Documentation for Acute Care Chapter 3 Content of the Acute Care Health Record.

In October 1998, the definition of a trans-fer in Medicare’s hospital prospective pay-ment system was expanded to include sever-al post-acute care (PAC) providers in 10high-volume PAC diagnosis-related groups(DRGs). In this methodological article, theauthors respond to a congressional mandateto consider more DRGs in the definition.Empirical results support expansion tomany more DRGs that are split in ways thatunderstate total PAC volumes, including 25DRG pairs (with/without complications)and DRG bundles (e.g., infections) thattogether exhibit high PAC volumes. By con-trast, some DRGs (e.g., craniotomy) arequestionable PAC candidates because oftheir heterogeneous procedure mix.
INTRODUCTION
Prior to the enactment of the BalancedBudget Act (BBA) of 1997, the only casesdesignated as transfers under Medicare’sinpatient hospital prospective payment sys-tem (PPS) were those discharged from oneacute care facility and readmitted to a sim-ilar facility on the same day. Under the cur-rent acute-to-acute transfer payment policy,the sending hospital is paid twice the DRGper diem amount for the first day and theper diem for all remaining days up to thefull DRG payment amount. The final dis-charging hospital still receives the fullDRG payment amount (Prospective
Payment Assessment Commission, 1993).The transfer payment policy was based onthe belief that it was inappropriate to paythe sending hospital the full DRG paymentfor less than the full course of treatment(Buczko, 1993).
Growth in PAC
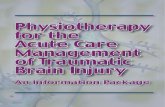
Fundamental changes in the health caremarket over the past decade have causedhealth policy analysts to rethink the tradi-tional distinction between acute and PACservices (Lee, Ellis, and Merrill, 1996). Anincrease in the number of PAC providers,as well as technological advances in medi-cine, have enabled these providers to treata wider range and severity of conditions,thereby permitting patients to be dis-charged earlier from acute care hospitals(Schneider, Cromwell, and McGuire, 1993;Medicare Payment Advisory Commission,1998; Federal Register, 1998b). Figure 1tracks the share of Medicare patients dis-charged from an acute care hospital to aPAC provider, defined as a skilled nursingfacility (SNF), home health agency, or facil-ity exempted from PPS reimbursement.PAC transfer rates rose steadily during the1990s, from 20.5 percent in 1991 to 30.2percent in 1998 (Gilman et al., 2000). A 10-percentage point increase translates into 1million more Medicare patients annuallyreceiving PAC services after discharge.The percent increase in the 20 DRGs withthe highest PAC rates in 1991 was evengreater, i.e., 38 to 54 percent (Gilman et al.,2000).
HEALTH CARE FINANCING REVIEW/Winter 2002/Volume 24, Number 2 95
The authors are with RTI International. The research for thisarticle was funded under HCFA Contract Number 500-95-0006.The views expressed in this article are those of the authors anddo not necessarily reflect the views of RTI International or theCenters for Medicare & Medicaid Services (CMS).
Expansion of Medicare’s Definition of Post-Acute CareTransfers
Jerry Cromwell, Ph.D., Suzanne Donoghue, and Boyd H. Gilman, Ph.D.

Reimbursing acute care hospitals forshort-stay patients transferred to PAC canbe justified on the same grounds as acute-to-acute transfers. When PPS standardizedamounts were first constructed in 1983,they were based on much longer stays andfar lower PAC rates. Costs for servicesthat were originally being incurred by hos-pitals are now being incurred by PACproviders that bill Medicare for their ser-vices. The program often pays twice forthe PAC-level care previously provided onan inpatient basis.
Because annual recalibration of DRG rel-ative weights supposedly captures shifts insite of care through lower inpatient charges,any transfer payment policy focused onPAC may seem redundant. Annual recali-bration, however, does not automaticallyreduce payments for either acute-to-acuteor PAC-related transfers. Greater reliance
today on PAC is found in practically allDRGs, but any diffused PAC effect is fac-tored out of payment updates by normaliza-tion of the annual DRG relative charges percase. More significantly, PAC transfersunder current policy are weighted by theratio of their acute lengths of stay (LOS) tothe DRG geometric mean stay before beingincluded in the denominator of CMS’s cal-culation of the charges per discharge. Theeffect is to raise average charges for PACdischarges in order to ensure that non-transfer discharges receive an actuariallyfair DRG full payment.
Description of PAC Transfer Policy
In 1997, Congress responded to the bur-geoning PAC utilization and possible dou-ble payment by directing HCFA to identify10 DRGs to test the feasibility of extending
96 HEALTH CARE FINANCING REVIEW/Winter 2002/Volume 24, Number 2
0
Year
Per
cen
t
35All ProvidersSkilled Nursing FacilityHome Health AgencyProspective Payment System-Exempt Facility
1991 1991 1991 1991 1991 1991 1991 1991
25
10
15
5
30
20
SOURCE: Health Care Financing Administration: Medicare Provider Analysis and Review Claims Files; databased discharge destination code, 1991-1998.
Figure 1
Share of Medicare Post-Acute Care Transfers, by Provider Type: 1991-1998

the PPS acute care transfer payment policyto include transfers to PAC settings. BBA1997, section 1886(d)(5)(J) required theSecretary of the Department of Health andHuman Services to select 10 DRGs“…based upon a high volume of dis-charges classified within such group and adisproportionate use of…” certain post-dis-charge services (Federal Register, 1998b).The act then defined a qualified post-acutedischarge as one where the patient wastransferred to a non-PPS hospital or SNFwithin 1 day or received home health ser-vices for care related to the acute admis-sion within 3 days of discharge.
HCFA staff put into operation the con-gressional mandate in two steps. First, allDRGs in 1996 were ranked in terms of thetotal number of Medicare PAC dischargesand the top 20 DRGs were identified.Second, staff “…considered the volumeand percentage of discharges to post-acutecare that occurred before the mean lengthof stay and whether the discharges occur-ring early in the stay were more likely toreceive post-acute care…” (FederalRegister, 1998b). Staff then selected thetop nine DRGs with more than 14,000 PACdischarges, plus a tenth, uncomplicated,low-volume DRG related to its longer com-plicated companion DRG. All 10 had veryhigh rates of short-stay PAC discharges.
Current Medicare policy for 7 of the 10PAC DRGs pays double per diems to thehospital on the first day of inpatient hospi-talization and single per diems on eachsubsequent day until full DRG reimburse-ment is reached. The DRG-specific perdiem is calculated using the hospital pay-ment rate and the national geometric meanLOS. For three DRGs (209, 210, 211)where this payment methodology failed tocover their average costs, CMS pays hospi-tals one-half the full DRG amount plus a fullper diem on the first day, and one-half theper diem for each additional day up to the
full DRG amount. Although the transferpolicy applies to all PAC transfer cases inthe 10 DRGs, hospitals effectively are paidon a per diem basis only for patients dis-charged to PAC at least 1 day short of thenational geometric mean LOS (refer toTechnical Note).
The payment policy change went intoeffect on October 1, 1998, and applies onlyto inpatient acute facilities. Initial simula-tions of program savings in the 10 DRGsfrom per diem payments were $276 millionover the first half of FY 1999 (Gilman et al.,2000). This estimate is considerably high-er than that of the Medicare PaymentAdvisory Commission’s (MedPAC) (2000),primarily because commission staff did nottake into consideration the lagged declinein the geometric mean LOS that narrowedthe count of short-stay patients. Ex antesavings for an unchanged geometric meanLOS are considerably larger. Responses ofacute and PAC providers to the paymentchange were minimal over the first 6months after the policy was implemented(Gilman et al., 2000). PAC providers havealso experienced dramatic changes in theirMedicare payment systems in the lastdecade. Whether these changes will haveany feedback effect on hospital PAC trans-fers is beyond the scope of this article.
Organization of this Study
This methodological article addressesthe question raised by Congress in theBBA of whether the PAC transfer policyshould be extended to more, or even to all,DRGs. By including more DRGs in the pol-icy, the government could recover part ofthe financial gains hospitals have enjoyedby discharging patients early and shiftingservices to post-acute providers. We beginthe analysis with a methodological discus-sion of the criteria used to identify candi-date DRGs. We also raise serious questions
HEALTH CARE FINANCING REVIEW/Winter 2002/Volume 24, Number 2 97

