
Extensor apparatus of hand injuries
48
PRESENTOR : DR SHAMENDRA ANAND SAHU VMMC & SAFDARJUNG HOSPITAL NEW DELHI ANATOMY OF EXTENSOR APPRATUS OF HAND AND DEFORMITIES CAUSED AT VARIOUS LEVELS
-
Upload
shamendra-sahu -
Category
Health & Medicine
-
view
725 -
download
1
Transcript of Extensor apparatus of hand injuries

PRESENTOR : DR SHAMENDRA ANAND SAHU
VMMC & SAFDARJUNG HOSPITALNEW DELHI
ANATOMY OF EXTENSOR APPRATUS OF HAND AND DEFORMITIES
CAUSED AT VARIOUS LEVELS

Extensor apparatus of hand Extensor apparatus of hand includes :
1. Muscles – Extrinsic / intrinsic 2. Anatomy at the level of wrist 3. Over the dorsum of the hand4.Over digits
Variation in anatomy at various levels

Extensor apparatus of hand
EXTRINSIC MUSCLES
PROXIMAL DISTAL
ECU,EDM,EDC ,ECRL,ECRB APL, EPB,EPL
Extensor apparatus of hand Intrinsic muscles of hand : 1.DI 2.PI 3.Lumbricles
Intrinsic muscles contribute to formation of extensor hood
Nerve supply : DI & PI – Ulnar nerve lumbricles

The tendons of the extensor muscles run under the extensor retinaculum.
They are separated into six compartments


Extensor apparatus of hand Over the dorsum of the hand :
Juncturae tendinae : interconnections
between the EDC tendons
Extensor apparatus of hand Lacerations proximal to the juncturae must be
examined carefully to avoid missing a tendon laceration.
The presence of a junctura can provide weak MP extension of a tendon with a proximal laceration.
Weak MP extension by a junctura and interphalangeal (IP) extension by the intrinsics lead the examining physician to conclude incorrectly that the divided EDC is intact.


EIP and EDM EIP and EDM tendons are independent
extensors with independent muscle origins.
The EIP also lacks a junctura.
On occasion, the EDM has a junctura from the ring EDC.

EIP and EDM These features of independent motor
control make them useful for tendon transfers.
The EIP and EDM are both ulnar to the EDC tendon at the MP joint.
This anatomic fact makes it easy to identify the EIP or EDM for a tendon transfer.

Extensor Apparatus Digits
Sagittal bands : At the MCPJ, the extensor tendon is held in position.
A sling that arises from the volar plate of the MCPJ and intermetacarpal ligaments.

Variations in no of tendon slips There are variations in the number of tendons
associated with each extensor muscle . This is important to remember in sorting out
extensor tendons lacerated at the wrist level. the fourth compartment is known to contain
four EDC tendons and the single tendon of the EIP. It can be confusing to find six to eight divided tendon slips in the compartment8 rather than the anticipated five tendons


Diagnosis/patient presentation Diagnosis of extensor tendon injuries is
often evident.
As a general rule : open lesions should therefore be surgically explored to identify the extent of the injury

The function of the EDC tendon should be assessed by extension of the MP joint of the affected digit against resistance.
Partial lesions can be missed if the remaining tendon is strong enough to create some extension force .
The EPB tendon inserts into the extensor tendon apparatus of the thumb at varying levels and may be able to extend the IP joint of the thumb.
If there is a questionable rupture of the EPL tendon, it should therefore not be tested by extension of the IP joint.
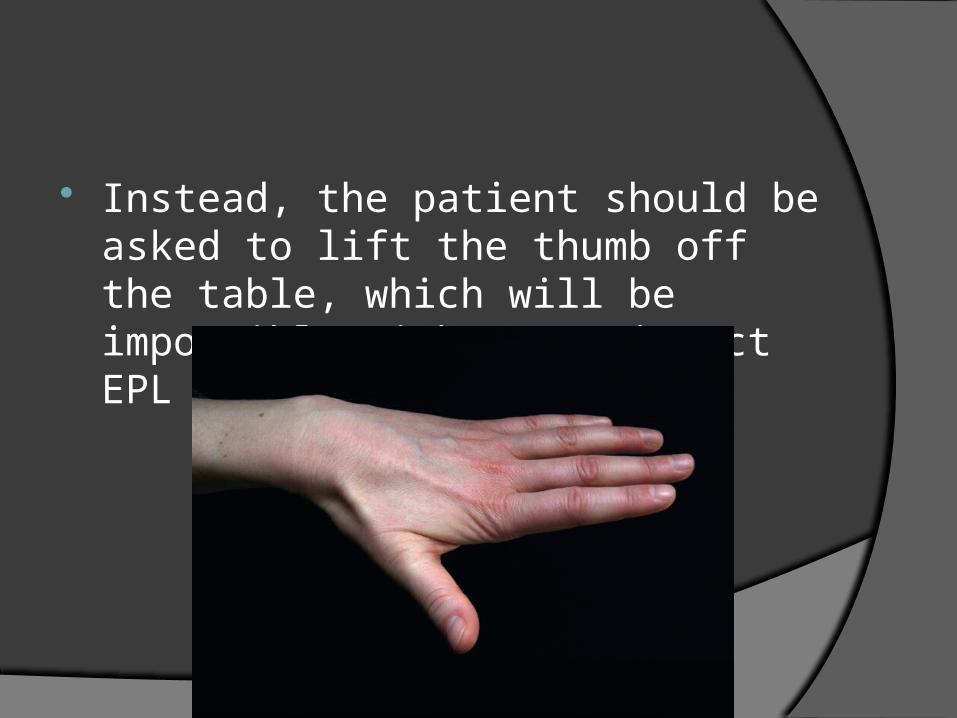
Instead, the patient should be asked to lift the thumb off the table, which will be impossible without an intact EPL tendon

