EYE & EARS & MOUTHS, OH MY! - American Academy of...
38
2/23/2017 1 EYE & EARS & MOUTHS, OH MY! FROM BASIC TO ADVANCED HEENT PROCEDURES USED IN PRIMARY CARE AND EMERGENCY SETTINGS Dian Evans, PhD, FNP-BC, ENP-BC, FAANP Michael D. Gooch, DNP, ACNP-BC, FNP-BC, ENP-C Chris Gisness, MSN, FNP-BC, FAEN Paula Tucker, DNP, FNP-BC, ENP Disclosure of Commercial Relationships Nature of Relationship Name of Commercial Entity Advisory Board None Consultant None Employee None Board Member None Shareholder None Speaker’s Bureau None Patents None Other Relationships None
Transcript of EYE & EARS & MOUTHS, OH MY! - American Academy of...

2/23/2017
1
EYE & EARS & MOUTHS, OH MY!FROM BASIC TO ADVANCED HEENT PROCEDURES USED IN PRIMARY CARE AND EMERGENCY SETTINGS
Dian Evans, PhD, FNP-BC, ENP-BC, FAANP
Michael D. Gooch, DNP, ACNP-BC, FNP-BC, ENP-C
Chris Gisness, MSN, FNP-BC, FAEN
Paula Tucker, DNP, FNP-BC, ENP
Disclosure of Commercial Relationships
Nature of Relationship Name of Commercial EntityAdvisory Board NoneConsultant NoneEmployee NoneBoard Member NoneShareholder NoneSpeaker’s Bureau NonePatents NoneOther Relationships None
2/23/2017
2
Objectives
• To review basic procedures used in assessing and treating common HEENT including dental complaints
• To understand the indications and contraindications for performing HEENT procedures
• To practice performing basic HEENT procedural skills including dental and oral anesthesia
Eye Examination Basics
• Use a systematic approach• Explain the exam to the patient• Wash hands and apply gloves• Visual acuity• Direct inspection• Eye movements, and if appropriate, visual fields• Ophthalmoscope• Using adjunctive methods (Woods Lamp/Slit Lamp)• Flourescein staining• TonoPen for pressure assessment

2/23/2017
3
Visual Acuity
• Vital sign of the eye
• Measured using the Snellen wall or pocket chart
• Pin hole test
• First part of every eye exam
• **Exceptions include:• Globe rupture, penetrating foreign body or chemical splash
Slit lamp and Wood’s light
• Used to assess corneal defects
• Slit lamp is standard of care in emergency settings
http://www.ophthobook.com/videos/slit-lamp-exam-video

2/23/2017
4
Foreign bodies to eye
http://emedicine.medscape.com/article/82717-overview
Penetrating Foreign Body
• Consider other trauma
• Protect from eye movement
• CT scan
http://www.medscape.com/viewarticle/560880_5

2/23/2017
5
“Tear Drop” Pupil
Penetrating injury
http://www.eyecasualty.co.uk/maincontent1/openeyetrauma.html
Seidel Test
Indicative of globe rupture
http://coreem.net/core/traumatic-ocular-injuries/
2/23/2017
6
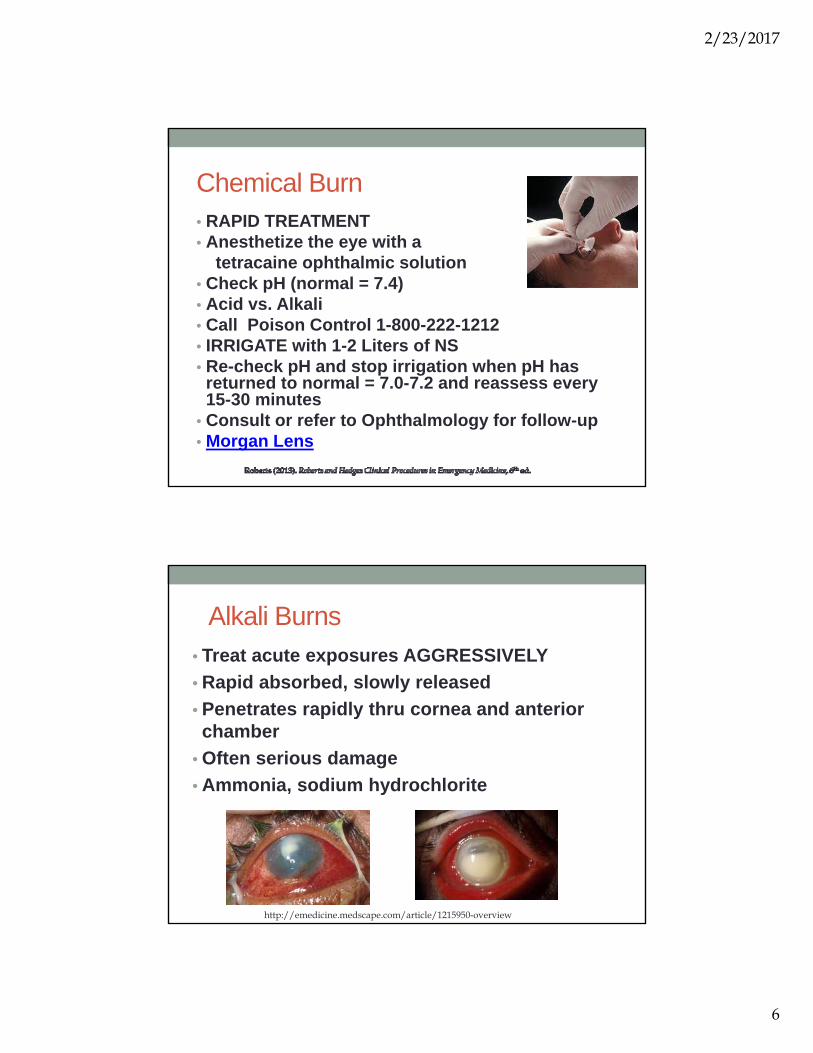
Chemical Burn• RAPID TREATMENT• Anesthetize the eye with a
tetracaine ophthalmic solution• Check pH (normal = 7.4)• Acid vs. Alkali• Call Poison Control 1-800-222-1212• IRRIGATE with 1-2 Liters of NS• Re-check pH and stop irrigation when pH has returned to normal = 7.0-7.2 and reassess every 15-30 minutes
• Consult or refer to Ophthalmology for follow-up• Morgan Lens
Alkali Burns• Treat acute exposures AGGRESSIVELY
• Rapid absorbed, slowly released
• Penetrates rapidly thru cornea and anterior chamber
• Often serious damage
• Ammonia, sodium hydrochlorite
http://emedicine.medscape.com/article/1215950-overview

2/23/2017
7
Acid Burn
• Looks bad
• Coagulation
• Heals quickly
• Battery acid
www.onjoph.com
External Examination
• General inspection periorbital region, eyelids, globe position, lid margins
• Observe for erythema, crusting, nodules, lashes, ulcerations
• Evert lids to assess for foreign bodies and lesions
https://www.nlm.nih.gov/medlineplus/ency/imagepages/19662.htm