about the wisdom of using individual DRGsas the unit of analysis, noting problemsarising from DRG fractionation and hetero-geneity. Next, we describe our Medicareclaims database. Empirical results firstcompare the PAC rates of the current 10transfer DRGs adopted by HCFA with 13additional DRGs identified by HCFA andMedPAC for future consideration. Twosubsequent empirical sections address theproblem of using aggregate DRG counts ofPAC discharges as the initial selection cri-terion by studying all DRG complicationpairs and bundles of treatment-relatedDRGs. A final empirical section examinesthe pitfalls in extending the PAC transferpolicy to heterogeneous procedure DRGswith bimodal LOS distributions. A con-cluding discussion section summarizes theresults as well as presenting administrativearguments for and against expanding thePAC transfer policy to more DRGs.
METHODOLOGY
Issues
Our approach to identifying candidateDRGs for expansion of the PAC transfer pol-icy under acute inpatient prospective pay-ment is presented in two parts. First, weexpand the set of criteria used by HCFAstaff in selecting the first 10 DRGs. Next,we critique the focus on individual DRGsand how it results in false-negative and false-positive selection errors, either becauseDRGs are too fractionated or are too het-erogeneous by themselves for targetedimplementation of the new transfer policy.
Selection Criteria
As a first step in identifying DRGs forexpansion, we reconsidered HCFA’s two-step approach of selecting DRGs withunusually high short-stay PAC rates within
the set of high PAC DRGs. HCFA strategytargeted DRGs with large numbers ofpatients discharged to PAC earlier thanexpected, given their higher severity andthe need for followup PAC. Highly skewedLOS distributions, however, could natural-ly generate many short-stay PAC (SPAC)discharges without any serious site-of-caresubstitution problem. Hence, we constructa companion ratio to the SPAC dischargerate, SPAC/SLOS, that standardizes for thetotal number of short LOS (SLOS) dis-charges. This indicator highlights DRGswith unusually high numbers of PAC trans-fers among just short-stay discharges.
Of course, some DRGs have high PACdischarge rates because of the natureand/or severity of the illness and inpatientprocedures performed, e.g., major jointsurgery. The PAC rate among all long LOS(LLOS) patients, LPAC/LLOS, should be agood proxy for the general severity level ina DRG as long-stay patients discharged toPAC are likely quite ill. The relative odds(RELODD) of short- versus long-stay PACpatients is a quick way of controlling foroverall high severity levels within DRGs, i.e.,RELODD = (SPAC/SLOS)/(LPAC/LLOS).We would expect PAC transfers to be farless frequent for shorter- versus longer-stay patients because short-stay patientsshould be healthier upon discharge(unless their acute stays have been trun-cated). Consequently, DRGs with particu-larly high odds ratios, we argue, haveunusually high short-stay PAC rates thatmerit attention.
Consider as well the dynamic implica-tions of PAC growth. Within DRGs overtime, inpatients are sicker on average, yetstay fewer days in the acute facility, and usePAC more often. This is strong circum-stantial evidence of a feedback effect ofPAC referrals shortening inpatient LOS.DRGs exhibiting significant increases inthe PAC discharge rate, coupled with
98 HEALTH CARE FINANCING REVIEW/Winter 2002/Volume 24, Number 2

declining average LOS, are likely undergo-ing extraordinary rates of site substitutionof care (Medicare Payment Advisory Commission, 1998). We analyzed thegrowth in PAC use from 1994 to 1996 anddisplayed DRGs with particularly highoverall PAC discharge rates of change,e.g., coronary bypasses.
Rapid increases in short-stay PAC dis-charges may be even more indicative ofhigh rates of site substitution, whileincreases in the relative odds of short- ver-sus long-stay PAC rates may be the singlebest indicator of site shifts in care, as it con-trols for PAC growth among long-staypatients.
Even with these more refined indicators,it should be clear that no single measurecompletely captures site-of-care substitu-tion. Moreover, because the criteria arecontinuous, no unique cutoff thresholdexists to single out ideal candidates. Thebest we can do is to array DRGs by the setof indicators and highlight those most like-ly to be experiencing unusually high site-of-care substitution.
Fractionated and HeterogeneousDRGs
To initiate the PAC transfer policy,Congress focused on 10 high-volumeDRGs, allowing HCFA time to identify othercandidates using alternative selection crite-ria. Emphasizing only total PAC volumesand rates, however, does not take into con-sideration the fact that many DRGs are frac-tionated. To avoid ignoring excellent butsmall-volume candidates (false negatives), itis necessary to go beyond single DRGs andput together DRGs with a common clinicalfactor that determines PAC needs.
DRGs are fractionated in several ways.Many appear in pairs stratified by compli-cations and age. HCFA staff did includeboth DRGs 263 and 264, skin graft for skin
ulcer with and without complications, outof concern for biasing hospital coding ofcases to maximize payments (refer toTechnical Note.) Extending their analysis,we identified and constructed PAC ratesfor the top 25 complication pairs based ontheir combined PAC volume. We thenexamined their suitability for the transferpolicy using the expanded set of criteria.
Other stratifiers that distinguish DRGsin potentially misleading ways include thepresence of trauma, length of coma, infec-tions, angioplasty, heart attack, complexdiagnosis or procedure, use of laparo-scope, malignancy, major or minor proce-dure, type of skin graft and location of frac-ture, e.g., thumb versus other hand orwrist procedures. As we show later, it isoften one of these qualifying characteris-tics of the DRG that determines the PACrate. To avoid overlooking DRGs becausethey exhibit low PAC volumes by them-selves yet have an underlying PAC-inten-sive characteristic in common, we firstranked all DRGs by their short-stay PACrates. Next, we searched the top 100 DRGsfor recurring characteristics (e.g., infec-tions, fractures) that likely require greaterPAC care. Finally, we assembled super-DRG bundles of clinically related DRGs,constructed overall PAC rates for eachbundle, and then compared them withHCFA’s 10 original DRGs. In effect, frac-tures, infections, etc., become the units ofanalysis for comparison purposes.
In identifying short-stay PAC patientsappropriate for per diem payment, DRGsnot only may be too narrow a unit of analy-sis due to fractionated DRGs, they can alsobe too broad in harboring heterogeneouspatients and/or procedures. The PACtransfer policy implicitly treats a PAC des-tination code as a potential indicator of atruncated stay. It assumes that any short-stay patient actually discharged to PAC issicker (upon discharge) than other short-
HEALTH CARE FINANCING REVIEW/Winter 2002/Volume 24, Number 2 99

