Fall2012 final
40
Summary • Vaso-occlusion, which is the obstruction of blood flow in a vessel, leads to ischemia, chronic pain, and, if left untreated, tissue death (Yale et. al. 1349-1356) • Caregivers are routinely unable to correlate the magnitude of a vaso-occlusive event and pain in patients with sickle cell disease.
-
Upload
francoisdecuir -
Category
Documents
-
view
249 -
download
2
Transcript of Fall2012 final
Summary
• Vaso-occlusion, which is the obstruction of blood flow in a vessel, leads to ischemia, chronic pain, and, if left untreated, tissue death (Yale et. al. 1349-1356)
• Caregivers are routinely unable to correlate the magnitude of a vaso-occlusive event and pain in patients with sickle cell disease.
Summary
The subjective pain scale is the primary method of detection
• Patient ranks his/her pain on a scale of 1-10
• Contains no biometric data that relates severity of vaso-occlusion to pain
Summary
• Purpose: develop a modified pulse oximeter that will measure oxygen saturation or perfusion levels in tissue.
• Goal: determine a correlation between the oxygen levels and/or perfusion within the region of pain and the level of pain the patient is experiencing
• The device will, hopefully, lead to more efficient treatment
Sickle Cell Disease
• Malformation of hemoglobin
• Results in sickle-shaped red blood cells with altered function and lifespan
• Complications include painful vaso-occlusive episodes, ACS, stroke, pulmonary hypertension, multi-organ damage, decreased life-span (Conran 1-2)
• Affects 70,000-100,000 individuals in the US (SCDAA.com)
Vaso-Occlusion
• Most common complication of sickle cell disease
• Painful
• Can occur in arms, legs, chest, abdomen (American Family Physician 1027)
Vaso-Occlusion
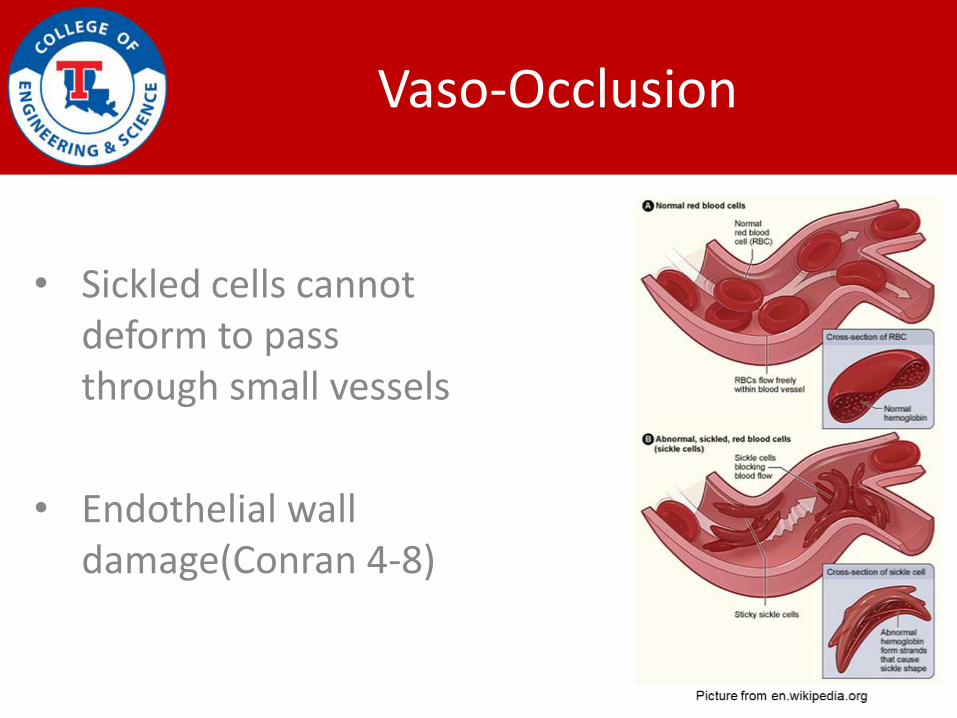
• Sickled cells cannot deform to pass through small vessels
• Endothelial wall damage(Conran 4-8)
Pain
• Caused by infection and/or ischemia
• Pain occurs in legs, arms, lower back, knees, chest, abdomen
• 5% of patients with sickle cell disease have 3-10 pain episodes per year
• Pain crises are the primary reason for ER visits

Pain Management
Drug Therapy
• Mild Pain : NSAIDs (acetaminophen, aspirin, ibuprofen, naproxen)
• Moderate-Severe Pain: Opioids
Pain Management
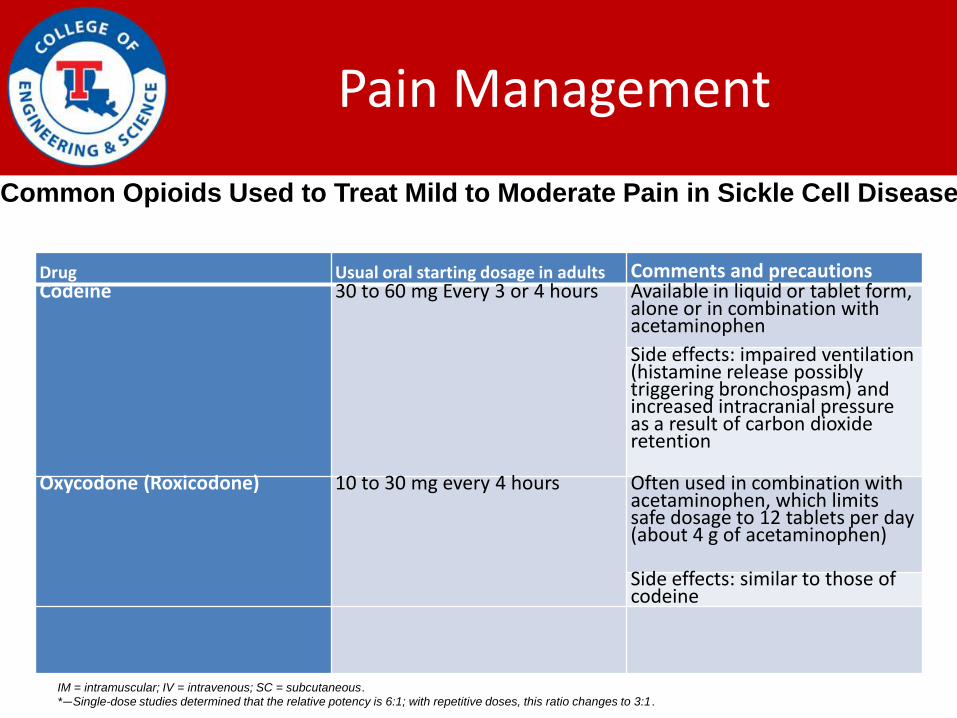
Drug Usual oral starting dosage in adults Comments and precautionsCodeine 30 to 60 mg Every 3 or 4 hours Available in liquid or tablet form,
alone or in combination with acetaminophen
Side effects: impaired ventilation (histamine release possibly triggering bronchospasm) and increased intracranial pressure as a result of carbon dioxide retention
Oxycodone (Roxicodone) 10 to 30 mg every 4 hours Often used in combination with acetaminophen, which limits safe dosage to 12 tablets per day (about 4 g of acetaminophen)
Side effects: similar to those of codeine
Common Opioids Used to Treat Mild to Moderate Pain in Sickle Cell Disease
IM = intramuscular; IV = intravenous; SC = subcutaneous.
