Facial nerve
89
1 Good Morning…
-
Upload
md-abdul-haleem -
Category
Education
-
view
28 -
download
0
Transcript of Facial nerve

1
GoodMorning…

2
FACIAL NERVE
DR. CHINNU VARGHESEDR. MOHAMED ABDUL HALEEM

3
CONTENTS INTRODUCTION NERVE AND ITS CONDUCTION CLASSIFICATION OF NERVOUS SYSTEM INTRODUCTION TO FACIAL NERVE EMBRYOLOGY NUCLEI OF ORIGIN FUNCTIONAL COMPONENTS COURSE BRANCHES AND DISTRIBUTION GANGLIA BLOOD SUPPLY SURGICAL ANATOMY OF FACIAL NERVE APPLIED ASPECTS CONCLUSION BIBLIOGRAPHY

4
A bundle of fibers that uses electrical and chemical signals to transmit sensory and motor information from one body part to another.
WHAT IS A NERVE?

5
NERVE AND ITS CONDUCTION
1. The Neuron (nerve cell)- is the structural unit of the nervous system.
2. It transmits messages between the CNS and all parts of the body.

6
NERVE AND ITS CONDUCTION
3. There are two basic types of neurons: the sensory(afferent) and motor (efferent).
4. Sensory neurons- are capable of transmitting the impulses from site to the CNS.
5. Motor neurons- conduct impulses from the CNS toward the periphery.

7
NERVE CONDUCTION

8
CLASSIFICATION OF NERVOUS SYSTEM
NERVOUSSYSTEM

9

10
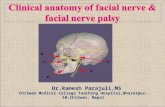
INTRODUCTION TO FACIAL NERVE
There are 12 cranial nerves.The Facial nerve is the 7th cranial nerve. It is the nerve of the second branchial arch.Hence supplies all the muscles that develop from
the mesoderm of this arch. It is a mixed nerve with a large motor root and a
small sensory root.

11
MICROANATOMY OF FACIAL NERVE It is estimated that each of the 7000 neuron cell
bodies which extend axons from the facial nucleus innervates 25 muscle fibers.
The smaller the ratio of muscle fibers to neuron cell bodies , the greater is the degree of specialized movement possible.

12
Diameter of facial nerve axons varies between 3-20µm and the nodes of ranvier are spaced from 0.1-1.8µm apart.
Because facial nerve fibers are myelinated the wave of depolarization can jump from one node of ranvier to the next, a process called saltatory conduction.
This accounts for the rapid conduction velocity of the facial nerve, which is 70-110m/sec.

13
EMBRYONIC DEVELOPMENT OF FACIAL NERVE
Facial nerve course, branching pattern, and anatomical relationships are established during the
first 3 months of prenatal life
The nerve is not fully developed until about 4 years of age
The first identifiable facial nerve tissue is seen at the third week of gestation-facioacoustic
primordium or crest

14EMBRYOLOGY OF FACIAL NERVE
Weeks Features
0-4 Appearance of facio-acoustic primordium/crestSplitting of facial nervePresence of chorda tympani
5-6 Separation of facial and acoustic nervesAppearance of geniculate ganglionFormation of GPN
7 Formation of peripheral branches
8 Formation of fallopian canal10-15 More extensive branching

15
NUCLEI OF ORIGIN AND THEIR COMPONENTS
Motor nucleus Upper face recieves bilateral innervation.
lower face receives unilateral innervation.
Muscles of facial expression.
posterior belly of digastric.
stylohyoid muscle.
stapedius.Lacrimatory and Superior salivatory nucleus
Submandibular & sublingual salivary glands
lacrimal glandNucleus of solitary tract ( gustatory nucleus)
Mediates taste

FUNCTIONAL COMPONENTS
16
MOTOR
• SPECIAL VISCERAL
• GENERAL SOMATIC
SENSORY
• SPECIAL VISCERAL
• GENERAL SOMATIC

17FUNCTIONAL COMPONENTS - motor
Branchial motor(special visceral efferent)
supply the muscles derived by the mesoderm of II branchial arch which are
the muscles of facial expression; occipitofrontalis; posterior belly of digastric muscle; stylohyoid, and stapedius.
Visceral motor(general somatic efferent)
Originates in superior salivatory nucleus and Parasympathetic innervation of the
lacrimal, submandibular, and sublingual glands, mucous membranes of nasopharynx, hard and soft palate.

