
FAILURE TO THRIVE - Robert Wood Johnson Medical...
68
FAILURE TO THRIVE
Transcript of FAILURE TO THRIVE - Robert Wood Johnson Medical...
FAILURE TO THRIVE

FTT-Introduction
Despite the childhood obesity epidemic, undernutrition in children remains a significant problem that must be identified and treated.
Undernutrition is usually an outcome of 3 factors: . household level food security, . access to health and sanitation services, and . child caring practices.

FTT -
Introduction
Recent studies show that children who failed to thrive in infancy, especially in the first few months of life are lighter and shorter at school age with adverse intellectual outcomes including poor arithmetic performance and poor work habits.
Environmental and behavioral causes predominate, and negative effects on neurocognitivedevelopment are well documented.

FTT-
Introduction
It is likely that neurocognitive deficits attributed to FTT are a result of both poor nutrition and the detrimental effects of poverty and psychosocial stress on child development.
These infants also have a higher prevalence of feeding problems.

FTT-Introduction
These children also have increased rates of infection and behavioral problems, including impaired communication skills and attention deficit disorder.

FTT-
Prevalence
The prevalence of FTT depends on the risks within populations.
In developing countries or countries torn by conflict, infectious diseases, and inadequate nutrition are the primary risks.
In developed countries, the primary risks are preterm birth and family dysfunction. In all settings there are a myriad of other causes

FTT-
Prevalence
It is estimated that up to 5 in 100 infants and children in the United States have FTT.
More than 90% of cases in most series do not have an underlying medical cause, and virtually all medical causes are identified by a careful history and physical exam.

FTT-Prevalence
It is estimated that about 16% of children across developing countries are born with low birth weight (LBW). LBW rates are highest in the south-central Asia region (27%) and lowest in South America.
In 2005, 20% of children <5 years of age in low-and middle-income countries were underweight (weight-for-age <−2 standard deviations [SD]), and 32% were stunted (height-for-age <−2 SD).

FTT-Prevalence
Surprisingly, underweight rates in many south Asian countries (India, Bangladesh, Nepal, and Pakistan) are much higher than, and often nearly double, the rates in many sub-Saharan African countries.
Even though underweight and stunting are more prevalent among the poor, the prevalence rates among the highest income families are also high, thereby reiterating the fact that undernutrition is not just a result of food insecurity.

FTT –
Food Security
To achieve food security, it is necessary to look at 3 aspects of food security:
1. Availability refers to the supply of food (generally grain in the market, reflecting economic conditions of production and trade),
2. Access is at the household level, reflecting purchasing power as well as transfer programs. Access also has an intrahousehold
dimension, because food is not necessarily shared equitably within a household.
3.
The utilization mainstay
reflects the fact that even when a
household has access to food, it does not necessarily achieve nutritional security.

Choronology
of Growth
Growth is the main characteristic of childhood and a sensitive indicator of the child’s nutritional status.
From conception to adulthood, growth can be divided into different periods, including intrauterine, infancy, childhood and adolescence (puberty).

Chronology of growth
Prenatal growth is the most dramatic phase, achieving a velocity that is never again matched.
Infancy is the second most rapid growth period, with the infant gaining 20cm a year during the initial months, contrasting with 10–20cm a year by the age of 1.

Choronology
of Growth
Growth failure is more common during infancy than during any other stage of life, because programmed growth rates and therefore nutrient requirements per kg body weight are significantly higher in growing children than in adults, whereas body stores are lower.
This makes the young child more vulnerable to the effects of malnutrition, therefore the requirement for early recognition and appropriate treatment
Agostoni
et al., 2005.

Choronology
of Growth
Adolescence is another period of rapid growth when nutrition is critical.
Both the first two years of life and puberty are not to be missed.
Even short periods of nutritional deprivation may have lasting effects on health, leading to the idea that there are critical periods of growth that, if missed, may not be recoverable
Dobbing, 1990.

FTT
The terms of “organic” FTT vs “nonorganic” FTT (or “psychosocial” FTT) are now outmoded. According to a large body of newer thinking, FTT is not a syndrome. It is, rather, a physical sign that a child is receiving inadequate nutrition for optimal growth and development.
The work of the pediatrician is to determine, in an ordered and logical process, what may be leading to the inadequate nutrition and, when possible, to treat the underlying pathophysiologic issues, which often are multifactorial.

