
Family Nurse Practitioners and Family Focused Nursing
54
Family Focused Nursing Practice Sharon A. Denham, PhD, RN Professor Emeritus, Ohio University School of Nursing Houston J. & Florence A. Doswell Endowed Chair in Nursing for Teaching Excellence, Texas Woman’s University, Dallas Campus
-
Upload
sharon-denham -
Category
Documents
-
view
41 -
download
4
description
This is the presentation initially shared with FNP students at Texas Woman's University College of Nursing in Dallas Texas on June 4, 2014
Transcript of Family Nurse Practitioners and Family Focused Nursing
Family Focused Nursing Practice
Sharon A. Denham, PhD, RNProfessor Emeritus, Ohio University School of Nursing
Houston J. & Florence A. Doswell Endowed Chair in Nursing for Teaching Excellence, Texas Woman’s University, Dallas Campus
Objectives
At the conclusion of this webinar, participants will be able to:
Discuss today’s changing landscape & needs for care delivery
Identify usefulness of the Family Health Model (Denham, 2003) Identify essential aspects of “thinking family” in nursing practice Characterize the nursing practices needed for relationship based care delivery Describe how a family lens can be used to drive care delivery across multiple contexts
Implications of Changing Health
Care System Landscape
∗Affordable Health Care Act∗Technology∗Growth in Knowledge∗Roles of Health Practitioners∗Consumers∗Chronic Illness Care Needs∗Aging Populations∗Increasing Diversity of the U.S. Population∗$$$$$$$
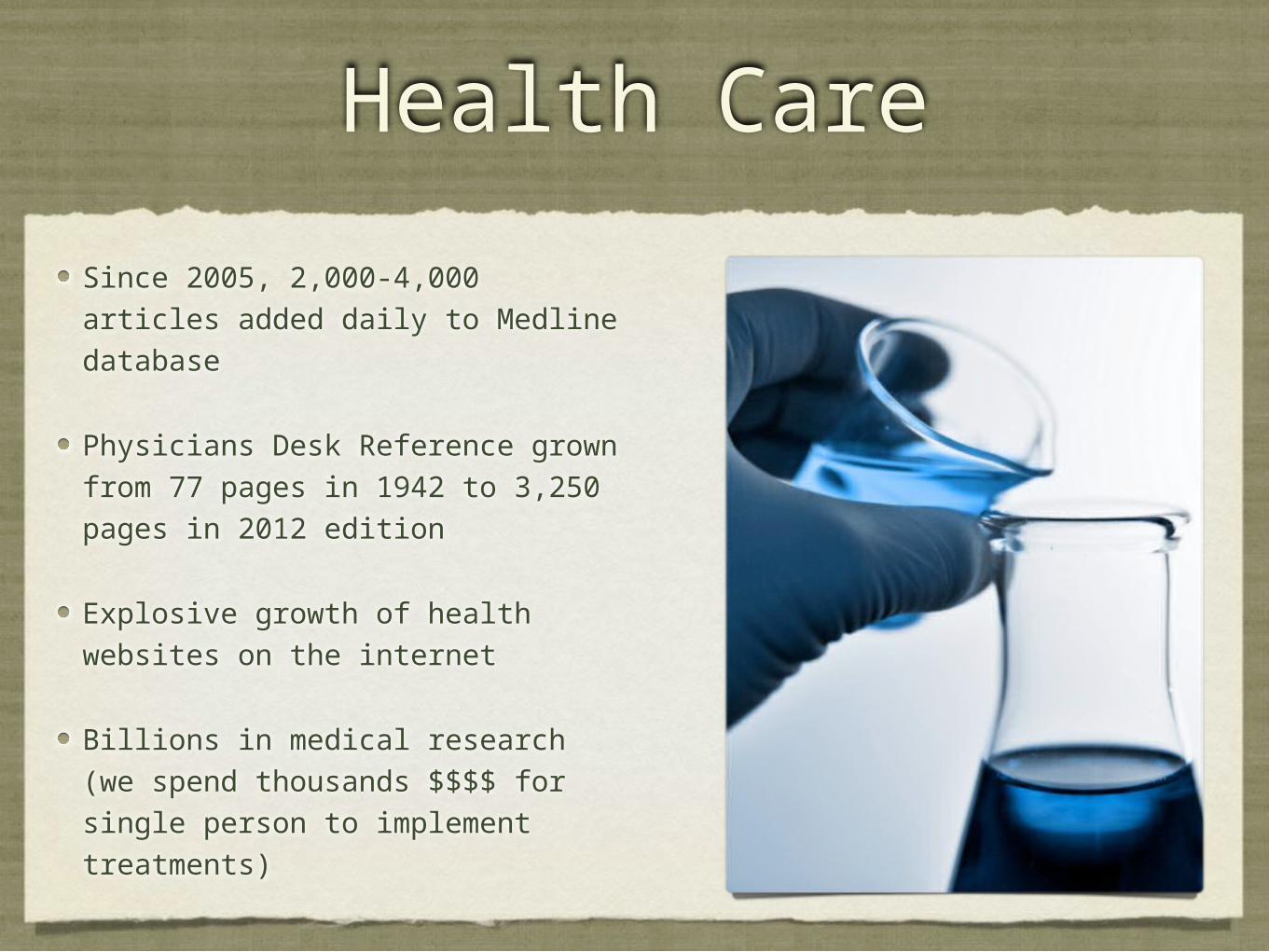
Health Care
Since 2005, 2,000-4,000 articles added daily to Medline database
Physicians Desk Reference grown from 77 pages in 1942 to 3,250 pages in 2012 edition
Explosive growth of health websites on the internet
Billions in medical research (we spend thousands $$$$ for single person to implement treatments)
divorc
e
Shared
commitm
enta loose affiliation
people descended from a common
ancestorFundamental social
group
blood
wedloc
k shared genetics
arranged
co-
habitation
group
foster care
a person having kinship with another or
others
aunts & uncles
adoptio
n
household