*—Single-dose studies determined that the relative potency is 6:1; with repetitive doses, this ratio changes to 3:1.
Pain Management
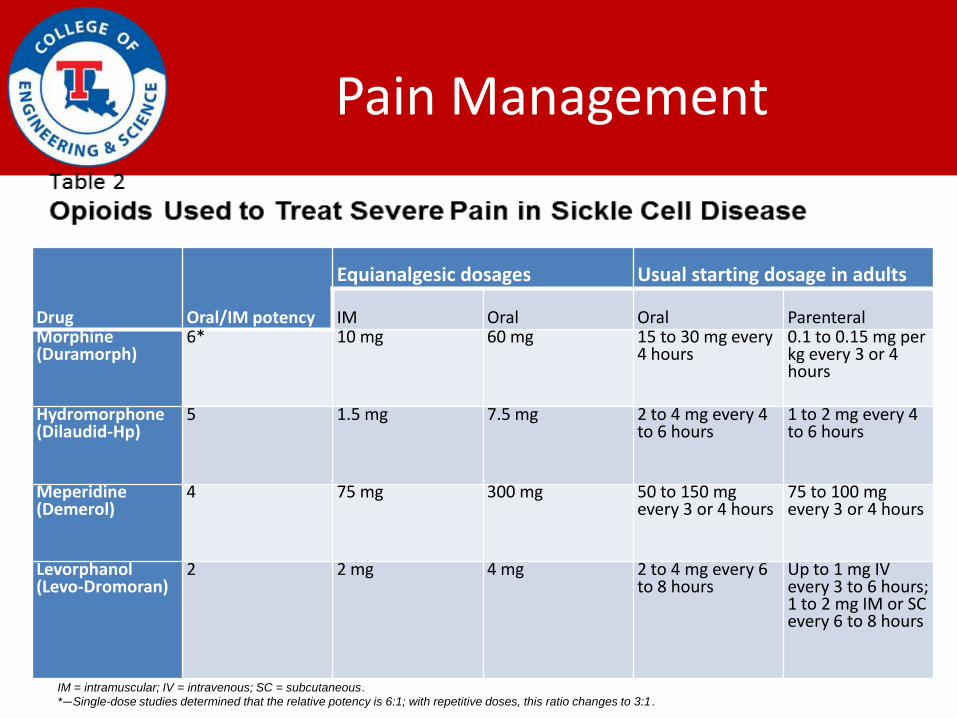
Drug Oral/IM potency
Equianalgesic dosages Usual starting dosage in adults
IM Oral Oral ParenteralMorphine (Duramorph)
6* 10 mg 60 mg 15 to 30 mg every 4 hours
0.1 to 0.15 mg per kg every 3 or 4 hours
Hydromorphone (Dilaudid-Hp)
5 1.5 mg 7.5 mg 2 to 4 mg every 4 to 6 hours
1 to 2 mg every 4 to 6 hours
Meperidine (Demerol)
4 75 mg 300 mg 50 to 150 mg every 3 or 4 hours
75 to 100 mg every 3 or 4 hours
Levorphanol (Levo-Dromoran)
2 2 mg 4 mg 2 to 4 mg every 6 to 8 hours
Up to 1 mg IV every 3 to 6 hours; 1 to 2 mg IM or SC every 6 to 8 hours
IM = intramuscular; IV = intravenous; SC = subcutaneous.
*—Single-dose studies determined that the relative potency is 6:1; with repetitive doses, this ratio changes to 3:1.
Reluctance of Pain Treatment
• Narcotic addiction & tolerance
• Excessive sedation
• Respiratory depression
• ‘Drug-seeking’ behavior
• Addiction in sickle cell patients = ~3% (Yale et. al)
Pain Validation
• Pain scale—subjective
• CT*
• Chest X-Ray*
*Not ordered regularly—very expensive
Need: A reliable, non-invasive, and inexpensive device to provide correlating data between the occurance and severity of vaso-occlusion and the pain that the patient is experiencing
Specifications
• Vaso-occlusion reduces the flow of oxygenated blood, which leads to a reduction of oxygen within the tissue.
• Reduced oxygenation leads to tissue damage and pain.
• The device proposed will adapt the principles of photoplethysmography to measure the oxygen saturation level at the site of pain.
