Ex vivo Lung Perfusion: A Platform for Lung Evaluation and ... · Ex vivo Lung Perfusion: A...
183
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair by Jonathan Chi-Wai Yeung A thesis submitted in conformity with the requirements for the degree of Doctor of Philosophy Institute of Medical Science University of Toronto © Copyright by Jonathan Chi-Wai Yeung, 2011
Transcript of Ex vivo Lung Perfusion: A Platform for Lung Evaluation and ... · Ex vivo Lung Perfusion: A...

Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
by
Jonathan Chi-Wai Yeung
A thesis submitted in conformity with the requirements for the degree of Doctor of Philosophy
Institute of Medical Science University of Toronto
© Copyright by Jonathan Chi-Wai Yeung, 2011

ii
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Jonathan C. Yeung
Doctor of Philosophy Institute of Medical Science
University of Toronto 2011
Abstract
Lung transplantation is a life-saving therapy for patients suffering from end-stage lung disease;
however, the majority of donor lungs are injured and attempts to transplant them results in a high risk of
primary graft dysfunction in the recipient, a type of severe acute lung injury. Previously, a novel method
of lung preservation known as ex vivo lung perfusion (EVLP) has been developed in which donor lungs
are continuously perfused and ventilated at normothermia using a protective strategy. Donor lungs have
been shown to tolerate at least 12 h of preservation in this manner without the accrual of injury. Hence,
EVLP could act as a platform on which injured donor lungs could potentially be evaluated and repaired.
To explore this concept, we utilized interleukin-10 (IL-10), an anti-inflammatory cytokine, as a
prototypical drug for ex vivo delivery. Because IL-10 protein has a prolonged half-life during EVLP, we
delivered recombinant IL-10 by the intravascular and intratracheal routes to clinically-rejected injured
human lungs. Intratracheal delivery resulted in elevated levels of IL-10 in both tissue and perfusate
whereas intravascular delivery resulted in elevated levels of IL-10 only in the perfusate over 12 h of
EVLP. There was, however, no beneficial effect to either lung function or lung inflammation. This was
thought to be a result of intratracheally delivered IL-10 leaking out into the perfusate where it may not
be biologically active. Constant IL-10 production within the lung tissue could be achieved using a gene

iii
therapy approach. Thus, we subsequently explored the delivery of IL-10 by adenoviral gene therapy
during EVLP. Ex vivo administered intratracheal adenoviral gene therapy could increase transgene
protein levels within the lung. More importantly, it did so with less vector-associated inflammation
when compared to in vivo delivery of adenoviral gene therapy.
Having explored drug delivery, we sought to develop a large animal injury model on which to
test ex vivo therapies. Given that the majority of organ donors are brain dead and therefore exposed to
the injurious sequelae resulting from brain death, we developed a brain-death injury model in pig. Use
of EVLP as a platform for repair necessitates an accurate recognition of both lung injury and lung
improvement during EVLP. Thus, we utilized this injury model to explore the profile of physiological
parameters when an injured lung is perfused during EVLP. Because of the alteration of the PO2 to
oxygen content relationship of an acellular perfusate, we found that PaO2 changes are less dramatic than
in the in vivo situation. However, as injured lungs begin to become edematous, the mechanical effects
on the lung by the increased water content can be measured by corresponding falls in compliance and
increases in airway pressure.
Overall, use of EVLP demonstrates promise for reducing the organ shortage currently prevalent
in clinical lung transplantation. Improved evaluation will instill confidence in transplant clinicians to
transplant previously questionable organs. Lungs which prove to be injured during evaluation can
potentially be repaired using IL-10 therapy as explored herein or with other therapies using the delivery
methods described.

iv
Acknowledgements
First and foremost, I would like to thank my supervisor, Dr. Shaf Keshavjee, for sharing his
knowledge, support, and encouragement throughout the production of this thesis. I am most fortunate
to have been mentored by such a successful surgeon, scientist, and leader during these past few years.
I am also indebted to my program advisory committee of Dr. Mingyao Liu and Dr. Jim Hu. This
thesis has greatly benefited from their input and I have personally benefited from their example of
running successful research programs.
This project would not have been possible without the help of my colleagues and friends in the
lab. Dirk Wagnetz, Terumoto Koike, and Manyin Chen are talented surgeons who helped with the large
animal transplant surgeries. Matt Rubacha helped with the long, often overnight, perfusion studies.
Paul Chartrand efficiently ran the lab and organized the materials for the experiments. I am also
indebted to Masaaki Sato for his critical review of this thesis and presentation.
I wish to also thank Marcelo Cypel for helping me start up in the lab and for his suggestions over
the years. Along those lines, I wish success to Tiago Machuca and Riccardo Bonato who will continue
the perfusion project.
I gratefully acknowledge the funding sources which made my Ph.D. studies possible. These
include the Department of Surgery at the University of Toronto, the Wyeth Canada/CIHR Rx&D
Fellowship, and the Vanier Canada Graduate Scholarship. I am also fortunate to pursue my residency at
the University of Toronto where the Surgeon-Scientist Program provides the funding and opportunity
to pursue this degree during my residency. Specifically, I would like to thank Dr. Lorne Rotstein and Dr.
Najma Ahmed, the General Surgery Residency Program Directors during my Ph.D. studies, for allowing
me these years in the lab.

v
I dedicate this thesis to my family:
my parents, Ed and Angela
my sister, Stephanie
and my wife, Andrea
for their dedication and support

vi
Table of Contents
Chapter 1 | Introduction 1.1 | Lung Transplantation .................................................................................................................... 1-1
1.1.1 History ...................................................................................................................................... 1-1
1.1.2 Outcomes ................................................................................................................................ 1-2
1.1.3 Organ Shortages ...................................................................................................................... 1-3
1.1.4 Donor Lung Criteria .................................................................................................................. 1-4
1.1.6 Donor Lung Injury .................................................................................................................... 1-5
1.1.5 Strategies to Increase Lung Transplant Volumes ....................................................................... 1-8 1.1.6 Primary Graft Dysfunction ....................................................................................................... 1-16
1.2 | Lung Preservation ....................................................................................................................... 1-19
1.2.1 Procurement Strategy............................................................................................................. 1-20
1.2.2 Normothermic Preservation ................................................................................................... 1-22
1.2.3 Normothermic Preservation for Evaluation ............................................................................. 1-26
1.2.4 Normothermic Preservation for Repair ..................................................................................... 1-31 1.3 | Interleukin-10 ............................................................................................................................ 1-32
1.3.1 Effect of IL-10 on Immunity ..................................................................................................... 1-33
1.3.2 Molecular Signaling of IL-10 .................................................................................................... 1-35
1.3.3 Therapeutic Usages of IL-10 ................................................................................................... 1-36
1.3.4 Delivery of IL-10 to the Lung ................................................................................................... 1-36
1.4 | Adenoviral Gene Therapy ............................................................................................................ 1-37 1.4.1 Adenovirus Biology ................................................................................................................ 1-38
1.4.2 Adenoviral vectors ................................................................................................................. 1-42
1.4.3 Immune Reaction to Adenoviral Vectors ..................................................................................1-45
1.5 | EVLP IL-10 Delivery Strategies ..................................................................................................... 1-52
1.5.1 Aerosol deposition .................................................................................................................. 1-53
1.6 | Summary .................................................................................................................................... 1-55
Chapter 2 | Rationale, Hypothesis, and Objectives
2.1 | Rationale ..................................................................................................................................... 2-1
2.2 | Hypotheses ................................................................................................................................. 2-3
2.3 | Objectives ................................................................................................................................... 2-3
Chapter 3 | Delivery of Recombinant IL-10 to Injured Human Lungs

vii
3.1 | Abstract ....................................................................................................................................... 3-1
3.2 | Introduction ................................................................................................................................ 3-2
3.3 | Materials and Methods ................................................................................................................ 3-4
3.3.1 Design ..................................................................................................................................... 3-4 3.3.2 Human lungs ........................................................................................................................... 3-4
3.3.3 Ex vivo lung perfusion ............................................................................................................. 3-4
3.3.4 Delivery of recombinant IL-10 .................................................................................................. 3-6
3.3.5 Biopsies .................................................................................................................................. 3-7
3.3.6 Homogenization of lung tissue ................................................................................................ 3-7
3.3.7 Inflammatory Profile in Human Lung Tissue Biopsies ............................................................... 3-8 3.3.8 Statistics ................................................................................................................................ 3-8
3.4 | Results ........................................................................................................................................ 3-8
3.4.1 Recombinant IL-10 delivered ex vivo is measurable 12 h after delivery in tissue and perfusate .. 3-9
3.4.3 Distribution of IL-10 within the lung following IT delivery ......................................................... 3-11
3.4.3 Effect of IL-10 on ex vivo lung physiology ............................................................................... 3-12
3.4.5 Effect of IL-10 on cytokine expression ..................................................................................... 3-15 3.5 | Discussion ................................................................................................................................ 3-18
Chapter 4 | Ex Vivo Adenoviral Vector Gene Delivery Results in Decreased Vector-Associated Inflammation Pre- and Post- Lung Transplantation
4.1 | Abstract ....................................................................................................................................... 4-1
4.2 | Introduction ................................................................................................................................ 4-2 4.3 | Materials and Methods ................................................................................................................ 4-3
4.3.1 Animals ................................................................................................................................... 4-3
4.3.2 Porcine Anesthesia ................................................................................................................. 4-4
4.3.3 Lung retrieval .......................................................................................................................... 4-4
4.3.4 Ex vivo lung perfusion ............................................................................................................. 4-5
4.3.5 Pig lung transplantation .......................................................................................................... 4-5 4.3.6 Gene Vector Creation .............................................................................................................. 4-6
4.3.7 Virus Transfection Technique ................................................................................................... 4-7
4.3.8 Biopsies ................................................................................................................................. 4-7
4.3.9 Histopathological Assessment ................................................................................................ 4-7
4.3.10 Green Fluorescent Protein Staining ........................................................................................ 4-8
4.3.11 Homogenization of lung tissue ............................................................................................... 4-9 4.3.12 Inflammatory Profile in Pig Lung Tissue Biopsies .................................................................... 4-9

viii
4.3.13 Statistics ............................................................................................................................. 4-10
4.4 | Results ...................................................................................................................................... 4-10
4.4.1 Intratracheal delivery of adenoviral vectors during EVLP results in transgene expression ........ 4-10
4.4.2 Delivery of an adenoviral vector encoding GFP in vivo results in reduced lung function compared to ex vivo delivery ........................................................................................................................... 4-12
4.4.3 IL-10 expression can reduce vector-associated inflammation in vivo ...................................... 4-13
4.4.4 In vivo delivery of AdGFP results in inflammation on histology ............................................... 4-16
4.4.5 Pro-inflammatory cytokines are increased in viral delivery groups .......................................... 4-18 4.4.5 Absence of vector-associated injury is preserved post-transplantation .................................. 4-20
4.4.6 Transgene expression is preserved post-transplantation ........................................................ 4-21
4.4.7 Pro-inflammatory cytokine expression is reduced in ex vivo transduced groups ..................... 4-21
4.4.8 Histologic inflammation is much higher in in vivo AdGFP group.............................................. 4-22
4.5 | Discussion ................................................................................................................................ 4-24
Chapter 5 | Physiological Characteristics of Ex vivo Lung Perfusion of a Brain Death Injured Lung
5.1 | Abstract ....................................................................................................................................... 5-1
5.2 | Introduction ................................................................................................................................ 5-2
5.3 | Materials and Methods ................................................................................................................ 5-3
5.3.1 Study Design ........................................................................................................................... 5-3
5.3.2 Brain death ............................................................................................................................. 5-4
5.4 | Results ........................................................................................................................................ 5-5 5.4.1 Brain Death Induction .............................................................................................................. 5-5
5.4.2 Physiologic Changes during EVLP ............................................................................................ 5-7
5.4.3 Edema formation during EVLP .................................................................................................. 5-7
5.4.3 Lung Function Following Transplantation ................................................................................. 5-9
5.4.4 Vascular Reactivity to Hypoxic Ventilation during EVLP .......................................................... 5-10
5.5 | Discussion................................................................................................................................. 5-10
Chapter 6 | Exploration of EVLP Physiology and Implications for Lung Evaluation
6.1 | Abstract ....................................................................................................................................... 6-1
6.2 | Introduction ................................................................................................................................ 6-2
6.3 | Materials and Methods ................................................................................................................ 6-6
6.3.1 Ex vivo lung perfusion .............................................................................................................. 6-6
6.3.2 Retrieval of blood..................................................................................................................... 6-6
6.4 | Results ........................................................................................................................................ 6-7

ix
6.4.1 Exploration of V/Q Matching .................................................................................................... 6-7
6.4.2 Exploration of Acellular Perfusion ............................................................................................ 6-9
6.4 | Discussion ................................................................................................................................ 6-12
Chapter 7 | Summary and Future Directions
7.1 | Summary ..................................................................................................................................... 7-1
7.1.1 Paradigm change in lung transplantation ................................................................................. 7-2
7.1.2 Lung evaluation ....................................................................................................................... 7-3
7.1.3 Lung repair .............................................................................................................................. 7-5
7.2 | Conclusion .................................................................................................................................. 7-9
7.3 | Future Directions ....................................................................................................................... 7-10 7.3.1 Exploration of recombinant IL-10 delivery with an animal model ............................................. 7-10
7.3.2 Continuous delivery of intra-tracheal IL-10 ............................................................................. 7-10
7.3.3 IL-10 Protein Engineering ........................................................................................................ 7-11
7.3.4 EVLP Gene Therapy for Lung Repair ......................................................................................... 7-11
7.3.5 Novel Vectors for Gene Therapy ............................................................................................. 7-12
7.3.6 EVLP Lung Evaluation of Other Lung Injury Models ................................................................. 7-12 7.3.7 Evaluation of Improving Lungs ................................................................................................ 7-13
7.3.8 Development of a Small Animal EVLP model ...........................................................................7-14
7.4 | Summary ....................................................................................................................................7-14
Chapter 8 | References

x
List of Figures
Figure 1.1: Kaplan-Meier Survival by Procedure Type Following Lung Transplantation between January 1994 and June 2008. Figure 1.2: Summary of Brain Death Changes Causing Lung Injury.
Figure 1.3: Schema of the Current Paradigm of Lung Transplantation Figure 1.4: Schematic of Ex vivo Lung Perfusion Figure 1.5: Schema of Paradigm of Lung Transplantation with EVLP Evaluation Figure 1.6: Schema of Paradigm of Lung Transplantation with EVLP Repair Figure 1.7: Diagram of Actions of IL-10 on Immune Cells Figure 1.8: Adenovirus Structure Figure 1.9: Schematic of Adenovirus Entry into a Cell Figure 1.10: Shuttle system for generating Adenoviral vectors from E. coli Figure 3.1: Perfusate IL-10 levels Figure 3.2: IL-10 levels in lung tissue Figure 3.3: IL-10 distribution in lung tissue 12h following delivery Figure 3.4: Effect of IL-10 delivery on PO2 at end of EVLP Figure 3.5: Compliance and airway pressures by IL-10 delivery group. Figure 3.6: Tissue cytokine levels after delivery of IL-10. Figure 3.7: Perfusate cytokine levels after delivery of IL-10. All values expressed as pg cytokine/ml. Figure 3.8: Cartoon representation of differences between IL-10 delivered IT via a recombinant protein approach and via a gene therapy approach. Figure 4.1: Expression of GFP transgene in a bronchiole and in alveoli 12h following ex vivo delivery. Figure 4.2: Identification of transduced alveolar macrophage. Figure 4.3: Levels of human IL-10 present in the perfusate following ex vivo AdhIL-10 delivery and levels of human IL-10 present in the plasma following in vivo AdhIL-10 delivery

xi
Figure 4.4: Lung function as measured by P/F ratio following vector delivery Figure 4.5: Physiologic measures following ex vivo vector delivery Figure 4.6: Representative histological sections of Ad transfected lung tissue (H&E stain) Figure 4.7: Quantitative scoring for inflammation post-viral vector delivery Figure 4.8: Inflammation in AdGFP delivered in vivo follows cellular transduction Figure 4.9: Pro-inflammatory cytokine expression in tissue 12h following delivery of vector Figure 4.10: PaO2 post-transplantation Figure 4.11: IL-10 levels in AdhIL-10 recipient plasma Figure 4.12: Cytokine/chemokine levels following transplantation Figure 4.13: Representative histological sections of Ad transfected lung tissue post-transplantation Figure 4.14: Quantitative scoring for inflammation post-transplant Figure 5.1: Confirmation of brain death Figure 5.2: Wet/dry ratio following 12h EVLP Figure 5.3: Changes in PaO2, PVR, Compliance and Airway Pressure during EVLP. Figure 5.4: Lung Function and PA Pressure Following Left Lung Transplantation and Occlusion of Right Pulmonary Artery Figure 5.5: Effect of ventilation with 100% N2 on pulmonary vascular resistance at the onset of EVLP versus following the development of injury at the end of EVLP Figure 6.1: Difference in PO2 to oxygen content curve between acellular Steen solution and blood. Figure 6.2: Differences in predicted PaO2 following shunt from clamping of left main bronchus. Figure 6.3: Changes in P(a-ET)CO2 with changes in perfusion flow. Dotted line signifies EVLP strategy flow rate. Figure 6.4: PO2 at different percentages of cardiac output Figure 6.5: Effect of clamping left main bronchus on PaO2. Figure 6.6: Effect of hematocrit on PaO2 following clamping of left main bronchus.

xii
Figure 7.1: Schema of transplantation in the current era and in the era of ex vivo evaluation and repair.

xiii
List of Tables
Table 1.1: ISHLT Criteria for Lung Acceptance Table 1.2: Maastricht Categories of Donation after Cardiac Death Table 1.3: ISHLT PGD Grading Table 1.4: Composition of Steen Solution Table 2.1: Summary of Previous Work on IL-10 and Ex vivo Lung Perfusion Table 3.1: Ventilation, Heating, and Perfusion Strategy for the First Hour of Perfusion Table 3.2: Characteristics of Injured Human Donor Lungs Table 6.1: Summary of EVLP-Associated Effects on Physiologic Measures of Lung Function

xiv
List of Abbreviations
Ad Adenovirus AdGFP Adenoviral vector encoding GFP AdhIL-10 Adenoviral vector encoding human IL-10 APC Antigen presenting cell ARDS Acute respiratory distress syndrome BAL Broncho-alveolar lavage BOS Bronchiolitis obliterans syndrome CAR Coxsackie adenovirus receptor CVP Central venous pressure CXR Chest radiograph DAB 3,3'-Diaminobenzidine DC Dendritic cell DCD Donation after cardiac death EVLP Ex vivo lung perfusion H&E Hematoxylin and Eosin HDAd Helper-dependent Adenovirus HMGB High mobility group box ICP Intracranial pressure (ICP) IL Interleukin ISHLT International Society for Heart and Lung Transplantation LPD Low potassium dextrose solution LPS Lipopolysaccharide MHC Major histocompatibility complex NK Natural killer cell P/F PaO2 to FiO2 ratio PA Pulmonary artery PAMP Pathogen associated molecular pattern PCR Polymerase Chain Reaction PEEP Positive End-Expiratory Pressure PFU Plaque forming unit PGD Primary graft dysfunction PGE1 Prostaglandin E1 Q Lung perfusion QOL Quality of life RGD Arginine-glycine-aspartic acid rIL-10 Recombinant IL-10 ROS Reactive oxygen species RT-PCR Real time reverse transcriptase polymerase chain reaction SVR Systemic vascular resistance TLR Toll-like receptor TNF Tumour necrosis factor V Lung ventilation VAP Ventilator-associated pneumonia XVIVO Ex vivo lung perfusion

1
Chapter 1
Introduction

1.1 | Lung Transplantation 1-1
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
1.1 | Lung Transplantation
Organ transplantation is one of the major medical achievements of the twentieth century and
spans the fields of science, medicine, surgery, ethics, and law. With this unique therapy, some patients
suffering from otherwise terminal organ failure can be returned to a productive and fruitful life. The first
long-term successes at lung transplantation were achieved around 30 years ago in Toronto by a team led
by Dr. Joel Cooper.1 Today, lung transplantation has matured into a successful therapy for selected
patients with end-stage lung disease. Between 1985 and 2010, more than 26,000 lung transplants have
been performed worldwide on patients suffering from a variety of end-stage lung diseases such as
pulmonary fibrosis, cystic fibrosis, emphysema, pulmonary hypertension, connective tissue disorders,
and rarer diseases such as lymphangioleiomyomatosis and sarcoidosis.2
1.1.1 History
Attempts at lung transplantation occurred as early as 1946 when Demikhov, a Soviet scientist,
attempted a single lung transplantation in a dog but ultimately failed due to bronchial dehiscence.3
Subsequently, Metras, in 1950, reported the first successful dog lung transplant and the first bronchial
artery and left atrial anastamoses.4 In a non-human primate model, Haglin performed lung
reimplantation and showed that these lungs were able to maintain function post-operatively, despite
denervation.5 Finally, on June 11, 1963, Hardy reported the first successful human lung transplant.6
However, the patient died from kidney failure on post-op day 18. The first real long-term survivor
during this early era of lung transplantation was a patient of Derom's in Belgium.7 This patient survived
10.5 months but, unfortunately, was the sole patient to benefit from lung transplantation before 1980.

1.1 | Lung Transplantation 1-2
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
The failure of this early experience in clinical lung transplantation can be summarized by inadequate
immunosuppression and difficulties with the bronchial anastamosis.
A revolution in transplantation occurred in the early 1980s with the advent of cyclosporine.8
The significant improvements in patient survival following liver and kidney transplantation due to
cyclosporine led to a resurgence of interest in heart & lung transplantation in Stanford and lung
transplantation in Toronto.9 Research done by Cooper's group in Toronto showed that corticosteroid
use was a major factor in the weakness of the bronchial anastamosis.10 With the use of cyclosporine,
corticosteroid use could be reduced, leading to improved bronchial anastamoses. In 1986, Cooper
reported the first successful single-lung transplantations for two patients with pulmonary fibrosis.1 His
team went on to perform successful double-lung transplants, first with an en bloc technique somewhat
plagued by airway complications, then with a bilateral sequential transplantation technique which
improved airway healing and had the additional benefit of avoiding cardiopulmonary bypass, if desired.11
The technique remains mostly in use to this day.
1.1.2 Outcomes
While lung transplantation has been shown to confer increased survival to selected patients with
end-stage lung disease, survival following lung transplantation is still only approximately 50% at 5-years.2
The major causes of death following lung transplantation vary with the time following transplantation.
Whereas thirty day mortality is generally related to surgical issues, donor lung preservation, and primary
graft dysfunction (PGD), infectious causes, malignancy and bronchiolitis obliterans syndrome (BOS), a
type of chronic rejection, predominate after the early post-transplant period. Figure 1.1 shows the
current survival curves of lung transplant recipients.

1.1 | Lung Transplantation 1-3
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Figure 1.1: Kaplan-Meier Survival by Procedure Type Following Lung Transplantation between January 1994 and June 2008. Adapted from Christie et al2
However, survival alone is an incomplete measurement of transplant benefit. To patients,
quality of life (QOL) can be as important as quantity of life and lung transplantation can almost be
considered a type of palliative treatment where quality of life is improved even if little or no gain in
quantity of life occurs. Indeed, clinical research is increasingly being devoted to study the QOL benefit
of lung transplantation. Multiple longitudinal studies have recently demonstrated improvements in
QOL following lung transplantation, some as early as 3 months post-transplant.12-14 Longer term studies
into QOL post-transplantation are currently underway.
1.1.3 Organ Shortages
0 1 2 3 4 5 6 7 8 9 10 11 12 130
20
40
60
80
100
Bilateral/Double Lung (N=14 055)
All Lungs (N=24 936)
Half-lives:Double Lung:6.6 yearsSingle Lung: 4.6 yearsAll Lungs: 5.3 years
Single Lung (N=10 869)
Year
Perc
ent s
urvi
val

1.1 | Lung Transplantation 1-4
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
With the success of lung transplantation as a therapy, increasing numbers of patients are being
listed for lung transplantation. Consequently, like all of solid organ transplantation, lung transplantation
is greatly limited by the number of available donor organs. However, unlike most other solid organ
transplants, organ shortages in lung transplantation is compounded by a low utilization rate of offered
donor organs. The United Network for Organ Sharing data reports that lungs were used from only
1,413 of 6,640 deceased donors in 2010 - a utilization of only 21%.15 As a comparison, 6,056 of those
donors were kidney donors. The low utilization rate of lungs results from a combination of stringent
donor criteria and an increased susceptibility of donor lungs to injury. This ultimately translates into
increased wait times and increased waitlist mortality.
1.1.4 Donor Lung Criteria
During the development of lung transplantation, strict criteria for donor suitability based were
defined.16 The current International Society for Heart and Lung Transplantation (ISHLT) criteria
outlining an ideal donor were based upon these criteria and helped establish safe, but conservative,
clinical lung transplantation (Table 1.1).
Table 1.1: ISHLT Criteria for Lung Acceptance. From Orens et al.16
• Age <55 years • ABO compatibility • Clear chest radiograph • PaO2 >300 on FiO2 = 1.0, PEEP 5 cm H2O • Tobacco history <20 pack-years • Absence of chest trauma • No evidence of aspiration/sepsis • No prior cardiopulmonary surgery • Sputum gram stain—absence of organisms • Absence of purulent secretions at bronchoscopy

1.1 | Lung Transplantation 1-5
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
When donor lungs are offered to an institution, blood samples are obtained to check the blood
group and to minimize the risk of donor-transmitted diseases.17 Size of the donor is then considered and
a potential recipient chosen based upon size and blood group. A chest x-ray is taken to exclude gross
parenchymal or pleural abnormalities and a bronchoscopy is performed to exclude gross infection or
anatomical abnormalities. Finally, the gas exchange capacity of the donor lungs is assessed with an
oxygen challenge. At retrieval, the surgeon performs a gross physical evaluation by macroscopic
observation and palpation to assess lung compliance and edema. Palpation is also used to exclude
intrinsic lung disease, areas of contusion, pneumonic infiltrates, or nodules. Observation of the
ventilated lungs during deflation is used to assess pulmonary compliance. As one can see, this evaluation
is mostly clinical and subjective in nature and more lungs could like be safely used. Indeed, if these
criteria are followed, only 20% of donor lungs can be utilized.
1.1.6 Donor Lung Injury
Currently, the largest pool of donor organs today are those retrieved from brain death donors.
In these donors, cessation of neurologic function results in a legal definition of death18, but organs
remain viable owing to preserved cardiac function and ICU support. While this situation is seemingly
ideal for organ transplantation, many factors can contribute to donor lung injury during the process of
donor death. Direct trauma, aspiration, pneumonia, and complications of ICU care such as ventilator-
induced lung injury, atelectasis, oxygen toxicity, and volume overload are all common causes of injury.
More importantly, it is being increasingly recognized that the process of brain death itself can injure
potential donor organs.

1.1 | Lung Transplantation 1-6
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
In the vast majority of cases, donors become brain dead following a rise in intracranial pressure
(ICP) owing to either massive intracranial hemorrhage or head trauma.19 This increased pressure in the
skull leads to cerebral venous engorgement and brain swelling, which further increases ICP. As the
pressure increases, the brain stem is pushed through the foramen magnum, leading to arterial
compression and brain infarction. This results in even more brain swelling and increases ICP to the
point of ceasing intracranial circulation.
The sequential death of each part of the brain stem results in characteristic physiologic
changes.20 Pontine ischemia produces a picture of mixed sympathetic and vagal response and results in
the “Cushing’s response” characterized by hypertension and bradycardia. As ischemia spreads to the
medulla, the vagal nuclei become ischemic and this results in unopposed sympathetic stimulation and
the “catecholamine storm” which results in increases in heart rate, cardiac index, and systemic
vasomotor tone. Finally, progression to complete ischemia of the brain stem results in a falloff in
catecholamine levels and then persistent hypotension.21, 22 This hypotension is multifactorial and
includes factors such as vasomotor centre death causing decreased systemic vascular resistance (SVR),
left heart dysfunction, and hypovolemia from both diabetes insipidus and the lingering effect of diuretics
used for treatment of increased ICP prior to brain death.23
Neurogenic pulmonary edema is a common injury in brain dead donors. While the mechanism
is not completely clear, it is thought that the sudden and profound increase in SVR generated by the
catecholamine storm during brain death leads to a fall in left ventricular output and an increase in left
atrial and pulmonary capillary pressure. This increased pressure can cause injury to the pulmonary

1.1 | Lung Transplantation 1-7
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
epithelium and, as a result, pulmonary edema forms by both hydrostatic and increased permeability
mechanisms.24
Following brain death, a systemic inflammatory response known as a 'cytokine storm' transpires.
Increased pro-inflammatory cytokines have been found in organs following brain death in rodent
models25 and in brain-dead patients26 and lung injury can occur as a result of this systemic inflammation
following brain death. Increased circulating pro-inflammatory cytokines results in the induction of cell
adhesion molecules on pulmonary endothelial and epithelial surfaces27 and leads to the recruitment of
neutrophils and monocytes to the lung causing inflammatory lung injury. de Perrot et al showed that
interleukin(IL)-8 levels in donor lung tissue before and after transplantation increased with time after
reperfusion and that patients who developed severe primary graft dysfunction had significantly higher
IL-8 levels during ischemia and after reperfusion.28, 29 Similarly, Fisher et al studied the levels of IL-8 in
bronchoalveolar lavage(BAL) fluid from 26 donor lungs used for transplantation and showed that a high
concentration of IL-8 in donor BAL was correlated with severe graft dysfunction and with early
postoperative deaths.30 Kaneda et al further studied the role of proinflammatory cytokines by using real-
time reverse transcriptase polymerase chain reaction (RT-PCR) to study the levels of IL-6, IL-1β, IL-8,
IL-10, interferon-γ, and tumor necrosis factor (TNF)-α in the donor lung at the end of cold ischemia
and found that the IL-6/IL-10 ratio was predictive of recipient 30-day mortality.31
A variety of mechanisms for this cytokine storm have been proposed.32 Circulating
inflammatory mediators or neuropeptides could be released from the ischemic brain and induce the
systemic inflammatory response. The catecholamine storm could also induce inflammation either from
(a) shear stress on endothelial cells during the hypertensive crisis, (b) a change to anaerobic

1.1 | Lung Transplantation 1-8
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
metabolism, or (c) transient gut ischemia. Metabolic derangement from the loss of hypothalamic and
pituitary regulation could also be responsible.
Recently, the importance of the vagus nerve in the control of inflammation has been
demonstrated.33 Given that brain death eliminates vagal tone, unopposed inflammation could be a
result. Hoeger et al tested this hypothesis in a rat model of brain death.34 Following the induction of
brain death, vagus nerve stimulation could reduce circulating TNF-α levels and lead to down-regulation
of a variety of pro-inflammatory genes in intestinal tissue. More importantly, vagal stimulation
significantly decreased the expression of E-selectin and IL-1β in renal tissue and, when the kidney was
transplanted, recipients of those grafts had superior early renal function. The innate immune system has
also been implicated in this mechanism. Vagus nerve activity inhibits the release of high mobility group
box-1 (HMGB1), an intranuclear protein, which when released extracellularly, is interpreted as a signal
of tissue damage by the body.35 Toll-like receptors (TLR) are key sensors of tissue damage for the
innate immune system and can be activated by HMGB1.36 In a recent study by Rostron et al, TLR2 and
TLR4 were desensitized in rats prior to the induction of brain death. In these rats, inflammatory
cytokine release following brain death was significantly reduced, strengthening the evidence for an
interactive role between the innate immune system and the vagus nerve in post-brain death
inflammation.37

1.1 | Lung Transplantation 1-9
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Figure 1.2: Summary of Brain Death Changes Causing Lung Injury. Adapted from Avlonitis et al27
1.1.5 Strategies to Increase Lung Transplant Volumes
Hence, organ shortages experienced by solid organ transplant programs world-wide are further
compounded in lung transplantation by a low utilization of offered donor organs. To help alleviate these
shortages, strategies have been developed not only to increase the absolute numbers of organ donors but
also to increase the utilization rate of organ donors.
Improving organ donation rate
The organ donation rate in Canada is approximately 14 per million population, less than half of
Spain or the United States and has remained stable for the past 10 years.38 A recent Canadian Ipsos-Reid
poll found that while 95% of respondents supported organ donation, only 50% have registered to donate
their organs.39 Approximately two-thirds of respondents did not know the organization responsible for
1.1 | Lung Transplantation 1-10
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
organ donation in their province; thus, this gap between attitudes and action may be a result of
confusion regarding the process. Organ donation in Canada is within the purview of the provincial and
territorial governments. This has resulted in a "patchwork" of donor allocation systems and waiting lists
across the country. Owing to the poor and static organ donation rate, the Canadian government has
recently proposed to nationalize aspects of organ donation under Canadian Blood Services, the national
not-for-profit organization managing blood donation. Parliament has proposed the following strategies
to increase organ donation: First, it intends to create a national database of intended donors and
mandate the declaration of whether a member of the public consents to organ donation, usually at the
time of renewal of a driver's license or health card. Currently, only British Columbia and Nova Scotia
maintains databases of intended donors. Second, it is considering mandating required referral and
required request, whereby required referral requires physicians to report all brain deaths and required
request obligates physicians to approach all families of potential organ donors. Only Manitoba currently
practices this approach. Third, professional training in donor recruitment will be offered to health care
professionals to assist in the capture more potential donors, particularly in rural hospitals where organ
donor coordinators may not be stationed. Hopefully, if implemented, these strategies will positively
impact organ donation in the next decade.
Use of Alternate Donor Sources
As an alternative source for lungs, some transplant programs have begun to re-explore the use of
circulation-arrested donors, so called donors after cardiac death (DCD).40,41 Because most patients
succumb as a result of cardiac arrest, the use of DCDs could open a completely new pool of donor
organs of such magnitude that ultimately the entire demand could be met.

1.1 | Lung Transplantation 1-11
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
In the first clinical lung transplantation by Hardy6, a DCD who died from a myocardial
infarction was utilized. At that time, use of DCD was a necessity as the concept of brain death was not
yet legally established. Once brain death had reached the status of general acceptance in the 1970s42, the
majority of organs were harvested from brain-dead donors with intact circulation. Renewed interest in
the potential use of lungs from DCDs followed a series of experiments in dogs by Egan et al in the early
nineties.43, 44 His group demonstrated that lung cells remain viable for a certain period after circulatory
arrest.45, 46 The lung is the sole solid organ that is not dependent on perfusion for aerobic metabolism but
rather uses a mechanism of passive diffusion through the alveoli for substrate delivery. Numerous
experimental studies continued to investigate the possibility of using lungs from DCDs for
transplantation.47, 48
At the First International Workshop on DCDs in Maastricht of the Netherlands in 1995, four
types of donors were identified, so called “Maastricht Categories” (Table 1.2).49 Categories I (dead on
arrival) and II (unsuccessful resuscitation) comprise the uncontrolled donors. Categories III (awaiting
cardiac arrest) and IV (cardiac arrest in brain-dead donor) include the controlled donors. A fifth
category, cardiac arrest in a hospital inpatient, has recently been added.50
Table 1.2: Maastricht Categories of Donation after Cardiac Death50
I Dead on Arrival to Hospital Uncontrolled
II Unsuccessful Resuscitation
III Awaiting Cardiac Arrest Controlled
IV Cardiac Arrest Following Brain Death
V Cardiac Arrest in a Hospital Inpatient Uncontrolled

1.1 | Lung Transplantation 1-12
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Clinically, the first description of the use of lungs from DCD is from Love et al in 1995 (n=3).51
This series, using lungs from category III donors, was updated in 2003 (n=20).52 In 2001, Steen
reported successful lung transplantation using a category II DCD who died in hospital after failed
resuscitation following myocardial infarction.53 In 2004, the Madrid group published results from 2
successful lung transplantations from uncontrolled DCDs (Category I).54 This series has been updated
more recently (n=17).55, 56 Several centers worldwide have now adopted DCD programs in their clinical
routine of lung transplantation and most reported series deal with controlled donation after withdrawal
from life support (Category III).57-60 The total experience with this category now amounts to more than
100 patients worldwide.
The majority of reported series using category III DCDs have comparable results to series of
DBD patients. A recent review of the United States experience using data retrospectively collected from
the UNOS database have shown an overall survival after lung transplantation of 94%, 94%, 94%, 94%,
and 87% at 1, 3, 6, 12, and 24 months, respectively, for recipients receiving lungs from DCD donors,
compared with 92%, 88%, 84%, 78%, and 69%, respectively, from DBD.61
Given the injuries acquired by potential donor lungs during brain death, there are theoretical
advantages with DCD lung utilization. Kang et al recently supported this principle in lungs by
comparing microarray data obtained from DCD and DBD lungs.62 Pre-transplant DCD and DBD lungs
clearly separated on principal component analysis and unsupervised hierarchical clustering. DBD lungs
showed significantly increased inflammatory features when compared to DCD lungs. Furthermore,
pathway analysis demonstrated that DBD lungs had enriched gene sets in the pathways of innate
immunity, intracellular signaling, cytokine interaction, cell communication and apoptosis.

