
Exploring thE cliEnt and family-cEntrEd carE movEmEnt
40
Autumn 2012 A publication of the Saskatchewan Medical Association Volume 52 Issue 3 EXPLORING THE CLIENT AND FAMILY-CENTRED CARE MOVEMENT Answers to your most frequently asked EMR questions Surgical checklists: a near miss... or a good catch?
Transcript of Exploring thE cliEnt and family-cEntrEd carE movEmEnt

Autumn 2012
A publication of the Saskatchewan Medical Association Volume 52 Issue 3
Exploring thE cliEnt and family-cEntrEd carE movEmEnt
Answers to your most frequently asked EMR questions
Surgical checklists: a near miss...or a good catch?

AUTUMN 2012 | VOLUME 52 ISSUE 3
SMA News Digest is the official member magazine of the Saskatchewan Medical Association. It is published four times per year and is distributed to nearly 90 per cent of practising physicians in Saskatchewan.
Upcoming issuesThe next issue of SMA News Digest will be distributed in December 2012; the fol-lowing issue will be distributed in Febru-ary 2013.
BylinesWhere bylines are not given, articles were written or solicited by SMA com-munications staff.
AdvertisingThe deadline for booking and submitting advertising for the winter issue is Monday, November 12, 2012. Rates for display ad-vertising are available upon request. Clas-sified ad placement is free for members promoting physician, locum and practice opportunities; ads should be submitted via email and must not exceed 150 words.
FeedbackMember feedback is valuable and en-couraged. Please direct comments, let-ters, ideas and advertising inquiries to:Nicole QuintalCommunications AdvisorSaskatchewan Medical Association 402 - 321A - 21st Street EastSaskatoon SK S7K 0C1(306) [email protected]
CEODr. Vino Padayachee
SMA missionThe mission of the Saskatchewan Medi-cal Association is to advance the edu-cational, professional and economic welfare of Saskatchewan physicians; to advance the honour and integrity of the profession; and to promote qual-ity health care practices, quality health services, and to advocate for a quality health care system for Saskatchewan.
contents3 Report on CMA General Council 2012
Over 800 delegates, observers and guests, including a delegation from the Saskatchewan Medical Association, converged on Yellowknife for the Canadian Medical Associa-tion’s General Council in August.
11 EMR: Frequently Asked QuestionsFind out the answers to some of the most common ques-tions the SMA receives about EMR implementation.
27 Rural bus tour 2012Brand-new medical students from the University of Sas-katchewan ventured to Shellbrook and Memorial Lake in August as part of the 2012 SMSS rural bus tour. The tour aims to introduce students to rural practice early in their medical training.

3
27
11
your SMAPresident’s note
Report on CMA General Council 2012
A message from the Hon. Randy Weekes
Council of the Federation receives health care report
Dr. Ulla Nielsen receives Sterling Award for outstanding
community contributions
Dr. Dattani recognized by American Society of
Hypertension for excellence in research
Spotlight on the Specialist Recruitment and Retention
Committee
Communities seek input from physicians to address local
concerns
EMR: Frequently Asked Questions
Correct claims corner
SMA strategic plan highlights report
health careFeature: Client and family-centred care
SIPPA: Clinics encouraged to work with RHAs
Surgical checklists: A near miss...or a good catch?
students and residentsRural bus tour 2012
autumn calendar
classifieds
obituaries
23567
8
8
10
111415
222426
29
32
33
autumn 2012
27

2 Autumn 2012 SMA News Digest
Connecting with our members is the most rewarding part of serving as SMA president. We have recently
had many opportunities to connect with many of you and get your opinion on how we are doing and what di-rection we should be heading in.
Over the summer, Insightrix conducted our first member-ship survey since 2006. Those who were able to participate in the survey indicated that advancing the educational, professional and economic welfare of Saskatchewan phy-sicians was your top priority, followed closely by advanc-ing the honour and integrity of the profession.
Overall, two-thirds of respondents are satisfied with the SMA representing their interests. You have also told us that we need to work on providing better resolution of disputes with employers and health regions; individual and group contract negotiations; and advocating for physician representation on provincial agencies and committees.
We are continually working on improving our methods of communication, although satisfaction with our web-site, the SMA News Digest and contact with SMA staff re-
mains high. Many comments centered around offering more electronic communications and we have recently started an email newsletter and social media accounts on Twitter and Facebook to offer more ways to communicate with members.
Of course, the best way to communicate with our mem-bers is face-to-face. We were able to connect with a num-ber of you on the recent stops of the annual fall tour, which took myself, vice-president Dr. Clare Kozroski and SMA staff across the province to talk about current issues and learn about physician concerns in each region.
A few common themes emerged on our tour, including questions on the province’s Collaborative Emergency Care initiative, retaining doctors in rural Saskatchewan, Lean program training, and the situations in Ontario and Alberta with fee rollbacks and budget cuts. We will be taking all that we have learned from the tour and the sur-vey back to the SMA Board of Directors to help us craft our new strategic plan and to guide us in anticipation of bargaining in the upcoming year.
We have another important opportunity to connect with our members coming up: The fall Representative Assembly in Regina on November 2 and 3. I encourage all of our mem-bers to attend the RA and connect with the organization. We will have a great program and there will be many oppor-tunities to connect with your fellow physicians.
Please keep the feedback coming! We are a better organi-zation thanks to your input.
SMA receives results of 2012 membership survey
Contact SMA President Dr. Janet Shannon by email: [email protected]
president’s note
SMA News Digest Autumn 2012 3
your SMA
Report on CMA General Council 2012
By Dallas Carpenter
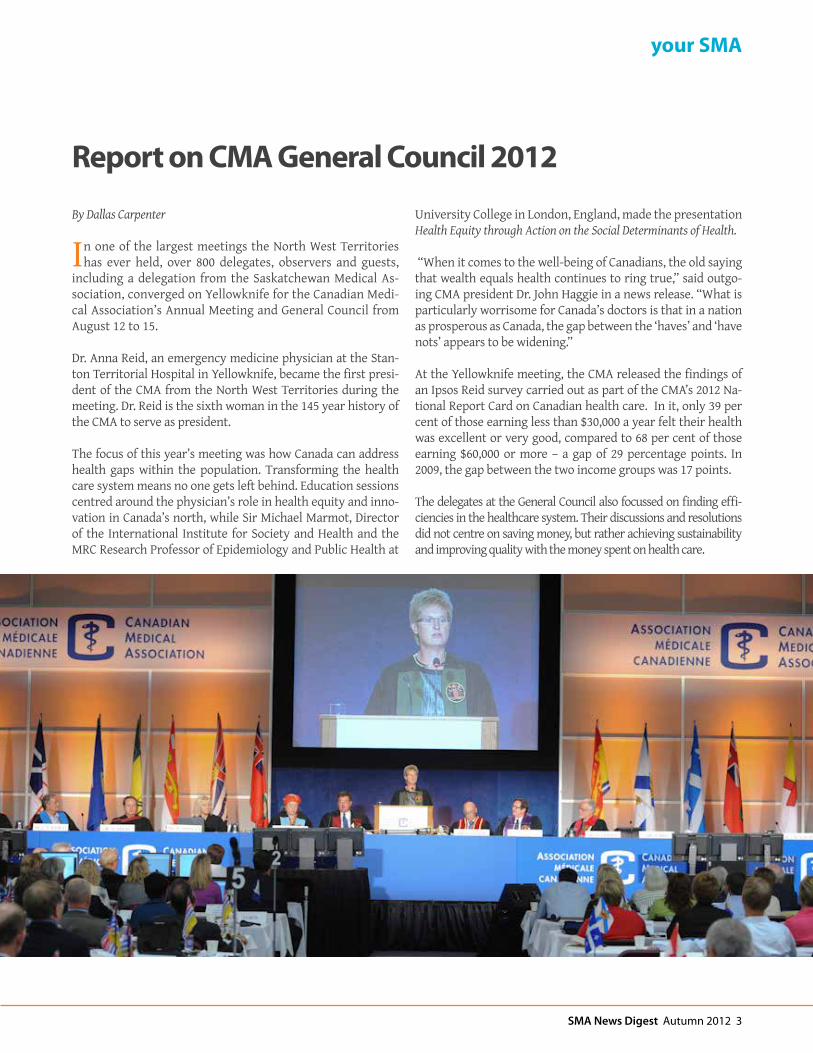
In one of the largest meetings the North West Territories has ever held, over 800 delegates, observers and guests,
including a delegation from the Saskatchewan Medical As-sociation, converged on Yellowknife for the Canadian Medi-cal Association’s Annual Meeting and General Council from August 12 to 15.
Dr. Anna Reid, an emergency medicine physician at the Stan-ton Territorial Hospital in Yellowknife, became the first presi-dent of the CMA from the North West Territories during the meeting. Dr. Reid is the sixth woman in the 145 year history of the CMA to serve as president.
The focus of this year’s meeting was how Canada can address health gaps within the population. Transforming the health care system means no one gets left behind. Education sessions centred around the physician’s role in health equity and inno-vation in Canada’s north, while Sir Michael Marmot, Director of the International Institute for Society and Health and the MRC Research Professor of Epidemiology and Public Health at
University College in London, England, made the presentation Health Equity through Action on the Social Determinants of Health.
“When it comes to the well-being of Canadians, the old saying that wealth equals health continues to ring true,” said outgo-ing CMA president Dr. John Haggie in a news release. “What is particularly worrisome for Canada’s doctors is that in a nation as prosperous as Canada, the gap between the ‘haves’ and ‘have nots’ appears to be widening.”
At the Yellowknife meeting, the CMA released the findings of an Ipsos Reid survey carried out as part of the CMA’s 2012 Na-tional Report Card on Canadian health care. In it, only 39 per cent of those earning less than $30,000 a year felt their health was excellent or very good, compared to 68 per cent of those earning $60,000 or more – a gap of 29 percentage points. In 2009, the gap between the two income groups was 17 points.
The delegates at the General Council also focussed on finding effi-ciencies in the healthcare system. Their discussions and resolutions did not centre on saving money, but rather achieving sustainability and improving quality with the money spent on health care.

4 Autumn 2012 SMA News Digest
your SMA
As governments across the country engage in economic re-straint, it is important that physicians be involved in the dis-cussions to reform the health system and be in closer contact with government ministries. With that in mind, former SMA presidents Dr. Guruswamy Sridhar and Dr. Phillip Fourie put forward three motions that direct the Canadian Medical As-sociation to support a strong, effective partnership between physician leaders and administrative leaders to achieve health care transformation.
The motions, which all passed with over 95 per cent of the ap-proval of delegates, will also examine physician leadership in system transformation and facilitate knowledge transfer of best practices in physician leadership and engagement across the country.
Delegates to the General Council also united behind the On-tario Medical Association in their impasse with the Ontario provincial government.
Dr. Anna Reid became the first CMA president from the North West Territories during the CMA General Council meeting in August.
Delegates at the CMA General Council meeting in Yellowknife.