living under one
roof
basic unit of society
association of people who share common beliefs or activities
step-
families
chosen
blended families
kinship parents
children
biological classificationcommon ancestry
extended
relativesprocreation
family of orientation
economics
conjuga
l
nuclear
a social unit living
together
matriloca
lspouse
groups linked through descent
partner
consanguinal
Same Sex
grandparents
patriarchal
Illness Care System
Exceptional almost miraculous
Billions wasted on unnecessary & inefficient services
Millions get too much or too little
Quality of care vs. volume of care services
Questions about the quality, adequacy, equity, value & satisfaction with care
Health vs. Illness
Acute illness: short duration, but usually severe
Chronic illness: persistent illness for >6 months, can worsen or get better
Health: “State of complete physical, mental and social well-being, not merely the absence of disease…”
www.diabetesfamily.net/family
see: Family Health Model
“An Ethnographic Study of Family Health in Appalachian Microsystems” (1995 -1996)
8 Appalachian families/4 interviews with each
Family Health During Transitional Change (funded by the American Nurses Foundation, 1996)
Family Health in a Disadvantaged Population (funded by the College of Health and Human Sciences, 1997)
Nurturing & emotionally supportive
A caring unit for its members
Meets individual needs, celebrates, and values members
Dynamic changes are likely to occur over the life course
HEALTHY FAMILY
Family Health
An adaptive state that occurs across the life course as the family unit serves as a major resource for the day-to-day living and wellbeing of its members.
A household phenomenon that effectively uses available resources to maximize the wellbeing of its members and the family unit through supportive interactions with their embedded systems, dynamic relationships, and member routines.
It is experienced when individuals fulfill personal goals, enjoy a meaningful life, and experience full capacity of wellbeing.
“Think Family”
Every time you see an individual...
Even when others are not physically present...
