
Potential Consumer Demand for midata: Findings of qualitative and ...
EXPLORING CONSUMER PERSPECTIVES ON GOOD PHYSICIAN
CARE: A SUMMARY OF FOCUS GROUP RESULTS
Donna Pillittere, Mary Beth Bigley, Judith Hibbard, and Greg Pawlson
January 2003 Support for this research was provided by The Commonwealth Fund. The views presented here
are those of the authors and should not be attributed to The Commonwealth Fund or its
directors, officers, or staff.
This report (#578) is available online only from The Commonwealth Fund’s website at
www.cmwf.org.

ii
CONTENTS
About the Authors......................................................................................................................iii
Executive Summary....................................................................................................................iv
Introduction ................................................................................................................................1
Methodology: Designing a Focus Group Study............................................................................2
Major Findings from Focus Group Exercises................................................................................3
Conclusions and Implications.....................................................................................................17
Appendix A: Focus Group Participants, Schedule, and Protocol.................................................19
Appendix B: Demographic Characteristics of Participants ..........................................................22
Appendix C: Three Main Concepts Tested................................................................................23
Appendix D: Individual Measurement Concepts Tested.............................................................24
Appendix E: List of Expert Panel Members................................................................................25
References ................................................................................................................................26
iii
ABOUT THE AUTHORS
Donna Pillittere, M.S., is a senior health care analyst for quality measurement at the National
Committee for Quality Assurance (NCQA). Ms. Pillittere is responsible for leading the
development of various HEDIS measures along with coordination of the HEDIS Public
Comment and Measure Reevaluation maintenance processes. She is directly involved in research
related to quality measurement at the health plan and physician practice level. Prior to joining
NCQA, she served as a fellow at the National Cancer Institute’s Mass Media branch, where her
main duties focused on translation and dissemination of scientific literature to the general public.
Ms. Pillittere earned her M.S. in epidemiology at the State University of New York at Buffalo.
Mary Beth Bigley, M.S.N, A.N.P., is currently an assistant professor at George Washington
University, School of Medicine and Health Sciences, serving as the program director of the Nurse
Practitioner Program. She received a master of science in nursing degree from George Mason
University and is certified as a nurse practitioner. Through a post-master’s fellowship, she was
awarded a Teaching Certificate from the University of Pennsylvania. She is a doctoral candidate
in the School of Public Health at George Washington University, with a concentration in health
service research.
Judith Hibbard, Dr.P.H., is a professor of health policy in the Department of Planning, Public
Policy and Management at the University of Oregon and a clinical professor of public health and
preventive medicine at the Oregon Health Sciences University. Professor Hibbard is an
investigator on the new CAHPS II project. She is a member of the Strategic Advisory Counsel of
the National Health Care Quality Forum, and she recently served on the Institute of Medicine’s
committee on Envisioning the National Health Care Quality Report. Her research interests focus on
how consumers and providers can more effectively use information to improve the quality of
care. She has published extensively about consumer use of comparative information for informing
health care choices. Professor Hibbard received her master’s degree from the School of Public
Health at UCLA and her doctorate from the U. C. Berkeley School of Public Health.
Greg Pawlson, M.D., M.P.H., is the executive vice president of NCQA. Prior to joining
NCQA, Dr. Pawlson was at the George Washington University Medical Center, most recently as
senior associate vice president for health affairs and as medical director for quality and utilization
management for the faculty practice. Dr. Pawlson’s areas of policy and research include health
professions education, health policy, health services, and health care financing, especially as they
relate to primary care and to the care of older persons. He has over 80 publications in books,
proceedings, and peer-reviewed journals, and has served on the editorial board of numerous
publications and on review panels for various foundations and agencies. Dr. Pawlson received his
undergraduate degree from Pennsylvania State University, his M.D. degree from the University of
Pittsburgh (served his internship/residency at Stanford) and completed his master of public health
degree at the University of Washington.
iv
EXECUTIVE SUMMARY
The study reported here is part of a multifaceted Commonwealth Fund–supported study,
“Developing Patient-Centered Measures of Physician Quality,” that explored consumer
preferences for information about physicians as well as potential sources for information. The
study was conducted by the National Committee for Quality Assurance (NCQA), a nonprofit
oversight organization that evaluates and produces reports on the quality of health plans. After an
extensive literature and “work in progress” search of research related to consumer preferences and
use of information, the NCQA project team determined that there was a need for further work in
the area using qualitative research methods. In consultation with members of the project advisory
group (see Appendix E), the team developed a protocol for six focus groups consisting of a cross
section of consumers of varying socioeconomic status and enrolled variously in commercial,
Medicare, and Medicaid health insurance plans. The focus group exercises were conducted by the
NCQA team between June 13 and 21, 2001.
A major goal of the focus groups was to determine if consumers could both understand
and value not only their own perceptions of quality at the physician office level, but also the
aspects of quality seen as important by physicians and experts. The team hypothesized that if
consumers were given a carefully constructed frame of reference, they would be able to
understand and value information related to domains of quality beyond patient-centered
perceptions of care. Thus, after eliciting initial preferences for information about physician
practice, the team presented participants with a framework for helping them understand multiple
dimensions of physician performance, including the three main concepts seen by physicians and
quality experts as critical: “Patient-Centered Care” (patient-centeredness), “Health Care That
Works” (effectiveness), and “Safe Health Care” (safety).
The primary finding of the research confirmed the initial hypothesis—namely that
consumers can understand and will value information about effectiveness and patient safety (as
well as patient-centeredness) if they are presented with information in a consumer-friendly
framework. These findings provide some basis for further research to determine if consumers will
actually use information about multiple domains of information on quality of physician care in
selecting or otherwise recognizing high quality physician practice. Coupled with a growing
recognition by physicians and quality experts of the critical importance of patient perceptions of
care (patient-centeredness), the finding also provides some hope that the medical community can
move toward the broad and comprehensive measures and use of information on quality suggested
in the Institute of Medicine (IOM) report Crossing the Quality Chasm: A New Health System for the
21st Century (2001).
v
Major findings from the focus group exercises included:
1. Consumers initially focused on the patient–doctor relationship. Consumer
understanding of and desire for information on physician performance was limited to
patient-centered concepts prior to the introduction of the framework. The focus group
participants emphasized the dynamics of the patient–doctor relationship, with the majority
of initial responses calling for empathetic qualities, e.g., “time,” “personal attention,”
“caring,” “good communication skills,” “showing concern,” and “good bedside manner.”
2. Once given a framework, consumers valued the concepts of safety and
effectiveness equally with patient-centeredness. After the framework was
introduced, consumers were able to understand the concepts of effective and safe physician
care as well as patient-centered concepts and appeared to value them about equally. This
understanding was tested by presenting the concepts to the participants and engaging them
in a discussion about what they thought the concepts meant, e.g., for “patient-centered
care” participants responded with “patient-focused…you have a voice in your care”; for
“effective care” participants responded with “consistent”; and for “safe health care”
participants responded with “ doing the right things, the right way.”
3. To a lesser extent, consumers also understood many of 12 specific
measurement areas associated with the three main concepts (see Appendix D).
For example, participants were presented with the measurement area, “doctor has up-to-
date information on patient drug allergies,” and 50 of the 55 individuals were able to
categorize the measurement area under the concept that most closely corresponded with
the measurement area “Safe Health Care.”
4. As has been noted in prior research, socioeconomic status and education
affected comprehension of some high-level concepts. The moderator and research
staff in attendance observed that the participants in the Medicaid and “blue collar” groups
struggled more than others with understanding some of the concepts and measurement
areas and were less able to describe how these areas relate to good physician care.
5. The Medicare population, more than other consumer groups, tended to equate
good physician care with aspects of the patient–doctor relationship and to a
lesser extent with the level of a doctor’s experience. These participants seemed to
give more emphasis to aspects of the interpersonal relationship between a patient and
doctor, such as aspects of communication, listening, and bedside manner, with comments
such as “I want to be more than just an appointment” and “A relationship is important…I
want him to know my name.”
6. Consumers want to work together with their physicians and be included in the
decision-making process but do not want to assume sole or primary
responsibility for their care. When the participants were asked to choose the definition
vi
that most closely encompassed the concept of patient-centered care; only 9 of the 55
participants selected “Doctor provides patient with the education and support to manage
their own health,” whereas 24 of the 55 participants selected “Doctor and patient work
together to make decisions that take into account the patient’s needs.”
7. The Medicare population appears to be more accepting and forgiving of
physician errors. Despite their apparent understanding of the concept of medical errors
and patient safety, these participants expressed a belief that health care can never be truly
safe, and the human component of physician care creates an inherent potential for medical
mistakes. This notion was particularly evident in the Medicare group, indicating that the
Medicare consumers may be more reluctant to undermine or question a doctor’s authority.
8. Consumers perceive a distinction between accountability for “physician” care
and for “health” care. Participants clearly struggled with the use of the term “health
care” in the three main concepts and suggested that measurement areas and concepts
should clearly specify the physician as the actor in any measurement describing a
component of the service a physician provides.
9. Consumers are very sensitive to word choices; when using text to describe
measures or concepts, each word may have a profound impact on consumer
comprehension. In the measurement area “doctor provides the right treatment for short-
term illness,” right can mean “correct,” as in the doctor provided the correct treatment for
the illness, or it can mean “effective,” as in the doctor provided a treatment that led to an
improvement in the patient’s condition.
Overall, focus group findings support the idea that consumer ability to understand and
value health care quality information, specifically that of the IOM concepts of patient-
centeredness, safety, and effectiveness, is enhanced when a consumer-friendly framework is
employed. Careful attention to the words used to define measurement is necessary to achieve the
correct understanding for the lay user; future cognitive evaluation of the measurements and the
appropriate level of detail needed is key to this process.
Clearly, much work remains to be done on how to design and use frameworks that
provide the critical level of consumer understanding, as well as exploration of whether the
“value” expressed by consumers in our qualitative focus group study translates into actual use of
the information in practice. An additional major barrier is the lack of reliable and valid
information on quality at the physician office practice level. While these issues must be addressed,
the conclusion that consumers can understand and value information on the safety and
effectiveness of physician practice, if confirmed, has important implications for clinicians and
consumers, as well as those interested in monitoring, improving, and reporting on physician office
practice quality.

1
EXPLORING CONSUMER PERSPECTIVES ON GOOD PHYSICIAN CARE:
A SUMMARY OF FOCUS GROUP RESULTS
INTRODUCTION
The Need for a Meaningful Evaluation System
As the science of performance measurement matures and public interest in information on health
care quality grows, efforts to report quality information have expanded. To date, the most
sophisticated forms of performance measurement and public reporting efforts have been limited to
managed care organizations and, in a more limited manner, to hospitals and nursing homes.
However, surveys indicate that consumers are most interested in information about quality of
physician care. Efforts are underway by researchers to create performance evaluation measures and
programs at the physician group and individual physician levels. In order to create evaluation
systems that are meaningful to consumers, as well as purchasers or clinicians, researchers have been
exploring what information related to the quality of physician care consumers feel they need or
want.
Obstacles to Assessing Consumer Preferences
While a number of studies have been conducted on the kind of information consumers want,
understanding consumer preferences has been hampered by a number of factors. The relatively
complex nature of medical practice and its evaluation, the limited knowledge of consumers about
the multiple domains of quality, and the lack of information on physician performance that is
actually available have all led to instability in what consumers indicate is important in selecting
physicians. Several investigators have also found that consumer preferences for information about
physicians are influenced by what information they are given and how it is presented. Consumer
reliance on limited information and the tendency to be easily swayed have contributed to what
appears to be a major gap between what practitioners and quality experts see as critical to
physician practice quality and how patients understand quality and use actual or experimental
information to choose physicians. While physicians and quality experts see valid and reliable
measures of safety, effectiveness, and efficiency as critical, studies of patient preferences suggest
that patients rely almost exclusively on their own perceptions of care or on the experience and
recommendations of friends and relatives, which are limited to a few basic characteristics of
physician practice. This disconnect causes physicians to distrust the ability of consumers to use
information on practice to choose wisely and casts considerable doubt on the future of consumers
as an effective “lever” to drive quality improvement.
