Fall ISSUE PracticePerspectives - social workers · • Social Workers in Mental Health Clinics &...
6
PracticePerspectives Essential Health Benefits & the Affordable Care Act: What Social Workers Need to Know Fall ISSUE NOVEMBER 2012 Summary A component of the Patient Protection and Affordable Care Act (ACA) will have a direct impact on the health and well-being of over 70 million Americans. Beginning in January 2014, most individual and small group health plans operating in the U.S. will be required to provide “essential health benefits” (EHB), a package of health services defined broadly by the ACA, but customized by each state. Social workers should be aware of the EHB development process in their states, to ensure that their state EHB plan addresses the needs of people with chronic disease, disabilities, and other complex health issues, including individuals with mental health and substance use disorders, and that access to social work services is maintained and strengthened. What is the EHB Process and Why is it Important? The individual and small group insurance markets in the U.S. have traditionally offered the most expensive—and most inadequate— coverage of all commercial health plans. The ACA addresses this problem through the EHB process. The ACA outlines ten broad categories of essential health benefits (see chart) deemed essential for all Americans. The ACA delineated these benefit categories to assure consumers and small businesses that health insurance plans purchased beginning in 2014 will be comprehensive, providing key services at appropriate levels to address serious health conditions (Greenwood, et al, 2012). Certain benefit categories, such as rehabilitative and habilitative services and treatment for mental health and substance use disorders, are particularly important for individuals with disabilities or chronic conditions, many of whom will be newly insured through the state health exchanges and the Medicaid expansion. However, these benefits are often poorly covered or absent in traditional small group insurance plans. Stacy Collins, MSW Senior Practice Associate [email protected] The National Association of Social Workers 750 First Street NE Suite 700 Washington, DC 20002-4241 SocialWorkers.org ©2012 National Association of Social Workers. All Rights Reserved.
Transcript of Fall ISSUE PracticePerspectives - social workers · • Social Workers in Mental Health Clinics &...
PracticePerspectives
Essential Health Benefits & the Affordable Care Act:What Social Workers Need to Know
FallI S S U E
N O V E M B E R2 0 1 2
SummaryA component of the Patient Protectionand Affordable Care Act (ACA) willhave a direct impact on the health andwell-being of over 70 million Americans.Beginning in January 2014, mostindividual and small group health plansoperating in the U.S. will be required toprovide “essential health benefits” (EHB),a package of health services definedbroadly by the ACA, but customized byeach state. Social workers should beaware of the EHB development processin their states, to ensure that their stateEHB plan addresses the needs of peoplewith chronic disease, disabilities, andother complex health issues, includingindividuals with mental health andsubstance use disorders, and thataccess to social work services ismaintained and strengthened.
What is the EHB Process and Why is it Important?The individual and small group insurancemarkets in the U.S. have traditionally offeredthe most expensive—and most inadequate—coverage of all commercial health plans. TheACA addresses this problem through the EHBprocess. The ACA outlines ten broad categoriesof essential health benefits (see chart) deemedessential for all Americans. The ACA delineatedthese benefit categories to assure consumersand small businesses that health insuranceplans purchased beginning in 2014 will becomprehensive, providing key services atappropriate levels to address serious healthconditions (Greenwood, et al, 2012). Certainbenefit categories, such as rehabilitative andhabilitative services and treatment for mentalhealth and substance use disorders, areparticularly important for individuals withdisabilities or chronic conditions, many ofwhom will be newly insured through the statehealth exchanges and the Medicaidexpansion. However, these benefits are oftenpoorly covered or absent in traditional smallgroup insurance plans.
Stacy Collins, MSW
Senior Prac t i ce Assoc ia te
sco l l [email protected]
Occupational Profiles: Available athttp://workforce.socialworkers.org/studies/other.asp• Social Work Salaries by Gender• Social Work Salaries by Race/Ethnicity• Social Workers in Colleges and Universities• Social Workers in Government Agencies• Social Workers in Health Clinics & Outpatient Health
Care Settings• Social Workers in Hospice and Palliative Care• Social Workers in Hospitals and Medical Centers• Social Workers in Mental Health Clinics & Outpatient Facilities• Social Workers in Private Practice• Social Workers in Psychiatric Hospitals• Social Workers in Schools• Social Workers in Social Service Agencies
Social Work Practice Perspectives: Available atwww.socialworkers.org/practice/default.asp• 2011 Medicare Changes for Clinical Social Workers• Accountable Care Organizations (ACOs): Opportunities for
the Social Work Profession• Adolescent Depression and Suicide Risk: How Social
Workers Can Make a Difference• Advocating for Clinical Social Workers: Highlights of 2010• Creativity and Aging• Dangerous Rites of Passage: Trends in College Alcohol
Consumption• Domestic Violence and Human Trafficking: Double Jeopardy
for Immigrant Women in the United States• Domestic Violence and Women of Color: Complex Dynamics• Engaging Young People in Their Transition Planning• Healthy People 2020: Social Work Values in a Public
Health Roadmap
• Opting Out of Medicare as a Clinical Social Worker• Results of 2010 Psychotherapy Survey• Support for Family Caregivers: The National Landscape
and the Social Work Role• Supporting the Child Welfare Workforce to Reduce
Child Maltreatment• The Medical Home Model: What Is It and How Do
Social Workers Fit In?