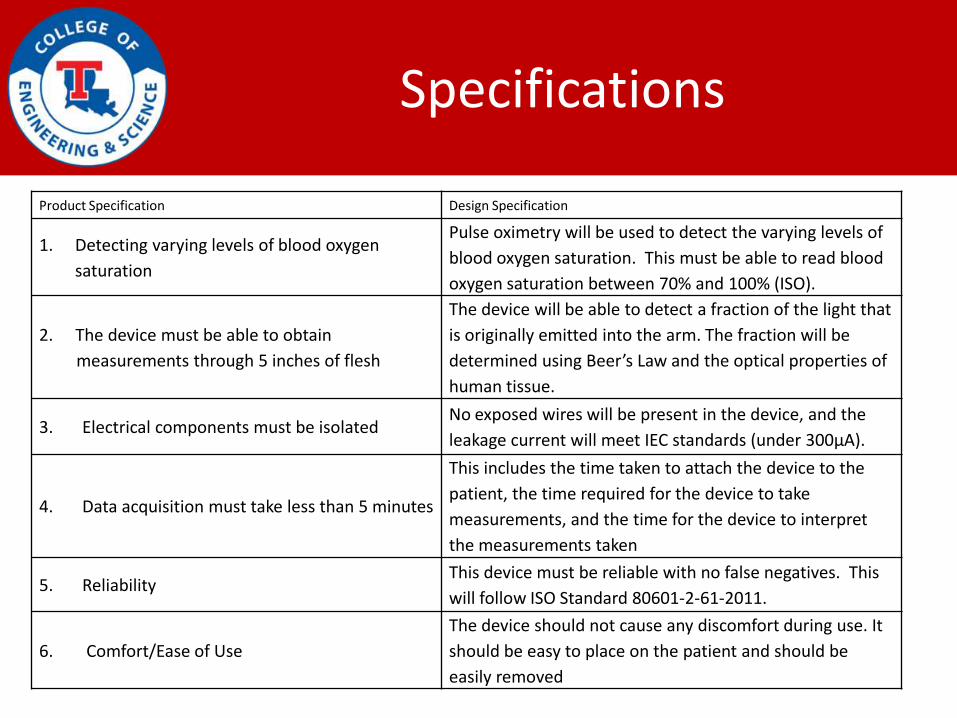
Specifications
Product Specification Design Specification
1. Detecting varying levels of blood oxygen
saturation
Pulse oximetry will be used to detect the varying levels of
blood oxygen saturation. This must be able to read blood
oxygen saturation between 70% and 100% (ISO).
2. The device must be able to obtain
measurements through 5 inches of flesh
The device will be able to detect a fraction of the light that
is originally emitted into the arm. The fraction will be
determined using Beer’s Law and the optical properties of
human tissue.
3. Electrical components must be isolatedNo exposed wires will be present in the device, and the
leakage current will meet IEC standards (under 300µA).
4. Data acquisition must take less than 5 minutes
This includes the time taken to attach the device to the
patient, the time required for the device to take
measurements, and the time for the device to interpret
the measurements taken
5. ReliabilityThis device must be reliable with no false negatives. This
will follow ISO Standard 80601-2-61-2011.
6. Comfort/Ease of Use
The device should not cause any discomfort during use. It
should be easy to place on the patient and should be
easily removed
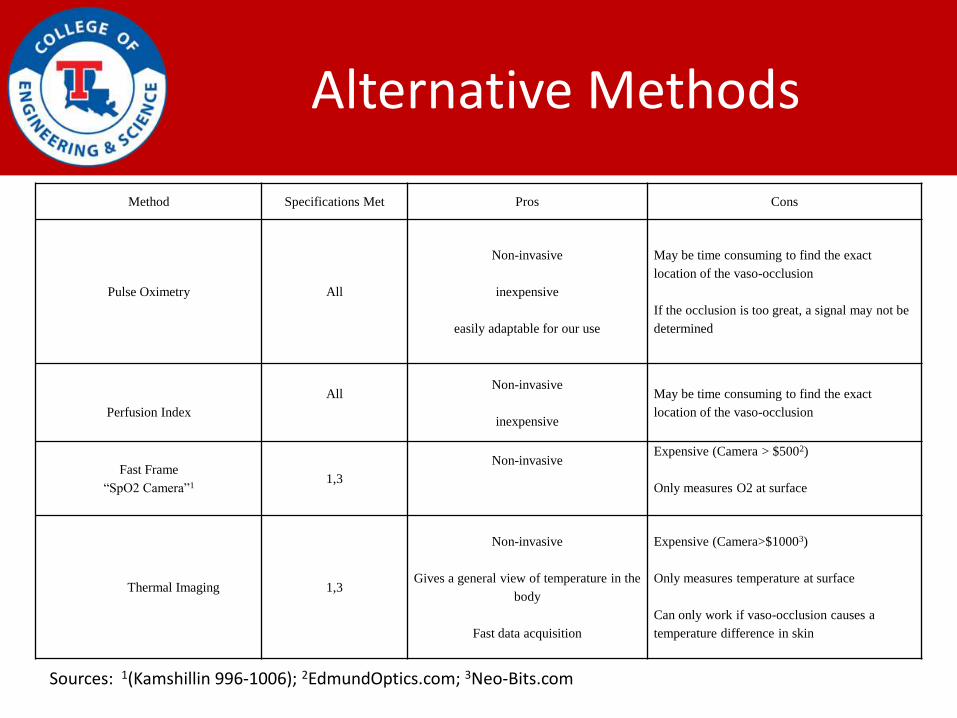
Alternative Methods
Method Specifications Met Pros Cons
Pulse Oximetry All
Non-invasive
inexpensive
easily adaptable for our use
May be time consuming to find the exact
location of the vaso-occlusion
If the occlusion is too great, a signal may not be
determined
Perfusion Index
AllNon-invasive
inexpensive
May be time consuming to find the exact
location of the vaso-occlusion
Fast Frame
“SpO2 Camera”11,3
Non-invasiveExpensive (Camera > $5002)
Only measures O2 at surface
Thermal Imaging 1,3
Non-invasive
Gives a general view of temperature in the
body
Fast data acquisition
Expensive (Camera>$10003)
Only measures temperature at surface
Can only work if vaso-occlusion causes a
temperature difference in skin
Sources: 1(Kamshillin 996-1006); 2EdmundOptics.com; 3Neo-Bits.com
Method Chosen
• Modified Pulse Oximeter
• Meets all specifications
• Low Cost
Further Research
Further research is needed in the following areas:
• Pathology of vaso-occlusion
• Location of vaso-occlusion
• Frequency of vaso-occlusion
• Size of affected area
• Time in which ischemia occurs
• Treatments for vaso-occlusion
(not pain treatment)
Specific Aims
1. Confirm that a Vaso-Occlusive Crisis Can be Detected
–Blood Oxygen Saturation
–Pulse Oximetry
–Photoplethysmography
Specific Aims
2. Develop a Device that Can Measure the Varying Oxygenation Levels
– The device will be developed using various programming software and hardware
–LabView
–LEDs
–Photodetector
Specific Aims
3. Design the Device so that it can be Attached to a Patient’s Arm of Varying Sizes
– This device should be able to adjust to varying thicknesses.