SMA News Digest Autumn 2012 5
your SMA
A message from the Hon. Randy Weekes, Minister Responsible for Rural and Remote Health September 2012
This past spring, Premier Brad Wall chose to create a new cabinet position specifically dedicated
to focusing on the health care needs of our province’s smaller communities. I am honoured and humbled that Premier Wall has invited me to serve as the Min-ister Responsible for Rural and Remote Health.
In the past five years, we have seen nu-merous and significant improvements to Saskatchewan’s health care system; surgical wait times have been signifi-cantly reduced, there are more doctors and nurses practicing in the province, more training seats have been created, and aging health care infrastructure is being updated and replaced. There is much more work to do, and I am work-ing closely with Health Minister Dustin Duncan to continue our government’s efforts to transform the health sys-tem with the quadruple aims of Better
Health, Better Care, Better Value and Better Teams. Our government aims to ensure that all Saskatchewan people enjoy the best possible quality of life – regardless of where they live. We recognize that resi-dents of rural and remote communities often face unique challenges and with respect to the availability and predict-ability of health services in their area.
In order to gain a first-hand perspec-tive on some of these challenges, I have spent my summer touring communi-ties in rural and northern Saskatch-ewan. By early October, I will have met with community leaders, local health foundations, Regional Health Author-ity representatives, facility staff and health care providers in 40 communi-ties all over the province. I have ben-efited greatly from the honest and in-sightful conversations I have had with dozens of dedicated physicians in rural and northern Saskatchewan.
Throughout my travels, the most com-mon concerns I have heard in rural com-munities relate to the recruitment and retention of physicians, the consistent availability of emergency services, and the need for better communication and collaboration between all parties in the health care system; including health re-gions, the Ministry of Health, provider groups, patients and their families and the communities themselves. In the months ahead, a significant part of my mandate will be working to find innova-tive solutions to these and other rural health care challenges. As we move for-ward, the Saskatchewan Medical Asso-ciation will continue to be a key partner in these efforts.
One potential solution to the challenge of providing twenty-four-seven emergency coverage in rural communities was iden-tified by the Council of the Federation’s Health Care Innovation Working Group, which was co-chaired by Premier Wall. The working group recommended that
Dr. Vino Padayachee, Chief Executive Officer (CEO) of the SMA accompanied the Minis-ter Responsible for Rural and Remote Health, the Honourable Randy Weekes, on a visit to Nova Scotia in July, where they toured Collaborative Emergency Centres to gain a first-hand perspective on their operations and applicability in Saskatchewan.
Hon. Randy Weekes

6 Autumn 2012 SMA News Digest
your SMAyour SMA
other provinces explore a model of primary and emergency health care delivery first developed in Nova Sco-tia. Collaborative Emergency Centres (CECs) are designed to enhance access to high quality, comprehensive prima-ry care that is capable of dealing with unexpected illness or injury in a timely fashion. These centres are open twenty four hours a day, seven days a week, and are staffed by a primary health care team during the day and – at one of Nova Scotia’s CEC sites - a team that includes a nurse and a paramedic, con-nected to a physician by telephone or telehealth during the night. This model can be tailored to the specific needs of an individual community, and to the needs and abilities of health care pro-viders within that community.
In July, I had the opportunity to travel
to Nova Scotia to tour two Collaborative Emergency Centres. I was very grateful that Dr. Vino Padayachee was able to ac-company me on that trip – his expertise and perspective was an invaluable asset as we listened and learned from the peo-ple in Nova Scotia who have successfully implemented these CECs.
On September 18, a delegation of of-ficials from Nova Scotia was in Regina to provide information and education about CECs to representatives from the Ministry of Health, Regional Health Au-thorities, health care provider associa-tions and unions, as well as stakeholder groups like SUMA and SARM. Armed with this valuable information about Nova Scotia’s experience, the CEC model can now be adapted to work within Sas-katchewan’s health care system, and an innovation site will soon be established.
I am very excited about the potential benefits this kind of team-based ap-proach to health care delivery holds for rural and remote Saskatchewan. Im-proving the predictability of service and access to care for patients is our primary goal. It is our intent that this model will also improve the quality of life for our rural doctors by alleviating their often rigourous on-call schedule.
I look forward to working with the Sas-katchewan Medical Association on this and other initiatives as we endeavour to improve the health and well-being of all Saskatchewan people.
Randy Weekes, Minister Responsible for Ru-ral and Remote Health
In late July, Canada’s premiers met in Halifax for the Council of the Federation’s Annual Meeting. One of the key activities on the agenda was receiving the report of the Council of the Federation Working Group on Health Care Innovation, From Innovation to Action.
The Working Group, which consisted of Saskatchewan Premier Brad Wall, PEI Premier Robert Ghiz and all provincial and territorial health ministers, fo-cused on practical innovations that each province and territory can put to use to enhance patient care and improve value for taxpayers.
The recommendations that prov-inces and territories intend to im-plement as they deem appropri-ate to their health care system, include:
• Promoting the adoption of clinical practice guidelines for treating heart disease and diabetes
• Pursuing a number of team based models to increase access for Canadians, such as the Collaborative Emer-gency Centres Model and other models listed in the report
• Sharing information on health human resources man-agement and supply
• Improving communication about health human re-sources labour markets
• Having the Working Group monitor the progress made on the initiatives contained in this first report
The Canadian Medical Association, the Canadian Nurses’ Association and the Health Action Lobby collaborated with the Working Group on this initiative. A progress report will be drafted in advance of the 2013 summer meeting of the Council of the Federation.
Council of the Federation receives health care report
SMA News Digest Autumn 2012 7
your SMA
Dr. Ulla Neilsen receives Sterling Award for outstanding community contributionsBy Nicole Quintal
The Silver Spoon Dinner, a fundraiser often labeled ‘Sas-katoon’s Premiere Ladies’ Night Out’, has become an annual staple for celebrating outstanding local women.
One such woman, Dr. Ulla Nielsen, was recognized at the May 7 event and was presented with the Sterling Award for her work with the Saskatchewan Abilities Council – a non-profit organi-zation that she’s been involved with for the past two decades.
There is no question of Dr. Nielsen’s passion and commitment to the organization that aims to enhance the independence of those with varying abilities. She has served as a volunteer di-rector with the council’s board of directors since 1992, as presi-dent from 2003 to 2005, and chaired numerous committees and fund raising campaigns. A retired pediatrician, her knowledge of disability issues and dedication to the cause have made a sig-nificant difference in the lives of both children and adults with disabilities.
Nonetheless, she said she was surprised to hear that she would be receiving the award.
“I was really confused,” she said with a laugh. “I hadn’t known anything at all about the nomination. It was really out of the blue.”
Dr. Nielsen was drawn to the work of the council in the late 1980s while working with disabled children at the Kinsmen Children’s Centre, most who had been diagnosed with cerebral palsy, muscular dystrophy and acquired brain injury. She said it was the children’s reaction when she asked them what they were doing for the summer that solidified her involvement with the Saskatchewan Abilities Council.
“Just to see some of these faces light up when they talked about going to Camp Easter Seal. I think that was the biggest draw,” she remembered.
Camp Easter Seal is one of the council’s most renowned pro-grams. The camp serves approximately 700 to 800 children per summer at its Manitou Lake Beach location. Dr. Nielson noted that although it’s located in a sloped area of terrain, it is com-pletely wheelchair accessible.
“There is no waiting list for children at camp. They are accom-modated,” she explained. “There is a whole variety of program-ming for young adults and adults at Camp Easter Seal. It’s a tremendous place.”
The council also houses programs such as Farmer’s with Dis-abilities, which focuses on educating children on the impor-tance of farm safety. Dr. Nielsen says this program is not as well-known as some of the others, but holds extreme impor-tance in our province.
“Farming is one of the most hazardous occupations in the province. It’s one of the occupations where there is a high level of disabilities that occur,” she said.
Dr. Nielsen says her goal is to continue to support the council and the progress it has made.
She would also like to thank the sponsors of the Sterling Award in addition to the past winners of the award – all volunteers who had not previously been recognized for their work, which is a criterion for choosing the Sterling Award recipient.
“It really supports the volunteer activities in the community. I just have to say thank you so much to them,” she said. “They do a job here that no one else is doing.”
Dr. Ulla Nielsen at the Silver Spoon Dinner.
Phot
o co
urte
sy o
f Hea
ther
Frit
z Pho
togr
aphy

8 Autumn 2012 SMA News Digest
your SMA
Dr. Dattani recognized by American Society of Hypertension for excellence in research
By Nicole Quintal
A local family physician has been rec-ognized by the American Society of Hy-pertension as a fellow for excellence in research and clinical contributions.
Dr. Dan Dattani of Acadia Medical Centre in Saskatoon received the accolade on
May 21, 2012. It is awarded to individuals who have excelled in and led efforts for high blood-pressure control.
Dr. Dattani, who has a special interest in hypertension, cardiovas-cular medicine and diabetes, said it’s a privilege to be recognized for the research he has done over the past 25 years.
“When you’re a family physician and you get recognition from a peer body, I consider it very special,” he said.
In 2003, his published study was accepted by the American Soci-ety of Hypertension; he initiated the study and enlisted the help of approximately 16 physicians from across Saskatchewan.
Dr. Dattani says the physicians contributed from a Saskatchewan perspective and considered questions regarding whether or not they were meeting the patient-treatment targets set out by the Canadian Hypertension Society.
“The whole idea is to continue to maintain research based on what the Canadian Hypertension Society tells us we should be doing at a primary care level,” he said.
The primary-care physician began researching hypertension 25 years ago and has participated in several national and interna-tional trials to determine the best way to manage hypertension and the implications of treating blood pressure.
Most of the studies he has participated in over the years have been landmark studies.
“Medicine is an evolving science. Participation in global land-mark studies has been a privilege for us and our patients as these studies challenge old established conventions,” he explained. “Conclusions from such studies lend support to creating evi-dence based guidelines that impact our day-to-day practice of medicine.”
Dr. Dattani was nominated for the award by the past-president of the American Society of Hypertension. The other nominees were people who worked with him on clinical trials.
After practising in Saskatoon for 31 years, Dr. Dattani says he is very proud of the community that he serves and is grateful to his patients, many who have participated in clinical trials and al-lowed him to conduct his work.
Spotlight on the Specialist Recruitment and Retention CommitteeBy Nicole Quintal
Since the mid-1990s, Saskatchewan has had difficulty at-tracting and retaining Saskatchewan-trained specialists.
Initially, bursaries were provided by the SMA and Ministry of Health through the Committee on Rural and Regional Prac-tice (CORRP) to residents at the University of Saskatchewan. These bursaries were extended to residents in one of eight specialties.
However in 2000, the SMA negotiated a fund targeted spe-cifically for recruiting and retaining specialists in the prov-
ince. As such, the Specialist Recruitment and Retention Committee (SR&R) was born, tasked with identifying strat-egies and developing programs to help keep specialists in Saskatchewan.
The Specialist Resident Bursary Program was the first launched by SR&R, which provides funding to specialty resi-dents enrolled at the University of Saskatchewan, or resi-dents who initially completed their undergraduate medical training at the University of Saskatchewan. Recipients of the award are required to provide a return-in-service to Sas-katchewan for a fixed period of time upon completing their training. (continued on page 9...)

