Failure mechanisms of osseointegrated oral implants
23
What is going on in the specialities IMPLANTS/PROSTHETICS MARCO ESPOSITO Senior Lecturer in Oral and Maxillofacial Surgery, School of Dentistry, and Editor of the Cochrane Oral Health Group, The University of Manchester, UK; Assoc Prof in Biomaterials, Göteborg University, Sweden Evidence for up-to-date clinical dental practice – a review of 10 years of the Cochrane Oral Health Group 30th-31st May 2006, Manchester
-
Upload
dentistryinfo -
Category
Documents
-
view
836 -
download
2
description
Transcript of Failure mechanisms of osseointegrated oral implants
What is going on in the specialitiesIMPLANTS/PROSTHETICS
MARCO ESPOSITO
Senior Lecturer in Oral and Maxillofacial Surgery, School of Dentistry, and Editor of the Cochrane Oral Health Group, The University of Manchester, UK; Assoc Prof in Biomaterials, Göteborg University, Sweden
Evidence for up-to-date clinical dental practice – a review of 10 years of the Cochrane Oral Health Group30th-31st May 2006, Manchester
AN OVERVIEW
From 11 Cochrane reviews on osseointegrated dental implants and 1
review on prosthetics
Updated to March 2006http://www.cochrane.org
http://www.cochrane-oral.man.ac.uk
GENERAL AIM
To test the efficacy of various materials and procedures for replacing missing teeth considering side effects and complications.
1 BONE AUGMENTATION PROCEDURES
A) to test whether and when bone augmentation procedures are necessary.
B) to test which is the most effective bone augmentation technique for specific clinical indications.
Trials were divided into 3 broad categories according to different clinical indications:
1) major vertical and/or horizontal bone augmentation2) implants placed in extraction sockets3) treatment of fenestration around implants.
1 BONE AUGMENTATION PROCEDURES
• Last literature search: October 2005
• 13 RCTs with 330 participants (17 RCTs excluded)
Bone augmentation of athrophic edentulous mandibles (1 trial)Stellingsma 2003 short implant vs “sandwich” bone graft
Sinus lifting (3 trials)Wannfors 2000 1-stage block vs 2-stage particulated boneHallman 2002 1-stage particulated bone vs 80%Bio-Oss/20%bone vs 100% Bio-OssSzabó 2005 2-stage: particulated bone vs 100% tricalciumphosphates (Cerasorb)
DESCRIPTION OF STUDIESVertical augmentation (2 trials)Chiapasco 2004 bone + titanium barrier vs distraction osteogenesisMerli submitted particulated bone: resorbable barrier + plates vs titanium barrier
Immediate implants in fresh extraction sockects (4 trials)Cornelini 2004 resorbable barrier + Bio-OssChen1 2005non-resorbable vs resobable + particulated boneChen2 2005particulated bone vs controlChen manuscript Bio-Oss vs Bio-Oss + resorbable barrier
Fenestrations and dehiscence around implants (3 trials)Dahlin 1991 non-resorbable barrier vs controlCarpio 2000 GBR + bone/Bio-Oss: resobable vs non-resorbableJung 2003 resorbable barrier & Bio-Oss + rhBMP-2 (placebo)
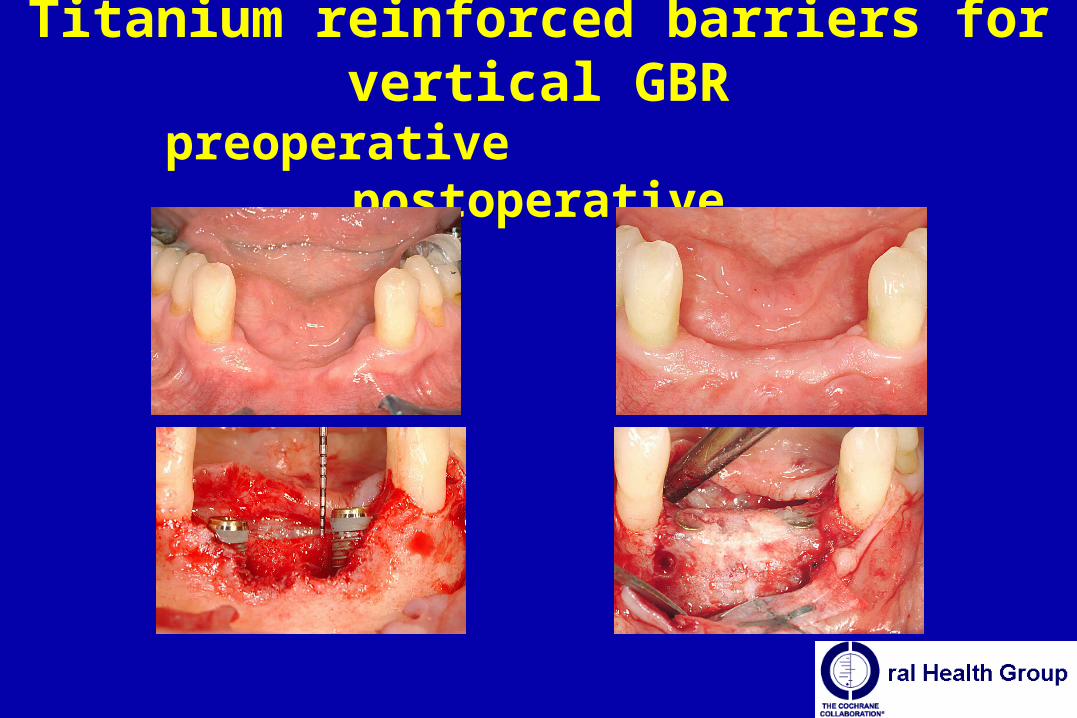
Titanium reinforced barriers for vertical GBRpreoperative postoperative
CONCLUSIONS• In atrophic edentulous mandibles there are more
implant failures, complications, pain, cost and longer treatment time using “sandwich” bone grafts than short implants.
• Sinus lifting with 100% bone substitutes (Bio-Oss and Cerasorb) might work with sinus floor < 5 mm.
