Experience of developing service user/survivor research Potential for this research agenda to impact...
37
Experience of developing service user/survivor research Potential for this research agenda to impact on mental health practice, service delivery models and policy Dr. Jan Wallcraft Dec 09
-
Upload
alaina-shepheard -
Category
Documents
-
view
213 -
download
0
Transcript of Experience of developing service user/survivor research Potential for this research agenda to impact...
Experience of developing service user/survivor research
Potential for this research agenda to impact on mental health practice, service delivery models and policy
Dr. Jan Wallcraft Dec 09
Involvement in mental health research based on liberation struggles
Liberation movements of various social groups in 1970s
Disability movement ‘nothing about us without us’
Aspirations of mental health service users for full citizenship and rights including
Where do survivor researchers come from?
• Service user activists who turned to research to make a difference and developed research skills
• Academics and researchers with lived experience of mental health services: using their skills in researching mental health
Voluntary efforts of small groupsService users began to carry out their own
research, sometimes supported by NGOsSometimes using conventional social
survey methods but with service users designing, asking the questions and analysing the results
Sometimes seeking forms of research based on liberation struggles– emancipatory, standpoint, action research, participatory methods
Personal perspectives, narrative methods
Survivor led researchEXPLAINS AND CELEBRATES THE ACHIEVEMENTS OF THE PAST 20 YEARS OF SURVIVORS DOING RESEARCH
(1978)
Leonard Roy Frank was treated with blitz ECT in the 1970s – large areas of his memory was erased.
He researched the history of shock treatment as a means of coming to terms with the damage he had suffered.
He compiled this book to give information (both pro and anti ECT) to others so they could make their own choices.
The History of Shock Treatment (1978)
Recent study of ECT by a survivor of the treatment – Linda Andre (2009)
Linda Andre was similarly motivated –
she was a talented photographer when
she was admitted to hospital and given
ECT. Her skills and knowledge
obliterated, she embarked on many
years of research and campaigning to
try to get ECT banned.
A psychiatrist, Stefan Kruszewski, who
formerly gave ECT, reviewed this book:
‘’ A brilliant analysis....the book made
me feel ignorant of ECT’s past and
deceived by having virtually none of the
information presented in Andre’s book
brought to my attention previously....’
The Well Being ProjectDr. Jean Campbell, a service user researcher
was principal investigator of the Well-Being Project, which ran from 1986–1989.
This influential survey programme, based in California, identified the factors that helped and hindered well-being of those labelled mentally ill.
The interviewers were all service users, trained as part of the programme, and carried out over 500 face to face interviews
producing a report (Campbell and Schraiber, 1989) a video documentary, a compendium of statistics, oral history, art and writings.
My first user-led research project for a government-funded disability project
Mental Health Foundation: user led research on alternatives
Healing Minds (1998) This report brings
together evidence for a range of complementary and alternative therapies in mental health, including acupuncture, homeopathy, nutritional remedies, aromatherapy, massage and spiritual healing
Coping with coming off - user-led research – Jim Read for MIND
CWCO research: Success rates for different drugs Nearly three quarters of those coming off
mood stabilisers succeeded in coming off. The success rate was lower for those on
SSRIs or anti-psychotics – just over half of these succeeded in coming off.
However, people on mood stabilisers were much more likely than those on SSRIs to be discouraged by doctors from attempting to come off
Difficulties with coming off drugs The longer people had been on the drugs, the
more likely they were to have difficulties when coming off: Only one quarter (25%) of those who had been on
less than 6 months had problems Four in five(80%) of those who had been on six
years or more had problems
CWCO - Staying off drugs Nearly half those interviewed (91 out of
204) were no longer taking any psychiatric drugs.
Of this group, nearly a quarter had been off drugs for 10 years or more.
This group included people who have taken all forms of psychiatric drugs except for those introduced recently
CWCO - People who help in coming off Those trying to come off generally found
that people with no involvement in prescribing drugs the most helpful. These include voluntary orgs, helplines,
complementary therapists, support groups, counsellors, and other service users.
Mental health workers, GPs and Psychiatrists were seen as least helpful.
Sainsbury Centre: user-led research on the service user movement
Agenda for mental health policy emerging from survivor work
RecoverySelf managementStrategies for livingWellness action planningService user-leadership and user involvement in mainstream research
Choice in medical treatments e.g. drugs
Service user involvement in mainstream research
The history of service user
involvement in mainstream
research is one of struggle
with the dominant ideology of
empirical science and
rational/logical positivism,
which rules us out as ‘non-
rational’ individuals
Involvement On Whose Terms? ‘Collaboration usually starts by academics
inviting user researchers to contribute to their projects and not the other way around. The way someone joins the project – on whose initiative and for what reasons – defines their role, at least at the beginning. [Service ] users are invited at various stages of someone else’s project. They are rarely invited to plan and seek funding for the research and to define the roles and responsibilities.’