2/23/2017
8
Chalazion
• Firm, well-demarcated cystic nodule just below lid margin
• Obstructed tarsal gland
• Symptom free- non-tender
• Warm compresses
• Refer for triamcinolone injection
Pterygium vs. Pinguecula
Noncancerous fleshy conjunctival growths
http://melbourneeyecentre.com.au/pterygium/ http://www.eyedolatryblog.com/2012/11/theres-bump-on-my-eye-part-1-pinguecula.html
2/23/2017
9
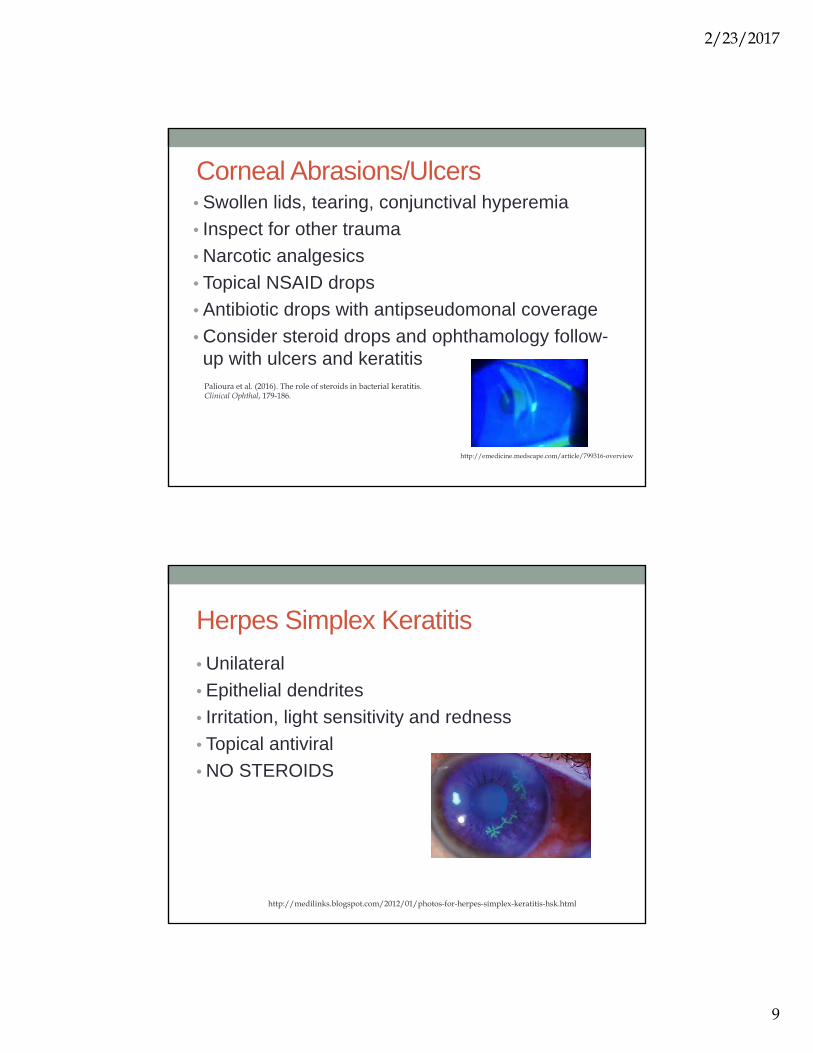
Corneal Abrasions/Ulcers• Swollen lids, tearing, conjunctival hyperemia
• Inspect for other trauma
• Narcotic analgesics
• Topical NSAID drops
• Antibiotic drops with antipseudomonal coverage
• Consider steroid drops and ophthamology follow-up with ulcers and keratitisPalioura et al. (2016). The role of steroids in bacterial keratitis. Clinical Ophthal, 179-186.
http://emedicine.medscape.com/article/799316-overview
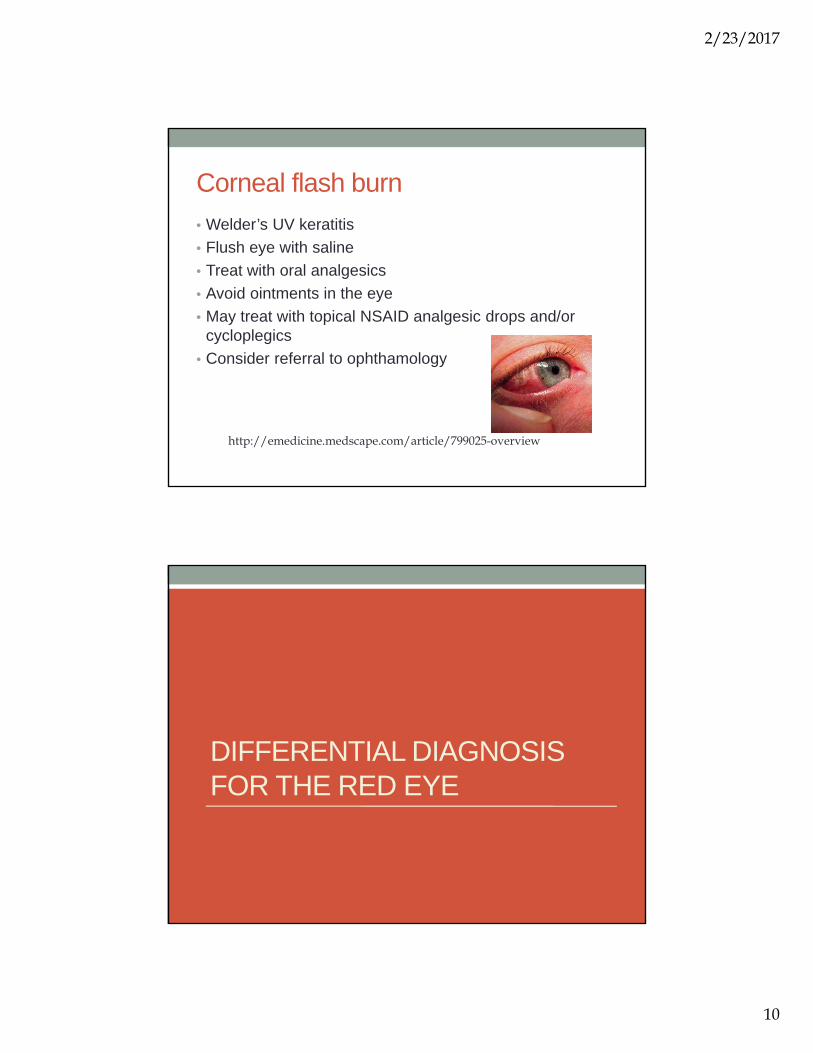
Herpes Simplex Keratitis
• Unilateral
• Epithelial dendrites
• Irritation, light sensitivity and redness
• Topical antiviral
• NO STEROIDS
http://medilinks.blogspot.com/2012/01/photos-for-herpes-simplex-keratitis-hsk.html
2/23/2017
10
Corneal flash burn
• Welder’s UV keratitis
• Flush eye with saline
• Treat with oral analgesics
• Avoid ointments in the eye
• May treat with topical NSAID analgesic drops and/or cycloplegics
• Consider referral to ophthamology
http://emedicine.medscape.com/article/799025-overview
DIFFERENTIAL DIAGNOSIS FOR THE RED EYE
2/23/2017
11
RED EYE
• Painful red eye: conjunctivitis, iritis, uveitis, episcleritis, narrow angle glaucoma
• Acute, narrow angle (closed angle) glaucoma is a medical emergency and if missed can cause permanent vision loss
• Use tonometry to measure
ocular pressure
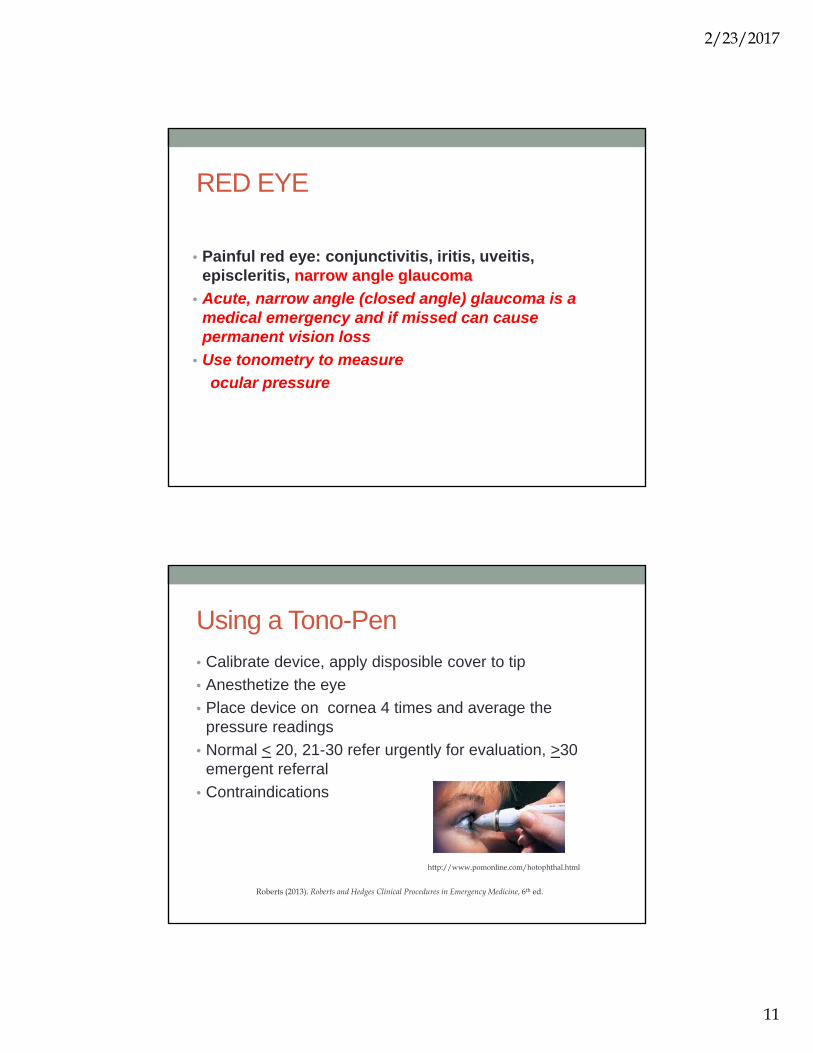
Using a Tono-Pen
• Calibrate device, apply disposible cover to tip
• Anesthetize the eye
• Place device on cornea 4 times and average the pressure readings
• Normal < 20, 21-30 refer urgently for evaluation, >30 emergent referral
• Contraindications
Roberts (2013). Roberts and Hedges Clinical Procedures in Emergency Medicine, 6th ed.
http://www.pomonline.com/hotophthal.html

