
EXERCISE AFTER STROKE Specialist Instructor Training Course L6 Exercise after stroke: theory and...
43
EXERCISE AFTER STROKE Specialist Instructor Training Course L6 Exercise after stroke: theory and evidence
-
Upload
jodie-underwood -
Category
Documents
-
view
224 -
download
0
Transcript of EXERCISE AFTER STROKE Specialist Instructor Training Course L6 Exercise after stroke: theory and...
EXERCISE AFTER STROKESpecialist Instructor Training Course
L6Exercise after stroke:theory and evidence
Overview of Session• What is fitness training? • How randomised controlled trials are
designed• Systematic review of fitness training after
stroke (2004)• STARTER• Systematic review (2008)• Contraindications to exercise training
Learning outcomesAfter this session you should be able to:
• Describe what is known, and what is not known about the effects of exercise on stroke recovery.
• Discuss the strengths and limitations of the evidence for exercise after stroke
• Explain how the STARTER trial informs the current course
• State the recommendations for exercise after stroke
• List the contra-indications for exercise after stroke
Physical FitnessA set of attributes which people have or achieve,that confers the ability to perform physical activity;
Cardiorespiratory fitness (central and peripheral components)
Muscular strength (maximum force that can be generated byA muscle) and muscle power (rate at which muscular forceCan develop during a single muscle contraction)
Body composition (relative amounts of muscle and adiposetissue)
Physical Fitness Training
• Planned, structured regimen of regular physical exercise deliberately performed to improve one or more components of physical fitness (UHDHHS 1996)
• Physical fitness training after stroke may, in theory– Improve function– Reduce disability– Improve quality of life – Improve mood – Reduce fatigue– Reduce the risk of falls– Improve vascular risk factors and so reduce risk of
recurrent stroke and death
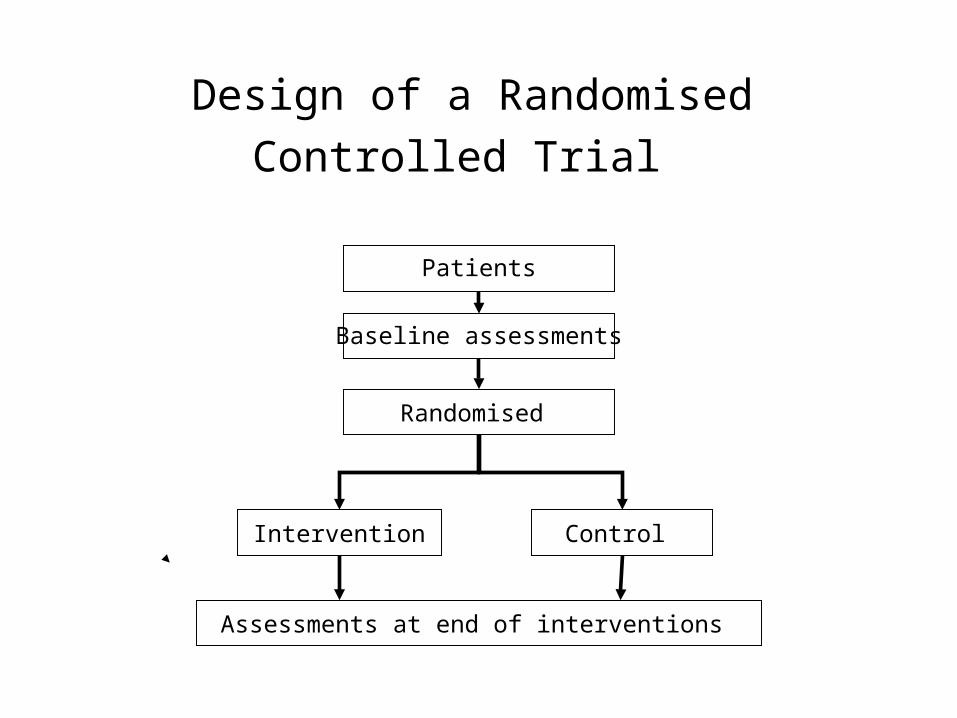
Design of a Randomised Controlled Trial
Patients
Baseline assessments
Randomised
Control Intervention
Assessments at end of interventions
Systematic reviews and meta-analyses
• Combines results of all trials of the same (or similar) intervention
• Provides a more precise measure of the
effectiveness (and risk) of an intervention than a single trial
• Widely used to guide clinical practice
Cochrane Systematic Review Physical fitness training after stroke
How?Extensive literature search and scrutiny of trials by 3Reviewers
We found; 12 trials (289 patients) BUTOnly 4 trials (60 patients) used ‘mixed’ trainingOnly 2 trials (33 patients) of adequate length to improvefitness Little information on feasibility More trials needed
Saunders Greig Young Mead 2004
What has happened since 2004?