(Russo and Statsny, in ‘Wallcraft et al 2009)
Allies and supporters of involvement in research However - service user/survivor
involvement in clinical research would not be possible without the work of committed people in government:
‘Involve’ : set up in 1996 by the Director of Research and Development in the NHS ‘Consumers are the ultimate recipients and
beneficiaries of the knowledge derived from research and development. It is therefore not only desirable, but essential that they be involved in developing and implementing strategies for R&D in the NHS.’
Evidence Based Medicine- or Evidence-based Mafia?
EBM in mental health is based on assumptions about madness that cannot be questioned or examined (from 19th century and earlier)
‘The currently used outcome measures are based on maintenance- symptom reduction and medication compliance. When 'community integration' is used as the outcome measure, the recovery model is more evidence based than the medical model ‘( p.114 Wallcraft et al 2009)
Many common practices are not evidence-based – e.g. Hospitalisation
Many drug trials fail to show any advantage over placebo
How pharma industry manages evidence in US and UK Ghost writing articles paying eminent researchers
to put their names to them Advertising (in USA direct to the public) Targeting pharmacists and doctors Supporting free journals to publish and
disseminate their results Suppressing negative results and drop-out/deaths Universities receive money in admin costs for
drug trials, speakers fees and consultation costs Influencing guidelines and evidence hierarchies
SPN -Questions that should be asked when starting research Who has been
involved in deciding what needs to be researched?
Who has relevant knowledge and expertise that may be used to guide the research?
Who is going to be participating +how do they give informed consent?
Who is it hoped will benefit from the research and in what way?
How will research findings be used and who will have access to them?
Do all stakeholders in the research process have equal power and influence?
New research concepts – or strengthening of existing onesDifferent ethical position.Challenge to positivist biomedical research
based on identifying and curing ‘diseases’Challenge to diagnostic system as an
explanation and predictive systemChallenge to neutral, objective researchers
measuring changes in passive subjects – e.g. RCT methods
Greater importance of empowering methodology, service users as conceptualisers of the research question, qualitative methods, narrative enquiry.
Involvement does change things Example 1 : ECT
SURE’s work on ECT – a systematic review of what patients say about ECT – this had never been done before: Included firsthand accounts of ECT. Found that very few studies follow up patients
even as long as 6 months Memory loss was found to be a persistent side
effect, profoundly affecting people’s lives No long-lasting benefit of ECT was found in
patients’ testimony
Eliciting users’ views of ECT (Philpot et al 2004)
‘Doctors who give ECT have shown remarkably little interest in their patients’ views of the procedure and its effects on them’ (Abrams 1997)
This study used a questionnaire designed by a mental health service user group, before and after patients received ECT.
45% reported persistent memory loss 47% felt they had been compelled through
pressure to have it despite only one actually being under section
First ever prospective study of ECT with an ECT user-designed questionnaire.
NICE’s Response re ECT
NICE had asked for this research, and had to act on it: ‘The Committee considered that the evidence
appraised supported the effectiveness of ECT in certain groups of individuals. However, the Committee recognised there remained a number of uncertainties, including a lack of information on longer-term outcomes. The Committee was aware of the negative experiences of some individuals who have undergone ECT. Therefore the Committee considered that that ECT should be used with caution and only in the restricted circumstances recommended in the guidance’
Example 2 – Personality Disorder – (Colchester) Colchester Research:
A group of service users diagnosed with PD met with an advocate, Heather Castillo in Colchester Mind in 1999 and developed a research project on service user perspectives of PD.
They were given support and funding from a local University and training by Mind.
They carried out a service user-led study of 50 people’s experiences of PD, diagnosis and treatment.
