
Extended Field Irradiation for Advanced Breast …gbcc2016.gbcc.kr/upload/Jiayii Chen.pdfEXTENDED...
39
EXTENDED FIELD IRRADIATION FOR ADVANCED BREAST CANCER PATIENTS, WHEN AND HOW? CHEN JIA-YI DEPARTMENT OF RADIATION ONCOLOGY RUI-JIN HOSPITAL, SCHOOL OF MEDICINE, SHANGHAI JIAO-TONG UNIVERSITY GBCC 2018
Transcript of Extended Field Irradiation for Advanced Breast …gbcc2016.gbcc.kr/upload/Jiayii Chen.pdfEXTENDED...

EXTENDED FIELD IRRADIATION
FOR ADVANCED BREAST CANCER
PATIENTS, WHEN AND HOW?
CHEN JIA-YI
DEPARTMENT OF RADIATION ONCOLOGY
RUI-JIN HOSPITAL, SCHOOL OF MEDICINE,
SHANGHAI JIAO-TONG UNIVERSITY
GBCC 2018
CONCERNS AND CONTROVERSIES
Decision of regional nodes irradiation (RNI)
• In high risk patients after axillary dissection
• In node positive patients undergoing sentinel biopsy without dissection
Indication of post-surgical radiation after NAC
• In patients with initial stage II-III diseases receiving neo-adjuvant systemic therapy
Neo-adjuvant RT advances
Synergy of Radiation therapy and immunotherapy

3EBCTCG 2014
EBCTCG 2014
RT AFTER MASTECTOMY AND ALND (ALN4+)
RT: significant benefit
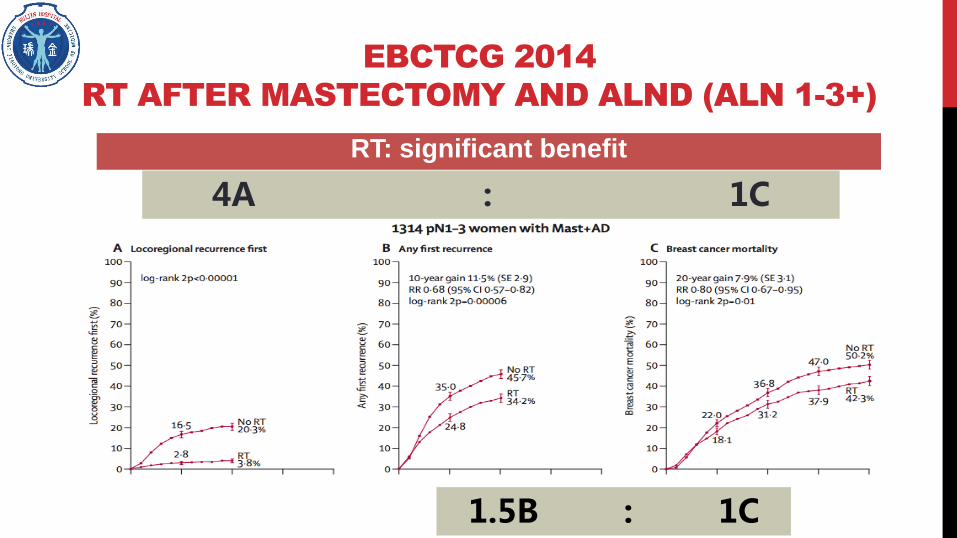
EBCTCG 2014
RT AFTER MASTECTOMY AND ALND (ALN 1-3+)
RT: significant benefit
4A : 1C
1.5B : 1C

RNI IN HIGH RISK PATIENTS AFTER ALND
French Trial EORTC 22922/10925 MA.20
Year of enroll 1991-1997 1996-2004 2000-2007
Sample size 1334 4004 1832
Pts selection N+ / inner quadrant N+/ inner quadrant N+ / high risk N0
N0% 40% 44.4% 9.7%
Median Age 57 54 54
Surgery mastectomy 76.1% BCS BCS
chemo % 61 85 91
ER/PR- 7 16 25
HR unknown % 40% 16% unknown
Breast/CW dose Individual discretion 50Gy/25F 50Gy/25F
SC 45Gy/25F both arm study 50Gy/25F Study 45Gy/25F
IMN Study arm 45Gy/25F Study 50Gy/25F Study 45Gy/25F
5MA 20 高危定义:T≥5cm,或T≥2cm,同时<10枚腋窝淋巴结取样,且ER-,G3或淋巴脉管受侵