• More trials have been performed, including our own STARTER trial
• A further systematic review and meta-analysis has been performed to determine the effect of physical fitness training on– Death – Dependence– Death and dependence– Disability– Physical function, physical fitness– Mood, fatigue – Whether benefits are retained after training complete
Aims of STARTER
• Determine feasibility of physical fitness training after stroke
• Obtain data about the effect of physical fitness compared with an attention control intervention
• Use STARTER results to design a bigger trial
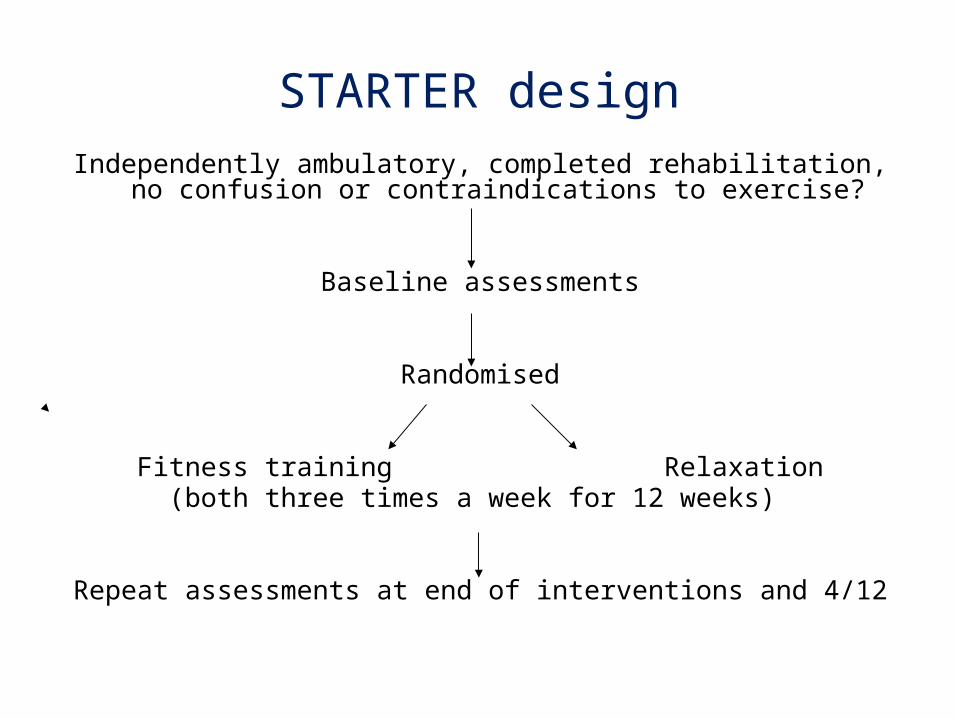
STARTER designIndependently ambulatory, completed rehabilitation, no confusion or
contraindications to exercise?
Baseline assessments
Randomised
Fitness training Relaxation(both three times a week for 12 weeks)
Repeat assessments at end of interventions and 4/12
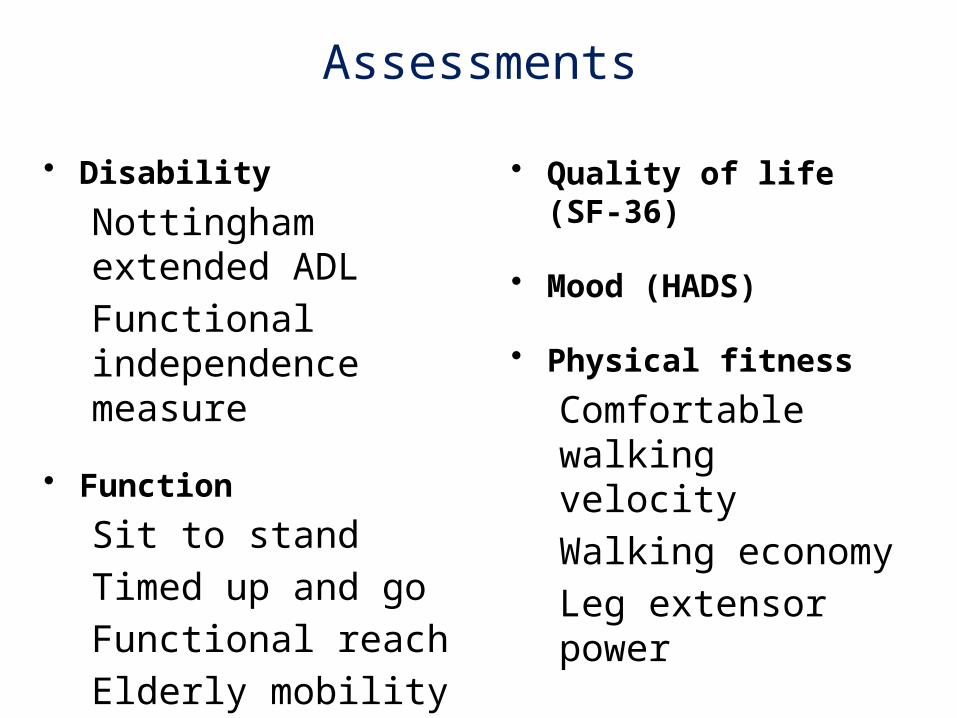
Assessments
• Disability
Nottingham extended ADL
Functional independence measure
• Function
Sit to stand
Timed up and go
Functional reach
Elderly mobility scale
Rivermead motor index
• Quality of life (SF-36)