Example 2 – Personality Disorder (St. George’s, London) St. George’s Trust PD research
Service user researchers involved in developing proposal and drawing up of original interview schedule
Service user researcher and doctor undertook all interviews jointly
Reflective diaries kept by all members of research team throughout project to explore the impact of service user involvement and collaborative research
First part of interview invites people to describe what ‘recovery’ means to them in the context of their experiences of PD
Second part of interview asks them to reflect on the relevance of other accounts of mental health recovery to them
Combination of narrative analysis (keeping individual recovery stories intact) and content analysis (comparing understandings of recovery and PD with other understandings of mental health recovery
Service user involvement in National PD programme Strategy for PD was sought by Department of
Health in London in 2001 Acknowledgement that service user voices
should be included Parallel reference group of service users set
up in 2002 Pilot PD services set up in 2004 and evaluated
with service user involvement in the evaluation process
NICE guidance on BPD NICE guidance was published in January 2009 Service users and carers were involved as
stakeholders in the process of creating this There is a sizeable section on service users’
experiences of BPD and services Guidance reflects principles emerging from
service users’ work, e.g. Importance of autonomy and choice trusting relationships the role of abuse and trauma and encountered stigma the role of psychological treatments and drug
treatments
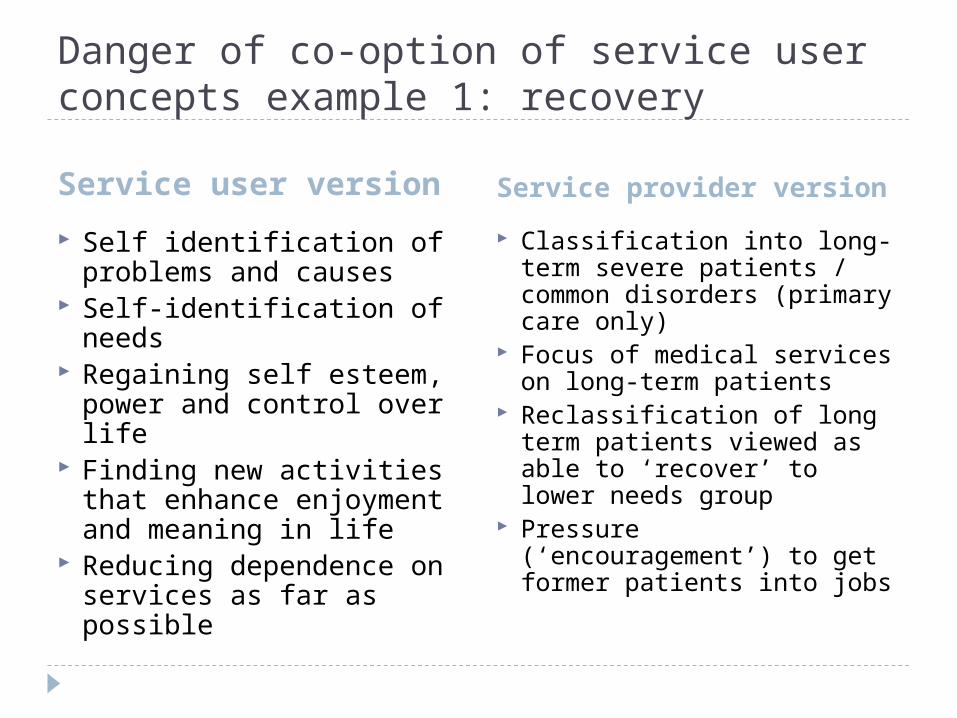
Danger of co-option of service user concepts example 1: recovery
Service user version Service provider version
Self identification of problems and causes
Self-identification of needs
Regaining self esteem, power and control over life
Finding new activities that enhance enjoyment and meaning in life
Reducing dependence on services as far as possible
Classification into long-term severe patients / common disorders (primary care only)
Focus of medical services on long-term patients
Reclassification of long term patients viewed as able to ‘recover’ to lower needs group
Pressure (‘encouragement’) to get former patients into jobs
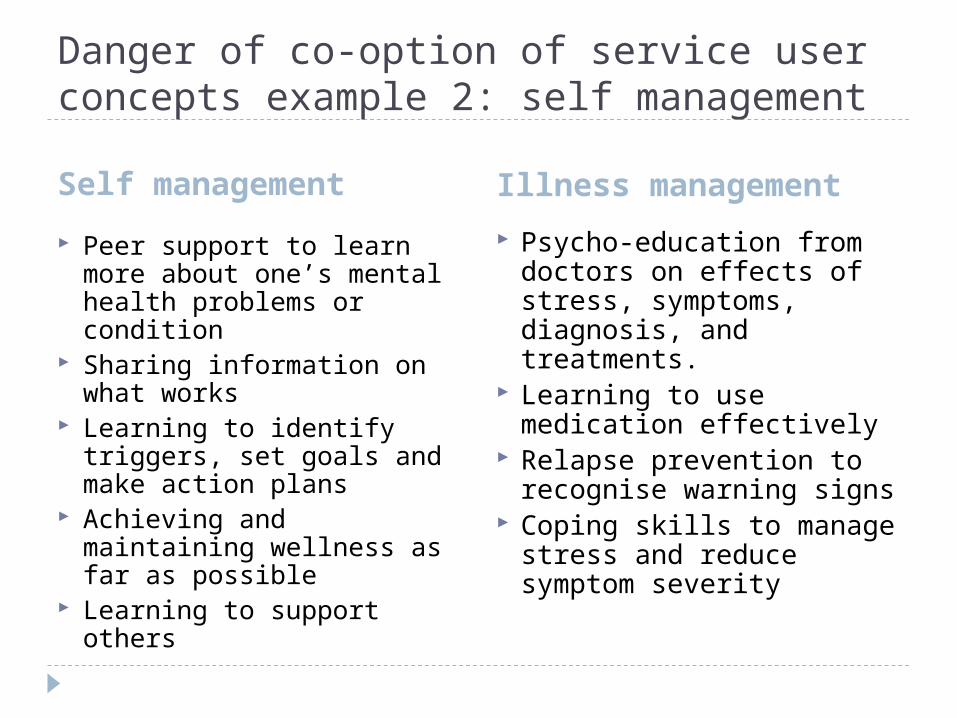
Danger of co-option of service user concepts example 2: self management
Self management Illness management
Peer support to learn more about one’s mental health problems or condition
Sharing information on what works
Learning to identify triggers, set goals and make action plans
Achieving and maintaining wellness as far as possible
Learning to support others
Psycho-education from doctors on effects of stress, symptoms, diagnosis, and treatments.