2/23/2017
12
Using an ICARE Tonometer
• No need to anesthetize the eye
• Obtain three readings and the device provides the average
https://www.google.com/search?q=icare+tonometer&rlz=1C1ASUM_enUS693US693&espv=2&biw=1920&bih=974&source=lnms&tbm=isch&sa=X&ved=0ahUKEwjS-9-Pv-zRAhVr2oMKHe9mB7IQ_AUICCgD#imgrc=y1paIKMwlwKkSM%3A
Subconjunctival Hemorrhage
• Acute, dense, blood red discoloration
• Blunt trauma, Valsalva’s
• REASSURANCE
• Examine for other trauma
medlibes.com/entry/subconjunctival-hemorrhage

2/23/2017
13
Hyphema
• Layering of red cells in the anterior chamber
• Look for foreign bodies
• Palpate orbital bones for fracture
• Admit if > 1/3 or if increased
intraocular pressure
https://www.optocase.com/archives/hyphema.aspx
Charting an eye procedure note
• Include:– Visual acuity
– Direct eye inspection, PERRLA, extraocular movements
– Funduscopic findings
– Medication administration
– Irrigation or any procedure used in assessment or treatment of condition
– Exam finding after flourescein staining
– Patient’s condition at the end of the exam and procedure

2/23/2017
14
POINTS TO REMEMBER
• Do not patch eyes except to immobilize in cases of penetrating injury to opposite eye
–Patches do not reduce pain or improve healing rates for corneal abrasions (2009, Cochrane Review)Accessed 8/29/2013 @ http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD004764.pub2/abstract=
• Check visual acuity first except for chemical exposures or penetrating globe injuries
• Consider use of anesthetic eye drops for 24 hours to reduce pain in reliable patients
• Waldman, Densie & Herbison. (2014). Academic Emergency Medicine, 374-382.
PROCEDURES FOR EAR PROBLEMSAnesthesia, foreign body removal, ear wick insertion, wound repair
2/23/2017
15
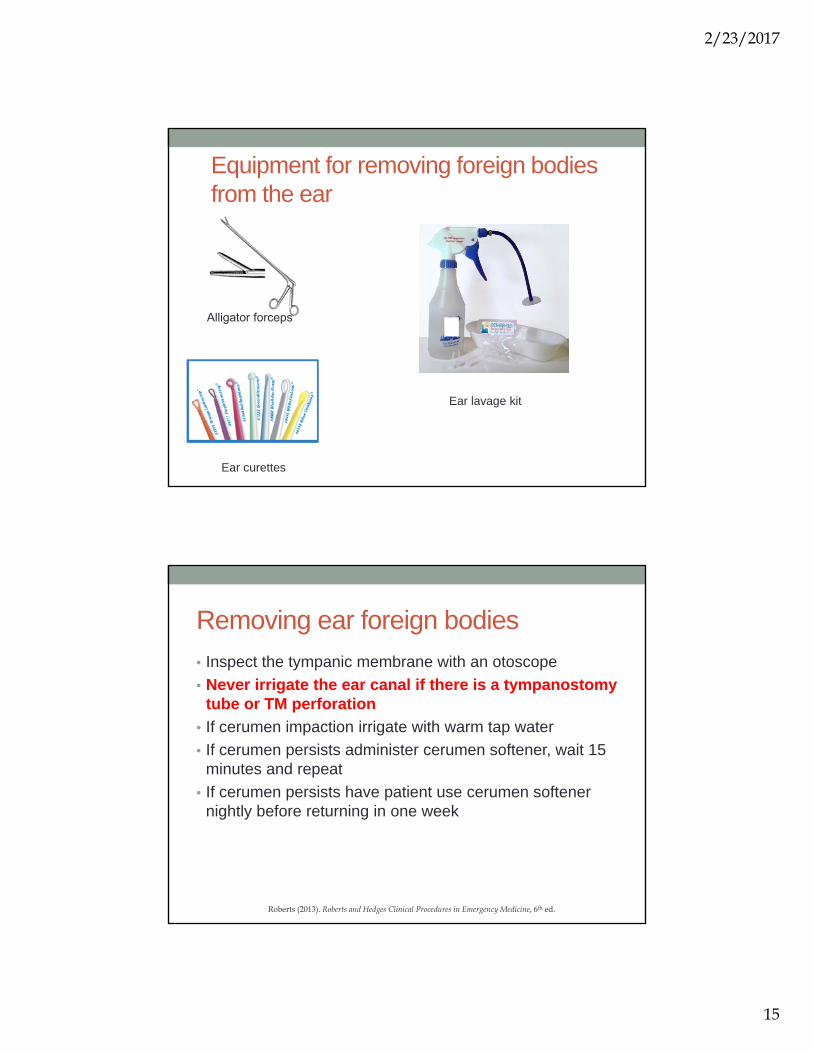
Equipment for removing foreign bodies from the ear
Alligator forceps
Ear curettes
Ear lavage kit
Removing ear foreign bodies
• Inspect the tympanic membrane with an otoscope
• Never irrigate the ear canal if there is a tympanostomytube or TM perforation
• If cerumen impaction irrigate with warm tap water
• If cerumen persists administer cerumen softener, wait 15 minutes and repeat
• If cerumen persists have patient use cerumen softener nightly before returning in one week
Roberts (2013). Roberts and Hedges Clinical Procedures in Emergency Medicine, 6th ed.
2/23/2017
16
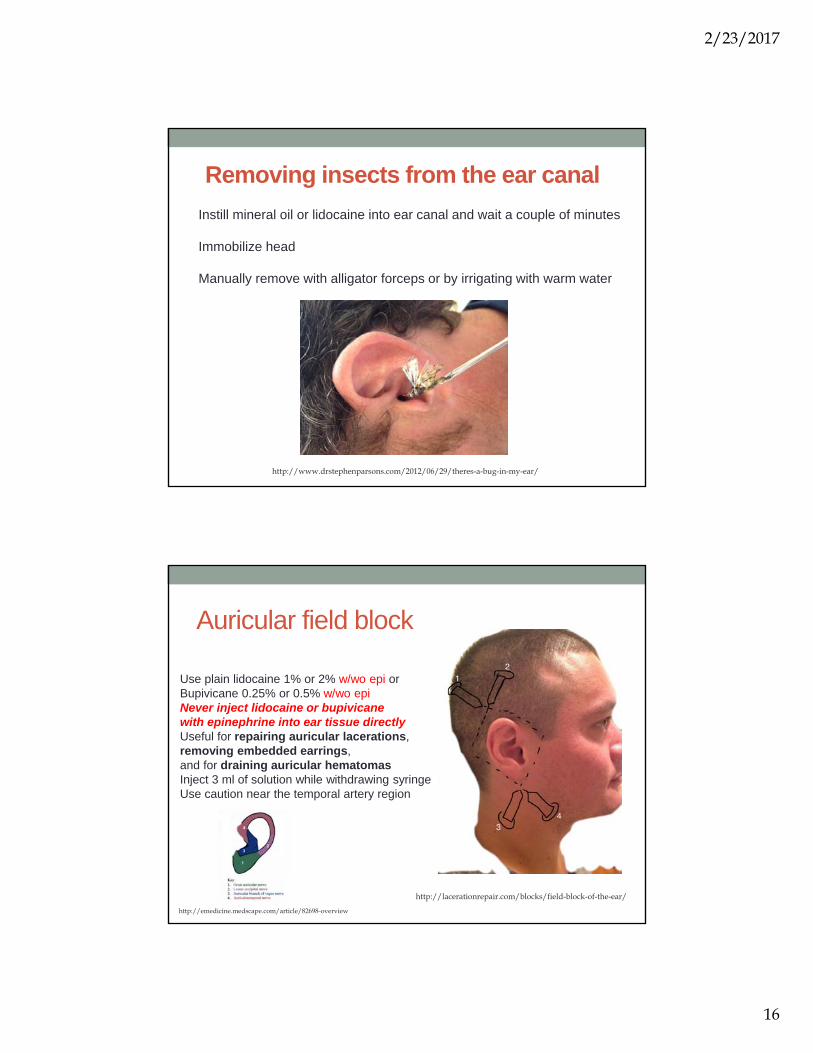
Removing insects from the ear canal
Instill mineral oil or lidocaine into ear canal and wait a couple of minutes
Immobilize head
Manually remove with alligator forceps or by irrigating with warm water
http://www.drstephenparsons.com/2012/06/29/theres-a-bug-in-my-ear/
Auricular field block
Use plain lidocaine 1% or 2% w/wo epi or Bupivicane 0.25% or 0.5% w/wo epi Never inject lidocaine or bupivicanewith epinephrine into ear tissue directlyUseful for repairing auricular lacerations, removing embedded earrings,and for draining auricular hematomasInject 3 ml of solution while withdrawing syringeUse caution near the temporal artery region
http://lacerationrepair.com/blocks/field-block-of-the-ear/
http://emedicine.medscape.com/article/82698-overview