• Mood (HADS)
• Physical fitness
Comfortable walking velocity
Walking economy
Leg extensor power
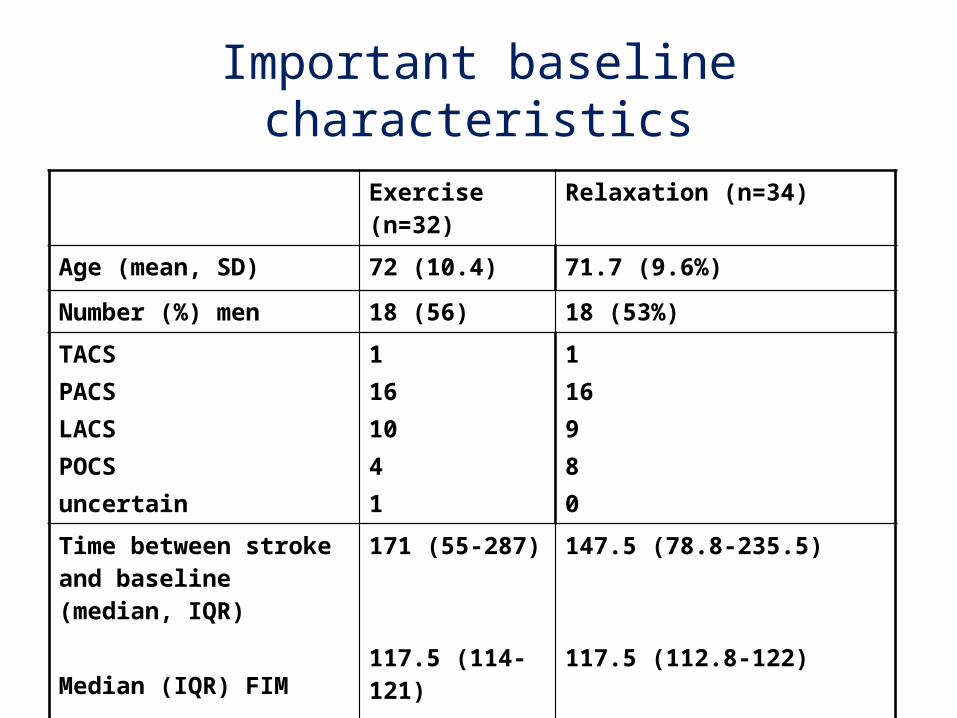
Important baseline characteristics
Exercise (n=32) Relaxation (n=34)
Age (mean, SD) 72 (10.4) 71.7 (9.6%)
Number (%) men 18 (56) 18 (53%)
TACSPACSLACS POCS uncertain
1 16 10 4 1
116980
Time between stroke and baseline (median, IQR)
Median (IQR) FIM
171 (55-287)
117.5 (114-121)
147.5 (78.8-235.5)
117.5 (112.8-122)
Fitness training intervention
• Devised by a Clinical Exercise Instructor in collaboration with a Specialist Stroke Physiotherapist (Mark Smith)
• Progressive in duration and intensity
• Warm up and cool down
• Cycling, marching, stepping, staircase, ball raises, chest press
• Resistance band exercises, sit-to-stand, arm press



Relaxation (attention control)
• Same venue as exercise class• Same instructor• 3 times a week, 12 weeks• Performed seated
– Deep breathing– Progressive muscle relaxation (no muscle
contraction)– During 12 weeks: progression

Feasibility: recruitmentAmbulatory patients assessed
(RIE, Liberton and AAH) 301Eligible 147 Agreed to take part 80