Note similar care needs in families with children & those with adult members
Family Theory (Domains)
Family Structure
Family Function
Family Process
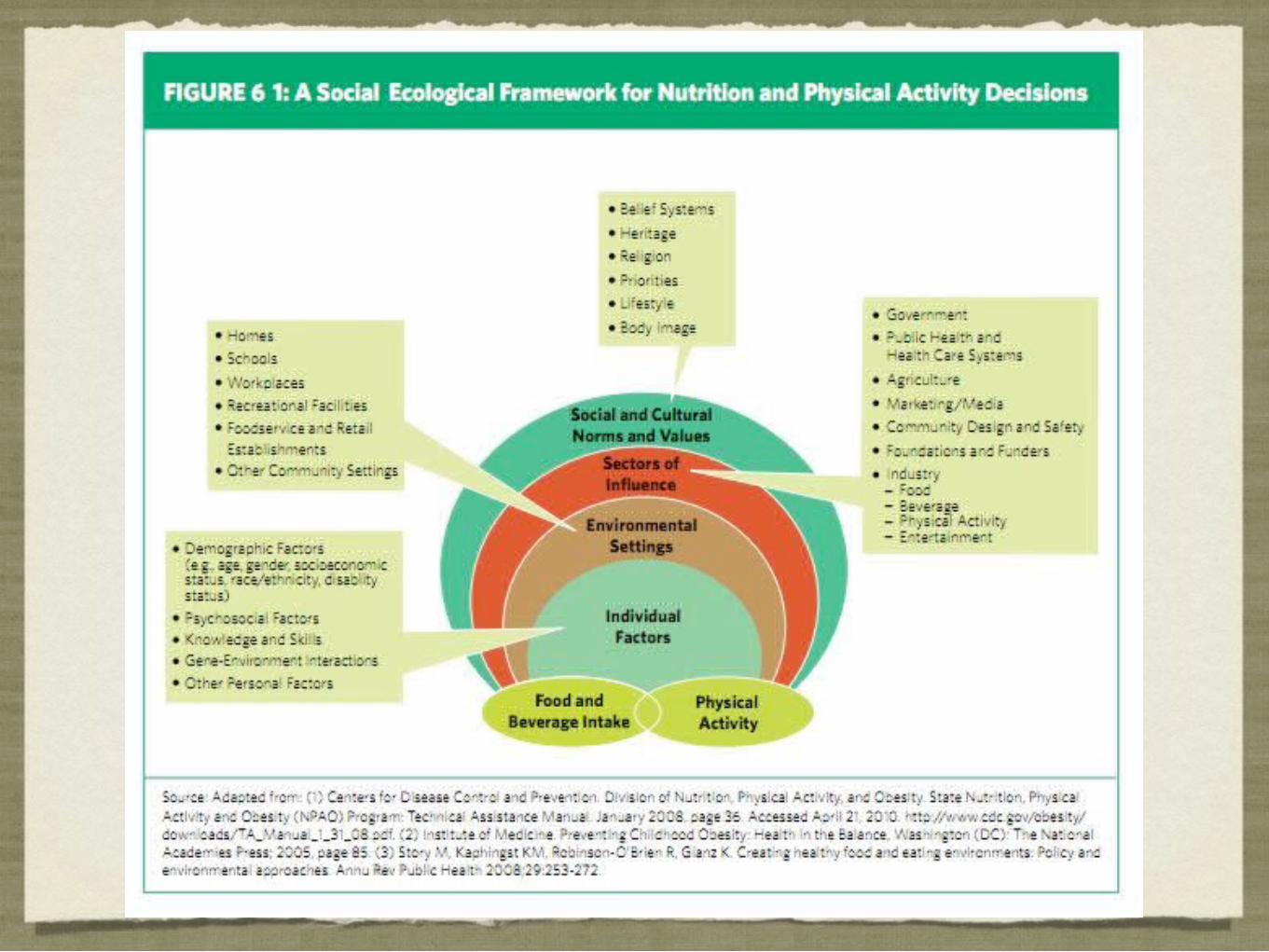
Family Systems Theories Family Health Model
• Contextual Domain
• Functional Domain
• Structural Domain
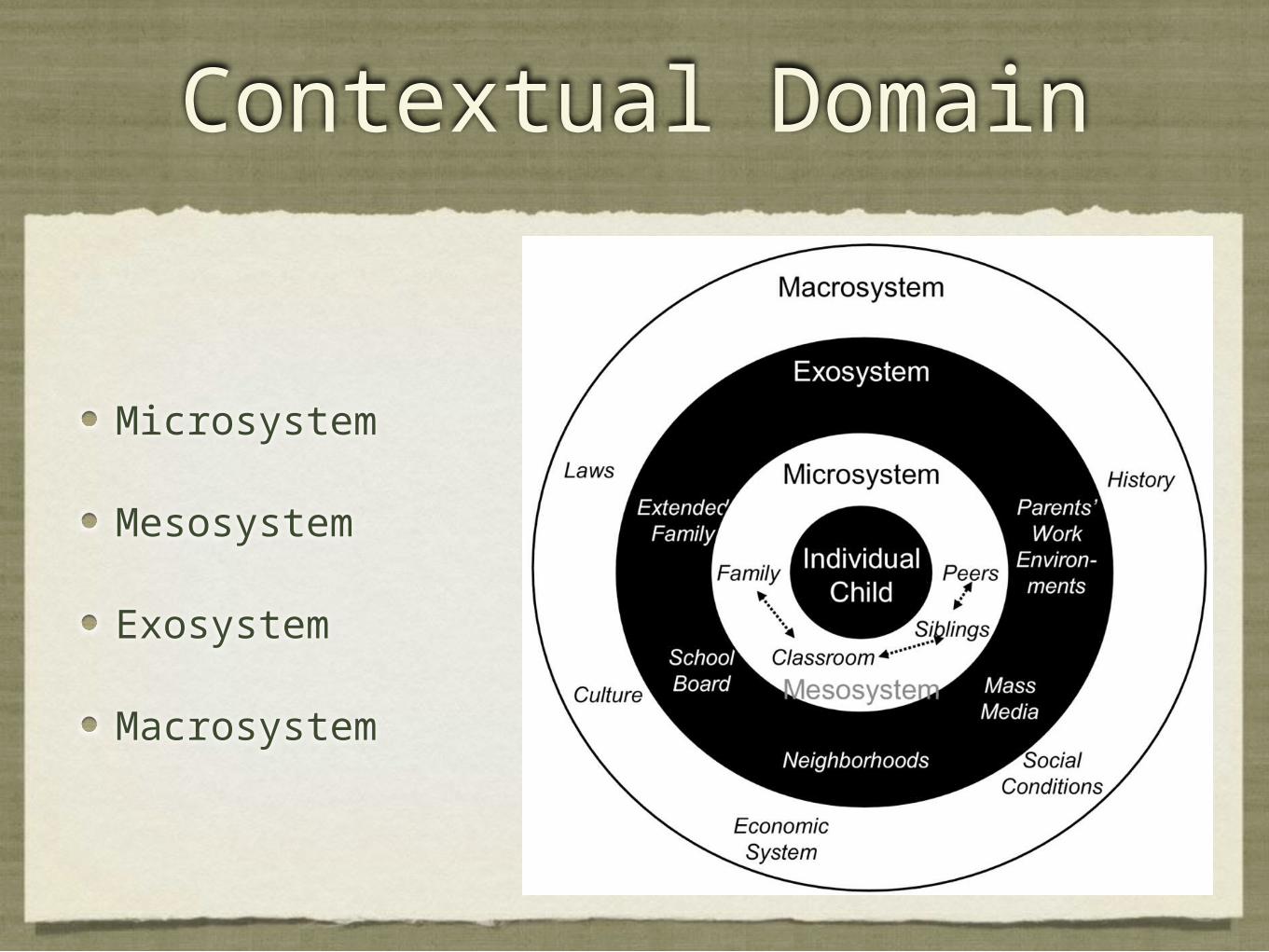
Contextual Domain
Microsystem
Mesosystem
Exosystem
Macrosystem

Contextual Domain
Household niche
Immediate neighborhood
Family members & close links to others that are like family
Characteristics, genetics, race, age, spirituality, culture, and other family traits
Microsystem

My Family Microsystem
Contextual Domain
Mesosystem: Multiple influences as individuals interact within member sub-systems within & outside the household niche.
Exosystem: Systems that do not directly involve individuals as active participants, but events still effect the family.
Macrosystem: Policy (e.g., social, health, public); larger environments
Chronosystem Timing of events. Number of events in a given time. Length of time of events. Perceptions of time over time. Social life course. Time and place. Human agency. Timing of lives. Interdependent lives. Actual passage of time. Special moments in time. Age differences. Intergenerational transmission. Historical past. Experienced and inexperienced present. Desired futures.

Normative & Non-Normative Events
Normative Events
* Events that developing persons and families anticipate; culturally bound events; have shared meanings (e.g., birth, puberty, graduation, marriage, retirement, etc.).
Non-Normative Events
* Events that appear unexpectedly; families ill-prepared; may be viewed as crisis; linked to historical contexts (e.g., genetic disorder, divorce, losing job, premature death, chronic illness, etc.)
Functional Domain
Individual factors (e.g., values, attitudes, beliefs, abilities, & roles)
Member processes (e.g., communication, leadership, decision making, problem solving, etc.).... dyads & triads
Family unit processes (e.g., cohesiveness, individuation, identity, boundaries, resilience, etc.)
