Facial Motion Disorders - cdn.ymaws.com · FACIAL NERVE (CN VII) •7,000 individual nerves...
61
FACIAL MOTION DISORDERS Tami Konieczny MS, OTR/L Anne-Ashley Field MOTR/L October 19, 2019
Transcript of Facial Motion Disorders - cdn.ymaws.com · FACIAL NERVE (CN VII) •7,000 individual nerves...

FACIAL MOTION DISORDERS
Tami Konieczny MS, OTR/L
Anne-Ashley Field MOTR/L
October 19, 2019

OBJECTIVES
• Identify and define anatomical structures involved in facial expression
• Identify primary causes of facial paralysis
• Identify functional impairments related to facial paralysis
• Review standardized assessment tools used with this population
• Review methods of evaluation and tracking progress
• Review treatment approaches
2

ANATOMY REVIEW – CRANIAL NERVE VII – FACIAL NERVE
3

FACIAL NERVE (CN VII)
• 7,000 individual nerves
• Mainly a motor nerve
• Allows us to laugh, cry, smile, frown
• “the nerve of facial expression”
• Also, carries nerve impulses to the tear glands, saliva glands, and transmits taste from the front of the tongue.
4

ANATOMY REVIEW- FACIAL MUSCLES
5
Frontalis
Orbicularis oculi
Zygomaticus Major/minor

HOW ARE FACIAL MUSCLES DIFFERENT
• Lack Muscle Spindles : tension receptors, muscle tone, and reflex receptors; specialized muscle fibers regulate muscle contraction and relaxation
• Facilitory techniques –tapping, vibration do not work
• Oppositional Action
• No oppositional muscles
• Returns to resting state
• Small motor units
• Ocular Muscles (6-10 muscle fibers)
• Gastrocsnemius (1800-2000 muscle fibers)
• Receive emotional information
6

FACIAL PALSY
• Acquired• Trauma • Stroke• Brain Tumor• Infections
• Ramsey Hunt (HSV)• Lyme
• Bell’s Palsy• Guillain Barre’ Syndrome
• Congenital• Developmental
• Crying Facies• Syndromic
• Möbius syndrome • CHARGE Syndrome
7

FACIAL PALSY –FEATURES
• Incomplete eye closure
• Corneal ulceration
• Facial droop
• Drooling
• Slurred speech
• Inability to smile
• Gross distortion of facial motion
8

EVALUATION-FUNCTION
• Oral competence • sucking
• blowing
• lip pucker
• smiling
• ADL’s – teeth brushing, feeding
• Eye closure
• Oral aperture • Measure –incisor
• Speech production
9

ACTIVE AND PASSIVE ROM
10

EVALUATION- PSYCHOSOCIAL
• Social isolation
• Self conscious
• Depression
• Anxiety
Lee J, Fung K, Lownie SP, Parnes LS. Assessing Impairment and Disability of Facial Paralysis in Patients With Vestibular Schwannoma. Arch Otolaryngol Head Neck Surg. 2007;133(1):56–60. doi:10.1001/archotol.133.1.5611
*FaCE Scale

EVALUATION- FACIAL MOTION
• SunnyBrook Facial Grading System • Rest• Voluntary Movement • Synkinesis
• Tone
• Other assessment tools• Photos
• No smile• Open smile• Closed smile
• House–Brackmann Scale• Surface EMG
12

13

SAMPLE PHOTO PROGRESSION
14
Date Closed mouth smile
Open mouth smile Eyebrow Raise
8/7/19
10/3/19

TREATMENT
• Surgical • 2 stage
• Lengthening Temporalis Myoplasty
• Non-Surgical • Therapy – to be discussed
• Botox
• NMES
15

2 STAGE FACIAL REANIMATION SURGERY “SMILE SURGERY”
Advantages:
• Spontaneous smile
• You don’t have to bite down to produce a smile
• GOLD STANDARD
Disadvantages:
• Can take up to 2 years to gain movement
• Only improves excursion of the commissure• Doesn’t correct wide
eye, lip elevation and depression

STAGE 1 FACIAL REANIMATION
• Sural nerve
• Harvest with limited incisions
• 2-3 using nerve stripper to minimize scarring


OT INTERVENTION: FOLLOWING STAGE I REANIMATION
Scar Management

OT INTERVENTION:PRIOR TO STAGE II REANIMATION
• Fabrication of Facial Hook Splint