changed their minds -14developed contraindications -11died -1
Additional Recruitment (WGH) 12 Total 66
Feasibility: attendance
• Median number of classes attended was – 36 (IQR 30 to 36.75) for exercise– 36 (IQR 30.5 to 37) for relaxation
• At post-intervention assessment– 64 (97%) attended 1st post-intervention
assessment– 62 (94%) attended 2nd post-intervention
assessment
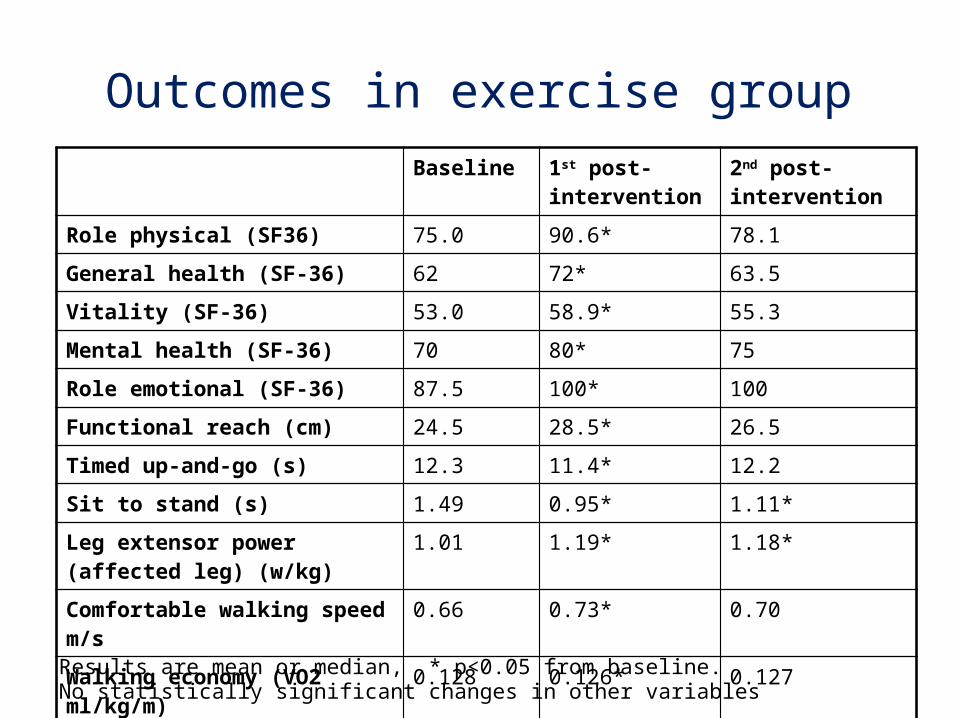
Outcomes in exercise group
Results are mean or median, * p<0.05 from baseline. No statistically significant changes in other variables
Baseline 1st post-intervention
2nd post-intervention
Role physical (SF36) 75.0 90.6* 78.1
General health (SF-36) 62 72* 63.5
Vitality (SF-36) 53.0 58.9* 55.3
Mental health (SF-36) 70 80* 75
Role emotional (SF-36) 87.5 100* 100
Functional reach (cm) 24.5 28.5* 26.5
Timed up-and-go (s) 12.3 11.4* 12.2
Sit to stand (s) 1.49 0.95* 1.11*
Leg extensor power (affected leg) (w/kg)
1.01 1.19* 1.18*
Comfortable walking speed m/s 0.66 0.73* 0.70
Walking economy (VO2 ml/kg/m)
0.128 0.126* 0.127
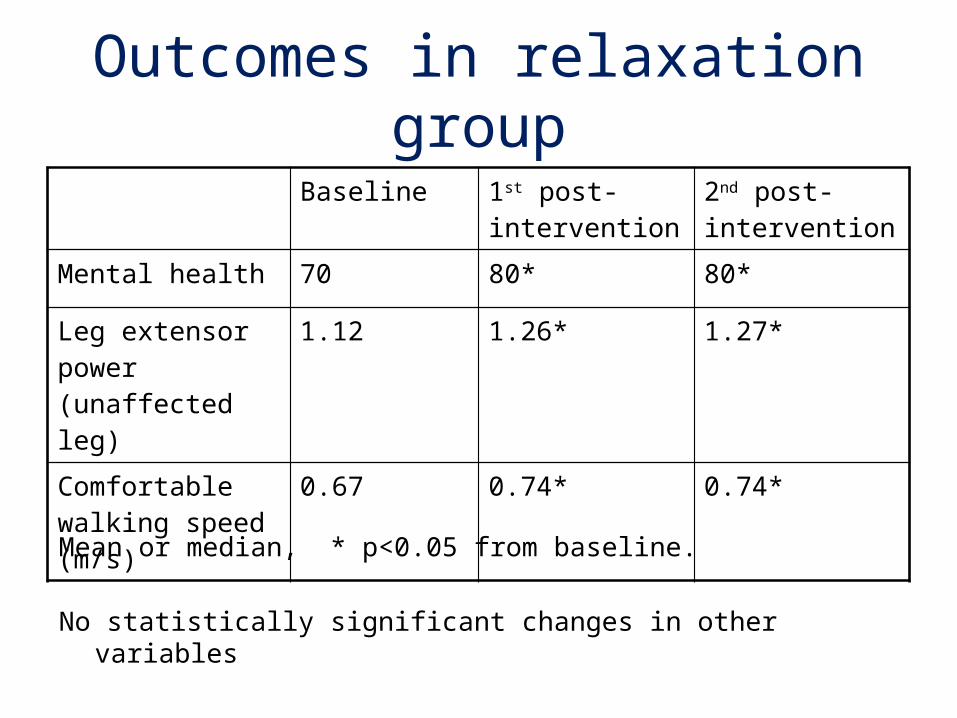
Outcomes in relaxation group
Mean or median, * p<0.05 from baseline.