1.1 | Lung Transplantation 1-13
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
The above two strategies have concentrated on increasing the absolute quantity of organ donors.
These subsequent two strategies aim to increase the usage of the current pool of organ donors and can
complement strategies aimed at increasing donor numbers.
Extension of Donor Criteria
While the best transplant outcomes will occur when ideal organs are carefully matched to ideal
recipients, considerations for the shortage of donor organs and the high waitlist morbidity and mortality
must also be made. A common strategy used to increase utilization of donor lungs has been to
transplant “extended criteria” organs; i.e. those organs which fall outside of ISHLT standard criteria but
still felt to be transplantable.63 Indeed, it is estimated that 40% of currently rejected donor lungs could
be safely used if a more detailed and accurate evaluation was available to identify these lungs.64 In order
to maximize the use of donors, many centers, particularly those with more experience, have been using
donors outside of the standard ISHLT criteria.65 Liberalization of donor criteria in these centers
included utilizing lungs from donors with an age >55, smoking history of >20 pack years, >4 days on
ventilator, or positive gram stain on bronchoalveolar lavage (BAL). Contraindications to organ
donation which risked disease transmission from donor to recipient such as sepsis, active extra-central
nervous system malignancy, and positive serology for human immunodeficiency virus remained
unutilized.
This experience using “marginal” or “extended criteria” lungs has now been published showing
mostly equivalent short-term outcomes.66-72 However, each center used different criteria to define the
extended donor which makes comparison difficult. Bronchoscopic and chest radiograph evaluation
remain the most subjective of the ISHLT criteria and it is within these criteria that there is evidence of

1.1 | Lung Transplantation 1-14
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
an increased risk of postoperative death. In 2002, Pierre et al. reported on their experience with 63
extended donors where part of the extended criteria included chest radiographic infiltrates and purulent
secretions on bronchoscopy.71 Within this series, there was a statistically significant higher 30- and 90-
day mortality when compared with recipients of standard criteria donors during the same timeframe.
Indeed, out of the 6 recipient deaths felt to be related to the quality of the donor lung, 3 had purulent
secretions at bronchoscopy and 5 had chest x-ray (CXR) infiltrates. This experience demonstrated that
donor lungs with truly purulent secretions and bilateral infiltrates are clearly at higher risk and should
not be used. Lardinois et al in 2005 showed equivalent 30-day and 1 year survival between recipients of
ideal and marginal lungs.70 However, a subgroup analysis did suggest that lungs with purulent secretions
and a PaO2 < 300 had a negative impact on recipient outcome. Gabbay et al reported on a series where
39 lungs with abnormal CXR and 24 lungs with infection were utilized.68 While they showed equivalent
30 day survival between marginal donors and ideal donors following transplant, infection was defined as
purulent secretions or positive gram stain but the amount of purulent secretions on bronchoscopy was
not reported. They did not transplant lungs with evidence of severe pulmonary infection. Clinical
judgment of the severity of abnormal CXR or bronchoscopy thus remains extremely important in
ensuring good outcomes.
Other factors should also be considered when extended criteria lungs are utilized. In the series
by Gabbay et al, graft ischemic times were found to be predictive of recipient PaO2/FiO2 (P/F) ratio.68
They did not transplant marginal lungs with ischemic times greater than 6 h. The Pierre series showed
that recipients of advanced age or with Burkholderia cepacia colonization had higher organ specific
mortality with the use of extended criteria lungs.71 Sundaresan et al reported a higher need to employ

1.1 | Lung Transplantation 1-15
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
cardiopulmonary bypass to facilitate implantation of the second graft when using extended criteria
lungs.72 This seems to imply that there is some lung dysfunction inherent in the use of such lungs. Thus,
they have suggested that single lung transplants using marginal lungs should occur in emphysema, where
the native lung can continue to contribute to oxygenation versus fibrotic lung disease where the native
lung may not.
Overall, many of the current criteria for an ideal donor do not appear to affect outcome in
multiple series from different centers. For centers with long waiting lists and limited donor pools, there
is a role for the thoughtful use of donor lungs which do not fit the current ISHLT donor criteria.
Improved Donor Management
Prior to organ retrieval and the onset of ischemia, careful and aggressive donor management has
helped increase organ recovery and has been shown to improve lung oxygenation from the time of initial
brain death to the time of organ retrieval.68, 73, 74 Standardized donor management criteria have been
circulated to ICUs around Canada in an attempt to improve organ recovery rates.
The current donor management guidelines are as follows. To avoid aggravating neurogenic
pulmonary edema and to avoid edema from hypervolemia, care to maintain euvolemia during donor
resuscitation is paramount. All potential donors should have central venous pressure (CVP) monitoring
to maintain the CVP between 4 and 10mmHg.75 A pulmonary artery (PA) catheter should also be
considered for wedge pressure measurements when left heart dysfunction is suspected. If needed,
dopamine (<10μg/kg/min) and vasopressin (<2.4 U/h) are the preferred vasopressors as first and
second choice, respectively,76 as norepinephrine and epinephrine have been associated with lung

1.1 | Lung Transplantation 1-16
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
dysfunction.77, 78 Vasopressin infusion has the added benefit of improving hypotension not only due to
its vasopressor action but also due to its antidiuretic hormone action when diabetes insipidus is
present.79-81 It should be titrated to a SVR of 800-1,200dyn·s/cm5 when a pulmonary artery catheter is
present.63
Protective lung ventilation strategies similar to the ARDSnet strategy (Tidal volume = 6-
8mL/kg, positive end-expiratory pressure=5 cm H2O, fractional inspired oxygen <0.5) should be
employed for ventilation of the donor.82 A methylprednisolone bolus at 15mg/kg has been shown to
improve lung function and post-transplant outcomes.74, 83 However, it is currently unclear whether this is
a result of the anti-inflammatory effect or a result of steroid replacement in the setting of ACTH
deficiency post brain death.
Lungs are also particularly susceptible to atelectasis, ventilator associated pneumonia (VAP),
and pneumonia. Frequent turning and suctioning for pulmonary toilet is important. Regular
recruitment maneuvers should be performed to avoid atelectasis. Bronchoscopy for the removal of
mucous plugs and BAL specimens should also be done. Serial chest radiographs should also be obtained
to monitor for the development of any possible infiltrates.63, 68, 76
Angel et al. have recently used retrospective data to show the impact of a standardized donor
management protocol on resuscitating poor quality donors.73 In the four year period following initiation
of their protocol, out of 254 donors initially classified as “poor”, 135 were able to be re-classified as
“extended” or” ideal” at the end of donor management. Ultimately, 21% of donors originally classified as
“poor” were actually used for lung transplantation. In comparison, prior to the initiation of the
standardized donor protocol, only 10% of lungs were used from donors originally classified as “poor”.

1.1 | Lung Transplantation 1-17
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Gabbay et al. have also had success with improving P/F ratio with a donor management strategy.68 Out
of 140 consecutive transplants, 20 donors who originally would have been rejected were able to be used
successfully without impact on 30 day and 3 year survival. Others have also shown increased yield with
aggressive donor management.74, 84, 85
1.1.6 Primary Graft Dysfunction
At the most fundamental level, fear of primary graft dysfunction (PGD) by transplant clinicians
is the cause of the low utilization of donor lungs. PGD can occur when an injured or inflamed lung is
transplanted into a recipient and is a type of acute lung injury which occurs within 72 h of
transplantation.86 It currently affects 11-25% of lung transplant recipients and represents the major
cause of early mortality.87 Clinically, PGD is represented by a severe hypoxemia, lung edema, and diffuse
pulmonary infiltrates on chest X-ray. Pathologically, PGD is represented by diffuse alveolar damage. In
addition to the acute effects of PGD, patients who survive PGD appear to be at higher risk for the
development of chronic graft dysfunction and BOS.88 Thus, prevention of PGD is of utmost concern for
both short and long term outcomes.
The pathogenesis of PGD is multifactorial and can be thought of as representing the summation
of insults to the donor lung sustained prior to transplantation. However, of these insults, ischemia-
reperfusion injury is thought to play the major role in the development of PGD.89 Ischemia-reperfusion
injury affects the transplanted lung by stimulating mechanisms of inflammation and generation of
reactive oxygen species (ROS).89 During ischemia and reperfusion, the entire population of resident
macrophages within the lung is simultaneously activated and subsequently release cytokines and
chemokines in a major and complex pro-inflammatory response.90 This leads to the direct recruitment

1.1 | Lung Transplantation 1-18
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
of neutrophils and leukocytes by chemokine signalling and the indirect recruitment of those cells by the
upregulation of adhesion molecules and the activation of complement pathways. These recipient
neutrophils and T-cells91 propagate the inflammatory response and cause injury to the alveoli.
Concurrently, the strong pro-inflammatory environment can act as strong co-stimulation for the
development of adaptive immune reactions towards the graft, possibly through the release of damage
associated molecular patterns. Thus, development of inflammation appears to follow a biphasic pattern,
with the initial phase caused by macrophage activation and the second phase caused by responding
neutrophils. Animal experiments with macrophage depletion with clodronate or gadolinium have
demonstrated reduced PGD, probably from reduction of the initial phase of macrophage inflammation,
leading to a much lower second phase of responder cell propagation of inflammation.92
Another major cause of lung injury following ischemia is the formation of reactive oxygen
species. During cold storage, anoxia causes ATP degradation which results in the production of
hypoxanthine.89 During ischemia, xanthine dehydrogenase, an enzyme which converts hypoxanthine to
xanthine, is converted to xanthine oxidase. At the time of reperfusion, xanthine oxidase converts
hypoxanthine to xanthine with superoxide, a ROS, as a byproduct. This causes direct injury to
pulmonary epithelium and endothelium thereby damaging the alveolar air-fluid barrier. In addition,
NADPH oxidase on endothelial and neutrophil cells can generate another source of ROS during
reperfusion, adding to the alveolar injury. Clinically, these two mechanisms result in the formation of
alveolar infiltrates and failure of gas exchange seen in the hours following transplantation.
PGD is quite similar to acute lung injury/acute respiratory distress syndrome (ARDS) where
increased permeability of the microvasculature due to inflammation leads to alveolar edema and diffuse

1.2 | Lung Preservation 1-19
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
alveolar damage. Thus, the currently used PGD scoring system is analogous to that for ARDS where
P/F ratios and chest infiltrates are key components and are assessed at timepoints up to 72 h (Table
1.3). This scoring system was validated by demonstrating that patients with grade 3 PGD within 48 h of
transplant had higher short and long term mortalities and longer hospital length-of-stay.
Table 1.3: ISHLT PGD Grading87
Grade P/F ratio Chest x-ray 0 > 300 Normal 1 > 300 Diffuse allograft infiltrates 2 200-300 Diffuse allograft infiltrates 3 < 200 Diffuse allograft infiltrates
In an attempt to better predict patients more susceptible to PGD, many centers have reviewed
their experience retrospectively.93 Unfortunately, due to the limited number of patients at single centers
and the collection of data over different eras of lung transplantation, the data from different studies
conflict. However, age >45, pulmonary arterial hypertension at the time of transplant, and a prolonged
ischemic time increases the risk of PGD in the majority of studies.
Treatment of PGD is supportive and again is similar to the strategy employed for ARDS
patients.94 Low volume ventilation is combined with careful fluid administration in an attempt to reduce
ventilator-induced lung injury and capillary leak. Drug treatments such as inhaled nitric oxide have
either proven to be ineffective or require further trials to test effectiveness. In severe cases,
extracorporeal membrane oxygenation has been utilized as a bridge-to-recovery, but optimal use of this
therapy has yet to be defined.95 Overall, at this point in time, the best treatment for PGD remains
prevention through the careful selection of donor lungs.
1.2 | Lung Preservation

1.2 | Lung Preservation 1-20
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
In the current paradigm of lung transplantation, the decision to utilize an organ for
transplantation is made at the time of donor surgery (Figure 1.2). Once the decision to utilize a donor
lung is made, the lungs must be procured from the donor at which point the obligate ex vivo phase
begins. Most often, the recipient operation will begin in parallel with the decision to utilize the lung,
thus, minimizing injury to the organ during this highly unnatural phase is of utmost concern.
Figure 1.3: Schema of the Current Paradigm of Lung Transplantation
1.2.1 Procurement Strategy
At the time of procurement, many strategies are employed in an attempt to better preserve the
donor lung.17 First, a lung protective strategy for ventilation is utilized during procurement to avoid
further injury from barotrauma and full anticoagulation of the donor (300 U Heparin/kg) is achieved to
minimize the risk of intravascular clot formation.
Once the assessment of the donor is complete, aortic crossclamp of the donor can commence.
This arrests the heart and organ recovery can begin. A dose of 500 μg of prostaglandin E1(PGE1) is
given into the pulmonary artery to lower the pulmonary vascular resistance by dilating the pulmonary
RecipientDonor
Retrieval Transplantation
Cold IschemiaOrgan Retrieval(DECISION POINT)
Reperfusion
Reject
Use
1.2 | Lung Preservation 1-21
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
vasculature. This facilitates the subsequent flushing of the pulmonary vasculature. PGE1 has been found
to also downregulate proinflammatory cytokine expression which may further help to reduce PGD.96
The vasculature of the lung is then flushed to cool the lung tissue and to remove blood from the
pulmonary vasculature, further minimizing the potential for clot formation and allowing for the removal
of demarginated inflammatory and immune cells. Early in the experience of lung transplantation, the
use of an extracellular type (i.e. low potassium) solution was found to be beneficial to lung preservation
as opposed to the intracellular type solution used in other organs.97 Dextran 40 was also found to be a
key ingredient in the lung flush solution and serves two purposes.98 First, it acts as an oncotic agent to
help keep fluid within the intravascular space. Second, it has the ability to reduce the aggregation of
erythrocytes and thrombocytes. This can help preserve flow through the microvasculature after
reperfusion, particularly in the bronchial microcirculation, and may play a role in reducing bronchial
anastamotic complications. Another key ingredient in the flush solution is glucose. Because the lungs
are stored inflated with oxygen, a unique situation arises during storage where the lungs are ischemic but
not hypoxic. Glucose helps support aerobic metabolism in the lung during preservation. This flush
solution is administered anterograde into the pulmonary artery and retrograde into each of the main
pulmonary veins.
Approximately 50-60 ml/kg of perfusate is utilized for anterograde and retrograde flush. The
desired flush pressure is a balance between too high a pressure leading to injury of the pulmonary
vasculature and too low a pressure leading to inhomogeneous flushing. In practice, the flush solution is
hung at 30 cm above the patient and driven by gravity. Use of low potassium dextran-glucose flush
solution (LPD-glucose) has improved post-transplant outcomes. In a retrospective study by Oto et al,

1.2 | Lung Preservation 1-22
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
they showed that recipients of lungs stored with LPD-glucose had lower rates of PGD, days on
ventilator, and 30 day mortality in comparison to other intracellular-type (high potassium) flush
solutions.99
Following the flush, the lungs are removed, inflated at an airway pressure of 20 cm H2O with
50% oxygen and stored on ice. Inflation of the lungs serves two purposes. First, it provides oxygen to
the lung parenchyma for aerobic metabolism and secondly, it preserves the alveolar structure during
storage. Accordingly, van Raemdonck et al have shown that inflation even with nitrogen is still superior
to atelectatic storage.100 An airway pressure of 20cm H2O has been found to be ideal. In the case of
donor lung transport by air, extra care should be taken to not overinflate the lungs as the low
atmospheric pressure in flight, despite pressurized cabins, will result in gas expansion and may cause
barotrauma to the lung during transport.
Once the lungs have been removed from the body, reduction of the metabolic rate by cooling of
the lungs remains the cornerstone strategy for lung preservation today. Kayano et al have shown in a rat
model that the optimal temperature for lung preservation is approximately 10 degrees Celsius.101
However, to simplify transport logistics, 4 degrees Celsius, the temperature of ice, is most commonly
used. Once removed from the body, transplantation into the recipient should occur as soon as possible.
PGD and 30-day mortality have been reported to increase with cold ischemic times longer than 8 h.102
While lungs with 10-12 h cold ischemic times have been transplanted with success, these lungs have
typically had fewer other donor and recipient risk factors.
1.2.2 Normothermic Preservation

1.2 | Lung Preservation 1-23
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
While the current cornerstone of clinical lung preservation has been to limit the metabolic rate
by hypothermia, this strategy best serves lungs meeting ideal acceptance criteria. With the current donor
organ shortage, most programs now utilize increasing numbers of extended criteria organs where lung
function is not as assured as in ideal lungs. Ideally, further evaluation and even reconditioning of the
lungs would be possible during the ex vivo phase of the organ before transplantation into the recipient.
As limitation of the metabolic rate by hypothermic preservation precludes the possibility of meaningful
lung evaluation and recovery, preservation of donor organs would need to occur at normothermic or
near-normothermic conditions to achieve these goals. One such strategy has been that of ex vivo lung
perfusion (EVLP). This strategy attempts to simulate the in vivo situation by ventilation and perfusion
of the donor lung graft. Originally proposed as early as 1938 by Carrel for organs in general and then in
1970 by Jirsch et al for the evaluation and preservation of lungs in cases of distant procurement, attempts
in those eras failed due to an inability to maintain the air/fluid barrier within the lung, leading to the
development of edema and increased PVR in the donor lung during EVLP.103, 104
Driven by the promise of better evaluation of DCD lungs, Steen and colleagues developed a
modern ex vivo perfusion system with the intent to evaluate lung function of this population of lungs ex
vivo.105 In doing so, Steen and colleagues developed a buffered, extracellular solution with an optimal
colloid osmotic pressure to act as the lung perfusate. This solution helps hold fluid within the
intravascular space during perfusion and provides nutrients needed to maintain lung viability. (Table
1.4). As one can see, the composition of Steen is quite similar to the current clinically utilized
preservation solution of LPD-glucose. The major addition is the human albumin which is meant to
maintain a higher oncotic pressure. Steen and colleagues utilized this solution mixed with red blood

1.2 | Lung Preservation 1-24
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
cells in combination with their circuit and were able to successfully perfuse and evaluate lungs in a large
animal model for one hour without the development of pulmonary edema and subsequent successful
transplantation.105 Following work in large animals, Steen's group was first to publish a case report of
successful transplantation of a nonacceptable lung following a brief period of EVLP in 2007.106
Subsequently, Steen's group has published a case series of six cases using short perfusion to evaluate
rejected donor lungs.107
Table 1.4: Composition of Steen Solution
Calcium chloride Magnesium chloride Sodium chloride Potassium chloride Sodium dihydrogen phosphate Glucose Sodium bicarbonate Water Dextran 40 Human serum albumin
The ultimate goal of Steen's studies has been to utilize EVLP as a method for lung evaluation
and thus the perfusion times have been short. For the applications of EVLP for preservation, improved
evaluation, and future goals of lung repair, much more time is required. Erasmus et al first attempted to
extend the EVLP duration to 6 h; however, circuit induced injury again became problematic with
increased PVR and airway pressures in the lung near the end of 6 h.108 Successful long-term (12 h)
perfusion was first described by Cypel et al using a lung protective strategy for perfusion and
ventilation.109

1.2 | Lung Preservation 1-25
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
To attain stable 12 h perfusion, several key lung protective strategies were employed by Cypel et
al.109 First, an acellular perfusate was utilized. They hypothesized that oxygen supply to the lung could
occur via the ventilator rather than via the vasculature. This concept has been shown by Egan's group,
where mere ventilation of a donor lung with room air at normothermia preserves cell viability for 24 h.45,
46 In addition, acellular perfusion is logistically simpler for clinical use and also avoids the problem of
limited lifespan of a red blood cell within the harsh environment of the perfusion circuit. Second, rather
than subject the lungs to perfusion at 100% of cardiac output, maximal flow was limited to 40%. This
lower flow aids in the reduction of hydrostatic edema caused by perfusion and, despite lower flows to
non-dependent areas of the lung, histology and post-transplant function in EVLP lungs were shown to
be normal. Third, they found that maintenance of a positive left atrial pressure of 3-5mmHg to be vital
for the success of long term perfusion. This small, but positive LA pressure tents open the distal veins
and prevents collapse of the veins from occurring during decreases of flow at inspiration.110 Absence of
positive LA pressures can lead to unstable alveolar geometry and results in decreased lung compliance.111
Finally, they expounded the importance of using a centrifugal pump. With ventilation, distension of the
alveoli will place pressure upon the peri-alveolar vessels leading to cyclical increases in PVR with every
breath. As a consequence of how a centrifugal pump functions, increased afterload to the pump will
result in decreased rotation and flow. Thus, the pump will back off during times of increased resistance
rather than force fluid through potentially causing injury or edema. During perfusion, oxygen is
removed and carbon dioxide is supplied via a membrane oxygenator as a simulation of cellular
metabolism (Figure 1.3). Removal of oxygen allows for the measure of lung function by taking the
difference between post-lung and pre-lung PaO2 and addition of carbon dioxide helps maintain the pH
of the perfusate.

1.2 | Lung Preservation 1-26
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Figure 1.4: Schematic of Ex vivo Lung Perfusion
Using this strategy, safe 12 h-perfusion has been demonstrated in porcine and human lungs and
this strategy of EVLP has been shown to interrupt ischemic damage caused by prolonged cold
ischemia.109, 112, 113 In a clinical trial using this strategy of EVLP for 4-6 h in extended criteria lungs,
equivalent outcomes in lungs evaluated and accepted based on EVLP criteria were found compared to
contemporary controls.114
1.2.3 Normothermic Preservation for Evaluation
Current lung evaluation is a clinical process greatly dependent on the judgment of the surgeon.
While some evaluation does occur prior to retrieval, i.e. chest x-rays and ICU bronchoscopy, the
majority of the evaluation leading to the decision of utilization occurs at one timepoint: organ retrieval.
Lungs which may be injured but have not yet had time to express that injury in the form of edema and
lower P/F ratios may still be utilized, inadvertently. Furthermore, donor physiology during retrieval

1.2 | Lung Preservation 1-27
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
may not be entirely conducive to accurate lung evaluation as blood pressure is often labile and under-
recruitment of the lung parenchyma may give falsely low PaO2.
Physiologic Evaluation
Ex vivo lung perfusion allows for the potential of lung evaluation over time, at a controlled
perfusion flow and ventilation strategy. More importantly, the decision to utilize the organ can be
delayed until ex vivo assessment at the recipient hospital, drastically improving decision-making (Figure
1.4). However, a better understanding of the physiology during EVLP as it applies to evaluation is
needed. One major variable in the clinical evaluation of lungs is PaO2. The ventilation/perfusion ratio is
an important determinant of this value as air must interact with fluid to achieve oxygen exchange.115 In
humans, the normal pulmonary ventilation (V) to pulmonary blood flow (Q) ratio is typically around
0.8 with a normal minute ventilation being around 4.2L/min and the normal perfusion rate being
around 5.5L/min. However, the overall V/Q ratio is only one factor. The overall V must be able to
interact with the overall Q in order to be effective, and this interaction brings about the concept of V/Q
matching. For example, in an extreme case, if all of the ventilation was to enter the left lung and all of the
perfusion was to enter the right lung, the overall V/Q would still be 0.8; however, as air is not able to
exchange with the perfusion fluid, there is no gas exchange, and the PaO2 would be equivalent to the
mixed venous PO2. This is an example of complete V/Q mismatch and illustrates the importance of
V/Q matching to PaO2.

1.2 | Lung Preservation 1-28
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Figure 1.5: Schema of Paradigm of Lung Transplantation with EVLP Evaluation
In the normal upright human, there is a physiologic V/Q mismatch across the normal lung.
Both ventilation and perfusion decline from the bases to the apices of the lung. For ventilation, the
transpleural pressure at the apex is more negative than the transpleural pressure at the base. Hence, the
lung tissue is less expanded at the base, and thus more compliant. Thus, when air begins to enter the
lung, it preferentially enters the base of the lung first and therefore more ventilation occurs in the base.
The effect of gravity of the distribution of blood flow to the lung can be explained by the hydrostatic
pressure difference between the top and bottom of the pulmonary arterial system. The level at the top of
the lungs is higher than the level of the heart. Hence, the PA pressure is relatively low in these areas and
alveolar pressure can exceed PA pressure leading to collapse of these vessels during ventilation and the
development of V>Q areas. In the middle zone, PA pressure exceeds alveolar pressure and in the lower
zone, PA and PV pressures exceed alveolar pressure. First described by West, these regions are known as
West Zones 1, 2, and 3, respectively.115 Thus, there is a physiological mismatch where the apex of the
lung is slightly V>Q with a concomitant area at the base which is V<Q. Since, by definition, more blood
will go to areas of V<Q, the net effect of V/Q mismatching (some areas V<Q and some areas V>Q) is

1.2 | Lung Preservation 1-29
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
that PaO2 will fall because the amount of hyperoxic blood coming from V>Q areas cannot correct for the
amount of relatively hypoxic blood coming from V<Q areas. This is particularly important when
pathological conditions arise in the lung. Common donor pathologies such as pneumonia, edema, and
aspiration all flood the alveoli leading to increased areas of V<Q. Consequently, V/Q mismatching
increases leading to a fall in PaO2. Indeed, ICU physicians increase PEEP in patients with these
conditions in order to reinflate the affected lung units and attempt to reduce V/Q mismatch.
Unique to the EVLP system is the drop in the overall Q relative to the overall V due to the lung
protective strategy of perfusion with 40% estimated cardiac output is employed. So while the
gravitational factors governing the physiologic V/Q mismatch are unchanged, the lowering of the overall
Q will affect how the lung oxygenates the blood. Since less than half of the normal flow is entering the
lung, the consequent PA pressure will be lower and thus one would expect that alveolar pressure will
exceed PA pressure in a larger proportion of the lung. In other words, West zone 1 will increase and
areas of V>Q will be increased with no concomitant increase in areas of V<Q. As the ratio of V>Q
approaches infinity, dissolved partial pressures of gas in the blood or perfusate leaving these lung alveolar
units approaches that of alveolar gas, hence an increased PO2 and decreased PCO2 results. Since edema,
pneumonia, or aspiration increases V/Q mismatching, it is currently unclear what the effect will be on
this altered physiology. As part of this thesis, we will explore the effect of increasing edema on PaO2
during EVLP.
Molecular evaluation
The extra time afforded by EVLP preservation may open the door for novel means of lung
evaluation. With improvements in the understanding of donor lung biology and immunology and

1.2 | Lung Preservation 1-30
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
concomitant advances in technology, attempts to combine clinical evaluation of lungs with more
objective molecular markers are taking place. High levels of inflammatory mediators at the time of
reperfusion can predispose the lung to ischemia-reperfusion injury.89 With current knowledge of lung
biology, the examination of cytokines has been a logical first step in looking for predictive markers of
donor lung function. However, the biology of lung transplantation is not completely understood and
other predictive markers may exist in pathways not currently thought to be involved in graft failure or in
completely novel pathways. Thus, two studies have used gene chip technology and pathway analysis in
an attempt to find novel markers of graft failure. Ray et al. compared the expression profile of genes in
PGD lungs and non-PGD lungs.116 A resulting 23 upregulated and 42 downregulated genes were
identified but only 13 and 11 transcripts were found to be focus genes on pathway analysis, respectively,
suggesting that many of these differentially expressed transcripts had no, as yet, known function. Anraku
et al. furthered the use of gene chips in donor lung evaluation by identifying 4 significantly upregulated
genes in PGD vs non-PGD patients and then verified their predictive ability in a test set of 81 patients.117
To take advantage of these identified genes for lung evaluation, a clinically relevant test needs to be
developed. We envision the use of this test pre- and post- EVLP to help with the clinical decision of lung
utilization. Currently, use of gene markers in the context of transplantation is challenging because of the
timeframes involved. For a test to be useful clinically, measurement of gene markers in donor lungs
needs to occur as quickly as possible, at most <2 h, in order for the clinician to decide on lung utilization
without unnecessary prolongation of cold ischemic time. Given that the best technology today requires
at least 4 h just for RNA extraction from a lung biopsy, further advances in RNA processing will need to
occur before clinical tests become a reality.

1.2 | Lung Preservation 1-31
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
1.2.4 Normothermic Preservation for Repair
The potential for repair of injured donor lungs is greatly increased with the development of safe
prolonged normothermic perfusion of lungs. Given that a large number of potential donor lungs are
injured by a variety of mechanisms including brain death, contusion, aspiration, infection, edema, and
atelectasis, one could imagine that targeted therapies for each of these injuries could be delivered ex vivo
for repair (Figure 1.5). Success would revolutionize clinical lung transplantation by greatly increasing
the donor lung pool. Consequently, strategies for direct intervention of common mechanisms of lung
injury are currently being investigated by groups around the world.
Brain dead donors remain the largest group of organ donors currently used but can be
accompanied by the aforementioned neurogenic edema and pro-inflammatory milieu.27 Possible
pharmaceutical interventions include use of high osmotic perfusates and β-adrenergic drugs to
accelerate removal of lung edema. Steen et al have shown limited data supporting this hypothesis in
lungs. In a series of 6 lungs, edema may have reduced by some amount following EVLP using Steen
solution.107 Moreover, alveolar fluid clearance has been shown to be increased simply by ventilation and
perfusion of a lung.118 When the β-adrenergic drug Terbutaline was administered to ex vivo perfused
human lungs, further increases in alveolar fluid clearance resulted.
Other early studies into the use of EVLP for lung repair have been reported, some still only in
abstract form. In a porcine model of brain death, Wipper et al showed that EVLP of 6 h potentially
reconditioned brain-death induced injury with reversal of histologic injury and clinical dysfunction.119
Another common mechanism of injury is aspiration. Inci et al have attempted to improve porcine lungs
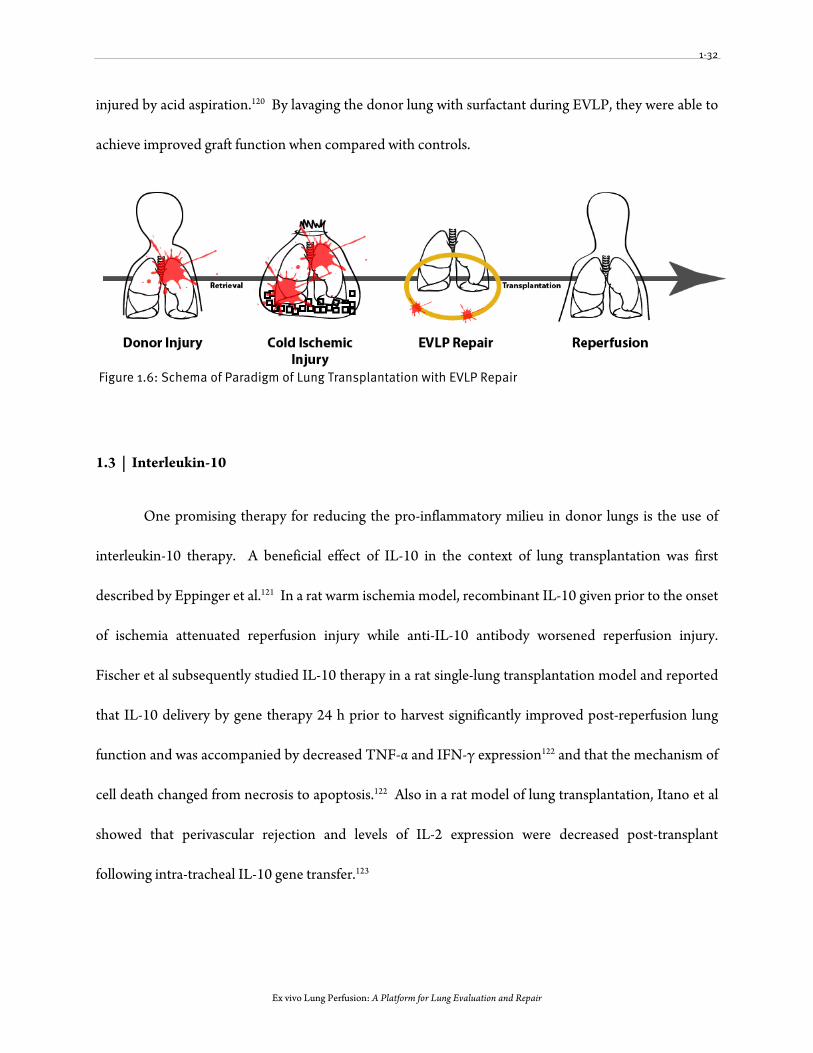
1-32
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
injured by acid aspiration.120 By lavaging the donor lung with surfactant during EVLP, they were able to
achieve improved graft function when compared with controls.
Figure 1.6: Schema of Paradigm of Lung Transplantation with EVLP Repair
1.3 | Interleukin-10
One promising therapy for reducing the pro-inflammatory milieu in donor lungs is the use of
interleukin-10 therapy. A beneficial effect of IL-10 in the context of lung transplantation was first
described by Eppinger et al.121 In a rat warm ischemia model, recombinant IL-10 given prior to the onset
of ischemia attenuated reperfusion injury while anti-IL-10 antibody worsened reperfusion injury.
Fischer et al subsequently studied IL-10 therapy in a rat single-lung transplantation model and reported
that IL-10 delivery by gene therapy 24 h prior to harvest significantly improved post-reperfusion lung
function and was accompanied by decreased TNF-α and IFN-γ expression122 and that the mechanism of
cell death changed from necrosis to apoptosis.122 Also in a rat model of lung transplantation, Itano et al
showed that perivascular rejection and levels of IL-2 expression were decreased post-transplant
following intra-tracheal IL-10 gene transfer.123

1.3 | Interleukin-10 1-33
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
IL-10 is a pleiotropic cytokine produced by activated T cells, B cells, monocytes, macrophages,
and mast cells. Originally recognized as a cytokine synthesis inhibitory factor due to its ability to
suppress macrophages, IL-10 is now known to modulate complex inflammatory and immune
processes.124
1.3.1 Effect of IL-10 on Immunity
The effects of IL-10 on immunity have been studied in a variety of infectious models in mice. In
mouse models of Toxoplasma gondii125 and Leishmania major126 infection, the relative levels of IL-10 and
IFN-γ produced by Th1 cells affects the balance between clearance and chronic infection. Low levels of
IL-10 allows for the clearance of these infections, but high levels of IL-10 over-impairs the immune
response, leading to a chronically infected state. Similarly in the lung, influenza is a common infection
where most victims are able to clear the virus effectively; however, a minority of patients die from
seemingly similar infections due to a massive inflammatory response against the virus. Indeed, IL-10
again appears to also play a role in this dichotomy. Following influenza infection, virus specific T-
effector cells produce large amounts of IL-10 within the lung which essentially acts as a negative-
feedback mechanism for the immune response. Blockage of IL-10 release leads to an uncontrolled and
lethal immune reaction to the virus and the variation in the lethality of influenza may be a result of
differences in IL-10 production within individuals of the population.127 Therefore, IL-10 appears to play
a central role in balancing pathology and protection from the immune system.
Though first isolated from mouse Th2 cells as a factor which limited cytokine production from
Th1 cells128, it is now clear that IL-10 is a broadly expressed cytokine and can be produced by Th1, Th2,
Th17, Treg, CD8+ and B cells of the adaptive immune system and dendritic cells (DC), macrophages,

