Excretion Urography / Intravenous Urography (IVU)
59
EXCRETION UROGRAPHY By: Sudil Paudyal B.Sc.MIT 2 nd year IOM,MMC 05/25/2022 1
-
Upload
sudil-paudyal -
Category
Health & Medicine
-
view
17.041 -
download
4
description
This ppt aims to deliver a quick info about the common radiological procedure of intravenous urography.
Transcript of Excretion Urography / Intravenous Urography (IVU)

04/11/2023 1
EXCRETION UROGRAPHY
By: Sudil Paudyal
B.Sc.MIT 2nd year
IOM,MMC

04/11/2023 2
Introduction
• Also known as intravenous urography (IVU).
• Most frequently employed radiologic investigation of renal drainage.
• The contrast material is administered intravenously.
• Best method for adults unless use of other methods is specified and is used in examinations of upper urinary tracts of infants and children.

04/11/2023 3
• Urogram: Visualization of kidney parenchyma, calyces and pelvis resulting from IV injection of CM.
• Pyelogram: Describes retrograde studies visualizing only the collecting system.
• So, IVP is misnomer, should be IVU
• Excretion urography used nowadays.

04/11/2023 4
Anatomy
Kidneys:• A pair of bean-shaped organs approximately 12 cm long.
They extend from vertebral level T12 to L3 when the body is in the erect position. The right kidney is positioned slightly lower than the left because of the mass of the liver.
Internal structure• Within the dense, connective tissue of the renal capsule,
the kidney substance is divided into an outer cortex and an inner medulla.

04/11/2023 5
• Cortex-contains glomeruli, Bowman's capsules, and proximal and distal convoluted tubules. It forms renal columns, which extend between medullary pyramids.
• Medulla-consists of 10 to 18 striated pyramids and contains collecting ducts and loops of Henle. The apex of each pyramid ends as a papilla where collecting ducts open.
• Calyces-the minor calyces receive one or more papillae and unite to form major calyces,of which there are two to three per kidney.
• Renal pelvis-the dilated upper portion of the ureter that receives the major calyces.

04/11/2023 6

04/11/2023 7
• Relations:• Anteriorly, a portion of the liver, duodenum and right colonic
flexure lie in front of the right kidney. the left part of the transverse colon, the left colic flexure, and upper part of the descending colon lie in front of the rest of the left kidney.
• Posteriorly, the psoas muscles lie behind each kidney. The upper part of each kidney lies on the inner surface of the respective twelfth rib.

04/11/2023 8
• Superiorly, the adrenal glands are sited on the superior surface of each kidney.
• Inferiorly. Coils of small bowel supported on their mesentery lie below each kidney.
• Medially, vertebral column lies between the two kidneys. Immediately in front of it are the great vessels, the aorta on the right and the inferior vena cava on the left and their associated renal blood supply and drainage.
Blood Supply:• Right and left renal arteries respectively, branches of the
abdominal aorta.Nerve supply:• Motor neurones from the autonomic nervous system.

04/11/2023 9

04/11/2023 10
• The large muscles on either side of the vertebral column cause the longitudinal plane of the kidneys to form a vertical angle of about 20° with the midsagittal plane. These large muscles include the two psoas major muscles. These muscle masses grow larger as they progress inferiorly from the upper lumbar vertebrae.

04/11/2023 11
• This gradual enlargement produces the 20° angle, wherein the upper pole of each kidney is closer to the midline than its lower pole.
• These large posterior abdominal muscles also cause the kidneys to rotate backward within the retroperitoneal space. As a result, the medial border of each kidney is more anterior than the lateral border.

04/11/2023 12
Ureters:
• These are two long tubes leading from the pelvis of each kidney to the bladder, descending on either side of the vertebral column and passing forward over the pelvic brim, to enter obliquely into the posterior base of the bladder.
• Are constructed so that urine passes along them by peristaltic action.
• There is an inner lining of mucous membrane supported on a submucosal layer, then a layer of plain circular involuntary muscle, and an outer layer of white fibrous tissue.
• The ureters have a length of approximately 20 cm and an internal diameter up to 3 mm.

04/11/2023 13
Ureteric constrictions: • The ureters vary in diameter
from 1 mm to almost 1 cm. • Normally, three constricted
points exist along the course of each ureter.
• If a kidney stone attempts to pass from kidney to bladder, it may have trouble passing through these three regions.
• The first point is the ureteropelvic (UP) junction, where the renal pelvis funnels down into the small ureter.

