exam
44
Vivien Puspitasari
description
exam
Transcript of exam
Vivien Puspitasari
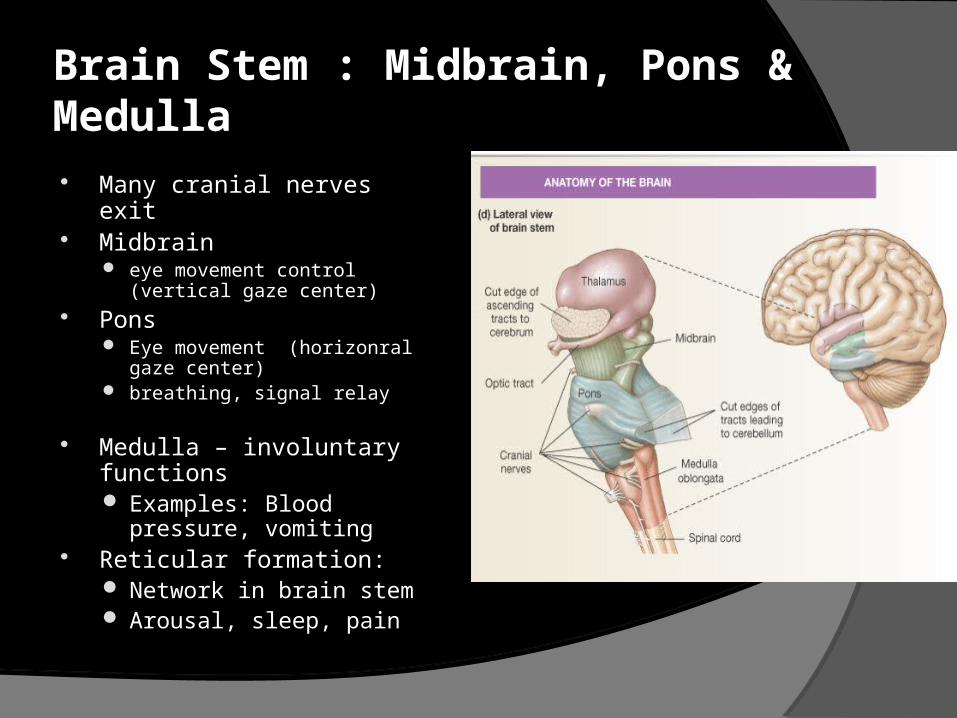
Brain Stem : Midbrain, Pons & Medulla Many cranial nerves exit Midbrain
eye movement control (vertical gaze center)
Pons Eye movement (horizonral
gaze center) breathing, signal relay
Medulla – involuntary functions Examples: Blood pressure,
vomiting Reticular formation:
Network in brain stem Arousal, sleep, pain
CONSCIOUSNESS is a state of awareness of self and the environment.
This state id determinded by two separated function:
Arousal ( level of consciousness) Awareness (content of consciousness)

Consciousness depends on two component :
an intact ascending reticular activating substance (ARAS) in the brainstem as the alerting or awakening element of consciousness → level of consciousness or arousal
a functioning cerebral cortex of both hemisphere which determines the content of that consciousness or awareness
Content depends on arousal but normal arousal does not guarantee normal content

THE ARASextending from the medulla through the pons to the midbrain which is continous caudally with the reticular intermediate grey lamina of the spinal cord and rostrally with the subthalamus, the hypothalamus and the thalamus
Receives input from numerous somatic afferents Projects to midline thalamic nuclei (which are in a circuit with
cortical structures) and the limbic system
Function of ARAS-Thalamic-Cortical system depends on:
Anatomic integrity of structures Metabolic integrity (circulatory integrity) Communicative integrity