Kleinert and Verdan proposed a system to classify lesions of the extensor tendon apparatus into eight zones according to the level of the lesion.
Doyle has added a ninth zone by dividing the forearm into the distal (zone 8) and proximal forearm (zone 9).


Odd numbered zones are located over the joints, whereas even numbered zones are found in between (i.e., zone 1 lies over the DIPJ, zone 3 over the PIPJ, zone 5 over MCPJ)
In the thumb, the interphalangeal joint (IPJ) is zone 1 and MCPJ is zone 3.

EXTENSOR TENDON INJURIES
EXTENSOR TENDON INJURY
Acute injury Chronic Deformities
ZONE I (DISTAL INTERPHALANGEAL JOINT, THUMB INTERPHALANGEAL JOINT)
Disruption of the extensor tendon results in a loss of distal phalangeal extension and a flexed posture.
This is called mallet finger, baseball finger, dropped finger, or extension lag.
The mechanism of injury is usually forced flexion of an actively extended distal joint.
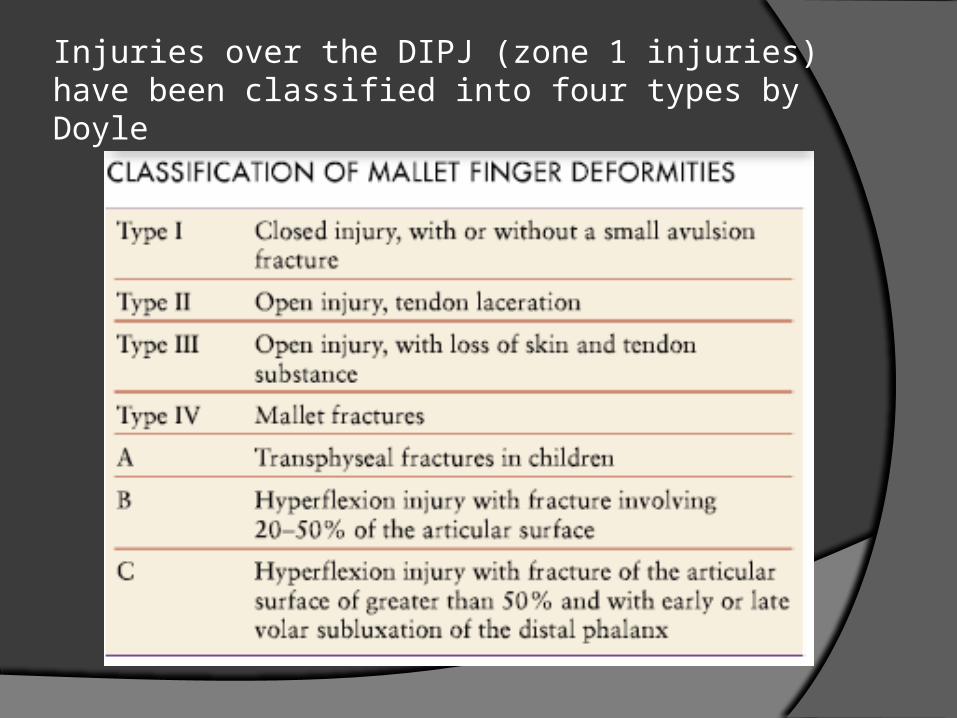
Injuries over the DIPJ (zone 1 injuries) have been classified into four types by Doyle

Zone 2 Injuries Extensor tendon width is greater in zone
II than in zone I. The extensor mechanism has two lateral
bands, each of which can extend the distal phalanx.
The mechanism envelops a significant portion of the curving middle phalanx.

Zone 2 Injuries Consequently, lacerations in this area
are often incomplete divisions of the tendon and do not result in a mallet deformity.
When evaluating these injuries, phalangeal extension should always be tested against resistance.

Zone 3 Injuries The functions of the central tendon and
lateral bands make zone III injuries unique. Closed PIP joint injuries : Until the
triangular ligament fibers stretch, the lateral bands remain dorsal to the PIP and can extend the joint.
The inability to completely extend the PIP joint with the wrist and MP joints in full flexion is evidence of a central slip disruption.