18
Special sensory(special visceral afferent)
Taste sensation from the
Anterior 2/3 of tongue Hard and soft palates.
General sensory(general somatic afferent)
General sensation from the skin of
external acoustic meatus and deeper parts of the auricle.
FUNCTIONAL COMPONENTS - sensory

19
COURSE1. Intra cranial course
Intra pontine courseAttachment to the brain stemCourse through posterior cranial fossa
3. Exit from the cranium
4. Extracranial course
2. Intrapetrous course Meatal partFacial canal part
labyrinthine segmentTympanic segmentMastoid segment

20INTRACRANIAL COURSE
Intrapontine Course:
the fibers from the motor nucleus course through the pons taking a sharp bend around the abducent nucleus producing internal genu of the facial nerve and they leave the pons between the nucleus of spinal tract of trigeminal and the other facial nucleus.

21
Attachment to the brain stem:
The sensory and motor roots are attached to the lateral aspects of the pontomedullary junction.
INTRACRANIAL COURSE

22INTRACRANIAL COURSE
Course Through Posterior Cranial Fossa
From the superficial attachment to the brainstem to the opening of the internal acoustic meatus the two roots of the facial nerve passlaterally and forward in the cerebellopontine angle along with vestibulochoclear nerve and labyrinthine artery. These structures together enter the internal acoustic meatus.

23INTRAPETROUS COURSE
Meatal segment: It is in the internal acoustic
meatus where the motor root is lodged in a groove on the antero-inferior surface of the vestibulochoclear nerve but the sensory root separates them.
At the bottom of the internal acoustic meatus , the two roots unite to form the trunk of the facial nerve and then it enters
the facial canal.

24
i. Labyrinthine segment : passes laterally above the vestibule of the inner ear to reach the anterior end of the medial wall of the middle ear. Here it bends backwards at a sharp turn called the external genu of the facial nerve which has the geniculate ganglion on it.
Facial canal part: is divided into 3 segments:
INTRAPETROUS COURSE

25
ii. Tympanic segment: passes backwards in the
medial wall of the middle ear till it reaches the posterior end of this wall. It is also known as the horizontal part.
INTRAPETROUS COURSE

26
iii. Mastoid segment or vertical segment: begins at the posterior end of the medial wall and passes downwards in relation to the posterior wall of the middle ear to reach the stylomastoid foramen.
INTRAPETROUS COURSE

27
EXIT FROM THE CRANIUM
The facial nerve leaves the cranium through stylomastoid foramen

28EXTRACRANIAL COURSE
The facial nerve crosses the lateral side of the base of the styloid process.
It enters the posteromedial surface of the parotid gland.

29EXTRACRANIAL COURSE
Within the gland it runs forward for a short distance superficially to the retromandibular vein and external carotid artery and then divides into
a)Temprofacial and b)Cervicofacial trunks.

30EXTRACRANIAL COURSE
Temporofacial and Cervicofacial Trunks.

31EXTRACRANIAL COURSE
The terminal branches radiate like a goose’s foot from the anterior border of the parotid gland – “Pes
anserinus”

32
BRANCHES AND DISTRIBUTIONI. Within the facial canal:a. Greater petrosal nerveb. Nerve to stapediusc. Chorda tympani nerveII. At the exit from the styomastoid foramen:a. Posterior auricular nerveb. Nerve to the digastricc. Nerve to stylohyoid

33
III. Terminal branches within the parotid gland:a. Temporal nerveb. Zygomatic nervec. Buccal nerve d. Marginal mandibular e. Cervical branchIV. Communicating branches with adjacent cranial
and spinal nerves

34
Within the facial canal

35Greater Petrosal Nerve

36Greater Petrosal Nerve
Carries gustatory and parasympathetic fibers.
Arises from the geniculate ganglion of the facial nerve, and enters the middle cranial fossa through the hiatus for the
greater petrosal nerve on the anterior surface of the petrous temporal bone.
It proceeds towards the foramen lacerum where it joins the deep petrosal nerve which carries sympathetic fibers to
form nerve of petrygoid canal.