EORTC 22922/10925
6
Distant metastasis
free survival
OS
ER – tumors:
10-year DFS in the control and RNI
arms :(71% and 82%, P<0.05);
10-year OS:74% and 81%
P.M.Poortmans et al. N Engl J Med 2015;373:317-27.
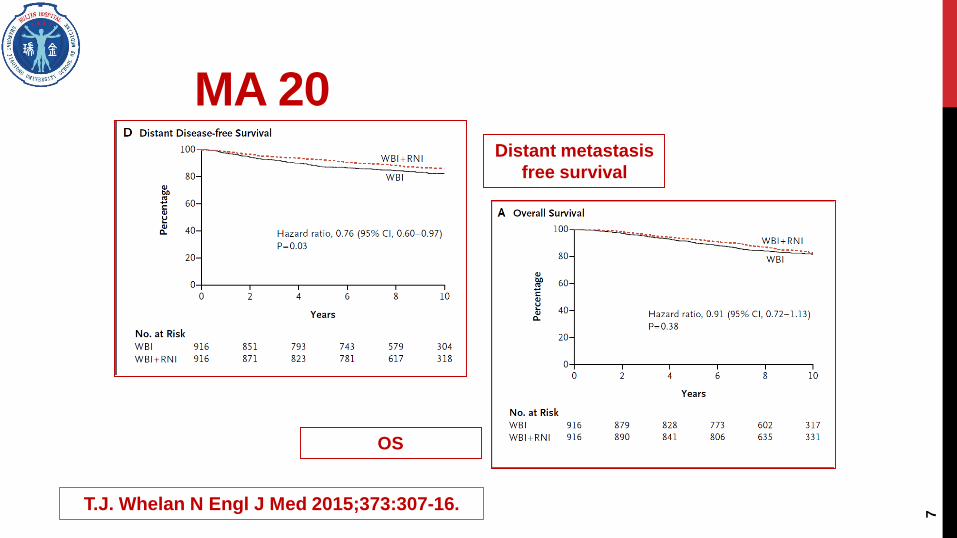
MA 20
7
Distant metastasis
free survival
OS
T.J. Whelan N Engl J Med 2015;373:307-16.

• pNmic were ineligible• 10% of patients with left-sided breast cancer did receive IMNI, who
were more frequently had many lymph nodes involved or a medial/central tumor
DBCG-IMN STUDY
Early Stage;
Lymph node
positive
Right-sided
(N=1492)
Fo
llow
-upLeft-sided
(N=1597)
WB/CW+RNI
(With IMN)
N=1437
WB/CW+RNI
(Without IMN)
N=1432
The study was a nationwide, prospective,
population-based cohort study, 2003/1-2007/12
Primary end points was overall survival
Secondary end points were breast cancer mortality and distant recurrence
DOI: 10.1200/JCO.2015.63.6456