2/23/2017
17
Ear laceration technique
Trott, A. (2012). Wounds and lacerations: Emergency care and closure. (4th ed.). Philadelphia: Elsevier Saunders.
Auricular Hematoma
Drain to prevent permanent deformity to cartilage
Start with auricular field blockPrep skin with Betadine®Incise with #11 blade scalpelDrain bloodApply compression dressingRecheck patient in 24 hours
Hematoma Cartilage deformity“Cauliflower ear”
http://www.myfacesurgeon.com/hab-home/hab-cauliflower-ear-music-audiologist/
2/23/2017
18
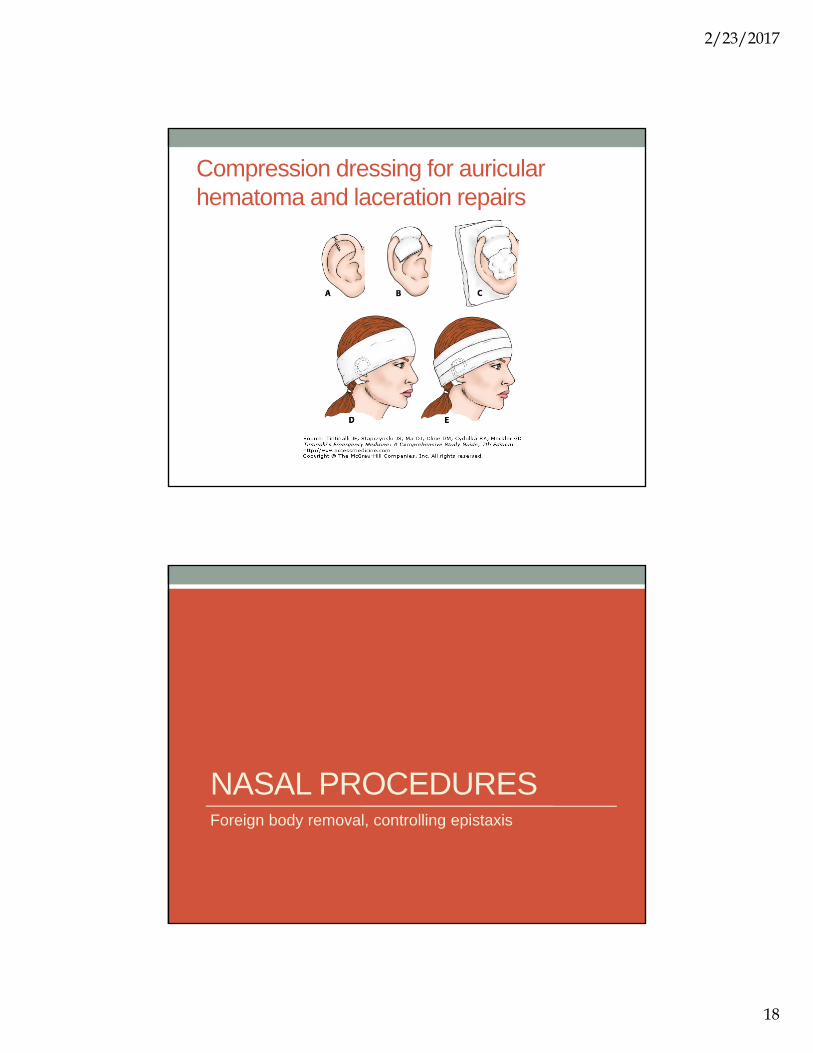
Compression dressing for auricular hematoma and laceration repairs
NASAL PROCEDURESForeign body removal, controlling epistaxis

2/23/2017
19
Nasal foreign bodies
Any foul smelling drainage from a child’s nose is a foreign body until proven otherwise
Don’t forget to look in both nostrils and in both ears too
http://www.youtube.com/watch?v=rQpIOdJrYIc
http://momwithastethoscope.files.wordpress.com
Devices for removal of nasal FB
eMedscape.com
2/23/2017
20
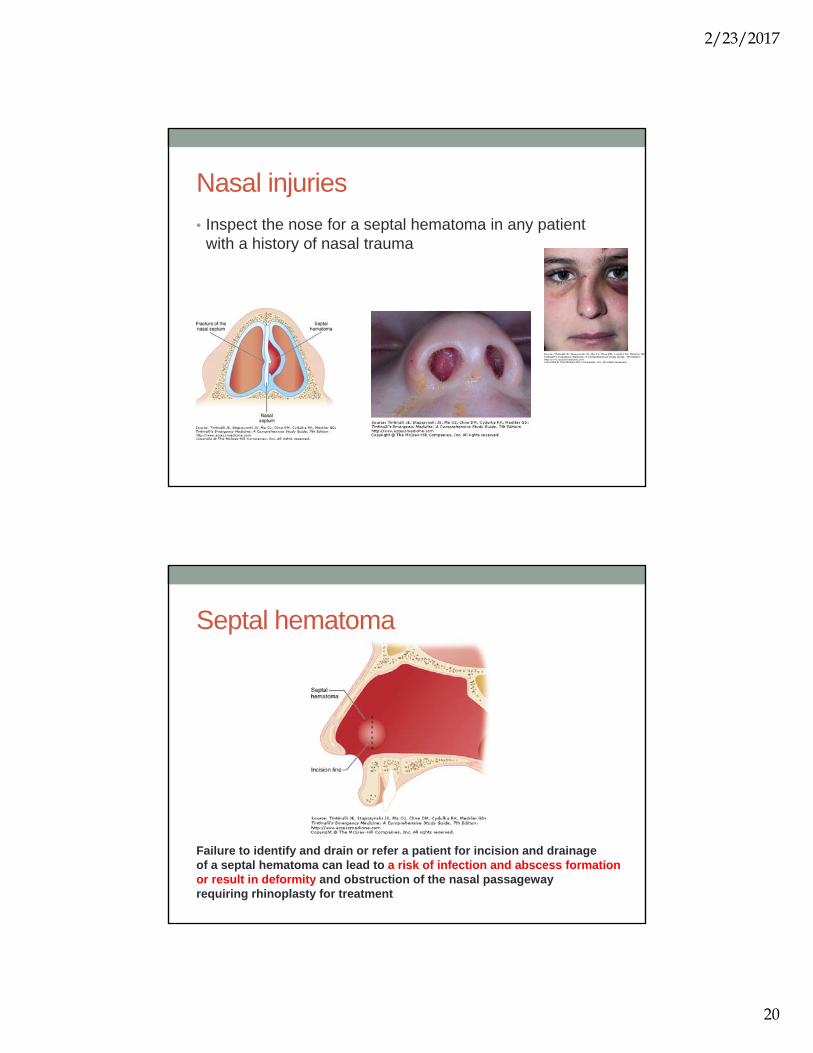
Nasal injuries
• Inspect the nose for a septal hematoma in any patient with a history of nasal trauma
Septal hematoma
Failure to identify and drain or refer a patient for incision and drainage of a septal hematoma can lead to a risk of infection and abscess formation or result in deformity and obstruction of the nasal passageway requiring rhinoplasty for treatment