• It is possible to augment bone vertically, however complications are frequent and it is unclear which is the most effective technique.
CONCLUSIONS• It unclear whether augmentation procedures are needed in
postextractive sockets and which is the most effective one. In sites treated with Bio-Oss + barriers, the gingival margins may be positioned 1.2 mm higher than in sites treated with barriers alone.
• GBR allows bone augmentation at fenestrated implants, but it is unclear whether it is needed, and which is the most effective technique.
• Complications with GBR procedures are common. There might be an association between bone retrieved with “bone filters” also using a dedicated suction device and infective complications.
2 Various implant characteristics/systemsIs a surface modification, an implant shape, a material or an implant system more effective than the others?Last literature search: February 2005.12 RCTs with 512 participants and 12 different implant systems (19 RCTs excluded). 4 RCTs with a 5-year follow-up.Minor statistically significant differences in marginal bone loss and in the occurrence of perimplantitis (20% risk reduction to have perimplantitis at 3 years around implants with a machined surface). No statistically significant difference in failure rates.
We do not know whether any implant system is superior to the others. It does not mean that they are all the same!
3 Immediate, early or conventional loading
Is there any difference if implants are immediately or early loaded?
Last literature search: February 2004.
5 RCTs with 124 participants (2 RCTs excluded).
For “good quality mandibles” we do not know whether a difference does exist. It does not mean that the techniques provide the same results!
4 MaintenanceWhich is the most effective maintenance technique or regimen?
Last literature search: June 2004.
5 RCTs with 127 participants (9 RCTs were excluded); electric (1 RCT) and sonic (1 RCT) vs manual toothbrush; phosphoric acid gel vs debridement (1 RCT); subgingival vs chlorhexidine mouthrinses (1 RCT); adjunctive Listerine mouthrinse vs placebo (1 RCT). Follow-up: 6 weeks-5 months.
Adjunctive Listerine mouthrinse reduces dental plaque and marginal bleeding.
5 Surgical techniquesIs there any surgical technique associated to higher success rates?
Last literature search: September 2002.
4 RCTs (5 RCTs excluded). 2 RCTs compared 2 versus 4 implants with mandibular overdentures (170 participants); 2 RCTs compared a crestal surgical incision with a vestibular incision (20 participants).
We do not know whether a surgical technique is superior, however, 2 mandibular implants can be sufficient to hold an overdenture. It does not mean that all techniques are the same!
6 Immediate, immediate-delayed and delayed implants in extraction sockets
How long time we need to wait to insert an implant in postextractive sockets?
Last literature search: March 2006.
1 RCT with 46 participants: immediate delayed (ca 10 days) vs delayed (ca 3 months) implants. Follow-up (loading) 1 year and half.
Patients treated with immediate-delayed implants were more satisfied, and the perimplant tissues position was judged to be more appropriate in relation to the neighbouring teeth by and independent and masked assessor.