37
The nerve of the pterygoid canal passes through the pterygoid canal to reach the pterygoplatanine ganglion. The
parasympathetic fibers relay in this ganglion.
Postganglionic parasympathetic fibers arising in the ganglion ultimately supply the lacrimal gland and the mucosal glands of
the nose, palate and pharynx.
The gustatory or taste fibers do not relay in the ganglion and are distributed to the palate.
Greater Petrosal Nerve

38Nerve To The Stapedius
Arises opposite the pyramid of the middle ear , and supplies the stapedius
muscle.
The muscle damps excessive vibrations of the
stapes caused by high-pitched sounds.

39The Chorda Tympani
It runs upwards and forwards in a bony canal. It enters the middle ear and runs forwards in close relation to the
tympanic membrane.
Arises in the vertical part of the facial canal about 6mm above the stylomastoid foramen.

40The Chorda Tympani
It leaves the middle ear by passing through pterygopalatine fissure. It then passes medial to
the spine of the sphenoid and enters the infratemporal fossa. Here it joins the lingual
nerve through which it is distributed.
It carries the preganglionic fibres to the submandibular and sublingual salivary glands and taste fibres from the anterior two-thirds of
the tongue.

41
At The Exit From The Stylomastoid Foramen

42Posterior auricular nerve
Arises just below the stylomastoid foramen. It ascends between the mastoid process and the
external acoustic meatus and supplies:
POSTERIOR AURICULAR BRANCH
a) The posterior auricularis
b) The occipitalisc) The intrinsic muscles
on the back of the auricle.

43The digastric branch
Arises close to the posteriorauricular nerve.It is short and supplies the posterior belly of
digastric .

44Stylohyoid branch
It arises with the digastric branch.It is long and supplies the stylohyoid muscle.

45
Terminal branches within the parotid gland

46

47Communicating branches

48Ganglia Associated With Facial Nerve

49
Ganglia Associated With Facial Nerve
-the taste fibers present in the nerve are present in the genigulate ganglion.
I. GENICULATE GANGLION :is located on the first bend of the facial nerve, in relation to the medial wall of the middle ear.
-it is a sensory ganglion

50
II. SUBMANDIBULAR GANGLION:
- is a parasympathetic ganglion for relay of secretomotor fibers to the submandibular and sublingual salivary glands.

51
II. SUBMANDIBULAR GANGLION:
the motor or parasympathetic fibers pass from the lingual nerve to the ganglion through the posterior
root. These are preganglionic fibers that arise in the superior salivatory nucleus and pass through the facial nerve- the chorda tympani and the lingual
nerve to reach the ganglion.
The fibers relay in the ganglion.

52
iii. PTERYGOPLATINE GANGLION (SPHENOPALATINE
GANGLION):

53
iii. PTERYGOPLATINE GANGLION (SPHENOPALATINE
GANGLION):
• Is the largest parasympathetic peripheral ganglion.
• It serves as a relay station for secretomotor fibers to the lacrimal gland and to the mucous glands of the nose,paranasal sinuses,palate and the pharynx.
• It is also called hay fever ganglion.

54
BLOOD SUPPLYThe facial nerve gets it’s blood supply from 4 vessels:
.
Anterior inferior cerebellar artery At the cerebellopontine angle
Labyrinthine artery (branch of anterior inferior cerebellar artery) – within internal acoustic meatus
Superficial petrosal artery(branch of middle meningeal artery) – geniculate ganglion and nearby parts
Stylomastoid artery(branch of posterior auricular artery) – mastoid segment

55
BLOOD SUPPLY
Venous drainage is into the venae comitantes
of the superficial petrosal and
stylomastoid viens.
The arteries form a external plexus lying within the epineurium and an internal plexus which is intraneural.