2/23/2017
21
Incision, drainage and packing procedure for a septal hematoma
From Tintinalli’s Emergency Medicine Chapter 239. Accessed fromhttp://www.accessmedicine.com.proxy.library.emory.edu/content.aspx?aID=6388137
Epistaxis
Epistaxis can result from either anterior or posterior arterial bleedsMost cases respond to direct manual pressure Position patient in “sniffing position”
Squeeze nostrils shut and maintain pressure for 15 minutesIf bleeding persists refer for nasal packing

2/23/2017
22
Epistaxis
• Which side is bleeding?
• Which side was bleeding initially?
• What is the estimated amount of blood loss?
• Is it recurrent?
• Is it in the pharynx?
• Has any trauma recently occurred?
• Are symptoms of hypovolemia present?
• What are the patient’s past medical history and current medications (eg, aspirin, warfarin)?
Anterior/Posterior Bleeds
http://emedicine.medscape.com/article/80545-overview
Anterior bleeds
Posterior bleeds-admit for observation after controlof epistaxis due to risk of bradyarrhythmias
https://www.youtube.com/watch?v=U-i46nghGr0

2/23/2017
23
Nasal Packing for Epistaxis
• Anesthetize the nostril with cotton balls soaked in 2% Lidocaine with epinephrine or topical cocaine
• Administer a topical nasal decongestant
• Insert packing material
Kucik & Clenney (2005). American Family Physician, Jan 15;71(2):305-311
ORAL AND DENTAL PROCEDURESNerve blocks, dental procedures, incision and drainage of peritonsillar abscess

2/23/2017
24
Adult Tooth Chart
Memorize tooth numbers 8,9 and 24, 25 that correspond to the upper and lower central incisors
http://www.buzzle.com/articles/dental-charts-to-understand-tooth-numbering-system.html
Apical abscesses requiring an I&D
Pointing
http://www.intelligentdental.com/2012/01/20/dangers-of-an-abscessed-tooth-part-1/
2/23/2017
25
Abscess Treatment
• Nerve block
• I&D with # 11 blade
• Suction
• Pen VK 500mg QID x 10 days, Keflex 500 mg TID or Clindamycin 300mg QID x 10 days $$$
• Dental referral for definitive treatment
• NSAID for analgesia
Dental Emergencies
• Avulsed permanent teeth must be immediately re-implanted
• Facial cellulitis can rapidly worsen
• Ludwig’s Angina is a potential airway emergency
2/23/2017
26
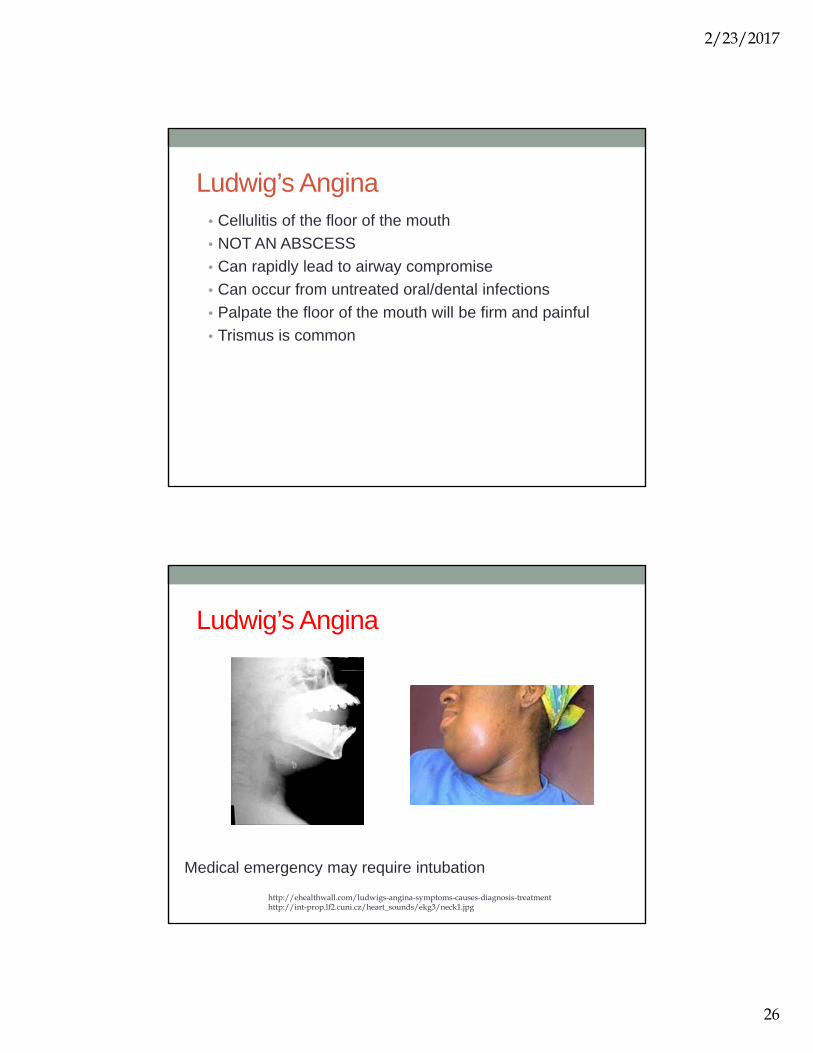
Ludwig’s Angina• Cellulitis of the floor of the mouth
• NOT AN ABSCESS
• Can rapidly lead to airway compromise
• Can occur from untreated oral/dental infections
• Palpate the floor of the mouth will be firm and painful
• Trismus is common
Ludwig’s Angina
Medical emergency may require intubation
http://ehealthwall.com/ludwigs-angina-symptoms-causes-diagnosis-treatmenthttp://int-prop.lf2.cuni.cz/heart_sounds/ekg3/neck1.jpg