2
METHODOLOGY: DESIGNING A FOCUS GROUP STUDY
The study reported here is part of a multifaceted Commonwealth Fund–supported study,
“Developing Patient-Centered Measures of Physician Quality,” that explored consumer
preferences for information about physicians as well as potential sources for information. The
study was conducted by the National Committee for Quality Assurance (NCQA), a nonprofit
oversight organization that evaluates and produces reports on the quality of health plans. After an
extensive literature and “work in progress” search of research related to consumer preferences and
use of information, the NCQA project team determined that there was a need for further work in
the area using qualitative research methods. In consultation with members of the project advisory
group (see Appendix E), the team developed a protocol for six focus groups consisting of a cross
section of consumers of varying socioeconomic status and enrolled variously in commercial,
Medicare, and Medicaid health insurance plans. The focus group exercises were conducted by the
NCQA team between June 13 and 21, 2001.
A major goal of the focus groups was to determine if consumers could both understand
and value not only their own perceptions of quality at the physician office level, but also the
aspects of quality seen as important by physicians and experts. The team hypothesized that if
consumers were given a carefully constructed frame of reference, they would be able to
understand and value information related to domains of quality beyond patient-centered
perceptions of care. An initial step in the focus groups was to elicit participant’s ideas about areas
of physician performance that would be useful in choosing a physician. Then the project team
shared with the groups three of the main concepts of quality noted in two recent reports from the
Institute of Medicine (IOM), Envisioning the National Health Care Quality Report and Crossing the
Quality Chasm: A New Health System for the 21st Century: “Patient-Centered Care” (patient-
centeredness), “Health Care That Works” (effectiveness), and “Safe Health Care” (safety).
The research was designed to:
• Determine whether presenting a framework for measuring physician performance would
expand consumer understanding of physician quality;
• Determine if participants would understand and value the three concepts of good
physician care: effectiveness, patient-centeredness, and safety;
• Explore different ways of describing the areas of physician performance so that it was most
meaningful and understandable to consumers; and
• Examine whether participants understand the measurement areas for each concept and
believe each measurement area represents good physician care.
3
NCQA contracted with The Family Research Group (FRG) to assist in the development
of focus group protocols, to moderate the focus groups, and to draft an initial analysis of the
groups. See Appendices A through D for detailed descriptions of focus group methodologies and
protocols. In addition, staff worked closely with Judith Hibbard in the development of the focus
group exercises and on the findings. Substantial input on the general conduct of the study and in
understanding the results was also provided by an expert panel. See Appendix E for a list of the
expert panel members.
MAJOR FINDINGS FROM FOCUS GROUP EXERCISES
Each of the nine major findings from the focus groups is discussed in more detail below. When
possible, we have included actual comments recorded during the focus groups. These comments
appear in italics.
1. Consumers initially focused on the patient–doctor relationship.
The initial focus group exercise asked participants to describe what constitutes good physician
care. All of the focus groups dealt primarily with the dynamics of the patient–doctor relationship.
The majority of initial responses called for empathetic qualities, such as “time,” “personal
attention,” “caring,” “good communication skills,” “showing concern,” and “good bedside
manner.” For example, participants said:
“I want a doctor who is going to take his time… explain things to me and not rush me out
of the office.”
“I want to be more than just an appointment.”
“It would be nice if they’re concerned about your comfort... their staff should care, too.”
“A relationship is important… I want him to know my name.”
These findings are consistent with current research showing that consumers are concerned
about the patient–doctor relationship and its impact on their care. Consumers list most often the
aspects of the interpersonal relationship between a patient and doctor such as communication,
listening, and bedside manner, as the items they would like to know about physician care,. This is
not surprising, since issues of the patient–doctor relationship and patient-centeredness are things
patients are familiar with, without having a meaningful framework for understanding and using
other types of quality information, such as information on effectiveness.
After the initial focus group exercise, safety and effectiveness frameworks were presented
to the groups. Overwhelmingly the groups indicated that if information about these elements was
available to them, they would review the data and use the information.
4
Implications: These findings suggest that consumers value the patient-centered aspects of
physician care. Some consumers may be more likely to prefer physicians who concentrate on
building and maintaining meaningful relationships with their patients and involve the patient in
the care process. However, framing quality information to help consumers understand the safety
and effectiveness aspects of quality care provides another source of information that consumers
will use when making choices.
2. Once given a framework, consumers valued the concepts of safety and effectiveness
equally with patient-centeredness.
One purpose of the focus groups was to determine whether consumers understand the concepts
of effective, patient-centered, and safe health care. The moderator tested this hypothesis by
presenting the concepts on poster boards and engaging the participants in a discussion about what
they thought the concepts meant. This discussion was followed by the presentation of three
definitions for each concept and a group discussion on how well the definitions described the
concept. The focus groups revealed that, in general, the participants understood the concepts,
although there were problems with language that the participants felt was confusing or vague.
For example, when asked “What is Patient-Centered Care?” most participants understood
the concept:
“Patient-focused… you have a voice in your care.”
“Accessible.”
“You have a relationship… he knows your name.”
“Doesn’t rush… takes time to explain to you what’s going on.”
Some participants, however, were confused by the concept:
“It’s a center for patients.”
“It’s a place where patients go… like a clinic.”
Throughout the discussions, the participants struggled to create a better way of phrasing
the concept behind Patient-Centered Care. After several sessions, members from one group
suggested that the term “patient–doctor relationship” is a better term to reflect the concept of
Patient-Centered Care. Later groups agreed with this term, indicating that “patient–doctor
relationship” more clearly indicates a mutually respectful relationship with two-way
communication and shared decision-making between the patient and the doctor.
5
In contrast to Patient-Centered Care, the majority of participants understood the concepts
of Health Care That Works and Safe Health Care. The participants described Health Care That
Works as:
“Effective.”
“Consistent.”
“Preventive and corrective care.”
The participants described Safe Health Care as:
“The doctor does not give you medicine you’re allergic to.”
“Doing the right thing, the right way.”
Implications: Consumers comprehend the IOM concepts of effectiveness, patient-
centeredness, and safety when the concepts are phrased using consumer-friendly terms. All three
terms resonate with consumers, although the specific wording of the concepts may affect
comprehension, as was seen in the case with Patient-Centered Care. The three concepts from the
IOM report could provide the foundation for an effective framework for health care quality
information for consumers.
3. To a lesser extent, consumers also understood many of 12 specific measurement
areas associated with the three main concepts (see Appendix D).
While the three main concepts of effectiveness, patient-centeredness, and safety may provide the
foundation for a framework for quality information, developers of quality information must pay
attention to the construction and portrayal of the individual measurement areas that comprise
each concept. As described in the protocol in Appendix A and the list in Appendix D, the
moderator presented 12 measurement areas to the focus group participants. The participants then
were instructed to categorize the measurement areas under one of the two concepts, Health Care
That Works or Safe Health Care.
Participants understood most measurement areas and were generally able to identify
whether a measurement area was categorized under Health Care That Works or Safe Health
Care. However, there was some confusion over items that could be interpreted in more than one
way. For example, staff considered the measurement area “doctor identifies illness early” to be
categorized under Health Care That Works, since this measurement area applies to preventive
care (e.g., mammography). In contrast, a few participants felt that a doctor who did not identify
illness early by failing to screen for cancer was risking a patient’s safety and therefore categorized
this concept under Safe Health Care.
6
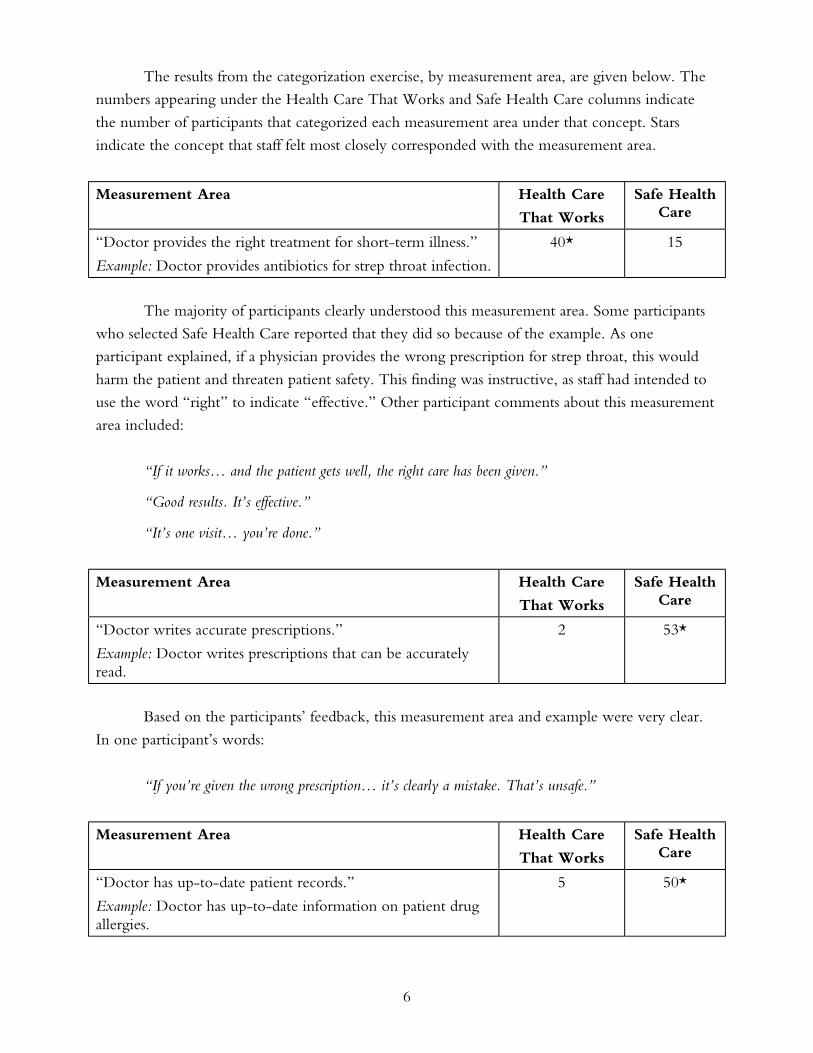
The results from the categorization exercise, by measurement area, are given below. The
numbers appearing under the Health Care That Works and Safe Health Care columns indicate
the number of participants that categorized each measurement area under that concept. Stars
indicate the concept that staff felt most closely corresponded with the measurement area.
Measurement Area Health Care
That Works
Safe Health Care
“Doctor provides the right treatment for short-term illness.”
Example: Doctor provides antibiotics for strep throat infection.
40* 15
The majority of participants clearly understood this measurement area. Some participants
who selected Safe Health Care reported that they did so because of the example. As one
participant explained, if a physician provides the wrong prescription for strep throat, this would
harm the patient and threaten patient safety. This finding was instructive, as staff had intended to
use the word “right” to indicate “effective.” Other participant comments about this measurement
area included:
“If it works… and the patient gets well, the right care has been given.”
“Good results. It’s effective.”
“It’s one visit… you’re done.”
Measurement Area Health Care
That Works
Safe Health Care
“Doctor writes accurate prescriptions.”
Example: Doctor writes prescriptions that can be accurately read.
2 53*
Based on the participants’ feedback, this measurement area and example were very clear.
In one participant’s words:
“If you’re given the wrong prescription… it’s clearly a mistake. That’s unsafe.”
Measurement Area Health Care
That Works
Safe Health Care
“Doctor has up-to-date patient records.”
Example: Doctor has up-to-date information on patient drug allergies.