1.3 | Interleukin-10 1-34
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
mast cells, natural killer (NK) cells, eosinophils, and neutrophils of the innate immune system.124 The
major role for IL-10 is as an immunosuppressive cytokine with anti-inflammatory properties, particularly
in the inhibition of macrophage and DC function.129 When these cells are stimulated by IL-10,
production of pro-inflammatory cytokines, expression of co-stimulation molecules, major
histocompatibility complex (MHC) class II molecules, and antigen presentation is impeded, leading to
impaired maturation and can even render these cells tolerogenic.130, 131
IL-10 can also impair adaptive immune responses. IL-10 directly inhibits proliferation and
cytokine production in naïve CD4+ T cells and can inhibit both Th1- and Th2- type responses.132, 133
However, previously activated and memory T-cells seem to be unresponsive to IL-10.134 More excitingly
for transplantation, IL-10 may mature naïve T-cells into a type of regulatory T-cell (Tr1) that produces
high levels of IL-10 and can suppress antigen-specific responses in vivo.135 (Figure 1.6)
However, IL-10 can also stimulate selected immune responses. IL-10 is a strong stimulator of
the cytotoxic responses of natural killer cells.136 NK cells pre-treated with IL-10 can lyse tumor cells
more effectively than unstimulated cells137 and in patients with graft-vs-host disease following bone
marrow transplant, high serum IL-10 levels is predictive of poor survival.138 IL-10 can also promote
humoral immune responses; B-cells stimulated by IL-10 have enhanced survival due to increased
expression of anti-apoptotic proteins.139 In addition, IL-10 stimulation increases the expression of high-
affinity IL-2 receptor on B cells, leading to enhanced responsiveness to IL-2, the key cytokine signaling
for immune cell proliferation.140 Similarly, IL-10 appears to be able to enhance proliferation in IL-2
activated CD8+ T cells and can rescue these cells from apoptotic cell death.141 IL-10 has even been used
to stimulate antitumor CD8+ T cells in vivo leading to reduced growth of tumors.142 Therefore, while

1.3 | Interleukin-10 1-35
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
IL-10 plays a central role in negative feedback of most pro-inflammatory responses, in select situations it
can also enhance selected immune responses and this dichotomy of action must be considered when
contemplating the use of IL-10 as therapeutic agent.
Figure 1.7: Diagram of Actions of IL-10 on Immune Cells. Adapted from Fujii et al143
1.3.2 Molecular Signaling of IL-10
The molecular signaling of IL-10 is complex. Cells responsive to IL-10 express IL-10 receptor
(IL-10R).144 Unsurprisingly, highly responsive cells such as macrophages and dendritic cells also express
a high amount of IL-10R. Following binding of IL-10 to IL-10R, the JAK-STAT pathway is activated.145
CD4
Th1Th2
mDC
imDC
Treg +
MØ
Inflammatory Cytokines/Chemokines
X
X XX X X
Blocks DC Maturation
ImpairsAPC Antigen Presentation
ReducesPro-inflammatory cytokines
Aids RegulatoryT-Cell Differentiation
Blocks Th1 & Th2 CellDifferentiation
CD8
NK
Activates CD8 and NK Cells
MemoryCD8

1.3 | Interleukin-10 1-36
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
While it is known that activation of STAT3 is vital for all known functions of the IL-10 anti-
inflammatory response146, the exact mechanism of how STAT3 activation can mediate such pleiotropic
effects in so many cell types is unclear. In a microarray study, IL-10 was found to selectively reduce the
expression of only 15-20% of genes induced by LPS stimulation.147 Interestingly, some genes were
further induced rather than reduced. Again, the identity of the genes responsible for the anti-
inflammatory phenotype has yet to be discovered.
1.3.3 Therapeutic Usages of IL-10
Considering the broad anti-inflammatory effects of IL-10, clinicians have desired to utilize IL-10
as a treatment of auto-inflammatory diseases such as psoriasis and Crohn's disease. Systemic
recombinant IL-10 was given to patients with the above diseases in phase I and II trials.148, 149 While
trends towards efficacy were found in these early studies, larger blinded randomized control trials
demonstrated only limited benefits. More importantly, patients suffered from fever and headaches,
suggesting pro-inflammatory side effects of IL-10. In Crohn's disease patients, doses around 5-
8mg/kg/day were found to be most effective, but higher doses were not.149 In fact, higher doses resulted
in increased levels of IFN-γ, granzyme B, and CXCL9 in their serum. This suggests that higher doses of
IL-10 may be stimulating the humoral and cytotoxic arms of the immune system described above and
reiterates the complexity of IL-10 function in vivo.
1.3.4 Delivery of IL-10 to the Lung
The lung is unique in that it is exposed to the outside environment via the airways. Thus,
intratracheal IL-10 delivery is possible and desirable, as a local increase of IL-10 can occur within the

1.4 | Adenoviral Gene Therapy 1-37
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
transplanted organ without unwanted systemic effects. Indeed, one only needs to look at the side-effects
of infection and malignancy from the current standard of systemic immunosuppression to appreciate the
benefit of local immunosuppression. Moreover, the activating effects of IL-10 described above may be
avoided with local administration.
Like all cytokines, IL-10 has an extremely short half-life in vivo.144 Consequently, the majority of
studies using IL-10 as a therapy have utilized some sort of intra-tracheal gene transfer technique to
achieve constant elevated IL-10 levels within the lung. Early attempts at IL-10 gene transfer have
included electroporation of plasmid DNA150, liposome mediated gene transfer151, and viral vector
mediated gene transfer.122 Studies from the Toronto group have systematically explored the use of
adenoviral gene therapy for the delivery of IL-10 and have shown excellent IL-10 expression and benefit
to post-transplant outcomes in small animal models to pre-clinical large animal models.122, 152
1.4 | Adenoviral Gene Therapy
The concept of gene therapy is simple: replace defective genes with wild-type copies to restore
function. To achieve this goal, a robust method of gene delivery to the cells of interest is needed and
transgene expression must occur in the timeframe required to avoid the disease state, usually lifelong.
With the understanding gained by virologists in the study of Adenovirus (Ad), this virus was one of the
first to be harnessed into a gene delivery vector.153 Ad was attractive as a gene therapy vector for a
number of reasons.154 It can efficiently transfer its genome to target cells in an episomal fashion,
reducing the fear of insertional mutagenesis. It can also transfect a variety of cell types, including
terminally differentiated cells. More practically, manipulation of adenovirus was facilitated by the prior

1.4 | Adenoviral Gene Therapy 1-38
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
sequencing of its genome and tools existed to culture the virus in large enough quantities and in high
enough concentrations for clinical application without affecting viral activity.
1.4.1 Adenovirus Biology
Adenovirus is a double-stranded DNA virus which can infect a variety of hosts including
rodents, pigs, dogs, and humans. In humans, adenovirus can infect many organs and tissues including
the adenoids, where it received its namesake, the respiratory epithelium, the conjunctiva, and the gut.155
More than fifty different adenoviral serotypes have been identified using neutralizing sera and these are
divided into subgroups A to E. Because of the significant interest into the treatment of cystic fibrosis and
the known preference of subgroup C to infect the respiratory tract, most adenoviral vectors have been
derived from serotypes 2 and 5 of that subgroup.
Viral Structure
Adenovirus is encapsulated by an icosahedral protein capsid of 70-100nm in diameter.156, 157
(Figure 1.7) Its genome consists of a single copy of a ~36,000bp double-stranded piece of DNA. Three
copies of a 105kDa hexon subunit forms the homotrimer hexon which is the major capsid protein. This
protein forms the 20 triangular faces of the capsid. Other capsid proteins, VI, VIII, and IX, are associated
with hexon and help stabilize the capsid. Protein loops which project out from hexon can be targeted by
antibodies and early methods to categorize adenoviruses have utilized this characteristic to organize
adenoviruses into serotypes.158 At each of the 12 capsid vertices, a penton capsomere is found which
consists of five copies of penton base and three copies of fiber. The fibers jut outwards from the penton
base and the fibers themselves consist of three domains: the base, the shaft, and the knob. The C-

1.4 | Adenoviral Gene Therapy 1-39
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
terminal domain, known as the knob, interacts with the high affinity receptor on the target cell. Except
for subgroup B, this receptor is the coxsackie and adenovirus receptor (CAR).159, 160 While it seems
strange that cells would evolve a receptor merely to allow viruses to enter the cell, other functions for
CAR are currently unknown. CAR itself is a single membrane spanning protein with two extracellular
immunoglobulin like domains.
Figure 1.8: Adenovirus Structure. Adapted from Glasgow et al161
Viral Entry
Following the CAR-fiber interaction, the adenovirus is tethered to the cell, allowing an amino
acid motif arginine-glycine-aspartate (RGD) of penton to interact with integrins (αVβ3, αVβ5) on the cell
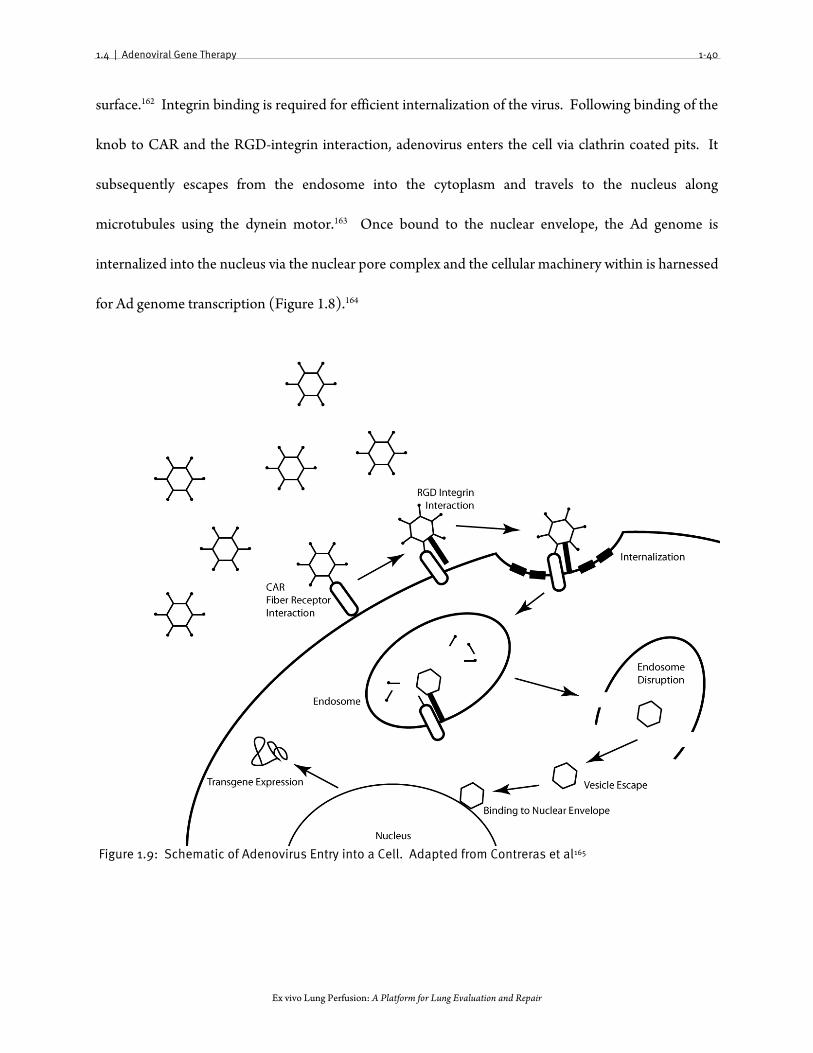
1.4 | Adenoviral Gene Therapy 1-40
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
surface.162 Integrin binding is required for efficient internalization of the virus. Following binding of the
knob to CAR and the RGD-integrin interaction, adenovirus enters the cell via clathrin coated pits. It
subsequently escapes from the endosome into the cytoplasm and travels to the nucleus along
microtubules using the dynein motor.163 Once bound to the nuclear envelope, the Ad genome is
internalized into the nucleus via the nuclear pore complex and the cellular machinery within is harnessed
for Ad genome transcription (Figure 1.8).164
Figure 1.9: Schematic of Adenovirus Entry into a Cell. Adapted from Contreras et al165

1.4 | Adenoviral Gene Therapy 1-41
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Adenoviral Gene Expression and Replication
The genome for type 5 adenovirus has been completely sequenced. It is 35 935bp in size and
the transcription map is functionally divided into early expression (E series) and late expression (L
series) regions. The E region consists of 5 genes with complex transcriptional regulation: E1, E2A, E2B,
E3, and E4. Upon entering the nucleus, E1A protein is created by alternate splicing of E1 mRNAs. E1A
is a major regulatory factor required for subsequent transcription of E1B, E2, E3, and E4.166 It can be
produced purely with existing host cellular proteins and acts to force the host cell into S phase. The
second E1 gene expressed is the E1B gene. This protein acts to inhibit the p53 tumor suppressor and
inhibits apoptosis of the cell.167 Together, E1A and E1B hijack the terminally differentiated epithelial
cell and converts it into an actively dividing cell. These two proteins are able to transform cells in culture
and thus have oncogenic potential. Subsequently, the E2 region is expressed. This region encodes 3
proteins needed for adenovirus DNA replication not provided by the host cell: Ad DNA polymerase,
ssDNA binding protein, and the preterminal protein.168 ssDNA binding protein binds to single stranded
DNA to protect it from nuclease digestion and preterminal protein forms a heterodimer with Ad DNA
polymerase to initiate viral DNA replication. The E3 region encodes proteins which aid in evasion of
host defenses169 and the E4 region encodes for genes which promote the selective expression of viral
genes over cellular genes.170 At about 6 h post-expression, expression of early genes is complete and
adenoviral DNA replication is underway. At this point, transcription of the late genes begins.171 These
genes encode the capsid proteins needed for the production of mature viruses. Once produced, these
proteins are moved into the nucleus where they are assembled with the newly produced adenoviral DNA
into new virions and then the new viruses are released.

1.4 | Adenoviral Gene Therapy 1-42
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
1.4.2 Adenoviral vectors
As the E1A product is vital for expression of early and late genes and subsequent DNA
replication, generation of replication-deficient adenoviral vector requires the deletion of the E1 region of
the adenovirus.172 With this deletion, the oncogenic potential of adenovirus is also mitigated. Human
embryonic kidney cell line 293 was originally established by transforming primary cells with adenovirus
5.173 Because of this, these cells contain a number of adenoviral genes, including E1, within its genome.
Thus, by transfecting this cell line with E1-deleted adenovirus, the deleted E1 region can be replaced in
trans by the 293 cell line allowing for replication of E1-deleted Ad virus and culture of engineered
vectors. The transgene of interest can be inserted in place of the E1-deleted region to a maximum size of
3062bp. Transgenes of a longer length have been incorporated into the vector by deletion of the E3
region to make room.
In the modern era, E1- E3- deleted adenoviruses are constructed and amplified as E. coli
plasmids.174 One common system involves the use of a shuttle plasmid and a backbone plasmid (Figure
1.9). The backbone plasmid contains the adenovirus genome except for the left hand end and the E1,
E3 deleted regions. The shuttle plasmid contains the right and left hand ends and the transgene in place
of the E1 region. The shuttle and backbone can then be recombined by co-transformation into E. coli
and selected for using antibiotic selection. Propagation of the new vector can then occur in 293 cells.
Recombinant adenovirus can be purified from lysed 293 cells by equilibrium cesium chloride density
gradients and function of the newly purified recombinant Ad can then be checked for by plaquing
efficiency on 293 cells and for contaminating wild-type virus on an E1- cell line, typically A549. Two
different measures of Ad concentration have been used to help standardize quantitation of dose: particle

1.4 | Adenoviral Gene Therapy 1-43
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
count and plaque forming units (pfu). Plaque forming units are measured by the number of plaques
formed on 293 cells per mL. Particle count is the number of viral particles per mL and can be calculated
by the absorbance at 260 nm where an absorbance of 1 is equivalent to 1.25×1012 particles/mL.
Typically this is 10-100 times the titer in pfu.
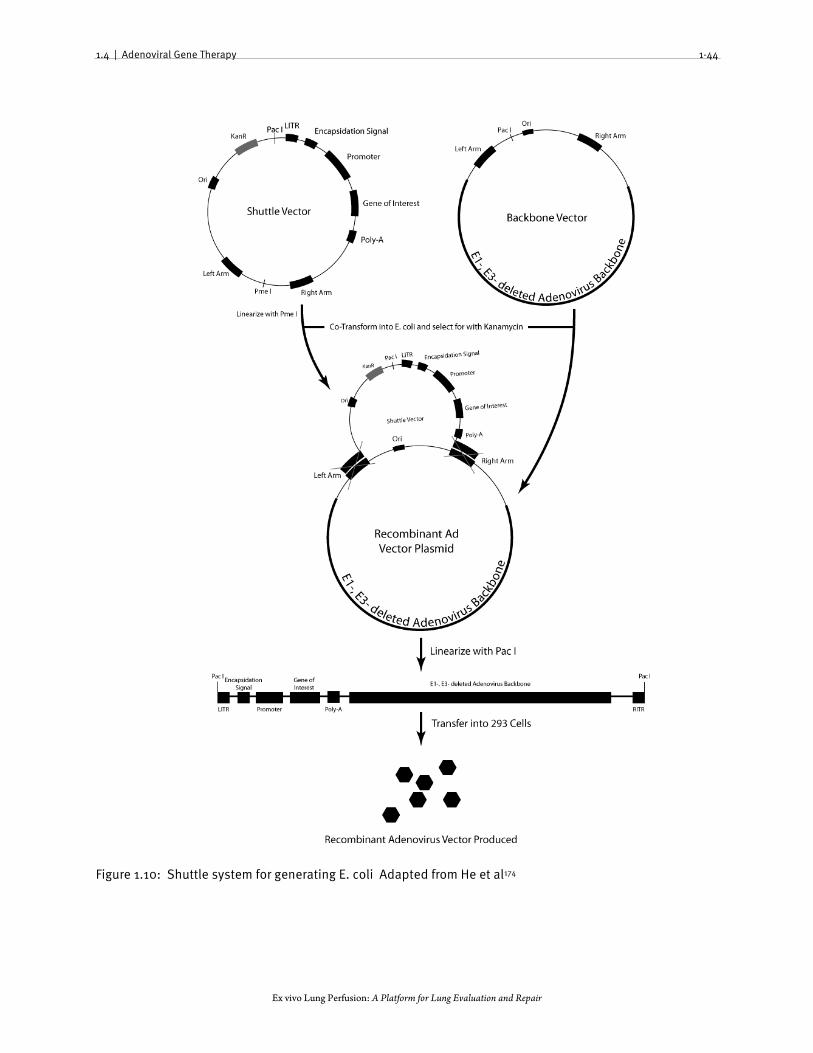
1.4 | Adenoviral Gene Therapy 1-44
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Figure 1.10: Shuttle system for generating E. coli Adapted from He et al174

1.4 | Adenoviral Gene Therapy 1-45
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
1.4.3 Immune Reaction to Adenoviral Vectors
A significant host response to replication-deficient adenovirus became apparent with its use in in
vivo models.175 While the ultimate goal for gene therapy is the lifelong replacement of defective genes
with wildtype transgenes, the duration of transgene expression mediated by Ad vectors was found to be
extremely short. Transgene expression peaked within 1-7 days and rapidly declined to undetectable
levels by 2-4 weeks.175 Attempts to re-administer the same viral vector resulted in a reduction of the
subsequent peak levels of the transgene, suggesting that adaptive immunity played a role in the clearance
of vector, but the timeframe at which it initially declined suggested that the innate immune response also
played a major initial role. Worgall et al administered adenoviral vector to athymic mice intratracheally
and found a similar clearance pattern in the short term to that of wildtype mice, confirming the
involvement of the innate immune response.176
Another side effect of the immune response to vector is a major and sometimes lethal
inflammatory response in the host.177 The immune response to adenovirus is thus highly problematic for
the application of gene therapy and strategies to reduce this immune response would benefit both the
timeframe of transgene expression and the safety of vector administration.
Innate immune response
The innate immune response is a phylogenetically ancient mechanism which acts as the first line
of defense against infection.178 Innate responses act to limit or clear microbe invasion in the host prior to
activation of the adaptive immune system. Moreover, due to years of co-evolution with the adaptive
immune system, the innate immune system can reprogram the adaptive immune response to optimize

1.4 | Adenoviral Gene Therapy 1-46
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
its response in clearance of the pathogen. Innate immunity in the lung is complex and consists of
multiple components.179 First, barriers such as the epithelium and the ciliary escalator act to physically
prevent the progression of pathogen invasion. Specific to adenovirus, tight junctions between epithelial
cells help prevent the virus from accessing the CAR on the basolateral side of the epithelial surface.
Second, effector cells such as macrophages, neutrophils, and natural killer cells act as the primary
effectors of pathogen clearance by internalizing and destroying pathogens as they progress throughout
the lung. To aid pathogen clearance, soluble proteins such as defensins and complement form a
secondary effector arm. These proteins recognize microbes by conserved surface structures and destroy
them either directly by microbial membrane perforation or by labeling them for destruction by
opsonization. Moreover, macrophages can present antigen required for activation of acquired immunity
and NK cells can secrete interferon-γ essential for the development of Th1 cells. Pro-inflammatory
cytokines form the final component of the innate immune response. These soluble proteins serve
critical pro-inflammatory and chemoattractive functions which orchestrate inflammatory and immune
events against invading pathogens.
The most important function of the innate immune system is the accurate and early recognition
of pathogens. This occurs through a number of receptors which recognize conserved molecular patterns
in pathogens in both the intracellular and extracellular compartments. Currently, the best studied
family of receptors are the Toll-like receptors (TLRs)36, but other receptors (NOD-LRR) are known to
exist. TLRs recognizing different pathogen associated molecular patterns (PAMPs) have now been
identified.180 These patterns include lipopolysaccharide (LPS), peptidoglycan, flagellin, unmethylated
CpG DNA, dsRNA, and ssRNA. TLRs are a family of at least 12 members and are expressed on many

1.4 | Adenoviral Gene Therapy 1-47
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
cell types, including professional antigen-presenting cells, T-cells, endothelial cells, and lung epithelial
cells.181 Currently, 10 TLRs have been identified in humans. TLRs 1, 2, 4, 5, 6, and 10 are expressed at
the cellular membrane, while the remaining TLRs are expressed within endosomes for the recognition of
bacterial and viral RNA and DNA. The intracellular position of TLR3 and TLR9 and their specificity for
viral motifs (dsRNA and CpG, respectively) makes them well located for the identification of
intracellular viral infection. TLR activation can result in downstream NF-κB activation, MAPK
activation, and type 1 interferon expression.182 Type 1 interferon expression is particularly interesting as
it is a characteristic first response to viral infection.183
Cytokine Responses
The induction of pro-inflammatory cytokines is an integral part of the innate immune response
to Ad vectors. Recruitment of the cells involved in the adaptive cellular response is cytokine mediated
and there is a temporal correlation between cytokine expression and cellular infiltration. Moreover,
cytokines can exert direct antiviral effects by stimulating anti-viral responses in neighbouring cells in a
paracrine fashion. Many in vitro studies have demonstrated cytokine induction in innate effector cells
such as dendritic cells, macrophages, and peripheral blood mononuclear cells following Ad vector
administration. In vivo, cytokine responses following intratracheal administration of an E1-, E3- deleted
adenoviral vector have been studied in mice.184 In that model, a rapid accumulation of the vector was
found in alveolar macrophages 10 min after vector administration. TNF-α, IL-6, MIP-2 and MIP-1α
levels were elevated in bronchoalveolar lavage 6 h after infection and MIP-2, a strong neutrophil
chemoattractant, was elevated by 3 h. Using in situ hybridization, TNF-α and IL-6 mRNA were found to
be localized solely to alveolar macrophages and MIP-2 mRNA levels were found to be elevated in both

1.4 | Adenoviral Gene Therapy 1-48
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
lung epithelial and alveolar macrophages, once again demonstrating the importance of the alveolar
macrophage to the cytokine response. Interestingly, the TLR system does not seem to be involved in
this response. In dendritic cells from mice where the downstream TLR adaptor protein MyD88 was
knocked out, TNF-α could still be induced by Ad vector185 and cytokine expression was unchanged in
TLR4 mutant mice.186 Ad vector also seems to be able to stimulate cytokine production by cells of non-
hematopoietic origin. Borgland et al transfected renal epithelial cell lines with Ad vector and found
RANTES and IP-10 expression.187 Despite this, in in vivo models, the majority of cytokines appear to be
produced by cells of a hematopoietic origin and these cells likely orchestrate the majority of the innate
immune response in the first few hours. Blockade of cytokine expression has a beneficial effect of
prolonging transgene expression. Use of steroids or IL-10 has demonstrated reduced cytokine
expression and prolonged transgene expression in lung models.184 Also, use of truncated soluble TNF-
receptor as a decoy can also prolong gene expression, implying a central role for TNF-α.188
Given that activation of innate immune signaling occurs as early as 30 minutes post-infection,
this suggests that an early mechanism of adenovirus infection is responsible for stimulating immune
responses. Specific mutants for proteins important in adenoviral entry have been made in an attempt to
better understand how the virus particle itself activates innate immunity. In a liver model, both first-
generation and UV-inactivated Ad vectors could induce an innate immune response, demonstrating that
viral gene expression is not needed for activation and that only the viral particle itself is required.189 In
Ad vectors with mutated knob proteins which cannot bind CAR, IP-10 and RANTES expression was
preserved compared to wild type. In vectors where the RGD motif was deleted, again induction of pro-
inflammatory signals was equivalent to wildtype. Since alveolar macrophages produce the majority of

1.4 | Adenoviral Gene Therapy 1-49
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
cytokines and take up adenoviral vectors by an unknown but alternate mechanism than with CAR/RGD
described above, it appears that viral entry into the epithelium plays a minor role, if any, in the induction
of the cytokine response. Consequently, Zsengeller et al studied adenoviral vector infection in alveolar
macrophages and demonstrated that vector internalization and escape into the cytoplasm was required
for TNF-α expression.190 If they acidified the endosome, thus impairing viral escape, TNF-α expression
was attenuated.190 Further work is needed in this area to fully define the mechanism of immune
activation following adenovirus delivery, but it appears that the alveolar macrophage plays a central role.
Innate Cellular Responses
Parallel to, and likely in response to, the cytokine response, a characteristic cellular response to
Ad vector has been described. Immediately following intratracheal infection of mice with replication-
deficient adenoviral vector, alveolar macrophages were found to take up a large amount of vector in an
attempt to clear the viral load. A major and fundamental difference between natural adenovirus
infection and adenoviral vector delivery is in the initial infecting inoculum. Natural adenovirus infection
begins with the deposition of aerosol droplets containing perhaps 1000 adenoviral virions onto the
mucosal surface of the respiratory epithelium with subsequent replication and release. In contrast, gene
therapy inoculates in large animal or human studies often number in the 1012 particle range, around a
billion times higher than natural adenoviral infections. While these vectors cannot replicate, the upfront
inoculum is huge and overwhelms macrophage uptake mechanisms, allowing Ad vectors to escape
uptake and thus enter epithelial cells. In studies where macrophages are impaired by clodronate
liposomes, expression of vector is further enhanced.191

1.4 | Adenoviral Gene Therapy 1-50
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Following the macrophage uptake of vectors, a rapid neutrophil infiltration occurs, peaking at 6
h and resolving over the next 4 days in animal models.192 This recruitment of neutrophils coincides with
MIP-2 expression, a strong neutrophil chemokine. The next cell type to be recruited in response to Ad
vector is the NK cell. In a model of intravenous injection of adenoviral vector to the murine liver, NK
cells were found to accumulate and peak over 7-10 days following infection. These cells contributed to
liver injury as depletion of NK cells with anti-NK1.1 or anti-asialo GM1 antibodies resulted in reduced
hepatocyte cell death.193 As NK cells are a source of IFN-γ, these cells can also stimulate the adaptive
immune system. Finally, from 4-7 days and fading over weeks, a final phase of cellular infiltration occurs
which consists of lymphocytes. These lymphocytes were shown to be directed at both adenoviral and
transgene proteins and could remove transfected cells by both direct lysis and by antibody-mediated
mechanisms.194 Despite the highly effective initial removal of virus by the innate immune system,
complete removal of infected cells appears to be dependent on the adaptive immune system, as
transfected athymic mice demonstrated greatly reduced but still present transgene expression for more
than 3 months.195 This suggests that some sort of limited immunosuppression could prolong transgene
expression for recipients of gene therapy.
Adaptive immune response
The second phase in the immune response has been described and corresponds to the adaptive
immune response. Following transduction by adenoviral vectors, antigen presenting cells travel to
lymph nodes and generate adenoviral- and novel transgene- specific T- and B- lymphocyte responses. In
the context of viral infection, cytotoxic (CD8+) T-cells directly eliminate virally infected cells and B-cells
generate antigen-specific antibodies for the elimination of extracellular Ad vector. Profound depletion

1.4 | Adenoviral Gene Therapy 1-51
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
of APCs by clodronate liposomes reduced TNF-α and IL-6 expression as expected but also reduced
adenovirus-specific cytotoxic T lymphocyte responses, the expected downstream effect.196 NK cell
activation also appears to be important in developing Ad specific T-cell responses. NK cell depletion
resulted in reduced CD8+ T cell responses193 and prolonged transgene expression and is thought to be
related to reduced secretion of IFN-γ by NK cells.197
Together, the humoral and cellular immune response results in complete elimination of
transgene expression and produces immunologic memory in the form of memory CD8+ T-cells and
circulating neutralizing antibodies and memory plasma cells. Therefore, attempts to readminister vector
results in a rapid neutralization of vector by antibodies, preventing cellular transduction. Cells which do
become transduced are rapidly killed by CD8+ T-cells.
Immunosuppression as a strategy to impede the adaptive immune response
Chronic immunosuppression with cyclosporine or cyclophosphamide has improved the length
of transgene expression in animal models of lung gene therapy. Administration of cyclophosphamide
resulted in blocked activation of cytotoxic T cells and helper T cells and reduced anti-Ad antibody
production.198 In contrast, though cyclosporine alone failed to reduce the production of neutralizing
antibodies in a model of hemophilia B in dogs, it was still effective in prolonging transgene expression.199
Given that the major effect of cyclosporine is to block IL-2 signal transduction, isolated reduction of the
T-cell response with the sparing of B-cell response was likely the reason for the above result. Regardless,
the morbidity of life-long systemic immunosuppression renders its use for gene therapy to be
impractical. However, in the context of gene therapy applications for transplantation, the obligate
immunosuppression needed for graft survival may aid in prolonging transgene expression. The triple

1.5 | EVLP IL-10 Delivery Strategies 1-52
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
regimen of transplant immunosuppression has resulted in enhanced and prolonged transgene expression
as demonstrated by Suga et al.200
Overall, immune responses against adenoviral vectors are complex and well-orchestrated events
that bridge innate and adaptive immunity. However, the majority of effector mechanisms rely on the
recruitment of responder cells from the circulation. Indeed, propagation of the initial cytokine response
requires responder neutrophils. It is as yet unclear how adenoviral gene therapy of a donor lung, isolated
on an EVLP circuit with no responder cells in the perfusate will propagate an inflammatory response.
1.5 | EVLP IL-10 Delivery Strategies
Clinical use of gene therapy for the purposes of lung transplantation was previously thought to
have been logistically impractical due to the time needed to achieve transgene expression (>6h) and
biologically impractical due to vector-associated inflammation which could harm the donor or other
potential donor organs. The normothermic environment afforded by EVLP preserves the metabolic
function of the lung and makes EVLP an attractive platform for the delivery of gene therapy. Cypel et al
have recently demonstrated this by delivering adenovirus encoding IL-10 intra-tracheally to rejected
human lungs for transplantation and found that lung function improved and pro-inflammatory cytokine
production was reduced over 12 h of EVLP.113
It has been recognized that the half-life of the IL-10 transgene product in the perfusate of lungs
transduced during EVLP with AdhIL-10 is significantly longer than that in vivo. This is likely a result of
the absence of a renal clearance mechanism for circulating cytokines during EVLP. Given that the
majority of drugs are removed by hepatic and renal clearance mechanisms, this effect can be exploited

1.5 | EVLP IL-10 Delivery Strategies 1-53
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
for EVLP drug delivery in general. There are certain advantages and disadvantages to direct
recombinant drug delivery during EVLP over gene therapy. With direct drug delivery, the beneficial
effects upon delivery are immediate and do not require the transgene expression time. Moreover, the
repertoire of available drugs is greatly broadened as one is no longer limited to drugs that are proteins.
But unlike gene therapy where the production of the therapeutic protein is anticipated to continue
through reperfusion, direct drug delivery will likely result in rapid clearance of the drug at or soon after
the time of reperfusion owing to recipient clearance mechanisms or the post-EVLP vascular flush.
Because IL-10 has a rather narrow therapeutic window, a gene therapeutic approach where IL-10
production is not easily controlled may indeed benefit from a recombinant approach. However, the
corollary to this is that IL-10 would not be present to mediate changes post-transplant. Thus, depending
on the intended application of therapy, either gene therapy or direct drug delivery may be the better
option.
1.5.1 Aerosol deposition
While intratracheal Ad gene therapy has been shown to be technically quite facile113, 152,
intratracheal protein delivery can be more complicated. While the inhalation of drugs for the treatment
of diseases such as asthma and chronic obstructive pulmonary disease is commonplace, aerosols of
proteins have yet to reach common clinical use and the delivery of aerosol to the distal alveolar spaces
remains challenging. Currently, three major techniques are utilized for the generation of aerosols. One
of the oldest and most common techniques is that of jet nebulization where a gas is delivered at high
flow through a liquid causing the liquid to break into an aerosol mist.201 Ultrasonic wave nebulization is
another technique where a piezoelectric element is placed in contact with a liquid reservoir and then

1.5 | EVLP IL-10 Delivery Strategies 1-54
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
vibrated at a high frequency by an electronic oscillator. The vibrations turn the liquid into an
aerosolized mist. In both these above techniques, a potential for protein denaturation is present due to
heat generation or from physical shear forces.202 In the newest technique known as vibrating mesh
technology, a mesh with 1000-7000 laser drilled holes vibrates at the top of the liquid reservoir, and
pushes fluid out through the holes.203 Due to the surface tension of water, as the fluid passes through the
small holes, rather than form a column of fluid, the fluid coalesces into small droplets of aerosol. This
technique generates less heat and is less prone to the denaturation of proteins. Vibrating mesh
technology has been used experimentally to aerosolize DNase with preservation of enzymatic
function.204
The therapeutic effect of aerosolized drugs is dependent on the dose delivered and its
distribution within the lung. Inhaled anti-inflammatory therapy such as IL-10 is probably best when
deeply and evenly distributed throughout the lung since the inflammatory cells are present throughout
the lung, and particularly in the case of the alveolar macrophage, present deep within the lung in the
alveoli. However, such homogeneous distribution of drugs to the lung by aerosolization is challenging.
The lung has an extremely large surface area. As airflow progresses into the lung, branching of the airway
greatly increases the cross sectional area leading to significant drop-offs in flow in the distal airway.
Aerosol particle size is another major variable in determining the dose deposited and the distribution of
drug in the lung. Fine aerosols (<3μm) are distributed on distally but deposit less drug per unit surface
area than larger particle aerosols (3-5μm) which deposit more drug per unit surface area, but on the
larger, more central airways.205 In practice, most clinically used aerosol generators also heterodisperse,
meaning that a wide range of particle sizes is delivered.206

1.6 | Summary 1-55
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
In theory, delivery of aerosol during EVLP has certain advantages. First, the lung is intubated,
thus loss of aerosol into the throat or mouth is absent. Second, the humidity of the ventilated gas is
controlled. Thus, a low humidity of gas can be delivered, reducing the increase in aerosol size caused by
humidification of the particle. The length of the endotracheal tube can also be shortened to minimize
the amount of impaction of aerosol on to the tube prior to entering the lung. Finally, the ventilation
parameters are completely controlled and no chest wall exerts pressure onto the lung. Thus, the
ventilation settings can be optimized for aerosol delivery without regard for the ventilation of the
patient, i.e. long inspiratory times and long inspiratory hold times in a completely recruited lung.
1.6 | Summary
Lung transplantation is hence a promising therapy for end-stage lung disease, but is currently
limited by a low donor rate and poor donor lung utilization rate. EVLP demonstrates promise as a
method to better evaluate lungs during the ex vivo phase of transplantation. Moreover, drug delivery to
lungs can be achieved during EVLP either with adenoviral gene therapy or by direct delivery to the
airways or perfusate. In these studies, I explored the physiology of EVLP as a means for lung evaluation
and characterize IL-10 delivery by both gene therapy and direct delivery mechanisms.