04/11/2023 14
• The second is near the brim of the pelvis, where the iliac blood vessels cross over the ureters.
• The third is where the ureter joins the bladder, termed the ureterovesical junction, or UV junction.
• Most kidney stones that pass down the ureter tend to hang up at the third site, the UV junction, and once the stone passes this point and moves into the bladder, it generally has little trouble passing from the bladder and through the urethra to the exterior.

04/11/2023 15
Bladder:• Bladder is situated in the anterior part of the pelvic cavity,
behind and just above the symphysis pubis.• Exact position depends on the degree of distension.• Acts as a reservoir for urine from the kidneys and
subsequently expels it via the external urethra.
• It is a hollow muscular organ lying in the anterior part of the pelvis outside the peritoneum.
• When empty it is pyramidal in shape and presents an apex behind the smphysis pubis, a base anteriorly and a superior and two inferolateral surfaces.

04/11/2023 16
• The ureters enter the postero lateral angles of the base and the urethra leaves inferiorly at the narrow neck.
• The interior of the bladder is covered with mucous membrane which thrown into folds, except in the trigone between the ureteric orifices, in the contracted state and stretched more smooth when the bladder is distended.

04/11/2023 17
Indications
• To see the anatomy and physiology of urinary system• Trauma• Calculi- renal, ureteric, bladder• Congenital anomalies- ectopic kidney, horseshoe kidney, renal
agenesis• Infective pathology• Renal tumour• Unknown Haematuria• Renal hypertension• Bladder pathology- diverticula, fistula• Vesico ureteric reflux

04/11/2023 18
Contraindications:
• Hypersensitivity to iodinated CM• Renal insufficency• Hepato renal syndrome• Thyrotoxicosis,• Pregnancy, (Allow 28 days from childbirth)

04/11/2023 19
Contrast media:
• Low osmolar contrast media (LOCM)- 300- 600mgI/ml• Adult dose : 50-100ml• Paediatric dose : 1ml/kg

04/11/2023 20
Equipment:
• Any standard radiographic unit is suitable to perform the procedure.
• High power x-ray generator.
• Immobilization band is usually not applied because the resultant pressure may interfere with the passage of fluid through ureters and may also cause distortion of canals.
• However, compression band is sometimes applied over distal ends of ureters to retard flow of opacified urine into bladder and to ensure adequate filling of renal pelves and calyces.

04/11/2023 21

04/11/2023 22
Pt. preparation
• NPO for 5h prior to examination. • Pts. should preferably be ambulant for 2h prior to the
examination to reduce bowel gas.• Bowel preparation is necessary to reduce the bowel gas
pattern which may obscure the region of interest.
• The routine administration of bowel preparation use makes the examination more unpleasant for the patients.
• Nowadays it is said to be unnecessary.

04/11/2023 23
• The technologist must check the patient's chart to determine the creatinine and BUN (blood urea nitrogen) levels. Patients with elevated blood levels have a greater chance of experiencing an adverse contrast media reaction. Normal creatinine levels for the adult are 0.6 to 1.5 mg/dl. BUN levels should range between 8 and 25 mg/100 ml.

04/11/2023 24
• Nowadays, dehydration is not necessary and doesnot improve image quality.
• Dehydration is contraindicated in the following situations:1. Renal failure2. Myeloma 3. Infancy
• If examination is to be performed on a pt who has previously had a severe CM reaction, consideraton should be given to administering methyl prednisolone 32mg orally 12 and 2 h prior to CM injection.

04/11/2023 25
SIGNING INFORMED CONSENT FORM:
• Venipuncture is an invasive procedure that carries risks for complications, especially when contrast media is injected. Before beginning the procedure, the technologist must ensure that the patient is fully aware of these potential risks and has signed an informed consent form.
• If a child is undergoing venipuncture, the procedure should be explained to both the child and the guardian, and the guardian should sign the informed consent form.

04/11/2023 26
Technique
• Venous access via the median antecubital vein is the preferred injection site because flow is retarded in the cephalic vein as it pierces the clavipectoral fascia.
• The gauge of the cannula/needle should allow the injection to be given rapidly as bolus to maximize the density of nephrogram.
• Upper arm or shoulder pain may be due to stasis of contrast in vein which may be relieved by abduction of the arm.

04/11/2023 27
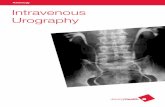
Films • Preliminary film: Supine, full length AP of
abdomen in inspiration. The lower border of
cassette is at the level of symphysis pubis and the x-ray beam is centred in the midline at the level of iliac crests.
To demonstrate bowel preparation, check exposure factor, and location of radiopaque stones or any radiopaque artifacts.