5 50*
7
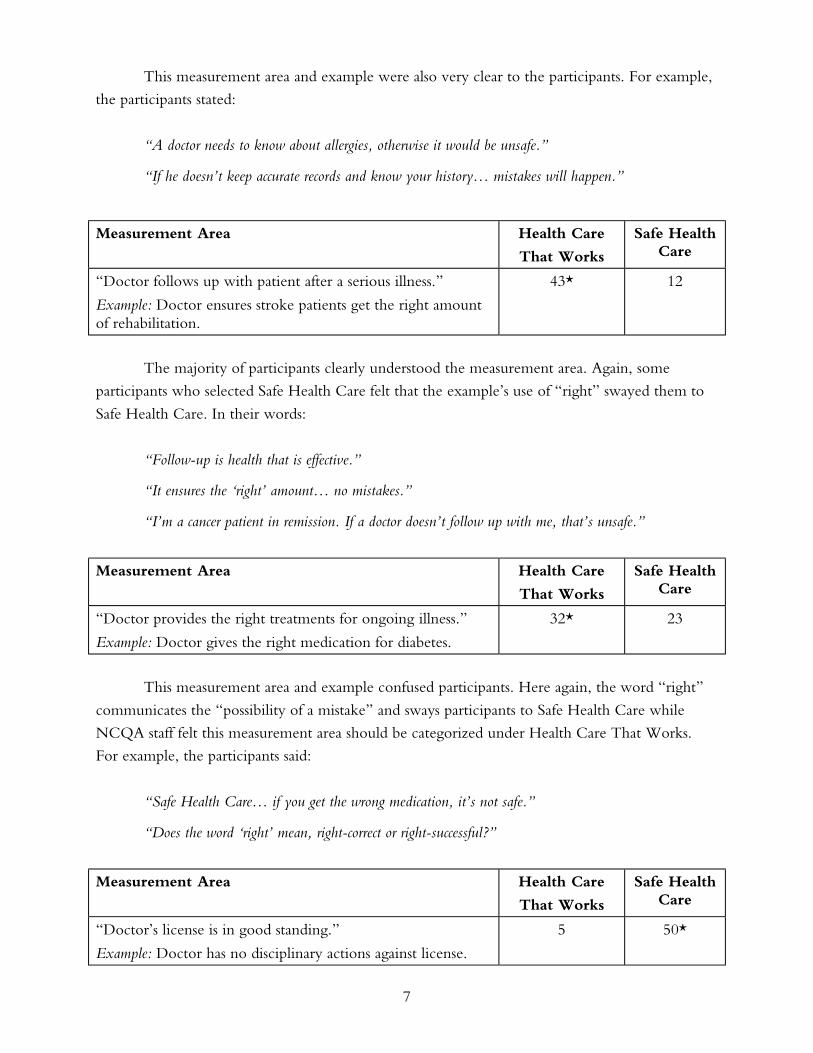
This measurement area and example were also very clear to the participants. For example,
the participants stated:
“A doctor needs to know about allergies, otherwise it would be unsafe.”
“If he doesn’t keep accurate records and know your history… mistakes will happen.”
Measurement Area Health Care
That Works
Safe Health Care
“Doctor follows up with patient after a serious illness.”
Example: Doctor ensures stroke patients get the right amount of rehabilitation.
43* 12
The majority of participants clearly understood the measurement area. Again, some
participants who selected Safe Health Care felt that the example’s use of “right” swayed them to
Safe Health Care. In their words:
“Follow-up is health that is effective.”
“It ensures the ‘right’ amount… no mistakes.”
“I’m a cancer patient in remission. If a doctor doesn’t follow up with me, that’s unsafe.”
Measurement Area Health Care
That Works
Safe Health Care
“Doctor provides the right treatments for ongoing illness.”
Example: Doctor gives the right medication for diabetes.
32* 23
This measurement area and example confused participants. Here again, the word “right”
communicates the “possibility of a mistake” and sways participants to Safe Health Care while
NCQA staff felt this measurement area should be categorized under Health Care That Works.
For example, the participants said:
“Safe Health Care… if you get the wrong medication, it’s not safe.”
“Does the word ‘right’ mean, right-correct or right-successful?”
Measurement Area Health Care
That Works
Safe Health Care
“Doctor’s license is in good standing.”
Example: Doctor has no disciplinary actions against license.
5 50*
8
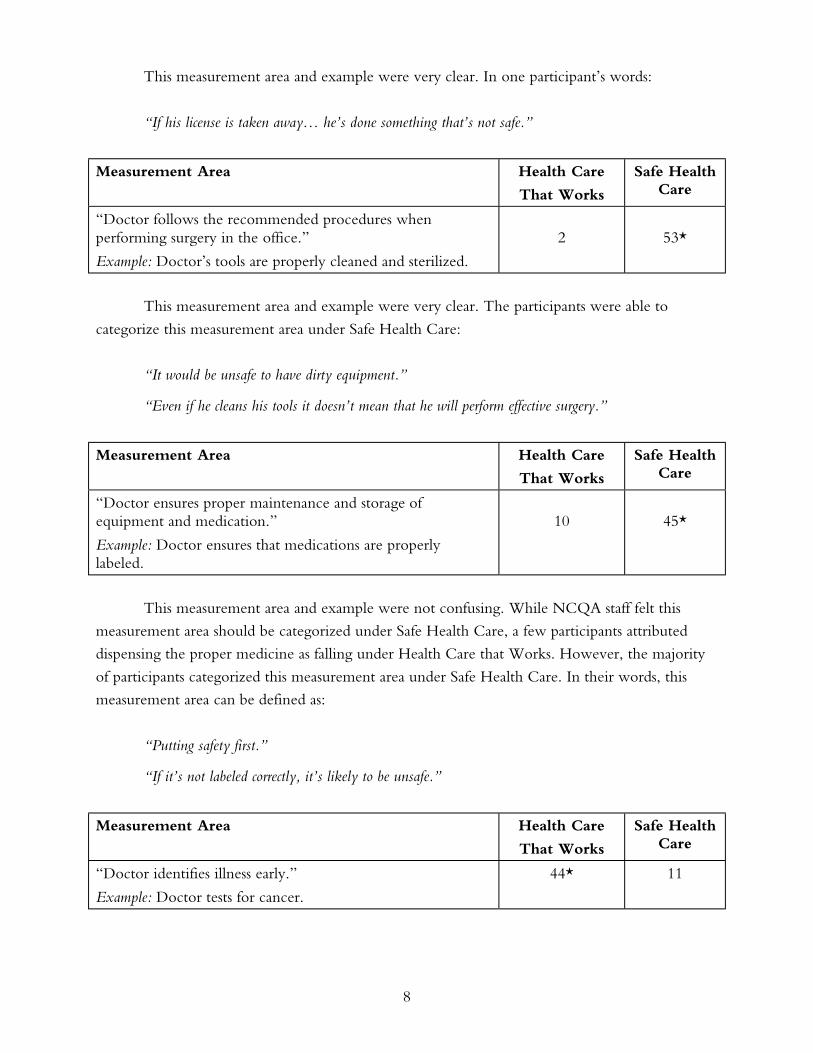
This measurement area and example were very clear. In one participant’s words:
“If his license is taken away… he’s done something that’s not safe.”
Measurement Area Health Care
That Works
Safe Health Care
“Doctor follows the recommended procedures when performing surgery in the office.”
Example: Doctor’s tools are properly cleaned and sterilized.
2
53*
This measurement area and example were very clear. The participants were able to
categorize this measurement area under Safe Health Care:
“It would be unsafe to have dirty equipment.”
“Even if he cleans his tools it doesn’t mean that he will perform effective surgery.”
Measurement Area Health Care
That Works
Safe Health Care
“Doctor ensures proper maintenance and storage of equipment and medication.”
Example: Doctor ensures that medications are properly labeled.
10
45*
This measurement area and example were not confusing. While NCQA staff felt this
measurement area should be categorized under Safe Health Care, a few participants attributed
dispensing the proper medicine as falling under Health Care that Works. However, the majority
of participants categorized this measurement area under Safe Health Care. In their words, this
measurement area can be defined as:
“Putting safety first.”
“If it’s not labeled correctly, it’s likely to be unsafe.”
Measurement Area Health Care
That Works
Safe Health Care
“Doctor identifies illness early.”
Example: Doctor tests for cancer.
44* 11
9
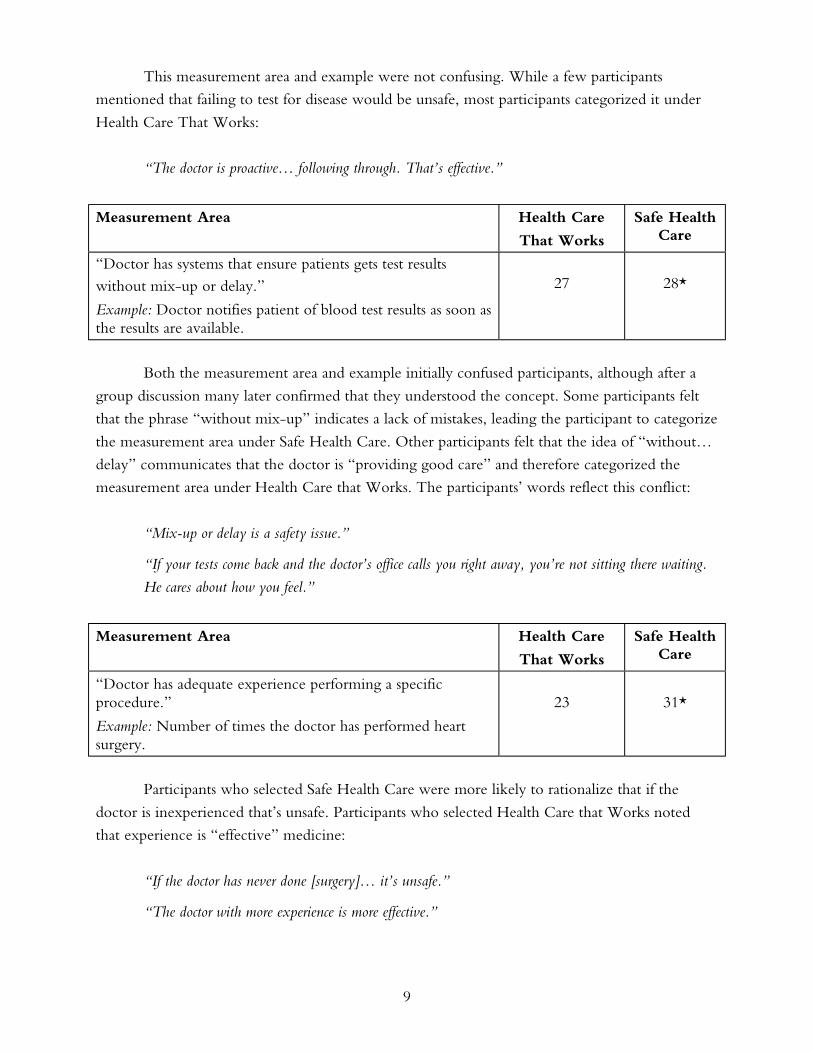
This measurement area and example were not confusing. While a few participants
mentioned that failing to test for disease would be unsafe, most participants categorized it under
Health Care That Works:
“The doctor is proactive… following through. That’s effective.”
Measurement Area Health Care
That Works
Safe Health Care
“Doctor has systems that ensure patients gets test results without mix-up or delay.”
Example: Doctor notifies patient of blood test results as soon as the results are available.
27
28*
Both the measurement area and example initially confused participants, although after a
group discussion many later confirmed that they understood the concept. Some participants felt
that the phrase “without mix-up” indicates a lack of mistakes, leading the participant to categorize
the measurement area under Safe Health Care. Other participants felt that the idea of “without…
delay” communicates that the doctor is “providing good care” and therefore categorized the
measurement area under Health Care that Works. The participants’ words reflect this conflict:
“Mix-up or delay is a safety issue.”
“If your tests come back and the doctor’s office calls you right away, you’re not sitting there waiting.
He cares about how you feel.”
Measurement Area Health Care
That Works
Safe Health Care
“Doctor has adequate experience performing a specific procedure.”
Example: Number of times the doctor has performed heart surgery.
23
31*
Participants who selected Safe Health Care were more likely to rationalize that if the
doctor is inexperienced that’s unsafe. Participants who selected Health Care that Works noted
that experience is “effective” medicine:
“If the doctor has never done [surgery]… it’s unsafe.”
“The doctor with more experience is more effective.”

10
Measurement Area Health Care
That Works
Safe Health Care
“Doctor provides preventive care at the right time.”
Example: Doctor offers flu shots to patients prior to the flu season.
46* 8
This measurement area and example were very clear:
“He knows effective medication for prevention.”
“This is preventive medicine. It works.”
Implications: The results from this exercise confirm that the concepts of effectiveness
and safety are not completely discrete ideas, but involve a degree of overlap. Indeed, many
participants indicated that a doctor that did not provide effective care was threatening a patient’s
safety. The indelible link between these concepts may make the categorization of individual
measures under those concepts more challenging. It seems that when the measure suggests any
possible “harm” some consumers think this means “safety.” Perhaps safety needs to be framed
more in terms of mistakes to help differentiate it from effectiveness. Clearly, more research will
need to be done before individual measures are “mapped” to the concepts of effectiveness and
safety for use in various reporting mechanisms.
4. As has been noted in prior research, socioeconomic status and education affected
comprehension of some high-level concepts.To some extent, the focus groups were
controlled for certain key demographics, such as socioeconomic status and education level.
Results from two groups, the Medicaid group and the “blue collar” group, were analyzed to
determine whether socioeconomic status affected the consumers’ ability to comprehend and their
willingness to value the three main concepts and the more detailed measurement areas.