–Adjustable armband
Specific Aims
4. Find a Correlation Between Oxygen Saturation in the Blood and Pain
–A pain scale can be created that ranges from one to ten.
– Each number on the pain scale can correlate to a specific range of oxygen saturation levels.
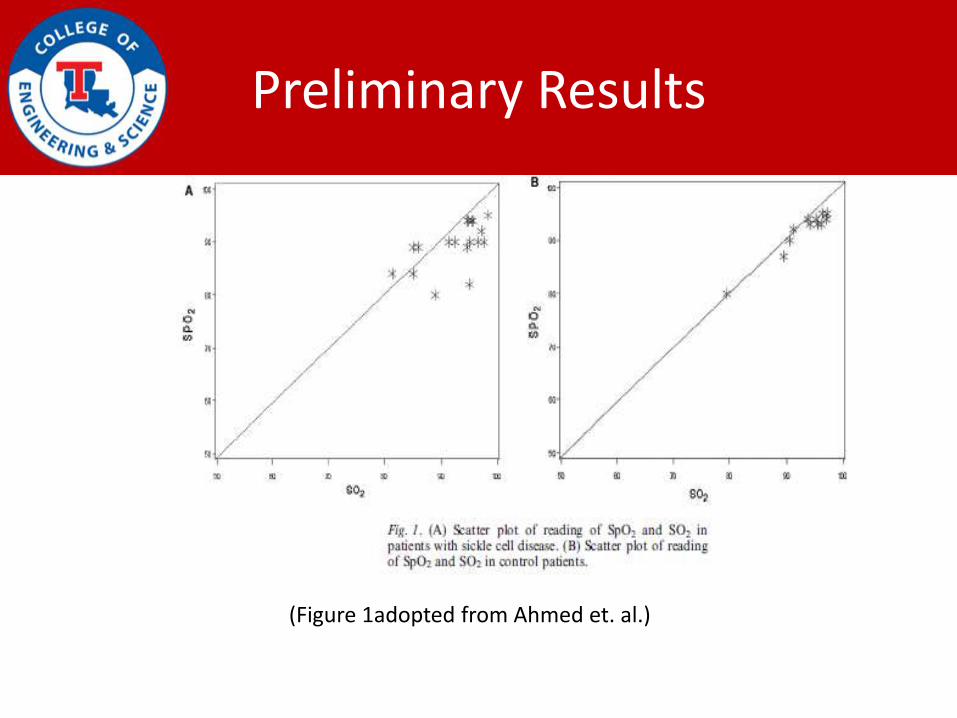
Preliminary Results
(Figure 1adopted from Ahmed et. al.)
Preliminary Data
• Methods of Data Collection
– Vaso-occlusive crisis was simulated
• A tourniquet was used to do this
– Different pulse oximeters were used
• Nano Tracker
• Medtronic Lifepak 12 Clinical Pulse Oximeter
• AD Instruments MLT321 Pulse Oximeters
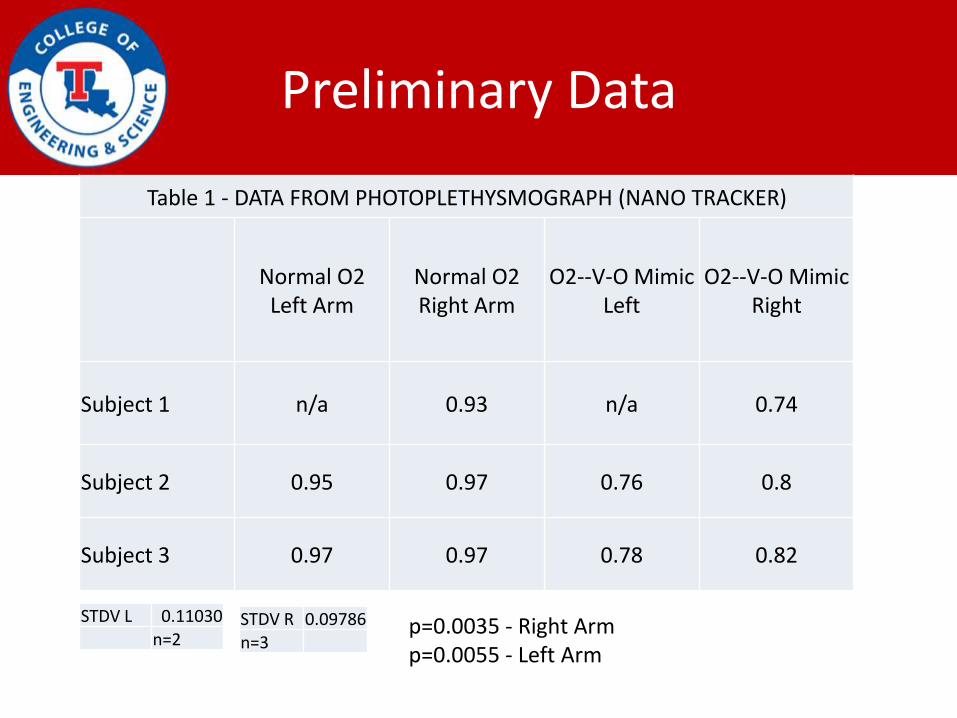
Preliminary Data
Table 1 - DATA FROM PHOTOPLETHYSMOGRAPH (NANO TRACKER)
Normal O2 Left Arm
Normal O2 Right Arm
O2--V-O Mimic Left
O2--V-O Mimic Right
