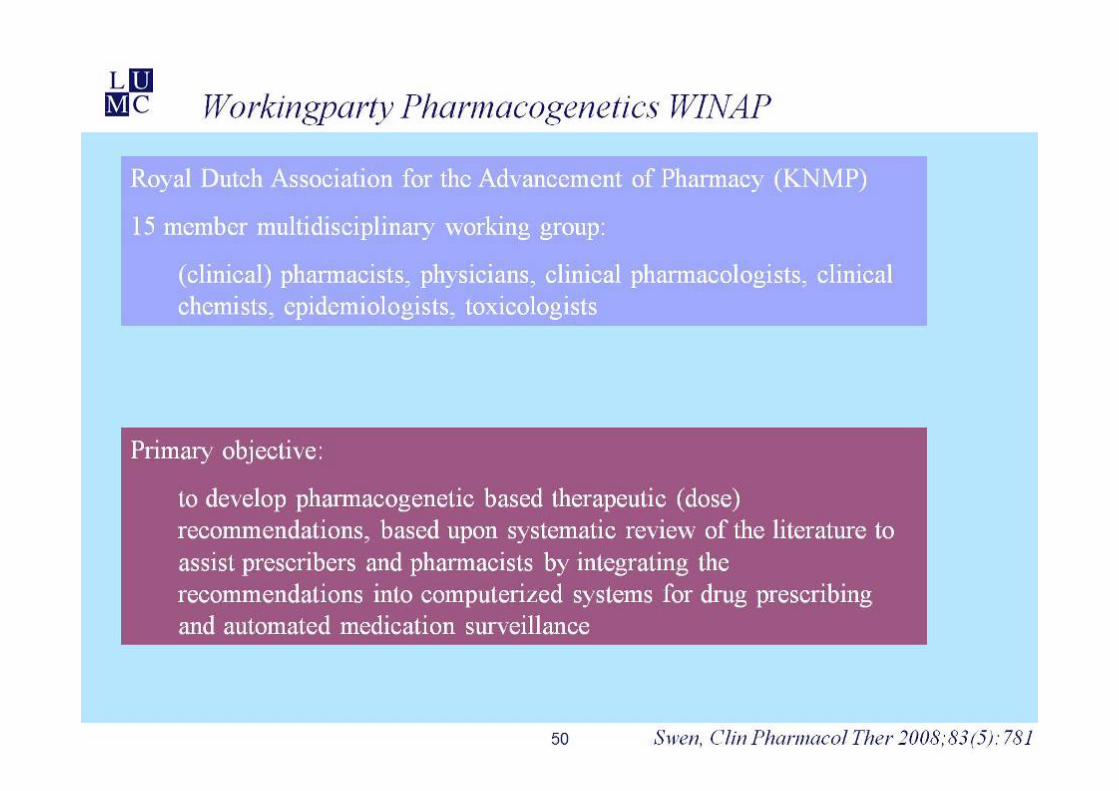
Dutch Pharmacogenetics Working Group
www.pharmgkb.org
81
Personal view for PGx (germline) testing recommendations
• TPMT – thiopurines
• CYP2C19 – clopidogrel
• CYP2C9-VKORC1 – coumarines
• DPYD – 5FU/capecitabine
• HLA-B – abacavir/carbamazepine
• G6PD – rasburicase
• UGT1A1 – irinotecan
• IL28B – pegintron
• SLCO1B1 – statine + spierpijn
• CYP2D6 – tamoxifen
• CYP3A5 - tacrolimus
• If I was a patient
82
Conclusions
• Drug response is a heritable trait
• Biomarkers are needed for predicting drug response
• Polygenetic markers in both the PK and PD predispose for toxicity and efficacy
• To increase the explained variance genetic markers should be combined with other determinants of drug response
• Pharmacogenetic studies should report actionable results
• Observational evidence from well designed and replicated studies may be acceptable to adjust the dose
• Pharmacogenetics is feasible in the clinic and well accepted by patients and physicians
• Pharmacogenetic guidelines for interpretation of test results are available
• There is an opportunity for clinical pharmacists to fulfill a new clinical role as an expert in PGx
83
84
Thanks to
Dr Tahar van der Straaten
Laboratory for Experimental and Clinical Pharmacogenetics
Prof dr Tom HuizingaProf dr Hans Gelderblom
Dr Jesse Swen


