8-year OS
(HR=0.82, p=0.005) 75.9% vs. 72.2%
8-year breast cancer mortality
(HR=0.85, p=0.03) 20.9% vs. 23.4%
8-year distant recurrence
(HR=0.89, p=0.07) 27.4% vs. 29.7%
DFS
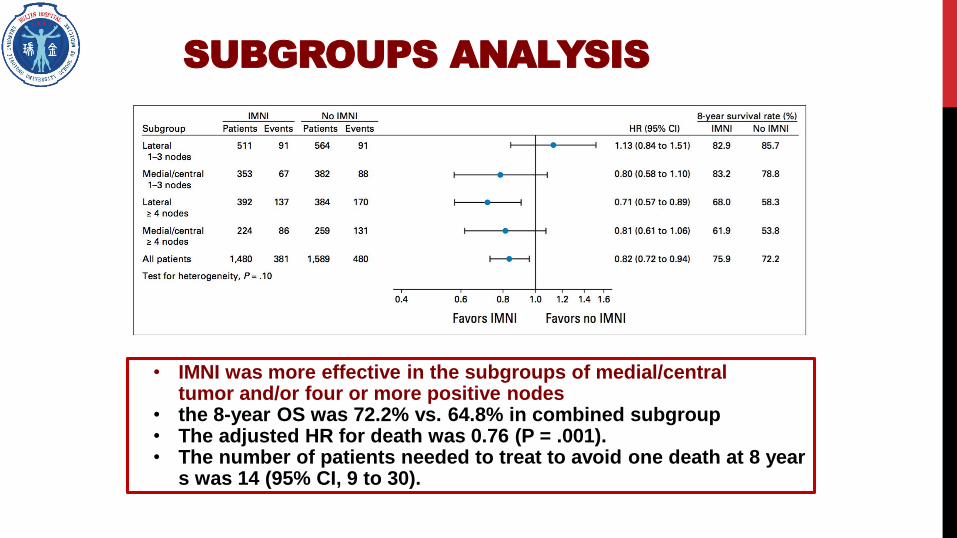
SUBGROUPS ANALYSIS
• IMNI was more effective in the subgroups of medial/central tumor and/or four or more positive nodes
• the 8-year OS was 72.2% vs. 64.8% in combined subgroup• The adjusted HR for death was 0.76 (P = .001). • The number of patients needed to treat to avoid one death at 8 year
s was 14 (95% CI, 9 to 30).

N1-3+ SUMMARY
MA.20 EORTC22922
HypothesisImprovement of 5% in 5y OS
(80% vs. 85%)
Improvement of 4% in 10y OS
(79% vs. 75%)
Patients 1832 4004
N1-3+ 85% 43.1%
T1-T2 99% 95.8%
BCS 100% 76.1%
Group WBI+RNI vs. WBI WBI/CW+RNI vs. WBI/CW
10-year OS 82.8% vs. 81.8% 82.3% vs. 80.7%
10-year breast cancer
mortality10.3% vs. 12.3% 12.5% vs.14.4%

SUBGROUP BENEFIT FROM RNI

EVOLUTION OF RNI RECOMMENDATION

RS AND LRR
- NSABP B28
1065 ER positive N+ pts
772 N1, 300 N2
461 BCS+WBI, 604 MRM
JNCI J Natl Cancer Inst, 2017, Vol. 109, No. 4

RS showed no significant
prognosis in 1-3 positive
ER+ patients
JNCI J Natl Cancer Inst, 2017, Vol. 109, No. 4
prospective trial is needed to evaluated the
role of RS on radiotherapy

0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2012 2013 2014 2015 2016
乳房切除术后T1-2N1的患者接受术后辅助放疗
不详
主诊医生决定
仅伴有不良预后因素
者做所有都做
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2012 2013 2014 2015 2016
保乳术后腋窝淋巴结1-3个转移的患者是否接受区域淋巴结照
射
主诊医生决定
伴有不良预后因素者
否
是
Questionnaire to 15 centers of radiotherapy
For N1,RNI after BCS and PMRT after mastectomy is the choice of
radiation oncologist in majority