Immediately after a central tendon disruption, the lateral bands, if uninjured, can remain in a dorsal location and continue to extend the PIP joint.
Over time, the triangular ligament may stretch and the lateral bands shift in a volar direction. The head of the proximal phalanx "buttonholes" through the extensor mechanism, creating the boutonnière deformity.
ZONE IV (PROXIMAL PHALANX, THUMB METACARPAL)
The zone IV extensor mechanism is broad and extends around the sides of the proximal phalanx .
A complete tendon division is uncommon in this location.
Partial lacerations (<50% of the tendon) do not require tendon sutures.

ZONE IV (PROXIMAL PHALANX, THUMB METACARPAL)
Subtotal lacerations (>50% of the tendon) and complete divisions :
When evaluating these injuries, phalangeal extension should always be tested against resistance.

Zone 5 Injuries A central tendon laceration can easily be
missed The intact portion of the extensor can
provide some MP joint extension, and the intrinsics extend the IP joints.
The tendon's continuity is examined by asking the patient to extend the MP joint against resistance.

The radial and ulnar sagittal bands centralize the central tendon over the MP joint by their attachments to the volar plate.
A laceration or blunt trauma can disrupt one of the bands and allow central tendon subluxation into the contralateral web space.
The patient complains of a snapping sensation with MP flexion. On examination, central tendon subluxation off the metacarpal head is evident with MP joint flexion.

ZONE VI (METACARPAL)
extensor tendon division in zone VI can initially be a subtle diagnosis
Complete laceration of an EDC tendon in zone 6 may not result in an extensor lag at the MCPJ because of the juncturae tendinae that interconnect the EDC tendons.

It is advisable, therefore, to surgically explore lacerations on the dorsum of the hand.
MP joint extension is checked against resistance
Zone 7 Injuries Zone VII injuries occur beneath the
dorsal retinaculum.
Tendon repair in this area usually requires opening a portion of the retinaculum.
Zone 8 Injuries Lacerations in zones VIII and IX can
divide a combination of tendon, muscle, and motor nerves
location of the laceration and the resultant motor deficit are compared with the site of motor innervation. This helps distinguish a motor nerve injury from a tendon laceration.

The motor branches to the ECRL and ECRB are proximal to the supinator muscle. Consequently, a laceration in the distal half of the forearm, with loss of a wrist extensor, is a musculotendinous rather than a motor nerve injury.
Motor branches to the hand extensors occur in two
forearm groups, a proximal-superficial group and a distal-deep group. The proximal-superficial group consists of the ECRB, ECRL, EDC, EDM, and ECU muscles. They originate and receive motor branches near the lateral epicondyle of the humerus.

The distal-deep group consists of the EIP, AbPL, EPB, and EPL. They originate in the distal half of the forearm, close to the skeletal plane. Consequently, a proximal forearm laceration with loss of distal group function is probably a motor nerve injury rather than a tendon division
CHRONIC EXTENSOR TENDONPROBLEMS Swan neck deformity (SND) PIPJ : Synovitis at the PIPJ can cause attenuation of the
volar plate and TRL, which allows dorsal translation of the lateral band, as well as destruction of the flexor digitorum superficialis insertion.
This allows hyperextension of the PIPJ, which in turn results in increased tension in the flexor digitorum profundus tendon, as well as loss of tension in the lateral bands, resulting in DIPJ flexion.
Over time, adhesions develop and convert this into a fixed deformity.
Swan neck deformity MCPJ - Synovitis at the MCPJ can lead
to weakening of the insertion of the long extensors into the base of the proximal phalanx, causing the force to be transmited to the base of the middle phalanx, resulting in PIPJ hyperextension.
Swan neck deformity DIPJ - Rupture of the terminal extensor
tendon, which can occur following trauma or due to synovitis, allows proximal migration and relaxation of the lateral bands.
Extensor power is then concentrated on the central slip, resulting in PIPJ hyperextension and SND as the volar restraints weaken over time
Swan neck deformity Wrist - Synovitis at the wrist can result in
carpal collapse, carpal supination, and ulnar translation. Carpal collapse causes relative lengthening of both long flexors and extensors, allowing the intrinsic muscles to overpower their action and cause MCPJ flexion and PIPJ extension, which in time can lead to an SND
Swan neck deformity

Boutonniere Defonnities Boutonniere deformities are
characterized by a flexion deformity of the PIPJ, with reciprocal extension at the MCPJ and DIPJ.
Boutonniere deformities develop due to pathology at the PIPJ alone, unlike SND

Boutonniere Defonnities The central slip becomes dysfunctional Triangular ligament stretches and allows
the lateral bands to sublux in a volar direction, maintaining persistent PIPJ flexion.
The ruptured central slip also allows the force from the lumbricals and interosseous muscles to be transmitted directly to the distal phalanx, resulting in DIPJ extension

Boutonniere Defonnities

THANK YOU


