2/23/2017
27
Types of Anesthesia• Topical
• LET (lidocaine, epinephrine, and tetracaine)• TAC (tetracaine, adrenaline, and cocaine)• Emla• Viscous xylocaine
• Injectable• Bupivacaine 0.25% or 0.5% (Marcaine, Sensorcaine)
• Max. adult dose = 175 mg• Onset 5-10 min. Duration 1-2.5 hrs• If using for a regional dental block; Onset 7-21 min. Duration 2-6 hrs
• Lidocaine (Xylocaine) 1% or 2% with/without epinephrine• Maximum adult dose = 300 mg• Can be buffered by adding 1 mL of sodium bicarb to 9 mL of anesthetic• Onset 3-5 min. Duration: 30-60 minutes • If using for regional dental block; Onset 5-10 min. Duration 1-1.5 hrs
If allergic to any of these agents mix 50mg/1mL of diphenhydramine solution into 4 mL of NS and use for local infiltration
Jones, T. (2012). Wound care. In Current Diagnosis and Treatment in Emergency Medicine.Retrieved from http://www.accessmedicine.com.proxy.library.emory.edu/content.aspx?aID=55752201
Inferior alveolar mandibular nerve block
An inferior alveolar nerve block anesthetizes the following structures:Mandibular teeth to the midlineThe anterior two thirds of the tongueThe floor of the oral cavity

2/23/2017
28
Maxillary dental blocks
Maxillary molars: Injection is given at the region of the second molar.
Maxillary premolars: Injection is given at the region of the second premolar.
Maxillary canine and incisors: Injection can be given above the roots of the anterior teeth or via an infraorbital nerve block.
Unlike the inferior alveolar nerve block that blocks all the teeth along one sidemaxillary teeth are innervated by several nerves and must be blocked separately.
Infraorbital Nerve Block
Best for repairing oral lacerations of upper lip and blocking the anterior upper teeth

2/23/2017
29
Mental Block
Best for repairing oral lacerations around the lower lip or anesthetizing the anterior lower teeth
Oral Trauma and Emergencies
• Palpate TMJ, orbits, sinus, check in nose for septal hematoma
• Feel each tooth for looseness, fractures, is there any bleeding?
• Does the jaw line up normally, can pt open and close normally?
• Tongue depressor can be used to determine jaw strength

2/23/2017
30
Oral Injuries
http://www.utahmountainbiking.com/firstaid/mouthcut.htm
http://ohiodentalclinics.com/curricula/care/mod4_4_4.html
http://lifeinthefastlane.com/quiz-trauma-017/
Ellis Classification of Tooth Fractures