No statistically significant changes in other variables
Baseline 1st post-intervention
2nd post-intervention
Mental health 70 80* 80*
Leg extensor power (unaffected leg)
1.12 1.26* 1.27*
Comfortable walking speed (m/s)
0.67 0.74* 0.74*
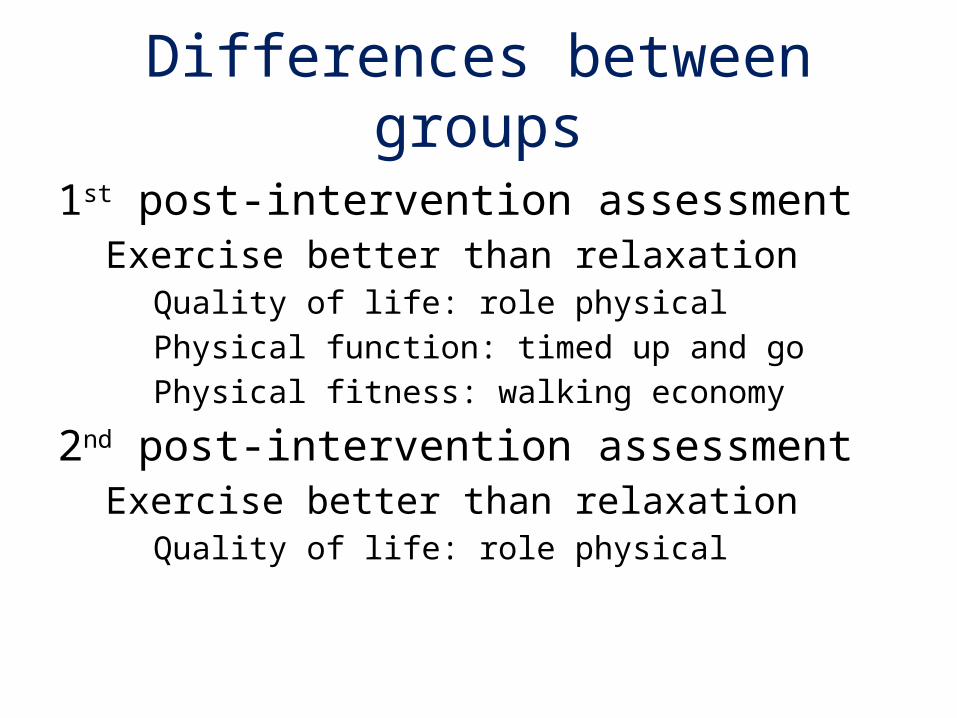
Differences between groups
1st post-intervention assessment Exercise better than relaxation
Quality of life: role physical
Physical function: timed up and go
Physical fitness: walking economy
2nd post-intervention assessment Exercise better than relaxation
Quality of life: role physical
Qualitative sub-study (benefits)
• Enjoyment– The class itself – Socialising – Getting out of the house
• Tuition– Endless praise for Irene (the exercise
instructor)– Participants felt ‘well looked-after’– Irene had a major role in the success of the
class
Qualitative sub-study (benefits)• Perceived benefits from both classes:
– Physical recovery– Getting back into a routine– Improved mood and wellbeing– Confidence
• Long term effects– Learning new skills– Practising at home– Attending other classes
To quote one participant…….
It was back in November and it was no joke
That was the time that I suffered a stroke….
Round came time for relaxation class
Others were there who’d been in the same boat…
The things we learned were useful and good….
The lady who ran the class is an excellent woman
Her voice is gentle and booming……
Thanks to the excellence of the wonderful Irene
Conclusions
• Trial design was feasible
• Exercise was more beneficial than relaxation for some outcomes
• Not all benefits were maintained long-term