Leadership Ladders: Steps to a Great Career in Social WorkAvailable at http://careers.socialworkers.org/professionaldev/default.asp• From the Front Line to the Corner Office• Letting Your Voice be Heard• Managing Stress• Navigating Large Service Systems• Opening a New Private Practice• Outside the Lines: Maximizing the Flexibility of a
Social Work Degree• Presenting Your Work to Others• Publishing as a Practitioner• Risk Management in Clinical Practice• Strengthening Your Writing Skills: An Essential Task for
Every Social Worker• The Tech-Savvy Social Worker: Prepared for the
Challenges of 21st Century Practice• The Value of Dual Degrees
New Practice StandardsFor a complete list of practice standards, visitwww.socialworkers.org/practice/default.asp• NASW Standards for Social Work Practice with Family
Caregivers of Older Adults (2010)
750 First Street NE, Suite 700Washington, DC 20002-4241SocialWorkers.org
The NationalAssociation ofSocial Workers
750 First Street NE
Suite 700
Washington, DC 20002-4241
SocialWorkers.org
©2012 National Association ofSocial Workers. All Rights Reserved.
Practice Perspectives Fall November 2012
Center for Workforce Studies & Social Work Practice Recent Publications
Federal regulation requires each state to select itsown EHB plan, known as a benchmark plan,which must be inclusive of all ten benefit categories.Ultimately, over 70 million people, both currentlyinsured and newly insured through the ACA, willhave health benefits defined by the EHB.
How does the state EHB process work?First, each state must select a benchmark planfrom one of the following four insurance groups:
• Any of the largest three plans (by enrollment)in the state’s small group insurance market
• Any of the largest three state employeehealth benefit plans (by enrollment)
• Any of the largest three national federalemployee health plans (by enrollment)
• The largest commercial non-Medicaid HealthMaintenance Organization (HMO)operating in the state.
Then states must review the plan for adherence tothe ten mandated benefit categories. If abenchmark plan does not include all ten benefitcategories, the state must provide supplementalcoverage to fulfill the requirement. A state’sbenchmark plan serves as the basis for all healthinsurance plans offered by the following entities:
• State health exchanges (the new on-lineinsurance marketplaces, also authorized bythe ACA, in which individuals and smallbusinesses can shop for coverage)
• All small group and individual plans operatingoutside of the state health exchange
• All plans offered to newly eligiblebeneficiaries in the Medicaid expansionpopulation.1
Self-insured and large group health plans are notrequired to comply with the state’s benchmarkplan. All benchmark plans must ultimately beapproved and certified by the Department ofHealth and Human Services (HHS).
According to the ACA, each state was requiredto communicate its selected benchmark plan toHHS by September 30, 2012. As of that date,21 states and the District of Columbia hadchosen a plan. HHS has indicated it will acceptstate benchmark plan submissions beyond theSeptember 30, 2012 deadline. If a state doesnot select a benchmark plan, the largest plan inthe small group market will be the state’sbenchmark plan by default. Before final approvaland certification of the state benchmark plans,HHS will offer an opportunity for public commenton all the proposed state plans.
What is needed to ensure appropriatecoverage in the benchmark plans?Proposed state benchmark plans should bereviewed carefully to ensure comprehensivecoverage for all enrollees, especially those withdisabilities or chronic conditions, andappropriate adherence to the mandated benefitcategories. NASW and other advocates havedeveloped the following recommendations forstate benchmark plans:
MENTAL HEALTH AND SUBSTANCE USEDISORDER TREATMENTRobust mental health and substance use disordertreatment is critical to prevent the development ofco-occurring chronic diseases and costly inpatienthospitalizations. Plans should offer access to thefull range of effective services, includingprevention, treatment, rehabilitation, and recoveryservices. With regard to treatment, specialattention should be given to medication assistedtherapies, residential services, and chronicdisease management programs. Plans shoulddemonstrate strong network adequacy, includingaccess to clinical social work services.