The moderator and staff in attendance felt that the participants in the Medicaid and “blue
collar” groups struggled with understanding the concepts and measurement areas and were less
able to describe how these areas relate to good physician care. However, there were no clear
patterns in either the written exercises or dialogue that allow for drawing conclusions on the
characteristics or severity of this problem.
Implications: Additional research must be conducted to probe whether individuals of
lesser socioeconomic status have information needs and preferences that differ from other
demographic groups. Developers of measures and reporting frameworks must ensure that products
are accessible and understandable by individuals of all socioeconomic backgrounds.
11
5. The Medicare population, more than other consumer groups, tended to equate
good physician care with aspects of the patient–doctor relationship and to a lesser
extent with the level of a doctor’s experience.
As described in Finding #1, consumers often value most aspects of the interpersonal relationship
between a patient and doctor such as communication, listening, and bedside manner. This is not
surprising, since issues of the patient–doctor relationship and patient-centeredness are what
patients are familiar with. These ideas are consistent with current research. Through these focus
groups, we have learned that the addition of a meaningful framework enhances consumers’ ability
to understand and value health care quality information, such as information on effectiveness of
care.
“I want a doctor who is going to take his time… explain things to me and not rush me out of the
office.”
“I want to be more than just an appointment.”
“It would be nice if they’re concerned about your comfort... their staff should care, too.”
“A relationship is important… I want him to know my name.”
To a lesser extent, participants offered traits such as “knowledgeable,” “trustworthy
reputation,” and “experience” as indicators of a good physician. Interestingly, few participants
directly referred to qualities related to clinical effectiveness or positive outcomes, such as
“prescribing the appropriate medicine” and “making me better” when asked open-ended
questions without having a framework or context for the information.
During this exercise, the participants were asked whether they value having access to
information on physician quality. The participants overwhelmingly responded that information on
physician quality is extremely important and desirable:
“Your life depends on [the doctor] you see… [information on quality] is extremely important.”
Implications: Consumers are very interested in knowing and using other quality
measures of physician care. Although additional research is needed, the Medicare population
concepts of clinical effectiveness appear to differ from other populations. Nevertheless, these
findings demonstrate that consumers are highly interested in having access to information that
provides insight into the quality of care that a physician provides.
12
6. Consumers want to work together with their physicians and be included in the
decision-making process but do not want to assume sole or primary responsibility for
their care.Recent shifts in the U.S. health care system have put a greater focus on the role of the
individual consumer in managing both their health and their health care benefits. Insurance
product types that emphasize the role of the individual consumer, such as defined contribution
models, have received increased attention as employers and the health care system struggle to
control escalating costs. Similarly, disease management programs, many of which focus on the role
of the patient to self-manage their condition, have become widely employed as an effort to
address many of the chronic diseases that require extensive resources to manage and treat. With
this increased emphasis on the individual’s responsibility for their own health and health care, it is
important to investigate consumers’ perspectives on their enhanced role in the health care system.
During the focus group sessions, the moderator described Patient-Centered Care as “being
responsive to and respectful of patients” and “making sure patients have what they need to
participate in their own care.” The moderator presented several definitions of Patient-Centered
Care, and participants were asked to discuss each definition and choose the one that best
represented the concept. These definitions were:
• Doctor has good communication skills and works with the patient to manage his or her
own health.
• Doctor and patient work together to make decisions that take into account the patient’s
needs.
• Doctor provides patient with the education and support to manage his or her own health.
The participants clearly preferred definitions of Patient-Centered Care that focused on a
reciprocal relationship between the patient and the doctor, two-way communication, and shared
decision-making. The participants disliked the definition “doctor provides patient with the
education and support to manage his or her own health,” perceiving this as emphasizing one-way
communication that leaves the patient to make decisions on his or her own. Several participants
specifically disliked this definition because they felt that the “doctor is the expert” and that
patients are ill equipped to make these decisions on their own.
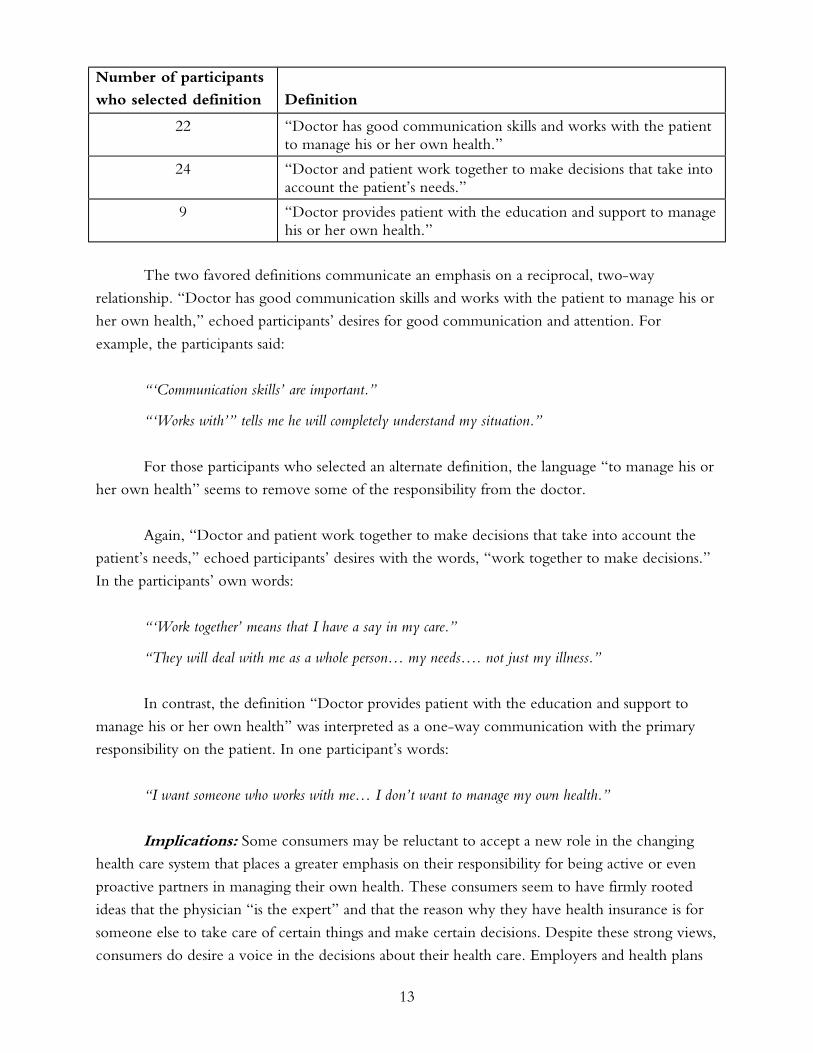
Below is a summary of the participants’ selections of the definition that is most meaningful
and most closely describes the concept of Patient-Centered Care.
13
Number of participants
who selected definition Definition
22 “Doctor has good communication skills and works with the patient to manage his or her own health.”
24 “Doctor and patient work together to make decisions that take into account the patient’s needs.”
9 “Doctor provides patient with the education and support to manage his or her own health.”
The two favored definitions communicate an emphasis on a reciprocal, two-way
relationship. “Doctor has good communication skills and works with the patient to manage his or
her own health,” echoed participants’ desires for good communication and attention. For
example, the participants said:
“‘Communication skills’ are important.”
“‘Works with’” tells me he will completely understand my situation.”
For those participants who selected an alternate definition, the language “to manage his or
her own health” seems to remove some of the responsibility from the doctor.
Again, “Doctor and patient work together to make decisions that take into account the
patient’s needs,” echoed participants’ desires with the words, “work together to make decisions.”
In the participants’ own words:
“‘Work together’ means that I have a say in my care.”
“They will deal with me as a whole person… my needs…. not just my illness.”
In contrast, the definition “Doctor provides patient with the education and support to
manage his or her own health” was interpreted as a one-way communication with the primary
responsibility on the patient. In one participant’s words:
“I want someone who works with me… I don’t want to manage my own health.”
Implications: Some consumers may be reluctant to accept a new role in the changing
health care system that places a greater emphasis on their responsibility for being active or even
proactive partners in managing their own health. These consumers seem to have firmly rooted
ideas that the physician “is the expert” and that the reason why they have health insurance is for
someone else to take care of certain things and make certain decisions. Despite these strong views,
consumers do desire a voice in the decisions about their health care. Employers and health plans
14
that wish to promulgate products and systems that place a greater emphasis on the consumers’ role
will need to closely manage the message about how much responsibility is expected of the patient.
For measure development activities and reporting frameworks, effort must be made to include
dimensions of how well a physician communicates with patients and provides a voice for the
patient in decision-making.
7. The Medicare population appears to be more accepting and forgiving of physician
errors.
The participants in NCQA’s focus groups recognized that safety is an important issue in health
care and were able to note several examples of medical errors (e.g., prescribing the wrong drug or
operating on the wrong limb). Despite this awareness, participants in all of the groups expressed a
belief that health care can never be truly safe and that the human component of physician care
creates an inherent potential for medical mistakes. This notion was particularly evident in the
Medicare group, indicating that the Medicare consumers may be more reluctant to undermine or
question a doctor’s authority.
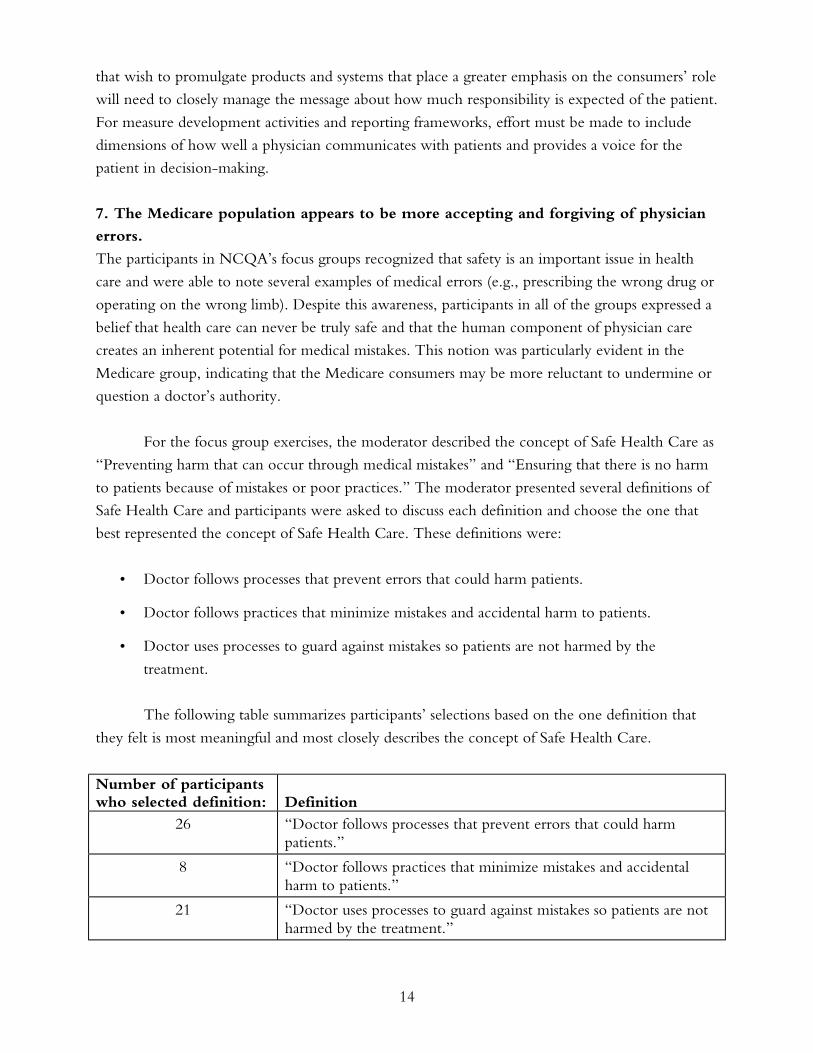
For the focus group exercises, the moderator described the concept of Safe Health Care as
“Preventing harm that can occur through medical mistakes” and “Ensuring that there is no harm
to patients because of mistakes or poor practices.” The moderator presented several definitions of
Safe Health Care and participants were asked to discuss each definition and choose the one that
best represented the concept of Safe Health Care. These definitions were:
• Doctor follows processes that prevent errors that could harm patients.
• Doctor follows practices that minimize mistakes and accidental harm to patients.
• Doctor uses processes to guard against mistakes so patients are not harmed by the
treatment.
The following table summarizes participants’ selections based on the one definition that
they felt is most meaningful and most closely describes the concept of Safe Health Care.