TO DEFINE RNI BEYOND ALN
LOW RISK N1?
age
molecular subtype
Number of +ALN
+ALN ratio
multi-gene model
……
HIGH RISK N0?
MA 20:
High risk N0 was defined as T≥5cm; T≥2cm,nodes analyzed<10 and one of these: ER-, Grade III, LVI+
EORTC 22922/10925:
High risk was defined as centrally or medially located
In house protocol of Institut Curie:
T3, T4,
≤40,multi-foci,LV+,grade III ,HER 2+,TN,PT2 (any of two or above )
17
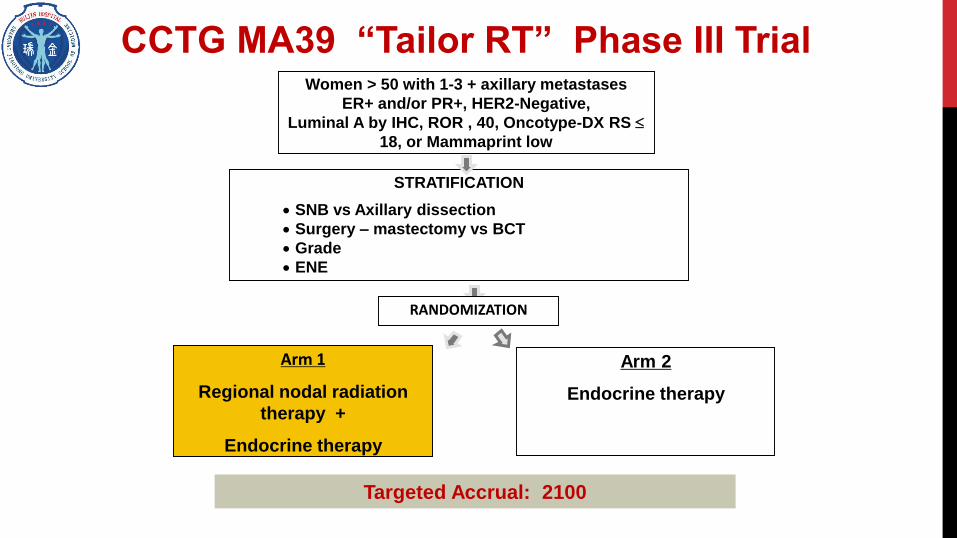
CCTG MA39 “Tailor RT” Phase III TrialWomen > 50 with 1-3 + axillary metastases
ER+ and/or PR+, HER2-Negative,
Luminal A by IHC, ROR , 40, Oncotype-DX RS
18, or Mammaprint low
STRATIFICATION
SNB vs Axillary dissection
Surgery – mastectomy vs BCT
Grade
ENE
RANDOMIZATION
Arm 1
Regional nodal radiation
therapy +
Endocrine therapy
Arm 2
Endocrine therapy
Targeted Accrual: 2100

SLN+ RESEARCH SUMMARY
Trials Tumor size BCS Group Conclusion
Z0011 cT1-2<3 SLN (+)*
95%SLN1-2+100% WBI**/ALND 13.0%
ALND Omitted
when WBI is given
IBCSG 23-
01T≤5cm
Micro SLN (+) ≥ 1
>99%SLN1-2+91% WBI/ ALND 27.8% ALND Omitted
AMAROS cT1-2, cN0SLN(+)
95%SLN1-2+82%
AxRT***/
ALND33%
AxRT can replace
ALND
19
*A total of 41% of SLNs were determined to have micrometastases (≤ 2 mm) or isolated tumor cell
**standard tangents or high tangents
***Axillary I/II/III+SC

ALND RECOMMENDATION
Omitting ALND:
•T1-2
•1-2 ALN+
•BCS+WBI
•No preoperative
chemotherapy