AMBULATORY PATIENT SERVICES Regular access to health care providers with theappropriate experience and expertise is a keycomponent of care for people living with chronicillness. Plans should offer people living withchronic conditions access to disease-appropriatespecialty services without visit limits.
PREVENTIVE AND WELLNESS SERVICESAlthough the ACA requires health plans toinclude all preventive services with an A or Brating from the United States Preventive ServicesTask Force, plan details should be read carefully,to ensure inclusion of important services such aswell-woman visits, domestic violence screening,and contraception. In addition, case managementand care coordination should be a requiredchronic disease management service forbenchmark plans.
REHABILITATIVE AND HABILITATIVE SERVICESAND DEVICESEssential rehabilitation and habilitation careshould include services and devices that improve,
maintain, and lessen the deterioration of apatient’s functional status over a lifetime and on atreatment continuum (Coalition to PreserveRehabilitation, 2012). Because many insuranceplans do not currently provide habilitativeservices and devices, special attention should begiven to ensure that any supplemental coveragefor this benefit category meets the care andtreatment needs of people living with chronicconditions and disabilities. Medicaid provides agood guide for determining specific benefits forinclusion in this category. In addition, because ofthe conditions that require this category ofservices, it is critical that medical necessitydeterminations for rehabilitative and habilitativeservices and devices are based on clinicaljudgment and not arbitrary limits or caps.
PRESCRIPTION DRUGSPeople living with chronic conditions oftenrequire access to a range of prescriptionmedications to effectively manage theirconditions and stay healthy. The HHS proposalto require plans sold through state exchanges tocover at least one drug per class will not ensureaccess to essential medications and is at oddswith the non-discrimination and access provisionsof the ACA. Other federal requirementsregarding prescription drug access—for instance,the Medicare Part D policy requiring plans tocover all of the medications in six protectedclasses—offer a better approach to ensureaccess to these vital benefits. At the very least,the prescription drug coverage of the benchmarkplan chosen in the state (which is often morerobust than the one drug per class floorarticulated in the HHS guidance) should be thefloor for prescription drug coverage.
STATE-MANDATED BENEFITSPrior to passage of the ACA, many statesalready had mandated coverage for selectedbenefits. Such state-level mandates vary widelyacross the nation. The ACA does not directlypreempt existing mandates, but does requirestates to pay the costs of state-mandated benefitsthat are not included in the ten essential benefitcategories. For example, autism treatment, whichis mandated in 30 states, might be assumed tobe included in habilitative or behavioral health
Proposed state
benchmark plans
should be reviewed
carefully to ensure
comprehensive
coverage for all
enrollees, especially
those with disabilities
or chronic
conditions, and
appropriate
adherence to the
mandated benefit
categories.
Before final
approval and
certification of the
state benchmark
plans, HHS will
offer an opportunity
for public comment
on all the proposed
state plans.