(neurotransmitter function) cholineric system monoaminergic system GABA (-aminobutyric acid) system
COMA is…
A state in which the patient makes no purposeful response to the environment and from which subject cannot be aroused
COMA implies dysfunction of : ARAS or Both hemi-cortices
Anatomically, this means Central brainstem structures (bilaterally)
from caudal medulla to rostral midbrain Both hemisphere
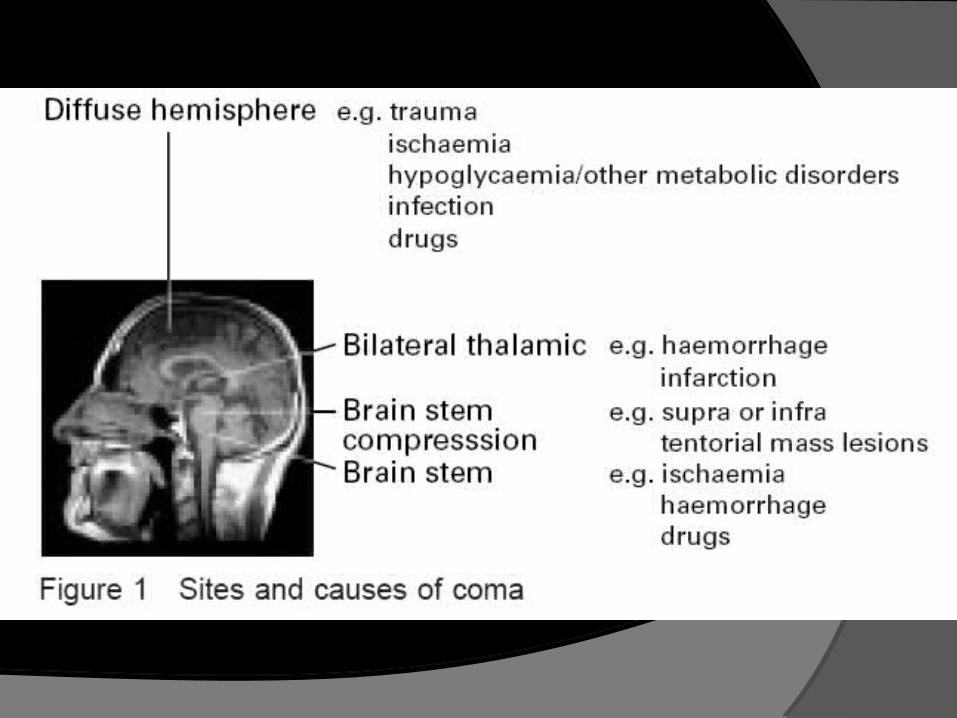
Causes of Coma: Intracranial origin
Head injuries Cerebrovascular accident CNS infection Tumours Increased ICP
Extracranial origin Vascular disorders (shock, hypotension caused by severe
hemorrhage) Metabolic disorders (hypoglicemia, uremia, hepatic coma, electrolite
imbalance) Intoxication (alcohol, barbiturates, narcotics, Carbonminoxide) Miscellaneous (hyperthermia, severe systemic infection)
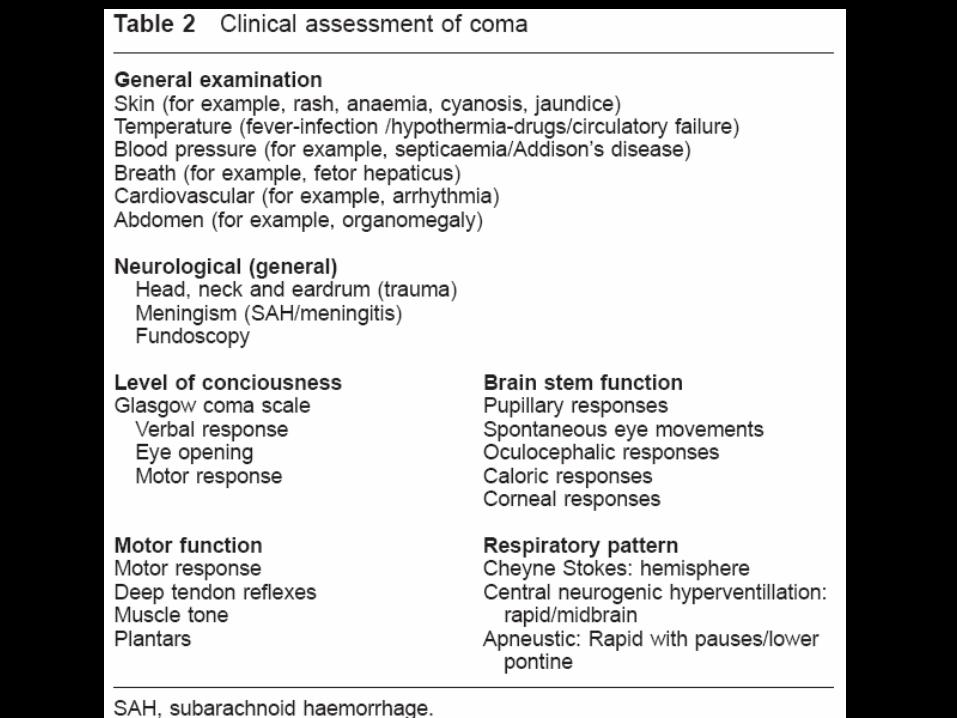
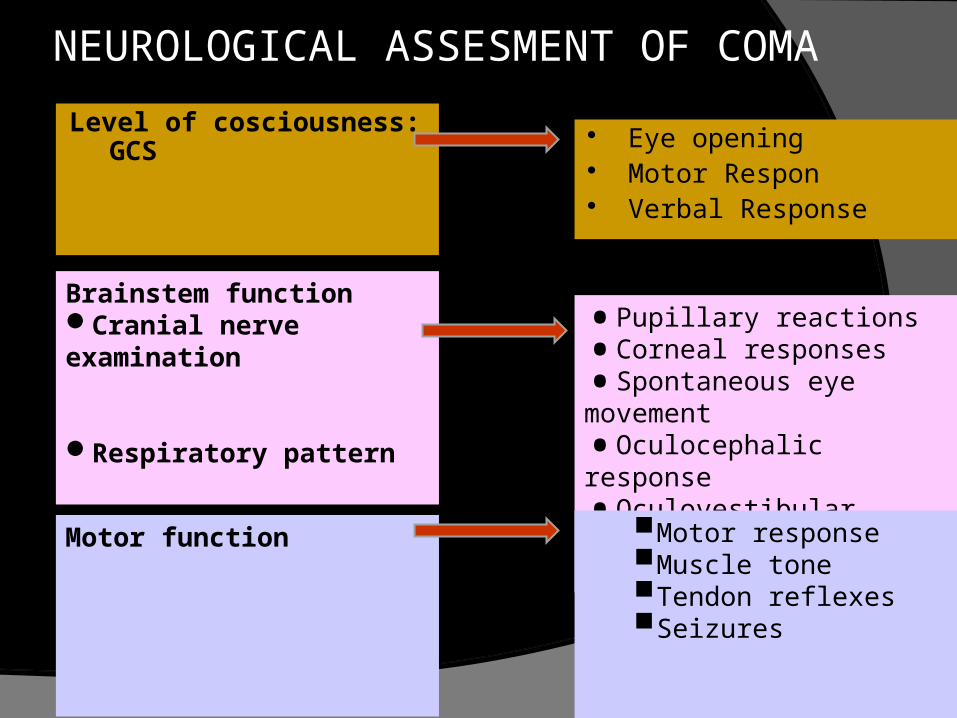
Level of cosciousness: GCS
Brainstem function Cranial nerve examination
Respiratory pattern
Motor function
NEUROLOGICAL ASSESMENT OF COMA
•Pupillary reactions
•Corneal responses
•Spontaneous eye movement
•Oculocephalic response
•Oculovestibular respon
•Gag Reflex
Eye opening Motor Respon Verbal Response
Motor responseMuscle toneTendon reflexesSeizures
Level of consciousness The Glasgow Coma Scale is the most useful
assessment of the level of consciousness The response to command, calling the
patient’s name, and painful stimuli are observed for eye opening, limb movement and voice.