Growth Assessment
Growth parameters should be measured serially and plotted on growth charts appropriate for the child’s sex, age, and, if preterm, postconceptualage.
Growth charts are also available for some known chromosomal abnormalities, such as Down syndrome William syndrome, Turner syndrome or Russell Silver syndrome.

Growth Assessment
WHO growth standards show that preschool children, from different parts of the world, seem to have the same growth pattern if they have optimal nutrition and socioeconomic conditions.
Growth velocity is the main indicator of nutritional status in pediatrics at any stage of development.
Monitoring growth is an important tool for assessing the health and well-being of children at any age, whatever the clinical situation or country.
Growth Assessment
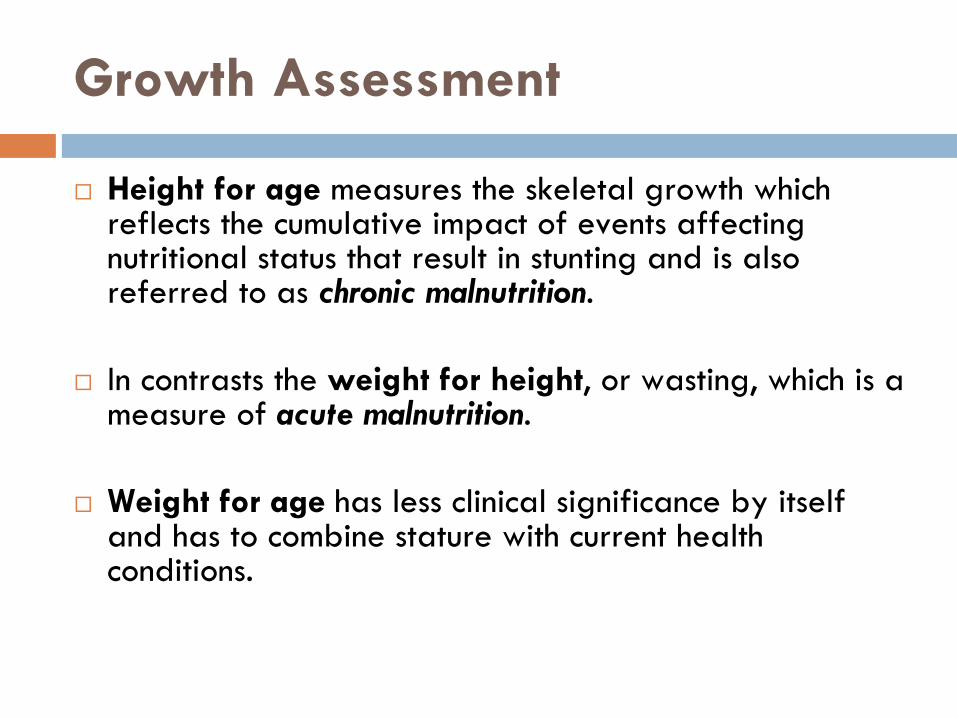
Height for age measures the skeletal growth which reflects the cumulative impact of events affecting nutritional status that result in stunting and is also referred to as chronic malnutrition.
In contrasts the weight for height, or wasting, which is a measure of acute malnutrition.
Weight for age has less clinical significance by itself and has to combine stature with current health conditions.

Growth Assessment
Weight-for-length is the ideal weight for a particular body length. It is the weight for the length percentile into which the child falls according to his/her age.
(Actual weight ÷ weight-for-length) × 100 is the formula used to calculate deviation (stated as a percentage).
BMI is calculated by dividing weight in kilograms by the square of height in meters.

Growth Assessment
Linear growth deficiency (stunting) is more likely to be due to congenital, constitutional, familial, or endocrine causes than to nutritional deficiency.
In endocrine disorders, length or height declines first or at the same time as weight; weight for height is normal or elevated.

Growth Assessment
In nutritional insufficiency, weight declines before length, and weight for height is low.
Children who have been chronically malnourished may be short (stunted) as well as thin, so that their weight-for-height curves may appear relatively normal.