Functional Domain
Relationships with others
Relationships with social systems and larger society Member development, health, and well-being Ways family resources are used Influences family health potentials and how they are met or unmet
Core Family Processes
Caregiving
Cathexis
Celebration
Change
Communication
Connectedness
Coordination
Caregiving
Health maintenance Disease prevention Risk reduction Health promotion Illness care Rehabilitation Acute episodic needs Chronic care concerns
Cathexis
Attachment Commitment Affiliation Loss Grief and mourning Normative life processes Complicated life processes
Celebration
Culture Family fun Traditions Rituals Religion/faith practices Hobbies Shared activities
Change
Control Meeting expressed needs Meanings of change Contextual influences Compare and contrast Similarities and differences Diversity

Communication Language Symbolic interactions Information access Coaching Cheerleading Teaching Counseling Knowledge and skills Emotional needs Affective care Spiritual needs
Connectedness Partnering relationships Kin networks Household labor Cooperation Member roles Family rules Boundaries Tolerance for ambiguity Marginalization
Coordination
Family tasks Forgiveness Problem solving Decision making Valuing Coping Resilience Respect Reconciliation Stress Management
Structural Domain
Rituals, traditions, & routines
Family health routines
Structural Domain
Ways members use beliefs, values, attitudes, information, knowledge, resources, & experience to construct behaviors that impact health & illness.
Provides insight into individual & collective behaviors lifestyle & health behaviors.
Useful for assessment, intervention, & evaluation of the complex patterns affecting individual & family health or illness.
Structural Domain
Prior research suggests that family routines have potential for conceptualization, planning and implementation of interventions to promote healthy lifestyles & manage chronic diseases.
(Denham, 2002a; Denham, 2002b)
Family Health Routines
Self-care Safety and precautions Mental health behaviors Family care Illness care Member care-taking
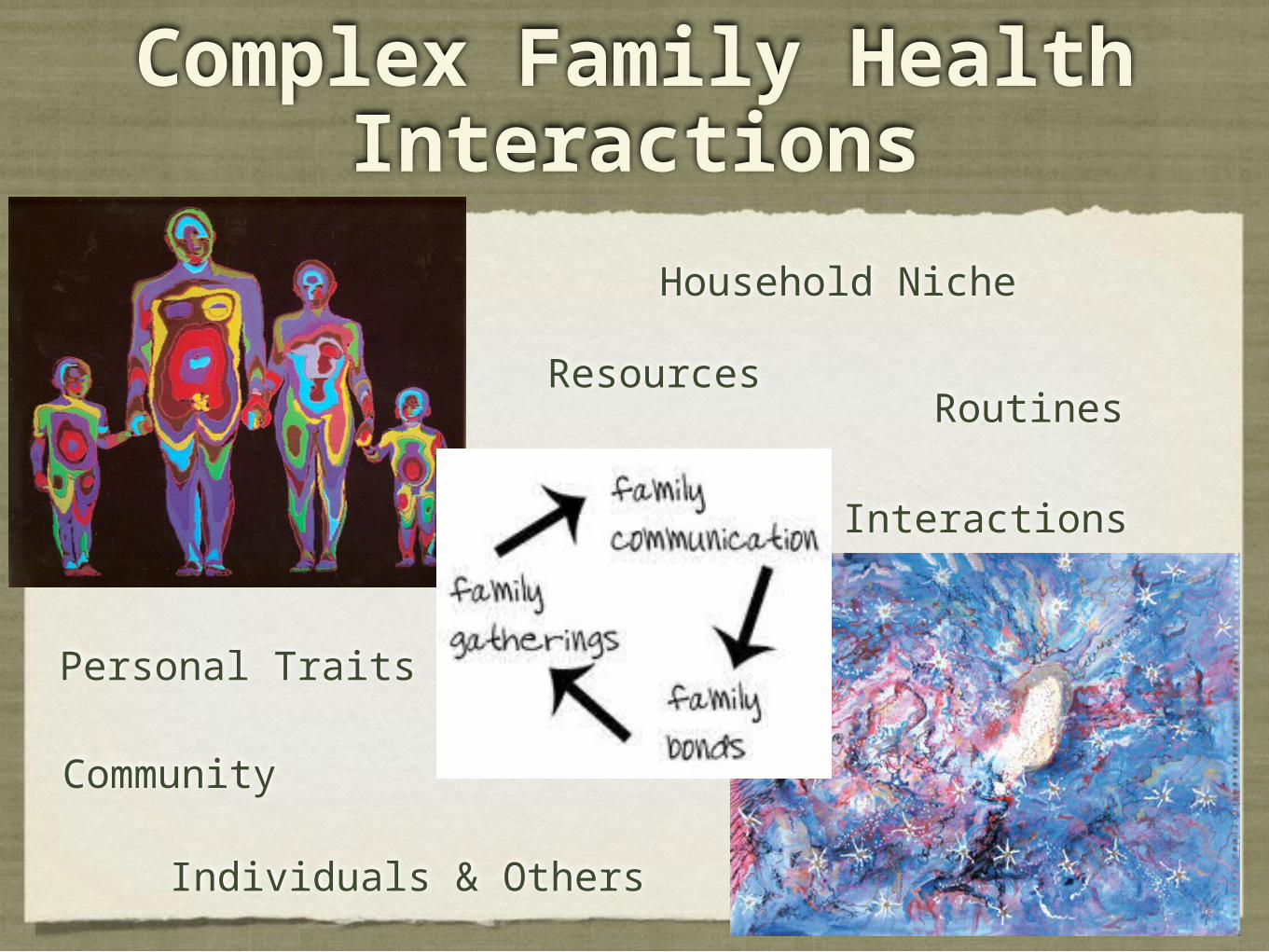
Complex Family Health Interactions
Household Niche
Individuals & Others
RoutinesResources
Personal Traits
Interactions
Community
Transform Nursing Practices
Household member behaviors
Meet individual Assess Family Needs
Tailor care One size does not fit all
No quick single fixes
Chronic care needs change over time
Family behaviors matter
Should not have to be on “our own”
Change Care Delivery
✦ Move beyond visiting hour debates
✦ Think outside of the acute care settings