Painful stimuli: supraorbital pressure, sternum pressure, nail bed pressure
Asymmetry between the responses may be importance may evidence for a focal lesion
The brainstem reflexes are particularly important in helping to identify those lesions that may affect the ARAS, explain the reason of coma
BRAINSTEM FUNCTION
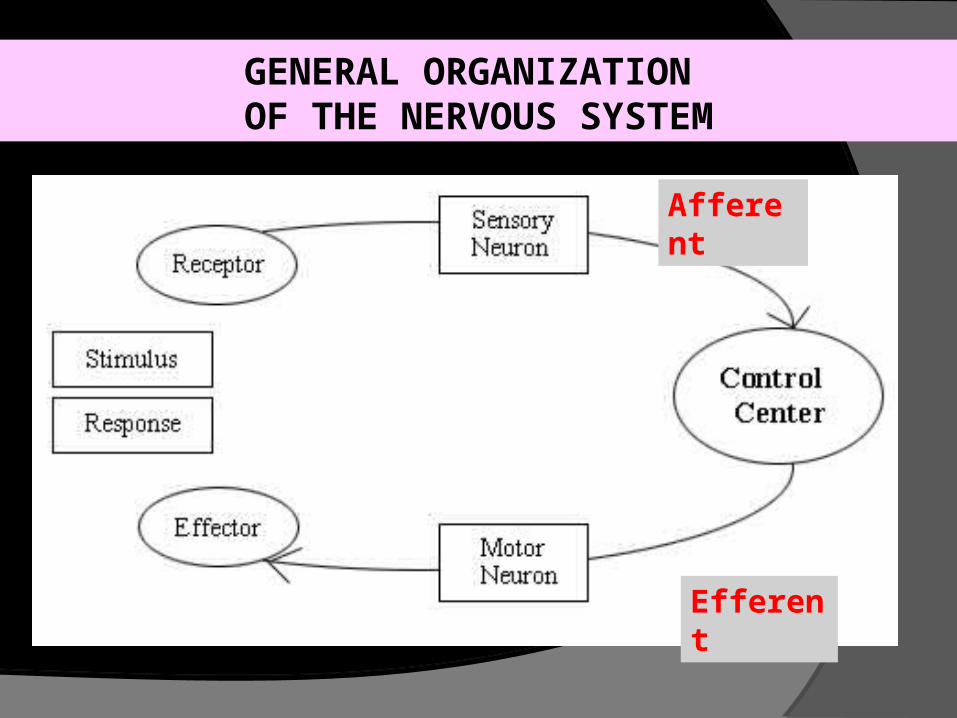
GENERAL ORGANIZATION OF THE NERVOUS SYSTEM
Afferent
Efferent
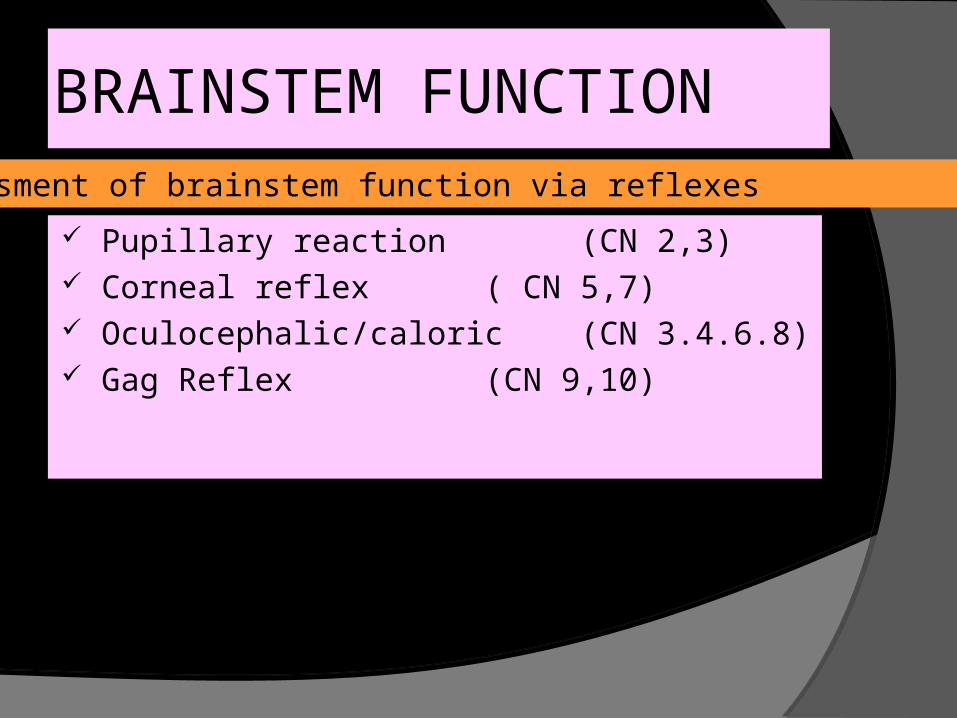
BRAINSTEM FUNCTION
Pupillary reaction (CN 2,3) Corneal reflex ( CN 5,7) Oculocephalic/caloric (CN 3.4.6.8) Gag Reflex (CN 9,10)
Assessment of brainstem function via reflexes
PUPILLARY REACTION
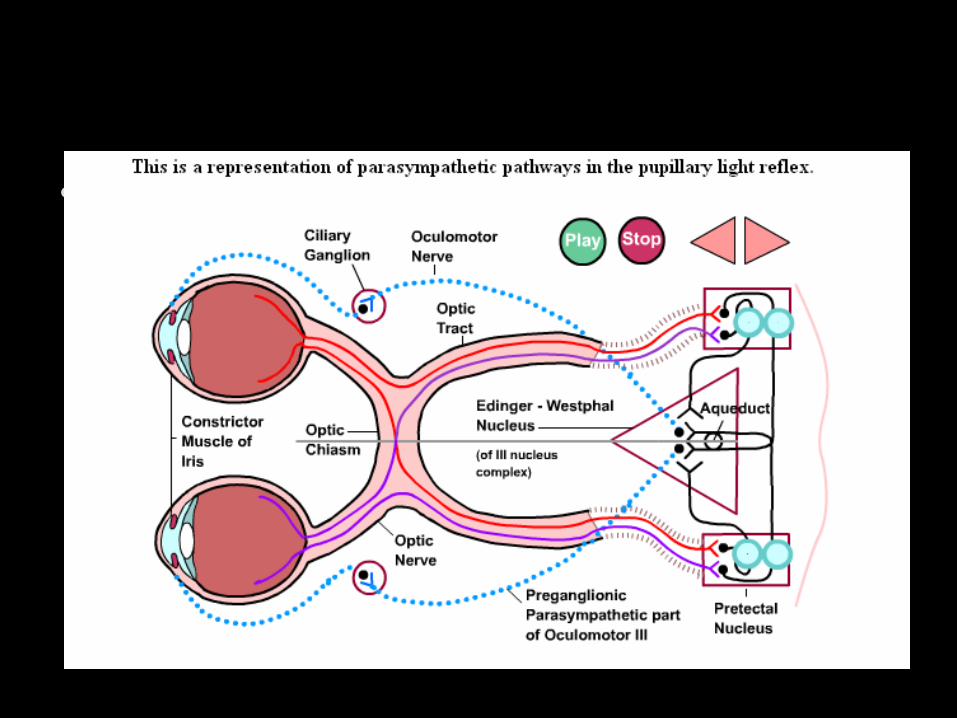
= PUPIL REFLEX / LIGHT REFLEX Pupillary respon to light stimulus Afferent : optic nerve (CN 2) tectum Efferent : parasympathetics via
occulomotor (CN 3) → m. constrictor pupil Abnormal response:
lesion on afferent & efferent pathwaysMidbrain integrity/tectum
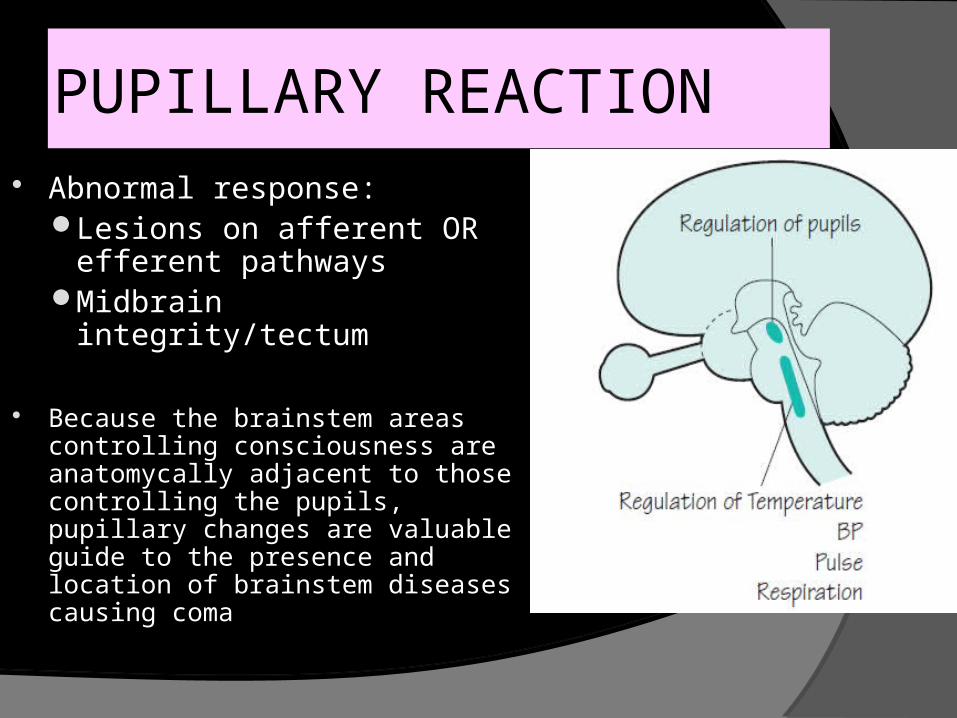
Abnormal response:Lesions on afferent OR
efferent pathwaysMidbrain integrity/tectum
Because the brainstem areas controlling consciousness are anatomycally adjacent to those controlling the pupils, pupillary changes are valuable guide to the presence and location of brainstem diseases causing coma