stay patients not requiring PAC. Therefore,any short-stay PAC patient may constitutea premature discharge. Yet, if patients inthe same DRG are undergoing very differ-ent procedures requiring very differentLOS, the sensitivity and specificity of thePAC indicator can be low. It can be insen-sitive in not identifying early PAC dis-charges of patients undergoing the morecomplicated, longer stay procedures (falsenegatives). It can also be unspecific in call-ing for per diem payment for longer-staypatients undergoing a simpler, shorter-stayprocedure (false positives). If LOS distri-bution in a DRG is bimodal, with clusters ofcases with very short and long LOS, theunderlying assumption of patient homo-geneity is untenable. Short of regroupingpatients into new DRGs that better reflectPAC needs, we first considered a fewDRGs with a broad mix of more or lesscomplex procedures. We illustrate theproblem of heterogeneous procedureDRGs using DRG1: Craniotomies.
Data Sources
We used HCFA’s Medicare ProviderAnalysis and Review (MedPAR) data filesexclusively for our analyses. MedPAR pro-vides records for 100 percent of Medicarebeneficiaries using inpatient services, aswell as DRG-specific information. Therewere roughly 12 million inpatient recordsin each of 2 years, 1992 and 1998. We identi-fied all cases discharged to a PAC providerusing hospital discharge destination codesthree (SNFs), five (PPS-exempt units), andsix (home health agencies). We did notverify PAC transfers using PAC claims. Aseparate validation of inpatient PAC trans-fer discharge destination codes for 1997-1998 using Medicare PAC claims con-firmed the accuracy of SNF codes (Gilmanet al., 2000). The home health destinationcodes underreported cases by 15 percent
versus 11 percent overreporting of PPS-exempt facility discharges. The overall dis-crepancy (only 1 percent) in coded versusactual PAC transfers is likely due to thenarrow time windows used in the currentPAC policy. Hospital discharge plannerswhen coding discharge destination did notconsider specific time lags to PAC care inmost of 1998 prior to the new policy. Allinpatient deaths and acute hospital trans-fers were excluded (discharge destinationcode = 20 or 2). Only PPS discharges wereincluded; distinct-part unit psychiatric andsubstance abuse patients were excluded.After calculating the geometric mean LOSfor each DRG based on included claims, wewere able to categorize PAC transfers aseither short- or long-stay cases. Short-staypatients were defined as those with LOS <=geometric mean LOS minus 1 day becausepatients with a longer LOS would be paidthe full DRG amount.
RESULTS OF THREE COMPARISONGROUPS
This section includes an evaluation ofpotential DRG candidates for the transferpayment policy. In considering HCFA’sand MedPAC’s initial expansion list, wefirst compared 13 additional DRGs (plusDRG 109) using our expanded criteriawith HCFA’s original 10 DRGs. The nexttwo groupings put DRGs together eitherwith versus without complications or by acommon clinical indicator (e.g., infections).DRGs can be candidates in all three group-ings.
Original 10 DRGs Versus Next 13PAC DRGs
In addition to the 10 DRGs that HCFAstaff selected to implement the PAC trans-fer policy under inpatient prospective pay-ment, 10 additional DRGs were considered
100 HEALTH CARE FINANCING REVIEW/Winter 2002/Volume 24, Number 2

by HCFA based on total PAC volume andshare of discharges. They were ultimate-ly rejected because they had lower rates ofshort-stay PAC discharges. MedPAC staff,in comments on the new transfer rule, sug-gested six more DRGs, three of whichoverlapped with HCFA’s expanded list, i.e.,the bypass DRGs, along with three addi-tional DRGs involving simple pneumonia.(In the 1999 DRG Grouper, heart bypasseswere split into three DRGs (106, 107, and109) from the original two (106 and 107).Care must be taken in analyzing trendsbecause 106, bypass with cardiac catheter-ization, was split and non-angioplasty casesput into 107. DRG 107 cases are now in109.) Table 1 reports results using ourPAC selection criteria for the 10 DRGs cur-rently included in the PAC-transfer pay-ment system plus the additional 13 consid-ered by HCFA and MedPAC.
The current 10 DRGs appear to be excel-lent choices based on our expanded set ofselection criteria. Most have fairly highshort-stay PAC rates (except possibly forstrokes, DRG 14, and mental retardation,DRG 429). They also have quite high rela-tive odds ratios. Ratios near 1.0 suggestthat the frequency of PAC cases is just aslikely to be found in short- as in long-staycases. Strokes (DRG14) had the lowestodds ratio, 0.67, which is still quite high,compared with all DRGs as a group (mean= 0.42). Despite all 10 DRGs alreadyexhibiting high odds ratios in 1992, 8 of 10saw their relative odds increase over thenext 6 years. With declining geometricmean LOS over time, DRG relative oddsshould fall, not increase, ceteris paribus, asmore cases should equal or exceed thegeometric mean LOS. Rising odds ratiossuggest a strong trend toward prematuredischarge of PAC patients.
The second group of 13 DRGs alsoexhibits high PAC volumes (with theexception of DRG 109, which is an artifact
of the shift of some bypass patients from107 to 109). Their PAC rates are generallylower than the top 10, however, althoughstill quite substantial in most instances,compared with other DRGs. Ten of the 13DRGs had short-stay PAC rates at least 50percent above the all-DRG average, and allbut 2 had above-average relative oddsrates. DRG 243, medical back problems,exhibited the lowest relative odds, at 0.356because of a low PAC occurrence amongshort-stay patients (4.1 percent). One rea-son for the low short-stay PAC rate is theshort overall geometric LOS of this DRG of4.7 days (excluding deaths and transfers toother acute hospitals). We return to theproblems created by PAC-induced reduc-tions in geometric mean LOS in the con-cluding section.
Top 25 DRG Complication Pairs
In selecting the top 10 DRGs for initialimplementation of the inpatient PAC trans-fer policy, HCFA staff decided to includeDRG 264, skin graft/debridement withoutcomplications, as a pair with DRG 263, skingraft/debridement with complications.HCFA argued that if DRG 264 were exclud-ed, an incentive would be created for hos-pitals not to code complications so as toreceive full DRG 264 payment.
More than 125 DRG complication pairsexist in the classification system based onage, cardiac catheterization, and complica-tions alone. To examine the effect onselection of splitting DRGs by presence orabsence of complications, we first rankedindividual DRGs appearing in pairs fromhigh to low, based on their own SPAC dis-charge rate. Once all DRGs were ranked,the top 25 DRGs were chosen for illustra-tive purposes, along with their companionDRGs. The results are presented in Table2. Pairs have been re-ranked by their com-bined PAC volume.
HEALTH CARE FINANCING REVIEW/Winter 2002/Volume 24, Number 2 101