SMA News Digest Autumn 2012 9
your SMA
Since that time, SR&R has expanded its program platform to include the following:
• SpecialistRecruitmentIncentive• SpecialistEmergencyCoverageProgram• SpecialistEnhancementTrainingProgram• SpecialistExtendedLeaveProgram• SpecialistResidentBursaryProgram
Meet Dr. Zenon Belak
In the spirit of SR&R, the SMA chose to interview a 2011 recipient of the Special-ist Resident Bursary, Dr. Zenon Belak, who is now a Clinical Fellow in the Divi-sion of Respirology at the University of Saskatchewan. We asked Dr. Belak why he chose to study in Saskatchewan and what he enjoys most about the province, from both practising and living perspec-tives. Here is what he had to say.
SMA: When did you initially come to Saskatchewan?ZB: I initially came to Saskatchewan in July of 2010.
SMA: Where were you before that?ZB: I was down in the United States, where I completed the majority of my clinical training as well as my post-graduate specialty training in the field of internal medicine.
SMA: Why did you decide to study in Saskatchewan?ZB: I was particularly interested in the tradition of excellence in clinical teaching, especially that provided by the Division of Respirology, as well as it being the province in which I was born and raised. Family and friends influenced that decision to a significant degree.
SMA: What do you enjoy most about practising in Saskatchewan?ZB: My medical education has, to my great benefit, allowed me to train in different locations both in the United States and in Canada, and I think one of the things that sort of came to the forefront and certainly does continue to on a daily basis is really just taking care of the people of Sas-katchewan. It’s really rewarding to take care of them as a health care professional.
SMA: What do you enjoy most about living in Saskatch-ewan?ZB: I think it has a significant amount of the modern ame-nities you would hope to have in an urban centre, both speaking to Saskatoon and Regina, but without a lot of the disadvantages of living in a very large metropolis, speaking mostly to cost of living and traffic.
SMA: Are there any programs offered in Saskatchewan that you found to be beneficial during your training?ZB: I can break it down to programs that I certainly found to be of benefit while I was a resident. Certainly there is avid support from the Department of Medicine in particular, and the Division of Respirology in supporting residents in participating education leadership and training opportuni-ties both at the national and international stage. What has also been impressive to me is the PAIRS organization, both in their representation of residents and the leadership they provide at that level. Certainly the SMA, from the perspec-tive of a resident, has taken a position that seemed to be a very open and inviting engagement with post-graduate medical residents. So that has certainly influenced me as a resident to have a positive experience, and there’s no doubt that in consideration of practice going forward the SMA provides a substantial amount of leadership and support for practising physicians in the province.
SMA: Would you recommend other medical learners and residents consider Saskatchewan as a future practice option?ZB: With regards to recently graduating physicians starting practice in Saskatchewan, I would highly recommend it. I think there’s ample need for physicians in many different specialties, both if your interests are primarily clinical and patient care, or academic and research. Furthermore, I think the practice environment in Saskatchewan is preferable, at least in my very biased opinion, to that found elsewhere in other provinces. Particularly through the SMA, it’s obvious to me that it has placed a significant amount of priority in recruiting both U of S graduates and newly graduated resi-dents in the form of resident bursaries, recruitment incen-tives, and a considerable amount of support going forward once you establish practice in the form of supporting the CMPA dues, Electronic Medical Records, practice enhance-ments, CME funding, and that sort of thing.
I’ve been pretty impressed with my experience with the SMA to date, and I look forward to an ongoing relationship with them based on everything that they seem to do for physicians in the province.

10 Autumn 2012 SMA News Digest
Communities seek input from physicians to address local concernsBy Nicole Quintal
Collaboration is a key word in the overall concept of primary health care.
The success of a health care system does not rest in the hands of one particular group, but is measured by the involvement of many different players. Communities, health care providers and patients must all be engaged and involved with designing a system tailored to their specific health care needs – and several stakeholders are stepping up to the plate.
The Heartland Regional Health Authority (HRHA) approached the Saskatchewan Medical Association (SMA) to provide rural-physician support information at its community consultation on July 18 – the third consultation the region has hosted with municipal officials in the area to address local health care pres-sures and needs. The SMA was also approached by the West Central Municipal Government Committee (WCMGC) and Touchwood Agency Tribal Council to provide similar informa-tion at council meetings in August and September.
Dr. Brian Geller, the SMA’s Director of Professional Affairs, says it is unprecedented to have three stakeholders approach the SMA in such a short span of time.
“This is the first time that communities have been proactive in asking the SMA to present physician support information,” Dr. Geller said. “Ordinarily these requests have centred around a crisis.”
Christa Garrett, HRHA Coordinator of Executive and Medical Affairs, said the idea for the region to host a community con-sultation was inspired during a meeting with the WCMGC, a committee which consists of officials from throughout west-central Saskatchewan who discuss municipal issues of mutual concern. She said physician recruitment was high on the agen-das of many of the communities.
“We need collaborative relationships with community part-ners because there are many players required to support new physicians when they are considering and then resettling in our communities,” Garrett said.
While stakeholders and communities are taking a more proac-tive approach toward addressing local health care needs, Dr.
Geller says physicians need to do the same ‘soul searching’ and ask themselves questions such as ‘what exactly do I need?’ and ‘what exactly do I need to provide?’
“Everyone needs to realize that the post World War Two physi-cian who was everything to everyone is completely unsustain-able in today’s world,” he explained.
He says ultimately it’s about needs and expectations; what do physicians expect from their communities and what do commu-nities expect from physicians and other health care providers.
“You do have to have that conversation that everyone’s been avoiding,” he said. “There is no such thing as a couple’s coun-sellor for communities and physicians, but that’s what needs to happen.”
Dr. Geller says it is a great first step and encouraging that com-munity groups are starting to ask questions and gather infor-mation about the physician programs and services available. In the same breath, he encourages physicians, hospitals, and other health care providers to think about what they bring to the table and collaborate with communities to determine what is reasonable for a community to expect and a physician to provide in terms of health care delivery.
“There is no such thing as a couple’s counsellor for communities and physi-cians, but that’s what needs to happen.”
-Dr. Brian Geller
your SMA

SMA News Digest Autumn 2012 11
your SMA
Frequently Asked QuestionsWhat is the Saskatchewan Electronic Medical Records (EMR) Program?The Saskatchewan EMR Program was created to assist physi-cians with the adoption and implementation of Electronic Medical Record systems. Through a joint initiative between the Saskatchewan Medical Association (SMA) and the Sas-katchewan Ministry of Health, physicians in Saskatchewan can receive ongoing funding and change management support to adopt one of the approved EMR solutions.
Who are the approved EMR vendors with the Saskatch-ewan EMR Program?• Med Access• MD Physician Services• Optimed
What support does the EMR Program offer?The Saskatchewan EMR Program will assist physicians, free of charge, throughout the EMR decision-making and implemen-tation process through services such as: providing an introduc-tion to the program, assessing feasibility to move to an EMR, converting from an existing EMR, assisting with pre-imple-mentation planning, assisting with implementation, go-live support, post-implementation support and Electronic Labora-tory Results integration.
How much will implementing an approved EMR cost me?Estimating the cost to implement an approved EMR in a practice is not an exact science. Most practices experience hard costs such as the purchase of the hardware, software licenses, new office fixtures to accommodate technology, etc., which will depend upon the precise specifications and needs of the practice. Once the practice’s specific needs are addressed, quotes can be obtained from the approved EMR vendors, as well as hardware vendors if required. Every EMR vendor has negotiated a pricing model with the Saskatch-ewan EMR Program.
What type of funding does the Saskatchewan EMR Pro-gram offer?• A fee of $1 for each visit/consultation service documented
in the EMR, which contains sufficient information to meet the profession’s generally accepted standard for medical records.
• A monthly fee of $300 (paid quarterly) to commence once the physician successfully documents and maintains 50 per cent of approved visits via the EMR. This fee shall continue through the first year of EMR operations, after which at least 95 per cent of approved visits must be suc-cessfully documented and maintained on an on-going ba-sis for the payment to continue.
• To encourage early adoption and to recognize that there

12 Autumn 2012 SMA News Digest
your SMA
are fewer benefits to the physician in the first years of the program due to fewer electronic health care services, bo-nus payments will be made available in the amount of:
o $200 per month (paid quarterly) until the first clini cal data interface (Electronic Laboratory Results Re pository) is available to the qualifying electronic medical record systems. o $100 per month (paid quarterly) until the second clinical data interface is integrated (PIP-Pharmaceu tical Information System) is available to the qualify ing electronic medical record systems.
How long will the funding last?The $300 monthly and $1 per visit payments will be ongoing for the period of time the Saskatchewan EMR Program is fund-ed by the Saskatchewan Ministry of Health and the SMA, which at this time no end date has been determined. Further to this, a physician’s funding is also dependent on maintaining funding status through meeting utilization and privacy requirements set out by the Saskatchewan EMR Program.
I have an EMR that isn’t one of the approved vendor prod-ucts. What do I need to do to get funding for an EMR?Any physician using an EMR that is not one of the approved ven-dor solutions must convert their practice to an approved ven-dor’s solution in order to receive funding. Saskatchewan EMR Program services will be available free of charge to physicians who decide to convert to an approved EMR vendor solution.
What Electronic Health Record (EHR) services are current-ly available and when will the rest be available?Currently, Standardized Electronic Laboratory Results are be-ing delivered to EMRs across Saskatchewan. Preliminary work is being performed to integrate Pharmaceutical Information Program (PIP) data electronically to the approved EMRs. For information on how to get Electronic Laboratory Results and updates on upcoming services that will be integrated with the EMR please contact the Saskatchewan EMR Program.
What is a Master Standing Agreement?The Master Standing Agreement is the legal contract between the SMA and each vendor which defines the specific require-ments both parties must abide by. It includes specific vendor requirements regarding service levels, support, pricing model, conformance testing and interoperability with EHR they must meet when working with a practice.
What is Conformance Testing?Conformance Testing is a process of ensuring that external software vendors’ products are ready to receive clinical data through eHealth Saskatchewan via standardized interfaces.
Conformance Services is responsible for integrating eHealth Saskatchewan Electronic Health Record applications with Point of Services systems (such as Pharmacy and EMR).
What is the Peer-to-Peer Program?eHealth Saskatchewan started its Peer-to-Peer Program in 2008 in conjunction with a Canada Health Infoway initiative to advance the adoption of the EHR. By offering clinical sup-port, advice and guidance from your colleagues who have early experience using an EHR product or solution in their own practice, your practice will benefit from a peer’s experi-ence and be better positioned to provide improved care and safety to your patients.
What is the cost of having Peer-to-Peer service and how long does it last?There is no cost to you to use this service. Peers are reim-bursed for their lost clinical time and for their travel expens-es by eHealth Saskatchewan. eHealth Saskatchewan is com-mitted to providing ongoing funding to this program. The length of time of an engagement will be determined during your first meeting with a peer, once they have a better un-derstanding of your situation. Typically, a peer will meet with a colleague about three times depending on the nature of the issue being addressed.
How do I communicate my interest in enroling in the Sas-katchewan EMR Program?The first step in enroling in the Saskatchewan EMR Program is to complete an ‘Expression of Interest’ form, which is found on the SMA website: www.sma.sk.ca/emr.aspx.Submitting an ‘Expression of Interest’ form creates the op-portunity to meet with a Saskatchewan EMR Program Change Management Advisor and discuss the services available.
For more information, contact the Saskatchewan EMR Program:Phone: (306) 244-2196 or toll-free at 1-800-667-3781Email: [email protected]/emr.aspx