Number of participants who selected definition: Definition
26 “Doctor follows processes that prevent errors that could harm patients.”
8 “Doctor follows practices that minimize mistakes and accidental harm to patients.”
21 “Doctor uses processes to guard against mistakes so patients are not harmed by the treatment.”
15
With this exercise, some participants were concerned by the use of certain words. For
example, the majority of participants favored the definition “Doctor follows processes that prevent
errors that could harm patients.” However, their rationale for this choice was based on the fact
that they disliked some of the words used in the other definitions:
“I don’t like, ‘guard against” or ‘minimize…’ ‘Prevent errors’ sounds more positive.”
The second most favored was the definition “Doctor uses processes to guard against
mistakes so patients are not harmed by the treatment.” Participants favoring this definition stated:
“You can only ‘guard against,’ you can not prevent errors.”
“It encompasses the other two definitions.”
“Accidents do occur... this definition takes that into account and I like, ‘are not harmed by the
treatment’.”
Some participants rejected the definition “Doctor follows practices that minimize mistakes
and accidental harm to patients” because of its negative tone, indicating that some words used to
describe measurement concepts may be so strong that the words divert attention from the
information communicated through the measure. For example, one participant disliked the
definition because:
“It’s such a negative statement… it scares me.”
In addition to strongly worded negative terms, participants did not like some terms that
neither the moderator nor NCQA staff had predicted. In several focus group sessions, participants
preferred the word “processes” to the word “practices” when used in the context of office
processes or practices. This was true even by participants who selected a definition that used the
word “practices” but who indicated a dislike for the term when the group discussed the term out
of the context of the definition.
Implications: It appears that many consumers have adopted fatalistic beliefs regarding the
ability for the health care system to prevent medical errors and mistakes. This idea must be further
tested to confirm whether this is a widespread view among consumers. If this belief is prevalent,
then national education efforts should be employed to inform the public about variation in safety
and substantial problems with medical errors. Until consumers understand that medical errors can
be prevented, they may devalue or misunderstand quality of care information that addresses the
ability of doctors or the health care system as a whole to protect patient safety.
16
8. Consumers perceive a distinction between accountability for “physician” care and
for “health” care.
The U.S. health care system is becoming increasingly fragmented. The major players of the
system no longer include only the physician, hospital, and insurer but can include a large number
of other entities that have taken on discrete functions that were previously performed by larger
organizations. Developers of measures and reporting frameworks should not make assumptions
about the way consumers perceive the health care system and issues of quality. One assumption
that was made by NCQA staff was that consumers would perceive “health care” to encompass the
care a physician provides in a one-on-one interaction with a patient. During the focus groups,
participants clearly struggled with the use of the term “health care” in the three main concepts
(Health Care That Works, Patient-Centered Health Care, Safe Health Care). The participants
suggested that measurement areas and concepts should clearly specify the physician as the actor in
any measurement describing a component of the service a physician provides. These participants
suggested that better terms for the three main concepts be Physician Care That Works, Patient-
Centered Physician Care (later more accurately described as the Patient–Doctor Relationship),
and Safe Physician Care.
Implications: As the health care system changes, research must be conducted to probe
how consumers relate to this less cohesive structure. Specifically, researchers should explore
consumer perceptions of the various components of the health care system and how consumers
perceive that the components work together. Through the NCQA focus groups, we found that
consumers perceive a distinction between physician care and care or services that are provided on
a systemwide basis. Without a broader understanding of these ideas, organizations are likely to
make assumptions about consumers’ knowledge and perception of the health care system that can
cause consumers to devalue performance measurement information. Clearly, consumers do have
the ability and prefer to distinguish care provided by a physician (“physician care”) from care or
services that are provided by a system (“health care”).
9. Consumers are very sensitive to word choices; when using text to describe
measures or concepts, each word may have a profound impact on consumer
comprehension.
The various report cards and other frameworks (e.g., healthchoices.org) currently used for
reporting quality information to consumers employ textual descriptions that accompany the results
from the quantitative measures. As has been seen through testing of specific report card formats,
the words chosen for those textual descriptions have as much impact on a user’s impression of the
information as the actual quantitative measures themselves. Results from NCQA’s focus groups
indicate that consumers may view some words so negatively that the use of the words may mask
or confuse the message behind the quantitative measures.
17
As was discussed earlier, some participants struggled with the wording of the concept of
Patient-Centered Care. The participants found the wording of the individual measurement areas
even more troublesome. One focus group exercise required the participants to consider a
measurement area (e.g., “doctor provides the right treatment for short-term illness”) and identify
the concept that corresponds with the measurement area (e.g., Health Care That Works). When
presented with measurement areas and examples, some participants felt that some of the words
used in the measurement areas had multiple meanings. For example, the term “right” can have
multiple meanings and the interpretation of “right” can affect whether a measurement area
corresponds with Health Care That Works or Safe Health Care. In the measurement area “doctor
provides the right treatment for short-term illness,” right can mean “correct,” as in the doctor
provided the correct treatment for the illness, or it can mean “effective,” as in the doctor
provided a treatment that led to an improvement in the patient’s condition.
Similarly, participants disliked some words because of their tone. Participants from several
groups were uncomfortable with the word “scientific” because the tone of the word implies
experimentation or a sterile environment that does not lend itself to physician care. Participants
disliked other words because they were too vague. They were very skeptical of words such as
“helpful” and “guard,” citing these words as indicating weaker action or less successful care than
words like “proven to work” and “preventing mistakes.”
Implications: The results from this exercise show that how a measure is described makes
a difference and that consumers may react to words without paying attention to the underlying
idea behind a message. Therefore, developers of reporting frameworks must not only test
reporting formats and the visual aspect of the framework but must also evaluate how users are
interpreting the textual descriptions that accompany the report.
CONCLUSIONS AND IMPLICATIONS
The primary finding of this focus group study is that consumers’ ability to understand and value
health care quality information is enhanced when a consumer-friendly framework is employed.
Moreover, when an appropriate framework is provided, consumers report that they value
information on physician office quality related to patient safety and effectiveness of care, as well as
areas such as office location and elements of the physician–patient relationship.
The implications of these findings, while needing further confirmation in studies with a
more rigorous experimental design, are important for those involved in evaluation or reporting of
elements of quality at the level of physician office practice. The focus groups provided
confirmation that there are major instabilities in consumer perceptions of quality. The marked
dependence of consumer perceptions on word choice is one indication of this instability. Small
changes in wording produced relatively large changes in how consumers understood various

18
concepts. This has been attributed in prior studies to the complexity of health care and the limited
understanding that most consumers have of it.
In addition, if no framework is provided, which is the case with most surveys and prior
studies, consumers indicate that they see quality as related almost exclusively to issues in the
physician–patient relationship. These include such items as listening, communication, and bedside
manner. By contrast, the IOM (in their report, Crossing the Quality Chasm) and most health
professionals see this as only one domain (patient-centeredness) of quality and see other domains,
such as patient safety and effectiveness, as of equal or even greater importance. This has led some
to conclude that consumers are not “interested in” or do not value areas of quality outside of
patient-centeredness and that there is a major rift between consumers and physicians in their
views of health care quality. However, our focus group findings suggest that this apparent rift may
not be as large as assumed, since when provided with explanations and a framework for
understanding other aspects of quality, consumers do express interest in knowing about the
domains of effectiveness and safety. While some concepts are still difficult for consumers,
especially those with less education, this study suggests that there can be a much closer
relationship between what “experts” see as important in quality and what consumers might value
in choosing or selecting practices.
Clearly, these findings from a set of focus groups, which were only one part of a larger
project, are subject to major limitations. The larger study included an extensive literature review
and explorations of how existing measures of quality might be adapted to inform consumers about
physician office practice quality. Moreover, the 55 participants were recruited from insured
managed care plan populations. Although they were enrolled in a variety of plans—commercial,
Medicare, and Medicaid—important differences may exist between this group and the population
of the United States at large. While we attempted to select individuals from different racial,
ethnic, and income groups, as well as those having different levels of experience with the health
care system, they were all from a relatively small geographic area (the mid-Atlantic region) and
did not include substantial numbers of younger persons or the uninsured. In addition, the study,
by design, was meant to be qualitative and interactive.
Clearly, much work remains to be done in designing and using frameworks that will
reveal a critical level of consumer understanding, as well as in exploring if the “value” expressed
by consumers in our qualitative focus group study translates into actual use of the information in
practice. A major barrier to consumer decision-making remains the lack of availability of reliable
and valid information on quality at the physician office practice level. While these issues must be
addressed, the conclusion that consumers can understand and value information on the safety and
effectiveness of physician office practice, if confirmed, has important implications for clinicians
and consumers, as well as those interested in monitoring, improving, and reporting on physician
office practice quality.
19
APPENDIX A: FOCUS GROUP PARTICIPANTS, SCHEDULE, AND PROTOCOL
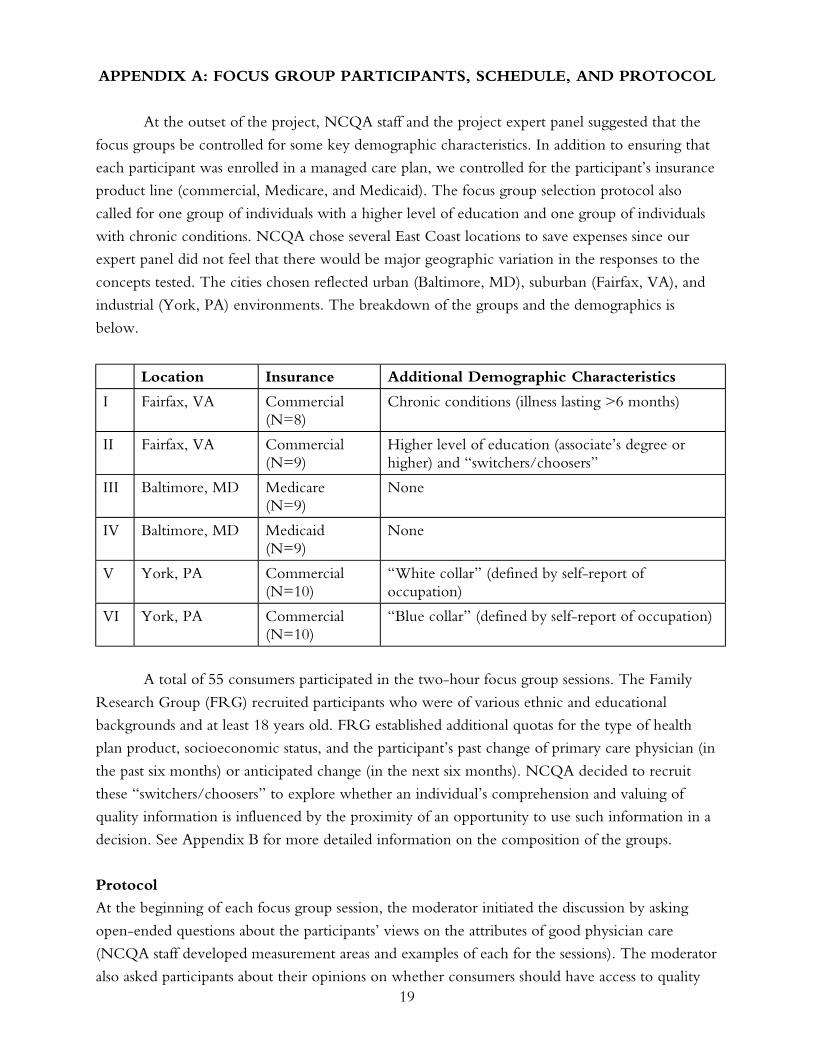
At the outset of the project, NCQA staff and the project expert panel suggested that the
focus groups be controlled for some key demographic characteristics. In addition to ensuring that
each participant was enrolled in a managed care plan, we controlled for the participant’s insurance
product line (commercial, Medicare, and Medicaid). The focus group selection protocol also
called for one group of individuals with a higher level of education and one group of individuals
with chronic conditions. NCQA chose several East Coast locations to save expenses since our
expert panel did not feel that there would be major geographic variation in the responses to the
concepts tested. The cities chosen reflected urban (Baltimore, MD), suburban (Fairfax, VA), and
industrial (York, PA) environments. The breakdown of the groups and the demographics is
below.