102 HEALTH CARE FINANCING REVIEW/Winter 2002/Volume 24, Number 2
Tab
le 1
Po
st-A
cute
Car
e F
req
uen
cy b
y S
ho
rt-V
ersu
s L
on
g-S
tay
Acu
te In
pat
ien
ts,b
y D
iag
no
sis-
Rel
ated
Gro
up
s:19
98
Sho
rt-S
tay
PAC
Tra
nsfe
rs2
All
PAC
Tra
nsfe
rs1
Sha
re o
fS
hare
of
Sha
re o
f Tot
alS
hort
-Sta
yR
elat
ive
Odd
s R
atio
3
DR
GV
olum
eTo
tal D
isch
arge
Dis
char
ges
Dis
char
ges
1998
1992
-199
8
(1)
(2)
(3)
(4)
Per
cent
Cha
nge
Per
cent
HC
FA’s
Ori
gin
al 1
011
4C
ereb
rova
scul
ar D
isor
ders
175,
457
60
.213
.645
.10.
676
6
113
Am
p fo
r C
irc S
yste
m D
isor
der
Exc
.Upp
er L
imb
& T
oe30
,905
75.0
31.4
73.5
0.96
6
320
9M
ajor
Joi
nt/L
imb
Rea
ttach
men
t of
the
Low
er E
xtre
mity
253,
985
75
.3
21
.2
80
.1
1.
089
9
210
Hip
/Fem
ur P
roc.
Exc
.Maj
or J
oint
, >
17w
/CC
103,
225
83
.4
25
.9
84
.0
1.
010
-3
211
Hip
/Fem
ur P
roc.
Exc
.Maj
or J
oint
, >
17
w/o
CC
22,4
38
78
.0
19
.5
74
.4
0.
938
-3
236
Frac
ture
s of
Hip
and
Pel
vis
25,6
99
75
.7
31
.8
73
.3
0.
946
2
263
Ski
n G
raft/
Deb
ridem
ent
for
Ski
n U
lcer
/Cel
lulit
is w
/CC
14,9
45
63
.1
28
.3
59
.9
0.
909
8
264
Ski
n G
raft/
Deb
ridem
ent
for
Ski
n U
lcer
/Cel
lulit
is w
/o C
C1,
922
51
.0
20
.5
49
.0
0.
931
22
429
Org
anic
Dis
t.A
nd M
enta
l Ret
arda
tion
15,9
40
58
.1
17
.9
50
.8
0.
819
1
483
Trac
heos
tom
y E
xcep
t Fa
ce,
Mou
th,
Nec
k21
,250
82.1
36.2
81.1
0.97
9
9
HC
FA’s
an
d M
edPA
C’s
Rec
om
men
ded
Exp
ansi
on
Tra
nsf
er11
1C
rani
otom
y, >
17 E
xc.T
raum
a15
,180
48.3
10.9
26.0
0.40
5
-217
9R
esp.
Infe
c.A
nd I
nfla
m.>
17 w
/CC
91,7
46
57
.2
22
.7
50
.7
0.
810
15
189
Sim
ple
Pne
umon
ia,
>17
w/C
C16
9,64
4
36.7
11.2
27.8
0.65
1
1019
0S
impl
e P
neum
onia
, >
17 w
/o C
C9,
530
21
.0
2.
2
10.8
0.45
6
-14
191
Sim
ple
Pne
umon
ia,
<18
0
NA
NA
N
A
N
AN
A10
64C
oron
ary
Byp
ass
w/
PT
CA
27,5
42
38
.5
13
.1
28
.7
0.
616
24
1074
Cor
onar
y B
ypas
s w
/ C
ardi
ac C
ath
25,3
35
36
.9
10
.9
26
.3
0.
593
24
1094
Cor
onar
y B
ypas
s w
/o C
ardi
ac C
ath
5,24
6
37.9
8.6
26
.0
0.
593
24
148
Maj
or B
owel
Pro
c w
/CC
51,7
77
41
.2
13
.9
27
.9
0.
511
8
239
Pat
h.Fr
actu
res,
Mus
cuos
kele
tal &
Con
nect
ive
Tis
sue
Mal
igna
ncy
29,5
47
58
.5
16
.4
51
.2
0.
828
8
243
Med
ical
Bac
k P
robl
ems
33,0
90
40
.8
4.
1
17.2
0.35
6
-22
296
Nut
r.an
d M
isc.
Met
abol
ic D
isor
ders
, >
17w
/CC
88,7
01
41
.6
12
.2
28
.8
0.
566
3
415
OR
Pro
c fo
r In
fect
/Par
asiti
c D
isea
se20
,604
57.7
22.1
48.6
0.74
6
2046
8E
xten
sive
OR
Pro
c.U
nrel
ated
to
Prin
cipa
l Dia
g.24
,066
46.7
10.1
27.2
0.46
8
14
All
DR
Gs
6,83
9
26.4
5.8
—
0.42
2
—1
Pos
t-ac
ute
care
(PA
C)
utili
zatio
n w
as id
entif
ied
usin
g M
edic
are
Pro
vide
r A
naly
sis
and
Rev
iew
(M
edPA
R)
disc
harg
e de
stin
atio
n co
des:
03,
skill
ed n
ursi
ng fa
cilit
y, 0
5, p
rosp
ectiv
e pa
ymen
t sy
stem
exe
mpt
, an
d06
, ho
me
heal
th a
genc
y.2
Sho
rt s
tays
def
ined
as
one
day
less
tha
n th
e ge
omet
ric m
ean
leng
th o
f st
ay.A
ll pa
tient
s w
ho d
ied
or w
ere
tran
sfer
red
to a
noth
er a
cute
hos
pita
l are
exc
lude
d.3
Rel
ativ
e od
ds r
atio
= r
atio
of
shor
t-st
ay P
AC
to
non-
PAC
pat
ient
s di
vide
d by
rat
e of
long
-sta
y PA
C t
o no
n-PA
C p
atie
nts.
4 P
rior
to 1
999
DR
G 1
06 c
over
ed C
oron
ary
Byp
ass
with
Car
diac
Cat
heriz
atio
n, a
nd D
RG
107
was
Cor
onar
y B
ypas
s w
ithou
t C
ardi
ac C
athe
rizat
ion.
How
ever
, in
199
8 D
RG
106
was
cha
nged
to
cove
rC
oron
ary
Byp
ass
with
Per
cuta
neou
s Tr
ansl
umin
al C
oron
ary
Ang
iopl
asty
(P
TC
A),
DR
G 1
07 C
oron
ary
Byp
ass
with
Car
diac
Cat
heriz
atio
n an
d D
RG
109
was
cre
ated
to
cove
r C
oron
ary
Byp
ass
with
out
Car
diac
Cat
heriz
atio
n.PA
C v
olum
es r
efle
ct p
artia
l con
vers
ion
to n
ew
cate
gorie
s.
NO
TE
S:D
RG
is d
iagn
osis
-rel
ated
gro
up.M
edPA
C is
Med
ical
Pay
men
t A
dvis
ory
Com
mis
sion
.NA
is n
ot a
vaila
ble.
SO
UR
CE
:Hea
lth C
are
Fin
anci
ng A
dmin
istr
atio
n:M
edPA
R C
laim
s F
iles,
199
8.