Growth Assessment
mid-parental height is calculated in inches as follows:
•
Boys: [(maternal height + 5) + paternal height]/2•
Girls: [maternal height + (paternal height −
5)]/2
•
13 cm (instead of ±
5 in) if using metric units

Growth Assessment
In constitutional growth delay, weight and height decrease near the end of infancy, parallel the norm through middle childhood, and accelerate toward the end of adolescence. Adult size is normal.
In familial short stature, both the infant and the parents are small; growth runs parallel to and just below the normal curves.

Growth Assessment
A. Delayed growth and development in either parent (50%)
B. Normal birth historyC. Absence of organic or psychologic
diseaseD. Normal growth for the first several monthsE. Discrete interval of severe growth
deceleration1. Duration: 1-3 years2. Onset: under age 2 years
F. Bone age lags chronological ageG. Final height appropriate for genetic height
potentialH. Onset puberty delayed
A. Short parents
B. Normal birth history and gestational
weight
C. Absence of organic or psychologic
disease
D. Short Stature
1. Normal linear growth velocity for age
2. Bone age consistent with
chronological age
E. Normal age for the onset of puberty
Constitutional growth delay Familial short stature


FTT -
Definition
Although the concept of FTT is widely used, no consensus exists regarding its specific definition. Anthropometric criteria for assessing FTT are a matter of debate.
FTT in children younger than 2 years of age include: . weight is below the 3rd or 5th
percentile for age on more than one consecutive occasion,
. weight drops down two major percentile lines,
. weight is less than 80% of the ideal weight for age,
. weight-for-length is below the 3rd or 5th percentile
Jaffe, AC. Ped
Rev 2011

FTT -
Definition
The indicators studied by Olsen et al. include
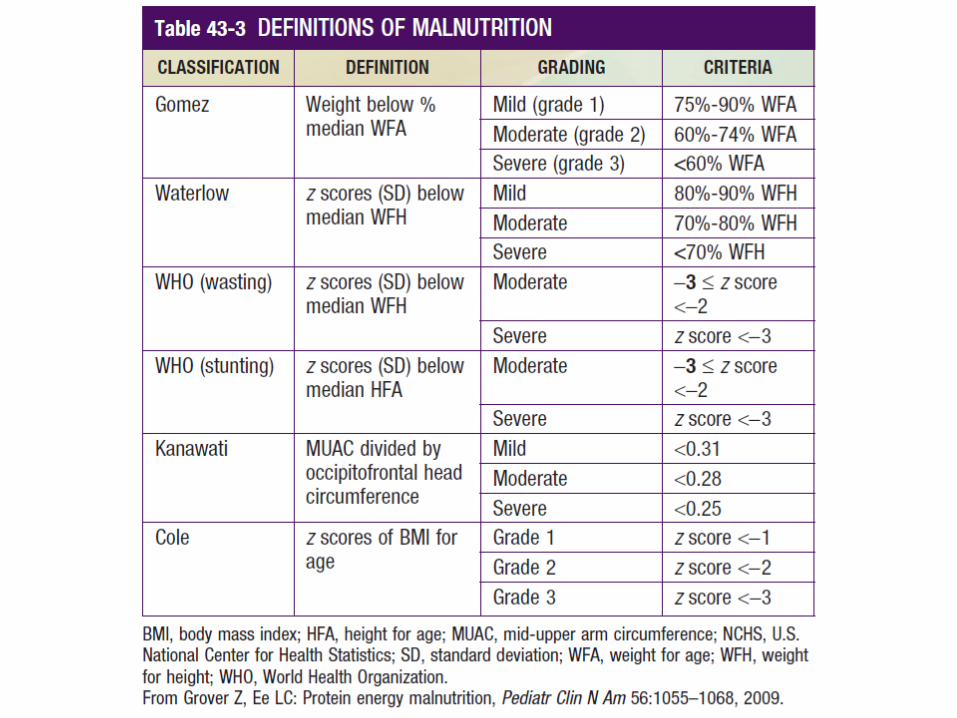
. weight < 75% of the median weight for chronological age (Gomez);
. weight <80% of the median weight for length (Waterlow);
. BMI for chronological age <5th centile;
. weight for chronological age <5th
centile; . length for chronological age <5th centile; . weight deceleration crossing more than two major centile
lines.
Olsen EM, et al., Arch Dis
Child 2007