Location Insurance Additional Demographic Characteristics
I Fairfax, VA Commercial (N=8)
Chronic conditions (illness lasting >6 months)
II Fairfax, VA Commercial (N=9)
Higher level of education (associate’s degree or higher) and “switchers/choosers”
III Baltimore, MD Medicare (N=9)
None
IV Baltimore, MD Medicaid (N=9)
None
V York, PA Commercial (N=10)
“White collar” (defined by self-report of occupation)
VI York, PA Commercial (N=10)
“Blue collar” (defined by self-report of occupation)
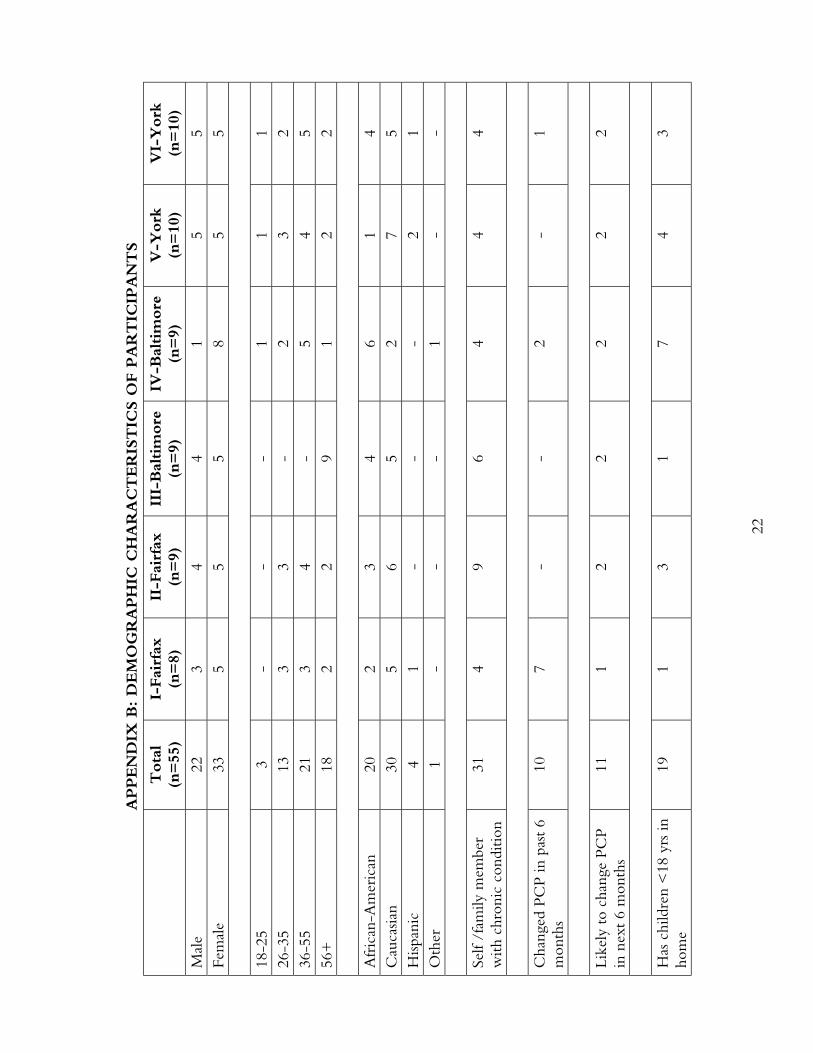
A total of 55 consumers participated in the two-hour focus group sessions. The Family
Research Group (FRG) recruited participants who were of various ethnic and educational
backgrounds and at least 18 years old. FRG established additional quotas for the type of health
plan product, socioeconomic status, and the participant’s past change of primary care physician (in
the past six months) or anticipated change (in the next six months). NCQA decided to recruit
these “switchers/choosers” to explore whether an individual’s comprehension and valuing of
quality information is influenced by the proximity of an opportunity to use such information in a
decision. See Appendix B for more detailed information on the composition of the groups.
Protocol
At the beginning of each focus group session, the moderator initiated the discussion by asking
open-ended questions about the participants’ views on the attributes of good physician care
(NCQA staff developed measurement areas and examples of each for the sessions). The moderator
also asked participants about their opinions on whether consumers should have access to quality
20
information about individual physicians. After this icebreaker, the moderator provided some basic
information about NCQA and its mission, along with an example and explanation of a sample
health plan report card.
After the opening exercise, the moderator used poster boards to present each of the three
concepts identified through the IOM report—effectiveness, patient-centeredness, and safety.
Consumer-friendly labels were used for each of the concepts—”Health Care That Works”
(effectiveness), “Patient-Centered Care” (patient-centeredness), and “Safe Health Care” (safety).
The moderator described each concept and presented three similar definitions for each concept.
For each concept participants then selected the one definition that was “most meaningful and
most closely described the concept.” The moderator then led the group through a brief discussion
to elicit the participants’ rationales for their choices. Using a scale of 5 to 1, with “5” meaning
“Extremely Important” and “1” meaning “Not at All Important,” the participants then rated how
important each concept was to their choice of physician. Refer to Appendix C for the concept
definitions that were tested.
Following the discussion on the concepts’ definitions, the moderator led the group
through an exercise that probed their understanding of detailed measurement areas that
correspond to each of the three concepts. Because of the significant amount of research that has
been conducted on the Computer Assessment of Health Plans (CAHPS) survey and issues of
patient centeredness, NCQA chose to concentrate the more detailed exercises on measurement
areas related to Health Care That Works (effectiveness) and Safe Health Care (safety). The
protocol for this exercise was slightly different in the first two groups than in the remaining focus
groups. In focus groups I and II (Fairfax), the moderator provided the participants with “Post-It”
notes that were preprinted with 12 detailed measurement areas that corresponded to one of the
three concepts. An example was also provided for each of the 12 measurement areas. Participants
were instructed to read the measurement area, identify the concept (Health Care That Works or
Safe Health Care) that most closely corresponded with the measurement area, and affix the Post-It
note to the corresponding poster board that included the concept and its definition. The
moderator then asked the participants to describe their interpretations of the measurement area
and the rationales for their choices.
Due to logistical challenges, the exercise with the Post-It notes proved to be problematic.
Therefore, the moderator changed the protocol slightly for the remaining groups. In the
remaining focus groups, participants were provided with a list of the 12 measurement areas and
asked to identify the concept (Health Care That Works or Safe Health Care) that most closely
corresponded with the measurement area. Participants indicated their choice by circling the
corresponding concept on a worksheet. Again, the moderator followed the exercise with a
discussion about the participants’ interpretations of the measurement concepts and the rationales
for their choices. Refer to Appendix D for the measurement concepts that were tested.
21
The focus group sessions concluded with a “Board of Directors” exercise, in which
participants assumed the role of NCQA’s leadership and were asked to identify other important
information they would like included in a report on physician quality.
22
APPEN
DIX
B: D
EM
OG
RA
PH
IC C
HA
RA
CT
ER
IST
ICS O
F P
AR
TIC
IPA
NT
S
T
ota
l (n
=55
) I-
Fai
rfax
(n
=8)
II
-Fai
rfax
(n
=9)
II
I-B
altim
ore
(n
=9)
IV
-Bal
tim
ore
(n
=9)
V
-York
(n
=10
) V
I-Y
ork
(n
=10
)
Mal
e 22
3
4 4
1 5
5 Fe
mal
e 33
5
5 5
8 5
5
18
-25
3 -
- -
1 1
1 26
-35
13
3 3
- 2
3 2
36-5
5 21
3
4 -
5 4
5 56
+
18
2 2
9 1
2 2
Afr
ican
-Am
eric
an
20
2 3
4 6
1 4
Cau
casia
n 30
5
6 5
2 7
5 H
ispan
ic
4 1
- -
- 2
1 O
ther
1
- -
- 1
- -
Self
/fam
ily m
embe
r w
ith c
hron
ic c
ondi
tion
31
4 9
6 4
4 4
Cha
nged
PC
P in
pas
t 6
mon
ths
10
7 -
- 2
- 1
Like
ly t
o ch
ange
PC
P in
nex
t 6
mon
ths
11
1 2
2 2
2 2
Has
chi
ldre
n <
18 y
rs in
ho
me
19
1 3
1 7
4 3
23
APPENDIX C: THREE MAIN CONCEPTS TESTED
Concept Definitions
Health Care That Works (Effective Health Care)
Definitions tested:
• Doctor uses procedures that have been tested and shown to produce good results.
• Doctor provides medical care that is scientifically proven to be helpful.
• Doctor provides medical care proven to work.
Safe Health Care
Definitions tested:
• Doctor follows processes that prevent errors that could harm patients.
• Doctor follows practices that minimize mistakes and accidental harm to patients.
• Doctor uses processes to guard against mistakes so patients are not harmed by
the treatment.
Patient-Centered Health Care
Definitions tested:
• Doctor has good communication skills and works with the patient to manage his or her
own health.
• Doctor and patient work together to make decisions that take into account the
patient’s needs.
• Doctor provides patient with the education and support to manage his or her own health.
24
APPENDIX D: INDIVIDUAL MEASUREMENT CONCEPTS TESTED
Individual Measurement Concepts
1. “Doctor provides the right treatment for short-term illness.” Example: Doctor provides
antibiotics for strep throat infection.
2. “Doctor writes accurate prescriptions.” Example: Doctor writes prescriptions that can be
accurately read.
3. “Doctor has up-to-date patient records.” Example: Doctor has up-to-date information on
patient drug allergies.
4. “Doctor follows-up with patient after a serious illness.” Example: Doctor ensures stroke
patients get the right amount of rehabilitation.
5. “Doctor provides the right treatments for ongoing illness.” Example: Doctor gives the right
medication for diabetes.
6. “Doctor’s license is in good standing.” Example: Doctor has no disciplinary actions against
license.
7. “Doctor follows the recommended procedures when performing surgery in the office.”
Example: Doctor’s tools are properly cleaned and sterilized.
8. “Doctor ensures proper maintenance and storage of equipment and medication.” Example: Doctor ensures that medications are properly labeled.
9. “Doctor identifies illness early.” Example: Doctor tests for cancer.
10. “Doctor has systems that ensure patients gets test results without mix-up or delay.”
Example: Doctor notifies patient of blood test results as soon as the results are available.
11. “Doctor has adequate experience performing a specific procedure.” Example: Number of
times the doctor has performed heart surgery.
12. “Doctor provides preventive care at the right time.” Example: Doctor offers flu shots to
patients prior to the flu season.
25
APPENDIX E: LIST OF EXPERT PANEL MEMBERS
1. Carolyn M. Clancy, M.D., Agency for Healthcare Research and Quality
2. Kathryn Coltin, M.P.H., Harvard Pilgrim HealthCare
3. Carol Cronin, M.S.W., Independent Consultant
4. François de Brantes, M.B.A., General Electric
5. Susan Edgman-Levitan, P.A., Consultant
6. Arnold Epstein, M.D., M.A., Harvard School of Public Health
7. Barbara Fleming, M.D., Ph.D., Centers for Medicare and Medicaid Services
8. Judith Hibbard, Dr.P.H., University of Oregon
9. Sherrie Kaplan, Ph.D., M.P.H., Tufts University School of Medicine
10. Trudy Lieberman, B.S., Consumer Reports
11. Debra L. Ness, M.S.W., National Partnership for Women and Families
12. R. Heather Palmer, M.B.B.Ch., S.M., Harvard School of Public Health
13. Shoshanna Sofaer, Dr.P.H., Baruch College, School of Public Affairs

26
REFERENCES
Acs, G., Long, S. H., Marquis, M. S. et al. (1996). “Self-Insured Employer Health Plans:
Prevalence, Profile, Provisions, and Premiums.” Health Affairs 15 (2): 266–78.
Beaulieu, N. (2002). “Quality Information and Consumer Health Choices.” Journal of Health Economics 21: 43–63.
Booske, B. C., Sainfort, F., and Hundt, A. S. (1999). “Eliciting Consumer Preferences for Health Plans.” HSR: Health Service Research 34 (4): 839–54.
Cleary, P., and Edgman-Levitan, S. (1997). “Perspectives Health Care Quality: Incorporating Consumer.” Journal of the American Medical Association 278 (19): 1608–12.
Cunningham, P. J., Denk, C., and Sinclair, M. (2001). “Do Consumers Know How Their Health Plan Works?” Health Affairs 20 (2): 159–66.
Druss, B., Miller, C., Rosenheck, R. et al. (2002). “Mental Health Care Quality Under Managed Care in the United States: A View from the Health Employer Data and Information Set (HEDIS).” American Journal of Psychiatry 159 (5): 860–62.