✦ What is collaborate care? How do we become partners in care?
✦ What are the implications of continuously coordinated care?
✦ How do we best support the lived experience linked with health & illness?
✦ See family, the household, & community as integral... PLACE MATTERS!!!!
✦ Focus on population needs & quality of life years
✦ Medical errors, safety, infection control, costs of care, etc.
Moving from Patient to Family Focused Care
∗Patient focused (dependent role)∗Individual focused (empowered role)∗Patient-centered & family-centered terms
∗Family physicians & family nurse practitioners
Family Focused Care
∗Nursing is an art & science∗Evidence based practice∗See individuals - Always “think
family”∗ Identify care needs of people in
context∗Holistic care
Family as the Unit of Care
∗Family is in the forefront∗Members are perpetually connected∗Even when members are not present, they are still
important∗Shared lives, resources, & identities
“Thinking Family”
∗An attitude & mindset∗Approach for all care ∗Value deeply connected & interdependent
lives∗Respect expertise of family units’
experiences
Traits of Family Focused Care
Needed by young & old
Intentionally focused
Communication (crisis, conflict, multiple members)
Identify household needs for individual members
Reflection
Individual-Nurse-Family Partnerships
∗Family is ALWAYS present, even when not physically present
∗Hear the family story∗Value the expertise of family members∗Not an extra task, but usual practice in every
situation∗Safe care (think home & community)
Family Communication
∗Who do I communicate with?∗What things need to be discussed?∗How do I conduct private conversations?∗How do I best use time to build trust & deliver care?∗What are the most important things to do?
Continuity of Care
∗Care coordination∗Address care fragmentation∗Self & family care management∗Family needs to know ways to support members care needs∗Health promotion, wellness, risk reduction & prevention∗Resources, barriers & needs∗Family strengths∗ Interprofessional care needs
Family Focused Nursing Practices
∗Assessment: Gather, analyze & synthesize information from a variety of sources
∗Clear communication∗Provide information, education, & support∗Care for acute, chronic, population care needs & wellness
“Doing For” & “Being With”
∗“Doing For” – Task orientation (actions, busyness)∗“Being With” – Sharing emotional presence (listen, hear
story, value other, learn)∗Both important∗Do together
Family Focused Care
∗ Intentionally focused∗Use reflection regularly∗Communicate effectively∗Trust & respect∗Build self-confidence


