HEALTH CARE FINANCING REVIEW/Winter 2002/Volume 24, Number 2 103
Table 2
Top 25 Diagnosis-Related Group (DRG) Complication Pairs Ranked, by Total Post-Acute Care(PAC) Volume: 1998
All PAC Transfers Short-Stay PAC TransfersShare of Total Share of Total Share of Short- Relative
DRG Volume Discharges Discharges Stay Discharges Odds Ratio
1891 169,644 0.37 0.11 0.28 0.651901 9,530 0.21 0.02 0.11 0.461911 0 0.00 0.00 0.00 —
2102 103,225 0.83 0.26 0.84 1.012112 22,438 0.78 0.19 0.74 0.94212 4 0.33 0.08 0.20 0.47
2961 88,701 0.42 0.12 0.29 0.57297 10,269 0.28 0.02 0.13 0.41298 3 0.03 0.01 0.05 1.61
1791 91,746 0.57 0.23 0.51 0.81181 2 0.22 0.11 0.33 2.00180 3,250 0.42 0.11 0.36 0.79
320 76,172 0.44 0.12 0.33 0.66321 7,225 0.27 0.05 0.16 0.51322 4 0.05 0.01 0.04 0.60416 78,850 0.48 0.16 0.39 0.71417 7 0.13 0.04 0.11 0.72121 51,730 0.40 0.12 0.28 0.58122 9,291 0.18 0.04 0.12 0.551061 27,542 0.38 0.13 0.29 0.621071 25,335 0.37 0.11 0.26 0.591091 5,246 0.38 0.09 0.26 0.591481 51,777 0.41 0.14 0.28 0.51149 2,602 0.16 0.04 0.11 0.57104 11,204 0.38 0.08 0.19 0.36105 10,663 0.42 0.10 0.27 0.54218 12,266 0.58 0.17 0.43 0.64219 7,156 0.38 0.02 0.13 0.30220 0 0.00 0.00 0.00 —112 3,384 0.61 0.18 0.44 0.611111 15,180 0.48 0.11 0.26 0.41113 1 0.14 0.00 0.00 0.002632 14,945 0.63 0.28 0.60 0.912642 1,922 0.51 0.21 0.49 0.93154 10,946 0.41 0.11 0.24 0.44155 527 0.09 0.01 0.02 0.12156 0 0.09 0.00 0.00 —172 9,745 0.38 0.11 0.25 0.53173 352 0.17 0.02 0.08 0.40128 5,178 0.56 0.13 0.37 0.55129 1,291 0.38 0.04 0.18 0.43116 5,128 0.47 0.11 0.31 0.54117 809 0.26 0.02 0.07 0.21117 5,283 0.48 0.11 0.30 0.50118 476 0.14 0.02 0.04 0.21269 3,700 0.44 0.12 0.31 0.59270 567 0.21 0.05 0.12 0.47170 3,946 0.41 0.12 0.27 0.52171 138 0.14 0.02 0.07 0.44183 3,401 0.52 0.15 0.41 0.71184 521 0.35 0.02 0.10 0.24
Refer to notes at end of table.

Out of the top 25 pairs, 15 had total PACcounts in 1998 of 10,000 or more. The low-est total PAC count was for DRG pair501/502 (knee procedures with infectionwith or without complications). Yet DRG501 had the highest SPAC transfer rate ofany DRG in any pair other than 210 or211—higher, even, than for any ofHCFA/MedPAC’s additional 13 DRGs(Table 1). Both DRGs 501 and 502 alsoexhibited very high relative odds ratios,and many other DRG pairs also exhibitedhigh relative odds above 0.50. CompanionDRGs were usually uncomplicated or ofyoung age and did not exhibit SPAC ratesas high as their top 25 companion. This islikely because uncomplicated dischargesare in less need of PAC services.
Super-DRG Bundles
Although several complication pairs inTable 2 seem logical candidates for inclu-sion in the PAC transfer policy, groupingDRGs with or without complications maynot be the optimal approach to identifyingthe best candidates. Other, equally impor-tant, criteria split DRGs in ways that under-count aggregate PAC use, as previously
explained. Table 3 presents 10 bundles ofrelated DRGs as potential candidates forexpansion of the PAC transfer policy. (Thenumber of DRGs included in each bundleis in parentheses next to the bundle name.)The bundles have been formed of DRGsthat are clinically related and usually havea common term in their title, e.g., trauma,fracture. Bundles are anchored by at least1 DRG ranked in the top 100 in terms of theshare of SPAC cases in all discharges.Average PAC rates across all DRGs areshown at the top of the table for referencealong with HCFA’s total PAC volume crite-rion of 14,000 discharges. The same DRGcan appear in more than one super-bundle,e.g., the burn DRGs involving trauma andskin grafts.
There were 18 DRGs together with morethan 31,000 PAC discharges reportingsome form of trauma; yet no DRG alonemet HCFA’s 14,000 PAC discharge mini-mum. DRG 280, trauma to skin, age >17w/cc, had the single largest PAC volume:7,320 cases. The trauma bundle had morethan double the average rate of short-stayPAC transfers compared with all DRGs.The relative odds of the group was alsoconsiderably above average.
104 HEALTH CARE FINANCING REVIEW/Winter 2002/Volume 24, Number 2
Table 2—Continued
Top 25 Diagnosis-Related Group (DRG) Complication Pairs Ranked, by Total Post-Acute Care(PAC) Volume: 1998
All PAC Transfers Short-Stay PAC TransfersShare of Total Share of Total Share of Short- Relative
DRG Volume Discharges Discharges Stay Discharges Odds Ratio
226 2,030 0.41 0.11 0.27 0.50227 969 0.23 0.03 0.10 0.32413 2,393 0.46 0.14 0.37 0.71414 142 0.25 0.05 0.14 0.42193 2,285 0.40 0.13 0.29 0.57194 126 0.17 0.03 0.10 0.47501 1,279 0.70 0.30 0.64 0.86502 308 0.56 0.19 0.47 0.771 Included in HCFA/Medicare Payment Advisory Commission’s additional 13 DRGs.2 Included in HCFA's original 10 DRGs.
NOTES: PAC utilization was identified using Medicare Provider Analysis and Review’s discharge destination codes: 03, skilled nursing facility, 05,prospective payment system exempt, and 06, home health agency. Relative odds ratio = ratio of short-stay PAC to non-PAC patients divided by rate oflong-stay PAC to non-PAC patients. All patients who died or were transferred to another acute hospital are excluded.
SOURCE: Health Care Financing Administration: Medicare Provider Analysis and Review Claims Files; data based discharge destination code, 1991-1998.

The 12 skin graft/wound debridementDRGs included more than 47,000 PAC dis-charges with a SPAC/discharge ratio threetimes the overall DRG average. DRG 271,skin ulcers, with 11,715 PAC discharges,exhibited an exceptionally high relativeodds ratio—higher, even, than DRG 263that currently is covered by the PAC trans-fer policy. Although there were only 480cases in total in the burn-related super-bun-dle, the overall relative odds of the eightDRGs was double the national average.
The 23 DRGs involving infections includ-ed more than 600,000 PAC cases, led byDRG 89: simple pneumonia with complica-tions, with 170,000. This DRG is on HCFA’ssecond 10 list. DRGs 79 and 415 in this infec-tions cluster are also on CMS’s list for futureexpansion. Nearly one-third of the infec-tions cases were discharged to PAC with arelative odds ratio 50 percent above average.
Both HCFA and MedPAC staffs targetedopen heart surgery and percutaneoustransluminal coronary angioplasty as poten-tial candidates for expansion. We expandedthe list to include eight major cardiac proce-dures including valve surgery and other
major cardiovascular surgery. Nearly100,000 cases annually would qualify underthis super-bundle that exhibits above-aver-age and rapidly rising SPAC rates. The rel-ative odds ratios of the other thoracic pro-cedures in the bundle were not materiallydifferent from the open heart and percuta-neous transluminal coronary angioplastyDRGs identified by the government.
The seven fracture and four amputationDRGs also exhibited much higher overallPAC and SPAC rates as expected. As agroup, their post-acute followup needs aresimilar to the hip/knee procedures DRGs(209-211) already included in the PACtransfer policy. For example, DRG 113,amputation except upper limb/toe, in thissuper-bundle is already included in thetransfer policy due to very high PAC vol-umes (31,000 cases; relative odds = 0.97).DRG 114, upper limb/toe amputation, andDRG 213, amputation for musculoskeletaland connective system disorders, exhibitvery similar SPAC and relative odds ratiosand should be included along withhip/knee and other amputation procedureDRGs.
HEALTH CARE FINANCING REVIEW/Winter 2002/Volume 24, Number 2 105
Table 3
Potential Post-Acute Care (PAC) Super-Diagnosis Related Group (DRG) Bundles, 1998
Short-StayAll PAC Transfers PAC Transfers
Share of Total Share of Total Relative DRG1 Volume Discharges Discharges Odds Ratio
PercentAll DRGs 14,0002 26.4 5.8 0.42Trauma (18) 31,660 51.0 13.5 0.57 Skin Grafts (12) 47,571 49.3 18.3 0.78 Burns (8) 480 47.5 16.7 0.84 Infections (23) 601,089 36.2 10.8 0.66 Major Cardiac (8) 97,789 34.8 9.2 0.52 Major Joint (17) 445,969 42.3 9.8 0.48 Fractures (7) 78,936 61.1 13.1 0.63 Amputations (4) 43,275 61.4 22.3 0.83 Tracheostomy (2) 24,441 68.3 28.1 0.89 Behavioral (14) 43,725 24.8 6.9 0.83 1 The number of DRGs included in each bundle is in parentheses next to the bundle name.2 HCFA’s total PAC volume threshold.
NOTE: Relative odds = share of short-stay PAC in all short-stay cases divided by similar share of long-stay patients.
SOURCE: Health Care Financing Administration: Medicare Provider Analysis and Review Claims Files, 1998.