2 STAGE FACIAL REANIMATION
• 9-12 months later
• Free muscle transfer (gracilis)
• Minimize bulkiness by using partial muscle and buccal fat pad debulking
• Stage 2 = Free segmental muscle transfer

2 STAGE FACIAL REANIMATION
• Position muscle to replicate smiling motion with contraction
• Post-operative exercise regimen critical to success

OT INTERVENTION:
AFTER STAGE 2 REANIMATION
• Scar Management
• About 2-3 months post surgery start facial exercises • 1 trial once per week to check for
innervation/movement
• Once movement begins, OT outpatient services 1 time per week. (≈4-6 months post stage II)• Stretching• Strengthening - Surface EMG• Functional tasks to promote movement

2 STAGE FACIAL RE-ANIMATION

2 STAGE FACIAL REANIMATION
Pre Post

[Lengthening of temporalis myoplasty and reanimation of lips. Technical notes]. Labbé D. Ann Chir Plast Esthet. 1997 Feb;42(1):44-7.

INTERNATIONAL FACIAL NERVE SYMPOSIUMLOS ANGELES, CA AUGUST 3-6, 2017
• Title: Mitigating Oral Opening Challenges Following Lengthening Temporalis Myoplasty
• Authors: Tami Konieczny, MS, OTR/L, Daniel M. Mazzaferro MBA, Anne-Ashley Field, MOTR/L, Ari Wes, BA, Scott P. Bartlett, MD, Phuong D. Nguyen, MD
• Introduction: Mouth opening following lengthening temporalis myoplasty (LTM) for facial reanimation may be challenging, leading to decreased oral intake and delayed muscle rehabilitation. We hypothesize that using a jaw motion rehabilitation device (TheraBite) postoperatively improves facial mobility and interincisal distance.
• Methods: A retrospective review of all patients who underwent LTM for facial reanimation at a single institution was performed. Postoperative maximal mouth opening was measured from maxillary central incisor to the mandibular central incisor. Surface EMG (sEMG) assessed muscle activity. A multilevel mixed-effects regression analysis was performed, controlling for age, sex, surgeon, and postoperative monthly treatment intervals.
• Results: Five subjects, 2 unilateral and 3 bilateral facial palsy patients, underwent LTM. Four of five patients (80%) demonstrated postoperative oral tightness. Three of five (60%) required use of TheraBite to improve oral excursion after failing traditional massage therapy. Average age at time of surgery was 14.3 ± 5.7 years. Patients started TheraBitetreatment on average 84.7 days after initial facial reanimation procedure. Univariate analysis revealed a significant difference with TheraBite use versus no use in sEMG (90.2 ± 33.6mV vs. 56.4 ± 32.3mV, p=0.0003) and interincisaldistance (23.8 ± 3.4mm vs. 20.6 ± 3.5mm vs., p=0.027). Mixed regression showed TheraBite use to have a sEMG of 7.79 ±9.53mV greater than without use (p=0.271); interincisal distance was 1.0 ± 1.1mm greater with TheraBite use (p=0.377). Critically significant increase of sEMG occurred in the fourth month (42.1±18.7mV, p=0.024) and interincisal distance in the third month (5.5 ± 1.7mm, p=0.001)
• Conclusion: Univariate analysis demonstrated sEMG and interincisal improvement with TheraBite use following LTM. There appeared to be a significant rise in sEMG of the temporalis muscle approximately one month after TheraBite use. Future studies will need to investigate implementation of TheraBite earlier in postoperative course and prior to surgery.

LENGTHENING TEMPORALIS MYOPLASTY
Pre Post

29
OT EVALUATION AND TREATMENT
29


ASSESSMENT (PHOTO)
• EXAMINE THE FACE AT REST
• EYE • WIDE
• NARROW
• NORMAL
• CHEEK (NASOLABIAL FOLD)
• NORMAL
• ABSENT
• LESS PRONOUNCED
• MORE PRONOUNCED
• MOUTH (COMMISSURE)
• NORMAL
• CORNER DROPPED
• CORNER PULLED UP/OUT

NO SMILE – RESTING SYMMETRY
1. Which side?2. Eye?3. Cheek?4. Mouth ?
1. Left 2. Wide (1)3. Less pronounced (1)4. Normal (0)
2 x 5 = 10

FOREHEAD WRINKLE
Score? Unable to initiate the movementGross asymmetry (1)