MD Physician Services provides financial products and services, the MD family of mutual funds, investment counselling services and practice management products and services through the MD group of companies. For a detailed list of these companies, visit md.cma.ca. TM Trademark of the Canadian Medical Association, used under licence.
Physicians First™
MD is the only wealth management firm that delivers medical practice incorporation advice engineered exclusively for physicians. Our clients benefit from the insight of a team of 250-plus trained incorporation experts who have been establishing best practices and producing powerful results since 1976. If you want to seize investment opportunities, save taxes, and achieve greater financial security, there’s only one choice.
The First . The Best . THE ONLY ONE.
Eileen Maltinsky VP Taxation Services and the Physician Incorporation Strategy Team
Talk to an MD advisor today.1 877 877-3707 l md.cma.ca/incorporation
MDPS032_Incorp_FullpgAd_SMA_v1.indd 1 12-05-16 11:43 AM

14 Autumn 2012 SMA News Digest
your SMA
CME: regular claim submission importantIn order to utilize your CME Fund entitlement, it is impor-tant to be submitting your claims on a regular basis. For any unclaimed CME activity from 2011 and any activity done to date in 2012, please make your submission now. A copy of the CME application form can be obtained by calling the SMA office, or going to the SMA website at sma.sk.ca. If you wish to discuss your CME activity or entitlement available, please contact Joelle Kostiuk, Membership Administrator, at (306) 244-2196 or [email protected].
Correct claims cornerBy Allan Florizone
After-hours premiums for work performed by residents
Q. When I bill for after-hours services provided by my resident, I enter the appropriate out-of-hours location code, and receive a premium. Is it appropriate to receive an out-of-hours payment for work done on my behalf by a resident?
A. The SMA Tariff Committee and the Payment Schedule Review Committee have both re-cently confirmed this as an acceptable billing practice. Our previous guidance on this issue (in 1998) indicated that billing for work done by residents was not acceptable, based upon the position taken (at the time) by MSB’s Medical Director and the SMA Intersectional Council. We were asked to revisit this policy, based upon the fact that the super-vising physician maintains responsi-bility for the patient after-hours, and is frequently consulted by the resident when problems occur.
Billing Quebec patients
Q. I am looking for guidance on the best way to bill for ser-vices provided to a patient from Quebec.
A. Quebec is the only jurisdiction in Canada without recipro-cal billing arrangements with other provinces (i.e. you can’t bill MSB and have them recover the money from the Quebec gov-
ernment). The SMA recommends that physicians bill Quebec patients directly using Saskatchewan’s
insured Payment Schedule rates. Be sure to include sufficient information about
the service (patient name, birth-date, service location, ICD and ser-
vice code) so that patients can seek reimbursement from the Quebec government. Because their government will reim-burse only at (typically lower) Quebec rates, the patient’s reimbursement will almost
always be less then what they paid in Saskatchewan. Patients
should be encouraged to send their concerns/complaints to the Quebec
government, as this will be the only way current policy is changed.

SMA News Digest Autumn 2012 15
Dear members,
On behalf of the SMA Board of Directors, we would like to present the strategic plan highlights from 2010 to
2012 to-date.
With this report, we wanted to provide you with an update on the progress we are making on each stragegic prior-
ity. Each target is tied to a performance measure which indicates how well we are doing at achieving each of our
four strategic priorities. The overall results are encouraging, but we still have work to do. We trust that you will
find this report helpful in keeping you informed about your association’s progress.
Kind Regards,
Dr. Janet ShannonSMA President
Dr. Vino PadayacheeChief Executive Officer
SMA Highlights 2010-2012

16 Autumn 2012 SMA News Digest
SaskatchewanSetting the course for success…The Saskatchewan Medical Association is dedicated to the ideals of our mission statement and turning it into reality for our members, staff, and patients. The SMA mission provides direction and purpose for the Association and those who work within it. Our daily actions should reflect our mission in everything we do.
To ensure that we are attuned with our mission, the SMA Board has developed four strategic priorities that form the basis of our Strategic Plan.
Our missionTo advance the educational, professional, and economic welfare of Saskatchewan physicians;
To advance the honour and integrity of the profession; and
To promote quality health care practices, quality health services, and advocate for a quality health care system for Saskatchewan.
STRATEGIC PRIORITY #1: Enhance physician well-being
STRATEGIC PRIORITY #2: Be the voice of Saskatchewan physicians
STRATEGIC PRIORITY #3: Enhance relationships with members
STRATEGIC PRIORITY #4: Advance physician leadership

SMA News Digest Autumn 2012 17
Dr. Paul Taillon, SASM President
Our Strategic Plan shapes our priorities for the next three years and builds on the strong foundational principles of our mission. The four strategic priorities guiding the SMA focus on members in the context of the changing health care environment in Saskatchewan.
The goals associated with each strategic priority direct the SMA’s daily activities and provide the association with targets for success.
Enh
ance
physi
cian well-being Be the voice of Saskatchewan physicians
Enhance relat onship with members Advance physic
ian le
ader
ship
Enhance physician leadership skills Promote partcipaton in quality improvement Partner with CPSS, College of Medicine, and HQC - Champions for Quality Improvement
Develop strong RA/RMA/sectons
Leverage SMA communicaton channels and technology for
improved informaton sharing
Expand avenues and opportunites for
member input
Achieve compettve
compensaton
Promote physician and family wellness
Improve retenton of physicians in Saskatchewan
Expand avenues and opportunites for member input
Communicate regularly with key organizatons
Deliver consistent and coordinated messages
Be strategic with media communicatons
STRATEGIC PRIORITY #1: Enhance physician well-being
STRATEGIC PRIORITY #2: Be the voice of Saskatchewan physicians
STRATEGIC PRIORITY #3: Enhance relationships with members
STRATEGIC PRIORITY #4: Advance physician leadership

18 Autumn 2012 SMA News Digest
In July 2012, a new memorandum of understanding (MOU) that provides a non-fee-for-service (NFFS) bar-gaining framework was signed by the SMA and the Saskatchewan Ministry of Health. The bargaining pro-cess will ensure consistency in compensation rates and work/service expectations across the province for NFFS physicians.
Within the MOU, the membership of the Negotiating Committee and Management Committee were set, as were the roles for the SMA, the Ministry and the Re-gional Health Authorities. The negotiating processes for both existing contracts and new contracts were outlined, while the processes for dispute resolution in non-compensation and compensation related dis-putes were also outlined.
The MOU is intended to align the bargaining frame-work with the patient first focus, which, among other objectives, will provide for a financially responsible and sustainable process for the negotiation framework for physician services and establish a fair, transparent and standardized approach that aligns with the strategic priorities of the health care system.
STRATEGIC PRIORITY #1: Enhance physician well-being
Measure Target Perfor-mance
Commentary
Achieve competitive compensa-tion
Alberta/BC average. 100% of target
Fees are competi-tive with Alberta/BC average* The four-year (2009-2013) fee-for-service agreement was secured in January 2011.
Improve physician retention
Improve 5-year retention rate by 1% annually.
Retain an average of 75% of our med school graduates annually within five years.
50% of target
The five year retention rate re-mains steady, but is not on target.
Room for improv-ing retention of med school graduates/resi-dents.
Promote physician and family wellness
100% of members and their families contact-ing the physician support program for as-sistance will receive it.
Implement an annual wellness conference aimed at physicians’ spouses.
100% of target
100% of target
Since 2010, all physicians, residents, stu-dents and family members request-ing assistance received it.
The second an-nual spousal edu-cation session was held May 4, 2012 with 26 attendees.
* Based on Canadian Institute of Health Information (CIHI) payment schedule comparison data, updated by the SMA to account for recent payment schedule increases, Saskatchewan’s fees now slightly exceed the Alberta-BC average.
PHYSICIAN HEALTH PROGRAM
This program assists physicians, physicians in training and their families who are struggling with physical, men-tal, personal, relational and addiction issues. Confidential referral, intervention and on-going supports are avail-able to physicians and their families. Initiatives under this program include self reflection tools on the SMA website, presentations at each Representative Assembly, educa-tion sessions with students, residents and physicians,
the Physician Wellness Initiaitve and annual spousal education sessions.
In 2011, 133 people accessed the Physician Health Program for assisstance, while 70 people have accessed the program to the end of August 2012.
PHYSICIAN RETENTION
The five year retention rate remains stable between 77 per cent and 78 per cent for the last year. This represents no real change from previous numbers and pos-sibly a small decline from 2011 numbers which were closer to 78.3 per cent.
Saskatchewan’s retention rate remains higher than the Canadian average of 72 per cent. Retention activities would have to dramatically increase to affect the re-tention rates by the target of one per cent annually.