2/23/2017
31
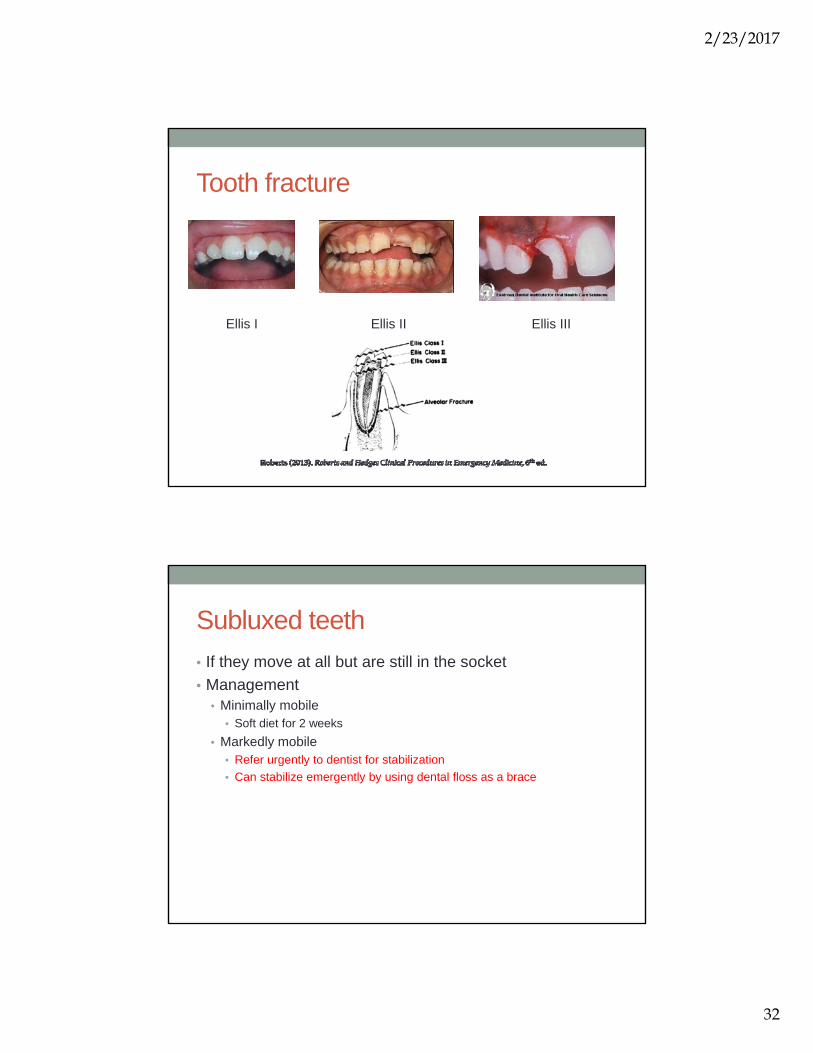
Tooth fractures
• Ellis I (Enamel involved)• Refer to dentist nonurgently for filing and cosmetic repair (file with
emory board)
• Ellis II (Dentin involved)• Cover injured tooth with composite or wax• See dentist urgently (within 24 hours)• Infection can spread quickly through the dentin layer into the pulp
Tooth fractures
• Ellis III (Pulp involved)• Differentiate from II’s by presence of pink blush or blood
• See dentist immediately
• Cover with moist gauze and dry foil
• Provide adequate analgesia
• Consider root involvement (Dx with x-ray)
2/23/2017
32
Tooth fracture
Ellis I Ellis II Ellis III
Subluxed teeth
• If they move at all but are still in the socket
• Management• Minimally mobile
• Soft diet for 2 weeks
• Markedly mobile• Refer urgently to dentist for stabilization
• Can stabilize emergently by using dental floss as a brace
2/23/2017
33
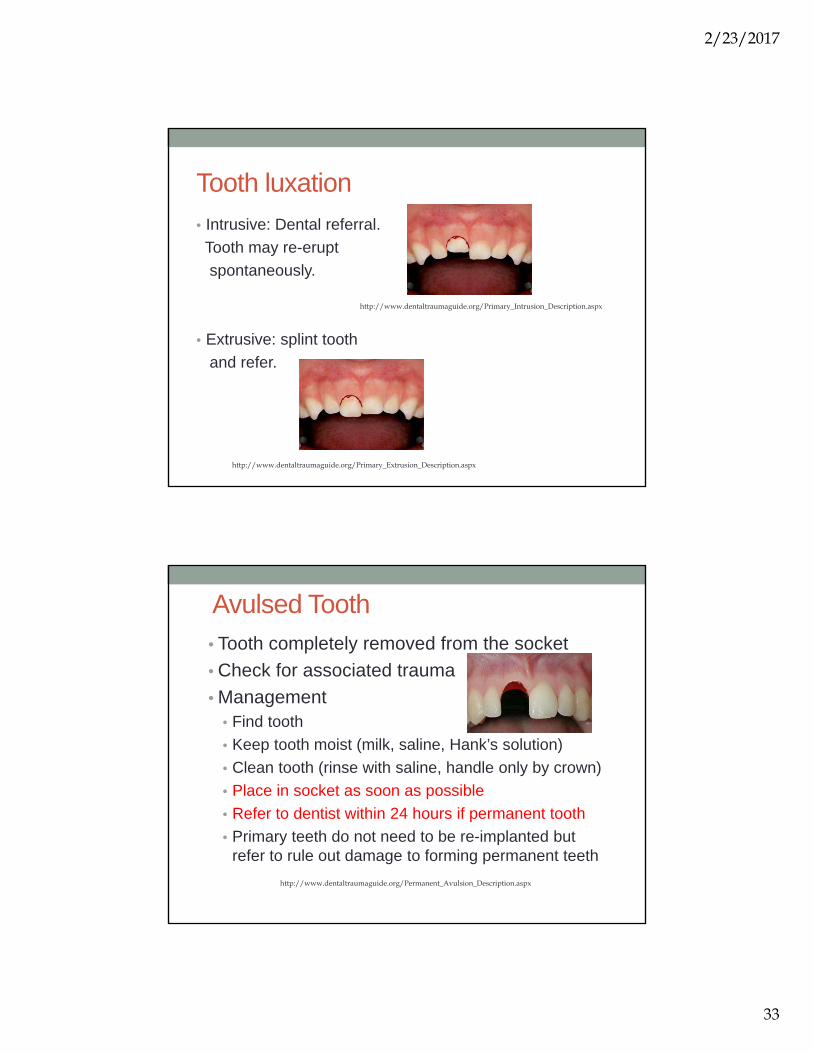
Tooth luxation
• Intrusive: Dental referral.
Tooth may re-erupt
spontaneously.
• Extrusive: splint tooth
and refer.
http://www.dentaltraumaguide.org/Primary_Intrusion_Description.aspx
http://www.dentaltraumaguide.org/Primary_Extrusion_Description.aspx
Avulsed Tooth• Tooth completely removed from the socket
• Check for associated trauma
• Management• Find tooth
• Keep tooth moist (milk, saline, Hank’s solution)
• Clean tooth (rinse with saline, handle only by crown)
• Place in socket as soon as possible
• Refer to dentist within 24 hours if permanent tooth
• Primary teeth do not need to be re-implanted but refer to rule out damage to forming permanent teeth
http://www.dentaltraumaguide.org/Permanent_Avulsion_Description.aspx
2/23/2017
34
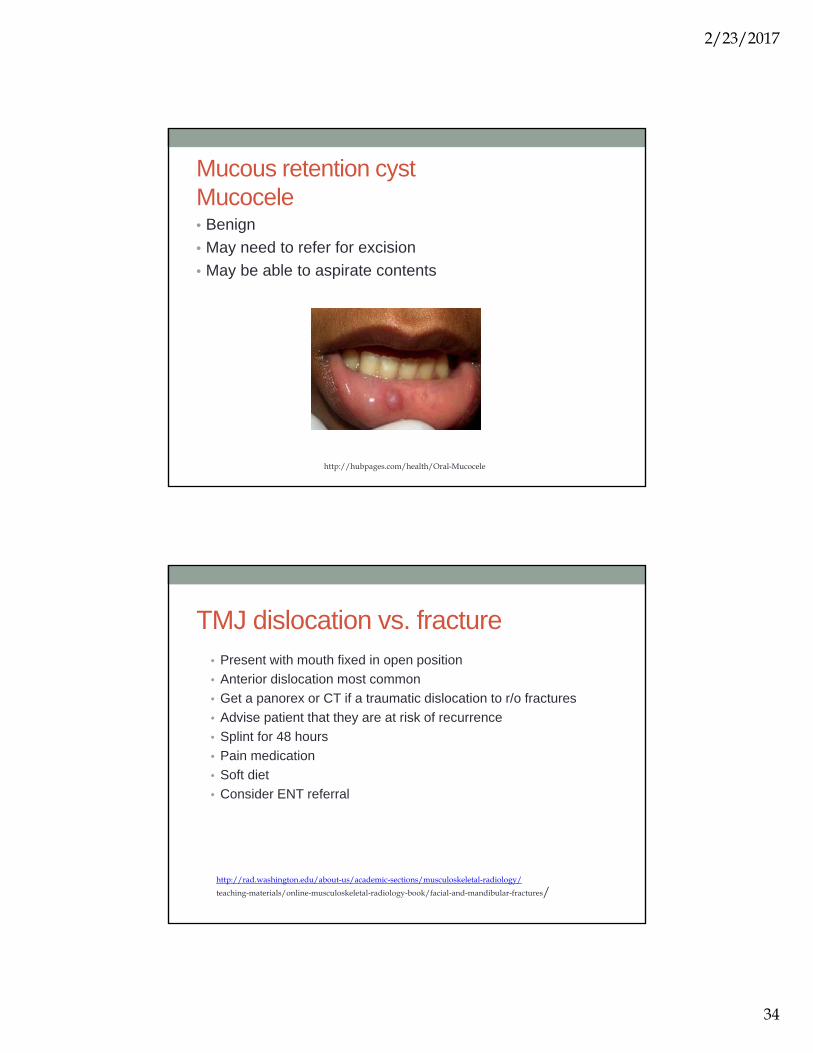
Mucous retention cystMucocele• Benign
• May need to refer for excision
• May be able to aspirate contents
http://hubpages.com/health/Oral-Mucocele
TMJ dislocation vs. fracture• Present with mouth fixed in open position
• Anterior dislocation most common
• Get a panorex or CT if a traumatic dislocation to r/o fractures
• Advise patient that they are at risk of recurrence
• Splint for 48 hours
• Pain medication
• Soft diet
• Consider ENT referral
http://rad.washington.edu/about-us/academic-sections/musculoskeletal-radiology/
teaching-materials/online-musculoskeletal-radiology-book/facial-and-mandibular-fractures/
2/23/2017
35
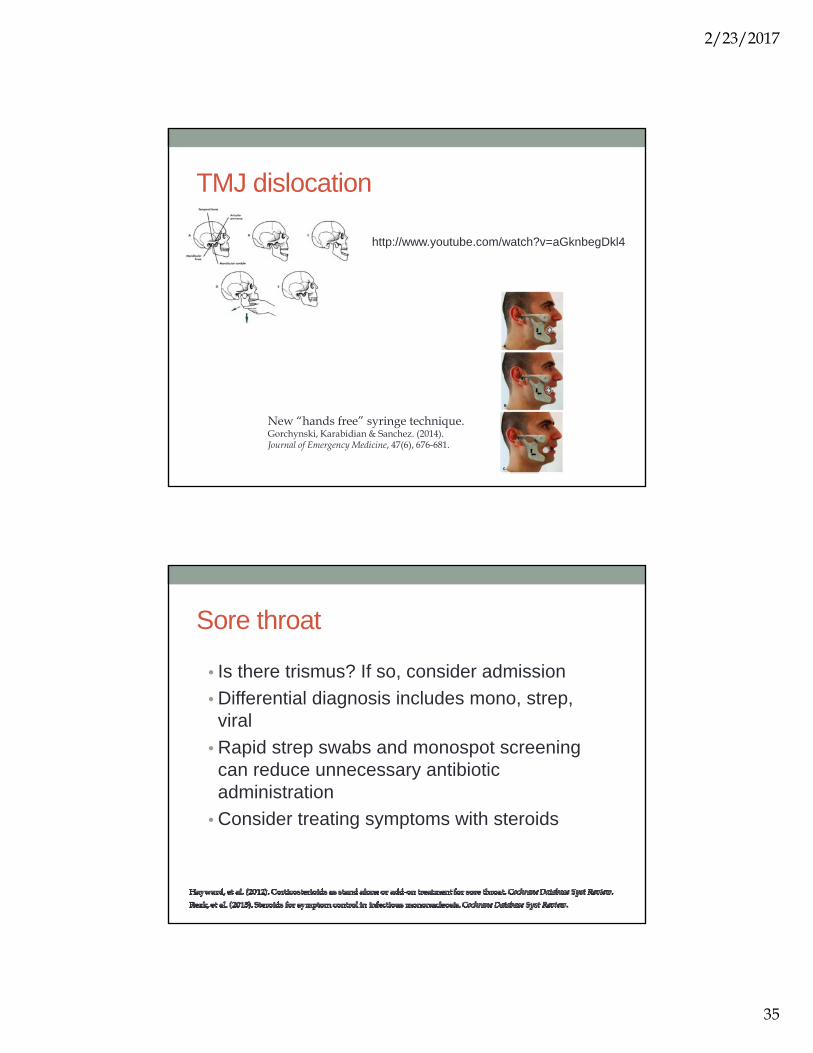
TMJ dislocation
http://www.youtube.com/watch?v=aGknbegDkl4
New “hands free” syringe technique.Gorchynski, Karabidian & Sanchez. (2014). Journal of Emergency Medicine, 47(6), 676-681.
Sore throat
• Is there trismus? If so, consider admission
• Differential diagnosis includes mono, strep, viral
• Rapid strep swabs and monospot screening can reduce unnecessary antibiotic administration
• Consider treating symptoms with steroids