Subject 1 n/a 0.93 n/a 0.74
Subject 2 0.95 0.97 0.76 0.8
Subject 3 0.97 0.97 0.78 0.82
STDV L 0.11030
n=2STDV R 0.09786n=3
p=0.0035 - Right Armp=0.0055 - Left Arm
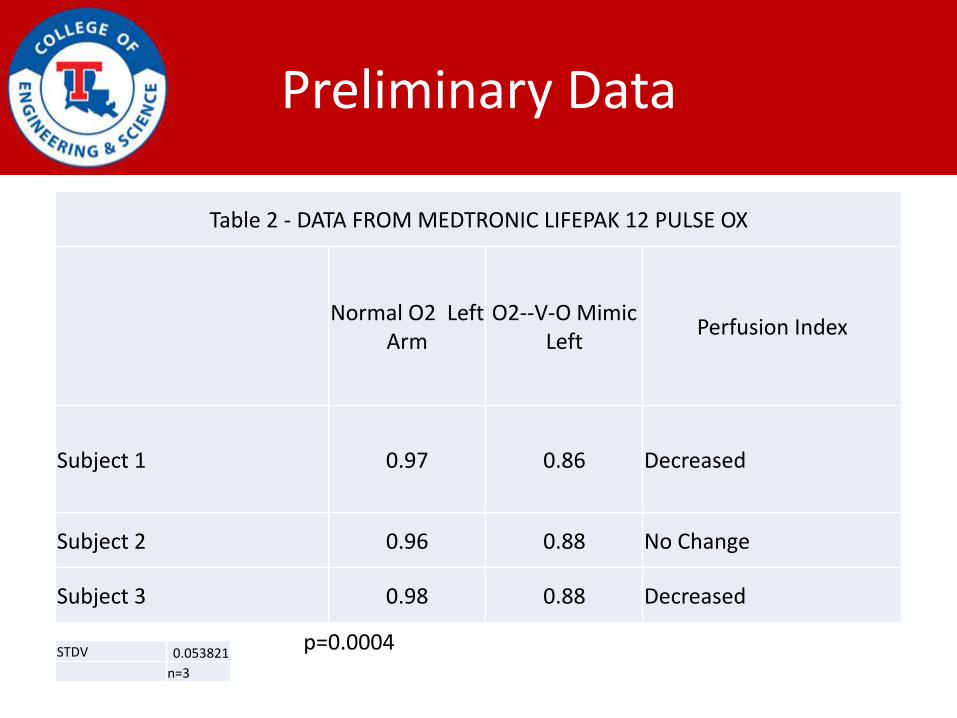
Preliminary Data
Table 2 - DATA FROM MEDTRONIC LIFEPAK 12 PULSE OX
Normal O2 Left Arm
O2--V-O Mimic Left
Perfusion Index
Subject 1 0.97 0.86 Decreased
Subject 2 0.96 0.88 No Change
Subject 3 0.98 0.88 Decreased
STDV 0.053821
n=3
p=0.0004
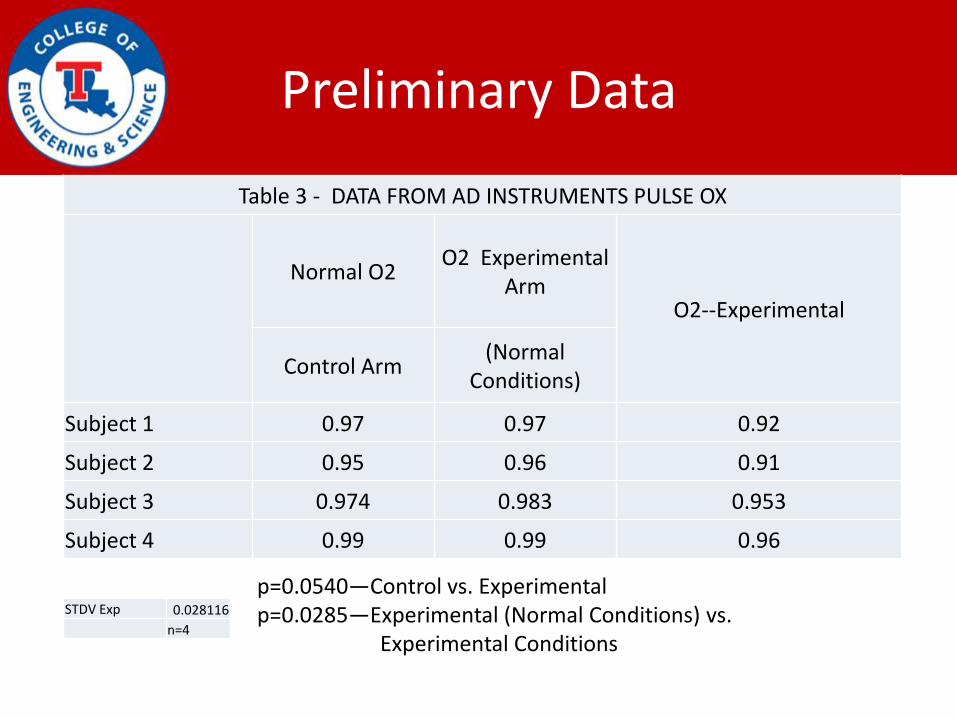
Preliminary Data
Table 3 - DATA FROM AD INSTRUMENTS PULSE OX
Normal O2 O2 Experimental
ArmO2--Experimental
Control Arm(Normal
Conditions)
Subject 1 0.97 0.97 0.92
Subject 2 0.95 0.96 0.91
Subject 3 0.974 0.983 0.953
Subject 4 0.99 0.99 0.96
STDV Exp 0.028116
n=4
p=0.0540—Control vs. Experimentalp=0.0285—Experimental (Normal Conditions) vs.