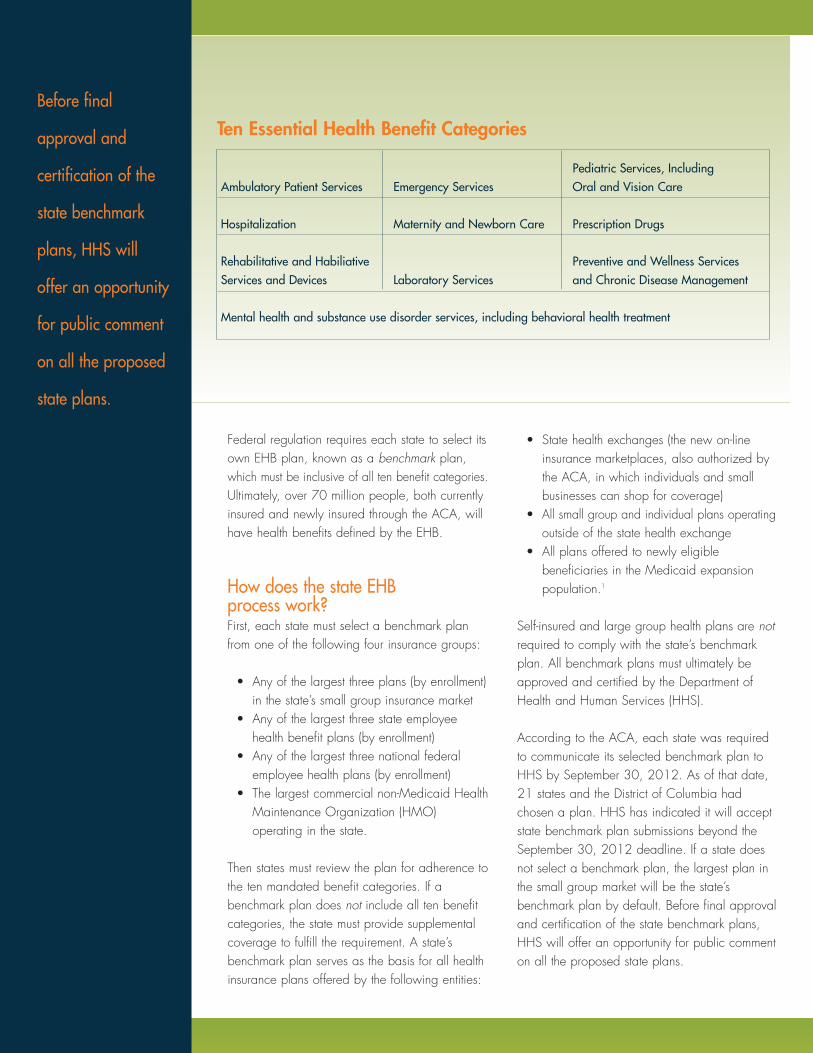
Ten Essential Health Benefit Categories
Pediatric Services, Including Ambulatory Patient Services Emergency Services Oral and Vision Care
Hospitalization Maternity and Newborn Care Prescription Drugs
Rehabilitative and Habiliative Preventive and Wellness ServicesServices and Devices Laboratory Services and Chronic Disease Management
Mental health and substance use disorder services, including behavioral health treatment

Federal regulation requires each state to select itsown EHB plan, known as a benchmark plan,which must be inclusive of all ten benefit categories.Ultimately, over 70 million people, both currentlyinsured and newly insured through the ACA, willhave health benefits defined by the EHB.
How does the state EHB process work?First, each state must select a benchmark planfrom one of the following four insurance groups:
• Any of the largest three plans (by enrollment)in the state’s small group insurance market
• Any of the largest three state employeehealth benefit plans (by enrollment)
• Any of the largest three national federalemployee health plans (by enrollment)
• The largest commercial non-Medicaid HealthMaintenance Organization (HMO)operating in the state.
Then states must review the plan for adherence tothe ten mandated benefit categories. If abenchmark plan does not include all ten benefitcategories, the state must provide supplementalcoverage to fulfill the requirement. A state’sbenchmark plan serves as the basis for all healthinsurance plans offered by the following entities:
• State health exchanges (the new on-lineinsurance marketplaces, also authorized bythe ACA, in which individuals and smallbusinesses can shop for coverage)
• All small group and individual plans operatingoutside of the state health exchange
• All plans offered to newly eligiblebeneficiaries in the Medicaid expansionpopulation.1
Self-insured and large group health plans are notrequired to comply with the state’s benchmarkplan. All benchmark plans must ultimately beapproved and certified by the Department ofHealth and Human Services (HHS).
According to the ACA, each state was requiredto communicate its selected benchmark plan toHHS by September 30, 2012. As of that date,21 states and the District of Columbia hadchosen a plan. HHS has indicated it will acceptstate benchmark plan submissions beyond theSeptember 30, 2012 deadline. If a state doesnot select a benchmark plan, the largest plan inthe small group market will be the state’sbenchmark plan by default. Before final approvaland certification of the state benchmark plans,HHS will offer an opportunity for public commenton all the proposed state plans.
What is needed to ensure appropriatecoverage in the benchmark plans?Proposed state benchmark plans should bereviewed carefully to ensure comprehensivecoverage for all enrollees, especially those withdisabilities or chronic conditions, andappropriate adherence to the mandated benefitcategories. NASW and other advocates havedeveloped the following recommendations forstate benchmark plans:
MENTAL HEALTH AND SUBSTANCE USEDISORDER TREATMENTRobust mental health and substance use disordertreatment is critical to prevent the development ofco-occurring chronic diseases and costly inpatienthospitalizations. Plans should offer access to thefull range of effective services, includingprevention, treatment, rehabilitation, and recoveryservices. With regard to treatment, specialattention should be given to medication assistedtherapies, residential services, and chronicdisease management programs. Plans shoulddemonstrate strong network adequacy, includingaccess to clinical social work services.