We added DRG 482, tracheostomy forface, mouth, and neck, to DRG 483, tra-cheostomy other than face, mouth, andneck, which is already included in the PACtransfer policy. DRG 482’s PAC rate andrelative odds ratio = 0.80 are double that ofthe average DRG. No strong clinical rea-son exists for exempting the roughly 3,000cases in DRG 482.
Finally, 14 behavioral health DRGs, withover 43,000 PAC cases altogether, wereslightly less likely to be discharged to PACthan the average DRG, but when theywere, the relative odds of short-staypatients transferred to PAC was quite high(0.83). Lower PAC rates, coupled withvery high relative odds ratios, may be dueto the fact that behavioral patients are gen-erally transferred only to psychiatric facili-ties, if at all, and not to nursing homes or tohome health care. Psychoses (DRG 430)and several of the substance abuse DRGswith detoxification and/or rehabilitationexhibited relative odds ratios well above1.0. Because psychiatric distinct-part unitsare excluded from PPS, it is important toremember that only scatter-bed patientsare included in our analysis. For some ofthe psychiatric DRGs in particular, it is notclear what kind of treatment is being pro-vided in these scatter beds (Freiman et al.,1988). Furthermore, the presumption thatan acute hospital can always treat thepatient at least as well as a PAC providermay be incorrect for behavioral patients inscatter beds.
HETEROGENEOUS DRGS: CASE STUDY OF CRANIOTOMY
The analysis so far has explored ways ofgrouping similar DRGs to improve the sen-sitivity of the transfer policy in identifyinglow-volume DRGs with high rates of PAC-truncated stays. However, while many inpa-tient discharges have been split across
DRGs in ways that mask total PAC use,other DRGs combine illnesses and proce-dures with markedly different LOS andPAC rates. To illustrate the bimodal/het-erogeneous DRG problem, DRG 1, cran-iotomy, age greater than 17 except for trau-ma, was chosen because it includes a dis-parate set of procedures: craniotomies,skull biopsies, cranial diagnostic proce-dures, brain excisions, ventriculostomies,and shunt insertion, repair and removal.Biopsies require the removal and examina-tion of tissue of the brain, skull, or cerebralmeninges for diagnostic purposes. Ventri-cular shunts are tube-like devices insertedto drain intracranial fluid from the brain toanother body cavity, such as the abdomen,for absorption into the blood stream. Aventriculostomy serves the same generalpurpose as a shunt, but without any tubeinsertion. Based on our clinical under-standing of DRG 1, we hypothesized thatbiopsies are among the least complex pro-cedures. Ventricle shunts are more chal-lenging, while craniotomies, craniectomies,and ventriculostomies require the mostinpatient medical attention and longeststays.
The 1998 MedPAR file was used to con-struct LOS frequency distributions and vol-umes for all DRG 1 procedures identifiedby International Classification of Diseases,Ninth Revision, Clinical Modification (ICD-9-CM) (Public Health Service and HealthCare Financing Administration, 1998) pro-cedure codes. Next, three procedure-spe-cific classes were developed based onaverage LOS patterns and perceiveddegree of clinical complexity. SurgeryClass 1, considered the least severe, con-sisted of biopsies, simple operations, diag-nostic procedures and some shunt replace-ment and insertion. Surgery Class 2,involving more severe cases, includedbrain excisions and cerebral meningesrepair. Surgery Class 3 included the most
106 HEALTH CARE FINANCING REVIEW/Winter 2002/Volume 24, Number 2

intense procedures, such as craniotomy,ventriculostomy, incisions, and some shuntremoval, irrigation and insertion. The dis-tribution of cases across the three sub-groups was roughly equal.
Geometric mean LOSs clearly indicatedistinct inpatient utilization patterns posi-tively correlated with perceived patientseverity of illness (Table 4). Classes 1 and 2had similar PAC discharge patterns with themajority of patients discharged tohome/selfcare. Even still, their PAC userates were well above average (42.1 and 43.5percent, respectively). Mortality rates wererelatively low (near 3 percent) for bothsurgery classes as expected. On the otherhand, Class 3 exhibited a very different dis-charge destination pattern. Only one-quar-ter were sent home with selfcare. A signifi-cant portion of cases were sent to a PACprovider (58.9 percent), and the rate of inpa-tient deaths was very high (23.1 percent).Finally, the geometric mean LOS for Class 3patients was greater than 13 days, despitethe high percentage of non-survivors.
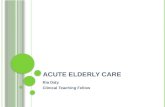
Surgery Classes 1, 2, and 3 have distinctLOS distribution curves (Figure 2). Themodal LOS for Class 1 is 2 days. Class 2peaks at day 4 and Class 3 at day 7. Noticehow the (bold) aggregate LOS frequencydistribution for DRG 1 masks procedure-
specific LOS differences that may beimportant in interpreting PAC dischargesas shifts in the site of care.
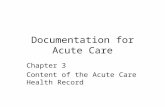
A closer comparison of Class 1 versusClass 3 procedures highlights the potentialproblem of including heterogeneous DRGsin the PAC transfer policy (Figure 3). TheClass 1 geometric mean LOS is 6.4 dayscompared with 13.1 for Class 3 while thegeometric mean LOS for all DRG 1 cases is9.4 days. All cases with LOS <= 9.4-1 = 8.4days would have been paid on a per diembasis under the current PAC policy. Thisincludes all cases under either surgicalclass’s probability density function to theleft of the overall DRG 1 mean. Eight per-cent of Class 1 procedure cases are long-stay PAC cases relative to their proceduregroup mean LOS (area A); yet becausethey have a length of stay of less than 9days, they would be reimbursed as short-stay per diem cases under the PAC transferpolicy. Conversely, 23 percent of the casesin the Class 3 procedure grid (area B)would receive full DRG payment despitebeing short-stay cases relative to their pro-cedure group mean LOS. Areas A and Brepresent false-positive and false-negativeerror rates of the PAC indicator in pickingup true short-stay cases undergoing possi-ble site-of-care substitution.
HEALTH CARE FINANCING REVIEW/Winter 2002/Volume 24, Number 2 107
Table 4
Geometric Mean Lengths of Stay, Mortality, and Post-Acute Care Rates, by Procedure Classes inDiagnosis-Related Group (DRG 1 Craniotomy): 1998
GeometricMean Length of Mortality Discharges with
Surgery Class1 Number of Cases2 Stay (Days) Rate3 Post Acute Care2
PercentTotal 24,356 9.3 — —
Class 1 (Least) 7,643 6.4 3.3 42.1
Class 2 (Moderate) 9,242 8.5 2.8 43.5
Class 3 (Most) 7,471 13.1 23.1 58.91 The perceived degree of clinical complexity is in parenthesis next to the surgery class.2 Excludes inpatient deaths.3 Based on all admissions in given class.
SOURCE: Health Care Financing Administration: Medicare Provider Analysis and Review Claims Files, 1998.