• These results are included in the updated Cochrane systematic review and meta-analysis
Physical Fitness Training for Stroke Patients
Protocol first published: Cochrane Library, Issue 4, 2001
Review first published: Cochrane Library, Issue 1, 2004
Review updated: Cochrane Library, Issue 4, 2009
Cochrane Library, Issue 4, 2011
Cochrane Library, Issue 4, 2013
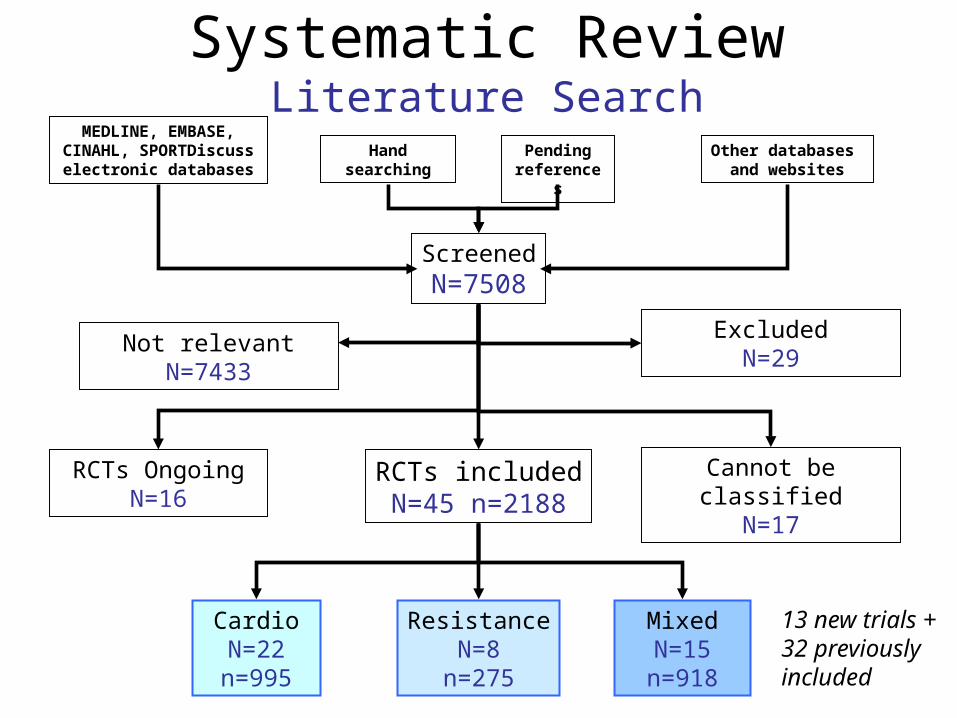
Systematic ReviewLiterature Search
ScreenedN=7508
RCTs includedN=45 n=2188
Not relevant N=7433
CardioN=22n=995
ResistanceN=8
n=275
MixedN=15n=918
MEDLINE, EMBASE, CINAHL, SPORTDiscuss
electronic databasesHand
searchingPending
referencesOther databases
and websites
13 new trials + 32 previouslyincluded
ExcludedN=29
RCTs OngoingN=16
Cannot be classifiedN=17
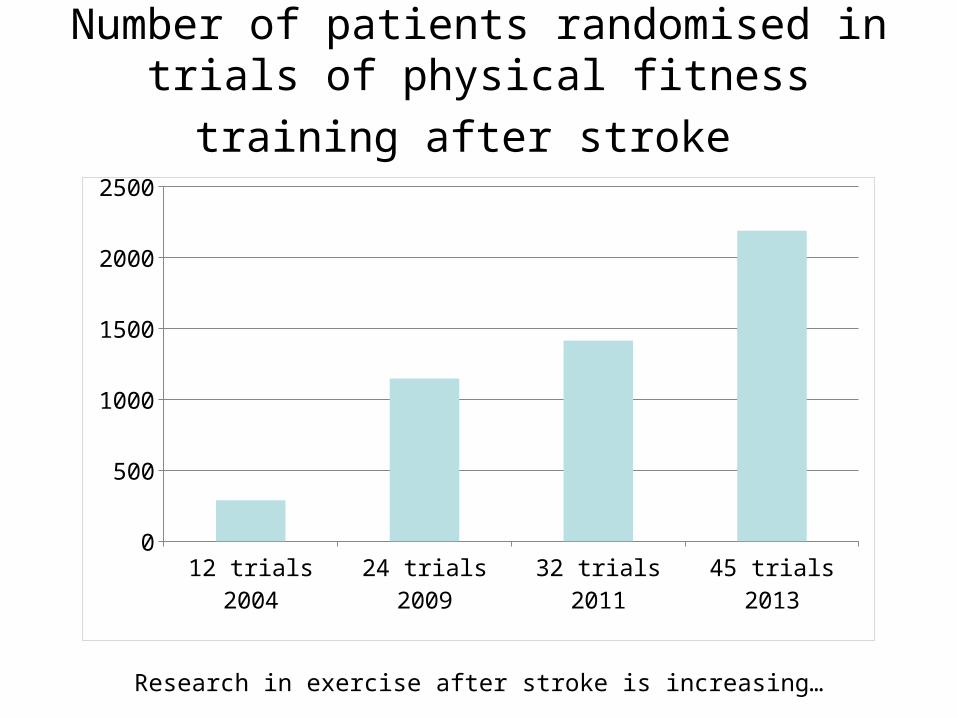
Number of patients randomised in trials of
physical fitness training after stroke
12 trials 2004 24 trials 2009 32 trials 2011 45 trials 20130
500
1000
1500
2000
2500
Research in exercise after stroke is increasing…
Trial participants
• Average age 64 years (i.e. younger than the median age of stroke onset of 72)
• 60% men, 40% women
• Majority were ambulatory
• Time since stroke: 8.8 days to 7.7 years
• PrimaryEffects of training on death & dependence unclear
Exercise improves of disability
• SecondaryExercise improves physical fitnessExercise improves walkingExercise improves balanceOther benefits unclear
ResultsPrimary & Secondary Outcomes
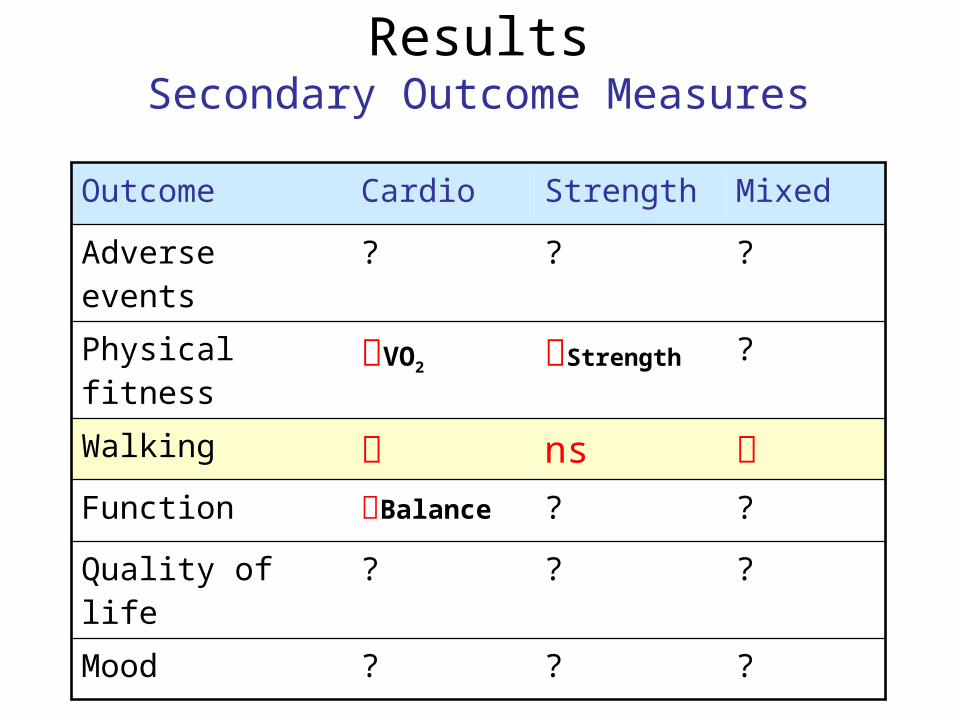
ResultsSecondary Outcome Measures
Outcome Cardio Strength Mixed
Adverse events ? ? ?