Chapter 2
Rationale, Hypothesis, and Objectives

2.1 | Rationale 2-1
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
2.1 | Rationale
Today, even the most aggressive lung transplant programs use at most 40% of offered donor
lungs for transplantation. The remainder are either felt to be or are actually too injured to be safely
utilized for transplantation. With the development of prolonged normothermic ex vivo lung perfusion,
there now exists great potential for: 1) the evaluation of questionable donor lungs and 2) the
individualized repair of injured human lungs during the lung preservation phase. Successful
development of this paradigm would greatly increase lung transplant volumes and reduce waitlist times
and mortality.
This research builds upon the work of previous members in the lab exploring ex vivo lung
perfusion and IL-10 therapy and their accomplishments are summarized in Table 2.1.
Table 2.1: Summary of previous work on IL-10 and ex vivo lung perfusion
IL-10 Therapy EVLP Intratracheal AdhIL-10 reduces ischemia-
reperfusion injury in the rat (Fischer, 2001)122 Protective strategy for EVLP (Cypel, 2008)109
IL-10 transgene expression reduces vector associated inflammation in the rat
(de Perrot, 2003)207
EVLP interrupts cold ischemic injury (Cypel, 2009)112
Intratracheal AdhIL-10 reduces ischemia-reperfusion injury in the pig (Martins, 2004)152
Ex vivo Intratracheal AdhIL-10 reduces ischemia-reperfusion injury in the pig and reduces pro-inflammatory cytokine expression in rejected human lungs (Cypel, 2009)113
Clinical trial using EVLP to evaluate marginal donor lungs (Cypel, 2011)114
During the experiments with ex vivo AdhIL-10 therapy, it was found that IL-10 protein has a
much longer half-life during EVLP. Thus, though the in vivo delivery of recombinant IL-10 (rIL-10) has
been limited by its short half-life, its expense, and the need for systemic delivery, ex vivo delivery of rIL-

2.1 | Rationale 2-2
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
10 appears to circumvent these limitations. Hence, we explored rIL-10 delivery using rejected human
lungs to assess its effect on lung function and cytokine production. If demonstrated to be effective, we
envision that clinical trials using recombinant IL-10 could follow very shortly.
Despite the potential benefits of ex vivo recombinant IL-10 delivery, gene therapy remains an
exciting approach for many therapeutic interventions in injured donor lungs. Gene therapy allows for
the continued production of transgene product during and after the initial phase of reperfusion;
timepoints at which recombinant therapies will have already been washed away or degraded by the
recipient. This may be a particularly desirable feature for future ex vivo therapies which aim to modify
the immunogenicity of the donor organ. However, one current impediment to gene therapy is vector-
associated inflammation. Because EVLP isolates the organ at the time of vector delivery, mounting of an
inflammatory response against the vector could be hindered. Thus, we further explored ex vivo gene
therapy in the context of vector-associated inflammation by using a first generation adenoviral vector
encoding GFP, a transgene with no anti-inflammatory effect, and comparing ex vivo to in vivo vector
delivery.
While clinically rejected human lungs utilized for the recombinant IL-10 study are most
representative of real-world lung injury encountered by lung transplant clinicians, use of these lungs can
be limiting in a research setting. The donor lung injuries leading to rejection for clinical use are highly
variable and range from consolidative injuries such as pneumonia to physical/traumatic injuries such as
contusion. However, the therapy being tested may only be suited for treating a limited subset of these
injuries. Moreover, the severity of injury is variable in each rejected block of lungs, further complicating
controlling for the variable of injury. Researchers would also become similarly limited as clinicians by

2.2 | Hypotheses 2-3
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
donor shortages and the regular availability of organs cannot be guaranteed. Thus on the whole, while
clinically rejected human lungs can play an important role in the immediate pre-clinical evaluation of
donor lung therapies, animal models are more useful for the development of potential lung therapies. In
this laboratory, all of the studies have been carried out using prolonged cold ischemia as the model of
injury. While technically simple, it is not representative of clinical donor lung injury. There is currently
no major need to extend cold ischemic times in the clinical arena. Rather, a large problem is the
inflammatory injury resulting from brain death which potentiates cold ischemic injury. Thus, we sought
to establish a clinically-relevant brain death injury model in pig for use with EVLP. Since no formal
study into the evaluation of injured donor lungs using EVLP has yet been done, we explored the
physiologic manifestations of lung injury during EVLP. Insights gained into EVLP evaluation will
greatly impact clinical use of EVLP for evaluation and the assessment of adequacy of lung repair
strategies such as IL-10.
2.2 | Hypotheses
1. Injured donor lungs can be reconditioned by therapeutic drug delivery during ex vivo lung perfusion.
2. Ex vivo perfusion of lungs allows for the sensitive evaluation of lung injury.
2.3 | Objectives
1. To evaluate the delivery of recombinant human interleukin-10 as an aerosol and as an additive to the
perfusate during ex vivo lung perfusion of clinically rejected human lungs.
2. To evaluate the safety and efficacy of ex vivo delivery of adenoviral-based gene therapy pre- and post-
transplantation in a porcine model of single left lung transplantation.

2.3 | Objectives 2-4
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
3. To assess the physiologic parameters of lung injury during ex vivo lung perfusion by using a porcine
brain-death, extended cold ischemia model of lung injury.

Chapter 3
Delivery of Recombinant IL-10 to Injured Human Lungs

3.1 | Abstract 3-1
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
3.1 | Abstract
Introduction: While IL-10 is a promising therapy for injured donor lungs, the short half-life of IL-10 in
vivo has necessitated the use of gene therapy for IL-10 delivery in almost all animal models of lung
transplantation. Because isolation of the donor lung on the EVLP circuit removes it from the influence
of renal and hepatic clearance mechanisms, a much prolonged half-life of IL-10 is predicted. Thus,
delivery of recombinant IL-10 to injured donor lungs while isolated on EVLP could be a clinically
relevant and logistically simple method of employing IL-10 therapy.
Materials and Methods: Injured human donor lungs clinically rejected for transplantation were
subjected to 12 h of EVLP and randomized to receive either saline (control), IL-10 in the perfusate, or
IL-10 aerosolized into the airways. Physiologic and cytokine profiles were measured to assess the effect.
Results: Intravascular delivery of rIL-10 did not alter the physiology or pro-inflammatory cytokine
profile of injured human donor lungs despite elevated IL-10 levels in the perfusate after 12 h of
perfusion. Intratracheal delivery of rIL-10 also did not alter the physiology or pro-inflammatory
cytokine profile of injured human donor lungs despite elevated tissue and perfusate levels after 12 h of
perfusion.
Conclusion: It appears that a large amount of intratracheally delivered IL-10 leeches into the perfusate
where it may not be biologically active. Intratracheal gene therapy may yet be a superior method of IL-
10 delivery as it allows for continued production of IL-10 within the alveoli where it has the potential to
continuously act on alveolar macrophages in a paracrine fashion.

3.2 | Introduction 3-2
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
3.2 | Introduction
Due to the success of lung transplantation for end-stage lung disease, widespread application is
now limited by the shortage of acceptable donor organs. The large majority of lungs offered for
transplantation are currently rejected, thus any increase in the rate of organ utilization would greatly
benefit lung transplant volumes. In addition, the successful development of strategies to increase the
yield of offered donor lungs would also benefit parallel strategies aimed at increasing the number of
offered donor lungs such as the recent re-exploration of using lungs from donors after cardiac death.
The cytokine and adrenergic storms which follow brain death in combination with mechanical
ventilation and other ICU interventions results in a hostile environment for donor lungs. By the time
organ retrieval can occur, most lungs are too injured to be utilized. While careful donor management in
the ICU does improve organ quality as demonstrated in studies by Angel et al73 and Gabbay et al68, even
the most experienced lung transplant programs today utilize at most 40% of lungs.
Because modern lung preservation strategies limit the metabolic rate through cold storage,
attempts to improve lung quality have effectively been limited to the timeframe prior to organ retrieval.
With the recent development of prolonged normothermic ex vivo lung perfusion (EVLP) which
preserves the metabolic rate, a potential for ex vivo repair now exists.109 Use of strategies for lung repair
during ex vivo perfusion has been employed experimentally by a variety of groups using different
strategies of EVLP. Inci et al used ex vivo surfactant delivery to an aspiration lung injury model with
some benefit and Neyrinck et al briefly reported finding accelerated clearance of pulmonary edema
following the delivery of an aerosolized beta-adrenergic drug to the airway.120

3.2 | Introduction 3-3
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
This laboratory has had success with utilizing interleukin-10 (IL-10) in both small and large
animal models of lung transplantation to reduce ischemia-reperfusion injury.122, 152 IL-10 is a cytokine
which has been shown to inhibit production of pro-inflammatory cytokines and chemokines by
macrophages and neutrophils, in vitro.144 Indeed, the alveolar macrophage has been shown to play a
major role in the initiation of ischemia-reperfusion injury90 and IL-10 can regulate the amount of pro-
inflammatory cytokine production by these cells.208 But because the half-life of IL-10 in vivo is around 2
h209 and the cost of recombinant IL-10 (rIL-10) is high, most therapeutic strategies using IL-10 have
employed gene therapy delivery strategies. When IL-10 was delivered via an intra-tracheal adenoviral
gene therapy approach to clinically rejected human lungs during EVLP, beneficial effects included
reduced pro-inflammatory cytokine formation and improved lung function.113 During the development
of EVLP and IL-10 gene therapy, it became apparent that the IL-10 protein does not breakdown as
readily during ex vivo perfusion and in fact demonstrates a much prolonged half life, likely due to the
absence of renal cytokine clearance. We thus envisioned the use of recombinant IL-10 as a simpler
method of IL-10 delivery and anticipate that the strategies developed for the delivery of recombinant IL-
10 could be able to be generalized to other potential protein and small molecule ex vivo therapeutics.
In this study, we characterize the delivery of recombinant IL-10 by intra-tracheal and
intravascular routes to rejected human donor lungs. Furthermore, we assess the effectiveness of
recombinant IL-10 delivery during EVLP in improving human lungs for transplantation.

3.3 | Materials and Methods 3-4
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
3.3 | Materials and Methods
3.3.1 Design
Human lungs clinically rejected for transplantation started on 12 h of EVLP and then randomly
assigned to receive IV rIL-10 (n=5), IT rIL-10 (n=5), or saline vehicle (n=5).
3.3.2 Human lungs
Injured human lungs clinically rejected for transplantation by all Canadian lung transplant
programs with donor consent for research were utilized. Institutional research ethics board and Trillium
Gift of Life Network research approval were also obtained.
3.3.3 Ex vivo lung perfusion
EVLP was performed as detailed by Cypel et al. for 12 h.109 A conical XVIVO cannula (Vitrolife
AB, Sweden) was sewn to the left atrium in a running fashion using 5-0 polypropylene monofilament. A
straight XVIVO cannula was tied into the pulmonary artery using 0 silk ties. Retrograde flushing of the
lungs using 1L of Perfadex® was then performed to flush out potential emboli and to check for leaks at
the suture line. The circuit was then prepared. A custom XVIVO pack was utilized (GISH, Pack
#11512) which consists of a circuit containing a pediatric reservoir, a centrifugal pumphead, an
oxygenator, a heat exchanger, and a leukocyte filter. This circuit was mounted onto a centrifugal pump
setup and a temperature and flow probe connected to it. A heater/cooler unit was then connected to the
heat exchanger and the connection de-aired. The circuit was then primed with 1.5L of Steen solution,
10,000 U of heparin, 500 mg of Solumedrol, and 1 g of Cefazolin. An XVIVO dome was then opened
and the lungs placed within it. By clamping distal to the bridge and connecting the atrial cannula, the

3.3 | Materials and Methods 3-5
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
lungs were then de-aired in a retrograde fashion using the circuit. Once deaired, the pulmonary artery
cannula was connected and anterograde perfusion started at 10% of calculated maximum flow which is
40% of the estimated cardiac output. After 10 min, the flow was increased to 20% of maximum flow and
the temperature increased to 30 degrees Celsius. Following another 10 min, the flow was increased to
30% of maximum flow and the heater/cooler set to 38 degrees Celsius. When the temperature of the
inflow perfusate reached 33 degrees Celsius, ventilation was started. Tidal volume was set at 7mL/kg of
body weight in pigs using a volume control mode of ventilation and an FiO2 of 21%. Flows continued to
be increased in a stepwise fashion every 10 min to 50, 80, and then 100% of the calculated maximal flow
(Table 3.1). This maximal flow was maintained until the end of EVLP. Lung physiologic parameters
including pulmonary artery pressure, pulmonary venous pressure, perfusate flow rate, dynamic
compliance, peak airway pressure, PaO2, and partial pressure of oxygen in the pre-lung perfusate (PvO2)
were measured. Pressures were measured with standard pressure monitoring equipment. Flow rate was
measured with an ultrasonic flow probe. Compliance and airway pressure measurements were recorded
from the ventilator (Servo-I, Maquet, Wayne, New Jersey). PaO2 and PvO2 were measured with a
arterial blood gas monitor (RapidLAB 348, Siemens, Deerfield, Illinois). Standardized lung inflation
was performed by measuring lung parameters exactly 10 min following recruitment of the lung to a
pressure of 25cm H2O. Evaluation occurred at an FiO2 of 21% and 100%.

3.3 | Materials and Methods 3-6
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Table 3.1: Ventilation, Heating, and Perfusion Strategy for the First Hour of Perfusion
After the final EVLP evaluation, the lung block was cooled to 15 degrees Celsius using the
heater-cooler and then both PA inflow and LA outflow was clamped and divided. The trachea was then
clamped to maintain the lung in an inflated state and ventilation stopped. The donor lungs could then
be removed from the circuit.
3.3.4 Delivery of recombinant IL-10
Intra-tracheal Aerosolization
Carrier-free recombinant human IL-10 (25 μg, R&D Systems) was dissolved in 6mL of
phosphate buffered saline. An Aeroneb Go vibrating membrane aerosol generator was attached to the
ventilator on the inhalational arm of the ventilator. The endotracheal tube was shortened to 15 cm and
the tip of the tube placed 2 cm proximal to the first bronchial bifurcation. This was confirmed by
bronchoscopy. The lung was fully recruited and then the ventilator set to a tidal volume of 12 mL/kg
Time (min) 0-10 10-20 20-30 30-40 40-50 50-60
Heater Setting Off 30 38 38 38 38
Achieved Temperature Room Temperature
30 33 37 37 37
Percent Calculated Flow 10 20 30 50 80 100
Ventilation OFF OFF ON ON ON ON
Membrane Gas OFF OFF ON ON ON ON
LA Pressure (mm Hg) 3-5 3-5 3-5 3-5 3-5 3-5

3.3 | Materials and Methods 3-7
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
and a respiratory rate of 15 breaths per minute with a hold of 2 seconds for aerosol delivery. Aerosol was
continuously generated during the time of delivery.
Intra-vascular Delivery
Carrier-free recombinant human IL-10 (5 μg, R&D Systems) was dissolved in 2mL of Steen
solution and added directly to the priming volume of Steen solution in the perfusion circuit of EVLP.
3.3.5 Biopsies
Biopsies of the superficial portions of the lung were performed at 1 h, at 3 h, and then at every
subsequent 3 h using a GIA60 (AutoSuture, Covidien, Mansfield, MA) stapler. To assess distribution of
IL-10 delivered, 3 biopsies per lobe were taken at various depths of the lung at the end of perfusion.
Perfusate samples were also taken with each biopsy.
3.3.6 Homogenization of lung tissue
Lung tissue homogenization and protein extraction were performed as previously described.152
Tissue frozen in liquid nitrogen was homogenized and crushed into a powder in a mortar and pestle
cooled with dry ice. Lung tissue (50mg) was then put into a microcentrifuge tube and 1 mL of lysis
buffer added. These mixtures were then sonicated for 10 seconds on ice thrice and then centrifuged at 4
degrees Celsius at 10,000 rcf for 15 min. The supernatant was then aliquoted and stored at -80 degrees
Celsius until analysis.

3.4 | Results 3-8
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
3.3.7 Inflammatory Profile in Human Lung Tissue Biopsies
Human IL-8, IL-1β, IL-6, IL-10, TNF-α and IL-12p40 were measured by flow cytometry in lung
tissue homogenates using a fluorescent cytometric bead array assay according to manufacturer's
instructions (Human Inflammation Kit; BD Biosciences, San Jose, CA). Each human inflammation
capture bead suspension (10 μL/test) was mixed. Fifty μL of the mixed capture beads were subsequently
added to assay tubes containing 50 μL of the Human Inflammation PE Detection Reagent and 50 μL of
sample or standards. The mixture was incubated for 3 h and washed. Finally, the bead pellet was
suspended and analyzed on a flow cytometer (LSR II, Becton Dickinson Immunocytometric Systems,
San Diego, CA) using BD CellQuest™ Software. For formatting sample data and subsequent analyses,
the BD™ CBA Software was used.
3.3.8 Statistics
All results were expressed as mean ± standard error of the mean. For comparisons between the
two groups at all timepoints, two-way ANOVA was utilized. For comparisons between three or more
groups, one-way ANOVA was utilized. Post-test analysis between each group was performed with
Bonferroni correction for multiple comparisons. p values less than 0.05 were considered significant.
3.4 | Results
For the fifteen lungs utilized for this study, median age, cold ischemic time until EVLP, last PaO2
in the donor, and reason for rejection did not differ between these groups and the characteristics are
summarized in Table 3.2.

3.4 | Results 3-9
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Table 3.2: Characteristics of Injured Human Donor Lungs
Control IV IL-10 IT IL-10 Significance Median Age in Years (Range)
42 (25-58) 58 (13-81) 24 (15-39) p=0.26
Cold Ischemic Time until EVLP in Hours (Range)
5 (4-10) 6(4-11) 5 (5-6) p=0.50
Last PaO2 in Donor Hospital in mmHg (Range)
290 (80-365) 303.5 (233-439) 423 (270-435) p=0.31
Reason for Rejection (Number)
Pneumonia (4), PA Hypertension (1)
Pneumonia (4), Donor malignancy (1)
Pneumonia (3), Aspiration (1),
Emphysema (1)
3.4.1 Recombinant IL-10 delivered ex vivo is measurable 12 h after delivery in tissue and
perfusate
Following the delivery of 5 μg of rIL-10 into 2 L of perfusate, we expected to achieve
approximately 2,500 pg/mL of IL-10. Indeed, we measured 2,493 pg/mL ± 255.5 after 3 hours of
perfusion. By 12 h of perfusion, the level of IL-10 in the perfusate fell to 908.8 ± 196.6 pg/mL. This
corresponds to a half life of 8.23h. In contrast, IL-10 perfusate levels in the control group remained
essentially absent at both timepoints. For the IT delivered group, IL-10 appeared to leach rapidly out
into the perfusate as IL-10 perfusate levels increased to 4244±1706 pg/mL at 3 h of perfusion then fell to
1149±523.7 pg/mL by 12 h of perfusion (Figure 3.1).

3.4 | Results 3-10
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Figure 3.1: Perfusate IL-10 levels. *p<0.05 compared to control at that timepoint.
When we examined IL-10 levels in lung tissue, IT delivered IL-10 levels were elevated compared
to both control and the IV delivered IL-10 group at 7.6 ± 2.6pg/mg protein at 3 h and 12.0 ± 3.9 pg/mg
protein at 12 h, p=0.04. There were no significant differences between the IV IL-10 group and the
control group (Figure 3.2).
IL-10 in Perfusate
3h 12h 3h 12h 3h 12h0
2000
4000
6000
8000
Control IV IL-10 IT IL-10
*
*
**IL
-10
Lev
el (
pg/m
l)

3.4 | Results 3-11
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Figure 3.2: IL-10 levels in lung tissue. IT IL-10 group had higher IL-10 levels than control or IV IL-10 group at both timepoints, *p<0.05 at that timepoint.
3.4.3 Distribution of IL-10 within the lung following IT delivery
To assess the distribution of IL-10 within the lung following aerosolized delivery, we next looked
at the tissue distribution of IL-10 at the end of 12 h of perfusion in the IT IL-10 group by taking biopsies
along the airway and out into the periphery. Unsurprisingly, levels of IL-10 were higher in the tissue by
the proximal airway than in the distal alveoli, p<0.05 (Figure 3.3).
3h 12h 3h 12h 3h 12h0
5
10
15
20
Control IV IL-10 IT IL-10
*
IL-1
0 L
evel
(pg
/mg
prot
ein)
*

3.4 | Results 3-12
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Figure 3.3: IL-10 distribution in lung tissue 12h following delivery. Distal represents biopsies from the alveolar parenchyma, proximal represents biopsies taken close to the first branch of the mainstem bronchus, middle represents biopsies taken between those two areas. * p<0.05
3.4.3 Effect of IL-10 on ex vivo lung physiology
We next examined the effect of IL-10 on the physiology of ex vivo perfused lungs. The IV IL-10
group had one lung which developed major edema during perfusion leading to an early termination of
EVLP with corresponding falls in compliance and PO2 and increases in airway pressure. However,
overall, there were no differences between the groups in PO2 at the end of EVLP (Figure 3.4).
Proximal Middle Distal0
5
10
15
20
25 *
IL-1
0 Le
vels
(pg/
mg
prot
ein)

3.4 | Results 3-13
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Figure 3.4: Effect of IL-10 delivery on PO2 at end of EVLP. p=0.84.
We next examined the physiologic parameters of compliance and airway pressure. Apart from
the aforementioned lung in the IV IL-10 group, there were no significant differences between the
compliances or airway pressures in the control, IV IL-10 group and the IT IL-10 group. In the control
group, compliance rose or was stable in all 5 cases. Compliance rose or was stable in 4 cases of the IV IL-
10 and this was mirrored in the IT IL-10 group. A similar stability was found in airway pressure
measurements between the three groups (Figure 3.5).
Control IV IL-10 IT IL-100
200
400
600
PaO 2
at 1
00%
FiO
2(m
m H
g)
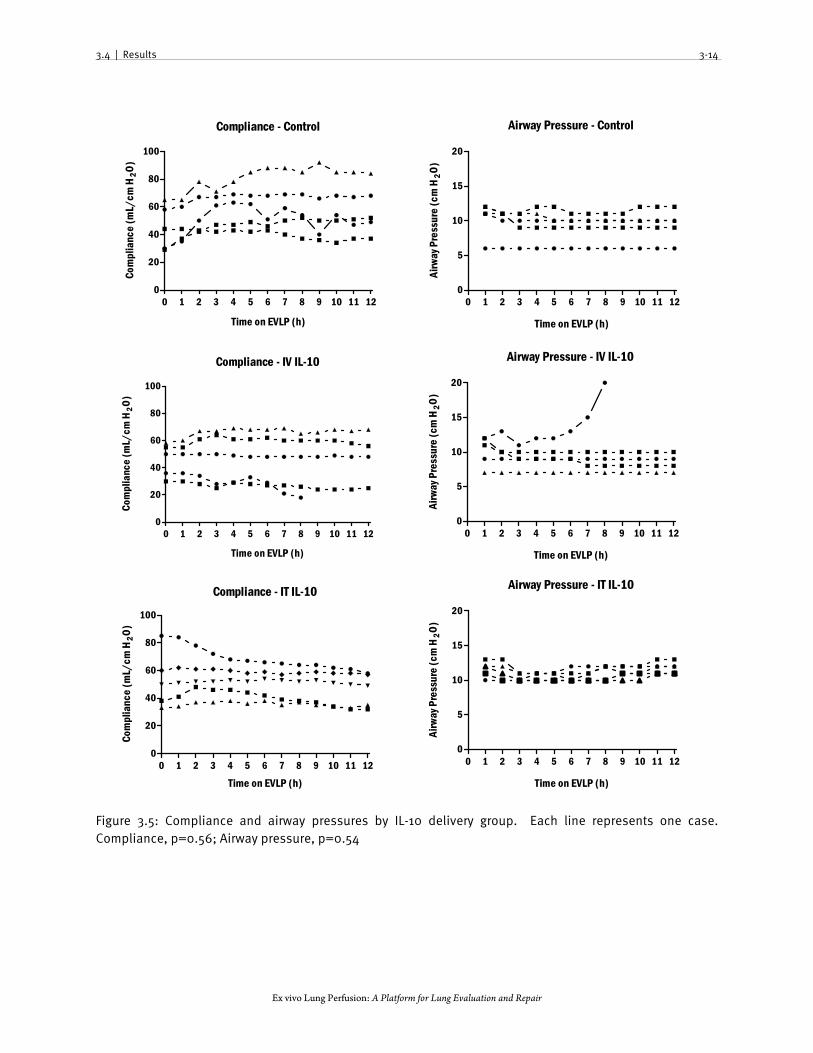
3.4 | Results 3-14
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Figure 3.5: Compliance and airway pressures by IL-10 delivery group. Each line represents one case. Compliance, p=0.56; Airway pressure, p=0.54
Compliance - Control
0 1 2 3 4 5 6 7 8 9 10 11 120
20
40
60
80
100
Time on EVLP (h)
Com
plia
nce
(mL/
cm H
2O)
Airway Pressure - Control
0 1 2 3 4 5 6 7 8 9 10 11 120
5
10
15
20
Time on EVLP (h)
Airw
ay P
ress
ure
(cm
H2O
)
Compliance - IV IL-10
0 1 2 3 4 5 6 7 8 9 10 11 120
20
40
60
80
100
Time on EVLP (h)
Com
plia
nce
(mL/
cm H
2O
)
Airway Pressure - IV IL-10
0 1 2 3 4 5 6 7 8 9 10 11 120
5
10
15
20
Time on EVLP (h)
Airw
ay P
ress
ure
(cm
H2O
)
Compliance - IT IL-10
0 1 2 3 4 5 6 7 8 9 10 11 120
20
40
60
80
100
Time on EVLP (h)
Com
plia
nce
(mL/
cm H
2O)
Airway Pressure - IT IL-10
0 1 2 3 4 5 6 7 8 9 10 11 120
5
10
15
20
Time on EVLP (h)
Airw
ay P
ress
ure
(cm
H2O
)

3.4 | Results 3-15
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
3.4.5 Effect of IL-10 on cytokine expression
Because the majority of the lungs had excellent PO2 and stable or improving compliances and
airway pressures, we examined the effect of IL-10 on the expression of pro-inflammatory cytokines.
Significant increases in tissue levels of IL-6 and IL-8 occurred in all groups, regardless of route of IL-10
administration. TNF-α levels remained mostly stable in all three groups. There was a significant
elevation in IL-1β in the IT IL-10 group compared to the other groups (p<0.05 at 12h, p=0.04 overall),
whereas the other cytokines remained statistically similar (Figure 3.6).
Figure 3.6: Tissue cytokine levels after delivery of IL-10. All values expressed as pg cytokine/mg total protein. IL-6: p=0.26, IL-8: p=0.60, TNF-α = 0.76, IL-1β = 0.04; *p<0.05 at that timepoint.
IL-6
0 1 2 3 4 5 6 7 8 9 10 11 120
2000
4000
6000
8000
Hours Following IL-10 Delivery
IL-6
Lev
els
(pg/
mg
prot
ein)
IL-8
0 1 2 3 4 5 6 7 8 9 10 11 120
2000
4000
6000
Hours Following IL-10 Delivery
IL-8
Lev
els
(pg/
mg
prot
ein)
TNF-
0 1 2 3 4 5 6 7 8 9 10 11 120
5
10
15
20
25
Hours Following IL-10 Delivery
TNF-
Lev
els
(pg/
mg
prot
ein)
IL-1
0 1 2 3 4 5 6 7 8 9 10 11 120
50
100
150
Hours Following IL-10 Delivery
IL-1
Leve
ls (p
g/m
g pr
otei
n)
Control
IV IL-10
IT IL-10
*

3.4 | Results 3-16
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
In order to avoid unnecessary injury to the lung, tissue biopsies during perfusion are taken from
the periphery of the lung. While these biopsies are assumed to represent cytokine production in the
whole lung, measured tissue cytokine levels only truly represent cytokine production from those areas.
Because cytokines are not cleared rapidly during EVLP, cytokines in the perfusate can be considered to
represent the cumulative amount of cytokines produced by the entire lung. We therefore subsequently
measured cytokine perfusate levels at two different timepoints. There was no difference in levels at 12 h
between the three groups. While the overall trend was similar to tissue levels, the difference in IL-1β
seen in tissue did not occur in the cytokine levels within the perfusate (Figure 3.7).

3.4 | Results 3-17
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Figure 3.7: Perfusate cytokine levels after delivery of IL-10. All values expressed as pg cytokine/mL. (IL-6, IL-8, TNF-α, IL-1β; p=0.21, p=0.33, p=0.31, p=0.78 respectively at 3h and p=0.55, 0.99, 0.46, 0.52 respectively at 12h)
IL-6 in Perfusate
3h 12h 3h 12h 3h 12h0
50000
100000
150000
200000
Control IV IL-10 IT IL-10
IL-6
Lev
el (p
g/m
l)IL-8 in Perfusate
3h 12h 3h 12h 3h 12h0
50000
100000
150000
Control IV IL-10 IT IL-10
IL-8
Lev
el (
pg/m
l)
TNF- in Perfusate
3h 12h 3h 12h 3h 12h0
50
100
150
Control IV IL-10 IT IL-10
TNF-
Lev
els
(pg/
ml)
IL-1 in Perfusate
3h 12h 3h 12h 3h 12h0
50
100
150
200
Control IV IL-10 IT IL-10
IL-1
Leve
ls (p
g/m
l)

3.5 | Discussion 3-18
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
3.5 | Discussion
The development of ex vivo lung perfusion has given us the potential to effect meaningful
change during the time donor lungs are spent outside of the body. Because IL-10 was found to have a
prolonged half-life during EVLP, we assessed the effect of recombinant IL-10 delivery during EVLP on
donor lung function and inflammation during EVLP. Recombinant IL-10 was delivered to the lungs by
two routes: intravascular and intratracheal. For the intravascular route, we simply added rIL-10 to the
circulating perfusate, whereas for the intratracheal route, we utilized an aerosol delivery method in an
attempt to homogeneously deliver rIL-10 to the distal portions of the lung.
While aerosolized drug delivery is commonplace for the treatment of asthma and other airway
diseases, the delivery of aerosols deep into the lung is more challenging. The cross-sectional surface
area of the lung increases drastically with each branching of the pulmonary airways. Consequently,
there is a significant drop off in the velocity of flow as air moves distally into the lung. This has
implications for aerosol delivery. Aerosol particles depend on a high flow velocity to push them around
corners and into the lung. When flow decreases, larger aerosol particles, which possess more inertia, will
fail to turn with the flow and impact onto the airway more proximally than smaller particles. While
smaller particles are more likely to reach the distal portions of the lung, they also carry much less drug
per particle since its volume is proportional to the cube of its radius. Hence, delivery time will be much
longer for fine aerosols. In general, aerosol particles with a diameter of 3-5 μm will deposit in the central
portion of the lung and particles with a diameter of 3 μm or smaller can be delivered more distally.
In the present study, we utilized an Aerogen Aeroneb Solo, a new nebulizer system intended for
ventilated patients. It generates an average aerosolized particle size of approximately 3.3μm which

3.5 | Discussion 3-19
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
balances delivery time with distal aerosol delivery. Delivery of an aerosol during EVLP has some
potential benefits. First, humidified air is not needed for ventilation, thus moisture from the air is less
likely to add to aerosol particle size during delivery. Second, removal of the lungs from the patient
enables the use of ventilation strategies aimed at maximizing aerosol delivery without needing to
consider adequate ventilation of the patient. In this study, we achieved delivery of rIL-10 to the distal
portions of the lung at a concentration of about 7μg/mg protein. Indeed, as expected, proximal IL-10
levels were higher at around 15μg/mg protein after 12 h of perfusion.
When we measured the effect of recombinant IL-10 either on measures of lung function and
cytokine expression, we could not detect any differences from the control group. This is in stark contrast
to a similar study performed by Cypel et al in which measures of lung function improved and tissue pro-
inflammatory cytokine levels fell following IL-10 delivery to the lung using intratracheal adenoviral gene
therapy.113 In that study, Cypel et al could demonstrate tissue levels of around 30pg/mg total protein
following gene therapy. This is higher than the level we could achieve with IT aerosol delivery.
Interestingly, intravenous delivery of rIL-10 did not result in a measurable increase in tissue levels of IL-
10, suggesting that IV rIL-10 could not enter the lung parenchyma.
The anatomical location of IL-10 appears to be important to its biological function. The in vitro
and in vivo effects of IL-10 center on reducing activation of antigen presenting cells (APC). Indeed,
APCs within the lung such as the alveolar macrophage and dendritic cells all express IL-10 receptor, and
the alveolar macrophage plays a central role in cytokine expression following ischemia-reperfusion
injury.92, 210 As an organ exposed to the outside environment, APCs within the lung such as the alveolar
macrophage are present on the epithelial side of the barrier rather than the endothelial side. Thus, IL-10

3.5 | Discussion 3-20
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
must also be present on the epithelial side to cause an effect and this may explain the observation that IV
delivered IL-10 appears to be ineffective.
Alveolar delivery of rIL-10 is already difficult to achieve in high concentrations for reasons
described above. Compounding this difficulty is the discovery that perfusate levels of IL-10 were greatly
elevated by 3 h of perfusion following IT delivery, suggesting that alveolar IL-10 is rapidly cleared into
the circulation over time and thus rIL-10 delivered IT only has a short time to act on APCs in the lung.
IL-10 clearance from the lung is well-described. In studies from this laboratory and others studying
intra-tracheal adenovirus mediated gene therapy, IL-10 levels increased in the circulation following IT
delivery.211 Interestingly, in a study by Minter et al, a comparison was made between intratracheal
adenovirus mediated therapy with human IL-10 and viral IL-10 and they found that viral IL-10
accumulated in the tissue at significantly increased levels compared to human IL-10.212 A future study
comparing the hIL-10 to vIL-10 amino acid sequence may allow for the engineering of an IL-10 protein
which prefers the tissue compartment.
The gene therapy approach may yet overcome these difficulties. Even small amounts of viral
delivery to the alveoli will eventually result in large amounts of alveolar IL-10 as IL-10 will be produced
by the alveolar cells themselves. This eliminates the difficulties with delivering large amounts of rIL-10
to the distal parenchyma. The other major problem is that IT rIL-10 appears to be rapidly cleared to the
perfusate. Thus, rIL-10 delivered IT into the lung has only a short time to act on alveolar macrophages
before leaking into the perfusate. Since IL-10 delivered by gene therapy continuously produces IL-10
within the lung tissue, transgene IL-10 which leeches into the perfusate is continuously replenished
(Figure 3.8). Continuous intra-tracheal rIL-10 aerosolization during EVLP could be considered as an

3.5 | Discussion 3-21
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
alternative solution; however, this reintroduces the problem of cost effectiveness which limited the use
of in vivo delivery of IL-10.
Figure 3.8: Cartoon representation of differences between IL-10 delivered IT via a recombinant protein approach and via a gene therapy approach.
For this study, we chose to deliver rIL-10 to rejected human lungs. Advantages to the use of
these lungs include their human origin and their representation of the complexities of real-world donor
lung injury. However, there can be pitfalls in the utilization of these lungs for experimental studies. The
Toronto Lung Transplant Program is an experienced and aggressive program and utilizes essentially all
transplantable lungs. Moreover, this study was performed in parallel with a clinical trial studying EVLP
evaluation of marginal donor lungs. Thus, the threshold for rejection for clinical use was much higher
and resulted in the majority of the lungs utilized in this study being infected. In this respect, rIL-10
should not have been able to overcome this type of injury and may have affected the benefit of IL-10.

3.5 | Discussion 3-22
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
So though rIL-10 delivery IT or IV did not appreciably affect lung function or cytokine
production in this population of lungs, this study can still demonstrate the concept of drug delivery
during EVLP and the basic pharmacokinetics of rIL-10 delivery. The majority of drugs today are small
molecules rather than proteins, and thus not amenable to gene therapy strategies. Putative therapies
using these drugs, such as antibiotics or β-adrenergic agonists, could benefit from aerosolized delivery to
the lung and this study will aid in the development of these strategies. In the context of clinical IL-10
therapy, the gene therapy delivery approach now appears to be the most attractive option. In the
subsequent chapters, we describe our studies in ex vivo gene therapy and the development of a large
animal injury model on which to test the this therapy.

Chapter 4
Ex Vivo Adenoviral Vector Gene Delivery Results in Decreased Vector-Associated Inflammation Pre- and Post- Lung Transplantation

4.1 | Abstract 4-1
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
4.1 | Abstract
Introduction: Gene therapy is a promising strategy to engineer donor lungs for improved post-
transplant outcomes and ex vivo lung perfusion is a promising platform on which gene therapy vectors
could be delivered. Because an acellular perfusate is used, we hypothesized that inflammation induced
by the vector itself would be reduced during ex vivo lung perfusion. Hence, we compared ex vivo to in
vivo intratracheal delivery of a first generation adenoviral vector.
Materials and Methods: Yorkshire pigs were randomized to either the ex vivo or in vivo group and
then randomized to receive either saline control, adenovirus encoding GFP (AdGFP), or adenovirus
encoding IL-10 (AdhIL-10). Twelve hours following delivery, both AdGFP groups were transplanted
and the post-transplant function verified. The ex vivo AdIL-10 group was also transplanted to assess
pharmacokinetics of IL-10 expression post-transplant.
Results: We could identify transgene expression by 12h in both in vivo and ex vivo delivered groups.
Preservation of lung function occurred in all ex vivo groups following viral vector delivery; however, lung
function decreased in the in vivo delivered AdGFP group with corresponding increases in IL-1β levels.
Good lung function remained in the transplanted ex vivo groups and poor lung function remained in the
transplanted in vivo AdGFP group. Transgene expression continued to occur post-transplant and IL-10
entered recipient plasma following reperfusion.
Conclusion: Adenoviral gene therapy can be successfully delivered ex vivo with less vector-associated
inflammation.