GENTLE EYE CLOSURE
Score? Initiates slight movementSevere asymmetry (2)

SNARL
Score?Initiates slight movementSevere asymmetry (2)

OPEN MOUTH SMILE
Score?Initiates slight movementSevere asymmetry (2)

CLOSED MOUTH SMILE
Score? Not included in the SunnybrookNote improved symmetry

PUCKER
Score? Movement almost complete Mild asymmetry (4)

SUNNYBROOK SCORING:
• RESTING SYMMETRY:• TOTAL (2) X 5 =10
• SYMMETRY OF VOLUNTARY MOVEMENT:• TOTAL (11) X 4 = 44
• SYNKINESIS • 0
• VOL MOVEMENT SCORE (44) – RESTING SYMMETRY SCORE (10) – SYNK SCORE (0)= 34

TREATMENT:
• EARLY INTERVENTION MAY PREVENT SURGERY
• USE IT OR LOSE IT
• AVOID MUSCLE ATROPHY
• CONSIDER sEMG
• MAINTAIN ROM (STRECHES AND MASSAGES)

EYELID STRETCHES:
• Don’t pull on the eyelid
• Grasp eyelashes and gently close the eye
• Hold for 20-30 seconds
• Try to volitionally close the eye
• Repeat

CHEEK STRETCH:
42
Curiosity of Queen Victoria Hospital, FTS-UK

THERAPY TREATMENT PROGRESSION
1. Initiate active movement
2. Strengthen the muscle
3. Increase endurance of the muscle• Sustain muscle contraction
4. Refine movement/achieve symmetry• Proprioception



FACIAL EXERCISES EXAMPLES:
• Open Mouth Smile- Hold for 5 seconds. Repeat __ times
• Closed Mouth Smile- Hold for 5 seconds. Repeat __ times
• Pucker- Tight and symmetrical
• Lip popping- Tight and loud
• Lip depression
• Eyebrow elevation
• Alternating left and right sided smiles
• “Mirror Therapy”- (to be discussed)

FACIAL EXERCISES

BIOMETRIC-BIOFEEDBACK

FUNCTIONAL EXERCISES

PROPRIOCEPTION RETRAINING
1. Perform symmetrical smile while looking in the mirror
2. Look away 3. Stop smiling4. Smile again5. Look back in the mirror
and check for symmetry 6. Trains the person to feel
what symmetry feels like without visual feedback

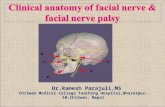
CLINICAL CASE: PRE AND POST THERAPY
2 weeks post AVM2 weeks after initiating facial motion excercises
AVM of Left MCA

CLINICAL CASE: PRE AND POST THERAPY
2 year old s/p blunt head trauma, left temporal bone fracture and complete facial palsy
10 days post-injury• No evidence of nerve
activity
2 months post injury• Partial spontaneous
recovery

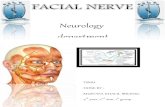
CLINICAL CASE: PRE AND POST THERAPY
Ramsey Hunt Syndrome

CLINICAL CASE: PRE AND POST THERAPY
54
2/22/2019 4/4/2019
Sclerotherapy for an ear AVM resulting in facial nerve injury

DOCUMENTATION
• PHOTOS
• SUNNYBROOK FACIAL GRADING
• CONSIDER – MEASURING MOUTH OPENING
• FACIAL MOTION GOAL (example):
• Pt. will perform an open mouth smile with moderate asymmetry as measured by the Sunnybrook Facial Grading System
• PROVIDE HEP

GROUP CASE STUDY:
58 year female with no significant medical history develops sudden onset of left sided facial paralysis. She was seen initially in the ED and prescribed antibiotics. She then followed up with her PCP regularly for the next 2 weeks but without improvement. She tested negative for Lyme and HSV. Referred to OT 1 month following onset of symptoms. Incomplete eye closure and decreased spontaneous blink noted on exam.
56
Open mouth smile Closed mouth smile
Snarl

CASE STUDY
57
Evaluation: ??
• SunnyBrook
• Functional Assessment
• Photos
Interventions: ??
• Massage
• Eyelid stretches
• Therapeutic exercises
• Functional Activities
Recommendations:??
• Ophthalmology
• HEP

58

MIRROR THERAPY:
• https://www.youtube.com/watch?v=WMfnLZWWW7U
59

NEUROMUSCULAR ELECTRICAL STIMULATION (NMES)
• Controversial • Causes synkinesis???

61