Physical fitness VO2 Strength ?
Walking ns
Function Balance ? ?
Quality of life ? ? ?
Mood ? ? ?
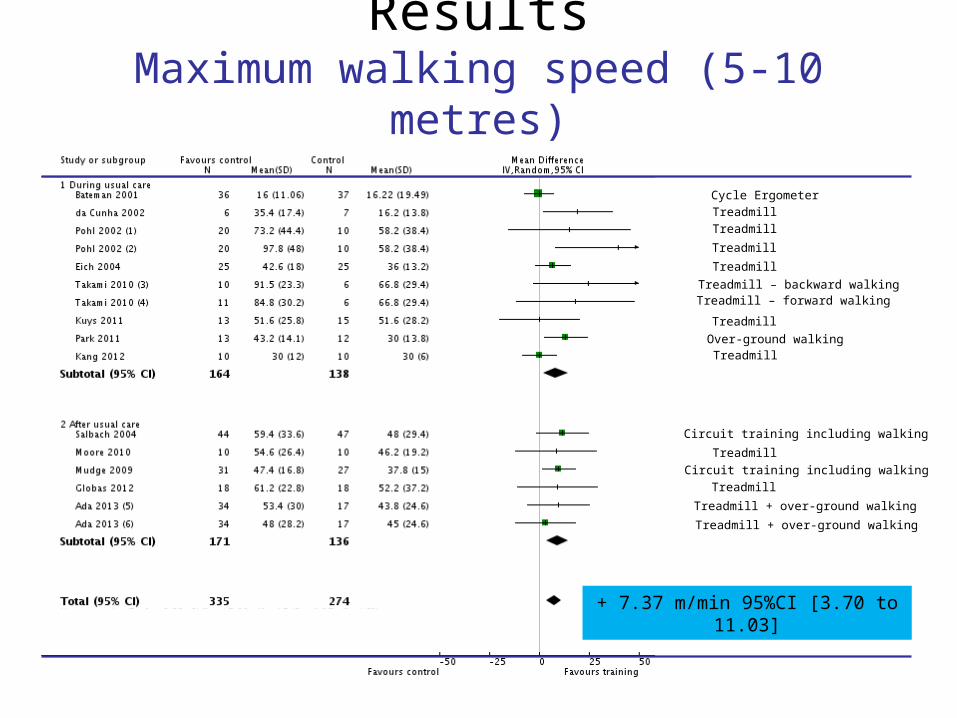
ResultsMaximum walking speed (5-10 metres)
Cycle Ergometer
Treadmill
Treadmill
Treadmill
Treadmill
Treadmill
Treadmill – backward walkingTreadmill – forward walking
Treadmill
TreadmillOver-ground walking
Circuit training including walking
Circuit training including walking
Treadmill
Treadmill + over-ground walking
Treadmill + over-ground walking
+ 7.37 m/min 95%CI [3.70 to 11.03]
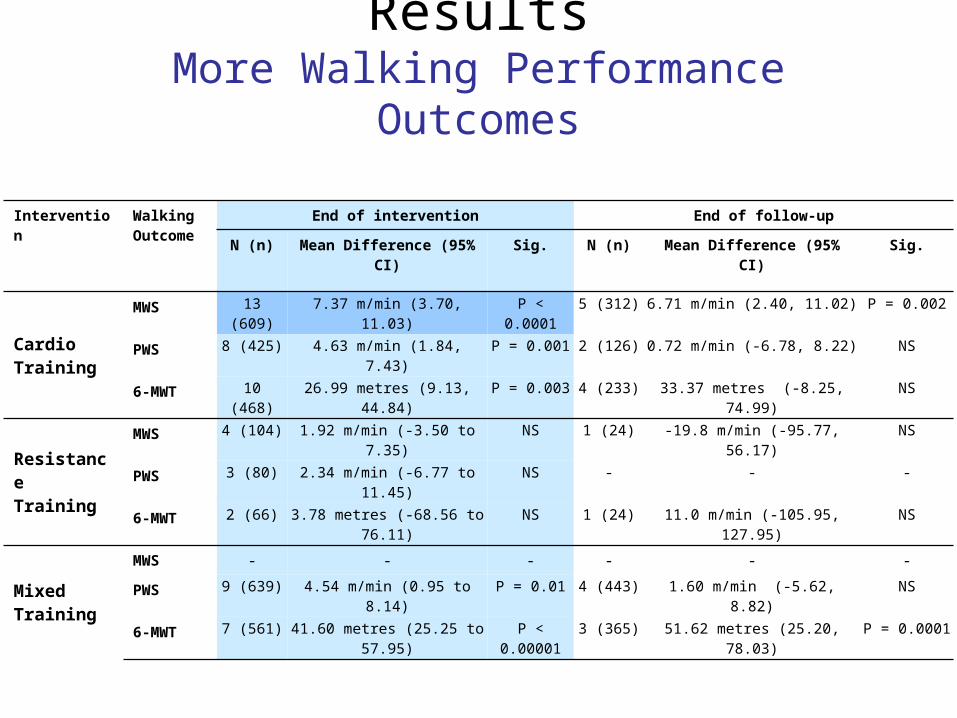
Intervention Walking Outcome
End of intervention End of follow-up
N (n) Mean Difference (95% CI) Sig. N (n) Mean Difference (95% CI) Sig.