04/11/2023 28
• If necessary the position of overlying opacities may be further demonstrated by:
• Supine AP of renal areas, in expiration. The x-ray beam is centred in the mid-line at the level of lower costal margin
Or
• 35° posterior oblique views, or,
• Tomography of the kidneys at the level of a third of the AP diameter of the patient (app.8-11 cm). The optimal angle of swing is 25-40°.
• The examination should not proceed until these films are reviewed by radiologist and claimed satisfactory.

04/11/2023 29
Films
• Immediate film : AP of the renal areas. This film is exposed 10-
14 s after the injection (app. Arm to kidney time)
Aims to show the nephrogram, i.e renal parenchyma opacified by contrast medium in renal tubules.

04/11/2023 30
• 5-min film: AP of renal areas. To determine if excretion is symmetrical and is invaluable for
assessing the need to modify the techinque, eg a further injection of CM if there has been poor initial opacification.

04/11/2023 31
• Compression band is now applied around the patient’s abdomen and the balloon positioned midway between the ASIS i.e. precisely over the ureters as they cross the pelvic brim. The aim is to produce better pelvicalyceal distension.
• Compression is contraindicated:1. After recent abdominal surgery2. After renal trauma3. If there is a large abdominal mass or aortic aneurysm.4. When the 5-min film shows already distended calyces.

04/11/2023 32
• 15 min film: Supine full length AP There is usually adequate
distension of the pelvicalyceal systems with opaque urine by this time.
Compression is released when satisfactory demonstration of the pelvicalyceal system has been achieved.

04/11/2023 33
• Release film (full bladder) : coned view of bladder area• Taken to show the bladder. If this film is satisfactory, the pt is
asked to empty the bladder.

04/11/2023 34
• After micturition film:• Either a full length abdominal film or a coned view of the
bladder with the tube angled 15° caudad and centred 5 cm above the symphysis pubis based on earlier findings.
• Main aim of films is to Assess bladder emptying To demonstrate return of dilated upper tracts with relief of bladder pressure. Aid diagnosis of VJ calculi Dx of bladder tumors Demonstrate urethral diverticulum. Residual vol of urine.

04/11/2023 35
Additional films:
• Posterior obliques of kidneys, ureters or bladder:
To determine whether the radiopaque shadow is in the ureter or outside.
Position: Pt. is rotated 30-35° in rt or lt side depending on pathology side.

04/11/2023 36
• Prone film: To investigate pelviureteric and ureteric obstruction as the
heavy contrast laden urine will more readily gravitate to the site of the obstruction.
To displace the overlying bowel gas towards periphery. Position: Pt. lies prone after doing 15 min full film and after 4-
5 min. of lying prone (so that lower ureter is dependent part) full film is taken.
• Tomography- when there are confusing overlying gas shadows in renal areas.

04/11/2023 37
• AP with caudal angulation: To separate the over shadows by stomach on left kidney. Position: AP position, film of kidney area with 25° caudal tube
angulation.
• Erect film: To determine where or not there is small ureteric calculus, erect oblique film of area of ureter. To demonstrate layering of calculi in cysts and abscesses.

04/11/2023 38
• Delayed films : may be necessary for up to 24 h after injection to demonstrate the actual site of ureteric obstruction.
• Children: films are taken in 3 min, 15 min, aden post mic after CM injection and further depending upon pathology.
• Pregnancy: film sequence is KUB and 15 min full film.

04/11/2023 39
Modification in case of pathology:
• In case of suspicious shadows in renal areas: Take lateral film of renal area. Take inspiratory and expiratory film of renal area to
demonstrate the relationship of opacities and filling defects of renal tract.
• In case of renal hypertension: take fast sequences (1min, 3 min, and 5 min film).

04/11/2023 40
• Ectopic kidney: full film KUB region from immediate to last film.
• Renal agenesis: full fim KUB from immediate to last film. Delayed films upto 24 hours.
• Bladder diverticulum: Abnormal pouch formed within bladder. Lateral film of bladder area.
• Vesicovaginal fistula: lateral film of bladder area.

04/11/2023 41
• VUJ obstruction: Oblique film of bladder area of obstruction side.
• Suspected renal failure, er urography, inadequate bowel preparation:
High dose IVU (dose of CM upto 600mgI/kg body wt.) is performed.
Common sequences and further delayed sequences ( 1 hrs, 3 hrs, 6 hrs, 12 hrs and 24 hrs) if kidney function is not seen.