AMBULATORY PATIENT SERVICES Regular access to health care providers with theappropriate experience and expertise is a keycomponent of care for people living with chronicillness. Plans should offer people living withchronic conditions access to disease-appropriatespecialty services without visit limits.
PREVENTIVE AND WELLNESS SERVICESAlthough the ACA requires health plans toinclude all preventive services with an A or Brating from the United States Preventive ServicesTask Force, plan details should be read carefully,to ensure inclusion of important services such aswell-woman visits, domestic violence screening,and contraception. In addition, case managementand care coordination should be a requiredchronic disease management service forbenchmark plans.
REHABILITATIVE AND HABILITATIVE SERVICESAND DEVICESEssential rehabilitation and habilitation careshould include services and devices that improve,
maintain, and lessen the deterioration of apatient’s functional status over a lifetime and on atreatment continuum (Coalition to PreserveRehabilitation, 2012). Because many insuranceplans do not currently provide habilitativeservices and devices, special attention should begiven to ensure that any supplemental coveragefor this benefit category meets the care andtreatment needs of people living with chronicconditions and disabilities. Medicaid provides agood guide for determining specific benefits forinclusion in this category. In addition, because ofthe conditions that require this category ofservices, it is critical that medical necessitydeterminations for rehabilitative and habilitativeservices and devices are based on clinicaljudgment and not arbitrary limits or caps.
PRESCRIPTION DRUGSPeople living with chronic conditions oftenrequire access to a range of prescriptionmedications to effectively manage theirconditions and stay healthy. The HHS proposalto require plans sold through state exchanges tocover at least one drug per class will not ensureaccess to essential medications and is at oddswith the non-discrimination and access provisionsof the ACA. Other federal requirementsregarding prescription drug access—for instance,the Medicare Part D policy requiring plans tocover all of the medications in six protectedclasses—offer a better approach to ensureaccess to these vital benefits. At the very least,the prescription drug coverage of the benchmarkplan chosen in the state (which is often morerobust than the one drug per class floorarticulated in the HHS guidance) should be thefloor for prescription drug coverage.
STATE-MANDATED BENEFITSPrior to passage of the ACA, many statesalready had mandated coverage for selectedbenefits. Such state-level mandates vary widelyacross the nation. The ACA does not directlypreempt existing mandates, but does requirestates to pay the costs of state-mandated benefitsthat are not included in the ten essential benefitcategories. For example, autism treatment, whichis mandated in 30 states, might be assumed tobe included in habilitative or behavioral health
Proposed state
benchmark plans
should be reviewed
carefully to ensure
comprehensive
coverage for all
enrollees, especially
those with disabilities
or chronic
conditions, and
appropriate
adherence to the
mandated benefit
categories.
Before final
approval and
certification of the
state benchmark
plans, HHS will
offer an opportunity
for public comment
on all the proposed
state plans.
Ten Essential Health Benefit Categories
Pediatric Services, Including Ambulatory Patient Services Emergency Services Oral and Vision Care
Hospitalization Maternity and Newborn Care Prescription Drugs
Rehabilitative and Habiliative Preventive and Wellness ServicesServices and Devices Laboratory Services and Chronic Disease Management
Mental health and substance use disorder services, including behavioral health treatment
Ultimately, strong
federal oversight
will be needed to
ensure that people
with chronic illnesses
or disabilities who
enroll in the
exchanges are
protected from
discrimination and
gain meaningful
access to care
and support.
treatment. However, given the difficulty that manyfamilies face in securing appropriate services forchildren with autism, advocates are requestingexplicit coverage language in the benchmarkplans (Autism Speaks, 2012). As such, somestates, including California and New York, haveincorporated autism coverage into their statebenchmark plans. Compliance with statemandated coverage should be given specialattention in the benchmark plan selection process.
Benchmark Plans and ParityThe ACA includes strong non-discriminationlanguage to ensure that plans sold through theexchanges do not discriminate against peoplewith chronic and complex conditions. The lawfurther mandates that benefit coverage isappropriately balanced among the categories of covered benefits. Additionally, all EHB plansshould include coverage for mental health andsubstance use disorders at parity withmedical/surgical benefits. Nevertheless,benchmark plans need to be reviewed closely for adherence to parity and non-discriminationrules. Ultimately, strong federal oversight will be needed to ensure that people with chronicillnesses or disabilities who enroll in theexchanges are protected from discrimination andgain meaningful access to care and support.