FTT-
Definition
The following deviations from the norm are typical of failure to thrive:
●
Weight-for-length <70% to 79% or
●
BMI <3rd percentile ●
Weight <3rd percentile●
Lack of increase in length and/or weight with percentile deviations >2 main percentiles (3rd, 10th, 25th, 50th, 75th, 90th,97th)
Nützenadel, W. Dtsch
Arztebl
Int, 2011

FTT-
Definition (Ped
Endo)
In a cross-sectional review of articles published in English between 2002 and 2004, FTT is defined most commonly by the finding of:
. weight for age of less than the 10th percentile,
. height for age of less than the 5th percentile, or
. weight for height of less than the 10th percentile.
Daniel, M et al. Clin
Pediatr
2008

Consequences of Undernutrition
The most immediate consequence of undernutrition is premature death.
The global estimates conclude that stunting, severe wasting, and IUGR jointly contributes to 2.2 million deaths of children <5 yr of age.
This accounts for 35% of all child mortality globally, even though this estimate is lower than those previously reported.

Consequences of Undernutrition
By the time children reach their first birthday, if undernourished, they could suffer irreversible physical and cognitive damage, thereby impacting their future health, welfare, and economic well being.
These consequences continue into adulthood, and the cycle of undernutrition is passed on to the next generation when undernourished women give birth to LBW babies.

Consequences of Undernutrition
In many low-income settings, the consequence of malnutrition leads to reduced lifetime earnings.
These effects can come about through impaired cognitive development, late school entrance leading to delayed entry into the labor force, fewer completed years of schooling, less learning per year of schooling, or a combination of these.

FTT –
Etiology
The causes of disease-related FTT in children are multifactorial including
1. failure of a caregiver to offer adequate calories,
2. failure of the child to take in sufficient calories, 3. failure of the child to retain and use sufficient
calories, and 4. increased metabolic demands.

FTT –
Etiology
The most common cause of FTT, however, is an inadequate intake especially of energy and protein, but also of micro-nutrients (vitamins, iodine, iron, folic acid and zinc).
Children who fail to grow with no known organic cause are likely to have a lower intake due to poor appetite regulation, sensory hypersensitivity, delayed introduction to solid foods, fear of new foods and/or oral-motor dysfunction.

COMMON CAUSES OF MALNUTRITION IN EARLY LIFE
0-6 MO
Breastfeeding difficultiesImproper formula preparationImpaired parent/child interactionCongenital syndromesPrenatal infections or teratogenic
exposuresPoor feeding (sucking, swallowing) or feeding refusal (aversion)Maternal psychological disorder (depression or attachment disorder)Congenital heart diseaseCystic fibrosisNeurologic abnormalitiesChild neglectRecurrent infections

COMMON CAUSES OF MALNUTRITION IN EARLY LIFE
6-12 MO
Celiac diseaseFood intoleranceChild neglectDelayed introduction of age-appropriate foods or poor transition to foodRecurrent infectionsFood allergy
AFTER INFANCY
Acquired chronic diseasesHighly distractible childInappropriate mealtime environmentInappropriate diet (e.g., excessive juice consumption, avoidance
of high-calorie foods)Recurrent infections

FAILURE TO THRIVE: DIFFERENTIAL DIAGNOSIS BY SYSTEM
PSYCHOSOCIAL/BEHAVIORAL
Inadequate diet because of poverty/food insufficiency, errors in
food preparationPoor parenting skills (lack of knowledge of sufficient diet)Child/parent interaction problems (autonomy struggles, coercive feeding, maternal depression)Food refusalRuminationParental cognitive or mental health problemsChild abuse or neglect; emotional deprivation

GASTROINTESTINAL
Pyloric stenosis
Gastroesophageal
refluxRepair of tracheoesophageal
fistula MalrotationMalabsorption
syndromes Celiac diseasePancreatic insufficiency syndromes Cystic fibrosisChronic cholestasis
Inflammatory bowel disease Chronic congenital diarrhea statesShort bowel syndrome Pseudo-obstructionHirschsprung
disease Food allergy