SMA News Digest Autumn 2012 19
STRATEGIC PRIORITY #2: Be the voice of Saskatchewan physicians
Measure Target Perfor-mance
Commentary
Expand avenues and opportuni-ties for mem-ber input
100% of commu-nication vehicles promote two-way communication opportunities for members.
100% of target
All SMA communica-tion vehicles offer two-way communica-tion opportunities. Social media such as Twitter and Facebook have expanded the avenues available for members to com-municate and interact with the Association.
Increase regular com-munications with key or-ganizations
SMA has input with key organiza-tions on 100% of the decisions that affect physicians.
90% of target
The SMA has worked to build relationships with the Saskatch-ewan Ministry of Health and organi-zations such as the Physician Recruitment Agency of Saskatch-ewan.
SMA representatives work closely with these organizations to ensure doctors have input on key deci-sions.
Deliver con-sistent and coordinated messages
SMA position de-livered with 100% accuracy.
100% of target
SMA representatives accurately presented the position of the organization 100% of the time.
Be strategic with media communica-tions
SMA messag-ing is reported accurately and balanced on all issues of strategic importance.
100% of target
SMA messaging was reported accurately and balanced fairly on all topics of strate-gic importance.
While the SMA does not have input on 100 per cent of the decicions that affect physicians, the organization is making progress in this area by nurturing relation-ships and alliances with key organizations.
The SMA and Saskatchwan Ministry of Health are working closer as part of the province’s commitment to strengthen health care in rural Saskatchewan. Dr. Vino Padayachee, Chief Executive Officer (CEO) of the SMA accompanied Minister responsible for Rural and Remote Health, Randy Weekes, on a visit to Nova Scotia, where they toured Collaborative Emergency Centres to gain a first-hand perspective on their op-erations and applicability in Saskatchewan.
The SMA has been asked for input on issues such as pooled referrals and clinical pathways. The SMA will insist that these initiatives be refined to provide real benefits for physicians and patients.
In early 2011, the SMA undertook three joint surveys with the Physician Recruitment Agency of Saskatch-ewan (SaskDocs). The surveys covered three groups of physicians: Those who left the province, those who are new arrivals in the province, and student and resi-dent physicians. Recritment and retention efforts are coordinated between the SMA and SaskDocs.
COMPREHENSIVE CARE PROGRAM
In July 2012, the Ministry of Health and SMA an-nounced the new Family Physician Comprehensive Care Program, which provides $9.83M in funding to encourage and reward family physicians in pro-viding patients with a full range of services. The announcement of this program resulted in front-page stories in both the Regina Leader-Post and Saskatoon StarPhoenix, featuring an interview with SMA Vice President Clare Kozroski.
The SMA is committed to work with the Ministry to further refine this program so that it can fully meet its objectives.

20 Autumn 2012 SMA News Digest
STRATEGIC PRIORITY #3: Enhance relationships with members
Measure Target Perf Commentary
Develop strong RA/RMA sections
10% annual increase in RA delegate atten-dance.
100% of RMAs fill their executive positions and communicate with the SMA.
Within two years, 100% of sections have adopted a constitution and designate formal representatives.
0% of target
50% of target
75% of target
The SMA is working to in-crease member attendance and participation at the RA, RMA, and section levels.
Ten of 12 RMAs have a full, elected executive. Only one RMA regularly sends the SMA their minutes, although the SMA commu-nicates with all RMAs.
Improve informa-tion shar-ing and member connec-tivity
10% rise annually in number of SMA members using the website.
10% rise annually in number of SMA member groups using the work-rooms.
Within two years, have an email failure rate of less than 5%.
75% of target
0% of target
On target
Members are using the information on the SMA website, although statistics show the overall use of the website has stagnated.
Not all members are utiliz-ing these services. The number of members using these services has gone down since 2011.
Access to resources and sup-port
Members have access to the information resources they require.
75% of target
Information about SMA programs and services are available to members online and in print.
The SMA is working on providing better access to CMA resources through the SMA website.
Optimize technol-ogy
60% of physicians to adopt an EMR by the end of 2012.
On target
Over 53% of SK physicians have adopted an EMR and are receiving funding.
Representative Assembly (RA). Out of a possible 83 delegates, 55 attended the Spring 2012 RA in Regina and 54 attended the Fall 2011 RA in Saskatoon. The SMA’s goal is to increase delegate attendance, al-though that has plateaued. The SMA will continue to pursue activities to attract more delegates to the RA and RMA meetings, such as providing:• Online access to reports and information• Interactive sessions • Delegate homework • CME credits
Regional Medical Associations (RMAs). To date, eight of the 12 RMAs have shared their updated consti-tutions with the SMA, which is one more than in 2011. All RMAs have a president, and 10 of 12 have all of their executive positions filled. The SMA currently exchanges information with each of the RMAs annually during the President’s Tour.
Sections. There are currently 25 sections of the SMA. Of these, 23 are represented on the Intersectional Council, which is unchanged from 2011. The two va-cancies are general surgery and pathology. Twenty of the sections have formal constitutions with formal representatives.
Three membership guides, one for general members and one each for students and resi-dents, were printed in 2012. These guides will be updated and distributed annually.
SMA News Digest Autumn 2012 21
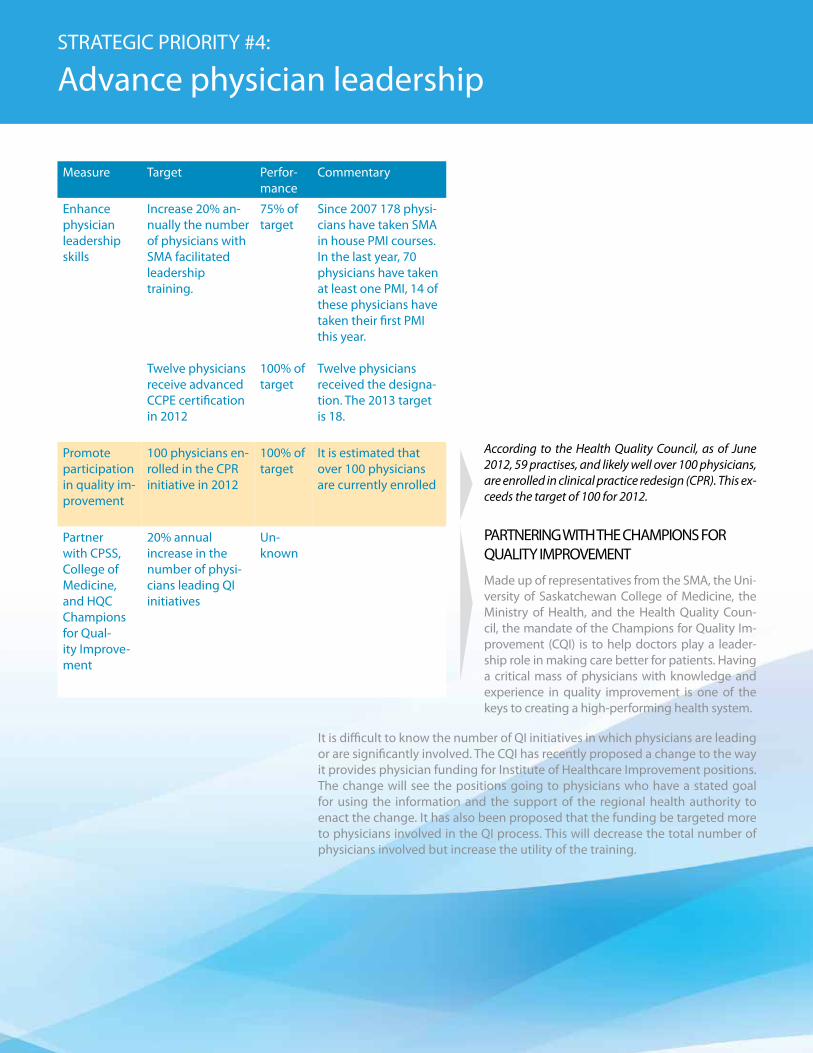
Measure Target Perfor-mance
Commentary
Enhance physician leadership skills
Increase 20% an-nually the number of physicians with SMA facilitated leadership training.
Twelve physicians receive advanced CCPE certification in 2012
75% of target
100% of target
Since 2007 178 physi-cians have taken SMA in house PMI courses. In the last year, 70 physicians have taken at least one PMI, 14 of these physicians have taken their first PMI this year.
Twelve physicians received the designa-tion. The 2013 target is 18.
Promote participation in quality im-provement
100 physicians en-rolled in the CPR initiative in 2012
100% of target
It is estimated that over 100 physicians are currently enrolled
Partner with CPSS, College of Medicine, and HQC Champions for Qual-ity Improve-ment
20% annual increase in the number of physi-cians leading QI initiatives
Un-known
STRATEGIC PRIORITY #4: Advance physician leadership
According to the Health Quality Council, as of June 2012, 59 practises, and likely well over 100 physicians, are enrolled in clinical practice redesign (CPR). This ex-ceeds the target of 100 for 2012.
PARTNERING WITH THE CHAMPIONS FOR QUALITY IMPROVEMENT
Made up of representatives from the SMA, the Uni-versity of Saskatchewan College of Medicine, the Ministry of Health, and the Health Quality Coun-cil, the mandate of the Champions for Quality Im-provement (CQI) is to help doctors play a leader-ship role in making care better for patients. Having a critical mass of physicians with knowledge and experience in quality improvement is one of the keys to creating a high-performing health system.
It is difficult to know the number of QI initiatives in which physicians are leading or are significantly involved. The CQI has recently proposed a change to the way it provides physician funding for Institute of Healthcare Improvement positions. The change will see the positions going to physicians who have a stated goal for using the information and the support of the regional health authority to enact the change. It has also been proposed that the funding be targeted more to physicians involved in the QI process. This will decrease the total number of physicians involved but increase the utility of the training.

22 Autumn 2012 SMA News Digest
health care
client &familycentred care
By Dallas Carpenter
The Saskatoon Health Region is on the leading edge of a movement designed to centre hospital care around the patient, involving families, physicians and other care
providers in a process that provides choice and empowers peo-ple to improve their health.
Client and Family Centred Care was formally adopted by the Region five years ago as a way to change the delivery and evaluation of healthcare. They envisioned it as a way to build partnerships between clients (the Region’s term for patients), families and care providers that would better meet the needs and expectations of clients. The partnerships are built around the pillars of respect and dignity, information sharing, partici-pation and collaboration, involving each stakeholder in a way that encourages communication continuous improvement in the delivery of care.
“One of the most significant strategies we have implemented is the establishment of patient-family advisory councils in our acute care, care groups,” explains Malori Keller, the former Client and Family Centred Care Specialist for the Saskatoon Health Region who recently moved on to the Saskatchewan Transplant Program. “On those councils, we have patients, families, staff and physicians, where possible. We always need more physicians there because physicians help bring patient and family-centred care at the bedside to life. There is a lot to be learned from meeting with patients and families on a regu-lar basis to identify what is working well and where we may be able to improve with regard to respect, dignity, information sharing, participation and collaboration. ”
The concept of patient and family-centred care started gain-ing prominence in the early 1990’s, focusing mainly on family-centred care and taking pediatric care to a new level. In Sas-katoon, that shift happened in 2005 in Maternal Child Health Services with initial efforts focused on staff education, sharing patient and family stories and changing practices such as visit-ing hours. Some of the first activities included the removal of
prohibitive signage and reno-vations to waiting rooms.
There have been a num-ber of positive changes brought to the Saska-toon Health Region by the Client and Fam-ily Centred Care team. However, as Keller explains, the founda-tion of the program is the meaningful partner-ships that have been cre-ated.
“The Region chose to establish advisory councils where clients and families who had experienced care or service in an area would be able to become a member for a stated period of time,” she says. “This helped to build relationships where we could have open discussions and learn on an on-going basis from these individuals. This has proven to be very beneficial and helps us to dive deeper into topics than a survey or focus group would.”
The opinions and of clients and families are valued beyond the levels they have the most contact with. The Saskatoon Health Region seeks to engage clients and families at the facility and organizational level to get their perspectives in areas such as facility design, patient safety, ethics, education and quality im-provement.
“At the organizational level,” continues Keller, “we have a steering committee that supports our regional directions, our priority setting and provides assistance in the design of new spaces like the children’s hospital. System-wide, across the province and across Canada, we need to have patient families advising us on the needs of the healthcare system, the types of