4.2 | Introduction 4-2
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
4.2 | Introduction
In the previous chapter, we attempted to deliver recombinant IL-10 to injured human donor
lungs in an attempt to reduce the pro-inflammatory milieu of the lung prior to transplantation.
However, neither significant reductions in cytokine expression nor improvements in the physiology of
the lung was observed following delivery of rIL-10 intravascularly and intratracheally. Because this was a
departure from previous studies in the lab where IL-10 delivery by adenoviral gene therapy (AdhIL-10)
in both small animal and large animal lung transplant models led to a reduced incidence of ischemia-
reperfusion injury, and AdhIL-10 therapy to a population of injured human donor lungs similar to the
previous chapter led to reductions in pro-inflammatory cytokine production, we chose to explore ex vivo
adenoviral mediated gene therapy for potential clinical translation.122, 152
In the current paradigm of transplantation, translation of the gene therapy strategy to the clinical
arena would necessitate vector delivery to the lungs prior to retrieval as cold preservation prevents any
meaningful gene expression.213 The complicated logistics of transporting and delivering the viral vector
to donors spread across the country combined with the concern of additional injury to donor organs
acquired during the extra hours needed to achieve transgene expression has essentially prevented the
clinical use of this strategy. With the use of ex vivo lung perfusion (EVLP), the metabolic activity of the
lungs is conserved during the preservation phase. This provides a unique opportunity to deliver gene
therapy to a donor organ outside of the body.
Because of the natural tropism of the virus for the respiratory epithelium, there has been
significant interest into the use of replication-deficient adenoviral gene therapy for lung diseases.
Unfortunately, clinical success has been hampered by, among others, vector-associated inflammation,

4.3 | Materials and Methods 4-3
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
finite transgene expression time, and an inadequate proportion of transduced epithelial cells. For our
intended application, many of these limitations are circumvented. First, transgene expression would
only need to occur during reperfusion, thus the finite transgene expression time is inconsequential.
Secondly, IL-10 functions in a paracrine fashion, thus transduction of only a small proportion of cells
would be needed. Thus, the major remaining issue is the difficulty with vector-associated inflammation.
Delivery of adenoviral vectors into the lung elicits an almost immediate innate immune response
in the form of a characteristic pattern of cytokine and chemokine expression by alveolar macrophages.
These signals recruit neutrophils into the lung which propagate the inflammatory response and
ultimately cause lung injury. Given that EVLP preservation utilizes an acellular perfusate, we
hypothesized that intratracheal delivery of a first generation adenoviral vector during ex vivo lung
perfusion would elicit less inflammation compared to in vivo delivery because of the absence of
neutrophils and other immune cells in the circulating perfusate during EVLP.
Herein, we show that delivery of a first generation E1-, E3- deleted adenoviral vector ex vivo
results in less vector-associated inflammation than in vivo delivery and have confirmed adequate gene
expression and good lung function post-transplantation.
4.3 | Materials and Methods
4.3.1 Animals
Male Yorkshire pigs weighing 25-35kg were utilized for studies. All animals received humane
care in compliance with the “Principles of Laboratory Animal Care” formulated by the National Society
for Medical Research and the “Guide for the Care of Laboratory Animals” published by the National

4.3 | Materials and Methods 4-4
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Institutes of Health. The Animal Care Committee of the Toronto General Research Institute approved
all studies.
4.3.2 Porcine Anesthesia
Pigs were sedated with ketamine (40 mg/kg i.m.), anesthetized with inhaled isoflurane (5%)
and maintained with propofol (5–8 mg/kg/h i.v.) and fentanyl citrate (2–20 mg/kg/h i.v.) for the
duration of all surgeries. The airway was secured by tracheostomy and intubation with a size 8.5 French
endotracheal tube.
4.3.3 Lung retrieval
Double lung blocks were retrieved from the pigs similar to that detailed by Pierre et al.214
Animals were ventilated using pressure-control ventilation to a pressure of 15 cm H2O above 5 cm H2O
post-expiratory end pressure (PEEP). Respiratory rate was set initially to 16 breaths per minute but
then titrated to an end-tidal CO2 of 35 mmHg. FiO2 was set to 0.5. Median sternotomy was then
performed. The pericardium was opened and the superior and inferior venae cavae and the ascending
aorta were encircled by 0 silk ties. A purse-string suture was placed into the proximal main pulmonary
artery using a 4-0 polypropylene monofilament suture and then cannulated. 10,000 U of sodium
heparin was then injected systemically. Immediately prior to flushing of the lung, 0.5 mg of
prostaglandin E1 (Prostin, Pfizer Canada, Kirkland, Canada) was injected into the pulmonary artery.
Inflow occlusion was then achieved by ligation of the superior vena cava and inferior vena cava and
division of the left sided azygous vein. Outflow occlusion was achieved by clamping the ascending aorta.
The left atrium was then opened for drainage and then 60 mL/kg of low potassium dextran solution

4.3 | Materials and Methods 4-5
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
(Perfadex, Vitrolife AB, Sweden) was flushed anterograde through the lungs at a height of 30 cm above
the heart. The lungs were then removed from the chest en bloc with the heart in an inflated state taking
extreme care to reduce traction injury and atelectasis of the lower lobes. The heart was dissected off of
the double lung block leaving a large left atrial cuff and long segment of main pulmonary artery.
4.3.4 Ex vivo lung perfusion
EVLP was performed as described in section 3.3.3.
4.3.5 Pig lung transplantation
Pig left lung transplantation was performed as described by Pierre et al.214 Following anesthesia,
monitoring of the pig was aided by insertion of a 9 French sheath into the left jugular vein for Swan-
Ganz catheterization and cannulation of a femoral artery for invasive blood pressure monitoring both by
cut-down. The pig was then turned to lie on its right side and a roll placed under the right chest.
Following shaving of the thoracotomy area, proviodine was applied to the skin. A left sided thoracotomy
was then performed. The left azygous vein was then identified and divided between ties. Nodal
dissection followed allowing for the identification of the left main bronchus and left pulmonary artery.
The left and right pulmonary arteries were then dissected out and encircled with an umbilical tape.
During dissection of the right pulmonary artery, the first branch was identified to ensure the umbilical
tape was placed proximal to it. The left pulmonary veins were then dissected and encircled. Following
heparinization (200 U/kg) with sodium heparin (Leo Pharma, Thornhill, Canada), the left pulmonary
artery was clamped and the pulmonary veins were tied and cut. The bronchus was then clamped and the
lung removed. Ventilation parameters were altered to maintain an end-tidal CO2 of 35 mmHg. The

4.3 | Materials and Methods 4-6
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
atrium was then dissected to allow for a clamp to be placed. The bronchial and arterial anastamoses
were then performed using 4-0 and 6-0 Polypropylene monofilament (Prolene, Ethicon, Johnson &
Johnson Medical Products, Peterborough, Canada) in a running fashion respectively and in that order.
The atrial clamp was then placed onto the atrium and the ligatures on the veins opened. The atrium was
then opened between those two veins to create an atrial cuff. The atrial anastamosis was then performed
using 5-0 Polypropylene using a running everting mattress stitch. Prior to tying the atrial anastamosis,
ventilation to the donor lung was started and the PA clamp opened slightly. This allowed for the de-
airing of the donor lung vasculature through the atrium. When approximately 10 mL of blood flowed
out of the atrium, the atrial anastamosis stitch was tied. The PA clamp was then opened gradually over
the next 5 min to allow for gentle reperfusion of the lung. Following 1 h of reperfusion, the right
pulmonary artery was clamped to ensure survival solely on the transplanted lung. Transplanted lung
function could then be tested by arterial blood gas analysis from the arterial line. PA and RV pressures
could be measured with the Swan-Ganz catheter.
4.3.6 Gene Vector Creation
A first generation (E1-, E3- deleted) serotype 5 adenoviral vector under the control of a
cytomegalovirus promoter and containing the human IL-10 gene was obtained from the Gene Transfer
Vector Core of the University of Iowa College of Medicine (Iowa City, IA). Human IL-10 cDNA was
obtained by polymerase chain reaction (PCR) with 5’ and 3’ flanking primers (5’- hIL-
10BamHI,5’CGCGGATCCCATGCACAGCT-CAGCACTG-3’; 3’-hIL 10BamHI,5’ -
CGCGGATCCGCCACCCT GATGTCTCAGT-3’), using the clone pSRahIL-10 as the template. The
PCR product was cloned, using the BamHI restriction site tails added to the oligonucleotide sequences,

4.3 | Materials and Methods 4-7
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
in a shuttle plasmid. This shuttle plasmid contains the genomic adenoviral sequences from 0–1 and 9–16
map U of human adenovirus type 5. Recombinant adenovirus expressing IL-10 was generated by
homologous recombination between AdhIL-10 and human adenovirus serotype 5 derivative dl309.
The control vector AdGFP was created in a similar manner with pSRaeGFP as the template.
4.3.7 Virus Transfection Technique
1x1010 pfu of AdGFP, 1x1010 pfu of AdhIL-10 or saline control was diluted with normal saline to
a final volume of 10 mL. 4.7 French polyethylene tubing (PE160, Becton Dickenson, Sparks, MD) was
then inserted into the port of a bronchoscope (Olympus Canada, Markham, ON). Ten mL of the
diluted virus mixture was then injected transtracheally via the tube into each of the segmental bronchi of
the lung. After delivery, an inspiratory hold was performed to a peak airway pressure of 25cmH2O and
the lungs ventilated at a higher rate of 10 mL/kg at 12 breaths per minute for a period of 10 min. This
procedure was followed in both the ex vivo and in vivo groups.
4.3.8 Biopsies
In pig lungs, biopsies of the superficial lung was performed every 2 h by ligation of a portion of
lung tissue with 0 silk ties. A portion of the biopsy was immediately snap frozen and another portion was
fixed in 10% buffered formalin for future embedding in paraffin. Perfusate samples were also taken at
this time.
4.3.9 Histopathological Assessment
Formalin fixed tissues of the lung at 12 h after virus delivery were fixed in 10% buffered formalin
for 24 h, embedded in paraffin, sectioned at 5 μm thickness, stained by hematoxylin and eosin (H & E)
4.3 | Materials and Methods 4-8
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
and examined for pathological changes under light microscopy. A staff pulmonary pathologist evaluated
mid-sagittal slices of lung sections in a randomized and blinded fashion to assess histopathological
grading of inflammation using the following parameters: parenchymal inflammation, peri-bronchial
inflammation, and peri-vascular inflammation. The severity of each finding was graded in a four point
scale as follows; 0: absent, 1: mild, 2: moderate and 3: severe and then summed to make a final score.215
4.3.10 Green Fluorescent Protein Staining
For GFP immunohistochemistry, formalin-fixed, paraffin-embedded tissue sections (4 μm
thick) were mounted on positively charged microscope slides. Antigen retrieval was performed with
microwave heating in citrate buffer (10 mM Sodium Citrate, 0.05% Tween 20, pH 6.0). Endogenous
peroxidase and biotin activities were blocked respectively using 3% hydrogen peroxide and avidin/biotin
blocking kit (Lab Vision, Fremont, CA). After blocking for 15 min with 10% normal horse serum diluted
in casein solution (Dako, Carpinteria, CA), polyclonal rabbit anti-GFP primary antibody (Ab290,
Abcam, Cambridge, MA) was applied at 1:1,000 dilution and incubated at room temperature for 30 min.
The detection procedure was performed using a biotinylated goat anti-rabbit secondary (Vector Labs,
Burlingame, CA) for 30 min and horseradish peroxidase-conjugated ultrastreptavidin labeling reagent
(ID Labs, London, Canada) for 30 min. Colour development was done with freshly prepared
diaminobenzidine solution (Vector Laboratories, Burlingame, CA). Finally, sections were
counterstained lightly with Mayer’s hematoxylin to better display nuclei. These slides were then imaged
on a Nikon 80i microscope following Köhler alignment and images recorded using an attached CCD
camera using ACT-4U software.

4.3 | Materials and Methods 4-9
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
For GFP and macrophage immunofluorescence, formalin-fixed, paraffin-embedded tissue
sections (4 μm thick) were mounted on positively charged microscope slides. Antigen retrieval was
performed with microwave heating in EDTA buffer (1 mM EDTA, 0.05% Tween 20, pH 9.0).
Endogenous peroxidase and biotin activities were blocked respectively using 3% hydrogen peroxide and
avidin/biotin blocking kit (Lab Vision, Fremont, CA). After blocking for 15 min with 10% normal horse
serum diluted in casein solution (Dako, Carpinteria, CA), polyclonal rabbit anti-GFP primary antibody
(Ab290, Abcam, Cambridge, MA) was applied at 1:1000 dilution and incubated at room temperature
for 30 min. Following wash with phosphate buffered saline(PBS), monoclonal mouse anti-MAC387
antibody (Ab22506, Abcam) was applied at 1:200 dilution and incubated at room temperature for 30
minutes. A mixture of secondary anti-rabbit and secondary anti-mouse antibodies conjugated with
Alexa Fluor 594 (red) and 488 (green), respectively was then applied at 1:200 dilution each and
incubated at room temperature for 60 min. Slides were then washed and mounted with Vectashield
mounting medium with DAPI.
4.3.11 Homogenization of lung tissue
Lung tissue homogenization and protein extraction were performed as in Section 3.3.6.
4.3.12 Inflammatory Profile in Pig Lung Tissue Biopsies
Supernatants of lung tissues, perfusate samples, and plasma were assayed in duplicate using the
specific ELISA kit for human IL-10, and porcine IL-6, IL-8, TNF-α, and IL-1β (R&D Systems,
Minneapolis, MN). The optical density of each well was read at 450 nm and corrected at a wavelength
of 540 nm according to the manufacturer’s instructions with an NM-600 microplate reader (Dynatech

4.4 | Results 4-10
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Laboratories, Chantilly, VA). The final concentration was calculated by converting the OD readings
against a standard curve.
4.3.13 Statistics
All results were expressed as mean ± standard error of the mean. For comparisons between the
two groups at all timepoints, two-way ANOVA was utilized. For comparisons between three or more
groups, one-way ANOVA was utilized. Post-test analysis between each groups was performed with
Bonferroni correction for multiple comparisons. Students’ t-test was utilized for comparing two groups.
p values less than 0.05 were considered significant.
4.4 | Results
4.4.1 Intratracheal delivery of adenoviral vectors during EVLP results in transgene expression
Adenovirus encoding GFP (AdGFP) was utilized as our vector for the study of vector-associated
inflammation because the GFP transgene product is foreign to the host, provides no known benefit
against vector-associated inflammation, and can act as a reporter in histology. Twelve hours following
the intratracheal delivery of AdGFP, GFP expression could be found in bronchioles and in alveoli.
(Figure 4.1) Distribution of the virus was somewhat patchy, resulting in some portions of the lung not
being transduced; however, GFP expression could be identified in all tissue blocks taken from AdGFP
transduced lungs.

4.4 | Results 4-11
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Figure 4.1: Expression of GFP transgene in a bronchiole and in alveoli 12h following ex vivo delivery. Distribution of GFP was not homogeneous leading to an absence of expression in some lung lobules. (Green: GFP, Anti-GFP; Blue: Nucleus, DAPI)
By assessing GFP expression, we could identify the cell types transduced and found alveolar
epithelial cells and alveolar macrophages expressing GFP (Figure 4.2).
Figure 4.2: Identification of transduced alveolar macrophage. (Red: Alveolar Macrophage, anti-MAC387; Green: GFP, Anti-GFP; Blue: Nucleus, DAPI)
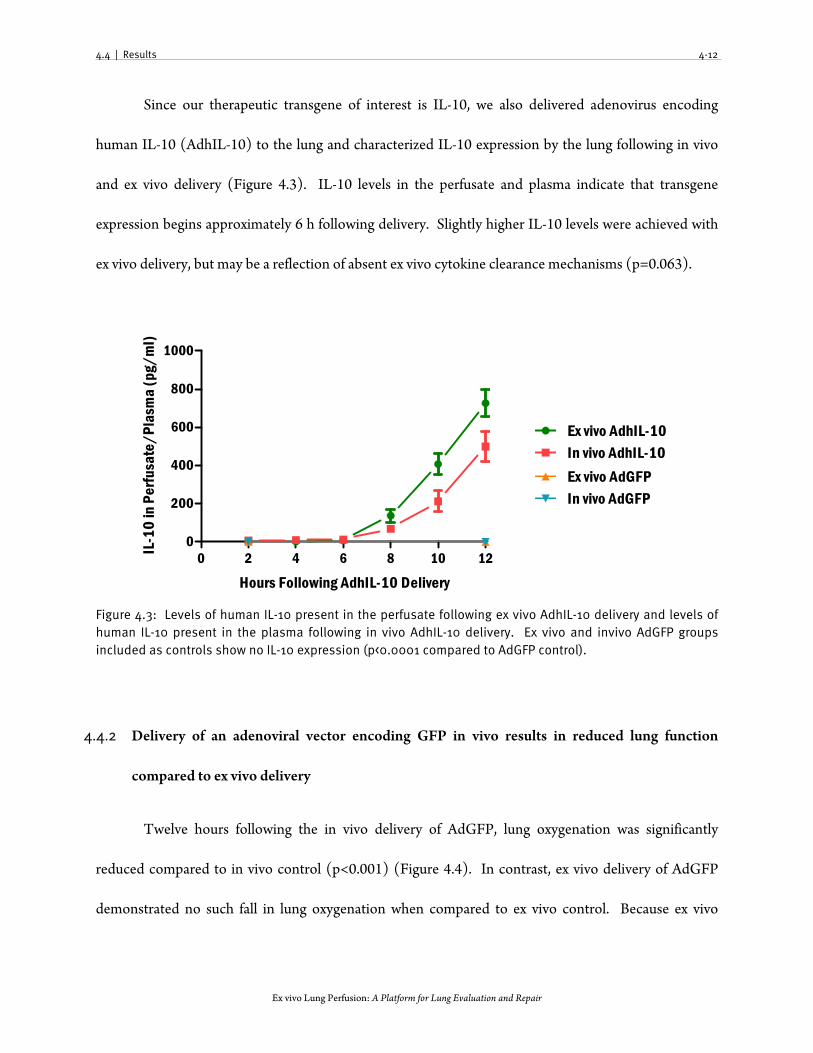
4.4 | Results 4-12
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Since our therapeutic transgene of interest is IL-10, we also delivered adenovirus encoding
human IL-10 (AdhIL-10) to the lung and characterized IL-10 expression by the lung following in vivo
and ex vivo delivery (Figure 4.3). IL-10 levels in the perfusate and plasma indicate that transgene
expression begins approximately 6 h following delivery. Slightly higher IL-10 levels were achieved with
ex vivo delivery, but may be a reflection of absent ex vivo cytokine clearance mechanisms (p=0.063).
Figure 4.3: Levels of human IL-10 present in the perfusate following ex vivo AdhIL-10 delivery and levels of human IL-10 present in the plasma following in vivo AdhIL-10 delivery. Ex vivo and invivo AdGFP groups included as controls show no IL-10 expression (p<0.0001 compared to AdGFP control).
4.4.2 Delivery of an adenoviral vector encoding GFP in vivo results in reduced lung function
compared to ex vivo delivery
Twelve hours following the in vivo delivery of AdGFP, lung oxygenation was significantly
reduced compared to in vivo control (p<0.001) (Figure 4.4). In contrast, ex vivo delivery of AdGFP
demonstrated no such fall in lung oxygenation when compared to ex vivo control. Because ex vivo
0 2 4 6 8 10 120
200
400
600
800
1000
Ex vivo AdhIL-10In vivo AdhIL-10
Ex vivo AdGFPIn vivo AdGFP
Hours Following AdhIL-10 Delivery
IL-1
0 in
Per
fusa
te/P
lasm
a (p
g/m
l)

4.4 | Results 4-13
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
perfusion utilizes a low flow protective perfusion strategy and removes the effect of the chest wall on the
compliance of the lung, PaO2 is higher in the ex vivo control group than in the in vivo control group and
the two control groups cannot be directly compared. Moreover, because of the acellular perfusate, PaO2
changes can be dampened (see Chapter 6). Thus, we also examined other physiologic parameters
during EVLP following Ad delivery but there were no differences in compliance, airway pressure, or
PVR between the three ex vivo vector delivery groups. (Figure 4.5)
4.4.3 IL-10 expression can reduce vector-associated inflammation in vivo
Our therapeutic transgene of interest, IL-10, has been shown to have a beneficial effect on
vector-associated inflammation in small animal models.207 As expected, no additional lung injury
occurred when AdhIL-10 was delivered ex vivo. More importantly, AdhIL-10 delivered in vivo resulted
in better lung function 12 h following delivery when compared to the AdGFP group, further supporting
the evidence that IL-10 can reduce vector-associated inflammation. (Figure 4.4)

4.4 | Results 4-14
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Figure 4.4: Lung function as measured by P/F ratio following vector delivery. At 12 hours, all ex vivo groups showed excellent lung function (p=ns) while in the in vivo groups, AdGFP demonstrated poorer lung function compared to AdhIL-10 and control groups. *p<0.05 at that timepoint, ***p<.001 at that timepoint.
0 1 2 3 4 5 6 7 8 9 10 11 120
200
300
400
500
600
In vivo AdGFP
In vivo AdhIL-10
In vivo Control
Ex vivo AdGFP
Ex vivo ControlEx vivo AdhIL-10
****
***
******
***
Time Post-Vector Delivery (h)
PaO
2 at
100
% F
iO2

4.4 | Results 4-15
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Figure 4.5: Physiologic measures following ex vivo vector delivery. A: Compliance; B: Airway pressure; C: Pulmonary vascular resistance. p=0.98, p=0.77, p=45, respectively
0 1 2 3 4 5 6 7 8 9 10 11 12 130
20
40
60
Time Following Vector Delivery
Com
plia
nce
(mL/
cm H
2O)
0 1 2 3 4 5 6 7 8 9 10 11 12 130
2
4
6
8
10
Time Following Vector Delivery
Airw
ay P
ress
ure
(cm
H2
O)
0 1 2 3 4 5 6 7 8 9 10 11 12 130
200
400
600
Time Following Vector Delivery
PVR
(dyns
cm-5
)
Control AdGFPAdhIL-10
A
B
C

4.4 | Results 4-16
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
4.4.4 In vivo delivery of AdGFP results in inflammation on histology
Examination of histology following Ad gene delivery mirrors the physiological results. In the ex
vivo gene therapy groups, an absence of lung inflammation is seen. However, in the in vivo gene therapy
groups, significant inflammation is observed in the AdGFP group and some inflammation is observed in
the AdhIL-10 group (Figure 4.6).
Figure 4.6: Representative histological sections of Ad transfected lung tissue (H&E stain). Panels A, C, E represent in vivo control, AdhIL-10, and AdGFP, respectively. Panels B, D, F represent ex vivo control, AdhIL-10 and AdGFP, respectively. Note the alveolar macrophages present within the bronchioles.

4.4 | Results 4-17
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Entire sections were blindly scored for inflammation by a pulmonary pathologist (Dr. David
Hwang, Figure 4.7).
Figure 4.7: Quantitative scoring for inflammation, *p<0.05 compared to respective control.
We noticed that some portions of the lung were more inflamed than others. Therefore, we
stained these sections for GFP to see if there was a correlation between transduction and inflammation.
Indeed, areas of the lung which were spared AdGFP infection do not demonstrate inflammation at 12h
after AdGFP delivery. (Figure 4.8)
Control
AdGFP
AdhIL-10
Control
AdGFP
AdhIL-10
0
2
4
6
8
In vivo Ex Vivo
Infla
mm
atio
n Sc
ore * *

4.4 | Results 4-18
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Figure 4.8: Inflammation in AdGFP delivered in vivo follows cellular transduction (Anti-GFP immunohistochemistry with DAB, hematoxylin-counterstained) Arrows indicate GFP expression. Rectangles represent enlarged areas.
4.4.5 Pro-inflammatory cytokines are increased in viral delivery groups
We subsequently measured cytokine and chemokine expression within the lung tissue. The ex
vivo and in vivo AdGFP groups expressed significantly higher levels of IL-1β than their respective
controls(Figure 4.9). Ex vivo transduced groups expressed higher levels of IL-8 levels than control. No
significant differences were found in IL-6 and TNF-α.

4.4 | Results 4-19
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Figure 4.9: Pro-inflammatory cytokine expression in tissue 12h following delivery of vector. Significant elevation in IL-8 occurred in ex vivo gene therapy groups following vector delivery when compared to control. Significant elevations in IL-1β occurred following AdGFP vector delivery in vivo and ex vivo. *p<0.05 compared to its respective control.
IL-8 Levels 12h Post-Delivery
Ex Vivo
Control
Ex Vivo
AdGFP
Ex Vivo
AdhIL-10
In Vivo Contro
l
In Vivo AdGFP
In Vivo AdhIL-10
0
20
40
60
80
IL-8
Lev
els
(pg/
mg
prot
ein) *
*
IL-1 Levels 12h Post-Delivery
Ex Vivo
Control
Ex Vivo
AdGFP
Ex Vivo
AdhIL-10
In Vivo Contro
l
In Vivo AdGFP
In Vivo AdhIL-10
0
100
200
300
400
500
IL-1
Leve
ls (p
g/m
g pr
otei
n)
*
*
IL-6 Levels 12h Post-Delivery
Ex Vivo
Control
Ex Vivo
AdGFP
Ex Vivo
AdhIL-10
In Vivo Contro
l
In Vivo AdGFP
In Vivo AdhIL-10
0
10
20
30
40
IL-6
Lev
els
(pg/
mg
prot
ein)
TNF- Levels 12h Post-Delivery
Ex Vivo
Control
Ex Vivo
AdGFP
Ex Vivo
AdhIL-10
In Vivo Contro
l
In Vivo AdGFP
In Vivo AdhIL-10
0
5
10
15TN
F-
Lev
els
(pg/
mg)

4.4 | Results 4-20
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
4.4.5 Absence of vector-associated injury is preserved post-transplantation
To assess whether vector-associated inflammation becomes evident upon reintroduction of the
transfected lung to an in vivo environment, we transplanted the left lung of the AdGFP transduced lungs
into another pig. Immunosuppression was not given to avoid dampening the inflammatory response.
Lung function in the ex vivo AdGFP group was excellent. In comparison, in vivo AdGFP transduced
lungs continued to demonstrate poor lung function post-transplant (Figure 4.10). Again, because IL-10
is our therapeutic transgene of interest, we also transplanted the ex vivo AdhIL-10 group as a proof-of-
concept of this approach and also to assess IL-10 expression and kinetics post-transplantation. Lung
function was preserved in the ex vivo AdhIL-10 group.
Figure 4.10: PaO2 post-transplantation. PaO2 in the ex vivo AdGFP group were superior to the in vivo AdGFP group. *p<0.05 compared to ex vivo AdGFP group, post-transplant data only.
0 2 4 6 8 100
12 13 14 15 16
200
300
400
500
600
700
In vivo AdGFP
In vivo AdhIL-10
In vivo Control
Ex vivo AdGFP
Ex vivo ControlEx vivo AdhIL-10
Pre-Transplant Post-Transplant
Transplant
**
**
Time (h)
PaO 2 a
t 100
% F
iO2

4.4 | Results 4-21
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
4.4.6 Transgene expression is preserved post-transplantation
In order for adenoviral gene therapy to be feasible, transgene expression needs to persist into the
early post-reperfusion period. Thus, we re-examined transgene expression 4h post-transplant. GFP
expression persisted in lungs post-transplantation in both ex vivo and in vivo transduced groups. IL-10
was produced at high enough levels to be detectable within the plasma and increased in a linear fashion
(Figure 4.11).
Figure 4.11: IL-10 levels in AdhIL-10 recipient plasma. Following ex vivo delivery of AdhIL-10, human IL-10 can increasingly be detected in the plasma of recipients over the 4 h of reperfusion.
4.4.7 Pro-inflammatory cytokine expression is reduced in ex vivo transduced groups
Reperfusion following transplantation further elevated all measured cytokines. IL-10
transduced lungs had reduced levels of IL-6 in the plasma. In vivo transduced lungs had higher levels of
IL-8, IL-1β, and IL-6 (Figure 4.12).
0 1 2 3 4 50
500
1000
1500
2000
2500
Time Post Transplant (h)
IL-1
0 Le
vels
in P
lasm
a (p
g/m
L)

4.4 | Results 4-22
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Figure 4.12: Cytokine/chemokine levels following transplantation. All numbers expressed as pg cytokine/mg tissue protein (* p<0.05).
4.4.8 Histologic inflammation is much higher in in vivo AdGFP group
We subsequently examined the histology of the lungs post-transplant and found significantly
increased inflammation within the tissue in the in vivo group, but the ex vivo groups remained generally
normal (Figure 4.13). Quantitative scoring is represented in Figure 4.14.
IL-8 Levels 4h Post Transplant
Ex vivo
AdhIL-10
Ex vivo
AdGFP
In vivo AdGFP
0
50
100
150
200
250
IL-8
Lev
els
(pg/
mg)
IL-1 Levels 4h Post-Transplant
Ex vivo
AdhIL-10
Ex vivo
AdGFP
In vivo AdGFP
0
500
1000
IL-1
Leve
ls (p
g/m
g)
IL-6 Levels 4h Post-Transplant
Ex vivo
AdhIL-10
Ex vivo
AdGFP
In vivo AdGFP
0
50
100
150
200
IL-6
Lev
els
(pg/
mg)
TNF- Levels 4h Post-Transplant
Ex vivo
AdhIL-10
Ex vivo
AdGFP
In vivo AdGFP
0
5
10
15
20TN
F-
Lev
els
(pg/
mg)
**
**

4.4 | Results 4-23
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Figure 4.13: Representative histological sections of Ad transfected lung tissue post-transplantation (H&E stain). Panels A, B, and C represent in vivo AdGFP, ex vivo AdGFP, and ex vivo AdhIL-10, respectively.
Figure 4.14: Quantitative scoring for inflammation, *p<0.05 compared to respective ex vivo AdGFP. p=0.0077 overall.
AdGFP
AdhIL-10
AdGFP
0
2
4
6
8
Ex Vivo In vivo
Infla
mm
atio
n Sc
ore
*

4.4 | Discussion 4-24
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
4.4 | Discussion
In this study, we described the use of EVLP as a platform for gene therapy using a first-
generation adenoviral vector in the context of lung transplantation. Despite the relatively recent
introduction of EVLP, there has been significant interest by the lung transplantation community and a
clinical trial has recently been completed by the Toronto Lung Transplant Program demonstrating
equivalent early outcomes following EVLP preservation of marginal donor lungs.114 We believe that
novel applications using EVLP will serve to further accelerate adoption of this technique into the clinical
arena.
In studies involving both small and large animal models of lung transplantation, intra-tracheal
IL-10 delivery by adenoviral gene therapy has been shown to impart beneficial effects following
reperfusion.122, 152 However, clinical implementation of this strategy has been impeded by several factors.
First, the current strategy of cold organ preservation reduces metabolic activity to the point that viral
delivery following organ retrieval does not result in transgene expression at reperfusion. Hence, in order
for adequate amounts of transgene to be expressed at the time of reperfusion, vector delivery to the lungs
needs to occur while still within the donor and organ retrieval must be delayed at least six to nine hours
to allow for transgene expression. During this time, donor organs would be susceptible to further injury
by the hostile brain-death environment. More critically, as Ad vector delivery to the lung activates the
innate immune system, the donor lungs would be also subject to vector-associated inflammation. This
causes not only direct injury while in the host but also exacerbates ischemia-reperfusion injury following
transplantation. IL-10 itself can help to reduce vector-associated inflammation and de Perrot et al have
described the use of methylprednisolone prior to AdhIL-10 delivery to combat the early vector-

4.4 | Discussion 4-25
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
associated inflammation which occurs prior to the expression of significant IL-10 levels.207 Indeed, our
in vivo AdhIL-10 group demonstrated reduced lung injury compared to our in vivo AdGFP group;
however, this effect would not be generalizable to other potentially beneficial transgenes which may not
possess an anti-inflammatory effect.
Since the acellular perfusate used for EVLP does not contain any pro-inflammatory cells, we
hypothesized that propagation of the inflammatory response to adenoviral vector would be limited
during ex vivo perfusion. Thus, in this study, we described the use of normothermic ex vivo lung
perfusion as a platform on which adenoviral gene therapy can be delivered to donor lungs for
transplantation. Using this strategy, we could demonstrate excellent transgene expression both pre- and
post- transplantation. Furthermore, lungs transduced with Ad vector ex vivo demonstrated reduced
functional and histological markers of injury compared to in vivo groups and reduced cytokine and
chemokine production, post-transplantation. This benefit was preserved into the early post-transplant
period where again both transgene expression and lung function were excellent and superior to in vivo
gene therapy groups.
With this schema of delivery, organs can be procured and transported back to the transplant
hospital in the usual fashion with gene therapy delivery occurring at the transplant hospital using EVLP.
As donors are spread out across the country, this greatly simplifies the logistics of vector delivery.
Furthermore, recent attempts to expand the donor pool have led to the increasing use of donor lungs
retrieved after cardiac arrest of the donor. As death is not pronounced until cardiac arrest, no
opportunity for gene therapy would be present prior to organ retrieval; hence, ex vivo gene therapy
would be the only option for this ever-increasing lung pool.

4.4 | Discussion 4-26
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Overall, this chapter demonstrates ex vivo IL-10 gene therapy as a clinically applicable and
biologically advantageous strategy for our goal of improving the resilience of donor lungs during
reperfusion.

Chapter 5
Physiological Characteristics of Ex vivo Lung Perfusion of a Brain Death Injured Lung

5.1 | Abstract 5-1
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
5.1 | Abstract
Introduction: Testing of EVLP drug therapies will necessitate the development of animal models to
simulate common lung injuries seen in clinical lung transplantation. Given that the vast majority of
organs today come from brain dead donors, almost all donor lungs have been exposed to the sequelae of
brain death. Thus, we elected to simulate brain-death lung injury in a porcine model of lung
transplantation and evaluate the physiologic characteristics of these lungs during EVLP.
Materials and Methods: Yorkshire pigs were randomized to injury by brain death and cold ischemia
and to control groups. Brain death was established by inflation of a Foley catheter in the epidural space
of the skull and confirmed by cerebral angiography. Lungs from these pigs were then stored at cold
ischemia and perfused on EVLP for 12 h.
Results: In injured lungs, lung compliance decreased and peak airway pressure increased during EVLP.
A high pulmonary vascular resistance was observed in injured lungs at the beginning of perfusion but
subsequently fell to near control levels by the end of perfusion. However, a high pulmonary vascular
resistance was found post-transplant and led to the death of three recipients. PaO2 remained stable
during perfusion in both injured and control groups and did not predict for post-transplant function
which was dismal in the injured group.
Conclusions: Lung injury caused by brain death and prolonged cold ischemia was detectable during
EVLP. This model can be used to test current and future EVLP therapies.
5.2 | Introduction 5-2
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
5.2 | Introduction
In the previous two chapters, we described different strategies for drug delivery to the lungs
during EVLP. As potential novel therapeutic strategies are envisioned and developed, the effectiveness
of these strategies will need to be tested in pre-clinical models of lung transplantation. In Chapter 3, we
utilized injured human lungs rejected for transplantation to test rIL-10 therapy. However, because of
both the aggressive use of donor lungs by the clinical lung transplant program and the clinical use of
EVLP for the evaluation of questionable lungs, the majority of the rejected lungs sent for research had
injuries such as pneumonia and aspiration and may not best represent lungs which can be repaired by IL-
10 therapy. Moreover, a regular supply of these lungs cannot be guaranteed and, more importantly,
post-transplant outcomes cannot be assessed. Thus, animal lung injury models need to be developed
which simulate common clinically-relevant lung injuries such as contusion, aspiration, and pneumonia
for a controlled and relatively high-throughput assessment of potential EVLP therapies.
Previous studies in the lab have utilized relatively gentle models of lung injury, if any, for EVLP.
Only normal lungs109 and lungs subjected to 12 h of cold ischemia112 have been assessed by Cypel et al
during the development of EVLP. In these previous studies, lungs which were injured by prolonged cold
ischemia have performed well for 12 h of EVLP but it is currently unclear how highly injured lungs
would perform during EVLP. Understanding how injured lungs express their injury during EVLP will be
important for the use of EVLP both as a lung evaluation platform and as a lung therapy platform.
Because transplantation of an injured lung can lead to primary graft dysfunction in the recipient,
lung transplant clinicians are highly conservative in the selection of donor lungs for transplantation.
Improved evaluation of donor lungs using EVLP would provide the confidence needed by lung

5.3 | Materials and Methods 5-3
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
transplant clinicians to transplant more borderline lungs, potentially allowing for a resultant increased
utilization of offered donor lungs simply due to improved evaluation itself. Accurate evaluation will also
appropriately direct the use of therapeutics and aid in the recognition of improvement in the lung
following therapeutic delivery.
Since the major source of organs today come from brain-dead donors, almost all lungs retrieved
and utilized for transplantation have been exposed to the sequelae of brain death. Simulating brain
death injury in an animal model thus appears to be an important first injury model towards the
development of clinically relevant injury models. Moreover, because the lungs would be exposed to the
pro-inflammatory milieu of brain death, this model is also perfectly suited for our therapy of interest, IL-
10.
Therefore, in this chapter, we describe the development and utilization of a porcine brain death
and prolonged cold ischemia injury transplantation model with EVLP and present data showing the
physiological pattern of an injured lung while on EVLP.
5.3 | Materials and Methods
5.3.1 Study Design
Pigs were randomized to either the control group (n=5) or the injury group (n=5). In the
control group, lungs were perfused without exposure to brain death and cold ischemia was limited to 1 h
during which the EVLP circuit was prepared. Injury group lungs were subjected to 10 h of brain death
and ventilation and then 24 h of cold ischemia prior to starting EVLP.