Like Z0011, like IBSCG 2301

DOSE TO OAR WHEN AXILLA IS
IRRADIATED
In comparison with high tangents or SC RT,
whole axilla RT is associated with increased
dose to ipsilateral lung
If axilla do necessite RT, more sophisticated
techinique is required.
WANG Shu-Bei et al. Cancer Radiothérapie,
acdepted
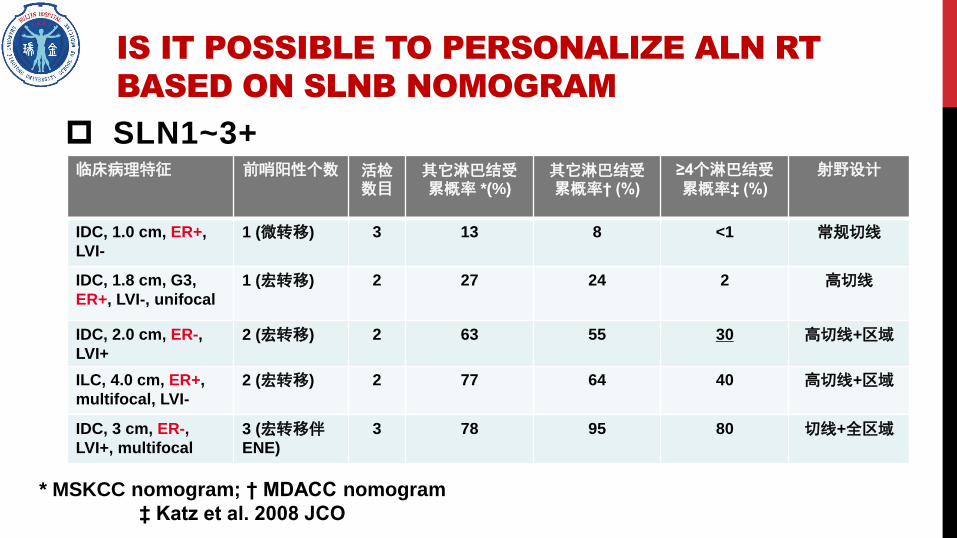
IS IT POSSIBLE TO PERSONALIZE ALN RT
BASED ON SLNB NOMOGRAM
SLN1~3+
* MSKCC nomogram; † MDACC nomogram
‡ Katz et al. 2008 JCO
临床病理特征 前哨阳性个数 活检数目
其它淋巴结受累概率 *(%)
其它淋巴结受累概率† (%)
≥4个淋巴结受累概率‡ (%)
射野设计
IDC, 1.0 cm, ER+,
LVI-
1 (微转移) 3 13 8 <1 常规切线
IDC, 1.8 cm, G3,
ER+, LVI-, unifocal
1 (宏转移) 2 27 24 2 高切线
IDC, 2.0 cm, ER-,
LVI+
2 (宏转移) 2 63 55 30 高切线+区域
ILC, 4.0 cm, ER+,
multifocal, LVI-
2 (宏转移) 2 77 64 40 高切线+区域
IDC, 3 cm, ER-,
LVI+, multifocal
3 (宏转移伴ENE)
3 78 95 80 切线+全区域

0
2
4
6
8
10
12
14
16
2012 2013 2014 2015 2016
保乳术后前哨淋巴结1-2个转移未行腋清的患者主要的放疗策
略为
不详
联合区域淋巴结
高位切线野
常规切线野
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2012 2013 2014 2015 2016
乳房切除术后T1-2前哨淋巴结微转移且未进行腋窝淋
巴结清扫的患者是否接受术后辅助放疗
主诊医生决定
伴有不良预后因素者
基本否
基本是
Questionnaire to 15 centers of radiotherapy
For BCS, SLNB1-2+ without ALND, RNI in addition to whole breast or
high-tangents is the choice of radiation oncologist in majority
More important controversies in pts after mastectomy

PMRT AFTER (NAC)------
CONSENSUS?
No prospective trial evaluating the role of PMRT after NAC