SMA News Digest Autumn 2012 23
health care
familyprograms and services we provide, and how we provide those services.”
Although the term “client” is used to refer to the hospital pa-tient or facility resident, it is not about treating the client as a
customer.
“One of the myths that I talk about in staff training is that patient and family-
centred care is not about customer service,” says Keller. ”It is about
respect and dignity. It’s not the expectation of patient and
family-centred care that you have to do everything the patient or their fam-ily wants. That’s some-times just not possible. It’s about meeting their needs, values and pref-erences to the greatest degree possible and en-
suring that at all times we preserve their dignity.
If there are times you can’t meet those wants, explain why
you can’t in an appropriate man-ner.”
Having physicians buy into the program has been critical to the evolution of Client and
Family Centred Care in the Saskatoon Health Region.
“We have some really good examples of where the staff and physicians have worked together to make changes to their processes and practices to improve the experience of the pa-tients and families” says Keller. “One example is in our criti-cal care units, where our patients and families have the option to participate in bedside rounding with their physicians and their interdisciplinary care team. Many physicians report that they feel it is saving them time as the team collaborates and discusses the care plan together and it is helping them com-municate with patients and their families. This is one example where physician support and buy-in really helped us to move forward a best practice.”
With the recent implementation of innovation and efficiency programs such as Lean, it appears that programs such as Cli-ent and Family Centred Care could get pushed aside as health-care providers shift their focus to efficiency. However, as Keller explains, the activities undertaken through Client and Family
Centred Care may have put the Saskatoon Health Region fur-ther along the innovation process, especially when it comes to Lean.
“Patient and family-centred care is very complimentary to Lean,” she says. “Lean uses patient-family experiences to help drive change. Patient and family-centred care is a precursor, in some respects, to Lean in that you have to have to have pa-tients and families involved to share their experiences and par-ticipate in Lean events.
“In the Saskatoon Health Region, we are using our patient/family advisors to fill this role. Their previous participation as advisors helps them to feel more comfortable participating in these events and they may know of some of the history of quality improvement or perhaps had the opportunity to learn about best practices in their previous work that would be rel-evant to the Lean event. Thus, when they participate in a Lean event, their experience in patient and family-centred care can provide a foundation for how innovation can be applied and what practices will deliver results.”
The Saskatoon Health Region has been recognized provincially and nationally for their approach to client and family-centred care and the innovations they have put in place. Interest from other health regions in Saskatchewan is particularly strong, as they work on implementing patient and family focused chang-es with limited resources.
Last June, Keller along with Kathleen Peterson from the Minis-try of Health, made a presentation to the Institute for Patient and Family Centered Care International Conference on the way the region and province are implementing changes.
“They’re very interested in what we’re doing here in Saskatch-ewan,” she says. “They’re interested in the way we are imple-menting client and family-centred care, because we’re doing it system wide. First of all, we have a government that has com-mitted that we are to be engaged in client and family-centred care, which is very different from other areas.
“Specifically, what we are doing here in the Saskatoon Health Region is building an infrastructure by having a set of adviso-ry councils across care streams. What we did was take it one step closer to the bedside in our organizational structure. So instead of being at an organizational level, we have advisory councils at the department level. It’s the scope and the quick pace we are doing this in that has received attention. We will have 13 advisory councils set up now and will have more by the end of the year, and that is a lot to have accomplished in only a few short years.”

24 Autumn 2012 SMA News Digest
Clinics encouraged to work with RHAs when bringing IMGs to SaskatchewanBy Nicole Quintal
The Saskatchewan International Phy-sician Practice Assessment (SIPPA)
has been fully implemented since May 2012, and as with any new program, us-ers may be unsure of some of the final program details.
There is one uncertainty currently on the horizon in terms of private clinics who recruit family medicine Interna-tional Medical Graduates (IMGs) indi-vidually; some private clinics were under the impression they would be excluded from the SIPPA process as a means to as-sess potential candidates’ readiness to practice in Saskatchewan.
This is not the case, says Dr. Penny Davis, Physician Program Director of SIPPA at the University of Saskatchewan’s College of Medicine.
Dr. Davis explained that SIPPA offers 30 seats for family medicine IMGs in each of three iterations per year starting in January, May and September. Regional Health Authorities (RHAs) hold two seats each and can nominate IMGs re-cruited to areas of need for these spots. As a result, there are additional seats for private clinics to submit candidates who have been identified as eligible by the College of Physicians and Surgeons of Saskatchewan.
“There are still eight seats at the end of the selection process, even after the re-gions have nominated candidates, so we have actually put some people through already who were privately recruited,” she said.
However, Dr. Davis says private clinics are encouraged to speak with their RHA
if they are interested in bringing a candi-date to Saskatchewan.
“If a private clinic has contact with somebody who wishes to come to Sas-katchewan, we encourage them to talk with their region,” she explained. “The regions are really looking for people who are going to come into the country and stay, and if candidates are recruited by a friend or a clinic that they know, they will be more likely to stay.”
She added that the RHAs and Saskdocs prioritize candidates based on the needs of both the region and the recruitment agency, so rural physicians are often more likely to have priority.
Dr. Davis suggests those interested in bringing a candidate to Saskatchewan contact their RHA recruiter as soon as possible for assistance with completing all necessary paperwork.
SIPPA reviewedDr. Davis says SIPPA has been received well overall, garnering a reliable review from a statistician who determined that the program should be repeated.
“We also had an internal review of just
the program content where we surveyed all the candidates who’d gone through. They were generally pleased with what we provided them with and gave us quite a few good suggestions for later,” she said.
Four iterations went through the pilot version of the program, and one itera-tion has gone through the fully-imple-mented program, says Dr. Davis. Twenty-four candidates are currently enrolled in the latest iteration.
“Through the pilot session we had a pass rate of around 80 per cent, which certainly is comparable with the previ-ous process when they went through the Clinician Assessment and Physician En-hancement Program (CAPE),” Dr. Davis said.
The long-term goal of SIPPA is to have 90 candidates per year through the as-sessment, while CAPE put forth about 55 candidates; however, Dr. Davis says al-though SIPPA would like to pass as many candidates as possible, there are strict rules on the passing marks so she antici-pates over time that the proportion of successful candidates will decrease.
health care
“There are still eight seats at the end of the selec-tion process, even after the regions have nominated candidates, so we have actually put some people through already who were privately recruited.”
-Dr. Penny Davis

SMA News Digest Autumn 2012 25
health care
From CAPE to SIPPAThe SIPPA process was designed to as-sess family medicine IMGs for readiness to practice in Saskatchewan. It began as a pilot project in January 2011 before mov-ing into full implementation in May 2012.SIPPA replaces the former CAPE pro-cess, where physicians would come to the province and work for up to three months before being sent to Manitoba to be assessed. This resulted in IMGs leav-ing their practices for several days to be assessed, and often needing to leave again for up to three months of upgrad-ing or even receiving a negative assess-ment and having to leave the province. This process was considered to be dis-ruptive to patients, communities and physician practices.
“The difference in this program [SIPPA] is that although the candidates are re-cruited to a region they don’t start to work there until they’ve been through an orientation and evaluation program,” Dr. Davis explained.
The new process is also Saskatchewan-based. Orientation is approximately 10 days to two weeks in duration and is followed by a series of examinations. Another week of orientation follows, which informs physicians of the con-text and practicalities of practising in Saskatchewan, such as how the air am-bulance service works and how to access information through the Saskatchewan Health Information Resource Partner-ship (SHIRP). This is followed by a six- or
12-week clinical assessment, depend-ing on in which country the doctor was trained.
Doctors who trained in the original six countries approved for licensure in Sas-katchewan (United Kingdom, United States, Australia, Ireland, New Zealand and South Africa) are required to under-go six weeks of training, while doctors from countries outside of those com-plete the 12-week program. Candidates are then issued an enduring license.
“We are hoping this will be a successful and physician-friendly program,” said Dr. Davis.
Saskatchewan has traditionally been dependent upon international medical graduates (IMGs) to provide health care delivery. The overall percentage of physicians providing care who are IMGs is approximately 53 per cent, and there is a higher percentage of family physi-cians in rural centres who obtained their training outside Canada.

26 Autumn 2012 SMA News Digest
health care
Surgical checklist: A near miss...or a good catch?Submitted by the Saskatchewan Surgical Initiative
Lynn Cushway, a Clinical Nurse Educator at Royal University Hospi-tal, tells a story that demonstrates a province-wide cultural change. It’s a positive change that began with the implementation of the surgical safety checklist.
Cushway recounts the event: “One of our resource nurses said to me, ‘you know, a horrible thing happened to us the other day. We were in a case and when I turned around from set-ting up my back table, the patient was asleep. We realized we had forgotten to do the briefing and everybody felt awful.’”
When the checklist was introduced, the same nurse may have felt embar-rassed about finding mistakes. Now, having seen how the checklist catch-es anomalies while there’s still time to fix them, she has come to see those near misses as good catches.
“I think it’s great,” says Cushway. “Instead of thinking of this as a bad thing, think about how far we’ve come. A year and a half ago, we would have forgot to do the briefing and it would have been no big deal, but now it’s become inherent in what we do.”
Dr. Corrine Jabs agrees. As the de-partment head of obstetrics and gy-necology in the Regina Qu’Appelle Health Region and the physician lead for the checklist in that region, she looks forward to seeing the next gen-eration of surgeons and obstetricians.
“They’ll have no difficulty incorpo-rating the checklist into their prac-tice because they’ve learned it while they’ve been in training,” she says. “It
will be as automatic and as comfort-able as putting on their seat belt.”
The surgical safety checklist is espe-cially valuable because it supports
established patient safety standards and can be adapted with minimal resources to any situation. When a surgical team makes a nice catch by
using the checklist, they’re protect-ing their patient, all while improv-ing surgical flow and saving time in the operating room. All 10 health re-gions where surgery is performed are working toward using the checklist 100 per cent of the time.
What is a nice catch in the operat-ing room? It’s picking up on the fact an antibiotic was not given before starting a procedure. It’s discover-ing equipment is missing or doesn’t work. It’s finding out the patient for-got to tell you about an allergy. Ac-cording to Margaret Farley, a Clini-cal Development Educator at Regina Qu’Appelle Health Region, “it’s not just the ‘great save’ such as a wrong site surgery; it’s catching all the small details.”
Use of the surgical safety checklist is part of the continuous improvement approach in Saskatchewan’s health system.
An operating room team at Regina General Hospital goes through the checklist before starting surgery. (Courtesy Regina Qu’Appelle Health Region)
“They’ll have no difficulty incorporating the checklist into their practice...it will be as automatic and as comfortable as putting on their seat belt.”
- Dr. Corrine Jabs