56
FUNCTIONThe facial nerve is responsible for:
-Contraction of the muscles of the face
-Production of tears from a gland (Lacrimal gland)
-Conveying the sense of taste from the anterior 2/3rd of the tongue (via the Chorda tympani nerve)
-The sense of touch at auricular conchae

57
SURGICAL ANATOMY OF FACIAL NERVE

58
Variations of facial nerve branching patterns
Flower (1961) reviewed seven variations including changes in angulation.
Curtis and May (1986) reported a case of progressive facial nerve canal along the internal
auditory canal, creating a double internal auditory canal.

59
Variations of facial nerve branching patterns
Caprosa and Klassen (1966) observed bifurcation of facial nerve just distal to the geniculate
ganglion.
Duncan, Shea and Sleeckx (1967) found bifurcation of branches of the chorda tympani.

60
CLINICAL RELEVANCE-DAMAGE TO THE FACIAL
NERVE

Three Degrees of Facial Nerve Fiber Injury
61

Three Degrees of Facial Nerve Fiber Injury
62

63
Level Of Nerve Injury And SymptomsThe facial nerve has a wide range of functions. Thus,
damage to the nerve can produce a varied set of symptoms, depending on the site of the lesion.

64
FACIAL PARALYSIS

65
Paresis: weakness of facial muscles to perform motor functions is called paresis (partial
dysfunction)
Paralysis: Total flaccidity of facial muscles to perform motor function is called facial paralysis

66
SUPRANUCLEAR FACIAL PARALYSIS
It is usually hemiplegia- it is the lower part of the
face that is chiefly affected, while the upper
part remains unaffected,i.e.,the
frontalis and orbicularis oculi muscles escape. This is because there is bilateral control

67
INFRA NUCLEAR FACIAL PARALYSIS
The lower motor neuron lesion of
facial nerve cause paralysis of all facial muscles on the same
side.
In LMN injury both the upper and lower parts will be involved

68
HOUSE-BRACKMAN(1985) CLASSIFICATION FOR FACIAL FUNCTION
Grade I-normal function without weakness. Grade II-mild dysfunction with slight facial asymmetry with a minor degree
of synkinesis. Grade III-moderate dysfunctions-obvious , but not disfiguring, asymmetry
with contracture and/or hemifacial spasm,but residual forehead motion and incomplete eye closure.
Grade IV-moderately severe dysfunction- obvious, disfiguring asymmetry with lack of forehead motion and incomplete eye closure.
Grade V-severe dysfunction-asymmetry at rest and only slight facial movement.
Grade VI-total paralysis-complete absence of tone or motion.

69
BELL’S PALSY It is defined as an idiopathic
paresis or paralysis of the facial nerve of sudden onset.
The name was ascribed to SIR CHARLES BELL, who in 1821 demonstrated the separation of motor and sensory innervation of face.

70
INCIDENCE- 15-40 cases per 1 lakh cases
SEX PREDILECTION- women more affected than men.3.3 more times common in pregnancy and in the third trimester.
AGE- can occur at any age, common in middle aged people.
SIDE INVOLVMENT- can be equally seen, usually unilateral.

71
CLINICAL FEATURES

72
CLINICAL FEATURES Inability to smile, close eye and raise eyebrow. Whistling is impossible Drooping of corners of the mouth. Slurred speech Inability to close eyelid (Bell’s sign) Loss of blinking reflex Inability to wrinkle forehead Mask like appearance of the face. Loss or alteration of taste.

73
COURSE AND PROGNOSIS
Partial paralysis always resolves completely within a few
weeks.
Recovery from complete paralysis takes longer (months) and
is complete in only about 60-70% of cases.
Approximately 15% of patients are left with troublesome
residual palsy.