DISCUSSION
In this section, we first make some rec-ommendations for DRG groups that arestrong candidates for the next round of pol-icy expansion. Then we review two typesof DRGs that, for clinical reasons, may notbe ideal candidates even though theyexhibit high PAC rates. Next, we presentadministrative arguments for and against amuch larger expansion of the transfer poli-cy to most (or all) DRGs before concludingwith a recommendation about how to cal-culate geometric mean LOS so as to avoida provider induced bias in the future.
Before moving to recommendations, it isworth reiterating that no single criterion orthreshold is clearly superior when recom-mending expansion of the PAC transfer
policy to other DRGs. The congressionalmandate to choose 10 high-PAC DRGs,therefore, was somewhat arbitrary.Nonetheless, HCFA staff selected whatappear to be excellent choices based on allthe criteria. All 10 not only exhibitedunusually high SPAC rates per discharge,but also high rates per short-stay dis-charge as well as relative to PAC ratesamong long-stay patients.
Recommended DRG Bundles
Most of the second 10 DRGs initiallyconsidered by HCFA staff, complementedby 3 additional DRGs recommended byMedPAC staff, also appear to be logicalchoices. Nearly all exhibit high rates ofSPAC discharges compared with most
108 HEALTH CARE FINANCING REVIEW/Winter 2002/Volume 24, Number 2
0
Length of Stay in Days
Nu
mb
er o
f C
ases
2,600TotalSurgery Class 1 (Least)Surgery Class 2 (Most)Surgery Class 3 (Most)
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
1,000
1,200
1,600
2,000
2,400
600
2,200
1,800
1,400
800
400
200
1 Excludes inpatient deaths.
SOURCE: Health Care Financing Administration: Medicare Provider Analysis and Review (MedPAR) Claims Files, 1998.
Figure 2
Frequency1 Distribution of Diagnosis-Related Group (DRG 1 Craniotomy), by Procedure Surgery Class: 1998

other DRGs as well as relative to their ownlong-stay PAC rates. DRG 1, craniotomy,may not be appropriate because of its dis-parate procedure mix.
Strong empirical and theoretical argu-ments can be made, however, to broadenthe scope of inclusion to consider DRGclusters with a common characteristic.Our research shows that underlying com-mon characteristics of DRGs lead to extra-ordinary PAC discharge rates and truncat-ed stays. Hence, serious omissions occurby ignoring individual DRGs that fail tomeet a minimum PAC discharge threshold(e.g., 14,000 cases). In particular, splittingDRGs by complication rates undercountsPAC use rates related in a fundamental wayto the reason for admission. This is whyHCFA staff (wisely) included DRG 264,skin graft/debridement for skin ulcer with-
out complications, in its original 10 DRGs.We recommend that HCFA staff alwaysinclude both DRGs in a complicated/uncomplicated pair to avoid overlookingPAC-truncated stays and gaming in the ini-tial coding of the case.
If HCFA staff wish to recommend inclu-sion of any of the 13 DRGs they (andMedPAC) had considered, initially, westrongly recommend including clusters ofrelated DRGs anchored by 1 of the 13DRGs. The consistently high SPAC ratesamong trauma, skin graft, burn, infection,fracture, and amputation patients is strik-ing and confirm the notion that early dis-charge to PAC is not isolated in a fewDRGs. For example, we would not limitexpansion to DRGs 79 and 89-91 pertainingto respiratory infections and pneumonia.Rather, we recommend including all 23
HEALTH CARE FINANCING REVIEW/Winter 2002/Volume 24, Number 2 109
0
Length of Stay in Days
Nu
mb
er o
f C
ases
1,400Surgery Class 1 (Least)Surgery Class 3 (Most)
1 3 5 7
A
Class 1 Mean6 Days
Class 1 Mean9 Days
Class 3 Mean13 Days
B
9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
400
600
800
1,000
1,200
200
SOURCE: Health Care Financing Administration: Medicare Provider Analysis and Review Claims Files; data baseddischarge destination code, 1991-1998.
Figure 3
Frequency of Diagnosis-Related Group (DRG 1 Craniotomy), Length of Stay, by Surgery Class: 1998

infection-related DRGs that exhibit system-atically high SPAC rates relative to otherDRGs and their own long-stay PAC rates.Particularly telling is the fact that severalother DRGs within the infections super-bundle exhibit even higher SPAC ratesthan DRGs 79 and 89-91, although theirPAC volumes do not meet Congress’ top 10volume criterion. The same argument wouldapply to the coronary bypass DRGs. Ifthey were included in any expansion, thensimilar major heart surgeries (e.g., valves)ought to be included as well given theirsimilar SPAC transfer rates.
Inappropriate DRGs for Expansion
By contrast, there may be two clinicalreasons for not automatically expandingthe PAC policy to some DRGs. First, het-erogeneous DRGs undermine CMS’s site-of-care justification for its per diem pay-ment policy. Hospitals could argue theyare only referring patients to PAC thathave above-average LOS for the particularprocedure included in a DRG. CMS couldstill argue on actuarial grounds that it isoverpaying for all SPAC cases, regardlessof procedure, if PAC rates have been risingfor short-stay patients. Besides calling fora thorough investigation of their draw-backs for per diem payment, heteroge-neous DRGs may call for a more refinedset of DRGs than currently in use in thePPS program in general.
Second, short-stay psychiatric/substanceabuse discharges to PAC may be appropri-ate. The set of behavioral health DRGs(i.e., psychiatric and substance abuse)exhibited particularly high relative oddsratios suggesting an unusually high fre-quency of short-stay patients discharged toPAC. Yet, it is not obvious that every gen-eral acute hospital is the optimal providerfor such patients. If smaller hospitals aresimply stabilizing patients before transfer
to a psychiatric or rehabilitation facility,CMS may not want to discourage suchbehavior with diminished per diem pay-ment. More study of these patients isneeded before including the psychiatricand substance abuse DRGs in the PACtransfer policy.
Having recommended several logicalclusters of DRGs for expansion, contrastedwith other DRGs that raise doubts about auniversal PAC transfer policy, let us nextsummarize the key administrative argu-ments for and against expanding the PACtransfer policy to many more DRGs.
Arguments for Expanding PAC DRGs
Shifts in site-of-care can occur in anyDRG. Early discharge to PAC likelyinvolves a shift in the site-of-care regardlessof how many PAC discharges there are in aDRG. Applying a minimum threshold toany continuous criterion, such as the over-all or SPAC rate, will always appear arbi-trary to providers by paying some PAC-truncated stays differently than others.
10 DRGs inequitable to some hospitals.Hospitals treating a disproportionate num-ber of cases in the 10 (or even expandedlist of) DRGs may be unfairly treated bythe narrow scope of the policy. One hospi-tal might concentrate on major jointsurgery that is subject to lower per diempayments while another competitor empha-sizes major heart surgery which is not; yet,both facilities may be discharging patientsearly to PAC.
Simple, uniform, formula-driven policy.The PAC per diem payment algorithm isformula driven and keys off the standarddischarge destination code on the claim. Acomprehensive formulistic policy alreadyin place would immediately begin pickingup SPAC transfers in other DRGs and auto-matically discourage premature transfers.It would be simple for Medicare fiscal
110 HEALTH CARE FINANCING REVIEW/Winter 2002/Volume 24, Number 2