5.3 | Materials and Methods 5-4
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
5.3.2 Brain death
Following anesthesia, brain death was induced in 30-35 kg Yorkshire pigs similar to that detailed
by Novitzky et al in the baboon.216 Following anesthesia, a temporal burrhole 6mm in diameter was
drilled into the skull taking care not to breach the dura. A Foley catheter was then inserted into the skull
extradurally and inflated slowly over 5 min to a total volume of 30ml. Intracranial pressure was
monitored with a pressure transducer and maintained at a level that exceeded the mean arterial pressure
by at least 50mmHg for 10h to obliterate cerebral perfusion. Lack of cerebral blood flow was confirmed
using a pre-/post-epidural balloon inflation cerebral angiogram. Cerebral angiography was performed
by surgically exposing the left femoral artery, distal ligation of the artery and placement of a proximal
ligature to permit the insertion of a 5 French endovascular catheter (Cordis Envoy, Cordis Canada,
Markham, Ontario) via a 3mm arteriotomy. The catheter was guided to the right internal carotid artery
under fluoroscopy (Philips BV-29, Philips Canada, Mississauga, Ontario) with intermittent 5-7 mL
boluses of Visipaque contrast solution (Iodixanol, 652 mg/mL, GE Healthcare Canada, Mississauga,
Ontario). Cerebral angiography was obtained using fluoroscopic subtraction angiography data
collection during a bolus of 10 ml Visipaque. Brain death was confirmed by repeat cerebral angiography
to confirm absence of cerebral blood flow, clinical examination to confirm absent motor exam and loss
of brainstem reflexes, and atropine (5mg) stimulation test. Lung retrieval commenced 10 h after
inflation of the Foley catheter.
5.3.3 Statistics
All results were expressed as mean ± standard error of the mean. For comparisons between the
two groups at all timepoints, two-way ANOVA was utilized. For comparisons between three or more

5.4 | Results 5-5
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
groups, one-way ANOVA was utilized. Post-test analysis between each groups was performed with
Bonferroni correction for multiple comparisons. Students’ t-test was utilized for comparing two groups.
p values less than 0.05 were considered significant.
5.4 | Results
5.4.1 Brain Death Induction
To confirm brain death status, we performed cerebral angiography. In brain dead pigs,
angiography failed to show flow into the cerebral vessels post-rete mirabele. (Figure 5.1A) These pigs
also demonstrated the expected brain death physiologic response with an initial hypertensive crisis
corresponding to the adrenergic storm followed by hypotension. (Figure 5.1B). Clinically, there was an
absence of brain stem reflexes and pupils were fixed and dilated. An atropine stimulation test, which
seeks tachycardia following an intravenous push of 5mg atropine was also negative at 1 h post-Foley
inflation.

5.4 | Results 5-6
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Figure 5.1: Confirmation of Brain Death
A: Cerebral angiography, right internal carotid injection (catheter tip at arrowhead) via a transfemoral endovascular catheterization demonstrating flow through the rete mirabele (*) with perfusion of bilateral cerebral hemispheres at baseline (Pre) and repeat injection following inflation of epidural foley catheter (Post) demonstrating absent flow in the cerebral hemispheres and retrograde flow down the contralateral internal carotid artery consistent with malignant intracranial hypertension.
B: Mean arterial pressure (MAP) following brain death induction. Significant increase in MAP immediately following inflation of epidural foley catheter consistent with sympathetic storm. Relative hypotension following brain death induction indicative of subsequent Cushing's response.
0 2 4 6 8 100
50
100
150
200
250
Hours
MAP
(mm
Hg)
B

5.4 | Results 5-7
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
5.4.2 Physiologic Changes during EVLP
PaO2 was similar in both injury and control groups across all 12 h of EVLP. (Figure 5.3, p=0.9)
While the PVR in the injury group was initially significantly higher than that of controls (p=0.01 @ 1h),
it decreased over 12h of EVLP to levels close to that of the control group (p>0.05 @ 12h). In the injury
group, dynamic compliance was initially similar to the control group (p>0.05 @1h), then subsequently
decreased further over the following 12 h of EVLP. Control lungs, in contrast, showed a slight increase
in dynamic compliance over that same timeframe. Airway pressure in the injured group was initially at
the same level as in control group lungs (p>0.05 @ 1h) but then continuously increased over the next 12
h. In contrast, control lungs slightly dropped their airway pressure over that time. Differences between
the two groups were statistically significant (p=0.0009).
5.4.3 Edema formation during EVLP
Edema formation was evident during EVLP in the injured lung group. There was a significant
increase in wet/dry ratio between control and injured lung groups (Figure 5.2).
Figure 5.2: Wet/Dry Ratio following 12 h EVLP. *p=0.0028

5.4 | Results 5-8
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Figure 5.3: Changes in PaO2, PVR, Compliance and Airway Pressure during EVLP. Labels - * p<0.05, ** p<0.01 at that timepoint. p value under each graph signifies overall difference between each group. (n=5)
A: PaO2 was stable during 12h of EVLP in both injured and control groups.
B: PVR started high in injured lungs but fell to near-control levels by 12h of EVLP. p=0.01
C: Compliance was similar between injured lungs and control lungs at 1h of perfusion, p>0.05. Compliance subsequently fell in injured lungs while control lungs experienced a slight increase in compliance, p<0.0001.
D: Airway pressure was stable in control lungs but rose significantly in injury lungs, p=0.0009.
PVR During EVLP
0 1 2 3 4 5 6 7 8 9 10 11 120
500
1000
1500 ** ** ** ** *
Time (h)
PVR
(dynsc
m-5
)
Airway Pressure During EVLP
0 1 2 3 4 5 6 7 8 9 10 11 120
10
20
30 * ** ** ** ** ** ** ** ** **
Time (h)
Airw
ay P
ress
ure
(cm
H2O
)
Compliance During EVLP
0 1 2 3 4 5 6 7 8 9 10 11 120
20
40
60 ** ** ** ** ** ** ** ** ******
Time (h)
Com
plia
nce
(mL/
cm H
2O
)PaO2 During EVLP
0 1 2 3 4 5 6 7 8 9 10 11 120
200
400
600
Time (h)
PaO
2 (m
mH
g)
Injured Lungs
p=0.0009p<0.0001
p=0.90 p=0.01
Control Lungs
A B
C D

5.4 | Results 5-9
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
5.4.3 Lung Function Following Transplantation
As PaO2 during EVLP remained similar to the control group in the brain death injured group
despite degradation in other physiologic parameters, we transplanted the left lung to confirm whether
the good PaO2 was predictive of post-transplant PaO2. There was a striking difference in lung function
between the control group and the injury group. The control group had excellent lung function
following transplantation while the injury group had very poor lung function. (Figure 5.4A) Moreover,
in the injury group, three recipients died following transplantation due to right heart failure from
ischemia-reperfusion related increases of PVR or no-reflow phenomenon in the transplanted lung; one
at 1h reperfusion and two at 2 h of reperfusion. (Figure 5.4B) The dead pigs were assigned their last
PaO2 for subsequent hours of evaluation.
Figure 5.4: Lung Function and PA Pressure Following Left Lung Transplantation and Occlusion of Right Pulmonary Artery. Labels - ** p<0.005 for that timepoint, ! signifies death of one recipient at that timepoint. (n=5)
A: Significantly lower PaO2 was observed in injured lungs compared to control lungs, p<0.001. Three recipients died in the injury group before 4h of reperfusion. Last PO2 recorded was assigned to deceased pigs to calculate means.
B: Following right PA clamp, a higher PA pressure was recorded in injured lungs, *p=0.0021.
PO2 Following Transplantation
0 1 2 3 4 50
200
400
600 ** ** ** **
Time Post Transplant (h)
PO2
(mm
Hg)
Mean PA Pressure Following Right PA Clamp
Control Injured0
20
40
60
80
Mea
n P
A Pr
essu
re (m
mH
g)
Injured LungsControl Lungs
! !!
A B
*

5.5 | Discussion 5-10
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
5.4.4 Vascular Reactivity to Hypoxic Ventilation during EVLP
Because of the fall in PVR over 12 h of EVLP despite evidence of lung injury, we chose to
evaluate lung vascular reactivity using ventilation with 100% N2 gas. Upon ventilation with 100% N2, we
would expect hypoxic vasoconstriction to increase PVR through the lung. Ventilation with 100% N2
resulted in a rapid increase in PVR at the onset of EVLP. However, following the development of
edema, ventilation with 100% N2 resulted in a greatly dampened PVR response at the end of EVLP
(Figure 5.5).
Figure 5.5: Effect of ventilation with 100% N2 on pulmonary vascular resistance at the onset of EVLP versus following the development of injury at the end of EVLP (p<0.001, n=2)
5.5 | Discussion
In this study, we sought to develop a clinically relevant injury model for use with EVLP and
EVLP based therapies. We developed and utilized a porcine lung injury model by subjecting pig lungs to
a combination of brain death and prolonged cold ischemia prior to EVLP for 12 hours.109 Using this
0 2 4 6 8 100
1000
2000
3000
4000
Beginning of EVLP
End of EVLP
Minutes following N2 Ventilation
Pulm
onar
y Vas
cula
r Res
ista
nce
(dyn s
cm
-5)

5.5 | Discussion 5-11
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
model, lungs were sufficiently injured for the injury to be detected during EVLP and for post-transplant
lung function to be dismal. By varying the time of brain death and cold ischemia, this injury model could
be useful for the testing of potential therapies such as IL-10.
Previous studies have utilized prolonged cold ischemia as an injury model but the injury was not
severe enough to be evident during EVLP. In this study, the physiological characteristics of an injured
lung during EVLP was characterized. The major differences in the physiological parameters measured
between the injury model group and the control group were compliance and airway pressure. PVR was
initially higher in the injury model group but subsequently fell back to near normal levels. PaO2 did not
differ between the two groups during all 12 hours of EVLP.
Development of lung edema is the common endpoint of the clinical syndrome of primary graft
dysfunction89 and is thought to begin with endothelial barrier injury leading to the development of
interstitial edema.217, 218 A similar process appears to occur during EVLP. As described by Staub et al,
fluid accumulating in the interstitial space will begin by surrounding the vessels and airways. When this
space is filled, edema of the alveolar wall will develop and lead to subsequent leakage of fluid into the
alveolus.219 Eventually, enough fluid accumulates within the alveolus such that the inflation pressure is
unable to maintain a stable inflated alveolus and the alveolus collapses into a new, smaller volume,
configuration. This leads to V/Q mismatch in the lung. The mechanical effects of increasing water
content in the lung is unchanged by the perfusion strategy and the stiffness generated by interstitial and
alveolar edema will lead to a fall in compliance. Indeed, clinically obvious edema formation occurred in
this injury model and was matched by a significant fall in compliance.

5.5 | Discussion 5-12
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Since we utilize a volume control mode for ventilation, a fall in the lung compliance will result in
higher airway pressures and translate to higher measured peak airway pressures on the EVLP system.
Theoretically, if pressure control ventilation was utilized for ventilation of the lung, a fall in the delivered
tidal volume would be measured instead; however, we have not utilized this mode of ventilation neither
experimentally nor clinically to confirm this. With volume control ventilation, usually by the time
alveolar edema is severe enough to impact PaO2, it should already be clinically evident that the lungs
should be rejected.
The response of our lung injury model on PVR was not anticipated. While there was an elevated
PVR during the initial hours of perfusion as would be expected with lung injury, there was a subsequent
fall in PVR down to levels close to that of control lungs by 12 h of perfusion, suggesting improvement.
However, lung injury by other measures were evident and severe lung injury was confirmed by
transplantation. We hypothesized that the progression of injury during EVLP injured the vasculature to
the point that reactive vasoconstriction was impaired and we tested this using the phenomenon of
hypoxic pulmonary vasoconstriction. This severe vascular injury could also help explain the post-
transplant "no-reflow" phenomenon observed upon clamping of the right pulmonary artery. Indeed,
following the fall in compliance and the development of edema, there was a significant reduction in
hypoxic pulmonary vasoconstriction in response to ventilation with 100% N2. However, the mechanism
remains unclear. Whether it is direct injury to the vasculature or a result of a metabolite generated by
lung injury is unclear. While the perfusate does become acidic owing to the buildup of lactate over
time220, it was shown in a dog model that metabolic acidosis potentiates rather than impairs hypoxic

5.5 | Discussion 5-13
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
pulmonary vasoconstriction.221 Certainly, further study of this phenomenon is warranted and EVLP
provides an excellent platform on which to study hypoxic pulmonary vasocontriction as a phenomenon.
The apparent lack of effect of developing edema and lung injury on PaO2 during EVLP also
needs to be explored. As this model creates lung injury by potentiating brain death injury with cold
ischemic injury, there is no obvious edema at the onset of EVLP. Thus, the formation of edema only
occurs during EVLP. This developing edema can cause V/Q mismatch but because this formation is
early, it is unlikely to cause shunt. Therefore, when combined with the high FiO2 and the PEEP of 5 cm
H2O utilized for evaluation, the effect of developing edema on PaO2 is minimized; however, the
mechanical effects can be seen in other physiological parameters.
In summary, we developed a severe lung injury model using brain death and cold ischemia and
characterized the physiologic effects of this model during EVLP. The development of EVLP therapies
will depend on both the availability of clinically relevant models of lung injury and the ability to
recognize when a lung is deteriorating or improving during EVLP. Despite increasing use of DCD lungs,
brain death donors will continue to be the major pool of donor lungs in the near-future. Thus, this
injury model represents a highly clinically relevant model of lung injury and will be particularly useful for
our therapeutic of interest, IL-10.

Chapter 6
Exploration of EVLP Physiology and Implications for Lung Evaluation

6.1 | Abstract 6-1
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
6.1 | Abstract
Introduction: In a brain-death injury model, PO2 did not fall appreciably during EVLP despite
clinically evident edema and poor post-transplant outcomes. We hypothesized that the acellular
perfusate utilized for EVLP alters the response of PO2 during injury. Thus, in this chapter, we utilized a
shunt model and a brain-death injury model with acellular and cellular perfusates to further explore this
hypothesis.
Materials and Methods: Lungs from 30-35kg Yorkshire pigs were utilized for this study. A shunt
model was created by clamping the left main bronchus during EVLP. A brain death lung injury model
was also utilized. Comparison of PO2 levels were made between acellular perfusion and cellular
perfusion.
Results: PO2 fell with the clamping of the left main bronchus during acellular perfusion. However, PO2
fell further with the addition of red blood cells to the perfusate. In the brain death injury model, addition
of red blood cells to the perfusate also further lowered the PO2. The P/F ratio was lower at an FiO2 of
21% than at an FiO2 of 100%, indicating that areas of V/Q mismatch were present within the lung.
Conclusions: PO2 is reactive to shunt during both acellular and cellular perfusion. However, the
amount of reactivity is dampened with the use of an acellular perfusate. This effect should be considered
during EVLP lung evaluation and clinical use of EVLP for evaluation should encompass other
physiologic measures in addition to just PO2.

6.2 | Introduction 6-2
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
6.2 | Introduction
In the above chapter, we developed a clinically-relevant injury model on which EVLP
therapeutic agents can be tested and we characterized its physiological parameters during EVLP.
Interestingly, PaO2 did not change appreciably despite dismal post-operative function. While this can be
partially explained by the high FiO2 (100%) and PEEP (5 cm H2O) used to evaluate the lung, there are
theoretical differences in lung physiology during EVLP when compared to lungs in the in vivo state.
These differences may further explain the PaO2 values obtained. Moreover, a deepened understanding
of this phenomenon will be important for the use of EVLP as a method of lung evaluation. The Toronto
method of EVLP perfusion differs from the in vivo state in two main respects: 1. perfusion flow is
lowered to 40% normal and 2. the perfusate is acellular. In this chapter, we explored the effect of these
differences on PaO2 as a measure of lung function during EVLP.
In the first major change, the perfusate flow is lowered to 40% of normal. Because ventilation is
not reduced by a similar amount, the overall V/Q ratio decreases. Thus, while the normal overall V/Q
ratio is approximately 0.8 in the average human, the overall V/Q ratio increases to approximately 1.8
during EVLP. The relative lowering of the perfusion rate results in a lower PA pressure and can lead to
an expansion of West Zone I within the lung. This would result in increased dead space or wasted
ventilation but this should not affect PaO2.
The second major change in the Toronto strategy is the use of an acellular perfusate. This
change could theoretically affect PaO2 due to an effect on the post-capillary mixing of perfusate. Oxygen
levels in the blood are measured clinically by the PO2 within the fluid; however, this is actually a
surrogate marker as the measurement of interest is oxygen availability but direct measurement of oxygen

6.2 | Introduction 6-3
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
this is difficult. Rather, by knowing the PO2 to O2 content curve, clinicians can approximate the O2
content from the much more easily measured value of PaO2. When mixing occurs, it is the oxygen
content which is being mixed and not the PO2; the oxygen content in the resulting mixed fluid generates
a new PO2. Oxygen content can be calculated from PO2 using equation 6.1. Since the hemoglobin level
is 0 in an acellular solution, the first term in that equation is zero and thus the PO2 to O2 content curve is
linear for an acellular solution (Figure 6.1). In contrast, in a cellular solution, the curve develops a
plateau with increasing PO2 as a result of saturation of hemoglobin molecules with oxygen. Since there
is no plateau in an acellular solution, perfusate leaving alveolar units with a high PO2 will greatly raise the
PO2 of perfusate leaving alveolar units with low PO2 when mixed. However, in a cellular solution, the
plateau in oxygen content with increasing PO2 limits the effect of high PO2 blood on low PO2 blood
(Figure 6.2).
Oxygen Content 1.36 0.0031
Equation 6.1: Oxygen Content Equation

6.2 | Introduction 6-4
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Figure 6.1: Difference in PO2 to oxygen content curve between acellular Steen solution and blood. Assumptions include: Hemoglobin concentration of 15mg/dl, pH=7.4, normothermia
To illustrate this concept, we can consider a lung with 40% shunt (Figure 6.2). Because of the
plateau, alveolar units producing well-oxygenated blood cannot overcome the blood with low PO2
coming from shunting alveolar units, but in the acellular solution, it can. Thus, a difference in PaO2 can
be predicted between perfusion with an acellular perfusate and that of blood.
Oxygen Content in Steen vs Blood
200 400 600-5
0
5
10
15
20
25
PO2 (mm Hg)Oxy
gen
Cont
ent (
ml O
2/10
0ml f
luid
)
Blood
Steen

6.3 | Materials and Methods 6-5
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Figure 6.2: Differences in predicted PaO2 following shunt from clamping of left main bronchus. Assumptions in this model: Perfusion to right lung is 60%. PaO2 at 100% is 650mmHg. Mixed venous PO2 is 70mmHg. Red and blue lines represent PO2 and the corresponding oxygen content of shunted perfusate and fully oxygenated perfusate, respectively. Green lines represent the oxygen content and its corresponding PaO2 following mixing. Dotted green lines are shown to represent the difference between PO2 in cellular and acellular solutions. Predicted PaO2 is 190 mmHg with blood and 380 mmHg with acellular Steen.
Thus while the de facto clinical standard is an assessment of lung function by PaO2 and, indeed,
published reports of lung evaluation during EVLP have utilized the partial pressure of oxygen in the
post-lung perfusate (PaO2) as the major parameter of lung function222, 223, a better understanding of PaO2
in the context of EVLP as performed in Toronto is needed for the intelligent evaluation of donor lungs
during EVLP.
6.3 | Materials and Methods
6.3.1 Ex vivo lung perfusion
Normal porcine lungs were subjected to EVLP as described in section 3.3.3.
0 200 400 600 8000
5
10
15
20
25
Oxy
gen
Cont
ent (
ml O
2/10
0ml f
luid
)
Cellular
PO2 (mm Hg)
50%
50%
0 200 400 600 8000.0
0.5
1.0
1.5
2.0
2.5
Oxy
gen
Cont
ent (
ml O
2/10
0ml f
luid
)
Acellular
PO2 (mm Hg)
50%
50%

6.4 | Results 6-6
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
6.3.2 Retrieval of blood
During the donor operation described in section 4.3.3, prior to cannulation of the pulmonary
artery, the sternotomy was extended into a laparotomy down to the bladder. Both renal arteries, the
celiac trunk, and the superior mesenteric artery were encircled with 0 silk ties. The pulmonary artery
was then cannulated after which the infra-renal aorta was cannulated with a 28F chest tube adapted to fit
a blood collection bag containing 50 ml of citrate phosphate dextrose blood preservation solution. All
the aforementioned arteries were then tied off and blood allowed to flow into the blood collection bag.
One liter of whole blood was collected into the blood bags and placed on ice. Lung retrieval then
proceeded as normal. Just prior to use, the collected whole blood was centrifuged at 1000 g for 9
minutes and the acellular fraction removed.
6.4 | Results
6.4.1 Exploration of V/Q Matching
Because the perfusion rate during EVLP is reduced to around 40% of normal, we studied V/Q
matching using the difference between the PaCO2 and the end tidal CO2 (P(a-ET)CO2) in normal
porcine lungs at different perfusate flow rates. This difference is a common measure of V/Q matching
throughout the lung. Lower relative amounts of perfusion for ventilation should cause a greater
difference in P(a-ET)CO2 due to dilution of the alveolar CO2 by hypocarbic deadspace gas upon
exhalation. Measurement of this difference is used clinically by intensive care physicians to assess
overventilation of intubated patients and has also been utilized to assess the adequacy of CPR during
periods of cardiac arrest, where like the EVLP situation, a lower cardiac output is experienced. At 40% of

6.4 | Results 6-7
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
perfusion, an increased P(a-ET)CO2 difference was found (8.2mm Hg), suggesting increased dead-
space ventilation. As perfusion flows were increased to 100% cardiac output, P(a-ET)CO2 fell to
3mmHg, suggesting reduced dead space ventilation and improved V/Q matching (Figure 6.3).
Figure 6.3: Changes in P(a-ET)CO2 with changes in perfusion flow. Dotted line signifies EVLP strategy flow rate. Dashed line signifies estimated normal cardiac output flow rate. P(a-ET)CO2 fell with increasing perfusion flows (7.1mmHg at 1.1L/min, 3.0mmHg at 3.0L/min) n=2.
However, this increased deadspace did not affect the outflow PO2. PO2 did not change between
various percentages of cardiac output (Figure 6.4).
0.0 0.5 1.0 1.5 2.0 2.5 3.0 3.50
10
20
30
40PaCO2
ETCO2
P(a-ET)CO2
Perfusion Flow
PCO
2(m
m H
g)

6.4 | Results 6-8
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Figure 6.4: PO2 at different percentages of cardiac output, n=2.
6.4.2 Exploration of Acellular Perfusion
We then explored the theoretical effects of an acellular solution on PaO2. Normal lungs were
started on EVLP, ventilated at 100% FiO2 and the PaO2 measured. The lungs were then ventilated at
21% of FiO2, deflated and then the left main bronchus clamped. This causes a shunt through the left
lung. The right lung was then ventilated at 100% FiO2 for 10 minutes and the PaO2 measured.
Following clamping, there was a fall in the measured PaO2 (Figure 6.5). As shunted perfusate
completely bypasses the lung, it is not affected by the lung and represents a venous admixture. This
hypoxic shunted perfusate mixes with oxygenated perfusate coming from the lung and dilutes the PaO2.
0 20 40 60 80 1000
200
400
600
800
FiO2 = 100%FiO2 = 21%
% Estimated Cardiac Output
PO2
(mm
Hg)

6.4 | Results 6-9
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Figure 6.5: Effect of clamping left main bronchus on PaO2. PaO2 fell from 630mmHg±10 pre-clamp to 393±18 post-clamp. (n=2, p=0.0075)
Subsequently, we added a concentrated volume of red blood cells to the initially acellular
perfusate. We measured the PaO2 at 5% hematocrit and 18% hematocrit. With each increase in
hematocrit, the PaO2 fell as predicted. (Figure 6.6)
Figure 6.6: Effect of hematocrit on PaO2 following clamping of left main bronchus, n=2, representative case shown.
No Shunt Shunt0
200
400
600
800
PaO
2 (m
mH
g)
0 5 10 15 200
100
200
300
400
500
Hematocrit (%)
PaO
2 (m
mH
g)

6.4 | Results 6-10
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
We then explored the effect of hematocrit on the lung injury model described in the previous
chapter. Following the fall in compliance and increase in airway pressure, we measured the PaO2 at an
FiO2 of 100% and 21%. We subsequently added RBCs to a hematocrit of 20% and measured the PaO2 at
an FiO2 of 100% and 21% and measured a distinct fall in PaO2. To confirm that the added RBCs did not
cause lung injury leading to the fall in PaO2, we then flushed out and re-primed the circuit with fresh
acellular Steen solution. Following the return to acellular perfusion, PaO2 returned to the pre-RBC level
(Figure 6.7). While the P/F ratios at 21% and 100% of FiO2 were similar during acellular perfusion,
there was an increased difference between these P/F ratios with cellular perfusion (Figure 6.8).
Figure 6.7: Effect of hematocrit on PaO2 in brain death injury model, n=2, representative case shown.
0% HCT
20% HCT
0% HCT0
100400
450
500
550
600Initial 0% HCT
Return to 0% HCT20% HCT
PaO
2 at 1
00%
FiO
2(m
m H
g)
0% HCT
20% HCT
0% HCT0
50
100
150
PaO
2 at 2
1% F
iO2
(mm
Hg)

6-11
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Figure 6.8: Comparison of P/F ratios at different hematocrit levels, n=2, representative case shown.
6.5 | Discussion
The apparent reduced effect of developing edema on PaO2 during EVLP seen in Chapter 5 was
explored in this chapter. We hypothesized that some aspect of our protective strategy for EVLP may
alter lung physiology to account for this effect. The protective EVLP strategy deviates from the in vivo
situation in two major ways: a reduced perfusion flow and an acellular perfusate. While we could
confirm that the reduced perfusion flow results in increased dead space, we also showed that this does
not affect PaO2.
We subsequently looked at the use of an acellular perfusate in EVLP. We first predicted the
effect of an acellular perfusate by using a mathematical model described in the introduction. This model
predicted that the use of an acellular perfusate would affect the PO2 due to the post-capillary mixing of
perfusate coming from poorly ventilated regions with perfusate coming from well ventilated regions. We
tested this hypothesis using two models. The first model involved clamping the left bronchus of a
0100200
300
400
500
6000% HCT20% HCTReturn to 0% HCT
21%100% 21%100% 21%100%
FiO2
P/F
Rati
o (m
mH
g)

6.5 | Discussion 6-12
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
normal lung which simulated a situation of pure shunt. This model is an extreme test as perfusate flow
from the entire left lung acts as a venous admixture. This is less clinically relevant but demonstrates a
large, easily measured difference and is independent of FiO2. We subsequently returned to our brain
death injury model in Chapter 5. While this model is less extreme in terms of venous admixture, it
represents the situation of combined V/Q mismatch and shunt and is thus more clinically relevant. In
both models, we could show that increasing the RBC content of the perfusate would lower the measured
PO2 when compared to acellular perfusion.
As a result, use of an acellular perfusate appears to minimize the fall in PO2 in response to injury.
Lung injury can cause lowered PO2 by two methods: V/Q mismatch and shunt. In shunt, alveoli are so
filled with fluid that blood passing through these alveolar units cannot be oxygenated and thus a venous
admixture occurs. Because the shunted alveolar units are not ventilated at all, raising FiO2 has no effect
on PaO2. In V/Q mismatch, alveoli are partially filled with fluid so that the V/Q ratio is lowered. In this
case, the alveolar unit has too low an amount of oxygen to fully oxygenate blood passing through that
unit. However, raising the FiO2 will increase the PO2 of fluid passing through that alveolar unit because
the increased FiO2 will increase the available alveolar PO2 within the lowered V/Q alveoli, however
small. Indeed, this is why clinicians ventilate patients at 100% FiO2 to remove hypoxia caused by V/Q
mismatch in the lung. In this experiment, we could demonstrate this concept by showing a difference in
the P/F ratio at an FiO2 of 21% and the P/F ratio at an FiO2 of 100% when a cellular perfusate was
utilized. Since giving an FiO2 of 100% obscures the effect of V/Q mismatch, this difference represents
the amount of V/Q mismatch in the lung and suggests that evaluation at an FiO2 of 21% would be more
sensitive to the detection of lung injury. Interestingly, this gap was not seen when an acellular perfusate

6.5 | Discussion 6-13
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
was utilized. This suggests that the lower oxygen flux needed for the equilibration of alveolar PO2 with
capillary PO2 also reduces the contribution of V/Q mismatch.
The above considerations can be summarized into a clinically applicable evaluation strategy
where physiologic parameters including PaO2, compliance, airway presssure, and PVR are considered
(Table 6.1). First, unlike the current clinical evaluation of lungs where the decision for utilization mostly
occurs at one timepoint, i.e. organ recovery, EVLP evaluation is best performed over a period of at least
3 to 4 hours to allow injury to express itself on the circuit. During this time, compliance, PO2 and airway
pressure should be continuously measured and the trends plotted to allow for the detection of edema
formation.
Table 6.1: Summary of EVLP-Associated Effects on Physiologic Measures of Lung Function
Summary
PO2 Largely a reflection of shunt Acellular solution decreases effect of shunt on PO2. Acellular solution removes effect of low V/Q regions on PO2.
Compliance and Airway Pressure Reflection of ongoing development of edema
Pulmonary Vascular Resistance Pulmonary vasoconstrictive response dampened during EVLP
Unlike our injury model, injured donor human lungs can present with pre-existing consolidation
from other conditions such as pneumonia or aspiration. These conditions will cause V/Q mismatch
and shunt and, thus, a fall in PaO2 at the onset of EVLP. Because of the reduced effect on PaO2 during
acellular perfusion, a higher threshold for concern in PaO2 should be established to better identify these
injuries. The other physiologic parameters are also important. If there is a downward trend in

6.5 | Discussion 6-14
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
compliance and an upward trend in airway pressure, this indicates that the air/fluid barrier is no longer
intact and serious consideration for rejecting those lungs should be made. Of note, these parameters are
mutually exclusive. Deteriorating compliance with a good PaO2 may signify the development of edema in
a lung with no shunt segments and is a bad sign. In contrast, stable compliance but low PaO2 could
merely be a result of atelectasis, or it could be a result of pre-existing consolidated pneumonia in which
case the lung should not be used.
Because lungs are often poorly inflated at the outset of EVLP, PaO2 will often increase over the
first hour of EVLP as the lung warms and atelectasis is recruited. It is important not to consider this an
improvement in the lungs themselves. Rather, it is merely the reduction of shunt caused by atelectasis
acquired during organ recovery and transport. Thus, we consider timepoint zero in our evaluation
process to be after the initial 1 h warm up of perfusion, and compare the subsequent compliance and
airway pressures for a further 3 to 4 hours only to this number.
In the immediate future, clinical adoption of EVLP will likely be driven by the promise of donor
lung evaluation. Thus, a good understanding of early physiological parameters of lung injury on the
EVLP circuit is necessary. Ultimately, we hope that EVLP physiologic evaluation, combined with future
molecular assessment and ex vivo therapeutic techniques will lead to safer and increased lung transplant
volumes.