74
RAMSAY HUNT SYNDROME
A special form of herpes zoster infection
of the geniculate ganglion with the
involvement of the external ear and the
oral mucosa

75
MELKERSSON ROSENTHAL SYNDROME
Recurrent attacks of facial paralysis Associated with multiple episodes of non-pitting,
non-inflammatory painless edema of the face Chelitis granulomatosa
Fissured tongue

76
MOBIUS SYNDROME
Results from the underdevelopment of
cranial nerve VI and VII
The VI cranial nerve controls lateral eye
movement, and the VII cranial nerve controls
facial expression and is manifested in infancy.

77
MOBIUS SYNDROMEBecause of partial or
complete facial paralysis, the infant exhibits :
No change in facial expression (mask like appearance)
Failure to close eyes during sleep.
Mouth may remain partially open

78
CROCODILE TEARS SYNDROME Due to injury to facial nerve
proximal to the geniculate ganglion, there may be a misdirection of nerve fibres to lacrimal gland instead of going to submandibular gland, through the greater petrosal nerve. As a result patient lacrimates is termed as ‘crocodile tear syndrome’ and can be treated by dividing greater petrosal nerve.

79
CLINICAL NOTES Parotid disease: Parotid tumours, trauma or
surgery may damage branches of the facial nerve. This would result in an ipsilateral facial palsy with wasting and functional loss. It would be unlikely to recover.
PATEY’S OPERATION

80
CLINICAL NOTES Stapedial hyperacusis: Dysfunction of the smallest muscle supplied by the facial nerve can
cause a distressing symptom.
Stapedius dampens the movements of the ossicular chain and if it is inactive, sounds will be
distorted and echoing.
This is hyperacusis.

81
This branch passes on or just below the lower margin of the
mandible. It is superficial even to the palpable facial
arterial pulse and is thus liable to injury.
The marginal mandibular branch of the facial nerve:
CLINICAL NOTES

82
The marginal mandibular branch of the facial nerve:
CLINICAL NOTES
Section of this nerve would
result in paralysis of the muscles of the corner of the
mouth: drooling would occur.

83
Facial nerve injury in babies: As the mastoid process is rudimentary(not completely developed) at birth, the facial nerve is more easily damaged in babies. Birth injuries or
other trauma, can therefore cause an ipsilateral facial palsy.
This is serious since buccinator, supplied by
VII, is necessary for sucking(feeding).
CLINICAL NOTES

84
Acoustic neuroma: This is a tumour of Schwann cells on the vestibular nerve in the IAM(Internal Acoustic Meatus). Since the tumour grows within a bony canal it may compress the
facial and vestibulocochlear nerves causing a particular type of deafness (nerve deafness) and an ipsilateral facial
palsy.
CLINICAL NOTES

85
Cerebellopontine angle tumours : Tumours in this
region would cause signs and symptoms of damage to the facial and vestibulocochlear nerves and cerebellar signs. These include facial palsy,
deafness, vertigo and poor coordination.
CLINICAL NOTES

86
Evaluation of Nerve function HISTORY is of vital importance to establish the onset
characteristics, duration and degree of recovery. Previous trauma, surgery or infection may help in arriving at a
diagnosis Examination of the face at rest and movement. Radiologic evaluations : CT, MRI Nerve function tests : topognostic testing, ear pain, taste,
tearing, salivation, stapeus reflex/auditory testing, vestibular testing, electronystagmography, Electrophysiologic testing: Evoked electromyography.

87
CONCLUSION
The most important thing about the intracranial course of Facial Nerve is its relationship to the middle ear.
The most important thing about the extracranial course is its relationship to the parotid gland.
Hence a complete understanding of its anatomy is essential and care should be taken during surgical procedures.

88
REFERENCES Gray’s anatomy 2nd edition Head and neck anatomy- Berkovitz ; Moxham Essentials of human anatomy : 9th edition. Russell T ; William B.D.Chaurasia’s Human Anatomy 4th edition Clinical Anatomy 2nd edition -Neeta V Kulkarni The Facial Nerve – May’s 2nd edition Handbook of local anaesthesia- Stanley F Malamed 5th edition Shafer’s Textbook of Oral Pathology -5th edition Atlas of clinical gross anatomy- Kenneth , John , Pedro.

89