NEUROLOGIC
Cerebral palsyHypothalamic and other CNS tumors (diencephalic
syndrome)Neuromuscular disordersNeurodegenerative disorders
RENAL
Recurrent urinary tract infectionRenal tubular acidosisRenal failure
ENDOCRINE
Diabetes mellitusDiabetes insipidusHypothyroidism/hyperthyroidismGrowth hormone deficiencyAdrenal insufficiency
GENETIC/METABOLIC/CONGENITAL
Sickle cell diseaseInborn errors of metabolism (organic acidosis, hyperammonemia, storage disease)Fetal alcohol syndromeSkeletal dysplasiasChromosomal disordersMultiple congenital anomaly syndromes (VATER, CHARGE)*

CARDIAC
Cyanotic heart lesionsCongestive heart failureVascular rings
PULMONARY/RESPIRATORY
Severe asthmaCystic fibrosis; bronchiectasisChronic respiratory failureBronchopulmonary
dysplasiaAdenoid/tonsillar
hypertrophyObstructive sleep apnea

MISCELLANEOUS
Collagen-vascular diseaseMalignancyPrimary immunodeficiencyTransplantation
INFECTIONS
Perinatal
infection (TORCHES)*Occult/chronic infectionsParasitic infestationTuberculosisHIV

FTT: Diagnostic work-up
History, physical examination, and observation of the parent-child interaction in the clinical or home environment usually suggest the most likely etiologies and thus direct appropriate workup and management.
A complete history should include a detailed nutritional, family, and prenatal history; documentation of who feeds and cares for the child; further information regarding the timing of the growth failure; and a thorough review of systems.

FTT: Diagnostic work-up
In young infants it is important to obtain a detailed dietary history, including quantity, quality, and frequency of meals, in addition to information about the caregiver’s response to excessive crying or sleeping.
In evaluating these infants and toddlers, physicians or health care providers should focus on formula preparation, feeding techniques, caloric intake, episodes of vomiting, interaction between the caregiver and the child, number of caregivers, and any financial difficulties faced by the family.

FTT –
Diagnostic work up
Typical screening laboratories include CBC&diff, CMP, iron studies, TFT’s, ESR/CRP, lead level, celiac panel and urine analysis.
Second line w/u: urine culture, allergy testing, stool studies including elastase, sweat test, PPD and HIV screen, serum aminoacids, urine aminoacids and organic acids. Also may include bone age, skeletal survey, EKG and endoscopies.

FTT-
Catch-up Growth
The ‘catch-up’ growth during infancy can be directly related to improved neurodevelopment, leading to the suggestion that the course of post-natal growth and not fetal growth determines later neurodevelopment (Latal-Hajnal et al., 2003).
Nonetheless, concern has been expressed that rapid growth during infancy may be associated with the development of insulin resistance and metabolic X syndrome (Ong, 2007). A dilemma, therefore, exists as to the best way to approach these high-risk infants (Yeung, 2006).

FTT: Catch-up growth
Nutritional rehabilitation with high-energy intakes results in increased weight gain and body fat, that is, the nature of the gain is directly dependent upon the compositional nature of intake. (MacLean and Graham, 1980; Jackson, 1990);
At hospital discharge, preterm infants accrue a significant protein deficit and are lighter, shorter and fatter than the reference infant at the same body weight or gestation (Embleton et al., 2001) (Uthaya et al., 2005; Cooke and Griffin, 2009).

FTT: Catch-up growth
After hospital discharge, a diet that is relatively high in energy may promote ‘catch-up’ that is paralleled by increased and/or altered adiposity; that is, central fat accretion.
A diet that better meets protein requirements may be paralleled by increased lean mass accretion.

FTT: Catch-up growth
Term infant formulas have a protein content of 1.8 g per 100 kcal. Nutrient-enriched formulas, as fed to preterm infants after hospital discharge, have a protein content that varies from 2.5 to 2.7 g per 100 kcal.
In a prospective randomized controlled trial, body size and composition were measured in preterm infants from discharge to 6 months: . Group A: a preterm formula (protein content =2.7 g/100 kcal), . Group B: a term formula (protein content 1.8 g/100 kcal), . Group C: a preterm formula to term and then a term formula to 6 months, or
. Group D: unfortified breast milk.
Cooke et al., 1999.