PUPILLARY REACTION
HOW TO LOOK PUPILLARY REFLEX Have the patient look at a distant object Look at size, shape and symmetry of pupils. Shine a light into each eye and observe
constriction of pupil. Flash a light on one pupil and watch it contract
briskly. Flash the light again and watch the opposite
pupil constrict (consensual reflex). Repeat this procedure on the opposite eye

Gb pupillary reflex
CONCLUSION
Pupillary reflex is one of important thing on the neurology examination
Pupillary reflex is pupillary respon to light stimulus with CN2 as afferent and CN3 as efferent
Abnormal pupil response can represent impairment of afferent or efferent pathway and midbrain integrity
Normal pupils : 3-4 mm in diameter & equal bilaterally, constrict briskly & symmetrically in response to light
Fixed dilated pupils : > 7 mm in diameter and fixed (nonreactive to light) compression of the oculomotor (III) cranial nerve
anywhere along its course from the midbrain to the orbit
Anticholinergic or symphatomimetic drug intoxication
The most common cause : transtentorial herniation of the medial temporal lobe from a supratentorial mass
PUPILLARY REACTION
Pinpoint pupils (1-1,5 mm in diameter)Focal damaged at pontine levelOpioid overdoseOrganophospate poisoningMiotic eye drops
Asymetric pupils (anisocoria) with difference ≥ 1 mmStructural lession affecting the mid brain or
oculomotor nerve
PUPILLARY REACTION

QUESTION
IF YOU FLASH THE LIGHT ON THE RIGHT PUPIL , and: Right pupil did not constrict, and neither left
pupil
THEN YOU FLASH THE LIGHT ON THE LEFT PUPIL, and:Left pupil constrict , and either right pupil
WHERE IS THE LESION ??
ANSWER
DEFECT ON RIGHT AFFERENT PATHWAY (Right Optic nerve)
Gb pupillary reflex
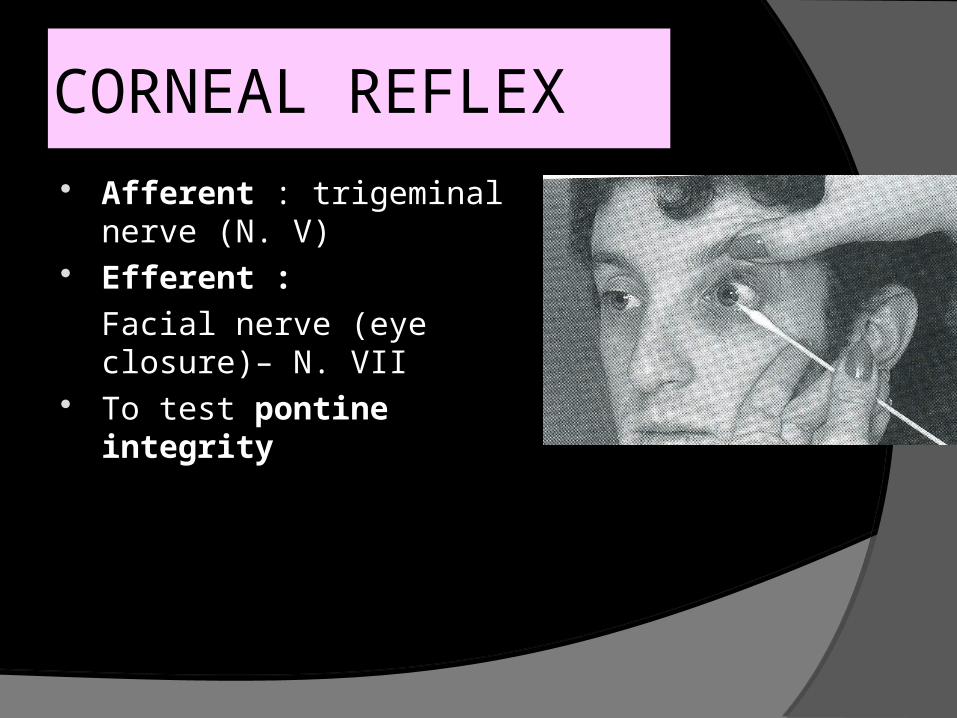
CORNEAL REFLEX Afferent : trigeminal nerve
(N. V) Efferent :
Facial nerve (eye closure)– N. VII
To test pontine integrity
REFLEX EYE MOVEMENT
Oculocephalic reflex = doll’s head maneuver○ stimulating the vestibular system by passive
head rotationOculovestibular reflex = caloric test
○ Stimulus cold/warm water irrigation againts the tympanic membrane
OCULOCEPHALIC RESPONSEWhen the head or body moves
unexpectedly, reflex movements of the head and eye muscles compensate and maintain fixation on the visual target.