Chapter 7
Summary and Future Directions

7.1 | Summary 7-1
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
7.1 | Summary
Arguably, the single most pressing concern facing lung transplantation today is the shortage of
acceptable donor organs. While organ shortage is a universal concern for all of solid-organ
transplantation, donor lung shortages are particularly severe owing to the low utilization of donor
organs. The major underlying reason for the low utilization of donor lungs is the concern about primary
graft dysfunction following transplantation of an injured organ. Indeed, this concern is justified as donor
lungs are particularly susceptible to injury from the sequelae of brain death and ICU care. However, this
problem is greatly compounded by the imprecise evaluation of donor lungs prior to transplantation.
The current evaluation of the donor lung graft is a combination of x-ray imaging, bronchoscopy, lung
function, immunologic testing, and clinical evaluation. While this method is particularly effective in the
identification of ideal lungs, ideal lungs only make up 10-15% of offered donor lungs. To increase the
utilization of donor lungs, almost all lung transplant centers now utilize extended criteria donor lungs.
However, defining an absolute cutoff of when a lung should or should not be used is difficult using the
current lung evaluation technique. Thus, more experienced centers tend to be able to utilize more
organs safely than less experienced centers. To effectively push the envelope of safe utilization of
extended criteria donor lungs by all centers, increased confidence in donor lung quality must be instilled
into the transplant clinicians. Certainly, increased experience in lung transplantation develops into
increased confidence, but this is not always a practical solution for all transplant programs around the
world due to geographic, demographic, social and/or political factors. Improved evaluation techniques,
then, would be a superior method to impart confidence for the use of extended-criteria donor lungs.
The recent development of stable prolonged ex vivo lung perfusion demonstrates great potential to act

7.1 | Summary 7-2
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
as a platform for the improved evaluation of donor lungs. More excitingly, lungs deemed to be injured
can potentially be recovered prior to transplantation while on EVLP. This thesis has begun to explore
this novel paradigm for lung transplantation.
7.1.1 Paradigm change in lung transplantation
The classical paradigm for lung transplantation is detailed in Figure 7.1. In this current
paradigm of lung transplantation, the decision to utilize donor lungs is made before explant and the
possibility to repair the organ is limited to the donor prior to retrieval. With the development of EVLP,
two new paradigms now exist. First, evaluation of the donor lung and, more importantly, the decision to
utilize the organ now can occur following retrieval and at the transplant hospital. Second, during the
time the lung is on EVLP, treatments individualized to identified lung injuries can be applied, salvaging
these lungs for utilization. (Figure 7.1, right)

7.1 | Summary 7-3
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Figure 7.1: Schema of transplantation in the current era and in the era of ex vivo evaluation and repair. Note delay of decision making and anticipated increase in transplanted organs.
7.1.2 Lung evaluation
Part of this thesis explored the unique physiology of EVLP in an attempt to better understand
parameters of evaluation during EVLP. Much like in vivo lung evaluation today, ex vivo lung evaluation
will need to encompass a variety of metrics for accurate lung evaluation. The strategy developed for safe
prolonged EVLP utilizes a lower, non-physiologic perfusate flow and an acellular perfusate.
Consequently, a better understanding of the resultant physiology is needed for the accurate evaluation
of lungs. The use of acellular perfusate changes the oxygen content to PO2 curve to a linear one and
does not plateau like the curve seen in blood. Thus, while blood with a very high PO2 does not contain
appreciably higher oxygen than blood with a moderate to low PO2, perfusate with a high PO2 contains
Ex Vivo Evaluation and RepairCurrent Standard
Donor Management
Organ Procurement
Cold Static Preservation
Ex vivo Evaluation
Transplantation
Employ Repair Strategy*DECISION*
Donor Management
Organ Procurement
Cold Static Preservation
Transplantation
Decline Questionable Organs*DECISION*
Good
Bad
Discard

7.1 | Summary 7-4
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
relatively much higher levels of oxygen than perfusate with a moderate to low PO2. As the arterial
pressure of oxygen leaving the lung represents the net value of a mixture of the perfusate coming from
each alveolar unit, perfusate PO2 is affected much less by poorly oxygenated alveolar units than blood
PO2. Thus, the effect of low V/Q units and shunt is minimized with acellular perfusate.
Because PaO2 changes are dampened by the acellular solution of EVLP, falls in PaO2 will mostly
be caused by shunt rather than by low V/Q segments, particularly if the FiO2 is 1. In the situation of
shunt, perfusate passing through the shunt segment acts as a venous admixture, thus lowering PaO2
regardless of lung function. Therefore, if an excellent (>450mmHg) PaO2 is not identified following
recruitment of the donor lung, a significant area of shunt will be present. If the recruitment was done
carefully and completely, the remaining causes of shunt segments will be consolidation from either
pneumonia, hemorrhage, or aspiration - all causes for rejection of the donor lung.
Though the protective perfusion strategy alters the use of PaO2 as an early measure of lung
function, the mechanical effects of increasing edema on the lung are unchanged. As fluid leaks into the
airspaces along the interstitium, the lung will become increasingly stiff and changes in compliance will
begin to occur. This is reflected, obviously, in the compliance measured by the ventilator. However, as
compliance is not constant over the range of differing pulmonary inflations, definition of a "normal"
compliance is difficult or impossible. As an injured lung is expected to continuously leak fluid into the
airspaces, compliance should thus continuously fall. Therefore, to utilize compliance as a measure of
lung injury, a series of compliances will need to be measured at the same ventilation settings, where a
decreasing compliance will suggest that the lung is beginning to leak fluid. This fall in compliance will
also affect airway pressure and tidal volume, depending on the mode of ventilation utilized. In these

7.1 | Summary 7-5
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
experiments, volume control ventilation was utilized so airway pressure will increase with decreased
compliance.
With the understanding of the altered lung physiology during EVLP, the objectivity and ease of
lung evaluation has been improved. Despite this, it is important to be reminded that lung evaluation,
even on EVLP, is based on a constellation of findings rather than one specific number. Moreover, even if
a theoretically ideal evaluation of the donor lung is available, donor evaluation is only half of the
equation. Recipient matching and recipient factors play major roles in the outcome of transplantation,
in particular known and as-of-yet unknown immunologic factors.
7.1.3 Lung repair
Improved lung evaluation is important to the immediate future because of the confidence it will
instill in transplant programs to utilize lungs which they currently consider too marginal or unsafe to
utilize. However, if lung evaluation is effective, it should also confidently identify lungs which are too
injured to be utilized. For these lungs, therapies individualized for the identified injury should be
developed to repair the lungs to a state of usability. In this thesis, we also explored ex vivo gene therapy
as a strategy for lung repair.
Gene therapy is a highly promising therapeutic strategy. Though originally envisioned as a
treatment for genetic diseases where loss-of-function mutations in key genes lead to a phenotype of
disease, clinical use of gene therapy has not been particularly successful in that regard due to the limited
timeframe of expression of the transgene and the immune reaction to the vector itself. In
transplantation, organs are most susceptible to injury and failure following the serious insult of cold

7.1 | Summary 7-6
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
ischemia at the time of reperfusion. Genetic modification of organs to produce a more resilient organ at
and through the time of reperfusion has been envisioned to improve post-transplant outcomes. As the
target event, reperfusion, is of a limited timeframe, lifelong gene expression is not required. Clinical
application of this concept has not occurred because of two major reasons. First, transgene expression of
clinically relevant levels, regardless of vector, requires 6-12h to achieve; this amount of time is currently
not available during donor management to allow for vector delivery. Second, inflammation caused by
the vector can injure the organ itself, limiting the usefulness of this strategy.
A portion of the thesis explored the use of ex vivo lung perfusion as a platform for the delivery of
gene therapy. As a platform, EVLP is inherently useful to the clinical translation of gene therapy in
transplantation as it solves the logistical problems of where and when gene therapy is delivered. In this
study, clinically relevant levels of transgene were detectable six to nine hours following ex vivo
intratracheal delivery to donor lungs. Moreover, transgene expression continued through reperfusion
and into the early post-transplant period. Thus, gene therapy could occur to donor lungs during EVLP
following retrieval from the donor body.
The second but more important problem is that of vector-associated inflammation. Delivery of
a viral vector has been shown to activate the innate immune response and lead to signaling events which
act to recruit pro-inflammatory cells from the peripheral circulation. In the unique situation of EVLP
where the lung is isolated from other organs, no peripheral inflammatory cells can be recruited and thus
no inflammatory response can be propagated. When adenoviral vector was delivered ex vivo, there was a
reduction in the amount of lung inflammation when compared to in vivo delivery. Lungs subjected to ex
vivo adenoviral delivery demonstrated no decrease in lung function during the entire 12 hour phase of ex

7.1 | Summary 7-7
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
vivo perfusion. In contrast, lungs subjected to in vivo adenoviral delivery suffered a significant decrease
in lung function during a similar amount of time. Histologically, there was increased inflammation
within the in vivo delivered group, particularly in the transduced parenchyma. Moreover, pro-
inflammatory cytokine expression was elevated in the in vivo transduced group which was likely the
precursor to the inflammation. To investigate whether the return of an immune system 12 hours
following adenoviral delivery would result in inflammation, the ex vivo transduced lungs were
transplanted into a recipient. These lungs continued to demonstrate excellent lung function and
transgene expression.
A more pressing concern facing transplant clinicians today are the majority of lungs which are
already injured at the time of retrieval by infection, aspiration, or contusion. While gene therapy may
eventually play a role in the treatment of such conditions, contemporary treatments for these conditions
include small molecules in addition to proteins. Thus, development of methods for the delivery of small
molecule therapeutics such as antibiotics is needed. In addition, since EVLP is unique in that it isolates
the lung from other organ systems, protein therapeutics which normally possess a short half-life in vivo
may have much lengthened half-lives ex vivo and therefore will not need gene therapy for delivery. In
another part of the thesis, recombinant IL-10 was utilized as a prototypical therapy to test EVLP drug
delivery. It was delivered to clinically-rejected injured human lungs in an attempt to reduce
inflammation and improve function both intravascularly via the perfusate and intratracheally as an
aerosol.
To deliver rIL-10 via the intravascular route, lyophilized rIL-10 was simply added to the
perfusate. For intratracheal delivery, an aerosol delivery method was utilized in an attempt to better

7.1 | Summary 7-8
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
uniformly deliver the drug of interest to the lung and to deliver the drug to the peripheral parenchyma.
Alveolar delivery was deemed to be important because the majority of lung injuries tend to affect the
alveolar spaces, i.e. pneumonia or contusion. In addition, for our application of IL-10, a cellular target of
interest was the alveolar macrophage, a major contributor of cytokines to reperfusion injury. When rIL-
10 was delivered to the perfusate, high levels of IL-10 could be detected in the perfusate even at 12 h of
perfusion, confirming the prolonged half-life of the cytokine in the EVLP circuit. However, perhaps
surprisingly, tissue levels of IL-10 were undetectable. For intratracheal delivery using an aerosol delivery
method, high IL-10 levels could be detected in the perfusate by 3 h of perfusion. While tissue levels were
higher near the central airways and lower in the periphery, detectable amounts of IL-10 could be found
throughout the lung. This gradient was expected as it is unlikely that any type of aerosol delivery will
result in equal peripheral and central delivery. Since peripheral IL-10 was indeed detectable, a
percentage of aerosolized drug is reaching the periphery thus increased dosage or repeated or
continuous administration could increase peripheral levels, if needed.
Following delivery of IL-10, no significant difference could be found in measures of lung
function between controls and both IL-10 groups. In all cases, pro-inflammatory cytokines IL-6, IL-8,
TNF-α, and IL-1β increased despite IL-10 therapy. This is in stark contrast to a previous study where
rejected human lungs which received adenoviral vector encoding IL-10 intratracheally demonstrated a
reduction in pro-inflammatory cytokines from baseline 12 hours following AdhIL-10 delivery. In both
delivery methods, high levels of perfusate IL-10 could be identified. Even though tissue levels of IL-10
were higher with transtracheal delivery, high levels of perfusate IL-10 suggest that the majority of the
dose is leeching into the perfusate, where it may not have a biological effect. In contrast, adenoviral
7.2 | Conclusion 7-9
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
vector delivered IL-10 is continuously produced by the epithelial cells where it has an opportunity to act
in a paracrine fashion before leeching into the perfusate. Thus, rather than a "one-shot" effect through
the lung as with intratracheal rIL-10 delivery, continuous production (and effect) is attained with gene
therapy.
Even though this specific application of IL-10 did not demonstrate any benefit, we were still able
to demonstrate delivery of a drug to the lung during EVLP with persistance throughout EVLP and some
pharmacokinetic effect, i.e. travel of rIL-10 from airspace to perfusate. Expansion of these delivery
strategies to other agents may yet prove to be beneficial to specific lung injuries.
7.2 | Conclusion
With the ongoing shortage of acceptable donor lungs for transplantation, strategies to expand
the donor pool are needed. Many strategies have focused on expanding the absolute quantity of lungs
available, but given that only 25% of available lungs are utilized today, a major impact on lung transplant
volumes could be made if utilization rate were simply to increase with no increase in donor number.
This thesis has introduced a paradigm where donor lungs are reassessed and then repaired ex vivo prior
to transplantation with the help of a new normothermic organ preservation technology known as ex vivo
lung perfusion. With increased understanding of the physiology of the lung during EVLP, parameters of
lung injury have been defined to help better evaluate potential organs. Organs which prove to be injured
can potentially be repaired during EVLP and most injured organs have tolerated 12 h of EVLP to allow
this process to occur. Gene therapy as a repair strategy is benefitted by EVLP due to a reduction in
vector-associated inflammation and delivery of drugs by both intratracheal and intravascular means
during EVLP is possible. Thus, though further studies into the specifics of lung repair are still required,

7.3 | Future Directions 7-10
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
this novel paradigm for lung transplantation demonstrates great potential to improve the future of lung
transplantation and patient outcomes.
Overall, this thesis explored a new paradigm in lung transplantation, where donor lungs are
better evaluated and reconditioned prior to transplantation outside of the donor body for increased safe
utilization of donor organs.
7.3 | Future Directions
7.3.1 Exploration of recombinant IL-10 delivery with an animal model
The pharmacokinetics of recombinant IL-10 delivery to injured human lungs was unexpected
and merits further investigation. We utilized injured human lungs because we felt that benefit in this
population of lungs would lead to rapid clinical translation. However, because of the seeming
ineffectiveness of recombinant IL-10, the next step should be to return to a large animal model for
further study. In this thesis, we developed a brain-death porcine model. This model is ideally suited to
the testing of IL-10 therapy as it exposes the lung to the cytokine storm and inflammatory response of
brain death. Use of an animal model would allow for much superior control of the type and severity of
lung injury and would better reveal subtle improvements by IL-10.
7.3.2 Continuous delivery of intra-tracheal IL-10
Delivery of rIL-10 intra-tracheally by aerosol led to a rapid increase in perfusate IL-10 levels,
suggesting that the majority of parenchymal IL-10 was leaking into the perfusate. One counter for this
effect would be to continuously aerosolize a lower dose of rIL-10 into the airway for the duration of
EVLP. Use of this delivery method as a separate arm of the above experiment using an animal model or

7.3 | Future Directions 7-11
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
with injured human lungs would allow for the study of the pharmacokinetics and effectiveness of this
strategy.
7.3.3 IL-10 Protein Engineering
An alternative to continuous delivery could be to modify the IL-10 protein itself to prefer to stay
within the alveolar space. Human IL-10 appears to be cleared relatively rapidly from lung tissue.
Indeed, given the effects of cytokines, this is logical. However, IL-10 produced by viruses is meant to
help viruses to evade the immune system. Thus, rapid clearance is undesirable and evolution seems to
have engineered an IL-10 which is cleared less rapidly.212 One step could be to confirm this
characteristic by delivering recombinant viral IL-10 intra-tracheally to lungs. If successful, the sequences
leading to this delayed clearance could be identified and engineered into a chimeric IL-10. Moreover,
the amino acid responsible for immune activation by IL-10 has been identified and this amino acid could
also be altered during this process.224
7.3.4 EVLP Gene Therapy for Lung Repair
Ex vivo perfusion appears to be an ideal platform for the delivery of gene therapy to lungs prior
to reperfusion in the recipient. The two major impediments to gene therapy in transplantation: time for
transgene expression and vector-associated inflammation, appear to be largely addressed. However, this
study only followed post-transplant outcomes for four hours. A future direction should be to develop a
survival model of transplantation to assess vector-associated inflammation at timeframes beyond 4 h of
reperfusion. Moreover, the timeframe of transgene expression in the presence of transplant
immunosuppression and the amount of IL-10 released into the systemic circulation can then be

7.3 | Future Directions 7-12
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
assessed. Demonstration of safety in this survival model will likely be the last step before clinical trials of
this technique.
7.3.5 Novel Vectors for Gene Therapy
Since the conception of this study, techniques to generate novel adenoviral vectors at quantities
amenable for use in humans/large animals have been developed. One such vector is the helper-
dependent adenovirus vector (HDAd). Lacking in all viral protein coding sequences, these vectors are
thought to generate less adaptive immunity following transduction as no foreign viral proteins are
expressed, and thus displayed by cell-surface MHC. In theory, immune responses against helper-
dependent Ad vectors will only occur by innate immune mechanisms against the capsid at the time of
delivery and cellular transduction. Hence, because EVLP reduces the propagation of this innate
immune response, HDAd delivery during EVLP will avoid innate immunity via EVLP and adaptive
immunity via HDAd. This could result in prolonged transgene expression following transplantation and
thus could be a strategy utilized for long term immunomodulation of the donor organ.
Chapter 4 demonstrated that IL-10 transgene product following AdhIL-10 transduction could
be detected in the plasma following transplantation. While this may be beneficial, one major problem is
the lack of control of transgene production following viral delivery. Specifically, some control of
transgenes with narrow therapeutic windows would be needed for safe clinical utilization. Recently,
adenoviral vectors with inducible promoters have been developed which could potentially be attempted
in a large animal model. Vectors have been created where the transgene is under the control of an IL-6
promoter.225 Thus, this transgene would potentially only be activated during states of inflammation.

7.3 | Future Directions 7-13
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
Other more traditional approaches to transgene expression control such as tetracycline switches could
also be investigated in a large animal model.226
7.3.6 EVLP Lung Evaluation of Other Lung Injury Models
Herein, we proposed that initial PaO2 be used to identify areas of consolidation and falls in
compliance be used to identify lungs developing edema during EVLP. In an attempt to generate a
clinically relevant model of lung injury, a brain death model was developed and utilized to create the
injury. However, as with all experimental models, this model does not completely encompass the
spectrum of clinical lung injury. Specifically, this model does not replicate common injuries
encountered in clinical practice such as consolidative injuries, i.e. pneumonia or aspiration, and
mechanical injuries, i.e. contusion. We believe that PaO2 can be used to assess for consolidative injuries
but this needs to be formally tested in injured lungs. Therefore, we propose two strategies to improve
this situation. First, as consolidation is a highly common finding, we suggest developing a lung
consolidation injury model in pig to use for EVLP assessment. This will help confirm the use of initial
PaO2 as a method to identify consolidated areas with the option of correlating evaluation to post-
transplant outcomes. Second, to better recognize patterns of injury, rejected human lungs with a known
mechanism of injury should be perfused for 12 hours. Though post-transplant outcomes following
EVLP of these human lungs cannot be ascertained, for obvious reasons, similar patterns seen in human
lungs as those found in the porcine models will strengthen the evidence of lung evaluation.
7.3.7 Evaluation of Improving Lungs
7.3 | Future Directions 7-14
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
EVLP based lung repair will rely heavily on accurate lung evaluation. Ideally, evaluation will
identify lungs needing therapy, characterize the injury for individualized therapy, and most importantly
recognize when the therapy ultimately renders the lung useable or disposable. Currently, lungs from our
injury model have deteriorated during EVLP and we believe that our evaluation technique demonstrates
this well. However, equally important is the demonstration that our evaluation technique can identify
improving lungs. Thus, one important future direction will be to develop an injury model where the
lung is initially injured, but improves over 12 hours of EVLP so that a difference in post-transplant
outcome can be seen in lungs transplanted pre- and post- EVLP. Likely, this injury model will somehow
create edema in the lungs while still in the donor which the hyperosmotic perfusate can subsequently
clear during EVLP. If EVLP can detect improvements in the compliance in this model, this will
strengthen the evidence that EVLP is able to detect repair as well as injury and will help the development
of lung repair strategies in the future.
7.3.8 Development of a Small Animal EVLP model
As more and more potential EVLP therapies are proposed, a higher throughput method of
screening for effectiveness needs to be developed to aid in the selection of therapies which show the
most clinical promise. Moreover, therapies targeting immunological pathways will benefit from access
to agents utilized by immunologists; typically, these are agents developed for small animals. To that end,
a small animal model of EVLP should be developed. Since a mature rat single lung transplantation
model exists, efforts should be made to develop a stable 12 hour normothermic lung perfusion system
for the rat lung similar to that achieved in pig and human. This model would allow researchers to more
rapidly test putative therapies than in a large animal model. In addition, rat clones are available allowing

7.4 | Summary 7-15
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
for either more in depth examination of immunologic outcomes or long-term post-transplant outcomes
without the confounding factor of rejection.
7.4 | Summary
In summary, novel therapeutics for injured donor lungs during EVLP is limited only by the
imagination of the researcher. The decades of research into molecular mechanisms of pulmonary
disease can now be targeted by therapeutics delivered to the lung. In the near-future, EVLP should be
deployed clinically to begin to reap the benefits of improved evaluation and also to begin to gain clinical
experience with the technique. Adenoviral IL-10 therapy is the most promising of the lung repair
strategies explored and clinical trials should be performed once animal survival studies are complete.

8 | References 8-1
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
8 | References
1. Cooper JD, Pearson FG, Patterson GA, Todd TR, Ginsberg RJ, Goldberg M, DeMajo WA. Technique of successful lung transplantation in humans. J Thorac Cardiovasc Surg. 1987; 93(2): 173-81.
2. Christie JD, Edwards LB, Kucheryavaya AY, Aurora P, Dobbels F, Kirk R, Rahmel AO, Stehlik J, Hertz MI. The Registry of the International Society for Heart and Lung Transplantation: twenty-seventh official adult lung and heart-lung transplant report--2010. J Heart Lung Transplant. 2010; 29(10): 1104-18.
3. Konstantinov IE. A mystery of Vladimir P. Demikhov: the 50th anniversary of the first intrathoracic transplantation. Ann Thorac Surg. 1998; 65(4): 1171-7.
4. Metras H. Note preliminarie sur la greffe total du poumon chez le chien. C R Acad Sci III. 1950; 231: 1176–7.
5. Haglin J, Telander RL, Muzzall RE, Kiser JC, Strobel CJ. Comparison of Lung Autotransplantation in the Primate and Dog. Surg Forum. 1963; 14: 196-8.
6. Hardy JD, Webb WR, Dalton ML, Jr., Walker GR, Jr. Lung Homotransplantation in Man. JAMA. 1963; 186: 1065-74.
7. Derom F, Barbier F, Ringoir S, Versieck J, Rolly G, Berzsenyi G, Vermeire P, Vrints L. Ten-month survival after lung homotransplantation in man. J Thorac Cardiovasc Surg. 1971; 61(6): 835-46.
8. Calne RY, White DJ, Thiru S, Evans DB, McMaster P, Dunn DC, Craddock GN, Pentlow BD, Rolles K. Cyclosporin A in patients receiving renal allografts from cadaver donors. Lancet. 1978; 2(8104-5): 1323-7.
9. Starzl TE, Klintmalm GB, Porter KA, Iwatsuki S, Schroter GP. Liver transplantation with use of cyclosporin a and prednisone. N Engl J Med. 1981; 305(5): 266-9.
10. Goldberg M, Lima O, Morgan E, Ayabe HA, Luk S, Ferdman A, Peters WJ, Cooper JD. A comparison between cyclosporin A and methylprednisolone plus azathioprine on bronchial healing following canine lung autotransplantation. J Thorac Cardiovasc Surg. 1983; 85(6): 821-6.
11. Patterson GA, Cooper JD, Goldman B, Weisel RD, Pearson FG, Waters PF, Todd TR, Scully H, Goldberg M, Ginsberg RJ. Technique of successful clinical double-lung transplantation. Ann Thorac Surg. 1988; 45(6): 626-33.
12. Cohen L, Littlefield C, Kelly P, Maurer J, Abbey S. Predictors of quality of life and adjustment after lung transplantation. Chest. 1998; 113(3): 633-44.
13. Gross CR, Savik K, Bolman RM, 3rd, Hertz MI. Long-term health status and quality of life outcomes of lung transplant recipients. Chest. 1995; 108(6): 1587-93.
14. Lanuza DM, Lefaiver C, Mc Cabe M, Farcas GA, Garrity E, Jr. Prospective study of functional status and quality of life before and after lung transplantation. Chest. 2000; 118(1): 115-22.
15. Reports UNfOSD. National Data. 2011 [cited 2011 January 24, 2008]; Available from: http://www.unos.org/data/about/viewDataReports.asp
16. Orens JB, Boehler A, de Perrot M, Estenne M, Glanville AR, Keshavjee S, Kotloff R, Morton J, Studer SM, Van Raemdonck D, Waddell T, Snell GI. A review of lung transplant donor acceptability criteria. J Heart Lung Transplant. 2003; 22(11): 1183-200.
17. Boasquevisque CH, Yildirim E, Waddel TK, Keshavjee S. Surgical techniques: lung transplant and lung volume reduction. Proc Am Thorac Soc. 2009; 6(1): 66-78.
18. Wijdicks EF, Varelas PN, Gronseth GS, Greer DM. Evidence-based guideline update: determining brain death in adults: report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2010; 74(23): 1911-8.
19. Smith M. Physiologic changes during brain stem death--lessons for management of the organ donor. J Heart Lung Transplant. 2004; 23(9 Suppl): S217-22.

8 | References 8-2
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
20. Schrader H, Hall C, Zwetnow NN. Effects of prolonged supratentorial mass expansion on regional blood flow and cardiovascular parameters during the Cushing response. Acta Neurol Scand. 1985; 72(3): 283-94.
21. Marshall VC. Pathophysiology of brain death: effects on allograft function. Transplant Proc. 2001; 33(1-2): 845-6.
22. Pratschke J, Wilhelm MJ, Kusaka M, Basker M, Cooper DK, Hancock WW, Tilney NL. Brain death and its influence on donor organ quality and outcome after transplantation. Transplantation. 1999; 67(3): 343-8.
23. Linos K, Fraser J, Freeman WD, Foot C. Care of the brain-dead organ donor. Current Anaesthesia & Critical Care. 2007; 18(5-6): 284-94.
24. Novitzky D, Wicomb WN, Rose AG, Cooper DK, Reichart B. Pathophysiology of pulmonary edema following experimental brain death in the chacma baboon. Ann Thorac Surg. 1987; 43(3): 288-94.
25. Takada M, Nadeau KC, Hancock WW, Mackenzie HS, Shaw GD, Waaga AM, Chandraker A, Sayegh MH, Tilney NL. Effects of explosive brain death on cytokine activation of peripheral organs in the rat. Transplantation. 1998; 65(12): 1533-42.
26. Lopau K, Mark J, Schramm L, Heidbreder E, Wanner C. Hormonal changes in brain death and immune activation in the donor. Transpl Int. 2000; 13 Suppl 1: S282-5.
27. Avlonitis VS, Fisher AJ, Kirby JA, Dark JH. Pulmonary transplantation: the role of brain death in donor lung injury. Transplantation. 2003; 75(12): 1928-33.
28. De Perrot M, Sekine Y, Fischer S, Waddell TK, McRae K, Liu M, Keshavjee S. Interleukin-8 release during ischemia-reperfusion correlates with early graft function in human lung transplantation. J Heart Lung Transplant. 2001; 20(2): 175-6.
29. De Perrot M, Sekine Y, Fischer S, Waddell TK, McRae K, Liu M, Wigle DA, Keshavjee S. Interleukin-8 release during early reperfusion predicts graft function in human lung transplantation. Am J Respir Crit Care Med. 2002; 165(2): 211-5.
30. Fisher AJ, Donnelly SC, Hirani N, Haslett C, Strieter RM, Dark JH, Corris PA. Elevated levels of interleukin-8 in donor lungs is associated with early graft failure after lung transplantation. Am J Respir Crit Care Med. 2001; 163(1): 259-65.
31. Kaneda H, Waddell TK, de Perrot M, Bai XH, Gutierrez C, Arenovich T, Chaparro C, Liu M, Keshavjee S. Pre-implantation multiple cytokine mRNA expression analysis of donor lung grafts predicts survival after lung transplantation in humans. Am J Transplant. 2006; 6(3): 544-51.
32. Barklin A. Systemic inflammation in the brain-dead organ donor. Acta Anaesthesiol Scand. 2009; 53(4): 425-35.
33. Tracey KJ. Physiology and immunology of the cholinergic antiinflammatory pathway. J Clin Invest. 2007; 117(2): 289-96.
34. Hoeger S, Bergstraesser C, Selhorst J, Fontana J, Birck R, Waldherr R, Beck G, Sticht C, Seelen MA, van Son WJ, Leuvenink H, Ploeg R, Schnuelle P, Yard BA. Modulation of brain dead induced inflammation by vagus nerve stimulation. Am J Transplant. 2010; 10(3): 477-89.
35. Scaffidi P, Misteli T, Bianchi ME. Release of chromatin protein HMGB1 by necrotic cells triggers inflammation. Nature. 2002; 418(6894): 191-5.
36. Akira S. Mammalian Toll-like receptors. Curr Opin Immunol. 2003; 15(1): 5-11. 37. Rostron AJ, Cork DM, Avlonitis VS, Fisher AJ, Dark JH, Kirby JA. Contribution of Toll-like receptor
activation to lung damage after donor brain death. Transplantation. 2010; 90(7): 732-9. 38. Norris S. Organ Donation and Transplantation in Canada. In: Division SaT, editor. Ottawa: Library of
Parliament; 2009. 39. Ipsos-Reid. Views Toward Organ and Tissue Donation and Transplantation; 2010. 40. Kootstra G, Kievit J, Nederstigt A. Organ donors: heartbeating and non-heartbeating. World J Surg.
2002; 26(2): 181-4.

8 | References 8-3
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
41. Steinbrook R. Organ donation after cardiac death. N Engl J Med. 2007; 357(3): 209-13. 42. A definition of irreversible coma. Report of the Ad Hoc Committee of the Harvard Medical School to
Examine the Definition of Brain Death. JAMA. 1968; 205(6): 337-40. 43. Egan TM, Lambert CJ, Jr., Reddick R, Ulicny KS, Jr., Keagy BA, Wilcox BR. A strategy to increase the
donor pool: use of cadaver lungs for transplantation. Ann Thorac Surg. 1991; 52(5): 1113-20; discussion 20-1.
44. Ulicny KS, Jr., Egan TM, Lambert CJ, Jr., Reddick RL, Wilcox BR. Cadaver lung donors: effect of preharvest ventilation on graft function. Ann Thorac Surg. 1993; 55(5): 1185-91.
45. Alessandrini F, D'Armini AM, Roberts CS, Reddick RL, Egan TM. When does the lung die? II. Ultrastructural evidence of pulmonary viability after "death". J Heart Lung Transplant. 1994; 13(5): 748-57.
46. D'Armini AM, Roberts CS, Griffith PK, Lemasters JJ, Egan TM. When does the lung die? I. Histochemical evidence of pulmonary viability after "death". J Heart Lung Transplant. 1994; 13(5): 741-7.
47. Egan TM. Non-heart-beating donors in thoracic transplantation. J Heart Lung Transplant. 2004; 23(1): 3-10.
48. Van Raemdonck DE, Rega FR, Neyrinck AP, Jannis N, Verleden GM, Lerut TE. Non-heart-beating donors. Semin Thorac Cardiovasc Surg. 2004; 16(4): 309-21.
49. Kootstra G, Daemen JH, Oomen AP. Categories of non-heart-beating donors. Transplant Proc. 1995; 27(5): 2893-4.
50. Sanchez-Fructuoso AI, Prats D, Torrente J, Perez-Contin MJ, Fernandez C, Alvarez J, Barrientos A. Renal transplantation from non-heart beating donors: a promising alternative to enlarge the donor pool. J Am Soc Nephrol. 2000; 11(2): 350-8.
51. Love RB, Stringham J, Chomiak PN, Pellett JR, R.M. Mentzer J. First successful lung transplantation using a nonheart-beating donor. The Journal of Heart and Lung Transplantation. 1995; 14(S): S88.
52. Love RB, D'Allesandro AM, Cornwell RA, Meyer KM. Ten year experience with human lung transplantation from non-heart beating donors. The Journal of Heart and Lung Transplantation. 2003; 22(1, Supplement 1): S87-S.
53. Steen S, Sjoberg T, Pierre L, Liao Q, Eriksson L, Algotsson L. Transplantation of lungs from a non-heart-beating donor. Lancet. 2001; 357(9259): 825-9.
54. Nunez JR, Varela A, del Rio F, Gamez P, Calatayud J, Cordoba M, Hernando F, Ussetti P, Gomez A, Carreno MC, Torres A, Gomez J, Balibrea JL, Lopez A. Bipulmonary transplants with lungs obtained from two non-heart-beating donors who died out of hospital. J Thorac Cardiovasc Surg. 2004; 127(1): 297-9.
55. Gamez P, Cordoba M, Ussetti P, Carreno MC, Alfageme F, Madrigal L, Nunez JR, Calatayud J, Ramos M, Salas C, Varela A. Lung transplantation from out-of-hospital non-heart-beating lung donors. one-year experience and results. J Heart Lung Transplant. 2005; 24(8): 1098-102.
56. de Antonio DG, Marcos R, Laporta R, Mora G, Garcia-Gallo C, Gamez P, Cordoba M, Moradiellos J, Ussetti P, Carreno MC, Nunez JR, Calatayud J, Del Rio F, Varela A. Results of clinical lung transplant from uncontrolled non-heart-beating donors. J Heart Lung Transplant. 2007; 26(5): 529-34.
57. Erasmus ME, van der Bij W, Verschuuren EAM. 56: Non-heart-beating lung donation in the Netherlands: The first experience. The Journal of Heart and Lung Transplantation. 2006; 25(2, Supplement 1): S63-S.
58. Butt TA, Aitchison JD, Corris PA, Wardle J, Clark S, Dark JH. 140: Lung transplantation from deceased donors without pretreatment. The Journal of Heart and Lung Transplantation. 2007; 26(2, Supplement 1): S110-S.

8 | References 8-4
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
59. Oto T, Levvey B, McEgan R, Davies A, Pilcher D, Williams T, Marasco S, Rosenfeldt F, Snell G. A practical approach to clinical lung transplantation from a Maastricht Category III donor with cardiac death. J Heart Lung Transplant. 2007; 26(2): 196-9.
60. Van Raemdonck D, Verleden GM, Dupont L, Van Hees D, Coosemans W, Decker G, De Leyn P, Nafteux P, Lerut T. 382: Initial Experience with Lung Transplantation from Non-Heart-Beating Donors. The Journal of Heart and Lung Transplantation. 2008; 27(2, Supplement 1): S198-S9.
61. Mason DP, Murthy SC, Gonzalez-Stawinski GV, Budev MM, Mehta AC, McNeill AM, Pettersson GB. Early experience with lung transplantation using donors after cardiac death. J Heart Lung Transplant. 2008; 27(5): 561-3.
62. Kang CH, Anraku M, Cypel M, Sato M, Yeung J, Gharib SA, Pierre AF, de Perrot M, Waddell TK, Liu M, Keshavjee S. Transcriptional signatures in donor lungs from donation after cardiac death vs after brain death: A functional pathway analysis. The Journal of Heart and Lung Transplantation. 2011; 30(3): 289-98.
63. de Perrot M, Weder W, Patterson GA, Keshavjee S. Strategies to increase limited donor resources. Eur Respir J. 2004; 23(3): 477-82.
64. Ware LB, Wang Y, Fang X, Warnock M, Sakuma T, Hall TS, Matthay M. Assessment of lungs rejected for transplantation and implications for donor selection. Lancet. 2002; 360(9333): 619-20.
65. Snell GI, Griffiths A, Levvey BJ, Oto T. Availability of lungs for transplantation: exploring the real potential of the donor pool. J Heart Lung Transplant. 2008; 27(6): 662-7.
66. Bhorade SM, Vigneswaran W, McCabe MA, Garrity ER. Liberalization of donor criteria may expand the donor pool without adverse consequence in lung transplantation. J Heart Lung Transplant. 2000; 19(12): 1199-204.
67. Botha P, Trivedi D, Weir CJ, Searl CP, Corris PA, Dark JH, Schueler SV. Extended donor criteria in lung transplantation: impact on organ allocation. J Thorac Cardiovasc Surg. 2006; 131(5): 1154-60.
68. Gabbay E, Williams TJ, Griffiths AP, Macfarlane LM, Kotsimbos TC, Esmore DS, Snell GI. Maximizing the utilization of donor organs offered for lung transplantation. Am J Respir Crit Care Med. 1999; 160(1): 265-71.
69. Kron IL, Tribble CG, Kern JA, Daniel TM, Rose CE, Truwit JD, Blackbourne LH, Bergin JD. Successful transplantation of marginally acceptable thoracic organs. Ann Surg. 1993; 217(5): 518-22; discussion 22-4.
70. Lardinois D, Banysch M, Korom S, Hillinger S, Rousson V, Boehler A, Speich R, Weder W. Extended donor lungs: eleven years experience in a consecutive series. Eur J Cardiothorac Surg. 2005; 27(5): 762-7.
71. Pierre AF, Sekine Y, Hutcheon MA, Waddell TK, Keshavjee SH. Marginal donor lungs: a reassessment. J Thorac Cardiovasc Surg. 2002; 123(3): 421-7; discussion, 7-8.
72. Sundaresan S, Semenkovich J, Ochoa L, Richardson G, Trulock EP, Cooper JD, Patterson GA. Successful outcome of lung transplantation is not compromised by the use of marginal donor lungs. J Thorac Cardiovasc Surg. 1995; 109(6): 1075-9; discussion 9-80.
73. Angel LF, Levine DJ, Restrepo MI, Johnson S, Sako E, Carpenter A, Calhoon J, Cornell JE, Adams SG, Chisholm GB, Nespral J, Roberson A, Levine SM. Impact of a lung transplantation donor-management protocol on lung donation and recipient outcomes. Am J Respir Crit Care Med. 2006; 174(6): 710-6.
74. Venkateswaran RV, Patchell VB, Wilson IC, Mascaro JG, Thompson RD, Quinn DW, Stockley RA, Coote JH, Bonser RS. Early donor management increases the retrieval rate of lungs for transplantation. Ann Thorac Surg. 2008; 85(1): 278-86; discussion 86.
75. Pennefather SH, Bullock RE, Dark JH. The effect of fluid therapy on alveolar arterial oxygen gradient in brain-dead organ donors. Transplantation. 1993; 56(6): 1418-22.