SCORING RESULTS
Scoring 1-3 (no recommendation for PMRT):
consensus of 80% or above: IIA, IIB, pCR or pN0
Scoring 7-9(recommendation for PMRT):
consensus of 80% or above: IIB , IIIA, pN+, or IIIC achieving PCR
Controversial population: IIIA/IIIB,achieving pCR or pN0,trends in
favor of PMRT
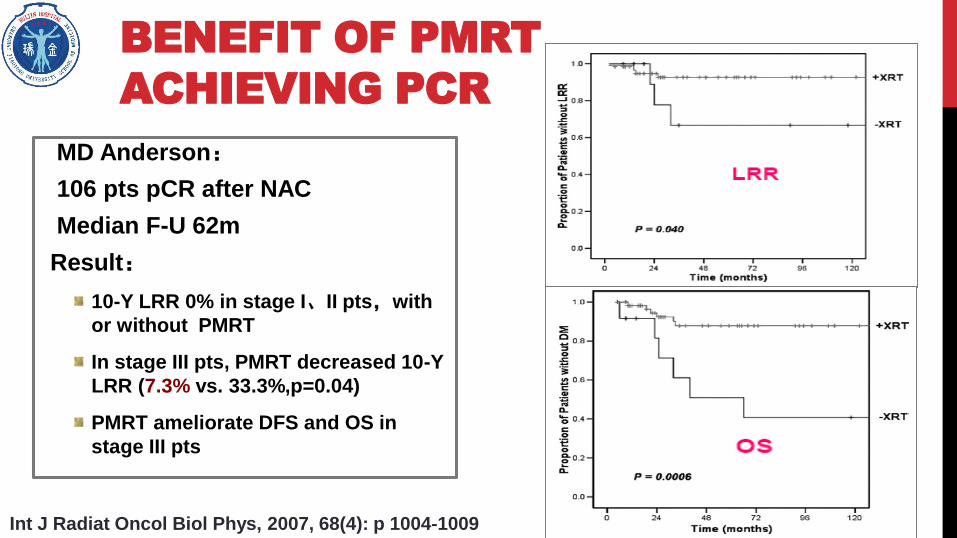
BENEFIT OF PMRT
ACHIEVING PCR
MD Anderson:
106 pts pCR after NAC
Median F-U 62m
Result:
10-Y LRR 0% in stage I、II pts,with
or without PMRT
In stage III pts, PMRT decreased 10-Y
LRR (7.3% vs. 33.3%,p=0.04)
PMRT ameliorate DFS and OS in
stage III pts
Int J Radiat Oncol Biol Phys, 2007, 68(4): p 1004-1009

KROG 12-05 : NO BENEFIT OF PMRT
IN STAGE II-III YPN0?
151 pts
105 W PMRT, 46 W/O PMRT
Median FU 59 mo
60/151 stage III
Age and pT stage affecting DFS
PMRT might not be necessary for pN0
patients after NAC
Int J Radiation Oncol Biol Phys, Vol. 88, No. 1, pp. 65e72, 2014

BENEFIT OF PMRT IN STAGE IIIB/C PN0
Oncotarget, Vol. 7, No. 17
1560 II-III stage ypN0
903 W PMRT, 657 W/O PMRT
Median FU 56 mo
1004 stage III patients
5-y OS rate: 84.6% for PMRT vs 81.7%
for no PMRT, P = 0.120
PMRT improved OS in patients with
clinical stage IIIB/IIIC disease

NEO-BIOSCORE
A staging system for NAC
patients which incorporated
treatment response and biologic
markers
Biologic markers and multi-gene
were highlighted in AJCC 8
JAMA Oncology. 2016 March 17.

THE ROLE OF NEO-BIOSCORE
FOR RNI AFTER NAC IN YPN0-1
Ruijin hospital
2009- 2014 163 pts
22.1% pCR, 54.6% ypN0,RNI (N=119)
Median FU 59.4 mo
Neo-Bioscore 1-3 (n=92)
5-y DRFS rate: 97% vs. 76.9% for
RNI or not (P=0.002)
5-y RFS rate: 95.5% vs. 76.9% for
RNI or not (P=0.007)
5-y BCSFS rate: 100% vs. 89.2% for
RNI or not (P=0.005)
Lu Cao,et al 2018 ASTRO abstract submitted.

NEO-ADJUVANT RT IN BREAST
RECONSTRUCTION
PMRT is increasingly
recommended for wider
indications
NACT followed by RT and
mastectomy and immediate
free flap reconstruction has
recently been shown to be
safe

NART IN RESTRUCTION RESEARCH
Trials Country Time Stage Treatment Early tocitySatisfaca
tion
5-y
DFS
Pailloch
er et alFrance 1997-2012 111
78% T1-2
40%N0,
54%N1
NART+MR
M+IBR
Seroma 54%
Necrosis 5.4%17/20 93.2%
Monrig
al et alFrance 1990-2008 210 Stage I-III
NART/RT*+
MRM+IBR
Total 21.9%
Necrosis 1% NR 75.6%
Grinsell
et alAustralia 2010-2015 29 NR
NART+MR
M+IBR
Necrosis 3%NR NR
*75 pts were initially treated by BCS and RT but requiring a secondary mastectomy in view of positive margins