Opportunities for Social WorkInvolvement in the EHB Selection ProcessOFFER YOUR KNOWLEDGE OF YOURSTATE’S POTENTIAL BENCHMARK PLANSContact local health reform advocates and find out if your state is engaged in a benchmarkplan selection process. If so, review the plansunder consideration (some state benchmarkinformation is posted on this website:www.statereforum.org/state-progress-on-essential-health-benefits). Offer your perceptions of andexperiences with the potential benchmark plans.
COMMENT ON YOUR STATE’S SELECTEDBENCHMARK PLANIt is vitally important for social workers and otheradvocates to review state benchmark plans
carefully and provide feedback to HHS. Concernhas already been expressed about shortcomingin benchmark plans submitted to HHS and thehigh degree of variability among state plans(Kliff, 2012). For example, the state of Utah haschosen a benchmark plan that offers nocoverage for inpatient or outpatient substanceuse treatment or autism therapy, and a maximumof eight visits per plan year for mental andbehavioral health outpatient services (NASHP,2012). By contrast, New York’s proposed EHBplan covers these services, and offers 30 visitsper plan year for mental and behavioral healthoutpatient services (NASHP, 2012).
It is projected that by December 2012, HHS willannounce the 51 selected benchmark plans andrequest public comment on them. As HHS ischarged with certifying each benchmark plan, thepublic comment process will give stakeholders,including social workers, an opportunity toreview the plans and provide comment to HHS,using the criteria specified above. NASW willfurther update members when the HHSannouncement is made.
ConclusionThe EHB process is a critical component of theAffordable Care Act. By establishing EHB plansthat offer adequate and appropriate benefits,states have an opportunity to greatly enhancehealth insurance coverage for millions ofAmericans who are uninsured or underinsured,particularly people with disabilities and othervulnerable populations.
ReferencesAutism Speaks. (2012, October 2). New York
Includes Autism Benefits in Health Care ReformPlan. Retrieved from www.autismspeaks.org/advocacy/advocacy-news/new-york-includes-autism-benefits-health-reform-plan
Coalition to Preserve Rehabilitation. (2012,October). Open letter to states on definingessential health benefits package. Retrieved fromwww.aahd.us/wp-content/uploads/2012/09/EHBRehabHabCCDHABCTechAssistSept-2012.pdf
Greenwood, K., Ragone, T.A., Jacobi, J.V. (2012,August). Implementing the Essential Health BenefitsRequirement in New Jersey: Decision Points andPolicy Issues. Newark, NJ: Rutgers Center forState Health Policy/Seton Hall Law.
Kliff, S. (2012, September 22). Is acupunctureessential health care? Weight loss surgery? UnderObamacare, states choose. Washington Post.Retrieved from www.washingtonpost.com/blogs/ezra-klein/wp/2012/09/22/is-acupuncture-essential-health-care-weight-loss-surgery-under-obamacare-states-must-choose/
National Academy for State Health Policy. (2012).State Progress on Essential Health Benefits.Retrieved from www.statereforum.org/state-progress-on-essential-health-benefits
ResourcesState Refor(u)m – A project of the NationalAcademy for State Health Policy, offers state-levelinformation on health reform implementation.www.statereforum.org
The Center for Health Insurance Reform – A project of Georgetown University Health Policy Institute. chir.georgetown.edu
1 The Supreme Court ruling in June 2012 rendered theMedicaid expansion optional for states. States that chooseto expand their Medicaid program must raise the eligibilitylevel to 133% of the federal poverty line.
By establishing EHB
plans that offer
adequate and
appropriate benefits,
states have an
opportunity to greatly
enhance health
insurance coverage
for millions of
Americans who
are uninsured or
underinsured,
particularly people
with disabilities and
other vulnerable
populations.

Ultimately, strong
federal oversight
will be needed to
ensure that people
with chronic illnesses
or disabilities who
enroll in the
exchanges are
protected from
discrimination and
gain meaningful
access to care
and support.
treatment. However, given the difficulty that manyfamilies face in securing appropriate services forchildren with autism, advocates are requestingexplicit coverage language in the benchmarkplans (Autism Speaks, 2012). As such, somestates, including California and New York, haveincorporated autism coverage into their statebenchmark plans. Compliance with statemandated coverage should be given specialattention in the benchmark plan selection process.