This compensatory vestibulo-ocular reflex
Lateral gaze centers : in the paramedian pontine reticular formation (PPRF)
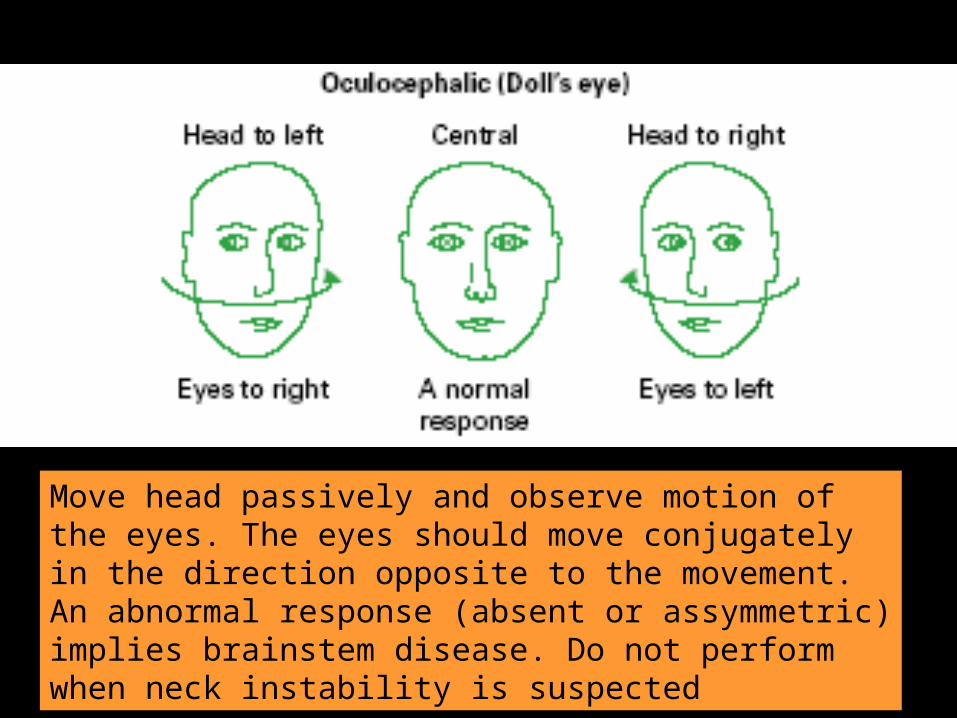
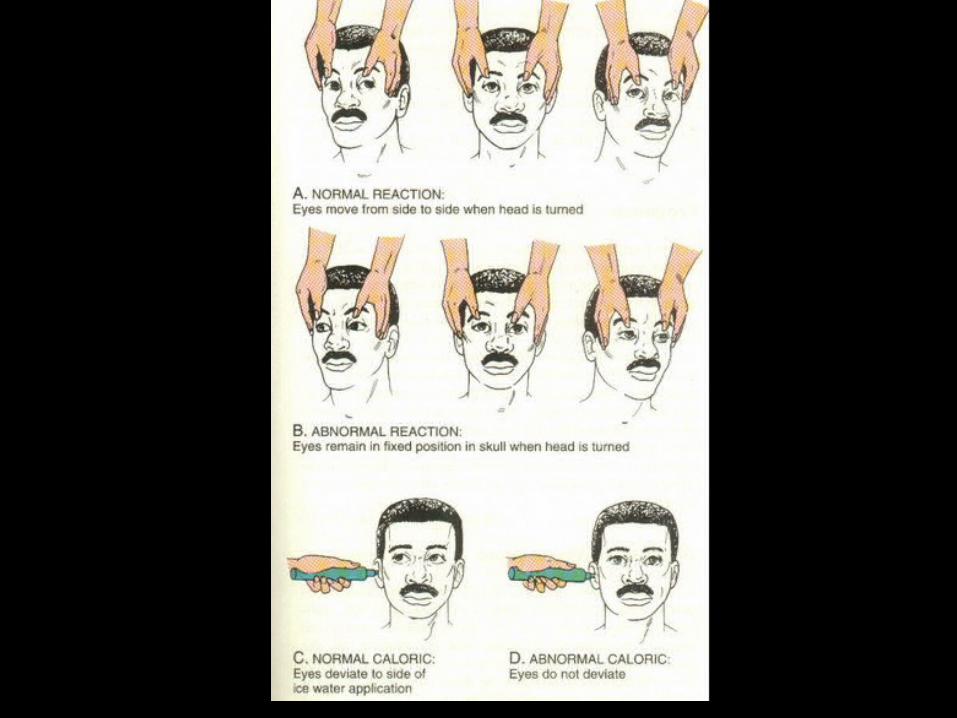
Move head passively and observe motion of the eyes. The eyes should move conjugately in the direction opposite to the movement. An abnormal response (absent or assymmetric) implies brainstem disease. Do not perform when neck instability is suspected
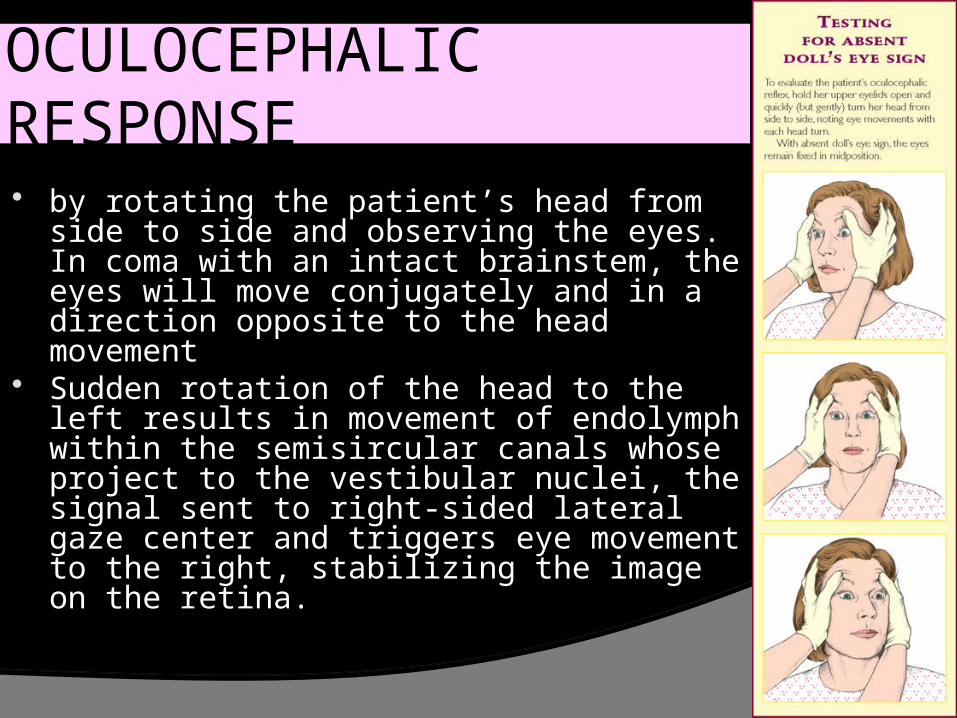
OCULOCEPHALIC RESPONSE by rotating the patient’s head from side to