Experimental Conditions
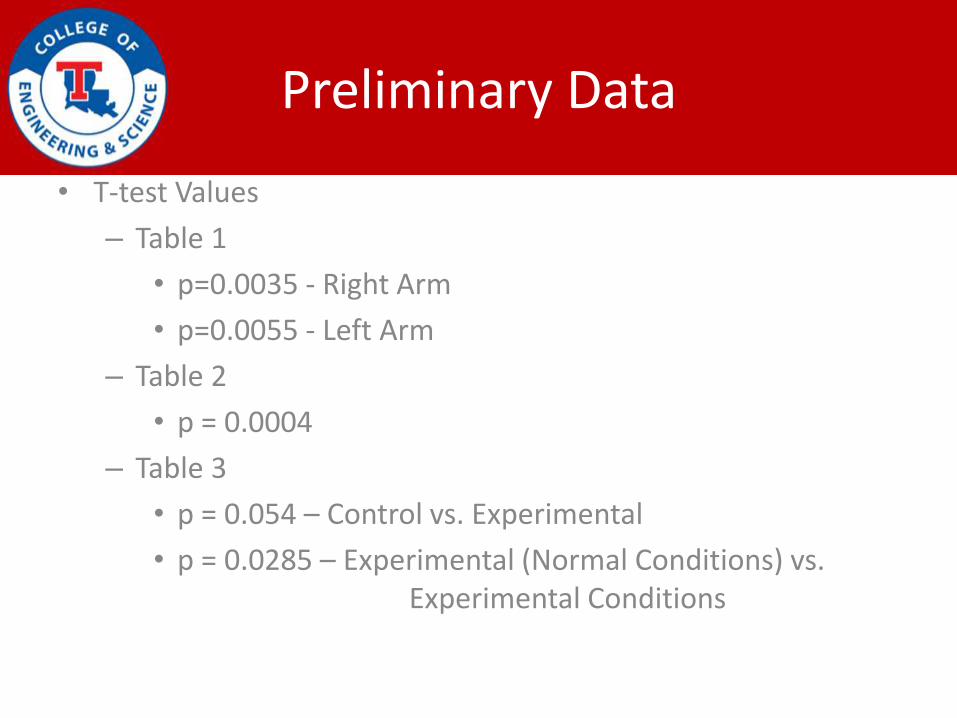
Preliminary Data
• T-test Values
– Table 1
• p=0.0035 - Right Arm
• p=0.0055 - Left Arm
– Table 2
• p = 0.0004
– Table 3
• p = 0.054 – Control vs. Experimental
• p = 0.0285 – Experimental (Normal Conditions) vs. Experimental Conditions
Purpose
• Detect Low oxygen concentration in extremities.
• Easy and cheap diagnostic technique for vaso-occlusion patient.
• Early diagnosis ease the treatment and prevent further damage.
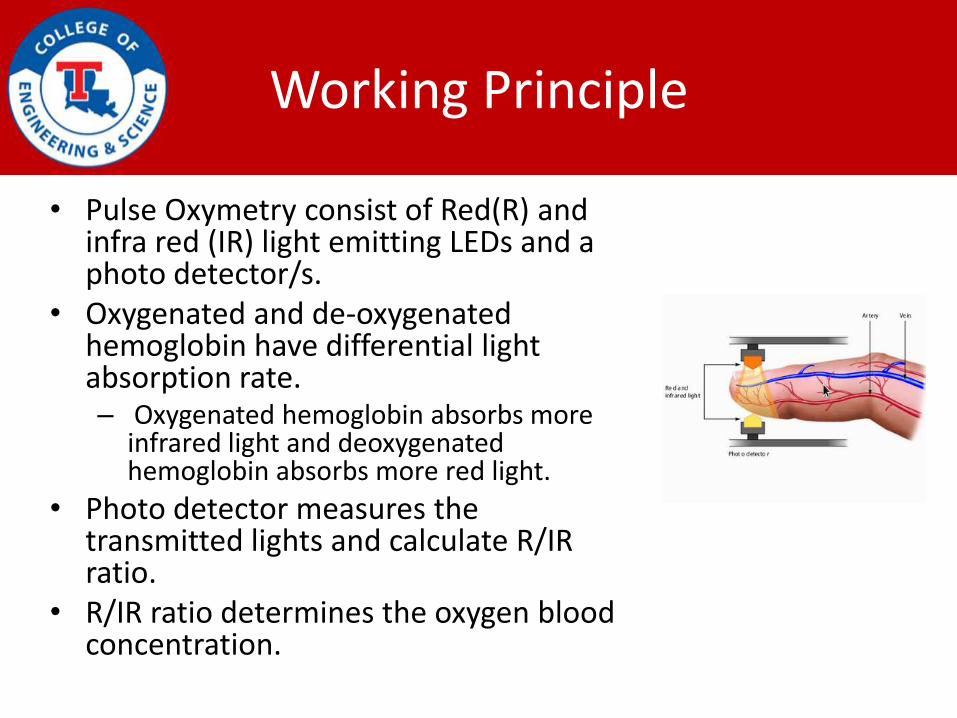
Working Principle
• Pulse Oxymetry consist of Red(R) and infra red (IR) light emitting LEDs and a photo detector/s.
• Oxygenated and de-oxygenated hemoglobin have differential light absorption rate.– Oxygenated hemoglobin absorbs more
infrared light and deoxygenated hemoglobin absorbs more red light.
• Photo detector measures the transmitted lights and calculate R/IR ratio.
• R/IR ratio determines the oxygen blood concentration.
Modification
• The pulse Oxymetry will be modified to fit in the extremities.
• High power LEDs will be used for larger parts.
• Two oximeters will be used for control and experimental data.
• Multi-array detector will be used if needed
Proposed Solution
• Single source multiple detector can be used.
• Uneven distribution on the detector can be analyzed mathematically.
• The output in the detector can be averaged out to find the occlusion.
• Non-linear transmission of the light can result the uniform result.
• Experiment can be conducted to test the linear behavior of the device.