Benchmark Plans and ParityThe ACA includes strong non-discriminationlanguage to ensure that plans sold through theexchanges do not discriminate against peoplewith chronic and complex conditions. The lawfurther mandates that benefit coverage isappropriately balanced among the categories of covered benefits. Additionally, all EHB plansshould include coverage for mental health andsubstance use disorders at parity withmedical/surgical benefits. Nevertheless,benchmark plans need to be reviewed closely for adherence to parity and non-discriminationrules. Ultimately, strong federal oversight will be needed to ensure that people with chronicillnesses or disabilities who enroll in theexchanges are protected from discrimination andgain meaningful access to care and support.
Opportunities for Social WorkInvolvement in the EHB Selection ProcessOFFER YOUR KNOWLEDGE OF YOURSTATE’S POTENTIAL BENCHMARK PLANSContact local health reform advocates and find out if your state is engaged in a benchmarkplan selection process. If so, review the plansunder consideration (some state benchmarkinformation is posted on this website:www.statereforum.org/state-progress-on-essential-health-benefits). Offer your perceptions of andexperiences with the potential benchmark plans.
COMMENT ON YOUR STATE’S SELECTEDBENCHMARK PLANIt is vitally important for social workers and otheradvocates to review state benchmark plans
carefully and provide feedback to HHS. Concernhas already been expressed about shortcomingin benchmark plans submitted to HHS and thehigh degree of variability among state plans(Kliff, 2012). For example, the state of Utah haschosen a benchmark plan that offers nocoverage for inpatient or outpatient substanceuse treatment or autism therapy, and a maximumof eight visits per plan year for mental andbehavioral health outpatient services (NASHP,2012). By contrast, New York’s proposed EHBplan covers these services, and offers 30 visitsper plan year for mental and behavioral healthoutpatient services (NASHP, 2012).
It is projected that by December 2012, HHS willannounce the 51 selected benchmark plans andrequest public comment on them. As HHS ischarged with certifying each benchmark plan, thepublic comment process will give stakeholders,including social workers, an opportunity toreview the plans and provide comment to HHS,using the criteria specified above. NASW willfurther update members when the HHSannouncement is made.
ConclusionThe EHB process is a critical component of theAffordable Care Act. By establishing EHB plansthat offer adequate and appropriate benefits,states have an opportunity to greatly enhancehealth insurance coverage for millions ofAmericans who are uninsured or underinsured,particularly people with disabilities and othervulnerable populations.
ReferencesAutism Speaks. (2012, October 2). New York
Includes Autism Benefits in Health Care ReformPlan. Retrieved from www.autismspeaks.org/advocacy/advocacy-news/new-york-includes-autism-benefits-health-reform-plan
Coalition to Preserve Rehabilitation. (2012,October). Open letter to states on definingessential health benefits package. Retrieved fromwww.aahd.us/wp-content/uploads/2012/09/EHBRehabHabCCDHABCTechAssistSept-2012.pdf
Greenwood, K., Ragone, T.A., Jacobi, J.V. (2012,August). Implementing the Essential Health BenefitsRequirement in New Jersey: Decision Points andPolicy Issues. Newark, NJ: Rutgers Center forState Health Policy/Seton Hall Law.
Kliff, S. (2012, September 22). Is acupunctureessential health care? Weight loss surgery? UnderObamacare, states choose. Washington Post.Retrieved from www.washingtonpost.com/blogs/ezra-klein/wp/2012/09/22/is-acupuncture-essential-health-care-weight-loss-surgery-under-obamacare-states-must-choose/
National Academy for State Health Policy. (2012).State Progress on Essential Health Benefits.Retrieved from www.statereforum.org/state-progress-on-essential-health-benefits
ResourcesState Refor(u)m – A project of the NationalAcademy for State Health Policy, offers state-levelinformation on health reform implementation.www.statereforum.org
The Center for Health Insurance Reform – A project of Georgetown University Health Policy Institute. chir.georgetown.edu
1 The Supreme Court ruling in June 2012 rendered theMedicaid expansion optional for states. States that chooseto expand their Medicaid program must raise the eligibilitylevel to 133% of the federal poverty line.
By establishing EHB
plans that offer
adequate and
appropriate benefits,
states have an
opportunity to greatly
enhance health
insurance coverage
for millions of
Americans who
are uninsured or
underinsured,
particularly people
with disabilities and
other vulnerable
populations.