side and observing the eyes. In coma with an intact brainstem, the eyes will move conjugately and in a direction opposite to the head movement
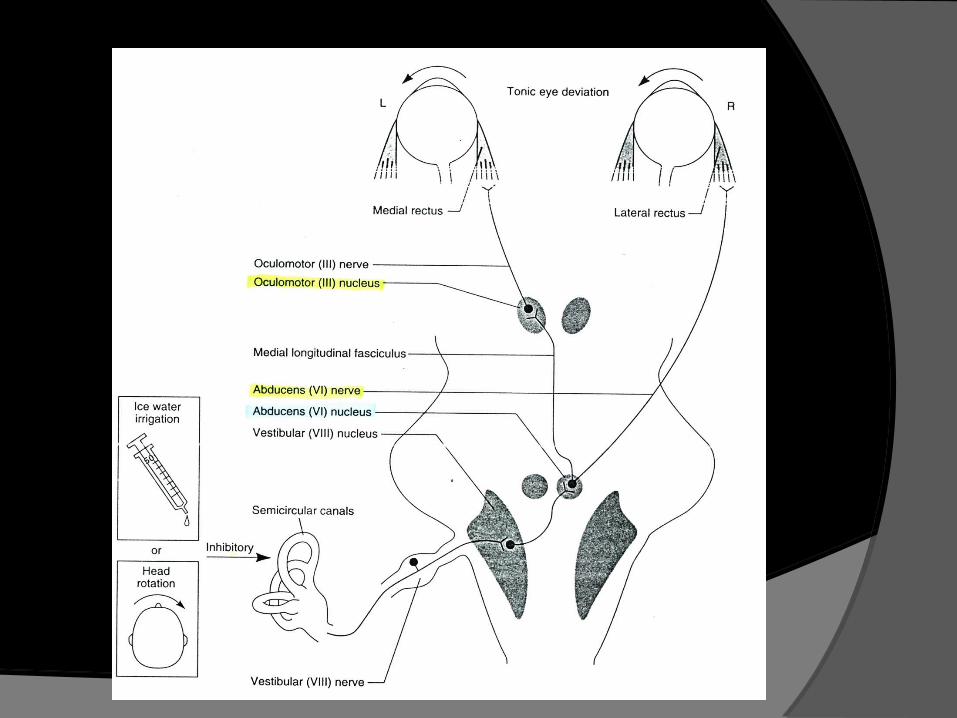
Sudden rotation of the head to the left results in movement of endolymph within the semisircular canals whose project to the vestibular nuclei, the signal sent to right-sided lateral gaze center and triggers eye movement to the right, stabilizing the image on the retina.

CALORIC TEST
by instilling 50-200 ml of ice cold water into the external auditory meatus.