Proposed Solution
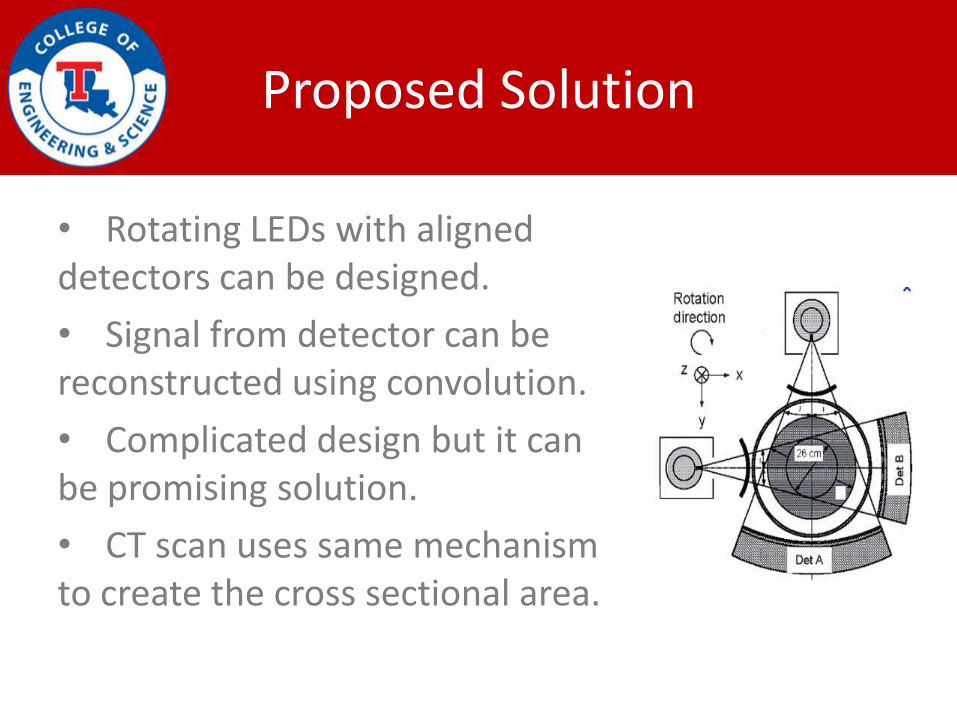
• Rotating LEDs with aligned detectors can be designed.
• Signal from detector can be reconstructed using convolution.
• Complicated design but it can be promising solution.
• CT scan uses same mechanism to create the cross sectional area.
Testing
• The device has to be calibrated for each individual.
• The device uses its data and compares with the control data.
• Device will correlate the severity of the vaso-occlusion measuring the blood oxygen concentration.
Design Specification
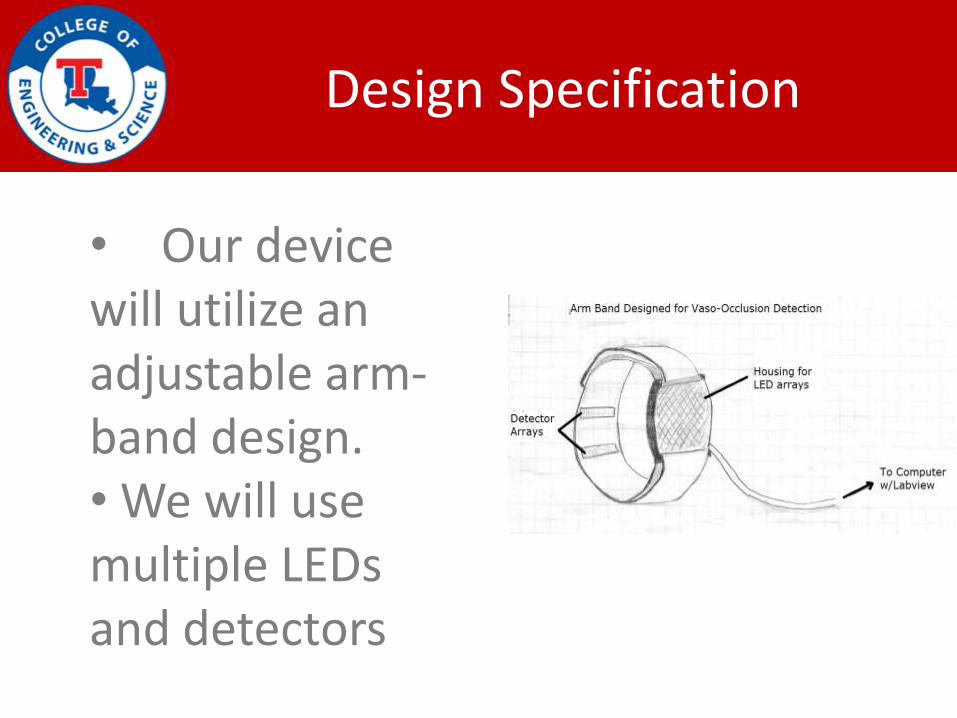
• Our device will utilize an adjustable arm-band design.• We will use multiple LEDs and detectors
Benefits of a Multiple LED system
• Produces more light which allows detector to see dark spots better
• Even if the crisis occurs outside of the emitance of the LED, our detectors can identify a crisis
Technique
• We will use two pulse oximeters• This can allow us to get a