04/11/2023 42
Radiation protection
• Direct lead rubber gonad protection using a half apron.• “Pregnancy” rule should be followed.
• If whole of renal tract is to be visualized, no gonad shielding is possible for the females, but for males the testis can be protected by placing a lead rubber sheet over upper thighs below lower edge of symphysis pubis.
• When bladder and lower ureters are not included then female can also be given gonad protection.

04/11/2023 43
Aftercare
• General psychological reassurance.
• Needle wound site dressed and checked for extravasation.
• Check patient understands how to receive the results.
• Ensure patient understands any preparation instructions are finished.
• Escort to changing rooms and bid good-bye.

04/11/2023 44
Advantage/disadvantage
• The strengths of urography are: rapid overview of the entire urinary tract, detailed anatomy of the collecting system,
demonstration of calcifications,
it is sensitive for obstruction, and
low cost,

04/11/2023 45
The weaknesses are that: • it depends on kidney function,
• it provides little assessment of parenchymal structure (eg. cystic vs. solid),
• the perinephric space is not demonstrated,
• it necessitates the use of radiation and contrast medium, and
• it provides no assessment of glomerular filtration rate.

04/11/2023 46
Complication
• Due to CM:Reactions due to CM: mild, moderate and severe.
• Due to technique: • Incorrectly applied abdominal compression may produce
intolerable discomfort or hypotension.• Swelling and pain during injection• Extravasation of CM

04/11/2023 47
Some pathologies
• Urinary obstructions:• Calculi: most commonly form in the kidneys• Ureteral calculi may form in lower portion at VUJ and pelvic
brim.• Bladder calculi are uncommon but they are relatively larger
when present.

04/11/2023 48
Congenital or hereditary diseases:Disorder Description Radiographic findings
Renal agenesis Solitary kidney Hypertrophic single functioning kidney
Supernumerary kidney
More than two kidneys
Hypoplstic 3rd kidney, may or maynot be fused
Malrotation Abnormal position Bizzare appearance of parenchymal calyces and pelvis.
Ectopic kidney Solitary kidney 2nd kidney in another location (pelvis or thorax)

04/11/2023 49
Horse shoe kidney Lower pole- parenchymal fusion
Kidney malrotation and possible nephrogram demonstrating parenchymal fusion
Duplication More than one renal pelvis or ureter
Double renal pelvis in single kidney; two ureters exit kidney and empty into bladder.
Ureterocele Located in distal ureter (VUJ)
Round or oval dilated ureter with radiolucent halo.

04/11/2023 50
Renal agenesis
Ectopic kidney

04/11/2023 51
Ureteric calculus Rotated kidney

04/11/2023 52
Bladder diverticulum
Stag horn calculus

04/11/2023 53
Horse shoe kidney
Duplex bilateral

04/11/2023 54
Polycystic kidney disease:
Polycystic kidney disease is a disorder marked by cysts scattered throughout one or both kidneys. This disease is the most common cause of enlarged kidneys. Its cause may be genetic or congenital, depending on the type of polycystic disease. These cysts alter the appearance of the kidney and may alter renal function.

04/11/2023 55
Additional modalities
Radio nuclide imaging for renal function evaluation. Ultrasound. C.T. for investigation of trauma and renal masses. Renal Angiography. Retrograde pyelography, Urethrography. Magnetic resonance imaging.

04/11/2023 56
Lastly .….
• Contrast is what we give intravenously
• Dye is used on clothes and in cooking to change the color of things—it is not given IV to patients!

04/11/2023 57
Conclusion
• Excretion urography has long been the cornerstone of the imaging evaluation of urinary tract disease. However, other imaging modalities such as USG,CT, and MRI are being used with increasing frequency.
• The declining use of urography in clinical practice presents a challenge for instruction in urographic technique and interpretation.
• In addition, alternative modalities also have their limitations, and despite their increasing use, the ideal “global” urinary tract examination remains controversial.
• Nevertheless, urography may still be important in the diagnosis of some urinary tract disease processes.

04/11/2023 58
References:
• A guide to radiological procedure by stephen chapman, fifth edition
• Clark’s special procedure in radiography
• Dyer et.al., intravenous urography, technique and interpretation, Radiographics,2001; 799-821
• www.xray-2000.co.uk• Various other websites and ppts.

04/11/2023 59Thank you