2/23/2017
36
Consider Fusobacterium necrophorum
• Adolescents & young adults• 10% incidence (pharyngitis)• Treat pharyngitis with Penicillin, Cephalosporins or
Metronidazole
• Associated with Lemierre syndrome• Avoid macrolides
• Can lead to bacteremia and thrombophlebitis of the internal jugular and septic emboli• Blood cultures can aid in diagnosis• Consider vascular ultrasound of neck• Admit for anticoagulation and IV antibiotics
Centor, R. (2009). Ann Intern Med. 151:812-815.Prakashchandra, S. et al. (2015). Journal of Clinical and Diagnostic Research, Vol-9(6): TD03-TD04
Incision and drainage or needle aspiration of a peritonsillar abscess• Provide suction to protect airway
• Risks include carotid artery incision with I&D
• Administer analgesia and topical anesthetic to pharynx
• Apply a needle guard on the syringe to avoid deep penetration and risk of carotid injury
https://www.youtube.com/watch?v=I5W27zV-dwI
http://www.acep.org/Clinical---Practice-Management/Tricks-of-the-Trade---Say-%E2%80%98Ah!%E2%80%99%E2%80%94Needle-Aspiration-of-Peritonsillar-Abscess/
2/23/2017
37
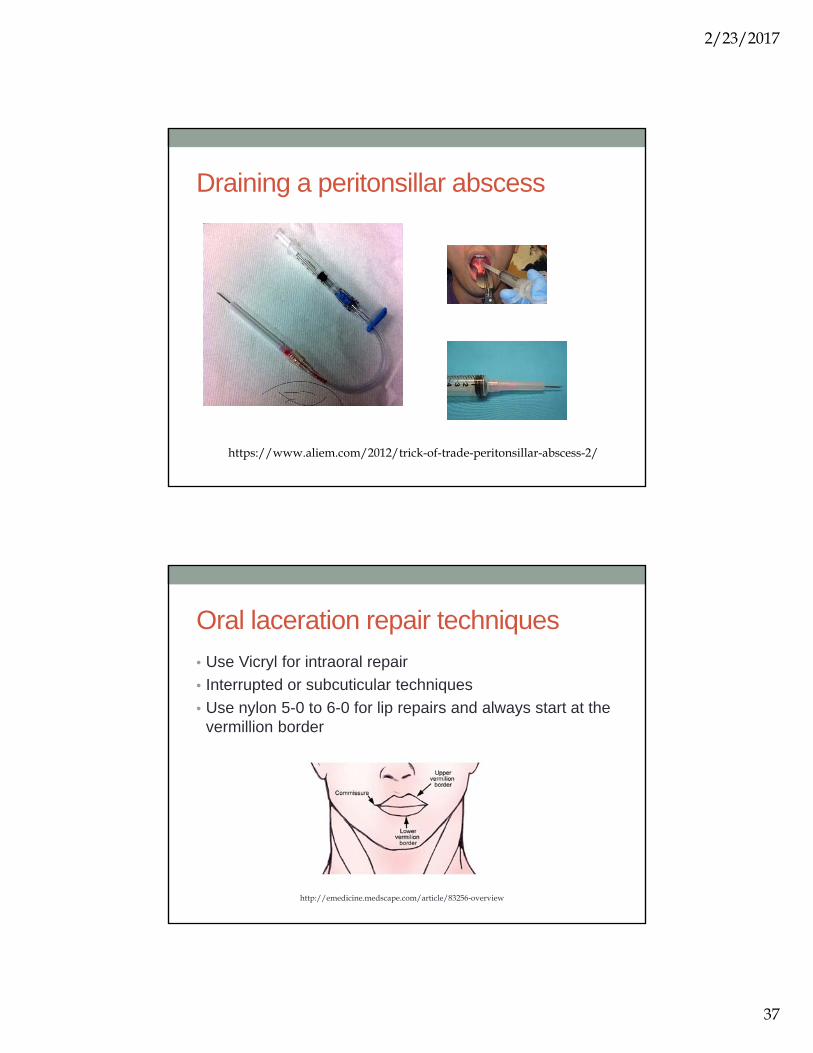
Draining a peritonsillar abscess
https://www.aliem.com/2012/trick-of-trade-peritonsillar-abscess-2/
Oral laceration repair techniques
• Use Vicryl for intraoral repair
• Interrupted or subcuticular techniques
• Use nylon 5-0 to 6-0 for lip repairs and always start at the vermillion border
http://emedicine.medscape.com/article/83256-overview

2/23/2017
38
Recommended Resources• For wound care and suturing
• Trott, A. (2012). Wound & lacerations: Emergency care and closures (4th ed). Philadelphia: Elsevier Mosby.
• For basic procedures• Campo, T.M. and Lafferty, K.A. (2015). Essential Procedures for Practitioners in Urgent and
Primary Care Settings: A Clinical Companion (2nd ed.). New York: Springer Publishing Company.
• For emergency procedures• http://www.acepnow.com/category/tricks-of-the-trade/• Roberts, J. & Hedges, J. (2013). Clinical procedures in emergency medicine (6th ed). Saunders
Elsevier. • Tintinalli, J., Stapczynski, J., Ma, O., Yealy, D., Meckler, G., & Cline, D. (2015). Emergency
medicine: A comprehensive study guide (8th ed.) New York: McGraw-Hill..
• For eye procedures and examination• http://www.ophthobook.com/
• For dental procedures and care • http://www.smilesforlifeoralhealth.org
• http://www.dentaltraumaguide.org
ReferencesCentor, R. (2009). Expand the pharyngitis paradigm for adolescents and young adults. Annals of Internal Medicine, 151(11), 812-815.Gorchynski, J., Karabidian, E. & Sanchez, M. (2014). The syringe technique: A hands-free approach for the reduction of acute nontraumatic tremporomandibular dislocations in the emergency department. The Journal of Emergency Medicine, Vol. 47, No. 6, pp. 676–681.Hayward, G., Thompson, M., Perera, R., Glasziou, P., Del Mar, C., & Heneghan, C. (2012). Corticosterioids as stand alone or add-on treatment for sore throat. Cochrane Database Systematic Reviews. Issue 10. Art. No.: CD008268. DOI: 10.1002/14651858.CD008268.pub2.
Kucik, C. & Clenney, T. (2005). Management of epistaxis. American Family Physician, Jan 15;71(2):305-311.Palioura, S., Henry, C., Amescua, G., & Alfonso, E. (2016). The role of steroids in the treatment of bacterial keratitis. Clinical Ophthamology, 10, 179-186.Prakashachandra, S., Patel, A., Patel, K., Doshi, R., & Patel, N. (2015). Grave complications of pharyngitis: Lemierre syndrome. Journal of Clinical & Diagnostic Research, 9(6), TD03-TD04.Rezk, E., Nofal, Y., Hamzeh, A., Aboujaib, M., Alkheder, M., & Hammad, M. (2015). Steroids for symptom control in infectious mononucleosis. Cochrane Database Systematic Reviews. Issue 11. Art. No.: CD004402. DOI: 10.1002/14651858.CD004402.pub3. . Roberts, J. & Hedges, J. (2013). Clinical procedures in emergency medicine (6th ed). Saunders Elsevier.Swaminathan, A., Otterness, K., Milne, K., & Rezaie, S. (2015). The safety of topical anesthetics in the treatment of corneal abrasions: A review. The Journal of Emergency Medicine, Vol. 49, No. 5, pp. 810–815.Tintinalli, J., Stapczynski, J., Ma, O., Yealy, D., Meckler, G., & Cline, D. (2015). Emergency medicine: A comprehensive study guide (8th ed.) New York: McGraw-Hill.Waldman, N., Densie, I., & Herbison, P. (2014). Topical tetracaine used for 24 hours is safe and rated highly effective by patients for the treatment of pain caused by corneal abrasions: A double-blind, randomized clinical trial. Academic Emergency Medicine, 21, 374-382.