7 Treatment of perimplantitisWhich is the most effective treatment for perimplantitis?
Last literature search: March 2006.
5 RCTs with 106 participants (2 RCTs excluded):• local antibiotics vs debridement (2 RCT)• mechanical (Vector) vs manual debridement (1 RCT)• laser vs debridement and Chlorhexidine irrigation/gel (1 RCT)• systemic antibiotics + 2 different local antibiotics + resective surgery + modification of the surface topography.
Follow-up 3 months – 2 years
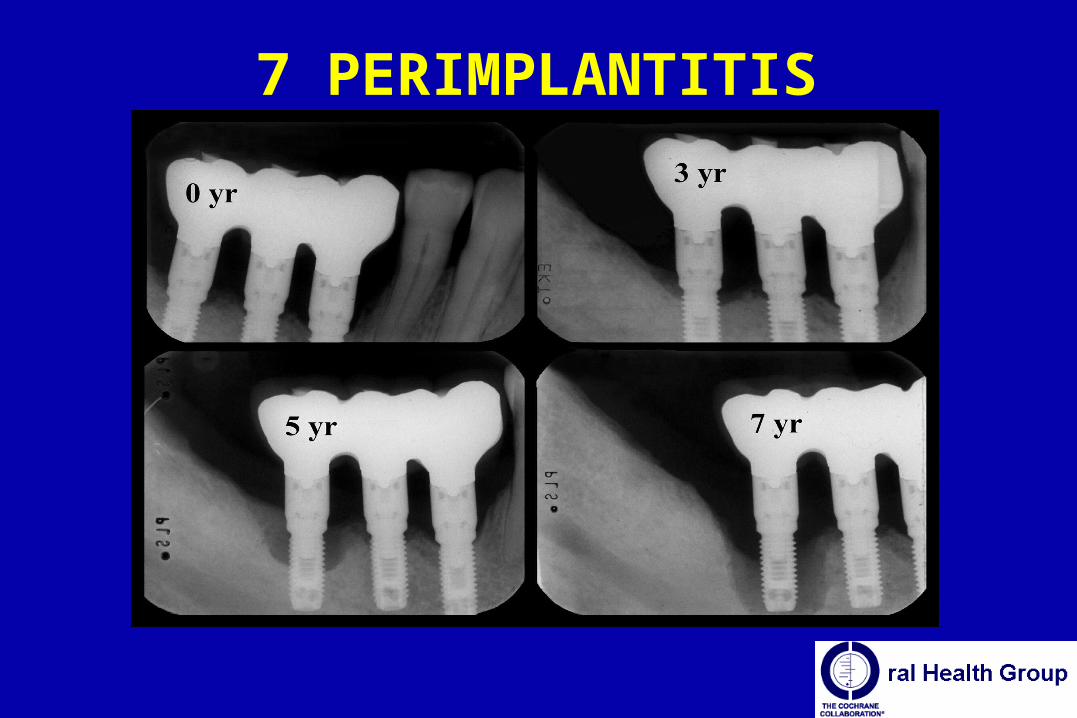
7 PERIMPLANTITIS
7 Treatment of perimplantitis
No difference between more complex procedures and conventional debridement in light forms of perimplantitis.
The adjunctive use of local antibiotics (doxycycline) to debridement showed an improvement of about 0.6 mm for PAL and PPD, after 4 months in patients affected by severe forms of perimplantitis (bone loss > 50%).
8 Preprosthetic surgery vs implants
Which intervention is more effective: preprosthetic surgery and dentures vs a implant supported denture?
Last literature search: October 2005.
1 RCT with 60 participants.
Patients treated with preprosthetic surgery and dentures are less satisfied than patients who received a mandibular overdenture on implants.
9 Use of prophylactic antibioticsDoes the use of prophylactic antibiotics at implant placement decreases postoperative complications and early failures?
Last literature search: March 2006.
0 RCT.
10 Zygomatic implants
Zygomatic implants with and without bone grafting versus conventional implants in augmented bone.
Last literature search: March 2006.
0 RCT.
11 Hyperbaric oxygen therapy
Does hyperbaric oxygen (HBO) therapy decrease implant failures and complications in irradiated patients?
Last literature search: March 2006.
0 RCT.
12 Denture chewing surface designs
Which denture chewing surface design should be used?
Last literature search: April 2004.
1 cross-over RCT with 30 participants (1 RCT excluded): lingualised (maxillary anatomic and mandibular non-anatomic) vs zero-degree teeth.
Patients preferred dentures with lingualised teeth.


