intermediaries to implement a policychange for all (or most) DRGs while avoid-ing confusion about which DRGs were eli-gible for PAC transfer payment.
PAC Discharges Result in ProgramOverpay-ments. Early discharges to PACproviders constitute a shift of the site-of-care resulting in overpayments to the acutefacility for care it did not provide. A roughestimate of the potential savings fromextending the PAC transfer policy to allDRGs would be slightly less than 1 percentof all Medicare acute hospital DRG pay-ments, or $720 million annually. This esti-mate is based on an average SPAC rate ofapproximately 6 percent (Table 1), an aver-age 15 percent per diem discount on fullDRG payment for PAC transfers (Gilman etal., 2000), and $80 billion in DRG expendi-tures in 1999. If hospitals lengthened PACstays or stopped discharging as frequentlyto post-acute providers, inpatient programsavings would be less, but so, too, wouldoutlays on PAC.
Arguments Against Expanding PACDRGs
Two administrative arguments can bemade against expanding the PAC transferpolicy to all DRGs.
Requires multiple per diem payment poli-cies. CMS has already determined that thestandard transfer payment policy fails tocover high front-end costs for DRGs 209-211. Were the policy extended to all (ormany) DRGs, CMS would have to evaluatethe daily cost patterns of 500 DRGs. Arelated concern is the asymmetric treat-ment of transfers to other acute hospitalsversus PAC transfers. Only PAC transfersin DRGs 209-211 enjoy a blended per diemthat pays one-half of the full DRG paymenton the first day. Transfers to other acutehospitals for the same set of DRGs receive
less generous double per diems for thefirst day. If CMS expands the list of DRGPAC transfers, it may have to reconsider itsper diem payment algorithm for acute-to-acute hospital transfers.
More auditing required. Fiscal interme-diaries are required to audit the dischargedestination codes for accuracy now thatthey are used for payment purposes.Extending the policy to many more DRGswould require extensive auditing. Thiswould require linking PAC claims fromother Part A and B providers with inpatientclaims because of the 24- and 72-hour post-discharge windows established by the poli-cy, a costly and time-consuming process.Also, with many more DRGs, CMS (andhospitals) would have more work sortingout unrelated from related PAC dis-charges. Annual program savings wouldpay for these administrative costs.
Long-Run Implications of ShorterStays
Besides the arguments against expand-ing the policy to more DRGs, the pervasivetrend toward shorter acute stays naturallylimits the policy’s effectiveness. Our analy-sis revealed many DRGs whose geometricmean LOS was: 3 days or less. As PACrates and truncated inpatient stays rise,DRG geometric mean stays fall, resultingin fewer and fewer short-stay PAC casesqualifying for per diem payment. This cre-ates a bias in the transfer payment policyby allowing the threshold criterion forreduced payment, i.e., geometric meanLOS, to be influenced by industry PAC dis-charge behavior. To avoid this bias, geo-metric mean LOS for payment purposesshould be based on discharges excludingtransfers to other acute hospitals or to PACproviders.
HEALTH CARE FINANCING REVIEW/Winter 2002/Volume 24, Number 2 111

ACKNOWLEDGMENTS
We wish to express our appreciation to DanMcGrane who provided valuable comments.
REFERENCES
Buczko, W.: Inpatient Transfer Episodes AmongAged Medicare Beneficiaries. Health CareFinancing Review 15(2):71-87, Winter 1993.Federal Register: Medicare Program: Changes tothe Hospital Inpatient Prospective PaymentSystems and Fiscal Year 2001 Rates; Final Rule.65FR(148):47079 (August 1, 2000).Federal Register: Medicare Program; Changes tothe Hospital Inpatient Prospective PaymentSystems and Fiscal Year 2001 Rates; Proposed Rule.65FR(88):26302 (May 5, 2000).Federal Register: Medicare Program: Changes tothe Hospital Inpatient Prospective PaymentSystems and Fiscal Year 1999 Rates; Final Rule.63FR(147): 40974 (July 31, 1998a).Federal Register: Medicare Program; Changes tothe Hospital Inpatient Prospective PaymentSystems and Fiscal Year 1999 Rates; Proposed Rule.63FR(89):25590 (May 8, 1998b).Freiman, M., McGuire, T., Ellis, R., et al.: AnAnalysis of Options for Including PsychiatricInpatient Settings in a Prospective Payment System.National Institute of Mental Health. Rockville, MD.June 1988.
Gilman, B.H., Cromwell, J., Adamache, W., andDonoghue, S.: Study of the Effect of Implementing thePostacute Care Transfer Policy under Inpatient PPS.Health Care Financing Administration. Baltimore,MD. July 31, 2000.Lee, J., Ellis, R., and Merrill, A.: Bundling Post-Acute Care with Medicare DRG Payments: AnExploration of the Distributional and RiskConsequences. Inquiry 33(3):381-394, Fall 1996.Medicare Payment Advisory Commission: Reportto Congress: Medicare Payment Policy. Washington,DC. March 2000.Medicare Payment Advisory Commission: Reportto Congress: Context for a Change Medicare Program.Washington, DC. June 1998.Prospective Payment Assessment Commission.Report to Congress: Medicare and the AmericanHealth Care System. Washington, DC. June 1993.Public Health Service and Health Care FinancingAdministration: International Classification ofDiseases, Ninth Revision, Clinical Modification. U.S.Department of Health and Human Services. U.S.Government Printing Office. Washington, DC.1998.Schneider, J., Cromwell, J., and McGuire, T.P.:Excluded Facility Financial Status and Options forPayment System Modification. Health CareFinancing Review 15(2):7-30, Winter 1993.
Reprint Requests: Jerry Cromwell, Ph.D., RTI International, 411Waverley Oaks Road, Suite 330, Waltham, MA 02452-8414. E-mail: [email protected]
112 HEALTH CARE FINANCING REVIEW/Winter 2002/Volume 24, Number 2

TECHNICAL NOTE
In the transfer policy, per diem paymentwill be less than the full DRG payment(DRG) for a patient with LOS if2[DRG/GLOS] + (LOS -1)[DRG/GLOS] <DRG where GLOS = the geometric meanand DRG/GLOS = the per diem rate.Solving the inequality, [DRG/GLOS](2+LOS-1) < DRG, or LOS+1 < GLOS.
With regard to payment biases fromexcluding a related DRG, the greater thedisparity in full payment between the DRGpair and the higher the geometric meanLOS of the uncomplicated DRG, the lessincentive there is not to code complica-tions. For the uncomplicated DRG to gen-erate the same or greater revenue than itscomplicated paired DRG, the per diem rev-enue from the complicated DRG must beless than the full DRG payment from
billing the uncomplicated DRG. Thisassumes that a patient’s LOS would qualifyfor full DRG payment in the uncomplicat-ed, but not in the complicated DRG. That is, DRGu > PDc (LOSi + 1) =(DRGc/GLOSc) (LOSi +1), where DRGuand DRGc = full payment for the uncompli-cated and complicated DRG pair, PDc = theper diem of the complicated DRG, GLOSc =the complicated DRG’s geometric meanstay, and LOSi = the i-th patient’s LOS.Rearranging the inequality gives (LOSi +1)/GLOSc <DRGu/DRGc. For the hospitalto have an incentive not to code complica-tions and receive full DRGu payment, thepatient’s LOS plus one day relative to thecomplicated DRG’s geometric mean LOSwould have to be less than the relative fullpayments of the DRG pair.
HEALTH CARE FINANCING REVIEW/Winter 2002/Volume 24, Number 2 113