Druss, B., Rosenheck, R., and Sledge, W. (2000). “Health and Disability Costs of Depressive Illness in a Major U.S. Corporation.” American Journal of Psychiatry 157 (8): 1274–78.
Druss, B., Schlesinger, M., and Allen, H. (2001). “Depressive Symptoms, Satisfaction with Health Care, and 2-Year Work Outcomes in an Employed Population.” American Journal of Psychiatry 158 (5): 731–34.
Edgman-Levitan, S., and Cleary, P. D. (1996). “What Information do Consumers Want and Need?” Health Affairs 15 (4): 42–56.
Feldman, R., Christianson, J., and Schultz, J. (2000). “Do Consumers Use Information to Choose a Health-Care Provider System?” The Milbank Quarterly 78 (1): 47–77.
Fowles, J., Kind, E., Braun, B. et al. (2000). “Consumer Responses to Health Plan Report Cards in Two Markets.” Medical Care 38 (5): 469–81.
General Accounting Office. (1995). Employers and Individual Consumers Want Additional Information on Quality. Washington, D.C.: GAO.
Gibbs, D. A., Sangl, J. A., and Burrus, B. (1996). “Consumer Perspectives on Information Needs for Health Plan Choices.” Health Care Finance Review 18 (1): 55–73.
Health Service Research, I. (1999). Summary of Discussions: Interest and Issues Associated with the Development of Sub-Health Plan Consumer Assessment Surveys. Washington, D.C.: Agency for Health Care Policy and Research, U.S. Department of Health and Human Services.
Hibbard, J. H., Slovic, P., Peters, E. et al. (2001). “Is the Informed-Choice Policy Approach Appropriate for Medicare Beneficiaries?” Health Affairs 20 (3): 199–204.
Hibbard, J. H. (1998). “Use of Outcome Data by Purchases and Consumers: New Strategies and New Dilemmas.” International Journal for Quality in Health Care 10 (6): 503–8.
Hibbard, J. H., Berkman, N., and McCormack, L. (2001). “The Impact of a CAHPS Report on Employee Knowledge, Beliefs, and Decisions.” Medical Care Research and Review 59 (1): 102–15.
Hibbard, J. H., Harris-Kojetin, L., Mullin, P. et al. (2000). “Increasing the Impact of Health Plan Report Cards by Addressing Consumer Concerns.” Health Affairs 19 (5): 138–43.
27
Hibbard, J. H., Slovic, P., Peters, E .M. et al. (2002) “Strategies for Reporting Health Plan Performance Information to Consumers: Evidence from Controlled Studies.” HSR: Health Services Research 37 (2).
Hibbard, J. H., and Jewett, J. J. (1996). “What Type of Quality Information Do Consumers Want in a Health Care Report Card?” Medical Care Research and Review 53 (1): 28–47.
Hibbard, J. H., and Jewett, J. J. (1997). “Will Quality Report Cards Help Consumers?” Health Affairs 16 (3): 218–28.
Hibbard, J. H., Slovic, P., and Jewett, J. J. (1997b). “Informing Consumer Decisions in Health Care: Implications from Decision-Making Research.” The Milbank Quarterly 75 (3): 395–415.
Hsee, C. K. (1995). “Elastic Justification: How Tempting But Task-Irrelevant Factors Influence Decisions.” Organizational Behavior and Human Decision Processes 62: 330–37.
Hsee, C. K. (1996). “The Evaluability Hypothesis: An Explanation for Preference Reversals Between Joint and Separate Evaluations of Alternatives.” Organizational Behavior and Human Decision Processes 67: 247–57.
Hsee, C. K. (1998). “Less Is Better: When Low-Value Options are Valued More Highly Than High-Value Options.” Journal of Behavioral Decision Making 11: 107–21.
Isaacs, S. (1996). “Consumers’ Information Needs: Results of a National Survey.” Health Affairs 15 (4): 31–41.
Jewett, J., and Hibbard, J. (1996). “Comprehension of Quality Care Indicators: Differences Among Privately Insured, Publicly Insured, and Uninsured.” Health Care Financing Review 18 (1): 75–94.
Henry J. Kaiser Family Foundation. (2000). National Survey on American as Health Care Consumers: An Update on the Role of Quality Information. Kaiser Family Foundation/Agency for Healthcare Research and Quality.
Kroll Letwat, J. (1999). “The Current Quality of Health Plan Report Cards.” Journal of Medical Systems 23 (4): 325–33.
Lubalin, J. S., and Harris-Kojetin, L. D. (1999). “What Do Consumers Want and Need to Know in Making Health Care Choices?” Medical Care Research and Review 56 (Suppl. 1): 67–102.
Midwest Business Group on Health. (2000). How We Choose Doctors-What Is and What Could Be. A Report on the MBGH Doctor Data Project. Consumer Information and Education Committee, MBGH.
McCormack, L., Garfinkel, S., Schnaier, M. et al. (1996). “Consumer Information Development and Use.” Health Care Finance Review 18 (15).
McCormack, L. A., Garfinkel, S., Hibbard, J. H. et al. (In press.). “Health Plan Decision-making with New Medicare Information Materials.” HSR: Health Services Research.
McGee, J., Kanouse, D., Sofaer, S. et al. (1999). “Making Survey Results Easy to Report to Consumers: How Reporting Needs Guided Survey Design of CAHPS. Consumer Assessment of Health Plans Study.” Medical Care 37 (3): MS32–MS40.
McGee, J., Sofaer, S., and Kreling, B. (1996). Findings from Focus Groups Conducted from National Committee for Quality Assurance, Medicare and Medicaid Consumer Information Projects. Washington, D.C.: NCQA.
28
McGlynn, E. (1997). “Choosing and Evaluating Clinical Performance Measures.” The Joint Commission Journal on Quality Improvement 24 (9): 470–79.
Mechanic, D. (1989). “Consumer Choices Among Health Insurance Options.” Health Affairs 8 (1): 138–48.
Moore, S., and Bopp, K. (1999b). “How Consumers Evaluate Health Care Quality: Part II.” Health Marketing Quarterly 17 (1).
Moore, S., and Bopp, K. (1999c). “How Consumers Evaluate Health Care Quality: Part III.” Health Marketing Quarterly 17 (2): 1–6.
Mukamel, D. B., and Mushlin, A. I. (2001). “The Impact of Quality Report Card on Choice of Physicians, Hospitals, and HMOs: a Midcourse Evaluation.” The Joint Commission Journal on Quality Improvement 27 (1): 20–27.
National Committee for Quality Assurance. (1994). Consumer Information Project Final Report. Washington, D.C.
Nelson, E., Batalden, P., Plume, S. et al. (1995). “Performance Measures and Measurement: Report Cards or Instrument Panels: Who Needs What?” Journal Quality Improvement 21 (4): 155.
Ouschan, R., Sweeney, J., and Johnson, L. (2000). “Dimensions of Patient Empowerment: Implications for Professional Services Marketing.” Health Marketing Quarterly 18 (1/2): 99–114.
Pham, H., Frick, K., Diener-West, M. et al. (2002). “Is Health Plan Employer Data and Information Set Performance Associated with Withdrawal from Medicare Managed Care?” Medical Care 40 (3): 212–26.
RAND. (2000). Taking the Pulse of Californians: A Survey of Consumer Attitudes on Health Care Quality.: The RAND/California HealthCare Foundation Report: Volume 1.
Risker, D. C. (2000). “Factors Influencing Employee Health Plan Choice in the Corporate Setting.” Health Marketing Quarterly 18 (1/2): 15–27.
Robinson, S., and Brodie, M. (1997). “Understanding the Quality Challenge for Health Consumers: The Kaiser/AHCPR Survey.” The Joint Commission Journal on Quality Improvement 23 (5): 239–44.
Sainfort, F., and Brooske, B. C. (1996). “Role of Information in Consumer Selection of Health Plans.” Health Care Finance Review 18 (1): 31–54.
Sangl, J. A., and Wolf, L. F. (1996). “Role of Consumer Information in Today’s Health Care System.” Health Care Finance Review 18 (1): 1–8.
Scanlon, D. P., Chernew, M., McLaughlin C. et al. (2002). “The Impact of Health Plan Report Cards on Managed Care Enrollment.” Journal of Health Economics 21: 19–41.
Scanlon, D. P., Chernew, M., and Lave, J. R. (1997). “Consumer Health Plan Choice: Current Knowledge and Future Directions.” Annual Review Public Health 18: 507–29.
Scanlon, D., Rolph, E., Darby, C. et al. (2000). “Are Managed Care Plans Organizing for Quality?” Medical Care Research and Review 57 (Suppl.): 9–32.
Schneider, E. C., and Epstein, A. (1998). “Use of Public Performance Reports: A Survey of Patients Undergoing Cardiac Surgery.” Journal of the American Medical Association 279 (20): 1638–42.
29
Scotti, D. J., Bonner, P. G., and Wiman, A. R. (1986). “An Analysis of the Determinants of HMO Reenrollment Behavior: Implications for Theory and Policy.” Journal of Health Care Marketing 6 (2): 7–16.
Slovic, P. (1995). “The Construction of Preference.” American Psychologist 50: 364–71.
Sofaer, S. (1997). “How Will We Know if We Got It Right? Aims, Benefits, and Risks of Consumer Information Initiatives.” The Joint Commission Journal on Quality Improvement 23 (5): 258–64.
Sofaer, S., Gruman, J., Connaughton, S. et al. (2000). “Developing Performance Indicators that Reflect an Expanded View of Health.” The Joint Commission Journal on Quality Improvement 26 (4): 189–202.
Stone, E., Heinold, J., Ewing, L., and Schoenbaum, S. (2002). Accessing Physician Information on the Internet. New York: The Commonwealth Fund.
Trandel-Korenchuk, D. (1998). “The Influence of the Mass Media on The Selection of Physicians.” Journal of Ambulatory Care Management 21 (1): 48–66.
Tumlinson, A., Bottigheimer, H., Mahoney, P. et al. (1997). “Choosing a Health Plan: What Information Will Consumers Use?” Health Affairs 16(3): 229–38.
Veroff, D., Gallagher, P., Wilson, V. et al. (1998). “Effective Reports for Health Care Quality Data: Lessons from a CAHPS Demonstration in Washington State.” International Journal for Quality in Health Care 6(6): 555–60.
VHA. (2000). Consumer Demand for Clinical Quality: The Giant Awakens. VHA, Inc.

30
RELATED PUBLICATIONS
In the list below, items that begin with a publication number are available from The Commonwealth
Fund by calling its toll-free publications line at 1-888-777-2744 and ordering by number. These
items can also be found on the Fund’s website at www.cmwf.org. Other items are available
from the authors and/or publishers.