CardioTraining
MWS 13 (609) 7.37 m/min (3.70, 11.03) P < 0.0001 5 (312) 6.71 m/min (2.40, 11.02) P = 0.002
PWS 8 (425) 4.63 m/min (1.84, 7.43) P = 0.001 2 (126) 0.72 m/min (-6.78, 8.22) NS
6-MWT 10 (468) 26.99 metres (9.13, 44.84) P = 0.003 4 (233) 33.37 metres (-8.25, 74.99) NS
Resistance Training
MWS 4 (104) 1.92 m/min (-3.50 to 7.35) NS 1 (24) -19.8 m/min (-95.77, 56.17) NS
PWS 3 (80) 2.34 m/min (-6.77 to 11.45) NS - - -
6-MWT 2 (66) 3.78 metres (-68.56 to 76.11) NS 1 (24) 11.0 m/min (-105.95, 127.95) NS
MixedTraining
MWS - - - - - -
PWS 9 (639) 4.54 m/min (0.95 to 8.14) P = 0.01 4 (443) 1.60 m/min (-5.62, 8.82) NS
6-MWT 7 (561) 41.60 metres (25.25 to 57.95) P < 0.00001 3 (365) 51.62 metres (25.20, 78.03) P = 0.0001
ResultsMore Walking Performance Outcomes
ConclusionsPhysical fitness training after stroke
• Training improves disability, physical fitness, walking performance & balance
• Benefits are confined to cardiorespiratory and mixed training
• Benefits are exercise-specific • Further research is required
(e.g. optimal ‘prescription’, long-term benefits, risks, costs, non-ambulatory patients)
What we don’t know• Effect of fitness training on many important
outcomes e.g. mood, fatigue, falls, disability, dependence and death
• Effect on vascular risk factors• Optimum type of training• Optimum mode, frequency, intensity, duration• Timing (e.g. in-patient, after usual rehab)• Whether any benefits are retained longer-term• Feasibility of exercise delivery to non-ambulatory
patients• Might some benefits be mediated by social
interaction? • How to ensure people continue exercise after
initial training programme
Implications for exercise classes after stroke
• Exercise training may improve walking ability if cardiorespiratory training is included
• Disability may be improved by cardiorespiratory training or mixed training
• Effects of strength training alone are uncertain
• Further research is needed
Absolute contraindications to exercise training
• Uncontrolled angina• Recent myocardial infarction• Resting systolic blood pressure
>180 mmHg or resting diastolic BP of >100mm Hg
• Significant drop in BP during exercise
• Uncontrolled resting tachycardia >100 beats per minute
• Unstable or acute heart failure• New or uncontrolled arrhythmia• Severe stenotic or regurgitant
valvular heart disease• Hypertrophic obstructive
cardiomyopathy• Third degree heart block • Acute aortic dissection • Acute myocarditis or
pericarditis
• Unstable diabetes• Uncontrolled visual or
vestibular disturbances• Recent injurious fall without
medical assessment• Proven inability to comply with
the recommended adaptations to the exercise programme and inability to maintain an upright posture in sitting
• Febrile illness • Extreme obesity, with weight
exceeding the recommendations or the equipment capacity (usually >159kg [350 lb.])
• Acute pulmonary embolus or pulmonary infarction
• Deep venous thrombosis
Relative contraindications
• Cardiomyopathy • Moderate stenotic valvular heart disease • Complex ventricular ectopy • Left main coronary artery stenosis • Electrolyte imbalance • Tachyarrhythmias or bradyarrhythmias• High degree atrio-ventricular block• Mental or physical impairment leading to inability
to exercise adequately
Acknowledgements
• Dr Dave Saunders, Lecturer, University of Edinburgh
• Dr Carolyn Greig, Senior Research Fellow, University of Edinburgh
• Professor Archie Young, Emeritus Professor, University of Edinburgh
• Hazel Fraser and Brenda Thomas Cochrane Stroke Group http://www.dcn.ed.ac.uk/csrg
Essential Reading
Further detail about the topics discussed in this
session can be found in section L6 of the
course syllabus.


















