EWMA 2013 - Ep462 - How about the Free Flap as the First Choice of Treatment for Diabetic foot?:...
10
How about the Free Flap as the First Choice of Treatment for Diabetic foot?: Tips for Success. Donghyeok Shin, M.D., Ph.D. Department of Plastic and Reconstructive Surgery Konkuk University Medical Center
-
Upload
ewma -
Category
Health & Medicine
-
view
90 -
download
1
Transcript of EWMA 2013 - Ep462 - How about the Free Flap as the First Choice of Treatment for Diabetic foot?:...

How about the Free Flap as the
First Choice of Treatment for
Diabetic foot?: Tips for Success.
Donghyeok Shin, M.D., Ph.D.
Department of Plastic and Reconstructive Surgery
Konkuk University Medical Center

Where Dose It Occur Frequently?
Mostly,
Prehensile area
Weight bearing area

What Should Reconstruction Provide?
• Well-vascularized tissue
• Protection
– Proper padding
– Durable skin
– Enduring shearing force
• Good contour

Which Flap Is the Most Proper?
• Local flap
• Distant flap
• Free flap

Conflict of Local and Distant Flap
• When
–Significant occlusion of vasculature
–Distal circulation depending on few
collaterals

Can you guarantee the
survival of local or distant
flap in patient with this
vascular status?
Patients and Methods
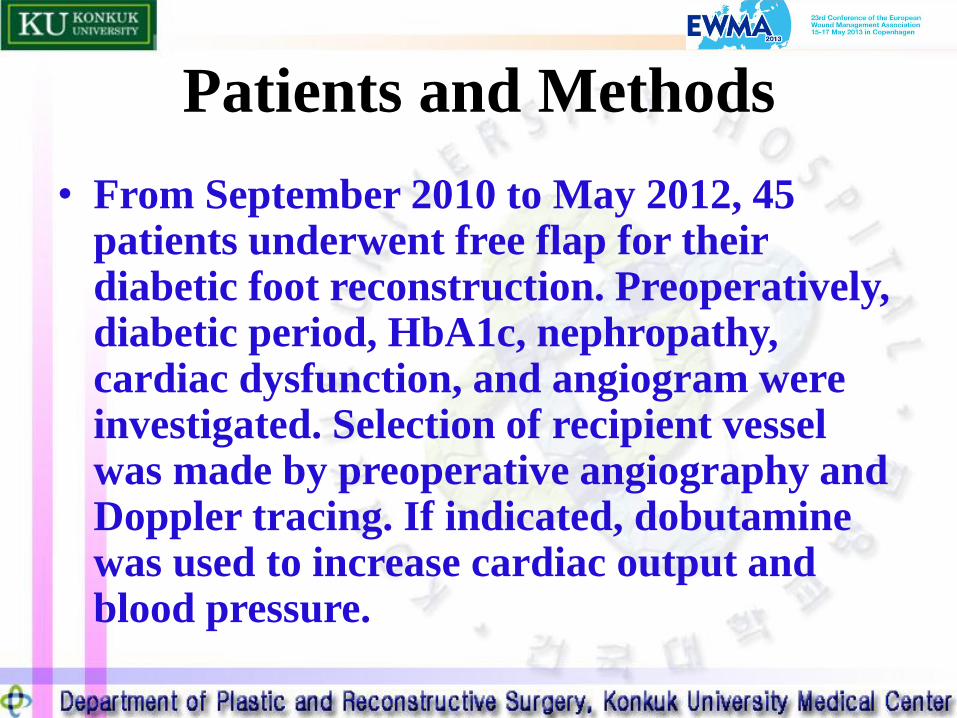
• From September 2010 to May 2012, 45 patients underwent free flap for their diabetic foot reconstruction. Preoperatively, diabetic period, HbA1c, nephropathy, cardiac dysfunction, and angiogram were investigated. Selection of recipient vessel was made by preoperative angiography and Doppler tracing. If indicated, dobutamine was used to increase cardiac output and blood pressure.

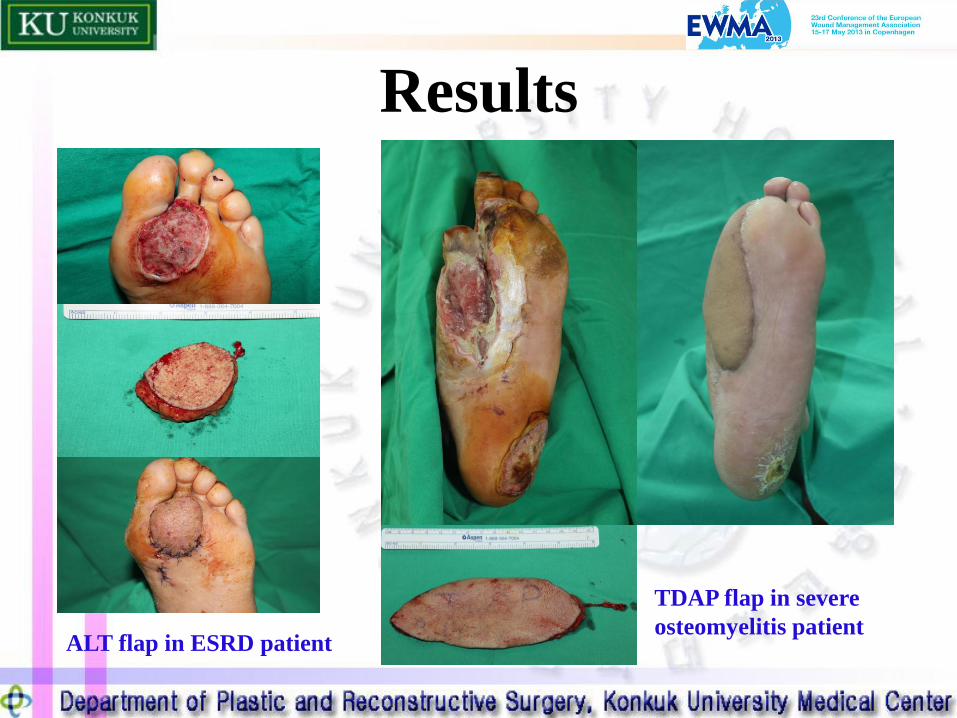
Results
• Overall, there were 7 total and 9 partial losses. 39 patients had preoperative interventional angioplasty and 7 total losses occurred in this group. In six patients, major vessels were used as recipient. Among six cases, 3 flaps were totally failed, and one showed partial loss. In case of 4 end-stage renal disease(ESRD), every flap survived completely. In five cases that had dobutamine infusion, there were one total and one partial loss.
Results
ALT flap in ESRD patient
TDAP flap in severe
osteomyelitis patient

Personal Surgical Protocol and Conclusion
• Thorough preoperative cardiovascular evaluation
and aggressive intervention
• Perfect eradication of infection
• Never use tourniquet
• Terminal branch as recipient vessel
• Never hesitate to use dobutamine
• Continuous postoperative heparinization