Learning to use medication effectively
Relapse prevention to recognise warning signs
Coping skills to manage stress and reduce symptom severity
Potential influence on service delivery models Recovery and wellness orientation
Collaborative services using concepts of wellness, recovery, self management, choice and strengths
Better acceptance of services, more positive outcomes New ways to evaluate services, in co-operation with
service user groups, using different outcome measures e.g. Recovery Enhancing Environment Measure, Recovery Assessment Schedule, Herth Hope Index, Empowerment Scales, or Goal Attainment Scaling
Greater involvement of families and friends to enhance community support and understanding of mental health issues
Ultimately, changes to legislation to give greater rights to quality services and eliminate discriminatory practices
Conclusions
What we don’t need What we DO need
Tokenism Co-option Hi-jacking service user
concepts to make policies look more acceptable
Domination of research agenda by pharma industry
More evidence that ignores service users preferences and views
New outcome measures that measure valued outcomes for service users
All mental health research on services to have service user input at all stages
More use of narrative methods
Implementation of research with service user input
Service users trained and supported to do research themselves
References Andre, L. (2009). Doctors of Deception: What They Don't Want You to Know about Shock Treatment, Rutgers Univ Pr. Beresford, P. and J. Wallcraft (1997). "Psychiatric system survivors and emancipatory research: issues, overlaps and
differences." Doing disability research: 67-87.• Bullock, W. A., M. O'Rourke, et al. (2006). "Effectiveness of the illness management and recovery program in promoting
recovery: Preliminary results." New Research in Mental Health Campbell, J. and R. Schraiber (1989). "The Well-Being Project: Mental health clients speak for themselves." San Dworkin,
R.J. (1992) Researching Persons With Mental Illness, London: Sage Publications Francisco, CA: California Department of Mental Health. Faulkner, A. and S. Layzell (2000). "Strategies for living: A report of user-led research into people’s strategies for living
with mental distress." Mental Health Foundation, London. Frank, L. (1978). The history of shock treatment, Leonard Roy Frank. Hanley, B. (1999) Involvement Works: The second report of the Standing Group on Consumers in NHS Research, London:
NHS Executive. Available online at: http://www.invo.org.uk/pdfs/involvement_works.pdf, accessed 25/10/08. Lewis, G., Anderson, L., Araya, R., Elgie, R., Harrison, G., Proudfoot, J., Schmidt, U., Sharp, D., Weightman, A. and Williams,
C. 2003. Self-help interventions for mental health problems. Report to the Department of Health R&D Programme O'Hagan, M. (1993). Stopovers on my way home from Mars, Survivors Speak Out. Philpot, M., C. Collins, et al. (2004). "Eliciting users' views of ECT in two mental health trusts with a user-designed
questionnaire." Journal of Mental Health 13(4): 403-413. Read, J. (2009). Psychiatric Drugs: Key Issues and Service User Perspectives, Palgrave Macmillan. Rose, D., P. Fleischmann, et al. (2003). "Patients' perspectives on electroconvulsive therapy: systematic review." British
Medical Journal 326(7403): 1363. Stastny, P., P. Lehmann, et al. (2007). Alternatives beyond psychiatry, Peter Lehmann Publishing. Sweeney, A., P. Beresford, et al., Eds. (2009). This is Survivor Research, PCCS Books. Tew, J., N. Gould, et al. (2006). "Values and methodologies for social research in mental health." London, SPN/SCIE. Wallcraft, J. (1998). "Healing minds." London: Mental Health Foundation. Wallcraft, J., M. Amering, et al. (2009). Handbook of Service User Involvement in Mental Health Research, Wiley-Blackwell. Wallcraft, J., J. Read, et al. (2003). On Our Own Terms: Users and survivors of mental health services working together for
support and change, Sainsbury Centre.