HOW TO IRRADIATE RN,
IMN?
34
“CW nodule
invading sternum”
“parasternal
mass”
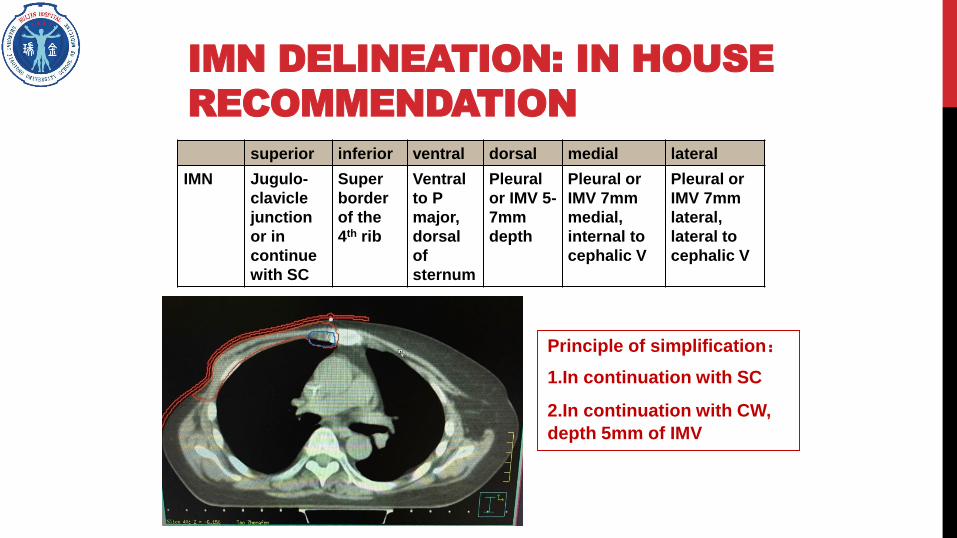
IMN DELINEATION: IN HOUSE
RECOMMENDATION
superior inferior ventral dorsal medial lateral
IMN Jugulo-
clavicle
junction
or in
continue
with SC
Super
border
of the
4th rib
Ventral
to P
major,
dorsal
of
sternum
Pleural
or IMV 5-
7mm
depth
Pleural or
IMV 7mm
medial,
internal to
cephalic V
Pleural or
IMV 7mm
lateral,
lateral to
cephalic V
Principle of simplification:
1.In continuation with SC
2.In continuation with CW,
depth 5mm of IMV

RADIATION THERAPY AND
IMMUNOTHERAPY
Immunotherapy, a series of agents designed to stimulate
the immune system in order to generate tumor-specific
immune response, is showing promise in treatment of
various cancers
Stone et al., in 1979, found that mice with fibrosarcoma
lacked T-cells required twice as high dose of radiation to
be cured compared to those with T-cells
J Natl Cancer Inst 1979;63:1229e35.

CLINICAL TRIALS OF IMMUNO-
RADIOTHERAPY IN BC
Signals Drugs Trial Phase Disease Statue
TLR
agonists
Imiquimod NCT01421017 I/II MBC Active, not
recruiting
TGF-β Fresolimumab NCT01401062 I/II MBC Active, not
recruiting
LY2157299 NCT02538471 II MBC Active, not
recruiting
OX40 MEDI6469 NCT01862900 I/II MBC(lung or liver) Active, not
recruiting
PD-1/PD-L1 MK-3475 NCT02303366 I oligometastatic BC Completed
Pembrolizumab NCT02730130 II mTNBC Active, not
recruiting
Nivolumab NCT02499367 II mTNBC Recruiting

TAKE HOME MESSAGE
The risk factors for LRR in node positive patients are quite complex
Traditional prognostic factors are basis of RT indications decision
Molecular subtype and 21-gene recurrence score could offer moreinformation
Elective RNI is recommended for SLN+ without ALND pts
Perspective trials needed for individualized RT
Response to NAC complicated RT choice for II-III pts
Staging system (Neo-bioscore) integrated biological information couldprovide guidance
NART followed IBR could be a safe option due to wider indications ofPMRT
Future clinical trials will elucidate the immuno-radiotherapy

39


