SMA News Digest Autumn 2012 27
students and residents
By Nicole Quintal
Students couldn’t have asked for a more perfect day as they ventured out on August 18 amongst sunshine and +25 degree temperatures to Shellbrook and Me-
morial Lake for the annual Student Medical Society of Sas-katchewan’s (SMSS) bus tour.
Fifty students headed to the rural community of 1,400 just one day after orientating as new medical students at the University of Saskatchewan’s College of Medicine.
So what purpose would sending students who’ve barely had time to open their textbooks serve?
It’s all part of a strategy aimed at introducing medical stu-dents to rural practice earlier and more often in hopes that they will consider rural practice as a rewarding prac-tice option upon completing their studies.
“We know that creating opportunities for medical stu-dents to have positive experiences in rural Saskatchewan increases the likelihood that they will consider rural prac-tice in the future,” said Dr. Brian Geller, the SMA’s Director of Professional Affairs.
As it sits, Saskatchewan has one of the lowest in-province graduate retention rate in Canada, and it is particularly worse in rural areas. According to Saskdocs, we retained 54 per cent of our own medical graduates (2010-11 figures). The goal is to retain 68 per cent for the current fiscal year.
This year, the SMSS chose the Prince Albert Parkland Re-gional Health Authority (PAPRHA) to take the reins on or-ganizing the SMA-funded tour.
Students were treated to a full day of activities, both medi-cal and recreation-themed, beginning in Shellbrook. They first visited the Hidden Hills of Shellbrook Golf Course be-fore venturing to the under-construction Shellbrook Inte-grated Facility, which is slated to open in September 2013. The new facility will be based on a primary care model, consisting of a 20-bed hospital, 34-bed special care home and community services. Shellbrook is currently one of seven primary health care sites in PAPRHA.
Rural bus tour2012

28 Autumn 2012 SMA News Digest
students and residents
The students also toured the current hospital and local clinic, including the primary health care wing, where they were tasked to rotate through suturing and casting sta-tions, and take blood pressure for the first time.
First-year students Jared Diederichs and Janessa Mah said they decided to participate in the rural bus tour based on advice from their peers.
“I heard from upper-year students that it was a really good experience,” Mah said. “Since I’m from the city, I’ve never really been to any rural areas, so I thought it’d be interesting.”
Diederichs said he thought it would be interesting to see the development of the new hospital.
Both students said it was hard to visualize what the com-pleted project will look like but agreed it was interesting to compare it to the current facility.
“Also a lot of the upper-year students were mentioning the casting and suturing clinics were really beneficial,” Diederichs said.
When asked if they would consider practising in a rural setting upon completing their studies, both Mah and Die-derichs kept an open mind.
“I honestly don’t know right now,” Mah said. “I’ve never really given it too much thought just because I have been in the city all my life, but it’s definitely something I’m open-minded to, and I think this is the first of many expo-sures that we’ll have.”
“I think I definitely would consider [rural practice], be-cause I have a lot of family up in Nipawin so I’ve spent some time in the hospital up there and speaking with some of the physicians, so it’s definitely an option,” Die-derichs added.
During a lunch presentation, local physicians from the PAPRHA, Dr. Nguegno (Shellbrook) and Dr. Senzani (Spir-itwood), offered words of encouragement about rural practice.
“It is enriching beyond words,” Dr. Senzani said to the stu-dents, adding that rural practice is a confidence booster because physicians can engage in a variety of practice.
The students wrapped up the day at Memorial Lake to enjoy the natural beauty of the region while having fun boating, canoeing and relaxing on the beach.
Under the umbrella of the recently launched SMA Roadmap Program for Students and Residents, the SMA is planning upcoming bus tours for second-year (Phase B) students to keep the rural-practice momentum alive.
Phase B students will receive their Roadmap ‘passports’ in October so that they can begin collecting travel stamps. Students will be asked to gather five stamps from five differ-ent rural and regional practice locations. The SMA will take the students to four locations via the bus tours, and stu-dents can then arrange their final practice visit with a rural physician to gain the fifth and final stamp (a list of potential practices to visit will be circulated to students).
Phase B students who gather five travel stamps will receive a grant in the amount of $500 and will also be entered to win a trip to the 2013 Rural and Remote Conference in Victoria, BC.
Stay tuned for more information about this contest in your Roadmap Electronic Travel Update or visit www.sma.sk.ca/roadmap.aspx.
Future bus tours in the works for Phase B students
The under-construction Shellbrook Integrated Facility is slated to open in September 2013.

SMA News Digest Autumn 2012 29
autumn calendar
12-13 Interprofessional Management of Nueropathic Pain ConferenceKeynote speaker: Dr. Pam SquireMoose Jaw, SKTo register, visit www.usask.ca/cme
24-25 AIME: Airway Interventions and Management in EmergenciesRegina, SK (in conjunction with SEMAC)To register, visit www.caep.ca/cpdcme/roadshows-current-cme/aime
25-27 2012 AMA-CMA-BMA International Conference on Physician HealthLe Westin Montréal Hotel, Montréal, QCFor more information, contact [email protected] or visitwww.cma.ca/physicianhealth
26-27 Saskatchewan Emergency Medicine Annual Conference (SEMAC IV)Ramada Hotel, Regina, SKTo register, visit www.usask.ca/cme
26-28 PMI: Self AwarenessSMA In-house PMI ProgramRadisson Hotel, Saskatoon, SKwww.sma.sk.caTo register, phone (306) 244-2196
2-4 Saskatchewan Provincial Medical BonspielCN Curling Club, Saskatoon, SKEntry fee: $200 per team ($50 per individual)To enter a team, email [email protected]
2-3 Fall meeting of the SMA Representative AssemblyHotel Saskatchewan, Regina, SKFor more information, phone (306) 244-2196 or visit www.sma.sk.ca
17 Saskatchewan Thoracic Society 2012 Professional Education DaySaskatoon Inn, Saskatoon, SKFor more information or to register, visit www.sk.lung.ca
23-24 Practical Management of Common Medical ProblemsSaskatoon Inn, Saskatoon, SK To register, visit www.usask.ca/cme
Upcoming courses, conferences and eventsoctober
*PHYSICIAN MANAGEMENT INSTITUTE*
For the latest information on upcoming events, view the events calendar at www.sma.sk.ca
november

2012 Saskatchewan provincial medical Bonspiel
November 2 to 4, 2012Saskatoon, SK
CN Curling Club
Entry fee - $200 per team ($50 per individual)Includes banquet supperGuaranteed three games
Limit of 16 teams
The Saskatchewan Provincial Medical Bonspiel was traditionally held within the prov-ince, rotating between communities such as Melfort, Swift Current, Prince Albert, Kindersley and Humboldt.
It started in 1954 and was held annually until 2000. In an attempt to re-establish this classic event it will be held in Saskatoon on November 2, 3, and 4 (Friday to Sunday) and will be limited to 16 teams.
Please come join us and help re-establish this great tradition.
Email: [email protected] to enter a team today

SMA News Digest Autumn 2012 31
BIOIDENTICAL HORMONE INITIATIVE SYMPOSIUM CLINICAL APPLICATION OF BIOIDENTICAL HORMONES
Saturday, October 27th, 2012 toronto, ON., CANADA
Canada’s most comprehensive BHRT Education Series“ Leading The Way To A Healthier Lifestyle Through Education And Bioidentical Hormone Replacement Strategies ”
Direct : 647.884.0663 (Toronto) | [email protected] www.trubalancehealthcare.com for all details / Agenda
To RegisTeR Please ConTaCT
FACULTY / DR. eRika sChwaRTz, MDDr. Schwartz. Graduate of NYU and AOA, and graduate cum laude SUNY Downstate College of Medicine. Leading expert in the field of BHRT, wellness, and disease prevention. The Founder and Director of a prominent New York medical practice and a Founding Director of the Bioidentical Hormone Initiative. Member of NAMS, MSSNY, ACOG, AFTRA/SAG, NYSSIM and is the president elect of the Alumni Board of Managers and Trustees at SUNY Downstate College of Medicine (2013). Since beginning her distinguished career, Dr. Schwartz has been committed to empowering patients and teaching physicians compassion alongside innovative scientific and clinical approaches. She has lectured at Harvard was the lead author in the Medical Clinics Of North America for three white paper publications on hormones (2008/ 2011).
6 AMA PRA CATEGORY 1 CREDITS approved course by SUNY Downstate College of Medicine. A highly sought after intensive one-day practitioner education symposium which covers the clinical application of BHRT, testing, diagnosis, clinical protocols for men and women, dosage titration, successful application of nutritional supplementation and an extensive review of case studies. Dr. Schwartz will discuss the latest medical evidence presented at the International Menopause Society World Congress in June 2011.
Seminar format will be in small groups and will include significant time devoted to individual participant dialogue, case studies, questions and dialogue of relevant issues encountered in clinical practice.
• Network with Leading Physicians• Scientific Perspectives: IMS, WHI, Million Women Study
OPTIMAL AUDIENCE• Designed for All Healthcare Professionals• Special Hotel & Airfare Rates Available
SYMPOSIUM FEE $899.00 CDN + HSTEARLY BIRD / SAVE $125 / REGISTER BY AUGUST 15TH
Add a staff member for $750Group rates available / Limited Seating! 40 People
140 Wall street, saskatoon •1,996 sF in prime downtown Wall street Medical Building (move-in ready) •suite 240 includes four (4) exam rooms, five (5) offices, lunchroom and washroom •Five (5) on-site secure parking stalls available •Net Lease Rate $17.00/SF Mls®
collierscanada.com/457
KenSuchan*
cell 306 221 1825 dir 306 664 [email protected]
KevinJohnsoncell 306 281 9929 dir 306 664 [email protected]
* ken suchan (ken suchan realty Inc.) has a contractual relationship with Colliers McClocklin real estate Corp.
forleaSe
Downtown Medical OfficeDowntown Medical Office
ColliersMcClocklinrealestateCorp.|+13066644433|www.colliers.com/saskatoon
classifieds