#563 Escape Fire: Lessons for the Future of Health Care (November 2002). Donald M. Berwick. In this monograph, Dr. Berwick outlines the problems with the health care system—medical errors, confusing and inconsistent information, and a lack of personal attention and continuity in care—and then sketches an ambitious program for reform. Achieving and Sustaining Improved Quality: Lessons from New York State and Cardiac Surgery (July/August 2002). Mark R. Chassin. Health Affairs, vol. 21, no. 4. Copies are available from Health Affairs, 7500 Old Georgetown Road, Suite 600, Bethesda, MD 20814-6133, Tel: 301-656-7401 ext. 200, Fax: 301-654-2845. Available online at http://www.healthaffairs.org/readeragent.php?ID=/usr/local/apache/sites/ healthaffairs.org/htdocs/Library/v21n4/s8.pdf. Improving Quality Through Public Disclosure of Performance Information (July/August 2002). David Lansky. Health Affairs, vol. 21, no. 4. Copies are available from Health Affairs, 7500 Old Georgetown Road, Suite 600, Bethesda, MD 20814-6133, Tel: 301-656-7401 ext. 200, Fax: 301-654-2845. Available online at http://www.healthaffairs.org/readeragent.php?ID=/usr/local/apache/sites/healthaffairs.org/htdocs/ Libraryv21n4/s9.pdf. Factors Affecting Response Rates to the Consumer Assessment of Health Plans Study Survey (June 2002). Alan M. Zaslavsky, Lawrence B. Zaborski, and Paul D. Cleary. Medical Care, vol. 40, no. 6. Copies are available from Paul D. Cleary, Department of Health Care Policy, Harvard Medical School, 180 Longwood Avenue, Boston, Massachusetts 02115, E-mail: [email protected]. #542 Comparison of Health Care System Views and Experiences in Five Nations, 2001 (May 2002). Cathy Schoen, Robert J. Blendon, Catherine M. DesRoches, and Robin Osborn. Based on The Commonwealth Fund 2001 International Health Policy Survey, this issue brief compares health care experiences of adults in Australia, Canada, New Zealand, the United Kingdom, and the United States. The data reveal that the United States has the highest share of residents facing access problems, driven in large part by the difficulty many face in paying for care. #539 Improving Health Care Quality: Can Federal Efforts Lead the Way? (April 2002). Juliette Cubanski and Janet Kline. This issue brief, prepared for the 2002 Commonwealth Fund/Harvard University Bipartisan Congressional Health Policy Conference, discusses the ways in which various federal agencies can work to improve health care quality for all Americans. Available online only at www.cmwf.org. #535 Assessing the Threat of Bioterrorism: Are We Ready? (April 2002). Patricia Seliger Keenan and Janet Kline. This issue brief, prepared for the 2002 Commonwealth Fund/Harvard University Bipartisan Congressional Health Policy Conference, examines federal preparedness, state and local infrastructure, congressional actions to improve preparedness, and regulatory and legal policies regarding the threat of bioterrorism in the United States. Available online only at www.cmwf.org. #534 Room for Improvement: Patients Report on the Quality of Their Health Care (April 2002). Karen Davis, Stephen C. Schoenbaum, Karen Scott Collins, Katie Tenney, Dora L. Hughes, and Anne-Marie J. Audet. Based on the Commonwealth Fund 2001 Health Care Quality Survey, this report finds that many
31
Americans fail to get preventive health services at recommended intervals or receive substandard care for chronic conditions, which can translate into needless suffering, reduced quality of life, and higher long-term health care costs. #520 Quality of Health Care in the United States: A Chartbook (April 2002). Sheila Leatherman and Douglas McCarthy. This first-of-its-kind portrait of the state of health care quality in the United States documents serious gaps in quality on many crucial dimensions of care: lack of preventive care, medical mistakes, substandard care for chronic conditions, and health care disparities. The chartbook is based on more than 150 published studies and reports about quality of care. A 58-Year-Old Woman Dissatisfied with Her Care, Two Years Later (March 27, 2002). Anne-Marie Audet and Erin Hartman. Journal of the American Medical Association, vol. 287, no. 12. Copies are available from Anne-Marie Audet, M.D., The Commonwealth Fund, 1 East 75th Street, New York, NY 10021-2692, E-mail: [email protected]. #523 Diverse Communities, Common Concerns: Assessing Health Care Quality for Minority Americans (March 2002). Karen Scott Collins, Dora L. Hughes, Michelle M. Doty, Brett L. Ives, Jennifer N. Edwards, and Katie Tenney. This report, based on the Fund’s 2001 Health Care Quality Survey, reveals that on a wide range of health care quality measures—including effective patient–physician communication, overcoming cultural and linguistic barriers, and access to health care and insurance coverage—minority Americans do not fare as well as whites. Delivering Quality Care: Adolescents’ Discussion of Health Risks with Their Providers (March 2002). Jonathan D. Klein and Karen M. Wilson. Journal of Adolescent Health, vol. 30, no. 3. Copies are available from Jonathan D. Klein, Strong Children’s Research Center, Division of Adolescent Medicine, Department of Pediatrics, University of Rochester School of Medicine and Dentistry, 601 Elmwood Avenue, RM 4-6234, Rochester, NY, Tel: 585-275-7660, E-mail: [email protected]. #503 Accessing Physician Information on the Internet (January 2002). Elliot M. Stone, Jerilyn W. Heinold, Lydia M. Ewing, and Stephen C. Schoenbaum. In this field report, the authors analyzed 40 websites that offer information about physicians. Finding many instances where websites had incomplete, missing, and possibly inaccurate or outdated data, the authors conclude that health care accrediting organizations, health plans, hospitals, and local and national industry organizations and associations should make efforts to improve the information on the Internet, saying that it is a potential valuable tool for consumers. #528 The APHSA Medicaid HEDIS Database Project (December 2001). Lee Partridge, American Public Human Services Association. This study (available on the Fund’s website only) assesses how well managed care plans serve Medicaid beneficiaries, and finds that while these plans often provide good care to young children, their quality scores on most other measures lag behind plans serving the commercially insured. For-Profit and Not-for-Profit Health Plans Participating in Medicaid (May/June 2001). Bruce E. Landon and Arnold M. Epstein. Health Affairs, vol. 20, no. 3. Copies are available from Health Affairs, 7500 Old Georgetown Road, Suite 600, Bethesda, MD 20814-6133, Tel: 301-656-7401 ext. 200, Fax: 301-654-2845, www.healthaffairs.org. Improving Quality, Minimizing Error: Making It Happen (May/June 2001). Elise C. Becher and Mark R. Chassin. Health Affairs, vol. 20, no 3. Copies are available from Health Affairs, 7500 Old Georgetown Road, Suite 600, Bethesda, MD 20814-6133, Tel: 301-656-7401 ext. 200, Fax: 301-654-2845, www.healthaffairs.org. #456 A Statistical Analysis of the Impact of Nonprofit Hospital Conversions on Hospitals and Communities, 1985–1996 (May 2001). Jack Hadley, Bradford H. Gray, and Sara R. Collins. In this study, the authors analyze the effects of private, nonprofit hospital conversions that occurred between 1985 and 1993 by comparing converting hospitals to a control group of statistically similar private nonprofit hospitals that were estimated
32
to have a high probability of conversion, but did not convert over the observation period. The report is available online only at www.cmwf.org. #455 The For-Profit Conversion of Nonprofit Hospitals in the U.S. Health Care System: Eight Case Studies (May 2001). Sara R. Collins, Bradford H. Gray, and Jack Hadley. This report examines the 87 for-profit conversions of nonprofit hospitals in the years 1985–1994, more than one-third of which took place in three states, and nearly half of which were in the Southeast. The report is available online only at www.cmwf.org. Measuring Patients’ Expectations and Requests (May 1, 2001). Richard L. Kravitz. Annals of Internal Medicine, vol. 134, no. 9, part 2. Copies are available from Richard L. Kravitz, Center for Health Services Research in Primary Care, University of California, Davis, 4150 V Street, PSSB Suite 2500, Sacramento, CA 95817, E-mail: [email protected]. Current Issues in Mental Health Policy (Spring 2001). Colleen Barry. Harvard Health Policy Review, vol. 2, no. 1. Adapted from an issue brief prepared for the John F. Kennedy School of Government/Commonwealth Fund Bipartisan Congressional Health Policy Conference in January 2001. Available online at http://hcs.harvard.edu/~epihc/currentissue/spring2001/barry.html. Health Plan Characteristics and Consumers’ Assessments of Quality (March/April 2001). Bruce E. Landon et al. Health Affairs, vol. 20, no. 2. Copies are available from Health Affairs, 7500 Old Georgetown Road, Suite 600, Bethesda, MD 20814-6133, Tel: 301-656-7401 ext. 200, Fax: 301-654-2845, www.healthaffairs.org. #448 Child Development and Medicaid: Attitudes of Mothers with Young Children Enrolled in Medicaid (March 2001). Susan Kannel and Michael J. Perry, Lake Snell Perry & Associates. This report on mothers with young children enrolled in Medicaid finds that while generally pleased with the overall care their sons and daughters receive, many mothers feel that the program—as well as pediatricians—could do a better job of providing guidance on early development. Patient Safety and Medical Errors: A Road Map for State Action (March 2001). Jill Rosenthal and Trish Riley. Copies are available from the National Academy for State Health Policy, 50 Monument Square, Suite 502, Portland, ME 04101, Tel: 207-874-6524, Fax: 207-874-6527. Available online at www.nashp.org/GNL37.pdf. #446 The Quality of American Health Care: Can We Do Better? (January 2001). Karen Davis. In this essay— a reprint of the president’s message from the Fund’s 2000 Annual Report—the author looks at health care quality: how to define it, how to measure it, and how to improve it. Envisioning the National Health Care Quality Report (2001). Committee on the National Quality Report on Health Care Delivery, Institute of Medicine. Copies are available from the National Academy Press, 2101 Constitution Avenue, NW, Box 285, Washington, DC 20055, Tel: 800-624-6242, E-mail: www.nap.edu. #428 Getting Behind the Numbers: Understanding Patients’ Assessments of Managed Care (November 2000). Margaret Gerteis, Teresa Harrison, Cara V. James, Michael Manocchia, and Susan Edgman-Levitan, The Picker Institute. Using data from the Medicare Managed Care Consumer Assessment of Health Plans Survey, this report examines nine managed care plans and identifies plan-level practices that contribute to a positive experience for plan members. #427 Effective Clinical Practices in Managed Care: Findings from Ten Case Studies (November 2000). Suzanne Felt-Lisk and Lawrence C. Kleinman. Using HEDIS effectiveness-of-care indicators, this summary analysis of ten high-performing managed care plans shows that the plans’ ability to improve their performance is influenced by both their overarching approach to managed care and by the specifics of their quality improvement efforts.
33
#409 Perspectives on PPO Performance Measurement from Consumers, PPO Leaders, and Employers (September 2000). Liza Greenberg, American Accreditation Healthcare Commission/URAC. This report presents findings from meetings with key players in the preferred provider organization (PPO) quality arena, in an attempt to determine if PPOs are capable of reporting standardized health care quality data using nationally recognized measures. #380 Educating Medicaid Beneficiaries About Managed Care: Approaches in 13 Cities (May 2000). Sue A. Kaplan, Jessica Green, Chris Molnar, Abby Bernstein, and Susan Ghanbarpour. In this report, the authors document the approaches used and challenges faced in Medicaid managed care educational efforts in 13 cities across the country. The Public Release of Performance Data: What Do We Expect to Gain? A Review of the Evidence (April 12, 2000). Martin N. Marshall, Paul G. Shekelle, Sheila Leatherman, and Robert H. Brook. Journal of the American Medical Association, vol. 283, no. 14. Copies are available from Genuine Article/Institute for Scientific Information, 3501 Market Street, Philadelphia, PA 19104, Phone: 1-800-336-4474 option 5, Fax: 215-386-4343, E-mail: [email protected]. Public Release of Performance Data: A Progress Report from the Front (April 12, 2000). Arnold M. Epstein. Journal of the American Medical Association, vol. 283, no. 14. Copies are available from Genuine Article/ Institute for Scientific Information, 3501 Market Street, Philadelphia, PA 19104, Phone: 1-800-336-4474 option 5, Fax: 215-386-4343, E-mail: [email protected]. #366 National Medicaid HEDIS Database/Benchmark Project: Pilot-Year Experience and Benchmark Results (February 2000). Lee Partridge and Carrie Ingalls Szlyk, American Public Human Services Association. This report summarizes the first year of a project to create national summaries of state Medicaid HEDIS data and national Medicaid quality benchmarks against which each state can measure its program’s performance. To Err Is Human: Building a Safer Health System (2000). Linda T. Kohn, Janet M. Corrigan, and Molla S. Donaldson (eds.). This book, produced by the Institute of Medicine’s Committee on Quality of Health Care in America, concludes that medical errors are far more common, and deadly, than previously thought. Copies are available from the National Academy Press, 2101 Constitution Avenue, NW, Lockbox 285, Washington, DC 20055, Tel: 888-624-8373, Fax: 202-334-2451, E-mail: [email protected]. Regulating Managed Care: Theory, Practice, and Future Options (2000). Stuart H. Altman, Uwe E. Reinhardt, and David R. Shactman. Copies are available from Jossey-Bass, 350 Sansome Street, San Francisco, CA 94104, Phone: 415-433-1740, Fax: 415-433-0499, E-mail: [email protected], www.josseybass.com. #359 Quality Management Practices in Medicaid Managed Care (November 10, 1999). Bruce Landon and Arnold Epstein. Journal of the American Medical Association, vol. 282, no. 18. In their study of Medicaid plan quality, the authors discover that plans serving predominantly Medicaid beneficiaries were more likely than those with mainly commercial enrollments to provide services to patients that address their special needs, including those related to transportation, literacy, and nutrition. #342 Income Levels of Bad-Debt and Free-Care Patients in Massachusetts Hospitals (July/August 1999). Joel S. Weissman, Paul Dryfoos, and Katharine London. Health Affairs, vol. 18, no. 4. In this study, the authors find that most hospital patients whose expenses are written off to bad debt had incomes below the federal poverty level and thus were presumably eligible for either public programs or hospital-based free care. This disputes the common notion that these patients are able to pay their bills.


