PracticePerspectives
Essential Health Benefits & the Affordable Care Act:What Social Workers Need to Know
FallI S S U E
N O V E M B E R2 0 1 2
SummaryA component of the Patient Protectionand Affordable Care Act (ACA) willhave a direct impact on the health andwell-being of over 70 million Americans.Beginning in January 2014, mostindividual and small group health plansoperating in the U.S. will be required toprovide “essential health benefits” (EHB),a package of health services definedbroadly by the ACA, but customized byeach state. Social workers should beaware of the EHB development processin their states, to ensure that their stateEHB plan addresses the needs of peoplewith chronic disease, disabilities, andother complex health issues, includingindividuals with mental health andsubstance use disorders, and thataccess to social work services ismaintained and strengthened.
What is the EHB Process and Why is it Important?The individual and small group insurancemarkets in the U.S. have traditionally offeredthe most expensive—and most inadequate—coverage of all commercial health plans. TheACA addresses this problem through the EHBprocess. The ACA outlines ten broad categoriesof essential health benefits (see chart) deemedessential for all Americans. The ACA delineatedthese benefit categories to assure consumersand small businesses that health insuranceplans purchased beginning in 2014 will becomprehensive, providing key services atappropriate levels to address serious healthconditions (Greenwood, et al, 2012). Certainbenefit categories, such as rehabilitative andhabilitative services and treatment for mentalhealth and substance use disorders, areparticularly important for individuals withdisabilities or chronic conditions, many ofwhom will be newly insured through the statehealth exchanges and the Medicaidexpansion. However, these benefits are oftenpoorly covered or absent in traditional smallgroup insurance plans.
Stacy Collins, MSW
Senior Prac t i ce Assoc ia te
sco l l [email protected]
Occupational Profiles: Available athttp://workforce.socialworkers.org/studies/other.asp• Social Work Salaries by Gender• Social Work Salaries by Race/Ethnicity• Social Workers in Colleges and Universities• Social Workers in Government Agencies• Social Workers in Health Clinics & Outpatient Health
Care Settings• Social Workers in Hospice and Palliative Care• Social Workers in Hospitals and Medical Centers• Social Workers in Mental Health Clinics & Outpatient Facilities• Social Workers in Private Practice• Social Workers in Psychiatric Hospitals• Social Workers in Schools• Social Workers in Social Service Agencies
Social Work Practice Perspectives: Available atwww.socialworkers.org/practice/default.asp• 2011 Medicare Changes for Clinical Social Workers• Accountable Care Organizations (ACOs): Opportunities for
the Social Work Profession• Adolescent Depression and Suicide Risk: How Social
Workers Can Make a Difference• Advocating for Clinical Social Workers: Highlights of 2010• Creativity and Aging• Dangerous Rites of Passage: Trends in College Alcohol
Consumption• Domestic Violence and Human Trafficking: Double Jeopardy
for Immigrant Women in the United States• Domestic Violence and Women of Color: Complex Dynamics• Engaging Young People in Their Transition Planning• Healthy People 2020: Social Work Values in a Public
Health Roadmap
• Opting Out of Medicare as a Clinical Social Worker• Results of 2010 Psychotherapy Survey• Support for Family Caregivers: The National Landscape
and the Social Work Role• Supporting the Child Welfare Workforce to Reduce
Child Maltreatment• The Medical Home Model: What Is It and How Do
Social Workers Fit In?
Leadership Ladders: Steps to a Great Career in Social WorkAvailable at http://careers.socialworkers.org/professionaldev/default.asp• From the Front Line to the Corner Office• Letting Your Voice be Heard• Managing Stress• Navigating Large Service Systems• Opening a New Private Practice• Outside the Lines: Maximizing the Flexibility of a
Social Work Degree• Presenting Your Work to Others• Publishing as a Practitioner• Risk Management in Clinical Practice• Strengthening Your Writing Skills: An Essential Task for
Every Social Worker• The Tech-Savvy Social Worker: Prepared for the
Challenges of 21st Century Practice• The Value of Dual Degrees
New Practice StandardsFor a complete list of practice standards, visitwww.socialworkers.org/practice/default.asp• NASW Standards for Social Work Practice with Family
Caregivers of Older Adults (2010)
750 First Street NE, Suite 700Washington, DC 20002-4241SocialWorkers.org
The NationalAssociation ofSocial Workers
750 First Street NE
Suite 700
Washington, DC 20002-4241
SocialWorkers.org
©2012 National Association ofSocial Workers. All Rights Reserved.
Practice Perspectives Fall November 2012
Center for Workforce Studies & Social Work Practice Recent Publications