32 Autumn 2012 SMA News Digest
classifieds
A day in the country. The Town of Raymore is welcoming ap-plications for a Family Physician. We are ideally located at the junction of highways #6 and #15, only 112 kilometres north of Regina (apx. 1 hour). The Raymore Health Centre requires a Family Physician one or two days a week, whatever would fit into your schedule; we are open for discussion. Our cur-rent practice covers a 30-mile radius, which includes two First Nations communities. The only cost to you is your staffing for the day. For more information, please contact the Town of Raymore by calling (306) 746-2100 or email [email protected] and look us up on the web at www.raymore.ca.
General practitioner in solo practice is looking for a lo-cum to cover practice in Weyburn, SK for the following dates: November 12 - 30 and December 24 - January 4 and also care for in-patients at hospital. Clinic hours are from 11 a.m. - 5:30 p.m. Please contact us at (306) 842-5404 or email [email protected].
Family Physician Associate - Prince Albert. The South Hill Minor Emergency Clinic opened in 1987 and was one of the first walk-in clinics to open in the province. We expanded in 2002 to in-clude family practice care. The complex has offices for many pro-fessional services. We also use EMR charting provided by Optimed/Accuro software. We offer an already established patient base with great earning potential. If you are interested in discussing a posi-tion with our clinic, please contact: Dr. J. N. Kriel at (306) 981-4611 or email [email protected]; Dr. S. Lombard at (306) 981-8100 or email [email protected]; or, Dr. L. N. deBeer at (306) 961-8783 or email [email protected].
Wanted: Locum/partner in a well established clinic with local hospital privileges. Contact (306) 937-7705 or (306) 937-7776.
Opportunity for family physician in a busy west-side Sas-katoon practice with three full-time physicians. Both part-time and full-time opportunities available with potential for association. Please contact Dr. Hussain at (306) 384-7800 or (306) 384-7550 (fax) or email [email protected].
PHYSICIAN OPPORTUNITIES
ANNOUNCEMENTSThe SMA and EMR Program are pleased to welcome new Pri-vacy Officer, Darcy Hryn. Darcy is available to help members with any questions or concerns they may have in regard to meeting privacy and security requirements.
Certification opportunities for physicians - The SMA would like our members to know about opportunities to ob-tain their CCFP (Certification in The College of Family Phy-sicians) or CCPE (Canadian Certified Physician Executive) certification.
The CCFP-ARC pilot project is a University of Saskatchewan College of Medicine initiative that provides support to fam-ily physicians who are interested in following the CFPC’s Al-ternate Route to Certification pathway to obtain their CCFP designation. A subsidy of $1500 is available to offset regis-
tration fees. For further information please contact Ms. Gail Greenberg at (306) 537-2430 or [email protected].
Developed by the Canadian Medical Association (CMA) and the Canadian Society of Physician Executives (CSPE), the CCPE credential is designed to recognize and advance phy-sician leadership and excellence through a national, peer-generated, standards-based assessment process.
Physicians awarded the CCPE have demonstrated that they have the leadership capabilities, knowledge and skills needed for successful performance and, more important, to direct, in-fluence and orchestrate change in Canada’s complex health care system. For more information on the CCPE, please visit the CMA website at http://www.cma.ca/learning/ccpe.

SMA News Digest Autumn 2012 33
obituaries
Dr. Muhammad Anwarul Haque passed away on August 18, 2012. He died peacefully in his Regina home where he was sur-rounded by his entire family. Dr. Haque was born in a village in Naogao, Bangladesh in 1935 and received his medical degree at Dhaka Medical College in 1958. In 1959, he left Bangladesh and con-tinued his training in Wales, England, Minneapolis, and Montreal, and finished his Otolaryngology training in Buffalo, New York. Af-ter reviewing various places to live, Dr. Haque decided to make Re-gina his home and joined the Medical Arts Clinic (now the Cornwall Professional Building) in 1969 where he maintained a full practice until April of this year when, at the age of 77, he was diagnosed with cancer.
Dr. Haque will be remembered as a loving husband, father and grandfather, as well as, a devoted doctor to his patients and an unselfish individual who worked to better the Muslim and non-Muslim communities. To the end, one of his greatest concerns was the care of his many patients who benefited from his allergy treat-ments. He is survived by his wife, Nilufar; his three children Sami, Sabreena and Munir; their respective spouses, Zarqa, Amir and Samira; as well as his eleven grandchildren Maysa, Inaya, Rashad and Zayn (Sami and Zarqa), Raeesa, Janan, Wisam and Sakeenah (Sabreena and Amir) and Isa, Rayyann and Medyna (Munir and Samira).
Dr. Ian Holmes passed away quietly on Sunday, August 19, 2012 in Samaritan Place, Saskatoon after a brief illness.
Dr. Holmes was born in Schreiber, Ontario to William and Charlotte Holmes. He received his medical degree at the University of Mani-toba in 1953, and his Certificate in Internal Medicine at the Uni-versity of Alberta in 1960. He practiced in Yorkton, Saskatchewan, in Edmonton and Red Deer, Alberta, and Saskatoon, Saskatchewan. While practicing in Saskatoon, he also taught in the Faculty of Medicine, until last year.
Dr. Holmes always instilled in his student’s minds the idea that patients were humans and were to be treated with respect and dignity. He also made sure that his students got all the help they needed to succeed. He always insisted that his students explore all possibilities, and think things through carefully and methodically. His passion for gardening was shown in the large amount of pro-duce he had for his family, neighbours and the Friendship Inn in Saskatoon.
Dr. Holmes was a long time member of Third Avenue United Church in Saskatoon, and was on the church board for many years. He was also on several other committees and boards such as the Oliver Lodge Board and the Inner City Council in Saskatoon. He leaves be-hind his wife of 60 years, Elizabeth; his son, Kenneth and his step-grandchildren, Cara and Jonathan; his daughter, Charlotte and her husband Paul and his granddaughters, Heidi and Lisa Schmidtke.
Dr. Wali A. Khan, 76, passed away peacefully after a brief illness at the Ottawa Heart Institute. A pathologist at Saskatoon City Hos-pital until 2010, he is also missed by his many friends, family and colleagues in Saskatchewan.
Dr. Khan was born in 1936 in what is now Bangladesh. He com-pleted his MBBS at the University of Dhaka in 1960, after which he worked at the Institute of Diseases of the Chest and Hospital. In 1963, he moved to the United States to continue his training. He met his future wife, Cristeta at The Elyria Memorial Hospital in 1963, and they were married in Guelph, Ontario two years later. His medical education also included the M.D. Anderson Hospital and Tumor Institute at the University of Maryland and the Baylor Col-lege of Medicine in Houston, Texas.
In 1972, Dr. Khan moved to Saskatoon CIty Hospital, where he worked as a pathologist until 2010. He and his wife lived in Saska-toon for more than 40 years, raising their two children and enjoy-ing an active life that included the Rotary Club, tennis and golf, and travel around the world, including a six-month medical volunteer role in Kathmandu, Nepal.
Please visit our website for details on the positions and more great health careers that await you!
www.hrha.sk.ca
HEARTLAND HEALTH REGION Healthy People, Healthy Communities and
Service Excellence in an Enduring Health System
EXPLORE OUR OPPORTUNITIES FOR PHYSICIANS People who care for and about one another are the heart and spirit of a community. At Heartland Health Region, our dedicated
employees share in the vision of providing safe, quality and
compassionate care for our clients and communities.
Quality Employees = Quality Care
Christa Garrett Coordinator of Executive & Medical Affairs
882‐4111 Ext. 236 [email protected]

classifieds
Exceptional opportunity for an experienced General Physician with an existing patient pool or a practitioner planning to establish
a successful practice
A brand new private walk-in medical clinic will be starting operations on the East side of Saskatoon near University of Saskatchewan, at Preston Crossing in March 2013. We are
looking for dynamic, friendly, conscientious, committed MDs to help our clientele with exceptional service and dedication. You will be surrounded by a competent support team and a
modern brand-new set up. Work as much or as little as you wish, with above average compensation and benefits. Earn above-average income with possibility of equity ownership (for the right candidate). Leave the management of the clinic to us, and get busy with the business of
being the best doctor you can be.
About you
$ You are a team player with excellent communication skills
$ You are a positive person who enjoys the practice of medicine $ You want to work hard, give excellent service and earn above average income
$ You are dedicated to improving and updating your skills at all times
About the clinic
$ Walk-in medical clinic $ 7-bed clinic
$ Fully computerized with electronic medical records $ Superb exposure and BUSY foot traffic: you will be exceptionally busy
within the first month of practice $ Excellent support team to ensure you can be as productive and attentive
to your patients as possible.
About the position
$ 3 positions available $ Walk-in clinic with adjunct paramedical services on board
$ Above average compensation, ranging from 65-75% plus bonuses, incentives and allowances (pending experience and length/level of commitment)
$ Equity position for the right candidate $ Work as much or as little as you wish $ Positive, efficient and fast-paced office
$ Intimate set-up with a positive and supportive work environment
For further information, please contact with a letter of interest: Dr. Parviz Yazdani

SMA News Digest Autumn 2012 35
classifieds

Family PhysiciansIt’s more than a practice...it’s a lifestyle!
www.northerndocs.com
Northern Medical Services is seeking family physicians for full-time, part-time, itinerant contract and locum positions available in northern Saskatchewan. NMS physicians are active participants in health care delivery to predominantly Aboriginal communities. They work closely with nurse practitioners and other primary care providers to meet the specific needs of each community.
We offer a competitive remuneration package (compensation in excess of $280,000-$362,000 per annum depending upon qualifications and employment location) plus additional personal and pro-fessional benefits too numerous to mention. We offer an excellent employee benefit plan: reloca-tion assistance package, furnished housing, 6 weeks of vacation and 3 weeks of education leave including financial support for CME.
Locum rate: $1300-1765 per day plus on-call stipend
Kerri Balon, Recruitment CoordinatorNorthern Medical Services Division of Academic Family Medicine404, 333 – 25th Street E.Saskatoon, SK Canada S7K 0L4
Phone: (306) 665-2898Fax: (306) 665-6077Toll Free: 1-866-NMS-DOCS (667-3627)Email: [email protected]

Helping Saskatchewan Physicians lead the way
with the Saskatchewan EMR Program
Why EMR?
Access to clinical data is one of many key benefits of computerization.
Improvements include:
coordination and continuity of care among providers
ease of access to information in emergency situations
reduction in adverse drug events.
Confidence for you
We are here to support you and your team in making the
transition to EMR.
Over 600 of your Saskatchewan colleagues are
already using Accuro®EMR
52% GPs/ 48% Specialists
Call for Accuro® demonstration 1-866-454-4681
Regina office Sean Stephenson (306) 292-9728 [email protected]
Visit www.CanadianEMR.ca for EMR comparisons and User ratings.

Return undeliverable Canadian addresses to:
Saskatchewan Medical Association 402-321A 21st Street East Saskatoon, SK CanadaS7K 0C1
Mail to:
40007031


