8 | References 8-5
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
76. Shemie SD, Ross H, Pagliarello J, Baker AJ, Greig PD, Brand T, Cockfield S, Keshavjee S, Nickerson P, Rao V, Guest C, Young K, Doig C. Organ donor management in Canada: recommendations of the forum on Medical Management to Optimize Donor Organ Potential. CMAJ. 2006; 174(6): S13-32.
77. Schnuelle P, Berger S, de Boer J, Persijn G, van der Woude FJ. Effects of catecholamine application to brain-dead donors on graft survival in solid organ transplantation. Transplantation. 2001; 72(3): 455-63.
78. Mukadam ME, Harrington DK, Wilson IC, Mascaro JG, Rooney SJ, Thompson RD, Nightingale P, Bonser RS. Does donor catecholamine administration affect early lung function after transplantation? J Thorac Cardiovasc Surg. 2005; 130(3): 926-7.
79. Rostron AJ, Avlonitis VS, Cork DM, Grenade DS, Kirby JA, Dark JH. Hemodynamic resuscitation with arginine vasopressin reduces lung injury after brain death in the transplant donor. Transplantation. 2008; 85(4): 597-606.
80. Pennefather SH, Bullock RE, Mantle D, Dark JH. Use of low dose arginine vasopressin to support brain-dead organ donors. Transplantation. 1995; 59(1): 58-62.
81. Debaveye YA, Van den Berghe GH. Is there still a place for dopamine in the modern intensive care unit? Anesth Analg. 2004; 98(2): 461-8.
82. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The Acute Respiratory Distress Syndrome Network. N Engl J Med. 2000; 342(18): 1301-8.
83. Follette DM, Rudich SM, Babcock WD. Improved oxygenation and increased lung donor recovery with high-dose steroid administration after brain death. J Heart Lung Transplant. 1998; 17(4): 423-9.
84. Straznicka M, Follette DM, Eisner MD, Roberts PF, Menza RL, Babcock WD. Aggressive management of lung donors classified as unacceptable: excellent recipient survival one year after transplantation. J Thorac Cardiovasc Surg. 2002; 124(2): 250-8.
85. Rosendale JD, Chabalewski FL, McBride MA, Garrity ER, Rosengard BR, Delmonico FL, Kauffman HM. Increased transplanted organs from the use of a standardized donor management protocol. Am J Transplant. 2002; 2(8): 761-8.
86. Christie JD, Sager JS, Kimmel SE, Ahya VN, Gaughan C, Blumenthal NP, Kotloff RM. Impact of primary graft failure on outcomes following lung transplantation. Chest. 2005; 127(1): 161-5.
87. Christie JD, Carby M, Bag R, Corris P, Hertz M, Weill D. Report of the ISHLT Working Group on Primary Lung Graft Dysfunction part II: definition. A consensus statement of the International Society for Heart and Lung Transplantation. J Heart Lung Transplant. 2005; 24(10): 1454-9.
88. Daud SA, Yusen RD, Meyers BF, Chakinala MM, Walter MJ, Aloush AA, Patterson GA, Trulock EP, Hachem RR. Impact of immediate primary lung allograft dysfunction on bronchiolitis obliterans syndrome. Am J Respir Crit Care Med. 2007; 175(5): 507-13.
89. de Perrot M, Liu M, Waddell TK, Keshavjee S. Ischemia-reperfusion-induced lung injury. Am J Respir Crit Care Med. 2003; 167(4): 490-511.
90. Zhao M, Fernandez LG, Doctor A, Sharma AK, Zarbock A, Tribble CG, Kron IL, Laubach VE. Alveolar macrophage activation is a key initiation signal for acute lung ischemia-reperfusion injury. Am J Physiol Lung Cell Mol Physiol. 2006; 291(5): L1018-26.
91. de Perrot M, Young K, Imai Y, Liu M, Waddell TK, Fischer S, Zhang L, Keshavjee S. Recipient T cells mediate reperfusion injury after lung transplantation in the rat. J Immunol. 2003; 171(10): 4995-5002.
92. Fiser SM, Tribble CG, Long SM, Kaza AK, Cope JT, Laubach VE, Kern JA, Kron IL. Lung transplant reperfusion injury involves pulmonary macrophages and circulating leukocytes in a biphasic response. J Thorac Cardiovasc Surg. 2001; 121(6): 1069-75.

8 | References 8-6
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
93. de Perrot M, Bonser RS, Dark J, Kelly RF, McGiffin D, Menza R, Pajaro O, Schueler S, Verleden GM. Report of the ISHLT Working Group on Primary Lung Graft Dysfunction part III: donor-related risk factors and markers. J Heart Lung Transplant. 2005; 24(10): 1460-7.
94. Shargall Y, Guenther G, Ahya VN, Ardehali A, Singhal A, Keshavjee S. Report of the ISHLT Working Group on Primary Lung Graft Dysfunction part VI: treatment. J Heart Lung Transplant. 2005; 24(10): 1489-500.
95. Meyers BF, Sundt TM, 3rd, Henry S, Trulock EP, Guthrie T, Cooper JD, Patterson GA. Selective use of extracorporeal membrane oxygenation is warranted after lung transplantation. J Thorac Cardiovasc Surg. 2000; 120(1): 20-6.
96. de Perrot M, Fischer S, Liu M, Jin R, Bai XH, Waddell TK, Keshavjee S. Prostaglandin E1 protects lung transplants from ischemia-reperfusion injury: a shift from pro- to anti-inflammatory cytokines. Transplantation. 2001; 72(9): 1505-12.
97. Keshavjee SH, Yamazaki F, Cardoso PF, McRitchie DI, Patterson GA, Cooper JD. A method for safe twelve-hour pulmonary preservation. J Thorac Cardiovasc Surg. 1989; 98(4): 529-34.
98. Keshavjee SH, Yamazaki F, Yokomise H, Cardoso PF, Mullen JB, Slutsky AS, Patterson GA. The role of dextran 40 and potassium in extended hypothermic lung preservation for transplantation. J Thorac Cardiovasc Surg. 1992; 103(2): 314-25.
99. Oto T, Griffiths AP, Rosenfeldt F, Levvey BJ, Williams TJ, Snell GI. Early outcomes comparing Perfadex, Euro-Collins, and Papworth solutions in lung transplantation. Ann Thorac Surg. 2006; 82(5): 1842-8.
100. Van Raemdonck DE, Jannis NC, Rega FR, De Leyn PR, Flameng WJ, Lerut TE. Extended preservation of ischemic pulmonary graft by postmortem alveolar expansion. Ann Thorac Surg. 1997; 64(3): 801-8.
101. Kayano K, Toda K, Naka Y, Pinsky DJ. Identification of optimal conditions for lung graft storage with Euro-Collins solution by use of a rat orthotopic lung transplant model. Circulation. 1999; 100(19 Suppl): II257-61.
102. Lee JC, Christie JD. Primary graft dysfunction. Proc Am Thorac Soc. 2009; 6(1): 39-46. 103. Carrel A, Lindbergh CA. The Culture of Whole Organs. Science. 1935; 81(2112): 621-3. 104. Jirsch DW, Fisk RL, Couves CM. Ex vivo evaluation of stored lungs. Ann Thorac Surg. 1970; 10(2): 163-
8. 105. Steen S, Liao Q, Wierup PN, Bolys R, Pierre L, Sjoberg T. Transplantation of lungs from non-heart-
beating donors after functional assessment ex vivo. Ann Thorac Surg. 2003; 76(1): 244-52; discussion 52.
106. Steen S, Ingemansson R, Eriksson L, Pierre L, Algotsson L, Wierup P, Liao Q, Eyjolfsson A, Gustafsson R, Sjoberg T. First human transplantation of a nonacceptable donor lung after reconditioning ex vivo. Ann Thorac Surg. 2007; 83(6): 2191-4.
107. Ingemansson R, Eyjolfsson A, Mared L, Pierre L, Algotsson L, Ekmehag B, Gustafsson R, Johnsson P, Koul B, Lindstedt S, Luhrs C, Sjoberg T, Steen S. Clinical transplantation of initially rejected donor lungs after reconditioning ex vivo. Ann Thorac Surg. 2009; 87(1): 255-60.
108. Erasmus ME, Fernhout MH, Elstrodt JM, Rakhorst G. Normothermic ex vivo lung perfusion of non-heart-beating donor lungs in pigs: from pretransplant function analysis towards a 6-h machine preservation. Transpl Int. 2006; 19(7): 589-93.
109. Cypel M, Yeung JC, Hirayama S, Rubacha M, Fischer S, Anraku M, Sato M, Harwood S, Pierre A, Waddell TK, de Perrot M, Liu M, Keshavjee S. Technique for prolonged normothermic ex vivo lung perfusion. J Heart Lung Transplant. 2008; 27(12): 1319-25.
110. Petak F, Habre W, Hantos Z, Sly PD, Morel DR. Effects of pulmonary vascular pressures and flow on airway and parenchymal mechanics in isolated rat lungs. . J Appl Physiol. 2002; 92: 169-78.
111. Broccard AF, Vannay C, Feihl F, Schaller MD. Impact of low pulmonary vascular pressure on ventilator-induced lung injury. Crit Care Med. 2002; 30(10): 2183-90.

8 | References 8-7
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
112. Cypel M, Rubacha M, Yeung J, Hirayama S, Torbicki K, Madonik M, Fischer S, Hwang D, Pierre A, Waddell TK, de Perrot M, Liu M, Keshavjee S. Normothermic ex vivo perfusion prevents lung injury compared to extended cold preservation for transplantation. Am J Transplant. 2009; 9(10): 2262-9.
113. Cypel M, Liu M, Rubacha M, Yeung JC, Hirayama S, Anraku M, Sato M, Medin J, Davidson BL, de Perrot M, Waddell TK, Slutsky AS, Keshavjee S. Functional repair of human donor lungs by IL-10 gene therapy. Sci Transl Med. 2009; 1(4): 4ra9.
114. Cypel M, Yeung JC, dePerrot M, Karolak W, Chen F, Sato M, Azad S, Madonik M, Hutcheon M, Chaparro C, Chow C-W, Yasufuku K, Pierre A, Singer LG, Waddell TK, Keshavjee S. Ex Vivo Lung Perfusion in Clinical Lung Transplantation – The “HELP” Trial. Journal of Heart and Lung Transplantation. 2010; 29(2): S88.
115. West JB. Respiratory Physiology: The Essentials. 8th ed: Lippincott Williams & Wilkins; 2008. 116. Ray M, Dharmarajan S, Freudenberg J, Zhang W, Patterson GA. Expression profiling of human donor
lungs to understand primary graft dysfunction after lung transplantation. Am J Transplant. 2007; 7(10): 2396-405.
117. Anraku M, Cameron MJ, Waddell TK, Liu M, Arenovich T, Sato M, Cypel M, Pierre AF, de Perrot M, Kelvin DJ, Keshavjee S. Impact of Human Donor Lung Gene Expression Profiles on Survival after Lung Transplantation: A Case-Control Study. Am J Transplant. 2008; In Press.
118. Matthay MA, Clerici C, Saumon G. Invited review: Active fluid clearance from the distal air spaces of the lung. J Appl Physiol. 2002; 93(4): 1533-41.
119. Wipper S, Dupree A, Lindner J, Sprathoff N, Pahrmann C, Reichenspurner H, Wagner FM. 330: Reconditioning of Donor Lungs after Brain Death Induced Dysfunction. The Journal of Heart and Lung Transplantation. 2008; 27(2, Supplement 1): S179-S80.
120. Inci I, Ampollini L, Arni S, Jungraithmayr W, Inci D, Hillinger S, Leskosek B, Vogt P, Weder W. Ex vivo reconditioning of marginal donor lungs injured by acid aspiration. J Heart Lung Transplant. 2008; 27(11): 1229-36.
121. Eppinger MJ, Ward PA, Bolling SF, Deeb GM. Regulatory effects of interleukin-10 on lung ischemia-reperfusion injury. J Thorac Cardiovasc Surg. 1996; 112(5): 1301-5; discussion 5-6.
122. Fischer S, Liu M, MacLean AA, de Perrot M, Ho M, Cardella JA, Zhang XM, Bai XH, Suga M, Imai Y, Keshavjee S. In vivo transtracheal adenovirus-mediated transfer of human interleukin-10 gene to donor lungs ameliorates ischemia-reperfusion injury and improves early posttransplant graft function in the rat. Hum Gene Ther. 2001; 12(12): 1513-26.
123. Itano H, Zhang W, Ritter JH, McCarthy TJ, Yew NS, Mohnanakumar T, Patterson GA. Endobronchial transfection of naked viral interleukin-10 gene in rat lung allotransplantation. Ann Thorac Surg. 2001; 71(4): 1126-33.
124. Moore KW, O'Garra A, de Waal Malefyt R, Vieira P, Mosmann TR. Interleukin-10. Annu Rev Immunol. 1993; 11: 165-90.
125. Neyer LE, Grunig G, Fort M, Remington JS, Rennick D, Hunter CA. Role of interleukin-10 in regulation of T-cell-dependent and T-cell-independent mechanisms of resistance to Toxoplasma gondii. Infect Immun. 1997; 65(5): 1675-82.
126. Wilson ME, Jeronimo SM, Pearson RD. Immunopathogenesis of infection with the visceralizing Leishmania species. Microb Pathog. 2005; 38(4): 147-60.
127. Bermejo-Martin JF, Martin-Loeches I, Rello J, Anton A, Almansa R, Xu L, Lopez-Campos G, Pumarola T, Ran L, Ramirez P, Banner D, Ng DC, Socias L, Loza A, Andaluz D, Maravi E, Gomez-Sanchez MJ, Gordon M, Gallegos MC, Fernandez V, Aldunate S, Leon C, Merino P, Blanco J, Martin-Sanchez F, Rico L, Varillas D, Iglesias V, Marcos MA, Gandia F, Bobillo F, Nogueira B, Rojo S, Resino S, Castro C, Ortiz de Lejarazu R, Kelvin D. Host adaptive immunity deficiency in severe pandemic influenza. Crit Care. 2010; 14(5): R167.

8 | References 8-8
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
128. Fiorentino DF, Bond MW, Mosmann TR. Two types of mouse T helper cell. IV. Th2 clones secrete a factor that inhibits cytokine production by Th1 clones. J Exp Med. 1989; 170(6): 2081-95.
129. Fiorentino DF, Zlotnik A, Vieira P, Mosmann TR, Howard M, Moore KW, O'Garra A. IL-10 acts on the antigen-presenting cell to inhibit cytokine production by Th1 cells. J Immunol. 1991; 146(10): 3444-51.
130. Steinbrink K, Graulich E, Kubsch S, Knop J, Enk AH. CD4(+) and CD8(+) anergic T cells induced by interleukin-10-treated human dendritic cells display antigen-specific suppressor activity. Blood. 2002; 99(7): 2468-76.
131. Steinbrink K, Jonuleit H, Muller G, Schuler G, Knop J, Enk AH. Interleukin-10-treated human dendritic cells induce a melanoma-antigen-specific anergy in CD8(+) T cells resulting in a failure to lyse tumor cells. Blood. 1999; 93(5): 1634-42.
132. de Waal Malefyt R, Yssel H, de Vries JE. Direct effects of IL-10 on subsets of human CD4+ T cell clones and resting T cells. Specific inhibition of IL-2 production and proliferation. J Immunol. 1993; 150(11): 4754-65.
133. Taga K, Mostowski H, Tosato G. Human interleukin-10 can directly inhibit T-cell growth. Blood. 1993; 81(11): 2964-71.
134. Asadullah K, Sterry W, Volk HD. Interleukin-10 therapy--review of a new approach. Pharmacol Rev. 2003; 55(2): 241-69.
135. Groux H, O'Garra A, Bigler M, Rouleau M, Antonenko S, de Vries JE, Roncarolo MG. A CD4+ T-cell subset inhibits antigen-specific T-cell responses and prevents colitis. Nature. 1997; 389(6652): 737-42.
136. Mocellin S, Panelli M, Wang E, Rossi CR, Pilati P, Nitti D, Lise M, Marincola FM. IL-10 stimulatory effects on human NK cells explored by gene profile analysis. Genes Immun. 2004; 5(8): 621-30.
137. Mocellin S, Marincola FM, Young HA. Interleukin-10 and the immune response against cancer: a counterpoint. J Leukoc Biol. 2005; 78(5): 1043-51.
138. Miura Y, Thoburn CJ, Bright EC, Chen W, Nakao S, Hess AD. Cytokine and chemokine profiles in autologous graft-versus-host disease (GVHD): interleukin 10 and interferon gamma may be critical mediators for the development of autologous GVHD. Blood. 2002; 100(7): 2650-8.
139. Itoh K, Hirohata S. The role of IL-10 in human B cell activation, proliferation, and differentiation. J Immunol. 1995; 154(9): 4341-50.
140. Itoh K, Inoue T, Ito K, Hirohata S. The interplay of interleukin-10 (IL-10) and interleukin-2 (IL-2) in humoral immune responses: IL-10 synergizes with IL-2 to enhance responses of human B lymphocytes in a mechanism which is different from upregulation of CD25 expression. Cell Immunol. 1994; 157(2): 478-88.
141. Cohen SB, Crawley JB, Kahan MC, Feldmann M, Foxwell BM. Interleukin-10 rescues T cells from apoptotic cell death: association with an upregulation of Bcl-2. Immunology. 1997; 92(1): 1-5.
142. Fujii S, Shimizu K, Shimizu T, Lotze MT. Interleukin-10 promotes the maintenance of antitumor CD8(+) T-cell effector function in situ. Blood. 2001; 98(7): 2143-51.
143. Fujii S-i, Lotze MT. IL-10 Effects on Innate Immunity. In: Marincola FM, editor. Interleukin-10. Georgetown, Texas: Landes Bioscience; 2006. p. 11-23.
144. Moore KW, de Waal Malefyt R, Coffman RL, O'Garra A. Interleukin-10 and the interleukin-10 receptor. Annu Rev Immunol. 2001; 19: 683-765.
145. Finbloom DS, Winestock KD. IL-10 induces the tyrosine phosphorylation of tyk2 and Jak1 and the differential assembly of STAT1 alpha and STAT3 complexes in human T cells and monocytes. J Immunol. 1995; 155(3): 1079-90.
146. Murray PJ. Understanding and exploiting the endogenous interleukin-10/STAT3-mediated anti-inflammatory response. Curr Opin Pharmacol. 2006; 6(4): 379-86.

8 | References 8-9
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
147. Lang R, Patel D, Morris JJ, Rutschman RL, Murray PJ. Shaping gene expression in activated and resting primary macrophages by IL-10. J Immunol. 2002; 169(5): 2253-63.
148. Asadullah K, Docke WD, Ebeling M, Friedrich M, Belbe G, Audring H, Volk HD, Sterry W. Interleukin 10 treatment of psoriasis: clinical results of a phase 2 trial. Arch Dermatol. 1999; 135(2): 187-92.
149. Fedorak RN, Gangl A, Elson CO, Rutgeerts P, Schreiber S, Wild G, Hanauer SB, Kilian A, Cohard M, LeBeaut A, Feagan B. Recombinant human interleukin 10 in the treatment of patients with mild to moderately active Crohn's disease. The Interleukin 10 Inflammatory Bowel Disease Cooperative Study Group. Gastroenterology. 2000; 119(6): 1473-82.
150. Heller LC, Heller R. In vivo electroporation for gene therapy. Hum Gene Ther. 2006; 17(9): 890-7. 151. Boasquevisque CH, Mora BN, Boglione M, Ritter JK, Scheule RK, Yew N, Debruyne L, Qin L, Bromberg
JS, Patterson GA. Liposome-mediated gene transfer in rat lung transplantation: A comparison between the in vivo and ex vivo approaches. J Thorac Cardiovasc Surg. 1999; 117(1): 8-14; discussion -5.
152. Martins S, de Perrot M, Imai Y, Yamane M, Quadri SM, Segall L, Dutly A, Sakiyama S, Chaparro A, Davidson BL, Waddell TK, Liu M, Keshavjee S. Transbronchial administration of adenoviral-mediated interleukin-10 gene to the donor improves function in a pig lung transplant model. Gene Ther. 2004; 11(24): 1786-96.
153. Kay MA, Glorioso JC, Naldini L. Viral vectors for gene therapy: the art of turning infectious agents into vehicles of therapeutics. Nat Med. 2001; 7(1): 33-40.
154. Wilson JM. Adenoviruses as gene-delivery vehicles. N Engl J Med. 1996; 334(18): 1185-7. 155. Horwitz MS. Adenoviruses. In: Fields BN, Knipe DM, Howley PM, editors. Fields Virology.
Philadelphia: Lippincott-Raven Publishers, Inc.; 1996. p. 2149-71. 156. Shenk T. Adenoviridae: The viruses and their replication. In: Fields BN, Knipe DM, Howley PM,
editors. Fields Virology. Philadelphia: Lippincott-Raven Publishers, Inc.; 1996. p. 2111-48. 157. Reddy VS, Natchiar SK, Stewart PL, Nemerow GR. Crystal structure of human adenovirus at 3.5 A
resolution. Science. 2010; 329(5995): 1071-5. 158. Athappilly FK, Murali R, Rux JJ, Cai Z, Burnett RM. The refined crystal structure of hexon, the major
coat protein of adenovirus type 2, at 2.9 A resolution. J Mol Biol. 1994; 242(4): 430-55. 159. Bergelson JM, Cunningham JA, Droguett G, Kurt-Jones EA, Krithivas A, Hong JS, Horwitz MS, Crowell
RL, Finberg RW. Isolation of a common receptor for Coxsackie B viruses and adenoviruses 2 and 5. Science. 1997; 275(5304): 1320-3.
160. Roelvink PW, Lizonova A, Lee JG, Li Y, Bergelson JM, Finberg RW, Brough DE, Kovesdi I, Wickham TJ. The coxsackievirus-adenovirus receptor protein can function as a cellular attachment protein for adenovirus serotypes from subgroups A, C, D, E, and F. J Virol. 1998; 72(10): 7909-15.
161. Glasgow JN, Everts M, Curiel DT. Transductional targeting of adenovirus vectors for gene therapy. Cancer Gene Ther. 2006; 13(9): 830-44.
162. Wickham TJ, Mathias P, Cheresh DA, Nemerow GR. Integrins alpha v beta 3 and alpha v beta 5 promote adenovirus internalization but not virus attachment. Cell. 1993; 73(2): 309-19.
163. Wang K, Huang S, Kapoor-Munshi A, Nemerow G. Adenovirus internalization and infection require dynamin. J Virol. 1998; 72(4): 3455-8.
164. Trotman LC, Mosberger N, Fornerod M, Stidwill RP, Greber UF. Import of adenovirus DNA involves the nuclear pore complex receptor CAN/Nup214 and histone H1. Nat Cell Biol. 2001; 3(12): 1092-100.
165. Contreras JL, Smyth CA, Curiel DT, Eckhoff DE. Nonhuman primate models in type 1 diabetes research. ILAR J. 2004; 45(3): 334-42.
166. Akusjarvi G. Proteins with transcription regulatory properties encoded by human adenoviruses. Trends Microbiol. 1993; 1(5): 163-70.
167. Steegenga WT, Shvarts A, Riteco N, Bos JL, Jochemsen AG. Distinct regulation of p53 and p73 activity by adenovirus E1A, E1B, and E4orf6 proteins. Mol Cell Biol. 1999; 19(5): 3885-94.

8 | References 8-10
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
168. Swaminathan S, Thimmapaya B. Regulation of adenovirus E2 transcription unit. Curr Top Microbiol Immunol. 1995; 199 ( Pt 3): 177-94.
169. Wold WS, Tollefson AE, Hermiston TW. E3 transcription unit of adenovirus. Curr Top Microbiol Immunol. 1995; 199 ( Pt 1): 237-74.
170. Bridge E, Ketner G. Redundant control of adenovirus late gene expression by early region 4. J Virol. 1989; 63(2): 631-8.
171. Shaw AR, Ziff EB. Transcripts from the adenovirus-2 major late promoter yield a single early family of 3' coterminal mRNAs and five late families. Cell. 1980; 22(3): 905-16.
172. Bett AJ, Prevec L, Graham FL. Packaging capacity and stability of human adenovirus type 5 vectors. J Virol. 1993; 67(10): 5911-21.
173. Graham FL, Smiley J, Russell WC, Nairn R. Characteristics of a human cell line transformed by DNA from human adenovirus type 5. J Gen Virol. 1977; 36(1): 59-74.
174. He TC, Zhou S, da Costa LT, Yu J, Kinzler KW, Vogelstein B. A simplified system for generating recombinant adenoviruses. Proc Natl Acad Sci U S A. 1998; 95(5): 2509-14.
175. McCoy RD, Davidson BL, Roessler BJ, Huffnagle GB, Janich SL, Laing TJ, Simon RH. Pulmonary inflammation induced by incomplete or inactivated adenoviral particles. Hum Gene Ther. 1995; 6(12): 1553-60.
176. Worgall S, Leopold PL, Wolff G, Ferris B, Van Roijen N, Crystal RG. Role of alveolar macrophages in rapid elimination of adenovirus vectors administered to the epithelial surface of the respiratory tract. Hum Gene Ther. 1997; 8(14): 1675-84.
177. Raper SE, Yudkoff M, Chirmule N, Gao GP, Nunes F, Haskal ZJ, Furth EE, Propert KJ, Robinson MB, Magosin S, Simoes H, Speicher L, Hughes J, Tazelaar J, Wivel NA, Wilson JM, Batshaw ML. A pilot study of in vivo liver-directed gene transfer with an adenoviral vector in partial ornithine transcarbamylase deficiency. Hum Gene Ther. 2002; 13(1): 163-75.
178. Bals R, Hiemstra PS. Innate immunity in the lung: how epithelial cells fight against respiratory pathogens. Eur Respir J. 2004; 23(2): 327-33.
179. Diamond G, Legarda D, Ryan LK. The innate immune response of the respiratory epithelium. Immunol Rev. 2000; 173: 27-38.
180. Bianchi ME. DAMPs, PAMPs and alarmins: all we need to know about danger. J Leukoc Biol. 2007; 81(1): 1-5.
181. Manicassamy S, Pulendran B. Modulation of adaptive immunity with Toll-like receptors. Semin Immunol. 2009; 21(4): 185-93.
182. Katakura K, Lee J, Rachmilewitz D, Li G, Eckmann L, Raz E. Toll-like receptor 9-induced type I IFN protects mice from experimental colitis. J Clin Invest. 2005; 115(3): 695-702.
183. Garcia-Sastre A, Biron CA. Type 1 interferons and the virus-host relationship: a lesson in detente. Science. 2006; 312(5775): 879-82.
184. Otake K, Ennist DL, Harrod K, Trapnell BC. Nonspecific inflammation inhibits adenovirus-mediated pulmonary gene transfer and expression independent of specific acquired immune responses. Hum Gene Ther. 1998; 9(15): 2207-22.
185. Philpott NJ, Nociari M, Elkon KB, Falck-Pedersen E. Adenovirus-induced maturation of dendritic cells through a PI3 kinase-mediated TNF-alpha induction pathway. Proc Natl Acad Sci U S A. 2004; 101(16): 6200-5.
186. Lieber A, He CY, Meuse L, Schowalter D, Kirillova I, Winther B, Kay MA. The role of Kupffer cell activation and viral gene expression in early liver toxicity after infusion of recombinant adenovirus vectors. J Virol. 1997; 71(11): 8798-807.
187. Borgland SL, Bowen GP, Wong NC, Libermann TA, Muruve DA. Adenovirus vector-induced expression of the C-X-C chemokine IP-10 is mediated through capsid-dependent activation of NF-kappaB. J Virol. 2000; 74(9): 3941-7.

8 | References 8-11
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
188. Suda T, Tagawa T, Kanaan SA, Kozower BD, Daddi N, Mohanakumar T, Patterson GA. Adenovirus encoding soluble tumor necrosis factor alpha receptor immunoglobulin prolongs gene expression of a cotransfected reporter gene in rat lung. J Thorac Cardiovasc Surg. 2003; 126(4): 1155-61.
189. Liu Q, Zaiss AK, Colarusso P, Patel K, Haljan G, Wickham TJ, Muruve DA. The role of capsid-endothelial interactions in the innate immune response to adenovirus vectors. Hum Gene Ther. 2003; 14(7): 627-43.
190. Zsengeller Z, Otake K, Hossain SA, Berclaz PY, Trapnell BC. Internalization of adenovirus by alveolar macrophages initiates early proinflammatory signaling during acute respiratory tract infection. J Virol. 2000; 74(20): 9655-67.
191. Kuzmin AI, Finegold MJ, Eisensmith RC. Macrophage depletion increases the safety, efficacy and persistence of adenovirus-mediated gene transfer in vivo. Gene Ther. 1997; 4(4): 309-16.
192. Muruve DA, Barnes MJ, Stillman IE, Libermann TA. Adenoviral gene therapy leads to rapid induction of multiple chemokines and acute neutrophil-dependent hepatic injury in vivo. Hum Gene Ther. 1999; 10(6): 965-76.
193. Ruzek MC, Kavanagh BF, Scaria A, Richards SM, Garman RD. Adenoviral vectors stimulate murine natural killer cell responses and demonstrate antitumor activities in the absence of transgene expression. Mol Ther. 2002; 5(2): 115-24.
194. DeMatteo RP, Chu G, Ahn M, Chang E, Burke C, Raper SE, Barker CF, Markmann JF. Immunologic barriers to hepatic adenoviral gene therapy for transplantation. Transplantation. 1997; 63(2): 315-9.
195. Yang Y, Li Q, Ertl HC, Wilson JM. Cellular and humoral immune responses to viral antigens create barriers to lung-directed gene therapy with recombinant adenoviruses. J Virol. 1995; 69(4): 2004-15.
196. Zhang Y, Chirmule N, Gao GP, Qian R, Croyle M, Joshi B, Tazelaar J, Wilson JM. Acute cytokine response to systemic adenoviral vectors in mice is mediated by dendritic cells and macrophages. Mol Ther. 2001; 3(5 Pt 1): 697-707.
197. Peng Y, Falck-Pedersen E, Elkon KB. Variation in adenovirus transgene expression between BALB/c and C57BL/6 mice is associated with differences in interleukin-12 and gamma interferon production and NK cell activation. J Virol. 2001; 75(10): 4540-50.
198. Jooss K, Yang Y, Wilson JM. Cyclophosphamide diminishes inflammation and prolongs transgene expression following delivery of adenoviral vectors to mouse liver and lung. Hum Gene Ther. 1996; 7(13): 1555-66.
199. Fang B, Eisensmith RC, Wang H, Kay MA, Cross RE, Landen CN, Gordon G, Bellinger DA, Read MS, Hu PC, et al. Gene therapy for hemophilia B: host immunosuppression prolongs the therapeutic effect of adenovirus-mediated factor IX expression. Hum Gene Ther. 1995; 6(8): 1039-44.
200. Suga M, Gladdy R, Xing Z, Keshavjee SH, Liu M. Transplant immunosuppression enhances efficiency of adenoviral-mediated gene retransfection: inhibition of interferon-gamma and immunoglobin G. Ann Thorac Surg. 2002; 73(4): 1092-7.
201. Dhand R. Basic techniques for aerosol delivery during mechanical ventilation. Respir Care. 2004; 49(6): 611-22.
202. Ip AY, Arakawa T, Silvers H, Ransone CM, Niven RW. Stability of recombinant consensus interferon to air-jet and ultrasonic nebulization. J Pharm Sci. 1995; 84(10): 1210-4.
203. Waldrep JC, Dhand R. Advanced nebulizer designs employing vibrating mesh/aperture plate technologies for aerosol generation. Curr Drug Deliv. 2008; 5(2): 114-9.
204. Johnson JC, Waldrep JC, Guo J, Dhand R. Aerosol delivery of recombinant human DNase I: in vitro comparison of a vibrating-mesh nebulizer with a jet nebulizer. Respir Care. 2008; 53(12): 1703-8.
205. Usmani OS, Biddiscombe MF, Barnes PJ. Regional lung deposition and bronchodilator response as a function of beta2-agonist particle size. Am J Respir Crit Care Med. 2005; 172(12): 1497-504.
206. Coates AL. Guiding aerosol deposition in the lung. N Engl J Med. 2008; 358(3): 304-5.

8 | References 8-12
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
207. de Perrot M, Fischer S, Liu M, Imai Y, Martins S, Sakiyama S, Tabata T, Bai XH, Waddell TK, Davidson BL, Keshavjee S. Impact of human interleukin-10 on vector-induced inflammation and early graft function in rat lung transplantation. Am J Respir Cell Mol Biol. 2003; 28(5): 616-25.
208. Thomassen MJ, Divis LT, Fisher CJ. Regulation of human alveolar macrophage inflammatory cytokine production by interleukin-10. Clin Immunol Immunopathol. 1996; 80(3 Pt 1): 321-4.
209. Radwanski E, Chakraborty A, Van Wart S, Huhn RD, Cutler DL, Affrime MB, Jusko WJ. Pharmacokinetics and leukocyte responses of recombinant human interleukin-10. Pharm Res. 1998; 15(12): 1895-901.
210. Naidu BV, Krishnadasan B, Farivar AS, Woolley SM, Thomas R, Van Rooijen N, Verrier ED, Mulligan MS. Early activation of the alveolar macrophage is critical to the development of lung ischemia-reperfusion injury. J Thorac Cardiovasc Surg. 2003; 126(1): 200-7.
211. McAuliffe PF, Murday ME, Efron PA, Scumpia PO, Ungaro R, Abouhamze A, Tannahill CL, Hutchins B, LaFace D, Moldawer LL. Dose-dependent improvements in outcome with adenoviral expression of interleukin-10 in a murine model of multisystem organ failure. Gene Ther. 2006; 13(3): 276-82.
212. Minter RM, Ferry MA, Rectenwald JE, Bahjat FR, Oberholzer A, Oberholzer C, La Face D, Tsai V, Ahmed CM, Hutchins B, Copeland EM, 3rd, Ginsberg HS, Moldawer LL. Extended lung expression and increased tissue localization of viral IL-10 with adenoviral gene therapy. Proc Natl Acad Sci U S A. 2001; 98(1): 277-82.
213. Cassivi SD, Cardella JA, Fischer S, Liu M, Slutsky AS, Keshavjee S. Transtracheal gene transfection of donor lungs prior to organ procurement increases transgene levels at reperfusion and following transplantation. J Heart Lung Transplant. 1999; 18(12): 1181-8.
214. Pierre AF, Xavier AM, Liu M, Cassivi SD, Lindsay TF, Marsh HC, Slutsky AS, Keshavjee SH. Effect of complement inhibition with soluble complement receptor 1 on pig allotransplant lung function. Transplantation. 1998; 66(6): 723-32.
215. Nishina K, Mikawa K, Takao Y, Maekawa N, Shiga M, Obara H. ONO-5046, an elastase inhibitor, attenuates endotoxin-induced acute lung injury in rabbits. Anesth Analg. 1997; 84(5): 1097.
216. Novitzky D, Horak A, Cooper DK, Rose AG. Electrocardiographic and histopathologic changes developing during experimental brain death in the baboon. Transplant Proc. 1989; 21(1 Pt 3): 2567-9.
217. Hidalgo MA, Shah KA, Fuller BJ, Green CJ. Cold ischemia-induced damage to vascular endothelium results in permeability alterations in transplanted lungs. J Thorac Cardiovasc Surg. 1996; 112(4): 1027-35.
218. Novick RJ, Gehman KE, Ali IS, Lee J. Lung preservation: the importance of endothelial and alveolar type II cell integrity. Ann Thorac Surg. 1996; 62(1): 302-14.
219. Staub NC, Nagano H, Pearce ML. Pulmonary edema in dogs, especially the sequence of fluid accumulation in lungs. J Appl Physiol. 1967; 22(2): 227-40.
220. Koike T, Yeung JC, Cypel M, Matsuda Y, Rubacha M, Liu M, Waddell TK, Keshavjee S. Lactate and Lactate/Pyruvate Ratio During Acellular Normothermic Ex Vivo Rejected and Clinical Human Lung Perfusion. . Transplantation. 2010; 90(355): S342.
221. Lejeune P, Brimioulle S, Leeman M, Hallemans R, Melot C, Naeije R. Enhancement of hypoxic pulmonary vasoconstriction by metabolic acidosis in dogs. Anesthesiology. 1990; 73(2): 256-64.
222. Wierup P, Haraldsson A, Nilsson F, Pierre L, Schersten H, Silverborn M, Sjoberg T, Westfeldt U, Steen S. Ex vivo evaluation of nonacceptable donor lungs. Ann Thorac Surg. 2006; 81(2): 460-6.
223. Egan TM, Haithcock JA, Nicotra WA, Koukoulis G, Inokawa H, Sevala M, Molina PL, Funkhouser WK, Mattice BJ. Ex vivo evaluation of human lungs for transplant suitability. Ann Thorac Surg. 2006; 81(4): 1205-13.
224. Ding Y, Qin L, Kotenko SV, Pestka S, Bromberg JS. A single amino acid determines the immunostimulatory activity of interleukin 10. J Exp Med. 2000; 191(2): 213-24.

8 | References 8-13
Ex vivo Lung Perfusion: A Platform for Lung Evaluation and Repair
225. Yang T, Duan R, Cao H, Lee BH, Xia C, Chang Z, Keith Tanswell A, Hu J. Development of an inflammation-inducible gene expression system using helper-dependent adenoviral vectors. J Gene Med. 2010; 12(10): 832-9.
226. Sipo I, Hurtado Pico A, Wang X, Eberle J, Petersen I, Weger S, Poller W, Fechner H. An improved Tet-On regulatable FasL-adenovirus vector system for lung cancer therapy. J Mol Med (Berl). 2006; 84(3): 215-25.