A dysconjugate response or no response indicates braistem damage
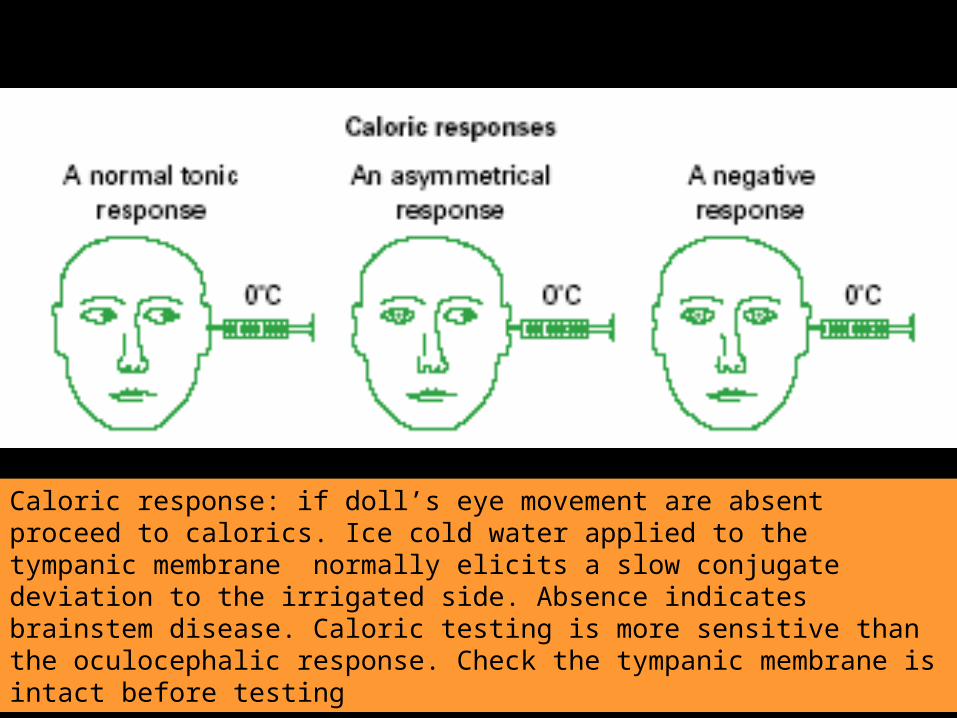
Caloric response: if doll’s eye movement are absent proceed to calorics. Ice cold water applied to the tympanic membrane normally elicits a slow conjugate deviation to the irrigated side. Absence indicates brainstem disease. Caloric testing is more sensitive than the oculocephalic response. Check the tympanic membrane is intact before testing

RESPIRATION Cheyne Stokes Respiration
after bilateral hemispheric dysfunctionRegularly alternating periods of hyperpneu and
apneuFrequently obseved in metabolic coma
Central Neurogenic hyperventilationExtreme hyperventilation diencephalic, midbrain
Cluster BreathingShort-cycle CRS (more irreguler)
Apneustic breathingPauses of several seconds in full inspiration)
Ataxic → irreguler, medullary damage, preterminal
Low pontine damage

MOTOR RESPONSE TO PAIN
Localize the stimulusA decorticate response to pain (flexion of the
arm at the elbow, adduction at the shoulder, extension of the leg and ankle)
A decerebrate response to pain (extension at the elbow, internal rotation at the shoulder & forearm, leg extension)
Asymmetric posturing○ Facial weakness○ Limb weakness

MOTOR RESPONSE TO PAIN

MOTOR RESPONSE TO PAIN

Tone & reflex Plantar response : Babinski
MOTOR RESPONSE TO PAIN
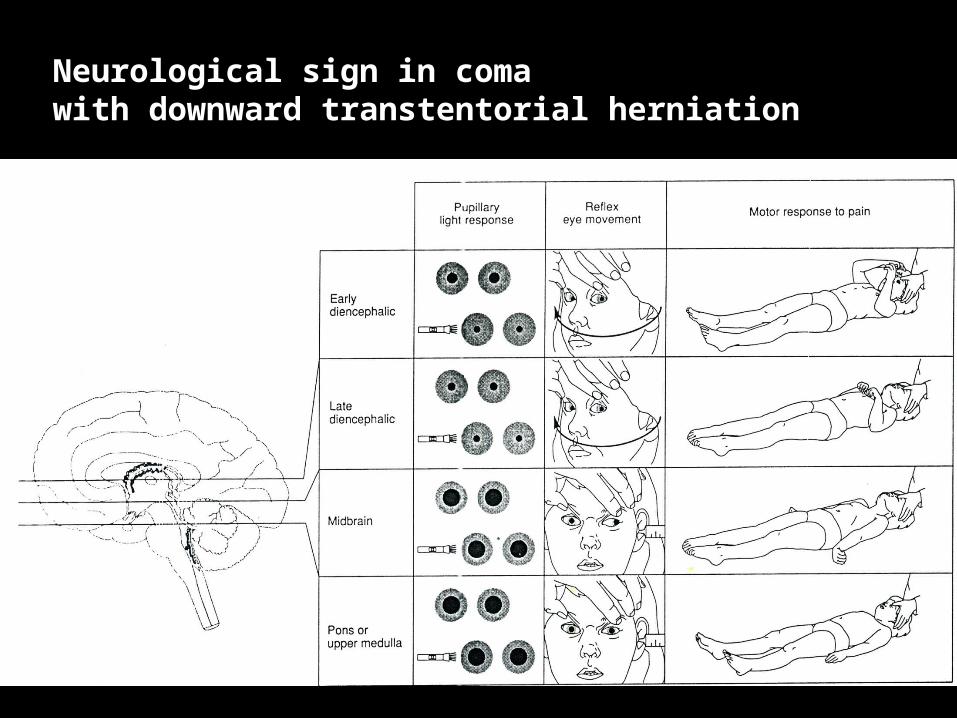
Neurological sign in coma with downward transtentorial herniation