FTT: Catch-up growth
There were no significant differences in z-scores for weight or length between the groups at hospital discharge.
However, ‘catch-up’ in weight and length were faster and more complete in infants fed the preterm formula. This was paralleled by an increase in lean body (non-fat) mass and total fat mass but not % fat mass.
No differences were detected in central fat mass between infants fed the preterm formula compared with the other groups.
Cooke et al., 1999.
FTT: Catch-up growth
Interestingly, central fat was very similar in infants fed the preterm formula compared with the breast-fed infants.
However, leg fat mass was greater in infants fed the preterm formula compared with the other groups. These data indicate that increased total fat mass primarily reflected peripheral and not central fat mass accretion.
Cooke et al., 1999.

FTT: Catch-up growth
Insulin sensitivity/resistance was not determined and it is unclear whether any relationship exists between insulin responses and dietary protein intake and/or central obesity in these infants. Future studies must answer these questions.

FTT: Catch-up growth
Following the recent WHO guidelines for catch-up growth, the focus of dietary management during faltering growth has changed from supplementing only with energy to optimizing catch-up by providing adequate energy and protein
These guidelines suggest that 8.9–11.5% of energy should be supplied as protein, to provide optimal catch-up growth of lean and fat mass (from 10 g/kg/day = 8.9 PE% to 20 g/kg/day =11.5 PE%; 73:27 lean:fatmass).
WHO/FAO/UNU expert consultation, 2007.

FTT: Catch-up growth
Minimal catch-up growth should generally be 2-3 times the average weight gain for corrected age.
Multivitamin supplementation should be given to all children with FTT to meet the recommended dietary allowance, because these children commonly have iron, zinc, and vitamin D deficiencies, as well as increased micronutrient demands with catch-up growth.

FTT-
Catch-up growth
Once energy and protein requirements have been established, it is often the presumption that requirements are automatically and easily met, with nutritional support.
However, this is rarely the case. Problems with delivery of nutrients, the child’s taste preferences and intolerance to oral/tube feeds are often described.
It is therefore important to ensure that the requirements set are practically achievable for the parent/child, that the supplement is accepted by the child and, most importantly, that parents are empowered to assist in improving the nutritional intake.

FTT-
Catch-up growth
The decision with regard to the optimal route of feeding is related to the child’s ability to achieve the energy requirement and demonstrate weight gain.
If a child does not achieve nutritional requirements orally (via oral supplements), then enteral feeding must be considered.
In cases where enteral feeding does not meet the requirements due to increased requirements, increased losses and/or poor tolerance parenteral nutrition may be indicated.

Refeeding
syndrome
Children with severe malnutrition must be re-fed carefully with an incremental increase in calories to avoid re-feeding syndrome.
The type of caloric supplementation is based on the severity of FTT and the underlying medical condition.
The response to feeding depends on the specific diagnosis, medical treatment, and severity of FTT.

Refeeding
syndrome
The hallmark of refeeding syndrome is the development of severe hypophosphatemia after the cellular uptake of phosphate during the 1st week of starting to refeed.
Serum phosphate levels of ≤0.5 mmol/L can produce weakness, rhabdomyolysis, neutrophildysfunction, cardiorespiratory failure, arrhythmias, seizures, altered level of consciousness, or sudden death.

Refeeding
syndrome
Phosphate levels should be monitored during refeeding, and if they are low, phosphate should be administered during refeeding to treat severe hypophosphatemia



FTT-
Conclusion
The growth chart is the most basic daily work tool for any pediatrician, whether in hospital or in the community.
Growth monitoring should be considered as an ongoing process in assessing the health and well-being of children.

FTT-Conclusion
Nutrition teams with adequate nutritional interventions are essential elements of clinical practice, and children with or at risk of growth faltering should be identified appropriately and followed up longitudinally.
FTT and protein energy malnutrition have severe consequences for health development, behavior and school performance.

FTT-
Conclusion
It is important to ensure that the nutritional management plan is achievable and is regularly monitored to adjust for the child’s specific nutritional requirements.
Although these interventions should be implemented widely, it is recognized that existing nutrition solutions, even if universally applied, would only avert a minority fraction of the estimated death and disability due to undernutrition.

FTT-
Conclusion
Appropriate assessment and intervention of cognitive and emotional development is necessary for all children with FTT.
Referrals to early intervention, Head Start, or Supplemental Security Income (SSI) may be beneficial.
Home intervention may attenuate some of these negative effects of early failure to thrive.




