baseline reading while simultaneously attempting to identify a crisis
• Preliminary testing has proven this method to be viable
Recreating a vaso-occlusion
• Vaso-occlusion causes less blood to reach tissue
• We were able to slow blood flow to the extremities using a sphygmomanometer
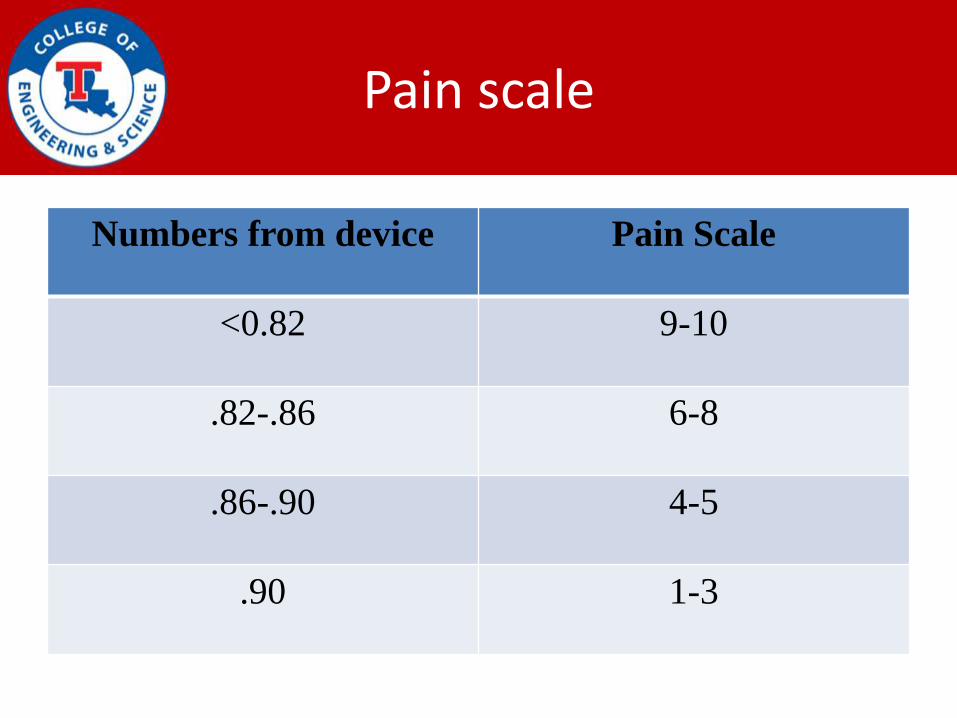
Pain scale
Numbers from device Pain Scale
<0.82 9-10
.82-.86 6-8
.86-.90 4-5
.90 1-3
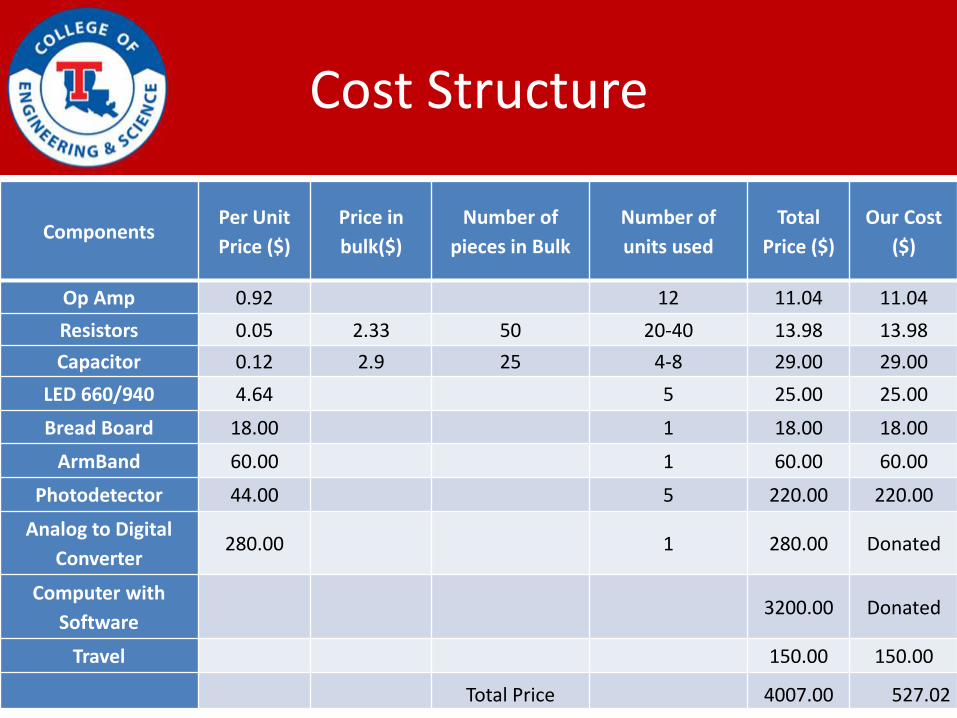
Cost Structure
ComponentsPer Unit
Price ($)
Price in
bulk($)
Number of
pieces in Bulk
Number of
units used
Total
Price ($)
Our Cost
($)
Op Amp 0.92 12 11.04 11.04
Resistors 0.05 2.33 50 20-40 13.98 13.98
Capacitor 0.12 2.9 25 4-8 29.00 29.00
LED 660/940 4.64 5 25.00 25.00
Bread Board 18.00 1 18.00 18.00
ArmBand 60.00 1 60.00 60.00
Photodetector 44.00 5 220.00 220.00
Analog to Digital
Converter280.00 1 280.00 Donated
Computer with
Software3200.00 Donated
Travel 150.00 150.00
Total Price 4007.00 527.02
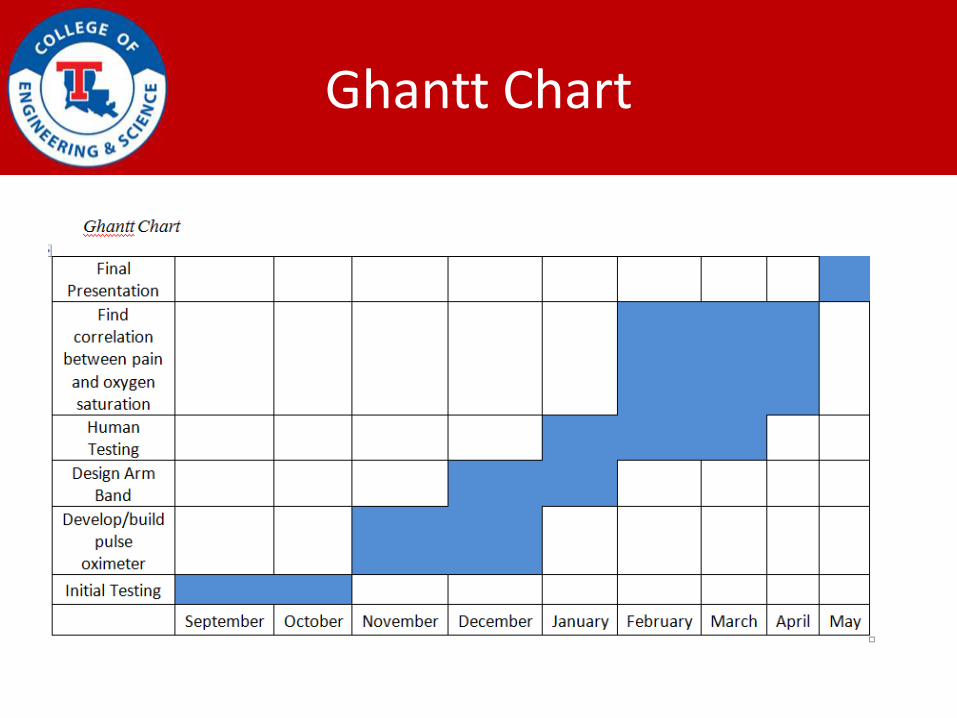
Ghantt Chart